

Abstract
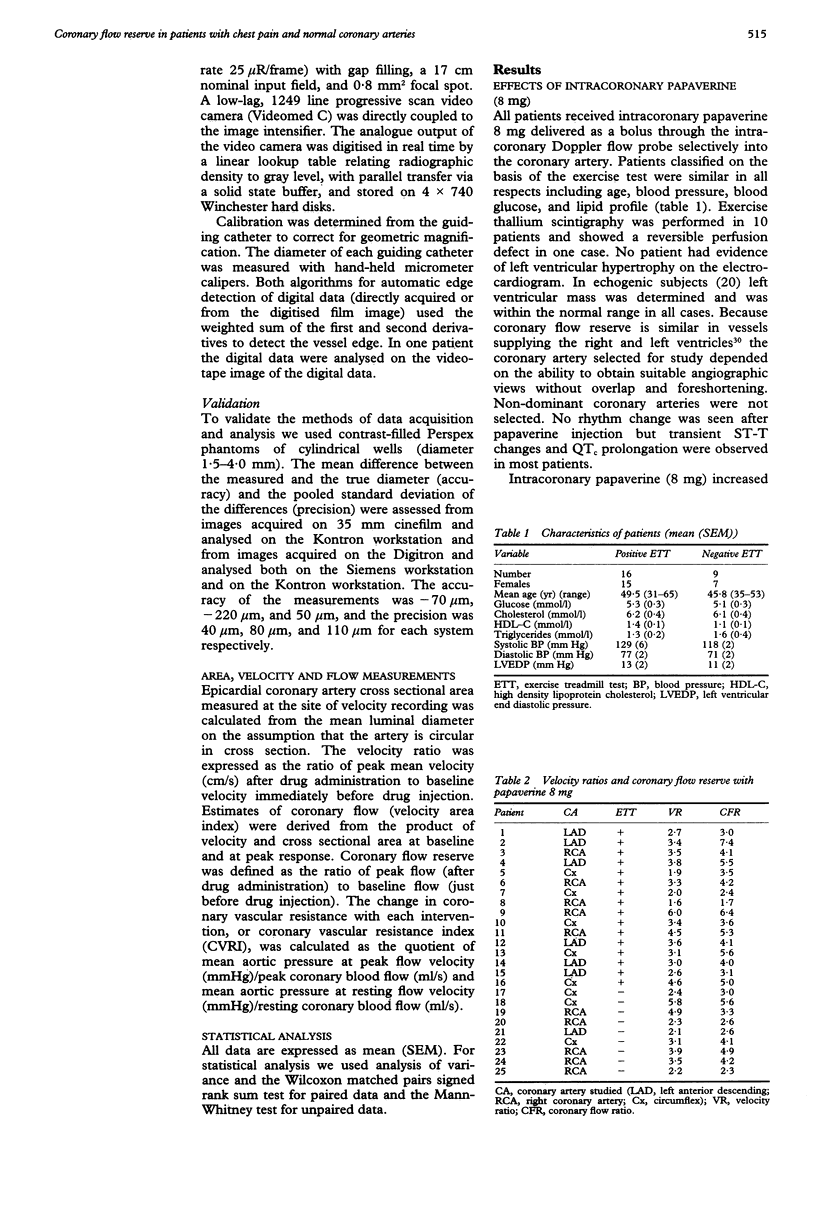
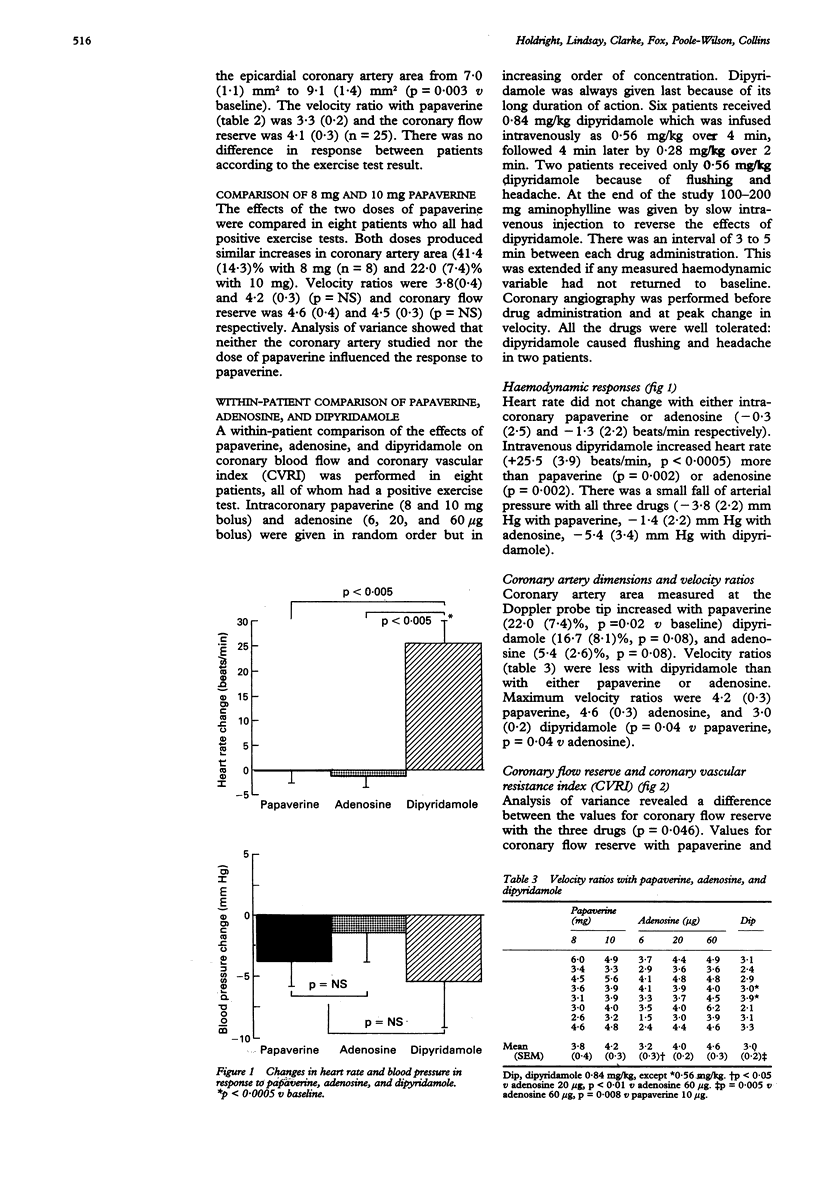
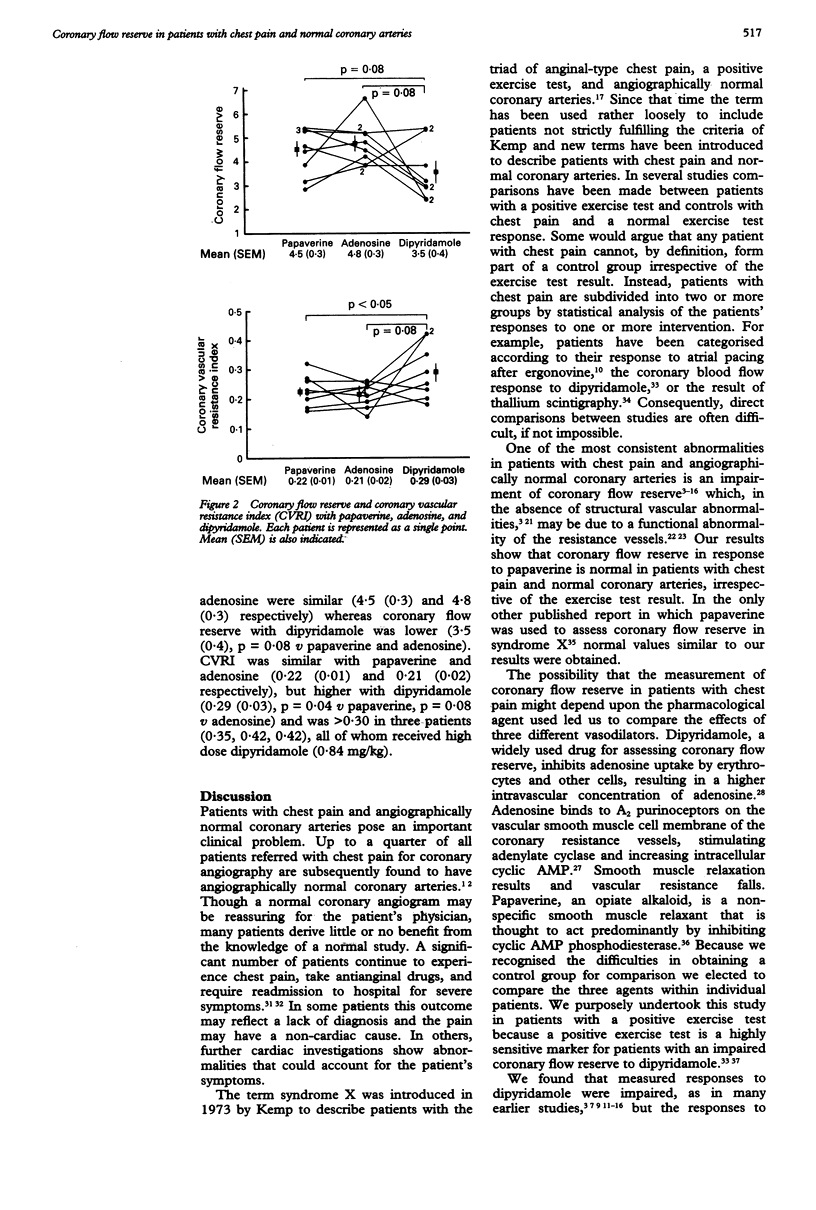
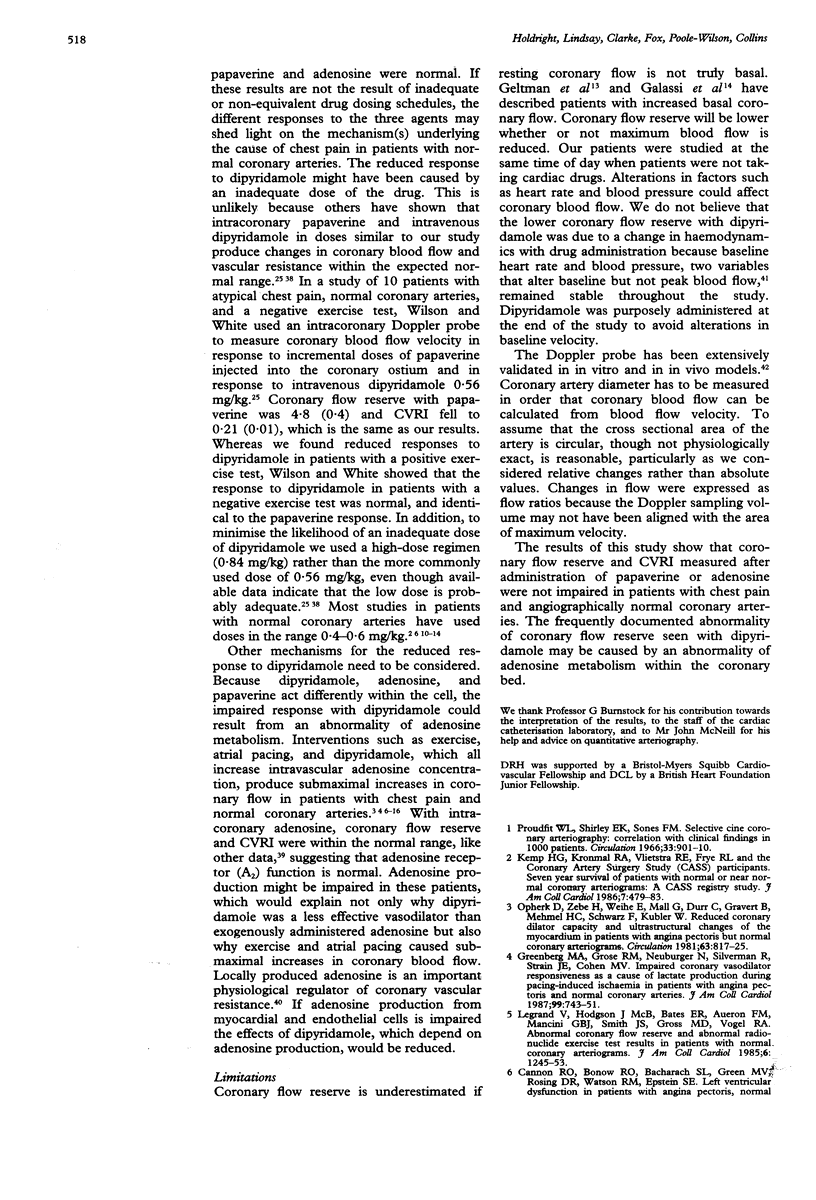
BACKGROUND--Many studies have shown that coronary flow reserve is reduced in patients with chest pain and angiographically normal coronary arteries. The methods used to assess coronary blood flow have varied, but in nearly all reports dipyridamole has been used to bring about vasodilatation. This study was designed to assess whether the apparent impairment of coronary flow reserve seen with dipyridamole could be reproduced with either papaverine or adenosine, which induce maximum coronary blood flow by different mechanisms. METHODS--25 patients with chest pain and angiographically normal coronary arteries were studied with an intracoronary Doppler flow probe and quantitative angiography to determine epicardial coronary artery area, coronary blood flow velocity, coronary flow reserve, and coronary vascular resistance index (CVRI, the ratio of resistance after intervention to basal resistance). All patients received papaverine 8 mg. Eight patients with positive exercise tests received intracoronary papaverine (8 and 10 mg), intracoronary adenosine (6, 20, 60 micrograms), and high-dose intravenous dipyridamole (0.84 mg/kg). RESULTS--The velocity ratio (peak after intervention: baseline) (mean (SEM)) after 8 mg papaverine was 3.3 (0.2) (n = 25) and the coronary flow reserve was 4.1 (0.3) (n = 25). There were no differences between patients with a positive (n = 16) or negative (n = 9) exercise test. In eight patients coronary flow reserve was measured after increasing doses of papaverine, adenosine, and dipyridamole. Coronary flow reserve was 4.5 (0.3) with papaverine, 4.8 (0.3) with adenosine, and 3.5 (0.4) with dipyridamole (p = 0.08 v papaverine and adenosine). CVRI was 0.22 (0.01) with papaverine, 0.21 (0.02) with adenosine, and 0.29 (0.03) with dipyridamole (p < 0.05 v papaverine, p = 0.09 v adenosine). CONCLUSIONS--These results indicate that measurement of coronary flow reserve and CVRI in patients with chest pain and normal coronary arteries depends on the pharmacological stimulus. Normal values were obtained with papaverine in all patients, irrespective of the exercise test response. In patients with a positive exercise test significantly lower values were obtained with dipyridamole than with papaverine, or adenosine. The reported impairment of coronary flow reserve in patients with angina and normal coronary arteries may reflect the variability in response to different pharmacological agents. The mechanism underlying this variability is unknown, but may involve an abnormality of adenosine metabolism in the myocardium.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bemiller C. R., Pepine C. J., Rogers A. K. Long-term observations in patients with angina and normal coronary arteriograms. Circulation. 1973 Jan;47(1):36–43. doi: 10.1161/01.cir.47.1.36. [DOI] [PubMed] [Google Scholar]
- Berne R. M. The role of adenosine in the regulation of coronary blood flow. Circ Res. 1980 Dec;47(6):807–813. doi: 10.1161/01.res.47.6.807. [DOI] [PubMed] [Google Scholar]
- Bortone A. S., Hess O. M., Eberli F. R., Nonogi H., Marolf A. P., Grimm J., Krayenbuehl H. P. Abnormal coronary vasomotion during exercise in patients with normal coronary arteries and reduced coronary flow reserve. Circulation. 1989 Mar;79(3):516–527. doi: 10.1161/01.cir.79.3.516. [DOI] [PubMed] [Google Scholar]
- Camici P. G., Gistri R., Lorenzoni R., Sorace O., Michelassi C., Bongiorni M. G., Salvadori P. A., L'Abbate A. Coronary reserve and exercise ECG in patients with chest pain and normal coronary angiograms. Circulation. 1992 Jul;86(1):179–186. doi: 10.1161/01.cir.86.1.179. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Bonow R. O., Bacharach S. L., Green M. V., Rosing D. R., Leon M. B., Watson R. M., Epstein S. E. Left ventricular dysfunction in patients with angina pectoris, normal epicardial coronary arteries, and abnormal vasodilator reserve. Circulation. 1985 Feb;71(2):218–226. doi: 10.1161/01.cir.71.2.218. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Cattau E. L., Jr, Yakshe P. N., Maher K., Schenke W. H., Benjamin S. B., Epstein S. E. Coronary flow reserve, esophageal motility, and chest pain in patients with angiographically normal coronary arteries. Am J Med. 1990 Mar;88(3):217–222. doi: 10.1016/0002-9343(90)90145-4. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Epstein S. E. "Microvascular angina" as a cause of chest pain with angiographically normal coronary arteries. Am J Cardiol. 1988 Jun 1;61(15):1338–1343. doi: 10.1016/0002-9149(88)91180-0. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Schenke W. H., Leon M. B., Rosing D. R., Urqhart J., Epstein S. E. Limited coronary flow reserve after dipyridamole in patients with ergonovine-induced coronary vasoconstriction. Circulation. 1987 Jan;75(1):163–174. doi: 10.1161/01.cir.75.1.163. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Watson R. M., Rosing D. R., Epstein S. E. Angina caused by reduced vasodilator reserve of the small coronary arteries. J Am Coll Cardiol. 1983 Jun;1(6):1359–1373. doi: 10.1016/s0735-1097(83)80037-0. [DOI] [PubMed] [Google Scholar]
- Coronary heart disease death, nonfatal acute myocardial infarction and other clinical outcomes in the Multiple Risk Factor Intervention Trial. Multiple Risk Factor Intervention Trial Research Group. Am J Cardiol. 1986 Jul 1;58(1):1–13. doi: 10.1016/0002-9149(86)90232-8. [DOI] [PubMed] [Google Scholar]
- Devereux R. B., Reichek N. Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation. 1977 Apr;55(4):613–618. doi: 10.1161/01.cir.55.4.613. [DOI] [PubMed] [Google Scholar]
- Epstein S. E., Cannon R. O., 3rd Site of increased resistance to coronary flow in patients with angina pectoris and normal epicardial coronary arteries. J Am Coll Cardiol. 1986 Aug;8(2):459–461. doi: 10.1016/s0735-1097(86)80067-5. [DOI] [PubMed] [Google Scholar]
- Geltman E. M., Henes C. G., Senneff M. J., Sobel B. E., Bergmann S. R. Increased myocardial perfusion at rest and diminished perfusion reserve in patients with angina and angiographically normal coronary arteries. J Am Coll Cardiol. 1990 Sep;16(3):586–595. doi: 10.1016/0735-1097(90)90347-r. [DOI] [PubMed] [Google Scholar]
- Greenberg M. A., Grose R. M., Neuburger N., Silverman R., Strain J. E., Cohen M. V. Impaired coronary vasodilator responsiveness as a cause of lactate production during pacing-induced ischemia in patients with angina pectoris and normal coronary arteries. J Am Coll Cardiol. 1987 Apr;9(4):743–751. doi: 10.1016/s0735-1097(87)80227-9. [DOI] [PubMed] [Google Scholar]
- Kaski J. C., Tousoulis D., Galassi A. R., McFadden E., Pereira W. I., Crea F., Maseri A. Epicardial coronary artery tone and reactivity in patients with normal coronary arteriograms and reduced coronary flow reserve (syndrome X) J Am Coll Cardiol. 1991 Jul;18(1):50–54. doi: 10.1016/s0735-1097(10)80216-5. [DOI] [PubMed] [Google Scholar]
- Kemp H. G., Jr Left ventricular function in patients with the anginal syndrome and normal coronary arteriograms. Am J Cardiol. 1973 Sep 7;32(3):375–376. doi: 10.1016/s0002-9149(73)80150-x. [DOI] [PubMed] [Google Scholar]
- Kemp H. G., Kronmal R. A., Vlietstra R. E., Frye R. L. Seven year survival of patients with normal or near normal coronary arteriograms: a CASS registry study. J Am Coll Cardiol. 1986 Mar;7(3):479–483. doi: 10.1016/s0735-1097(86)80456-9. [DOI] [PubMed] [Google Scholar]
- Legrand V., Hodgson J. M., Bates E. R., Aueron F. M., Mancini G. B., Smith J. S., Gross M. D., Vogel R. A. Abnormal coronary flow reserve and abnormal radionuclide exercise test results in patients with normal coronary angiograms. J Am Coll Cardiol. 1985 Dec;6(6):1245–1253. doi: 10.1016/s0735-1097(85)80209-6. [DOI] [PubMed] [Google Scholar]
- Marcus M., Wright C., Doty D., Eastham C., Laughlin D., Krumm P., Fastenow C., Brody M. Measurements of coronary velocity and reactive hyperemia in the coronary circulation of humans. Circ Res. 1981 Oct;49(4):877–891. doi: 10.1161/01.res.49.4.877. [DOI] [PubMed] [Google Scholar]
- Maseri A., Crea F., Kaski J. C., Crake T. Mechanisms of angina pectoris in syndrome X. J Am Coll Cardiol. 1991 Feb;17(2):499–506. doi: 10.1016/s0735-1097(10)80122-6. [DOI] [PubMed] [Google Scholar]
- Neumann F. J., Waas W., Zimmermann R., Haupt H., Tillmanns H., Kübler W. Haemorheologic studies in patients with reduced coronary vasodilator capacity but normal coronary angiogram (syndrome X). Eur Heart J. 1989 Jun;10(6):509–513. doi: 10.1093/oxfordjournals.eurheartj.a059520. [DOI] [PubMed] [Google Scholar]
- Olsson R. A., Davis C. J., Khouri E. M., Patterson R. E. Evidence for an adenosine receptor on the surface of dog coronary myocytes. Circ Res. 1976 Jul;39(1):93–98. doi: 10.1161/01.res.39.1.93. [DOI] [PubMed] [Google Scholar]
- Opherk D., Zebe H., Schuler G., Weihe E., Mall G., Kübler W. Reduced coronary reserve and abnormal exercise left ventricular reserve in patients with syndrome X. Arch Mal Coeur Vaiss. 1983 Feb;76(Spec No):231–235. [PubMed] [Google Scholar]
- Opherk D., Zebe H., Weihe E., Mall G., Dürr C., Gravert B., Mehmel H. C., Schwarz F., Kübler W. Reduced coronary dilatory capacity and ultrastructural changes of the myocardium in patients with angina pectoris but normal coronary arteriograms. Circulation. 1981 Apr;63(4):817–825. doi: 10.1161/01.cir.63.4.817. [DOI] [PubMed] [Google Scholar]
- Proudfit W. L., Shirey E. K., Sones F. M., Jr Selective cine coronary arteriography. Correlation with clinical findings in 1,000 patients. Circulation. 1966 Jun;33(6):901–910. doi: 10.1161/01.cir.33.6.901. [DOI] [PubMed] [Google Scholar]
- Quyyumi A. A., Cannon R. O., 3rd, Panza J. A., Diodati J. G., Epstein S. E. Endothelial dysfunction in patients with chest pain and normal coronary arteries. Circulation. 1992 Dec;86(6):1864–1871. doi: 10.1161/01.cir.86.6.1864. [DOI] [PubMed] [Google Scholar]
- Richardson P. J., Livesley B., Oram S., Olsen E. G., Armstrong P. Angina pectoris with normal coronary arteries. Transvenous myocardial biopsy in diagnosis. Lancet. 1974 Sep 21;2(7882):677–680. doi: 10.1016/s0140-6736(74)93260-7. [DOI] [PubMed] [Google Scholar]
- Rossen J. D., Winniford M. D. Effect of increases in heart rate and arterial pressure on coronary flow reserve in humans. J Am Coll Cardiol. 1993 Feb;21(2):343–348. doi: 10.1016/0735-1097(93)90673-o. [DOI] [PubMed] [Google Scholar]
- Sax F. L., Cannon R. O., 3rd, Hanson C., Epstein S. E. Impaired forearm vasodilator reserve in patients with microvascular angina. Evidence of a generalized disorder of vascular function? N Engl J Med. 1987 Nov 26;317(22):1366–1370. doi: 10.1056/NEJM198711263172202. [DOI] [PubMed] [Google Scholar]
- Sibley D. H., Millar H. D., Hartley C. J., Whitlow P. L. Subselective measurement of coronary blood flow velocity using a steerable Doppler catheter. J Am Coll Cardiol. 1986 Dec;8(6):1332–1340. doi: 10.1016/s0735-1097(86)80305-9. [DOI] [PubMed] [Google Scholar]
- Triner L., Vulliemoz Y., Schwartz I., Nahas G. G. Cyclic phosphodiesterase activity and the action of papaverine. Biochem Biophys Res Commun. 1970 Jul 13;40(1):64–69. doi: 10.1016/0006-291x(70)91046-6. [DOI] [PubMed] [Google Scholar]
- Tweddel A. C., Martin W., Hutton I. Thallium scans in syndrome X. Br Heart J. 1992 Jul;68(1):48–50. doi: 10.1136/hrt.68.7.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson R. F., Laughlin D. E., Ackell P. H., Chilian W. M., Holida M. D., Hartley C. J., Armstrong M. L., Marcus M. L., White C. W. Transluminal, subselective measurement of coronary artery blood flow velocity and vasodilator reserve in man. Circulation. 1985 Jul;72(1):82–92. doi: 10.1161/01.cir.72.1.82. [DOI] [PubMed] [Google Scholar]
- Wilson R. F., White C. W. Intracoronary papaverine: an ideal coronary vasodilator for studies of the coronary circulation in conscious humans. Circulation. 1986 Mar;73(3):444–451. doi: 10.1161/01.cir.73.3.444. [DOI] [PubMed] [Google Scholar]
- Wilson R. F., Wyche K., Christensen B. V., Zimmer S., Laxson D. D. Effects of adenosine on human coronary arterial circulation. Circulation. 1990 Nov;82(5):1595–1606. doi: 10.1161/01.cir.82.5.1595. [DOI] [PubMed] [Google Scholar]
- Zijlstra F., Serruys P. W., Hugenholtz P. G. Papaverine: the ideal coronary vasodilator for investigating coronary flow reserve? A study of timing, magnitude, reproducibility, and safety of the coronary hyperemic response after intracoronary papaverine. Cathet Cardiovasc Diagn. 1986;12(5):298–303. doi: 10.1002/ccd.1810120505. [DOI] [PubMed] [Google Scholar]