

Abstract
Objective
Alcohol craving is a predictor of continued drinking and a diagnostic criterion for alcohol use disorder. Rewarding subjective effects potentiate craving, but it remains unclear if relations are expectancy-driven vs. alcohol-induced. In addition, it remains unclear if relations operate solely at the person level, or if there is also within-person dynamic change.
Methods
Participants (N = 448) come from a placebo-controlled alcohol administration study. Participants in the alcohol condition reported subjective effects and alcohol craving on ascending (BAC = .068), peak (BAC = .079), and descending (BAC = .066) BAC limbs. Participants in the placebo condition were yoked to alcohol condition participants. Multilevel models tested whether (1) within-person deviations in subjective effects predicted within-person deviations in craving, (2) between-person levels of subjective effects predicted between-person levels of craving, and (3) effects were dependent upon experimental condition.
Results
At the within-person level, increases in high arousal positive/stimulant effects were associated with within-person increases in alcohol craving, regardless of experimental condition. At the between-person level, interactions were observed between high arousal positive/stimulant (and low arousal positive/relaxing) effects and condition. Probing suggested that the association between person-level high arousal positive/stimulant effects and craving was statistically significant in the alcohol but not the placebo condition. Conversely, the association between person-level low arousal positive/relaxing effects and craving was positive and statistically significant in the placebo but negative in the alcohol condition.
Conclusions
Findings suggest expectancy-like relations among high arousal positive/stimulant effects and craving within-person. However, alcohol-induced positive reinforcement (i.e., stimulation) facilitated heightened person-level craving, whereas expectancy-like negative reinforcement (i.e., relaxation) attenuated person-level craving.
Keywords: Subjective response, Alcohol craving, Placebo, Alcohol expectancies
Introduction
Alcohol craving is defined as an urge, want, or desire for alcohol (Kavanagh et al. 2013; Love et al. 1998), and is a central aspect of theoretical models of addiction (e.g., Monti et al. 2000; Robinson & Berridge 1993). Alcohol craving is a diagnostic criterion for alcohol use disorder (AUD; American Psychiatric Association 2013, 2022; World Health Organization 1992), and has been an effective intervention target for heavy drinking and AUD (Anton 1999; Kranzler and Edenberg 2010; Waddell et al. 2022; Witkiewitz et al. 2013). Furthermore, alcohol craving is thought to be a proximal antecedent of continued drinking during drinking episodes (e.g., Green et al. 2019; Wycoff et al. 2022; Tiffany & Conklin 2000). Despite its importance, ecological momentary assessment and alcohol administration studies have largely ignored craving as an outcome of interest.
One consistent predictor of alcohol craving is subjective response, often defined as the combination of pharmacological and expectancy effects of alcohol on mood and behavior. Subjective response can be broken into four domains indicative of high arousal positive/stimulant (i.e., positive reinforcement/reward), low arousal positive (i.e., negative reinforcement/tension reduction), high arousal negative (e.g., aggression), and low arousal negative/sedative (i.e., cognitive/behavioral impairment) subjective effects (e.g.,Morean et al. 2012, 2013). Across studies, heightened high arousal positive/stimulant and blunted low arousal negative/sedative alcohol effects are typically associated with heavier drinking, high arousal negative alcohol effects with more alcohol-related problems, and low positive effects with less drinking (e.g.,Morean et al. 2013, 2015; Quinn & Fromme 2016; Waddell et al. 2020).
Theoretically, both high arousal positive (i.e., positively reinforcing) and low arousal positive (i.e., negatively reinforcing) subjective effects would be expected to potentiate acute alcohol craving, as an individual may become motivated to continue feeling and/or enhance rewarding and/or tension reducing effects (e.g.,Baker et al. 2004; Cho et al. 2019; De Wit & Phan 2010; Koob 2013). In support of this hypothesis, two alcohol administration studies found that individuals with higher levels of high arousal positive/stimulant effects reported higher levels of craving (Bujarski and Ray 2014; Green et al. 2019), but research suggests no relations among tension reduction and craving (Bujarski and Ray 2014). Because these studies only focused on between-person effects (e.g., individuals with higher levels of stimulation), they do not inform our understanding of potential within-person deviations in subjective responses during a drinking episode or their relations to fluctuations in craving. In contrast, other alcohol administration studies have tested such within-person relations, finding that within-person increases in high arousal positive/stimulant alcohol effects at a given moment were associated with within-person increases in alcohol craving (Hendershot et al. 2015; Wardell et al. 2015), and within-person increases in low arousal negative/sedative effects were associated with within-person decreases in alcohol craving (Wardell et al. 2015).
Although research clearly points to subjective effects as predictors of acute alcohol craving, no study to date has focused on the role of acute alcohol expectancies (i.e., subjective effects due to expectations about alcohol response rather than pharmacology). Using placebo-controlled alcohol administration, studies have shown that levels of low arousal positive/relaxing subjective response are largely similar between those who receive a placebo vs. alcoholic beverage, but that levels of high arousal positive, high arousal negative, and low arousal negative subjective response substantially differ (Corbin et al. 2015, 2021; Waddell et al. 2021). Similarly, studies have found that levels of alcohol craving are largely similar in those who receive alcohol and placebo (e.g., Waddell et al. 2021), and having alcohol cues in sight increases craving, whether drinking or not (Kohen et al. 2022). Thus, the mere act of drinking a beverage (i.e., acute expectancies) appears to play a crucial role in a variety of subjective effects and alcohol craving.
One possibility is that relations among subjective effects and craving are due to increases in affect when in a drinking situation, regardless of whether alcohol is consumed or not. This may be the case particularly for low arousal positive effects, which show a strong placebo response (Corbin et al. 2021; Waddell et al. 2021). On the contrary, individuals who report higher levels of high arousal positive subjective effects may report higher levels of craving in the alcohol vs. placebo condition, considering a clear difference in high arousal positive effects between those who receive alcohol vs. placebo (e.g., Corbin et al. 2021). Furthermore, it is also possible that within-person relations among subjective response and craving are particularly susceptible to expectancy (placebo) effects for both high arousal positive and low arousal positive effects. Thus, if an individual feels an increase (from their within-person average) in high arousal positive or low arousal positive subjective effects at a given moment while drinking, such increases may perpetuate increased levels of craving, regardless of beverage condition.
The current study
The current study used data from a large placebo-controlled alcohol administration study in emerging adult drinkers to test between- and within-person relations between subjective response and alcohol craving and the extent to which these relations differ by beverage condition. Participants were heavy drinkers without an AUD, allowing the current study to test the process through which in-the-moment drinking and related consequences develop and may become reinforced over time. Participants were randomized to either an alcohol or placebo condition, allowing for examination of differences in subjective response and craving based on whether alcohol was consumed or not. All participants also completed comprehensive measures of subjective responses to alcohol and craving, allowing for test of both positive and negative reinforcement mechanisms. Finally, the current study assessed individuals at three time points across the blood alcohol concentration (BAC) curve (i.e., at ascending, peak, and descending BACs), allowing for separation of between-person effects and within-person deviations.
It was hypothesized that individuals who felt stronger high arousal positive effects would crave more if they were in the alcohol vs. placebo condition, whereas individuals who felt stronger low arousal positive effects would crave more, regardless of beverage condition. It was also hypothesized that within-person increases in both high arousal positive and low arousal positive effects during a given moment would be associated with within-person increases in craving during a given moment, regardless of beverage condition. Between- and within-person relations among high arousal negative and low arousal negative subjective effects and craving were also examined, but these analyses were considered exploratory. Hypotheses were not pre-registered.
Methods
Participants
Participants were emerging adult drinkers from a larger placebo-controlled alcohol administration study of contextual influences on alcohol response (see Corbin et al. 2021). Participants were recruited via online and in-person advertisements surrounding a southwestern US university between 2013 and 2017. Eligibility criteria were being age 21–25 and reporting past-month binge drinking (i.e., 4 + drinks in a night for women, 5 + for men). Exclusion criteria included meeting diagnostic criteria for a past-month alcohol use disorder (AUD) or depressive/anxiety disorder, serious mental illness and/or medical conditions, use of psychotropic or pain medications, negative reactions to alcohol, daily or near daily marijuana use, a history of treatment seeking for alcohol problems, or being pregnant/nursing. The mean age of participants was 22.17 (SD = 2.21), 43.3% were female, and 66.5% were White, with the remainder identifying as Asian (9.7%), Black (7.6%), American Indian/Alaskan Native (1.6%), and other (14.6%); 26% of participants identified as Hispanic/Latinx (see Table 1 for descriptive statistics).
Table 1.
Descriptive statistics
| Variable | N | Mean (SD) |
|---|---|---|
| Age | 448 | 22.27 (1.25) |
| Sex | 448 | |
| Male | 253 (56.5%) | |
| Female | 194 (43.3%) | |
| Missing | 1 (.2%) | |
| Race | 448 | |
| White/Caucasian | 296 (66.1%) | |
| Asian | 43 (9.6%) | |
| Black/African American | 34 (7.6%) | |
| American Indian/Native | 7 (1.6%) | |
| Other | 65 (14.5%) | |
| Missing | 3 (.7%) | |
| Ethnicity | 448 | |
| Hispanic/Latinx | 113 (25.2%) | |
| Non-Hispanic/Latinx | 321 (71.7%) | |
| Missing | 14 (3.1%) | |
| Average drinking quantity | 4.63 (2.21) |
N = 448; average drinking quantity was computed as total drinks consumed over the past 30 days divided by total number of drinking days
Procedure
Interested participants completed an online/telephone screener survey to determine eligibility. If eligible, participants were scheduled for two subsequent laboratory sessions. The first laboratory session consisted of a structured clinical interview (Grant et al. 2003) followed by a battery of self-report questionnaires. During this session, if participants did not meet criteria for any of the aforementioned exclusion criteria, they were scheduled for a second laboratory session, consisting of alcohol (or placebo) administration. The second session was scheduled on a weekday between 4 and 6 p.m. Participants were asked not to drink alcohol within 24 h of the session and not to drink caffeine nor eat within 4 h of the session. Before the participant arrived at the second session, research assistants randomly assigned participants to receive either alcohol (N = 270; 60% of participants) or a placebo (N = 178; 40% of participants), and to context conditions crossing social (i.e., drinking alone or in a group of 2–3 participants) and physical (i.e., simulated bar vs. sterile lab) contexts.
When participants arrived for session 2, participant age (21–25) was verified and female participants were administered a pregnancy test and asked to confirm negative results. In addition, a baseline breath alcohol concentration (BAC) reading was administered via an Intoxilyzer 5000 to ensure a 0.00% BAC. Next, research assistants used a computer algorithm (Curtin & Fairchild 2003) to determine the amount of alcohol each participant needed to achieve a 0.08% BAC based upon their sex, height, and weight. Alcohol condition participants were administered three equal-sized beverages made with a ratio of 1 (alcohol) to 3 (mixer; lemon-lime soda, cranberry juice, lime juice). Placebo condition participants were also administered three equal-sized beverages made with a ratio of 1 (decarbonated tonic water) to 3 (mixer). Alcohol (and placebo; decarbonated tonic water) doses were poured out of a vodka bottle to facilitate placebo response; furthermore, glasses were rimmed with vodka, and a squirt of vodka was added to each drink to also facilitate placebo response. Participants in both conditions were given 6 min to drink each drink with a 1-min break in between drinks.
An 8-min absorption period was allowed before periodic breathalyzer readings (using an Alco-Sensor IV) began. Breathalyzer tests occurred every 10 min until participant in the alcohol condition achieved a BAC of 0.06%, which marked the ascending limb of the BAC curve. If a BAC of 0.06% BAC was not achieved within 60 min of the first reading (N = 12), the ascending limb measurements were set to occur at the 60-min mark. BAC measurements were administered every 10 min, and another set of measurements were administered at peak BAC as well as when the BAC most closely matched the exact time of the ascending limb measurement (i.e., descending limb). For those in the placebo condition, timing of ascending, peak, and descending limb assessments was yoked to participants in the alcohol condition. For a full list of procedures, see Corbin et al. (2021).
Measures
Demographics
Participants reported on their sex at birth (male vs. female).
Alcohol use
Participants reported on their past 30-day average drinking quantity via a timeline followback (TLFB) interview (Sobell & Sobell 1992). The TLFB was administered in-person by a research assistant during the first laboratory session. Average drinking quantity was computed as past 30-day number of drinks consumed divided by the number of drinking days.
Subjective response
Subjective response to alcohol (and placebo) was assessed using 14 items from the Subjective Effects of Alcohol Scale (SEAS; Morean et al. 2013). High arousal positive (e.g., talkative, sociable), high arousal negative (e.g., demanding, rude), low arousal positive (e.g., relaxed, mellow), and low arousal negative (e.g., wobbly, dizzy) subjective effects were assessed on a scale of 0 (not at all) to 10 (extremely). All subscales had adequate internal consistency across participants (ω = 0.73–0.86). The SEAS was administered at the ascending, peak, and descending limb measurements.
Alcohol craving
Alcohol craving was assessed via a visual analog scale asking participants how much they want/desire alcohol on a scale of 0–100. This item is in line with other studies using similar items to test liking and wanting during alcohol administration (e.g.,Amlung et al. 2015; King et al. 2011; Motschman et al. 2022; Wardell et al. 2016).
Data analytic plan
Assumptions of normality were examined across variables, and variable outliers (i.e., ± 3 SD from the mean) were winsorized (Tabachnick et al. 2013). Perceived intoxication and number of perceived drinks consumed were examined at the first subjective assessment to test placebo effectiveness.
Since the current study assessed subjective response and craving at three time points within each participant, multilevel modeling was used to test whether (1) within-person deviations in subjective response at a given time point predicted within-person deviations in craving, (2) between-person levels of subjective response predicted between-person levels of craving, and (3) whether within-person and between-person relations among subjective response and craving differed as a function of beverage condition (alcohol versus placebo). A model-building approach was taken for all analyses. First, within-person and between-person main effects of subjective response on craving were entered into the model. All four subjective responses (i.e., high arousal positive, high arousal negative, low arousal positive, low arousal negative) were entered into the model as primary predictors at both the within-person and between-person level. At the within-person level, current assessment limb (i.e., ascending, peak, descending) was covaried. At the between-person level, beverage condition (i.e., alcohol vs. placebo), social context (i.e., social vs. solitary), physical context condition (i.e., simulated bar vs. sterile lab), sex assigned at birth, age, and average drinking quantity were covaried. All exogenous variables were allowed to freely covary.
Second, beverage condition was removed as a predictor at the between-person level, and a multigroup multilevel model was specified with beverage condition (i.e., alcohol vs. placebo) as the grouping variable. In this model, scaled X2 difference testing (Satorra & Bentler 2001) was used to test whether both within-person relations among subjective response and craving (i.e., cross-level) and between-person relations among subjective response and craving (i.e., between-person level) differed based upon whether participants received alcohol or placebo. In the presence of a statistically significant scaled X2 test, simple slopes in the alcohol vs. placebo condition were tested.
Analyses were run in Mplus Version 8.8. All models used maximum likelihood estimation with robust standard errors (MLR estimation), and full information maximum likelihood (FIML) was used to estimate missing data. In line with recommendation from Enders and Tofighi (2007), within-person continuous predictors were group mean centered and between-person continuous predictors were grand mean centered.
Sensitivity analyses
Given documented differences in subjective effects and alcohol outcomes based upon BAC limb (e.g., Corbin et al. 2021; Waddell et al. 2020, 2021), within-person interactions between BAC limb and subjective response predicting within-person deviations in craving were examined. In addition, given documented differences in motivation to drink for relief/reward among men vs. women (McHugh et al. 2018), within-person and between-person interactions between sex and subjective response predicting within-person deviations (and between-person levels) of craving were examined. Since sex was a between-person predictor, multigroup multilevel models tested these moderated effects. However, since BAC was a within-person predictor, multigroup multilevel analyses were not possible. Therefore, standard interaction terms were computed since both predictors (i.e., subjective response and BAC limb) were at level 1.
Results
Outliers and placebo manipulation check
The placebo response was strong. Only 6 participants reported that they believed they had not consumed alcohol (N = 4) or had a 0.00% BAC (N = 2) at the first assessment after beverage administration. Furthermore, there were miniscule differences in subjective effects between these participants compared to the full sample (η2p = 0.001–0.006), and thus, all participants were retained for analysis. Five participants had extreme values for average drinking quantity (> 3 SDs above the mean), and these values were winsorized.
Intraclass correlations were high for alcohol craving (ICC = 0.713) and high arousal positive (ICC = 0.744), high arousal negative (ICC = 0.668), low arousal positive (ICC = 0.671), and low arousal negative (ICC = 0.600) subjective effects, but 30–40% of the variance in each was attributable to the momentary assessment level (i.e., limb) suggesting the utility of multilevel models.
Main effect model
Across beverage conditions, a within-person increase in high arousal positive but not high arousal negative, low arousal positive, or low arousal negative subjective effects was associated with within-person increases in alcohol craving (see Table 2). Similarly, across beverage conditions, higher between-person levels of high arousal positive subjective effects but not high arousal negative, low arousal positive, nor low arousal negative effects were associated with higher between-person levels of alcohol craving.
Table 2.
Multilevel main effects predicting alcohol craving
| b | SE | p value | 95% CI | |
|---|---|---|---|---|
| Within-person level | ||||
| High arousal positive SR | .12 | .04 | .003 | (.04, .20) |
| High arousal negative SR | −.001 | .03 | .97 | (−.06, .06) |
| Low arousal positive SR | −.04 | .03 | .22 | (−.10, .02) |
| Low arousal negative SR | −.01 | .03 | .72 | (−.07, .05) |
| BAC limb | −.30 | .03 | < .001 | (−.35, −.24) |
| Between-person level | ||||
| High arousal positive SR | .19 | .06 | .001 | (.07, .30) |
| High arousal negative SR | .10 | .05 | .059 | (−.004, .21) |
| Low arousal positive SR | −.02 | .05 | .65 | (−.12, .07) |
| Low arousal negative SR | −.002 | .06 | .98 | (−.12, .11) |
| Condition | .17 | .05 | .001 | (.07, .27) |
| Social context | .06 | .05 | .22 | (−.04, .16) |
| Physical context | .05 | .05 | .29 | (−.04, .14) |
| Average drinking quantity | .07 | .06 | .23 | (−.04, .18) |
| Sex at birth | −.16 | .05 | .001 | (−.25, −.06) |
| Age | .09 | .05 | .097 | (−.02, .19) |
Within-person predictors were group-mean centered, and between-person predictors were grand-mean centered
Covariate effects were as follows: at the within-person level, later limbs on the BAC curve were associated with within-person decreases in craving. At the between-person level, being in the alcohol condition and being male were associated with higher between-person levels of alcohol craving (see Table 2).
Interaction models
At the within-person level, relations between high arousal positive (Δχ2(1) = 0.06, p = 0.81), high arousal negative (Δχ2(1) = 2.98, p = 0.08), low arousal positive (Δχ2(1) = 0.92, p = 0.34), and low arousal negative (Δχ2(1) = 0.40, p = 0.53) subjective effects and craving did not differ based upon beverage condition. However, at the between-person level, the relation between high arousal positive subjective effects and craving (Δχ2(1) = 4.07, p = 0.043) and the relation between low arousal positive subjective effects and craving (Δχ2(1) = 9.68, p = 0.001) varied as a function of beverage condition (Table 3).
Table 3.
Differences by beverage condition
| Alcohol condition | Placebo condition | |
|---|---|---|
| Within-person level | ||
| High arousal positive SR → alcohol craving | .12* | .14* |
| High arousal negative SR → alcohol craving | −.02 | .07 |
| Low arousal positive SR → alcohol craving | −.01 | −.08* |
| Low arousal negative SR → alcohol craving | −.03 | .02 |
| Between-person level | ||
| High arousal positive SR → alcohol craving | .26*† | .08† |
| High arousal negative SR → alcohol craving | .10 | .08 |
| Low arousal positive SR → alcohol craving | −.14*† | .16*† |
| Low arousal negative SR → alcohol craving | −.01 | .03 |
Statistically significant effect size within condition
Statistically significant difference between condition
Simple slopes suggested that individuals who had stronger high arousal positive subjective effects reported significantly higher craving if they were in the alcohol but not placebo condition (see Fig. 1). In contrast, individuals who had stronger low arousal positive subjective effects reported significantly lower levels of craving if they were in the alcohol condition but significantly higher levels of craving if they were in the placebo condition (see Fig. 2). The relation between high arousal negative (Δχ2(1) = 0.02, p = 0.87) and low arousal negative (Δχ2(1) = 0.15, p = 0.70) subjective effects and alcohol craving did not differ by beverage condition.
Fig. 1.
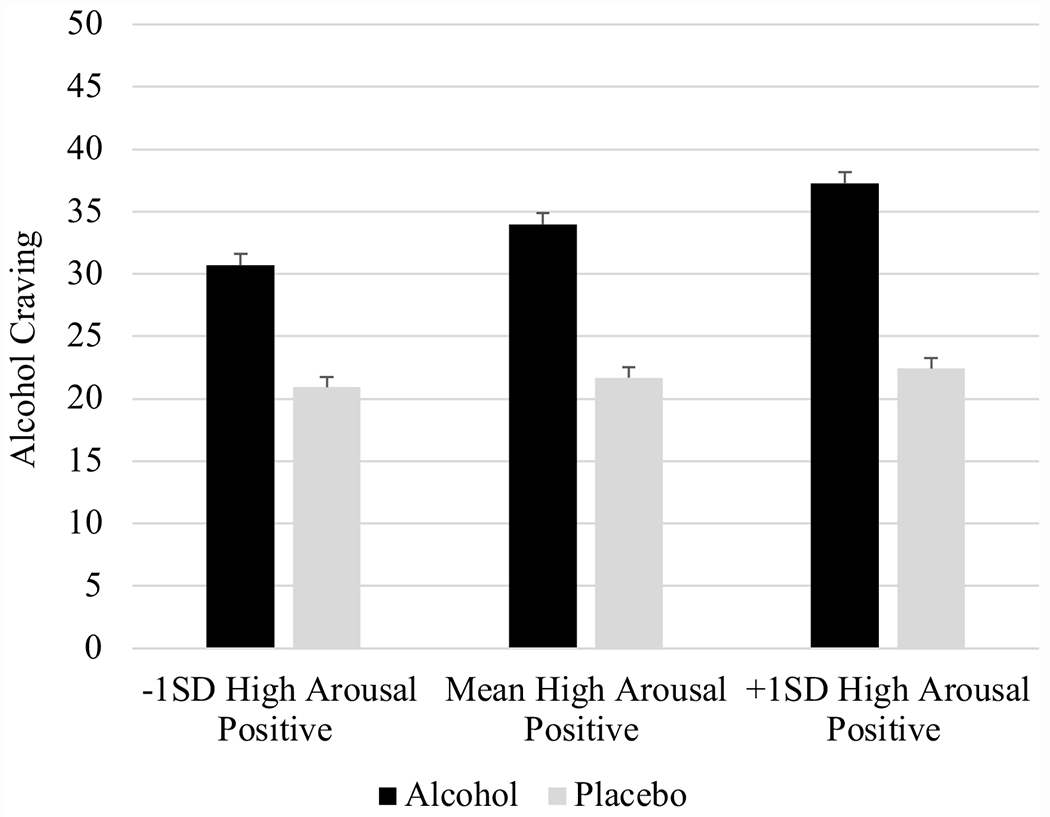
Between-person high arousal positive interaction. Models covaried BAC limb, physical/social context in the laboratory, sex at birth, age, and average drinking quantity
Fig. 2.
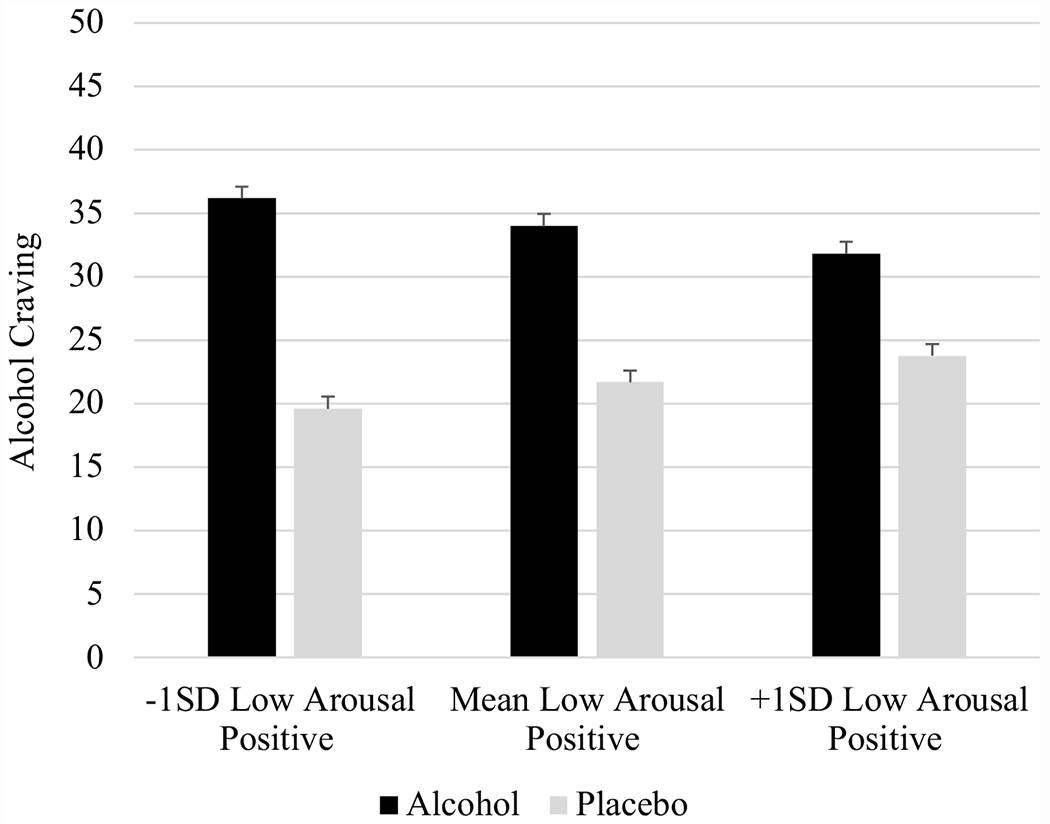
Between-person low arousal positive interaction. Models covaried BAC limb, physical/social context in the laboratory, sex at birth, age, and average drinking quantity
Sensitivity analyses
At the within-person level, the relations between high arousal positive (b = − 0.01, SE = 0.09, p = 0.89), high arousal negative (b = − 0.01, SE = 0.09, p = 0.91), low arousal positive (b = 0.10, SE = 0.12, p = 0.43), and low arousal negative (b = 0.06, SE = 0.08, p = 0.496) subjective response and craving did not vary by beverage condition.
At the within-person level, relations between high arousal positive (Δχ2(1) = 1.23, p = 0.27), high arousal negative (Δχ2(1) = 0.04, p = 0.83), low arousal positive (Δχ2(1) = 0.65, p = 0.42), and low arousal negative (Δχ2(1) = 0.67, p = 0.41) subjective effects and craving did not differ based upon sex. At the between-person level, relations between high arousal positive (Δχ2(1) = 0.19, p = 0.67), high arousal negative (Δχ2(1) = 0.75, p = 0.39), low arousal positive (Δχ2(1) = 0.04, p = 0.84), and low arousal negative (Δχ2(1) = 1.71, p = 0.19) subjective effects and craving did not differ based upon sex.
Discussion
Alcohol craving is a central aspect of theoretical models of addiction, yet event-level methodologies (i.e., EMA, alcohol administration) have largely ignored craving as an outcome of interest. Some studies suggest that subjective response to alcohol is a predictor of acute alcohol craving, but it remains unclear at which level of analysis and if relations are indicative of pharmacological effects or mere expectancies from drinking. Therefore, the current study used placebo-controlled alcohol administration to test whether subjective responses were within-person and/or between-person predictors of acute alcohol craving, and whether these relations differed based upon whether participants received alcohol or a placebo.
At the within-person level, within-person increases in high arousal positive subjective effects (i.e., positive reinforcement) were associated with within-person increases in alcohol craving. However, contrary to hypotheses, there was no moderation by beverage condition, suggesting that, regardless of whether participants received alcohol or not, a within-person increase in positive reinforcement was associated with increased craving for alcohol. Hypotheses regarding within-person effects were grounded in reinforcement theories, which suggest that an increase in positive/negative reinforcement would potentiate alcohol craving out of a desire to continue feeling and/or enhance positive effects (e.g., Baker et al. 2004; Cho et al. 2019; De Wit & Phan 2010; Koob 2013). Therefore, it would make sense that a within-person increase in positive reinforcement, regardless of whether alcohol vs. placebo-induced, would translate into increased desire for more alcohol. Furthermore, it is likely that a variety of contextual influences may have influenced in-the-moment subjective effects (e.g., a group of individuals being more talkative in that moment, an individual attending to a funny scene on the TV screen; e.g., Kohen et al. 2022), which could have increased momentary levels of reward. Thus, these findings point to the important role of acute expectancies at the within-person level, as a momentary increases in reward, regardless of whether alcohol-induced or not, translated into potentiated craving.
At the between-person level, high arousal positive subjective effects were associated with heightened alcohol craving, but only in the alcohol condition. Alternatively stated, individuals who experienced higher average levels of positive reinforcement over a drinking episode reported heightened alcohol craving only in the alcohol (vs. placebo) condition. Thus, between-person relations between high arousal positive effects and craving appeared to be alcohol-induced. One interpretation of these findings is that there is a pharmacological and/or physiological process in the prediction of reward-based craving for those who received alcohol but not placebo. Alcohol-induced high arousal positive/stimulant effects are associated with opioid receptor activity (e.g., Ray et al. 2010, 2013), which is thought to increase reinforcing alcohol effects (e.g., Méndez and Morales-Mulia 2008). Similarly, research suggests that acute ingestion of alcohol is associated with physiological markers of arousal (i.e., heart rate, amylase; Cofresí et al. 2020; King et al. 2023), which are associated with heightened craving (e.g., Chaplin et al. 2010; Coffey et al. 2010). Therefore, it is possible that alcohol-induced physiological arousal + subjective reward potentiates craving relative to subjective reward without alcohol-induced physiological arousal. Since alcohol-induced reward potentiated craving, individuals who are sensitive to positively reinforcing and arousing alcohol effects may be particularly susceptible to acute craving. For example, individuals with a family history of AUD and/or genetic risk for AUD are known to experience more positive reinforcement and arousal when drinking (e.g., Morean & Corbin 2010; Schuckit 2000), and thus may be particularly prone to increased craving when feeling arousal + subjective reward. Furthermore, impulsive traits are a known mechanism of familial/genetic risk for AUD (e.g., Sher 1991; Waddell et al. 2022), and are known to increase alcohol-induced stimulation (e.g., Berey et al. 2019). Thus, person-level risk enacted from familial, genetic, and personality factors may be associated with alcohol-induced reward, which then may potentiate craving during acute drinking episodes.
In contrast, between-person levels of low arousal positive subjective effects, or negative reinforcement, were associated with heightened alcohol craving in the placebo condition but were associated with lesser alcohol craving in the alcohol condition. It is likely that these relations are due to a strong placebo response, as there are little-to-no differences in such effects depending on whether one received alcohol or placebo (e.g., Waddell et al. 2021). Thus, in contrast to high arousal positive findings, pharmacological/physiological effects + subjective negative reinforcement may translate into lesser craving, likely due to the mismatch between pharmacological/physiological arousal and subjective satiation/relaxation. Alternatively stated, physiological arousal induced from drinking alcohol may contrast subjective relaxation, leading to a mismatch of subjective and objective effects and less desire to continue drinking/feeling such effects. On the contrary, when tension reduction is purely expectancy-induced (i.e., placebo), such tension reducing effects may be more enjoyable/satisfying, thereby predicting increased desire for more alcohol. Put together, findings point to alcohol-induced positive reinforcement and expectancy-induced negative reinforcement as predictors of increased craving.
Findings should be interpreted in line with the study sample. The current sample encompassed emerging adults who binge drank but did not meet criteria for an AUD. Models of addiction staging suggest that the early stages of addiction are focused on impulsive use indicative of positive reinforcement, which turns to compulsive use indicative of negative reinforcement when an AUD is developed (e.g., Koob 2013; Vollstädt-Klein et al. 2010). Therefore, the current finding that positive reinforcement potentiated craving fits within these models of reinforcement. Furthermore, Bujarski and Ray (2014) found a similar pattern of effects in heavy drinkers, but rather found that AUD drinkers showed relations among tension reduction and craving. Therefore, the current findings may display aspects consistent with the beginning stages in the process of addiction, and may provide important information for interventions attempting to prevent the progression from positive to negative reinforcement-based drinking.
Findings therefore have important implications for interventions seeking to reduce craving in non-AUD drinkers. First, just-in-time interventions may benefit from tracking subjective reward during acute drinking episodes, and motivating protective strategies (e.g., mixing in water, spacing out drinks; Martens et al. 2007) during moments/times of increased reward. Thus, the current findings suggest that such interventions could be effective at reducing craving, regardless of how much alcohol has been consumed. Second, strong alcohol (but not placebo)-induced relations among positive reinforcement and craving coupled with strong placebo (but not alcohol)-induced relations among negative reinforcement and craving suggest that pharmacological treatments targeting positive reinforcement (e.g., O’Malley et al. 2015) and expectancy challenge treatments targeting negative reinforcement (e.g., Darkes & Goldman 1998) may be most effective in attenuating alcohol craving during drinking episodes.
Findings must be interpreted in light of study limitations. First, a single item assessed craving rather than a validated questionnaire, such as the Alcohol Urge Questionnaire (Bohn et al. 1995). Second, subjective response and craving were assessed 3 times, but other studies have assessed each 5–10 times across a drinking episode (e.g., Motschman et al. 2022), allowing for a more refined assessment of within-person variability. Third, participants were lower-risk drinkers compared to other studies (e.g., Bujarski and Ray 2014; Green et al. 2019), and it is unclear if there are differences based on drinking severity. Fourth, the current study assumed that acute alcohol craving would translate into continued drinking, but ad libitum drinking data was not assessed. Research suggests that craving is consistently associated with continued drinking (e.g., Green et al. 2019; Wycoff et al. 2022), but future research is needed to test between- and within-person processes through which pharmacological/expectancy effects contribute to continued drinking. Finally, although the use of a between-subject design was deemed a strength due to the strong placebo response, future research using within-subject designs should replicate the current pattern of results.
Conclusion
The current study found that relations among subjective response and craving are quite complex. First, within-person relations among acute reward and craving appeared to be expectancy-driven, since there was no difference in those who received alcohol vs. placebo. Second, between-person levels of subjective reward potentiated craving when alcohol-induced, whereas between-person levels of subjective relaxation/calming effects potentiated craving when placebo-induced but attenuated craving when alcohol-induced. Findings may inform theoretical models of reinforcement-motivated craving and may inform interventions seeking to reduce alcohol craving and further drinking behavior.
Funding
This study was supported by funding from the National Institute on Alcohol Abuse and Alcoholism grants R01-AA021148 (PI: William R. Corbin) and F31-AA030167 (PI: Jack T. Waddell).
Footnotes
Conflict of interest The authors declare no competing interests.
Data availability
Data is available from the corresponding author upon reasonable request.
References
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (5th ed.). [Google Scholar]
- American Psychiatric Association (2022) Diagnostic and statistical manual of mental disorders (5th ed. TR). [Google Scholar]
- Amlung M, McCarty KN, Morris DH, Tsai CL, McCarthy DM (2015) Increased behavioral economic demand and craving for alcohol following a laboratory alcohol challenge. Addiction 110(9):1421–1428 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anton RF (1999) What is craving? Models and implications for treatment. Alcohol Res Health 23(3):165–175 [PMC free article] [PubMed] [Google Scholar]
- Baker TB, Piper ME, McCarthy DE, Majeskie MR, Fiore MC (2004) Addiction motivation reformulated: an affective processing model of negative reinforcement. Psychol Rev 111(1):33–45 [DOI] [PubMed] [Google Scholar]
- Berey BL, Leeman RF, Chavarria J, King AC (2019) Relationships between generalized impulsivity and subjective stimulant and sedative responses following alcohol administration. Psychol Addict Behav 33(7):616–625 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bohn MJ, Krahn DD, Staehler BA (1995) Development and initial validation of a measure of drinking urges in abstinent alcoholics. Alcohol Clin Exp Res 19(3):600–606 [DOI] [PubMed] [Google Scholar]
- Bujarski S, Ray LA (2014) Subjective response to alcohol and associated craving in heavy drinkers vs. alcohol dependents: an examination of Koob’s allostatic model in humans. Drug Alcohol Depend 140:161–167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chaplin TM, Hong K, Fox HC, Siedlarz KM, Bergquist K, Sinha R (2010) Behavioral arousal in response to stress and drug cue in alcohol and cocaine addicted individuals versus healthy controls. Hum Psychopharmacol Clin Exp 25(5):368–376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cho SB, Su J, Kuo SI, Bucholz KK, Chan G, Edenberg HJ, Dick DM (2019) Positive and negative reinforcement are differentially associated with alcohol consumption as a function of alcohol dependence. Psychol Addict Behav 33(1):58–69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coffey SF, Schumacher JA, Stasiewicz PR, Henslee AM, Baillie LE, Landy N (2010) Craving and physiological reactivity to trauma and alcohol cues in posttraumatic stress disorder and alcohol dependence. Exp Clinical Psychopharmacol 18(4):340–351 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cofresí RU, Bartholow BD, Fromme K (2020) Female drinkers are more sensitive than male drinkers to alcohol-induced heart rate increase. Exp Clin Psychopharmacol 28(5):540–549 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corbin WR, Scott C, Boyd SJ, Menary KR, Enders CK (2015) Contextual influences on subjective and behavioral responses to alcohol. Exp Clin Psychopharmacol 23(1):59–70 [DOI] [PubMed] [Google Scholar]
- Corbin WR, Hartman JD, Bruening AB, Fromme K (2021) Contextual influences on subjective alcohol response. Exp Clin Psychopharmacol 29(1):48–60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtin JJ, Fairchild BA (2003) Alcohol and cognitive control: implications for regulation of behavior during response conflict. J Abnorm Psychol 112(3):424–432 [DOI] [PubMed] [Google Scholar]
- Darkes J, Goldman MS (1998) Expectancy challenge and drinking reduction: process and structure in the alcohol expectancy network. Exp Clin Psychopharmacol 6(1):64–72 [DOI] [PubMed] [Google Scholar]
- de Wit H, Phan L (2010) Positive reinforcement theories of drug use.
- Enders CK, Tofighi D (2007) Centering predictor variables in cross-sectional multilevel models: a new look at an old issue. Psychol Methods 12(2):121–133 [DOI] [PubMed] [Google Scholar]
- Grant BF, Dawson DA, Stinson FS, Chou PS, Kay W, Pickering R (2003) The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV): reliability of alcohol consumption, tobacco use, family history of depression and psychiatric diagnostic modules in a general population sample. Drug Alcohol Depend 71(1):7–16 [DOI] [PubMed] [Google Scholar]
- Green R, Grodin E, Lim AC, Venegas A, Bujarski S, Krull J, Ray LA (2019) The interplay between subjective response to alcohol, craving, and alcohol self-administration in the human laboratory. Alcohol Clin Exp Res 43(5):907–915 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hendershot CS, Wardell JD, Strang NM, Markovich MS, Claus ED, Ramchandani VA (2015) Application of an alcohol clamp paradigm to examine inhibitory control, subjective responses, and acute tolerance in late adolescence. Exp Clin Psychopharmacol 23(3):147–160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kavanagh DJ, Statham DJ, Feeney GF, Young RM, May J, Andrade J, Connor JP (2013) Measurement of alcohol craving. Addict Behav 38(2):1572–1584 [DOI] [PubMed] [Google Scholar]
- King AC, de Wit H, McNamara PJ, Cao D (2011) Rewarding, stimulant, and sedative alcohol responses and relationship to future binge drinking. Arch Gen Psychiatry 68(4):389–399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- King SE, Waddell JT, Corbin WR (2023) A preliminary investigation of salivary alpha-amylase as a novel biomarker of subjective response to alcohol: a brief report. Advanced Online Publication, Experimental and Clinical Psychophamarcology; [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohen CB, Cofresí RU, Bartholow BD, Piasecki TM (2022) Alcohol craving in the natural environment: moderating roles of cue exposure, drinking, and alcohol sensitivity. Advance Online Publication, Experimental and Clinical Psychopharmacology; [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koob GF (2013) Negative reinforcement in drug addiction: the darkness within. Curr Opin Neurobiol 23(4):559–563 [DOI] [PubMed] [Google Scholar]
- Kranzler H, Edenberg JH (2010) Pharmacogenetics of alcohol and alcohol dependence treatment. Curr Pharm Des 16(19):2141–2148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Love A, James D, Willner P (1998) A comparison of two alcohol craving questionnaires. Addiction 93(7):1091–1102 [DOI] [PubMed] [Google Scholar]
- Martens MP, Pedersen ER, LaBrie JW, Ferrier AG, Cimini MD (2007) Measuring alcohol-related protective behavioral strategies among college students: further examination of the Protective Behavioral Strategies Scale. Psychol Addict Behav 21(3):307–314 [DOI] [PubMed] [Google Scholar]
- Martin CS, Sayette MA (1993) Experimental design in alcohol administration research: limitations and alternatives in the manipulation of dosage-set. J Stud Alcohol 54(6):750–761 [DOI] [PubMed] [Google Scholar]
- McHugh RK, Votaw VR, Sugarman DE, Greenfield SF (2018) Sex and gender differences in substance use disorders. Clin Psychol Rev 66:12–23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Méndez M, Morales-Mulia M (2008) Role of mu and delta opioid receptors in alcohol drinking behaviour. Curr Drug Abuse Rev 1(2):239–252 [DOI] [PubMed] [Google Scholar]
- Monti PM, Rohsenow DJ, Hutchison KE (2000) Toward bridging the gap between biological, psychobiological and psychosocial models of alcohol craving. Addiction 95:S229. [DOI] [PubMed] [Google Scholar]
- Morean ME, Corbin WR (2010) Subjective response to alcohol: a critical review of the literature. Alcohol Clin Exp Res 34(3):385–395 [DOI] [PubMed] [Google Scholar]
- Morean ME, Corbin WR, Treat TA (2012) The Anticipated Effects of Alcohol Scale: development and psychometric evaluation of a novel assessment tool for measuring alcohol expectancies. Psychol Assess 24(4):1008–1020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morean ME, Corbin WR, Treat TA (2013) The Subjective Effects of Alcohol Scale: development and psychometric evaluation of a novel assessment tool for measuring subjective response to alcohol. Psychol Assess 25(3):780–793 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morean ME, Corbin WR, Treat TA (2015) Evaluating the accuracy of alcohol expectancies relative to subjective response to alcohol. Addict Behav 51:197–203 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Motschman CA, Amlung M, McCarthy DM (2022) Alcohol demand as a predictor of drinking behavior in the natural environment. Addiction 117(7):1887–1896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Malley SS, Corbin WR, Leeman RF, DeMartini KS, Fucito LM, Ikomi J, Kranzler HR (2015) Reduction of alcohol drinking in young adults by naltrexone: a double-blind, placebo-controlled, randomized clinical trial of efficacy and safety. J Clin Psychiatry 76(2):17169–17180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quinn PD, Fromme K (2011) Subjective response to alcohol challenge: a quantitative review. Alcohol Clin Exp Res 35(10):1759–1770 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quinn PD, Fromme K (2016) Individual differences in subjective alcohol responses and alcohol-related disinhibition. Exp Clin Psychopharmacol 24(2):90–100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ray LA, Miranda R Jr, Tidey JW, McGeary JE, MacKillop J, Gwaltney CJ, Monti PM (2010) Polymorphisms of the μ-opioid receptor and dopamine D-receptor genes and subjective responses to alcohol in the natural environment. J Abnorm Psychol 119(1):115–124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ray LA, Bujarski S, MacKillop J, Courtney KE, Monti PM, Miotto K (2013) Subjective response to alcohol among alcohol-dependent individuals: effects of the mu-opioid receptor (OPRM1) gene and alcoholism severity. Alcohol Clin Exp Res 37:E116–E124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson TE, Berridge KC (1993) The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Res Rev 18(3):247–291 [DOI] [PubMed] [Google Scholar]
- Satorra A, Bentler PM (2001) A scaled difference chi-square test statistic for moment structure analysis. Psychometrika 66(4):507–514 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuckit MA (2000) Genetics of the risk for alcoholism. Am J Addict 9(2):103–112 [DOI] [PubMed] [Google Scholar]
- Scott-Sheldon LA, Terry DL, Carey KB, Garey L, Carey MP (2012) Efficacy of expectancy challenge interventions to reduce college student drinking: a meta-analytic review. Psychol Addict Behav 26(3):393–400 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sher KJ (1991) Children of alcoholics: a critical appraisal of theory and research. University of Chicago Press [Google Scholar]
- Sobell LC, Sobell MB (1992) Timeline follow-back: a technique for assessing self-reported alcohol consumption. Meas Alcohol Consum Psychosoc Biochem Methods 41–72 [Google Scholar]
- Tabachnick BG, Fidell LS, Ullman JB (2013) Using multivariate statistics (Vol. 6, pp. 497–516). Boston, MA: pearson. [Google Scholar]
- Testa M, Fillmore MT, Norris J, Abbey A, Curtin JJ, Leonard KE, Hayman LW (2006) Understanding alcohol expectancy effects: revisiting the placebo condition. Alcohol Clin Exp Res 30(2):339–348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tiffany ST, Conklin CA (2000) A cognitive processing model of alcohol craving and compulsive alcohol use. Addiction 95(8s2):145–153 [DOI] [PubMed] [Google Scholar]
- Vollstädt-Klein S, Wichert S, Rabinstein J, Bühler M, Klein O, Ende G, … Mann K (2010) Initial, habitual and compulsive alcohol use is characterized by a shift of cue processing from ventral to dorsal striatum. Addiction 105(10):1741–1749 [DOI] [PubMed] [Google Scholar]
- Waddell JT, Corbin WR, Chassin L, Anderson SF (2020) The prospective interactive effects of alcohol expectancies and subjective response on future drinking behavior. Exp Clin Psychopharmacol 30(3):300–311 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waddell JT, Corbin WR, Leeman RF (2021) Differential effects of UPPS-P impulsivity on subjective alcohol response and craving: an experimental test of acquired preparedness. Advanced Online Publication, Experimental and Clinical Psychopharmacology; [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waddell JT, Corbin WR, MacKinnon DP, Leeman RF, DeMartini KS, Fucito LM, O’Malley SS (2022) Within- and between-person effects of naltrexone on the subjective response to alcohol and craving: a daily diary investigation. Alcohol Clin Exp Res 46(3):477–491 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wardell JD, Ramchandani VA, Hendershot CS (2015) A multilevel structural equation model of within-and between-person associations among subjective responses to alcohol, craving, and laboratory alcohol self-administration. J Abnorm Psychol 124(4):1050–1061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wardell JD, Ramchandani VA, Hendershot CS (2016) Drinking motives predict subjective effects of alcohol and alcohol wanting and liking during laboratory alcohol administration: a mediated pathway analysis. Alcohol Clin Exp Res 40(10):2190–2198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Witkiewitz K, Bowen S, Douglas H, Hsu SH (2013) Mindfulness-based relapse prevention for substance craving. Addict Behav 38(2):1563–1571 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization, WHO, & WHO Staff (1992) The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines (Vol. 1). World Health Organization. [Google Scholar]
- Wycoff AM, Motschman CA, Griffin SA, Freeman LK, Trull TJ (2022) Momentary subjective responses to alcohol as predictors of continuing to drink during daily-life drinking episodes. Drug Alcohol Depend 241:10967. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.