

Abstract
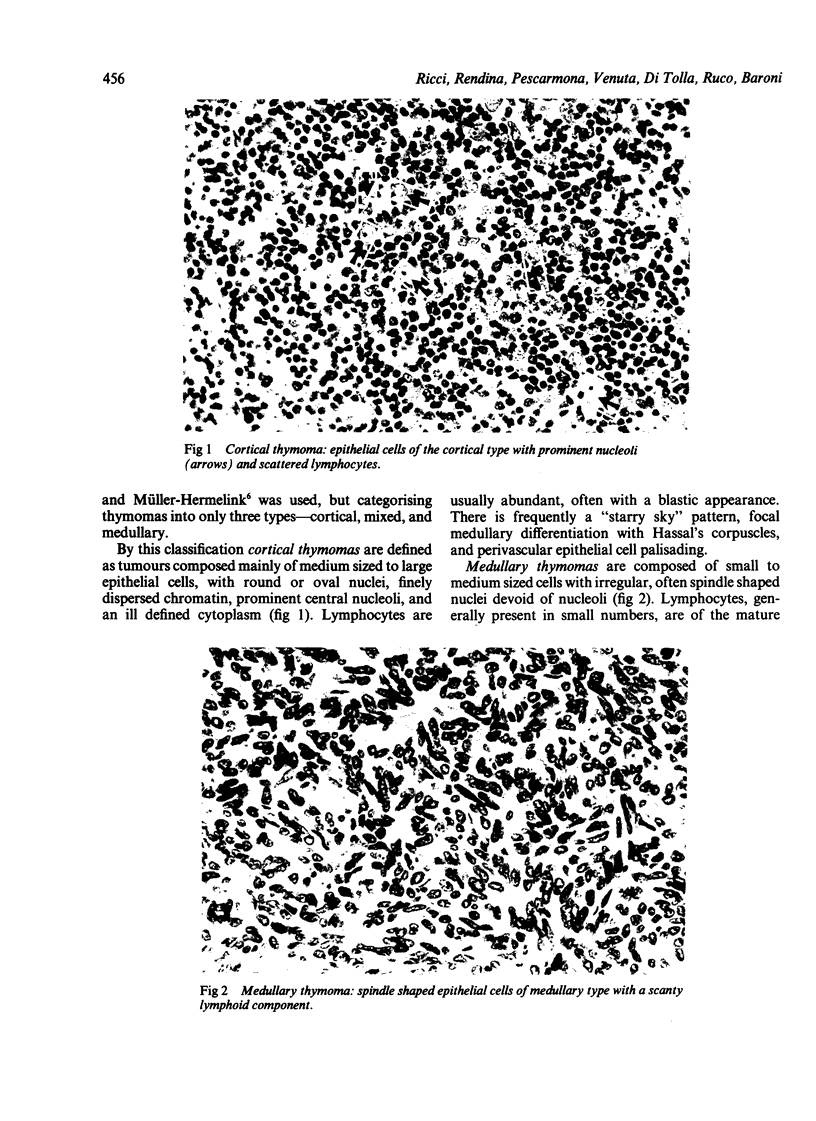
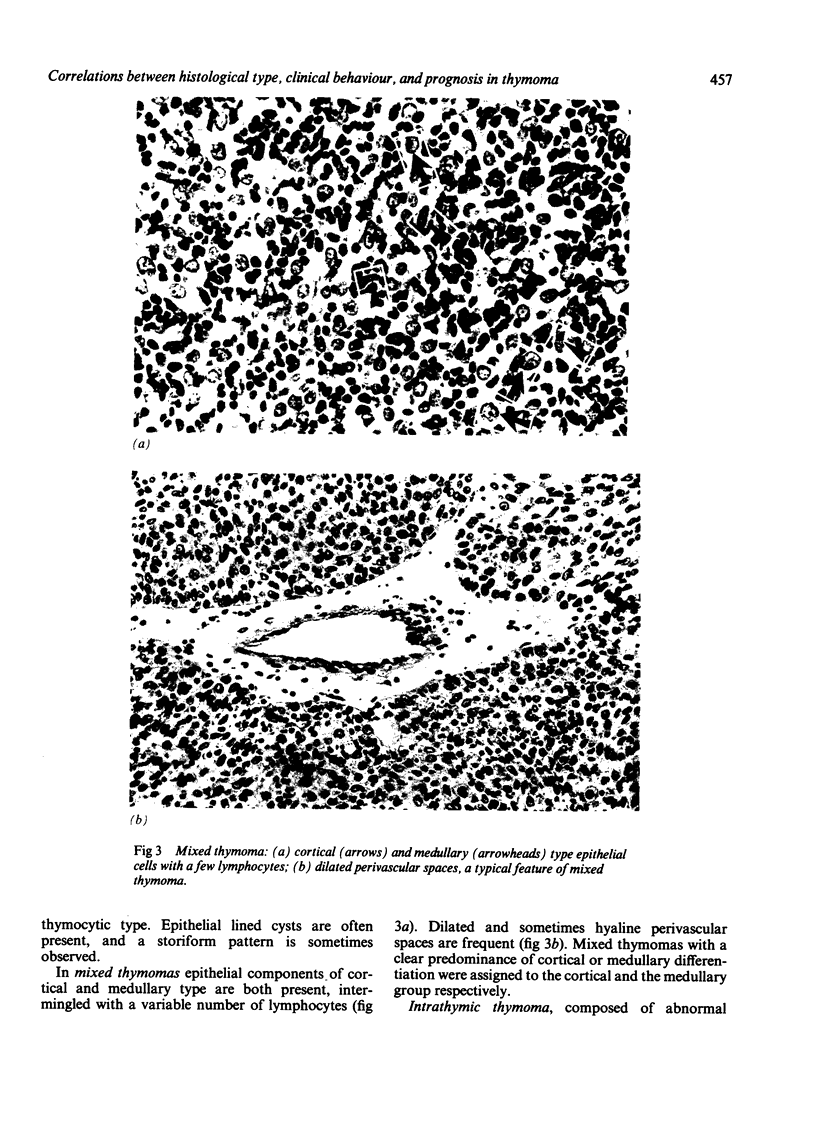
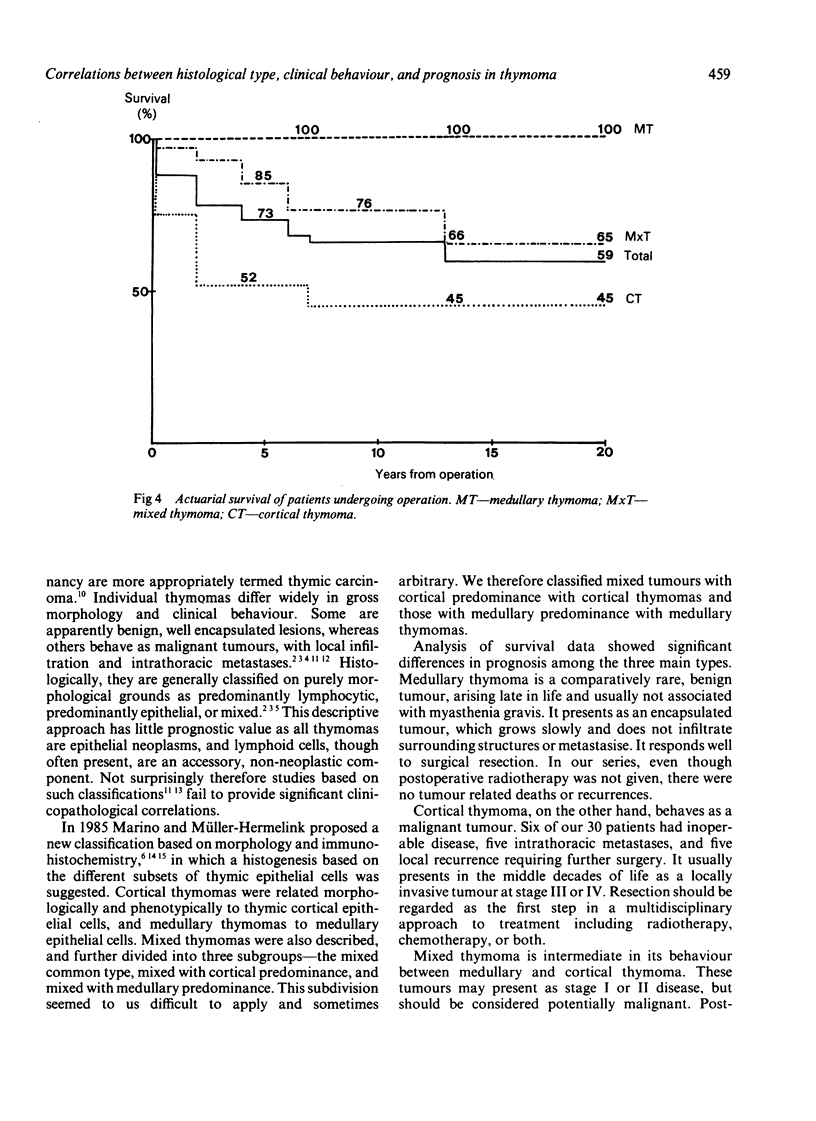
Seventy four cases of thymoma were reclassified into three histological categories--cortical (30), medullary (9), and mixed (34) (the remaining patient had an intrathymic thymoma)--for an investigation of the relation between histological type, clinical behaviour, and long term prognosis. There were significant differences between the histological types in the frequency of myasthenia gravis and of the different tumour stages, the mean age of the patients, and prognosis. Myasthenia gravis occurred more commonly in patients with cortical (33%) and mixed thymoma (35%) than in patients with medullary thymoma (11%). Five, 10, 15, and 20 year actuarial survival was 100% for medullary thymoma; 85%, 76%, 65% and 65% respectively for mixed thymoma; and 52%, 45%, 45%, and 45% for cortical thymoma. Medullary thymoma is a benign tumour arising late in life and there was no mortality in this series after surgery alone. Cortical thymoma usually presented in middle age and must be regarded as malignant; mortality was 50% at five years despite a multidisciplinary approach, with surgery and postoperative radiotherapy in all patients and chemotherapy in selected cases. Mixed thymoma had a better prognosis than cortical thymoma, but must be regarded as potentially malignant. One third of the total patients had died by 10 years despite radical tumour resection.
Full text
PDF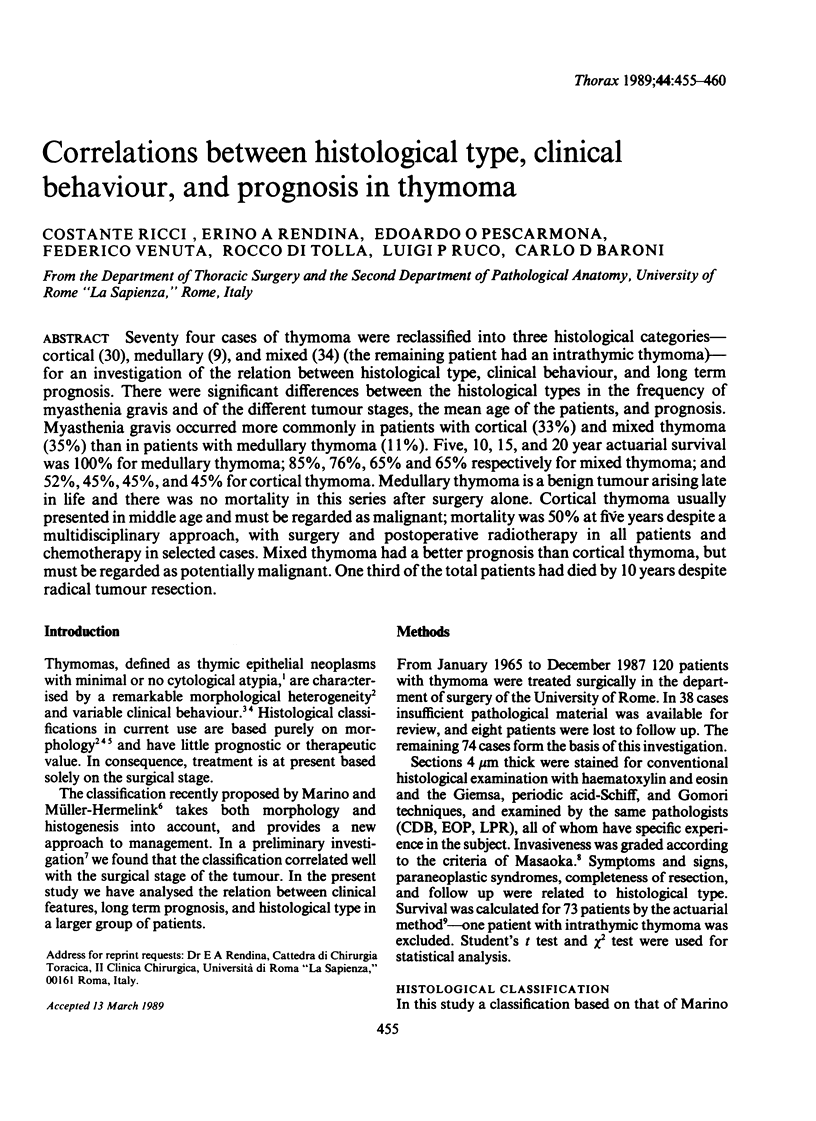
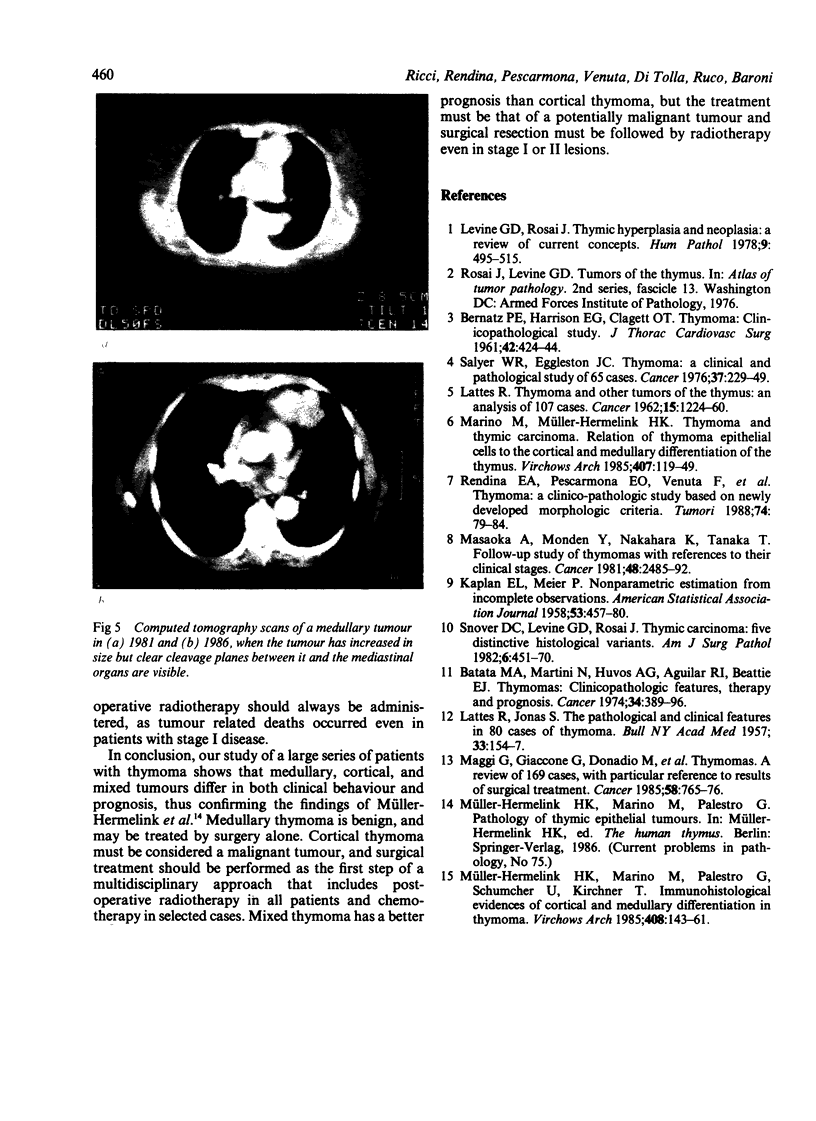
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BERNATZ P. E., HARRISON E. G., CLAGETT O. T. Thymoma: a clinicopathologic study. J Thorac Cardiovasc Surg. 1961 Oct;42:424–444. [PubMed] [Google Scholar]
- Batata M. A., Martini N., Huvos A. G., Aguilar R. I., Beattie E. J., Jr Thymomas: clinicopathologic features, therapy, and prognosis. Cancer. 1974 Aug;34(2):389–396. doi: 10.1002/1097-0142(197408)34:2<389::aid-cncr2820340224>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- Levine G. D., Rosai J. Thymic hyperplasia and neoplasia: a review of current concepts. Hum Pathol. 1978 Sep;9(5):495–515. doi: 10.1016/s0046-8177(78)80131-2. [DOI] [PubMed] [Google Scholar]
- Maggi G., Giaccone G., Donadio M., Ciuffreda L., Dalesio O., Leria G., Trifiletti G., Casadio C., Palestro G., Mancuso M. Thymomas. A review of 169 cases, with particular reference to results of surgical treatment. Cancer. 1986 Aug 1;58(3):765–776. doi: 10.1002/1097-0142(19860801)58:3<765::aid-cncr2820580326>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- Marino M., Müller-Hermelink H. K. Thymoma and thymic carcinoma. Relation of thymoma epithelial cells to the cortical and medullary differentiation of thymus. Virchows Arch A Pathol Anat Histopathol. 1985;407(2):119–149. doi: 10.1007/BF00737071. [DOI] [PubMed] [Google Scholar]
- Müller-Hermelink H. K., Marino M., Palestro G., Schumacher U., Kirchner T. Immunohistological evidences of cortical and medullary differentiation in thymoma. Virchows Arch A Pathol Anat Histopathol. 1985;408(2-3):143–161. doi: 10.1007/BF00707978. [DOI] [PubMed] [Google Scholar]
- Rendina E. A., Pescarmona E. O., Venuta F., Nardi S., De Rosa G., Martelli M., Ricci C. Thymoma: a clinico-pathologic study based on newly developed morphologic criteria. Tumori. 1988 Feb 29;74(1):79–84. doi: 10.1177/030089168807400114. [DOI] [PubMed] [Google Scholar]
- Salyer W. R., Eggleston J. C. Thymoma: a clinical and pathological study of 65 cases. Cancer. 1976 Jan;37(1):229–249. doi: 10.1002/1097-0142(197601)37:1<229::aid-cncr2820370133>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- Snover D. C., Levine G. D., Rosai J. Thymic carcinoma. Five distinctive histological variants. Am J Surg Pathol. 1982 Jul;6(5):451–470. [PubMed] [Google Scholar]