

Abstract
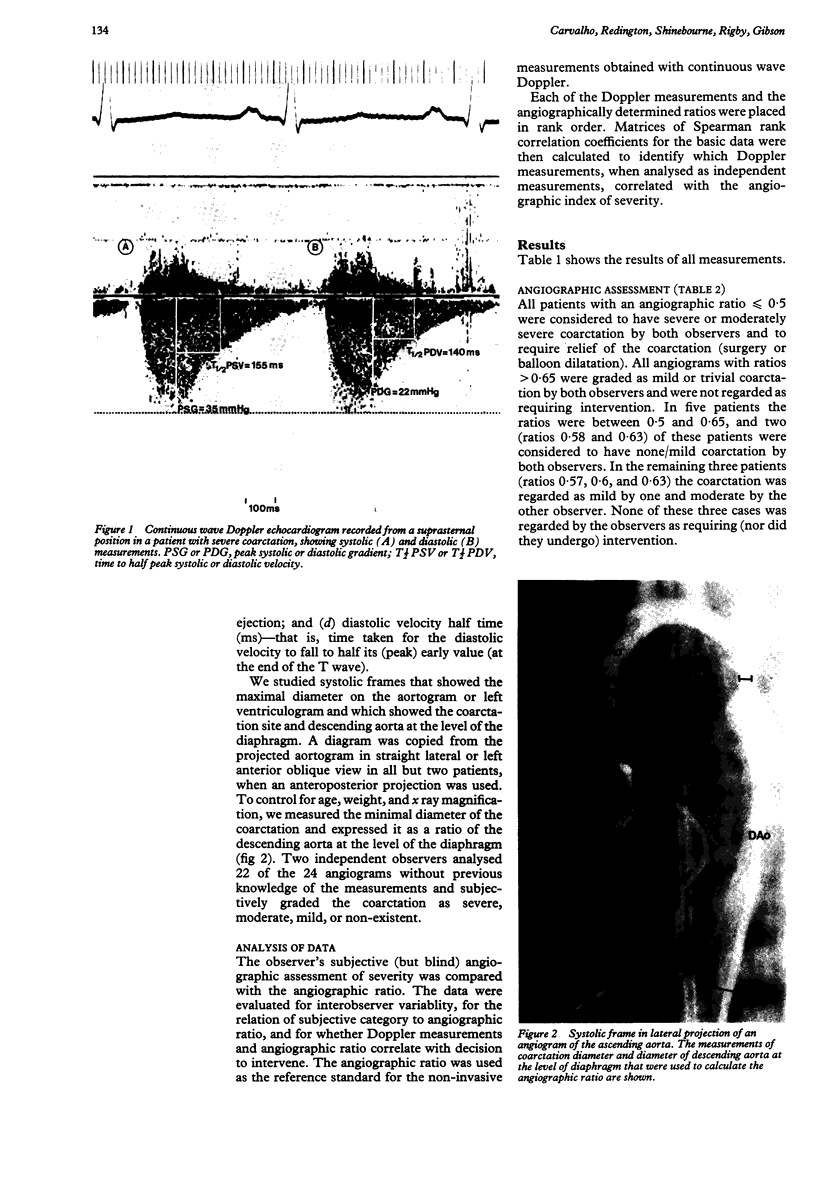
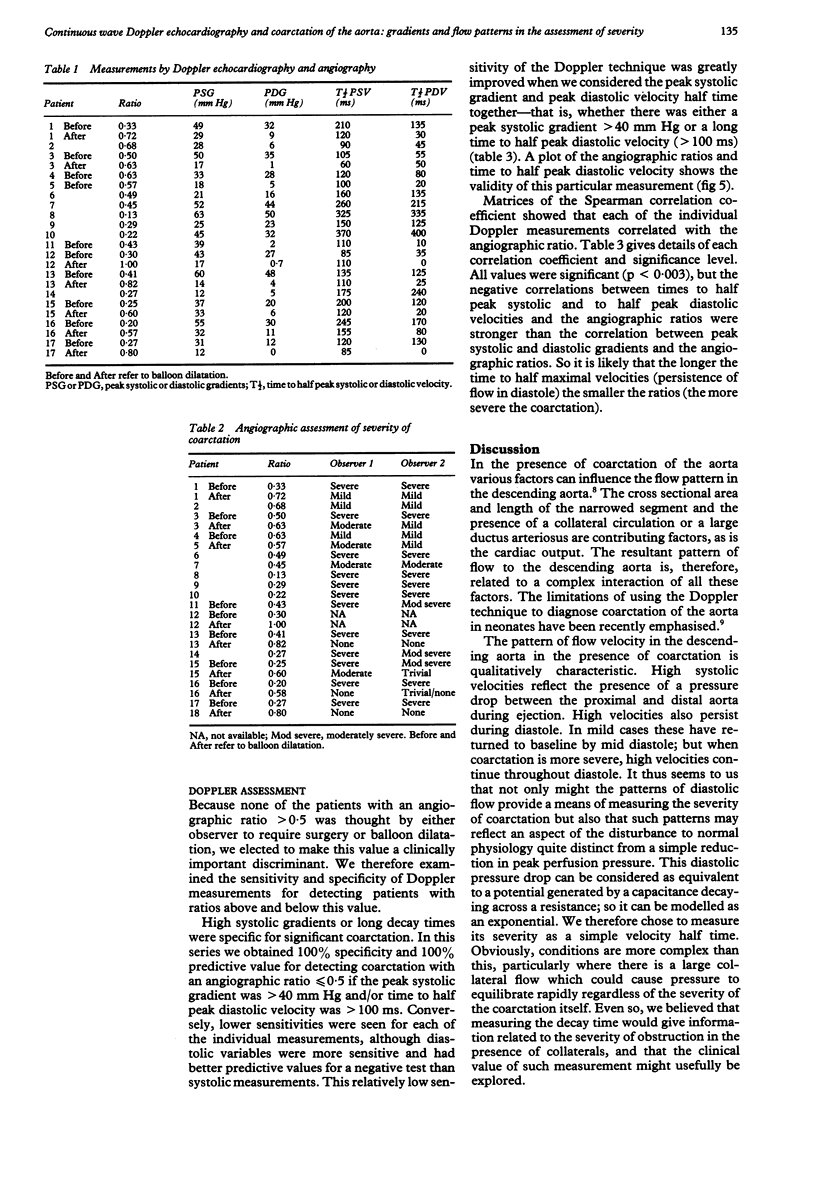
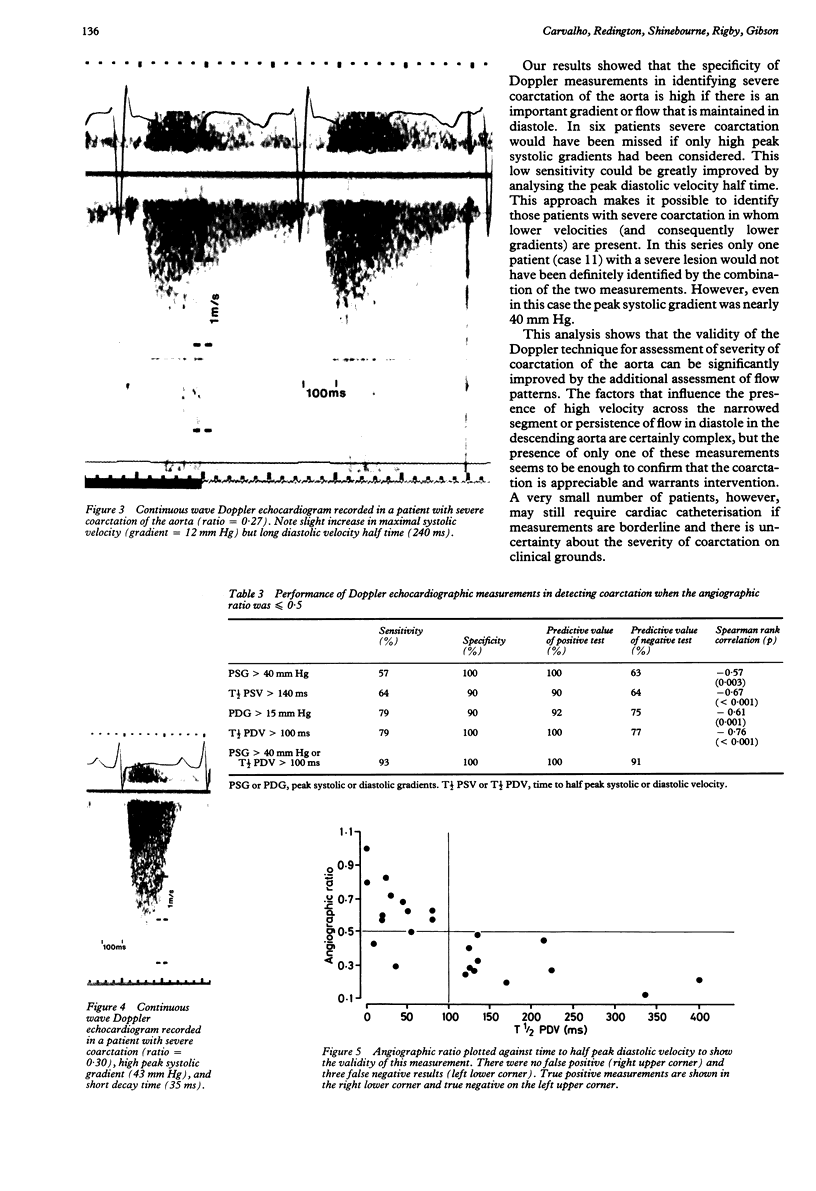
Indices of the severity of coarctation derived from non-invasive Doppler echocardiography were compared with measurements derived from cardiac catheterisation and angiography. In 24 Doppler studies from 17 children instantaneous peak systolic and diastolic gradients and time to half peak systolic and diastolic velocities were compared with the ratio of the coarctation diameter to the diameter of descending aorta at the level of diaphragm obtained from angiographic systolic frames of the aorta. A high peak systolic gradient (greater than 40 mm Hg) or long time to half peak diastolic velocity (greater than 100 ms) (that is, maintenance of flow in diastole) were both highly specific (100%) in detecting coarctation of the aorta where the angiographic ratio was less than or equal to 0.5. Diastolic measurements, however, were more sensitive (79% both for peak diastolic gradient and for time to half peak diastolic velocity) than systolic (57% for peak systolic gradient and 64% for time to half peak systolic velocity). Even higher sensitivity (93%) was obtained when the peak systolic gradient was greater than 40 mm Hg or the time to half peak diastolic velocity was greater than 100 ms. Examination by continuous wave Doppler echocardiography is an effective non-invasive method of assessing the severity of coarctation of the aorta, particularly when systolic and diastolic events are considered together. This approach overcomes the relatively low sensitivity of peak systolic gradient alone.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Houston A. B., Simpson I. A., Pollock J. C., Jamieson M. P., Doig W. B., Coleman E. N. Doppler ultrasound in the assessment of severity of coarctation of the aorta and interruption of the aortic arch. Br Heart J. 1987 Jan;57(1):38–43. doi: 10.1136/hrt.57.1.38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marx G. R., Allen H. D. Accuracy and pitfalls of Doppler evaluation of the pressure gradient in aortic coarctation. J Am Coll Cardiol. 1986 Jun;7(6):1379–1385. doi: 10.1016/s0735-1097(86)80160-7. [DOI] [PubMed] [Google Scholar]
- Rao P. S., Carey P. Doppler ultrasound in the prediction of pressure gradients across aortic coarctation. Am Heart J. 1989 Aug;118(2):299–307. doi: 10.1016/0002-8703(89)90189-0. [DOI] [PubMed] [Google Scholar]
- Robinson P. J., Wyse R. K., Deanfield J. E., Franklin R., Macartney F. J. Continuous wave Doppler velocimetry as an adjunct to cross sectional echocardiography in the diagnosis of critical left heart obstruction in neonates. Br Heart J. 1984 Nov;52(5):552–556. doi: 10.1136/hrt.52.5.552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teirstein P. S., Yock P. G., Popp R. L. The accuracy of Doppler ultrasound measurement of pressure gradients across irregular, dual, and tunnellike obstructions to blood flow. Circulation. 1985 Sep;72(3):577–584. doi: 10.1161/01.cir.72.3.577. [DOI] [PubMed] [Google Scholar]
- Wilson N., Sutherland G. R., Gibbs J. L., Dickinson D. F., Keeton B. R. Limitations of Doppler ultrasound in the diagnosis of neonatal coarctation of the aorta. Int J Cardiol. 1989 Apr;23(1):87–89. doi: 10.1016/0167-5273(89)90333-1. [DOI] [PubMed] [Google Scholar]
- Wyse R. K., Robinson P. J., Deanfield J. E., Tunstall Pedoe D. S., Macartney F. J. Use of continuous wave Doppler ultrasound velocimetry to assess the severity of coarctation of the aorta by measurement of aortic flow velocities. Br Heart J. 1984 Sep;52(3):278–283. doi: 10.1136/hrt.52.3.278. [DOI] [PMC free article] [PubMed] [Google Scholar]