

Abstract
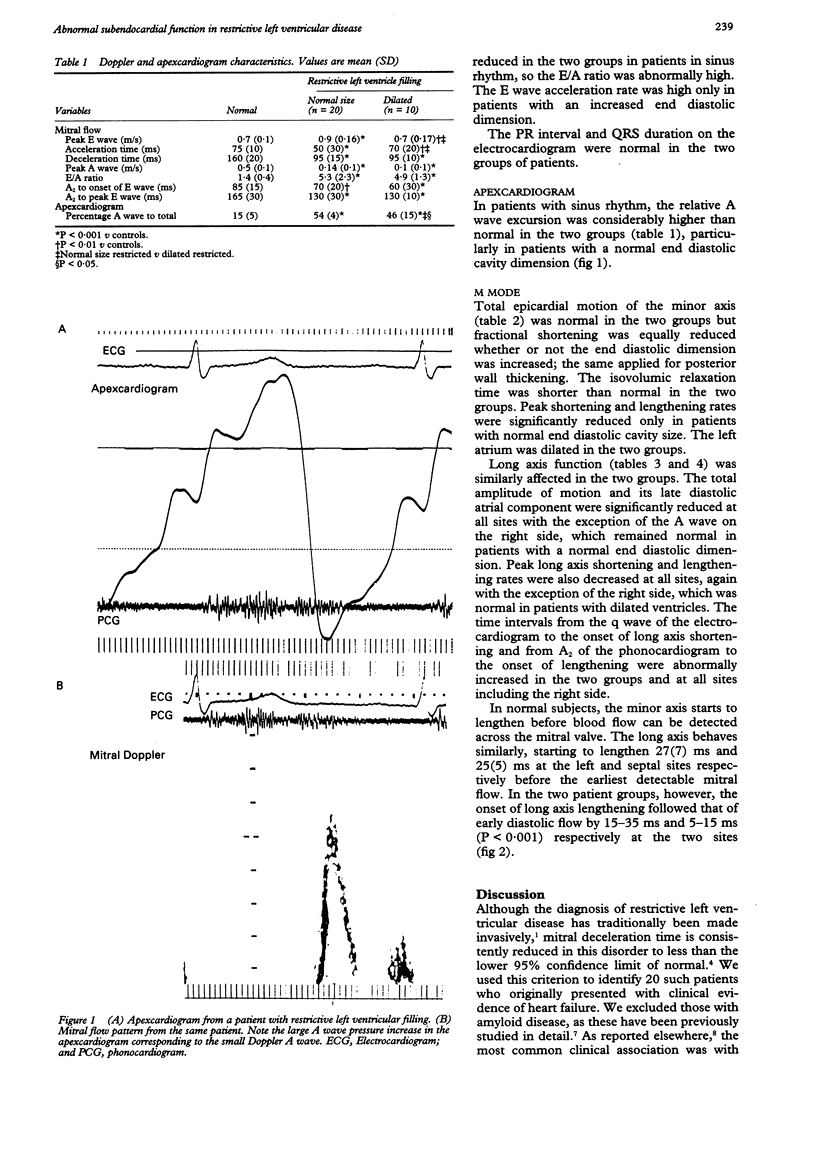
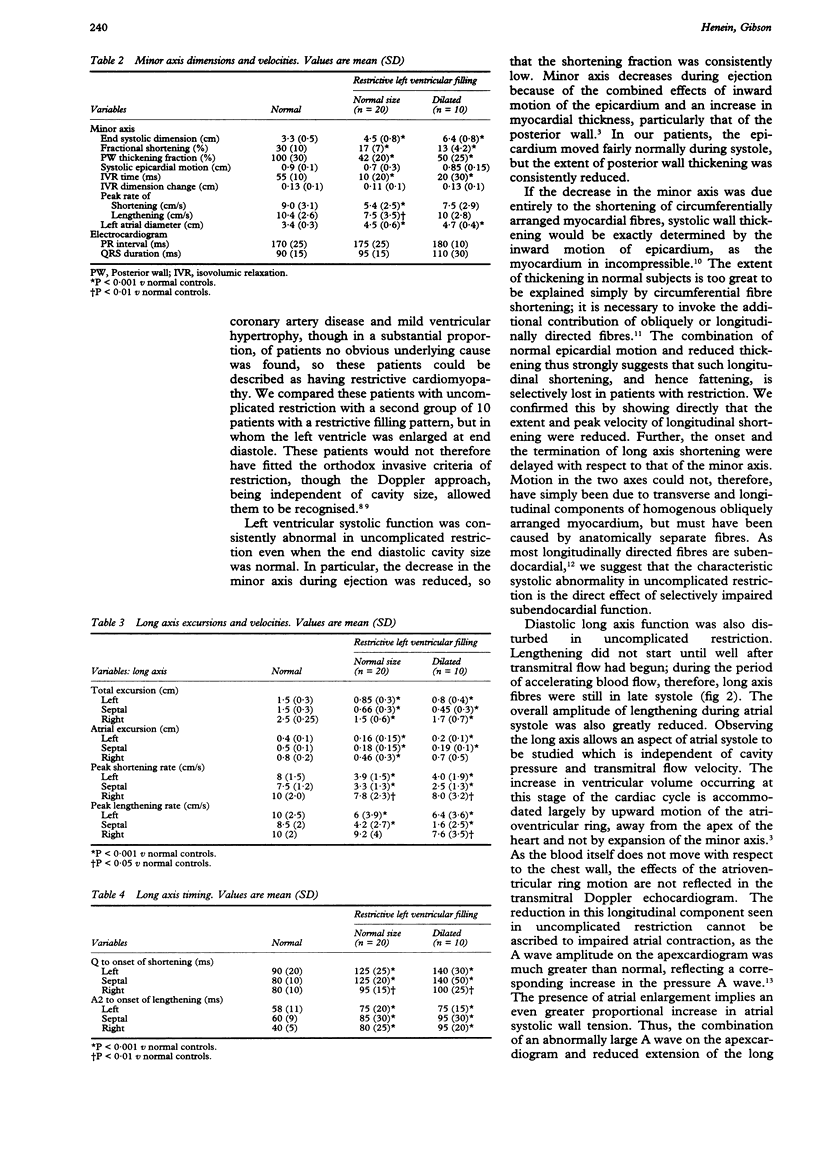
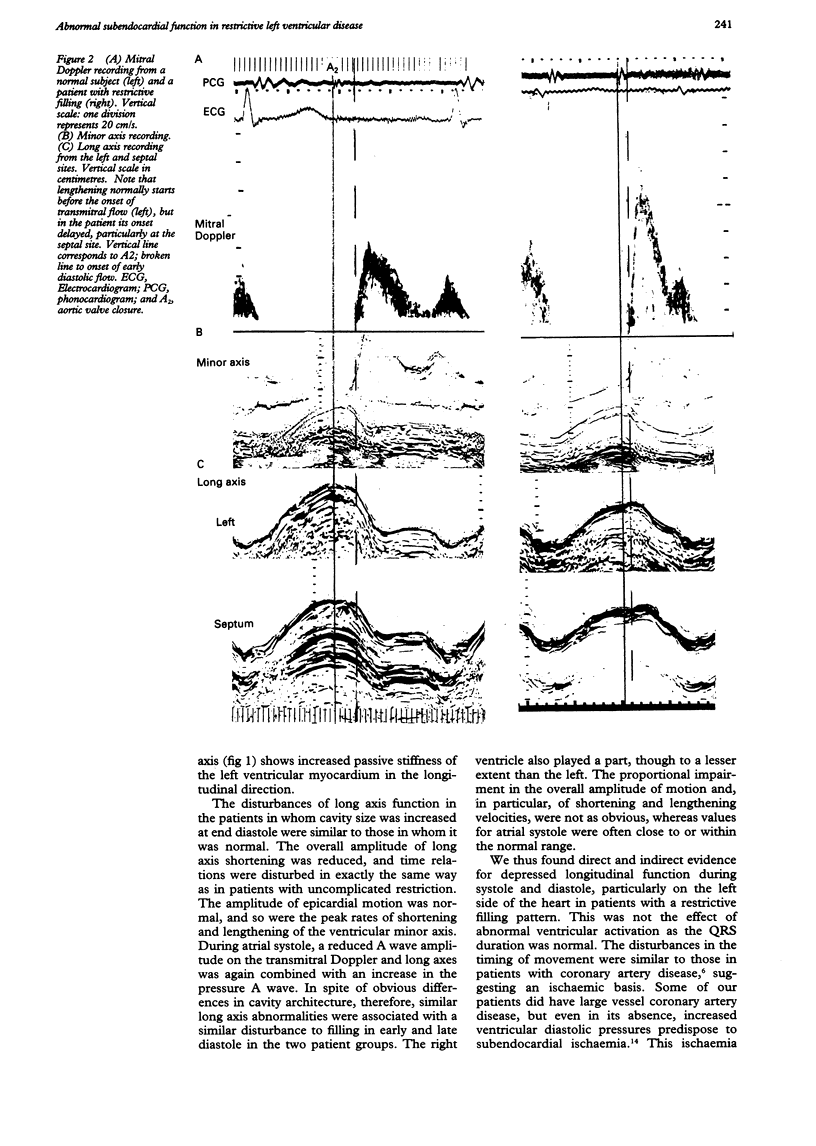
OBJECTIVE--To study possible disturbances in left ventricular long axis function in patients with a restrictive filling pattern. DESIGN--Prospective examination of the left ventricular transverse and longitudinal axes, transmitral flow, and the apexcardiogram. SETTING--A tertiary referral centre for cardiac diseases. SUBJECTS--21 normal subjects, age (SD) 51(11); 30 patients of similar age with a restrictive left ventricular filling pattern, defined as short early diastolic deceleration time less than the lower 95% confidence limit of the normal value (120 ms). 20 patients had a normal and 10 had an increased left ventricular end diastolic cavity size. RESULTS--Mitral Doppler echocardiography: E wave velocity was high only in patients with a normal cavity size. A wave velocity was greatly reduced in the two groups (P < 0.001) so that the E/A ratio was abnormally high. The relative A wave amplitude on the apexcardiogram was greatly increased in the two groups: 46(15)% (mean (SD)) and 54(4)% v 15(5)%. Minor axis: Fractional shortening was reduced from 30(10)% to 17(7)% in patients with normal cavity size and to 13(4.2)% in those with a dilated cavity (P < 0.001), as was the posterior wall thickening fraction from 100(30)% to 42(20)% and 50(25)% respectively (P < 0.001). Total systolic epicardial motion was normal and isovolumic relaxation time was short in the two groups. Long axis: Left ventricular abnormalities included reduced total amplitude of motion and its component during atrial systole (P < 0.001 for the two groups at both sites). Peak long axis shortening and lengthening were decreased at both left ventricular sites (P < 0.001). The time intervals from q wave of the electrocardiogram and A2 (aortic valve closure) to the onset of shortening and lengthening respectively were increased (both P < 0.001). Right ventricular long axis function was similarly affected but to a lesser extent. CONCLUSION--Left ventricular long axis function is consistently abnormal in patients with restrictive disease whether or not cavity size is increased. Not only are the extent and peak velocity of shortening reduced, but during diastole the peak early diastolic lengthening rate and amplitude during atrial systole are impaired. Early diastolic long axis motion is asynchronous with respect to transmitral flow and left ventricular minor axis. These effects will impair the overall left ventricular systolic and diastolic function independently of any decrease in passive cavity compliance. Unlike fibrosis, these long axis abnormalities are potentially amenable to treatment.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Appleton C. P., Hatle L. K., Popp R. L. Demonstration of restrictive ventricular physiology by Doppler echocardiography. J Am Coll Cardiol. 1988 Apr;11(4):757–768. doi: 10.1016/0735-1097(88)90208-2. [DOI] [PubMed] [Google Scholar]
- Benotti J. R., Grossman W. Restrictive cardiomyopathy. Annu Rev Med. 1984;35:113–125. doi: 10.1146/annurev.me.35.020184.000553. [DOI] [PubMed] [Google Scholar]
- Brecker S. J., Xiao H. B., Mbaissouroum M., Gibson D. G. Effects of intravenous milrinone on left ventricular function in ischemic and idiopathic dilated cardiomyopathy. Am J Cardiol. 1993 Jan 15;71(2):203–209. doi: 10.1016/0002-9149(93)90739-y. [DOI] [PubMed] [Google Scholar]
- Denef B., Werf F. V., Geest H. D., Kesteloot H. Calibrated apexcardiography and assessment of left ventricular dynamics in man. Eur J Cardiol. 1976 May;4 (Suppl):143–152. [PubMed] [Google Scholar]
- Denison S. H., Sands A., Tindall D. J. A tyrosine aminotransferase glucocorticoid response element also mediates androgen enhancement of gene expression. Endocrinology. 1989 Feb;124(2):1091–1093. doi: 10.1210/endo-124-2-1091. [DOI] [PubMed] [Google Scholar]
- Dumesnil J. G., Shoucri R. M., Laurenceau J. L., Turcot J. A mathematical model of the dynamic geometry of the intact left ventricle and its application to clinical data. Circulation. 1979 May;59(5):1024–1034. doi: 10.1161/01.cir.59.5.1024. [DOI] [PubMed] [Google Scholar]
- Gibson D. G., Brown D. J. Continuous assessment of left ventricular shape in man. Br Heart J. 1975 Sep;37(9):904–910. doi: 10.1136/hrt.37.9.904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenbaum R. A., Ho S. Y., Gibson D. G., Becker A. E., Anderson R. H. Left ventricular fibre architecture in man. Br Heart J. 1981 Mar;45(3):248–263. doi: 10.1136/hrt.45.3.248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawthorne E. W. Symposium on measurements of left ventricular volume. 3. Dynamic geometry of the left ventricle. Am J Cardiol. 1966 Oct;18(4):566–573. doi: 10.1016/0002-9149(66)90012-9. [DOI] [PubMed] [Google Scholar]
- Henein M. Y., Priestley K., Davarashvili T., Buller N., Gibson D. G. Early changes in left ventricular subendocardial function after successful coronary angioplasty. Br Heart J. 1993 Jun;69(6):501–506. doi: 10.1136/hrt.69.6.501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones C. J., Raposo L., Gibson D. G. Functional importance of the long axis dynamics of the human left ventricle. Br Heart J. 1990 Apr;63(4):215–220. doi: 10.1136/hrt.63.4.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keren A., Popp R. L. Assignment of patients into the classification of cardiomyopathies. Circulation. 1992 Nov;86(5):1622–1633. doi: 10.1161/01.cir.86.5.1622. [DOI] [PubMed] [Google Scholar]
- Klein A. L., Hatle L. K., Taliercio C. P., Taylor C. L., Kyle R. A., Bailey K. R., Seward J. B., Tajik A. J. Serial Doppler echocardiographic follow-up of left ventricular diastolic function in cardiac amyloidosis. J Am Coll Cardiol. 1990 Nov;16(5):1135–1141. doi: 10.1016/0735-1097(90)90545-z. [DOI] [PubMed] [Google Scholar]
- Mattheos M., Shapiro E., Oldershaw P. J., Sacchetti R., Gibson D. G. Non-invasive assessment of changes in left ventricular relaxation by combined phono-, echo-, and mechanocardiography. Br Heart J. 1982 Mar;47(3):253–260. doi: 10.1136/hrt.47.3.253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinamonti B., Di Lenarda A., Sinagra G., Camerini F. Restrictive left ventricular filling pattern in dilated cardiomyopathy assessed by Doppler echocardiography: clinical, echocardiographic and hemodynamic correlations and prognostic implications. Heart Muscle Disease Study Group. J Am Coll Cardiol. 1993 Sep;22(3):808–815. doi: 10.1016/0735-1097(93)90195-7. [DOI] [PubMed] [Google Scholar]
- Sallin E. A. Fiber orientation and ejection fraction in the human left ventricle. Biophys J. 1969 Jul;9(7):954–964. doi: 10.1016/S0006-3495(69)86429-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Upton M. T., Gibson D. G. The study of left ventricular function from digitized echocardiograms. Prog Cardiovasc Dis. 1978 Mar-Apr;20(5):359–384. doi: 10.1016/0033-0620(78)90003-8. [DOI] [PubMed] [Google Scholar]