

Abstract
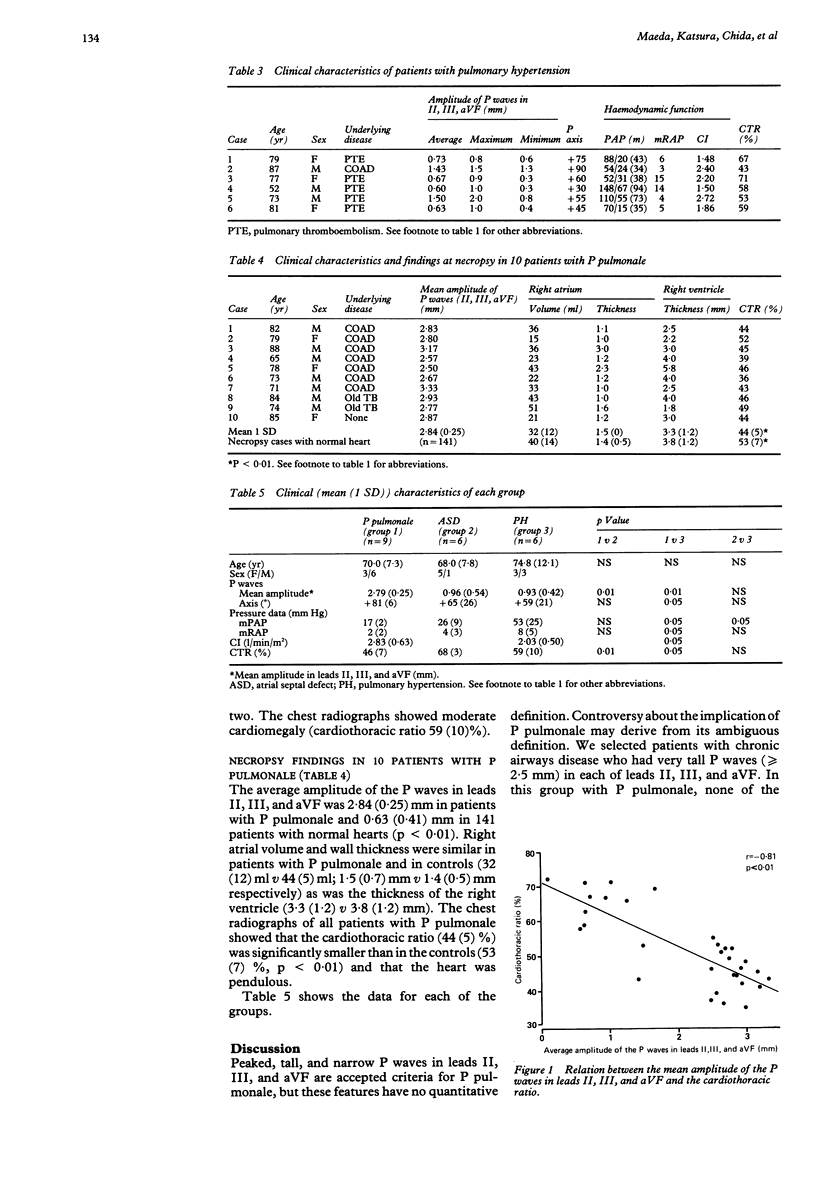
The correlation between P pulmonale and right atrial overload in chronic lung disease was studied. Right atrial pressure, pulmonary artery pressure, and cardiac output were measured with a Swan-Ganz catheter in nine patients with chronic lung disease and P pulmonale on the electrocardiogram (P wave amplitude of greater than or equal to 2.5 mm (0.25 mV) in leads II, III, and a VF. The results were compared with those in six patients with an atrial septal defect (left to right shunt greater than or equal to 50%) and six patients with pulmonary hypertension (mean pressure greater than or equal to 30 mm Hg without left sided heart disease). Right atrial volume and wall thickness were measured in 10 cases of P pulmonale among 1000 necropsy cases and compared with 141 normal hearts from the same series. The patients with P pulmonale did not show a significant increase in right atrial or pulmonary artery pressures. None of the patients with an atrial septal defect or pulmonary hypertension had P pulmonale on the electrocardiogram. In the necropsy cases of P pulmonale mean (1 SD) in right atrial volume (32 (12) ml) and wall thickness (1.5 (0.7) mm) were not significantly increased (40 (14) ml and 1.4 (0.5) mm in the normal hearts). There was a significant inverse relation between the presence of P pulmonale and the cardiothoracic ratio. In all the patients with P pulmonale chest x ray showed a low cardiothoracic ratio, a considerably depressed diaphragm, and a pendulous heart. This study showed no correlation between P pulmonale and right atrial overload in chronic lung disease. A more vertical anatomical position of the heart, particularly of the right atrium, seems to be the major factor responsible for generation of P pulmonale in chronic airways disease.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- CAIRD F. I., WILCKEN D. E. The electrocardiogram in chronic bronchitis with generalized obstructive lung disease. Its relation to ventilatory function. Am J Cardiol. 1962 Jul;10:5–13. doi: 10.1016/0002-9149(62)90260-6. [DOI] [PubMed] [Google Scholar]
- Calatayud J. B., Abad J. M., Khoi N. B., Stanbro W. W., Silver H. M. P-wave changes in chronic obstructive pulmonary disease. Am Heart J. 1970 Apr;79(4):444–453. doi: 10.1016/0002-8703(70)90248-6. [DOI] [PubMed] [Google Scholar]
- Saha N. C. Study of the P wave in normal and obstructive lung disease in Delhi. Am Heart J. 1970 Aug;80(2):154–161. doi: 10.1016/0002-8703(70)90162-6. [DOI] [PubMed] [Google Scholar]
- WASSERBURGER R. H., KELLY J. R., RASMUSSEN H. K., JUHL J. H. The electrocardiographic pentalogy of pulmonary emphysema. A correlation of roentgenographic findings and pulmonary function studies. Circulation. 1959 Nov;20:831–841. doi: 10.1161/01.cir.20.5.831. [DOI] [PubMed] [Google Scholar]
- WILDER C. S. ACUTE RESPIRATORY ILLNESSES REPORTED TO THE U. S. NATIONAL HEALTH SURVEY DURING 1957 TO 1962. Am Rev Respir Dis. 1963 Sep;88:SUPPL–21. doi: 10.1164/arrd.1963.88.1.14. [DOI] [PubMed] [Google Scholar]