

Abstract
The recent pace, extent, and impact of paradigm-changing cancer prevention science has been remarkable. The American Association for Cancer Research (AACR) convened a 3-day summit, aligned with five research priorities: (i) Precancer Atlas (PCA). (ii) Cancer interception. (iii) Obesity-cancer linkage, a global epidemic of chronic low-grade inflammation. (iv) Implementation science. (v) Cancer disparities. Aligned with these priorities, AACR co-led the Lancet Commission to formally endorse and accelerate the NCI Cancer Moonshot program, facilitating new global collaborative efforts in cancer control. The expanding scope of creative impact is perhaps most startling—from NCI-funded built environments to AACR Team Science Awarded studies of Asian cancer genomes informing global primary prevention policies; cell-free epigenetic marks identifying incipient neoplastic site; practice-changing genomic subclasses in myeloproliferative neoplasia (including germline variant tightly linked to JAK2 V617F haplotype); universal germline genetic testing for pancreatic cancer; and repurposing drugs targeting immune- and stem-cell signals (e.g.,IL-1β,PD-1,RANK-L) to cancer interception. Microbiota-driven IL-17 can induce stemness and transformation in pancreatic precursors (identifying another repurposing opportunity). Notable progress also includes hosting an obesity special conference (connecting epidemiologic and molecular perspectives to inform cancer research and prevention strategies), co-leading concerted national implementation efforts in HPV vaccination, and charting the future elimination of cancer disparities by integrating new science tools, discoveries and perspectives into community-engaged research, including targeted counter attacks on e-cigarette ad exploitation of children, Hispanics and Blacks. Following this summit, two unprecedented funding initiatives were catalyzed to drive cancer prevention research: the NCI Cancer Moonshot (e.g., PCA and disparities); and the AACR-Stand Up To Cancer bold “Cancer Interception” initiative.
AACR’s Contributions to Cancer Prevention
Over its 110-year history, the American Association for Cancer Research (AACR) has led the field of cancer research. The organization’s commitment to cancer prevention research is reflected in its mission statement to “prevent and cure cancer through research, education, communication, and collaboration.”
The AACR accelerates dissemination of scientific advances through meetings, conferences (http://www.aacr.org/meetings/), and publications (http://aacrjournals.org/), specifically Cancer Prevention Research and Cancer Epidemiology, Biomarkers, and Prevention. The AACR magazine Cancer Today (https://www.cancertodaymag.org/) focuses on cancer prevention, as does the annual AACR Cancer Progress Report (http://www.cancerprogressreport.org), which is distributed to members of the U.S. Congress and made available to the public. Partnering with leading organizations in all areas of cancer health disparities research community ensures that cancer research benefits all populations and patients regardless of race, ethnicity, age, gender identity, sexual orientation, socioeconomic status, or the communities in which they live (1, 2).
The AACR has a long history of supporting cancer prevention studies, launching its second century of leadership catalyzing a paradigm-changing collaborative funding mechanism to greatly accelerate progress against cancer. This unprecedented new initiative, Stand Up To Cancer (SU2C), was a collaboration between the AACR and the Entertainment Industry Foundation to raise money for breakthrough research and awareness about cancer. The boldest SU2C initiative began a year ago, with the award of four grants, including two Interception (lung and pancreas) Dream Teams, bringing the total number Teams (awarded since in 2009) to 22. Elizabeth H. Blackburn, PhD, winner of the 2009 Nobel Prize in Physiology or Medicine, authored a seminal 2011 article on “cancer interception” published in Cancer Prevention Research (3). Cancer Interception focuses on developing technologies (to detect precancerous activity at an earlier junction) and Interventions to halt its progression. The development of cancers, like heart disease, can be intercepted with risk-reducing agents in the same way that cardiovascular disease can be intercepted with antihypertensive agents, statins, and other interventions. The AACR promotes education and training through workshops, travel awards, and grants to students, post-doctoral fellows, and early-career investigators interested in cancer prevention. The AACR advocates on behalf of researchers, patients, and survivors to support increased and sustained government funding for cancer research and to guide biomedical funding as well as prevention-related public policy. The AACR has established a Cancer Prevention Standing Committee as the major initiative under AACR President Elizabeth Blackburn, to identify high-impact, compelling scientific opportunities in cancer prevention research and guide all AACR efforts dedicated to this field.
To step back and reexamine the field, AACR convened 70 global experts to a three-day summit charged with identifying the five research priorities for further investment. Co-chaired by Drs. Ernest T. Hawk and Scott M. Lippman, the summit covered the full spectrum of research domains relevant to cancer prevention, ranging from basic to population sciences and interception to dissemination. Here, we present an integrated synthesis, based on this comprehensive reassessment and foundation, of the top research priorities and aligned strategic initiatives.
Prioritizing Cancer Prevention
The potential for prevention to reduce the global cancer burden has never been greater and is now recognized by a variety of disciplines (Fig. 1; refs. 4–6). This focus on cancer prevention represents a shift from previous approaches. The cancer research community is redefining the perception of prevention, introducing and implementing the new concept of cancer “interception” (2) and improving the understanding of how and when intervention might optimize health benefits and minimize risks.
Figure 1.
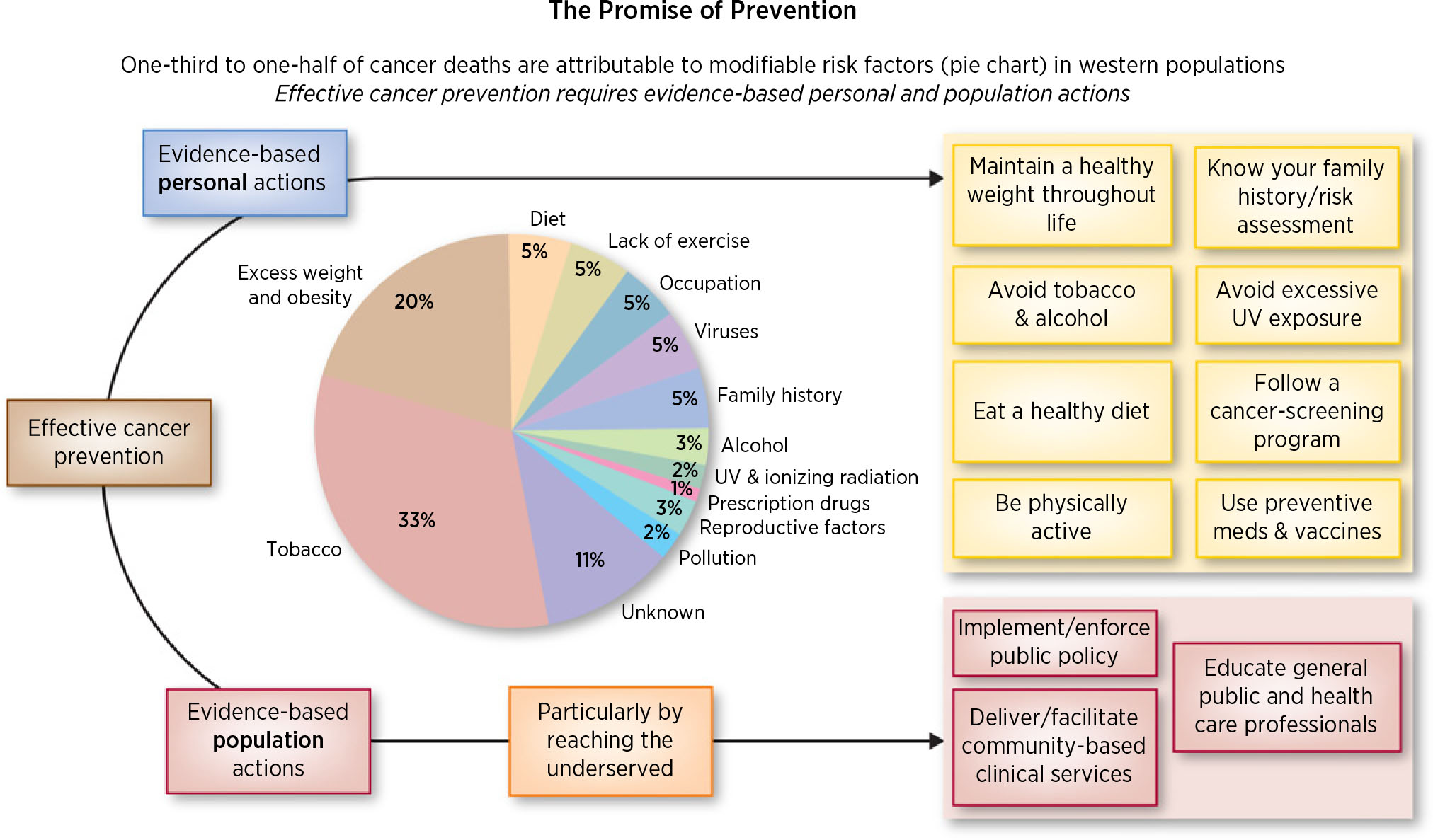
The promise of prevention.
Prevention science has matured over the last 30 years, shifting from primarily descriptive studies that suggested prevention’s potential (7), to interventional studies that prove it.
Cancer research has improved our understanding of the events that initiate and promote oncogenesis and insight into how germline genetics interact with somatic molecular and cellular-related drivers of this process, for example, germline variation can directly affect the mutational landscape of oncogenesis and developing tumors (8).
The U.S. population is growing, becoming more racially and ethnically diverse, and its age distribution is shifting. Increased life expectancy is producing a population that is both larger and older than in previous decades. As age is a strong risk factor for most cancers, this birth-cohort shift will result in more cancer cases as well as more cancer survivors at an increased risk of developing second cancers (9).
Unhealthy lifestyle choices, such as physical inactivity, sedentary behavior and tobacco use, and consequent health outcomes, such as obesity, are unacceptably common, particularly among some racial and ethnic minority groups and low socioeconomic status individuals. High rates of unhealthy lifestyles predict an epidemic of chronic diseases above and beyond that caused by changing demographics alone (10).
Some subpopulations carry a greater burden of unhealthy lifestyle factors and/or exposures and will bear the brunt of the consequent cancers and other chronic diseases. Unhealthy lifestyle patterns are occurring worldwide, particularly in developing countries undergoing rapid economic development. Most future cancer cases will occur in low- and middle-income countries, and yet these countries have limited resources to cope with rising cancer occurrence. New approaches to prevention are needed to reduce the projected cancer incidence in currently underserved populations (e.g., rapidly increasing rates of hepatocellular cancer (HCC) and its precursor nonalcoholic steatohepatitis (NASH; ref. 11) in Hispanic populations linked to obesity and the immigration wave from Latin America.
Cancer prevention has received greater prioritization in the United States due to the passage of the Patient Protection and Affordable Care Act in 2010 with its emphasis on preventive services. Although the future of the Affordable Care Act legislation remains uncertain, the shift toward better health and wellness that the legislation promoted may well be one of its lasting legacies (12).
Prevention efforts have been bolstered by the growing prominence of “value-based” health assessments and care delivery. Such assessments have supported the increased use of cancer prevention interventions, resulting in changes to existing health care quality assessment, guidelines, and reimbursement standards.
Technological advances, such as biomonitors and mobile devices with health applications, have the potential to improve the quality of individual health and health care systems. Real-time assessments and electronic medical records systems can promote more informed communications between institutions, providers, and individuals.
The diversity of factors, underscored by HPV vaccination uptake, including behavioral, psychological, genetic, medical, religious, and social, which influence cancer incidence and outcomes, provide a range of opportunities for preventive intervention.
The resistance of advanced/recurrent cancers to therapy motivates efforts to identify and stop cancers earlier. Cancer interception via early detection and intervention may halt neoplastic progression that could later progress to refractory cancer.
State of Cancer Prevention Science
Cancer control and clinical translation
Cancer prevention is benefiting from new scientific discoveries, and some of these have been translated into tools for risk assessment or risk reduction (13) along pathways resembling those with which diagnostic or therapeutic devices and drugs have been developed. However, several factors differentiate translational pathways supporting prevention from those supporting therapy. Prevention has generally focused on healthy or relatively healthy populations, thus requiring greater vigilance to avoid harm and to assess short- and long-term efficacy. Typical clinical trials, however, do not cover the longer time frame in which prevention could occur before a cancer develops (14). Assessment of preventive measures is further complicated by the lack of consensus among patients, providers, and regulators on what is a meaningful, measurable, and reproducible “clinical benefit” from prevention.
Nevertheless, the pathway from scientific discovery (T0) to population health benefit (T4) is reasonably well-defined (Fig. 2; refs. 15, 16). For example, development of a target-oriented, preventive intervention begins with the design and conduct of phase I and II biomarker-driven clinical trials intended to establish a safe and active dose for further testing (T1 research). T2 research follows, with design and conduct of phase III trials. These trials compare an intervention to established standard preventive regimens, or a placebo if no established preventive standard exists, to determine the relative benefit of the experimental intervention in terms of both safety and efficacy. With sufficient evidence of value, FDA approval is requested. This developmental process is conceptually straightforward, albeit challenging. Few examples of success exist in this pipeline, however, thus discouraging private investments in prevention.
Figure 2.
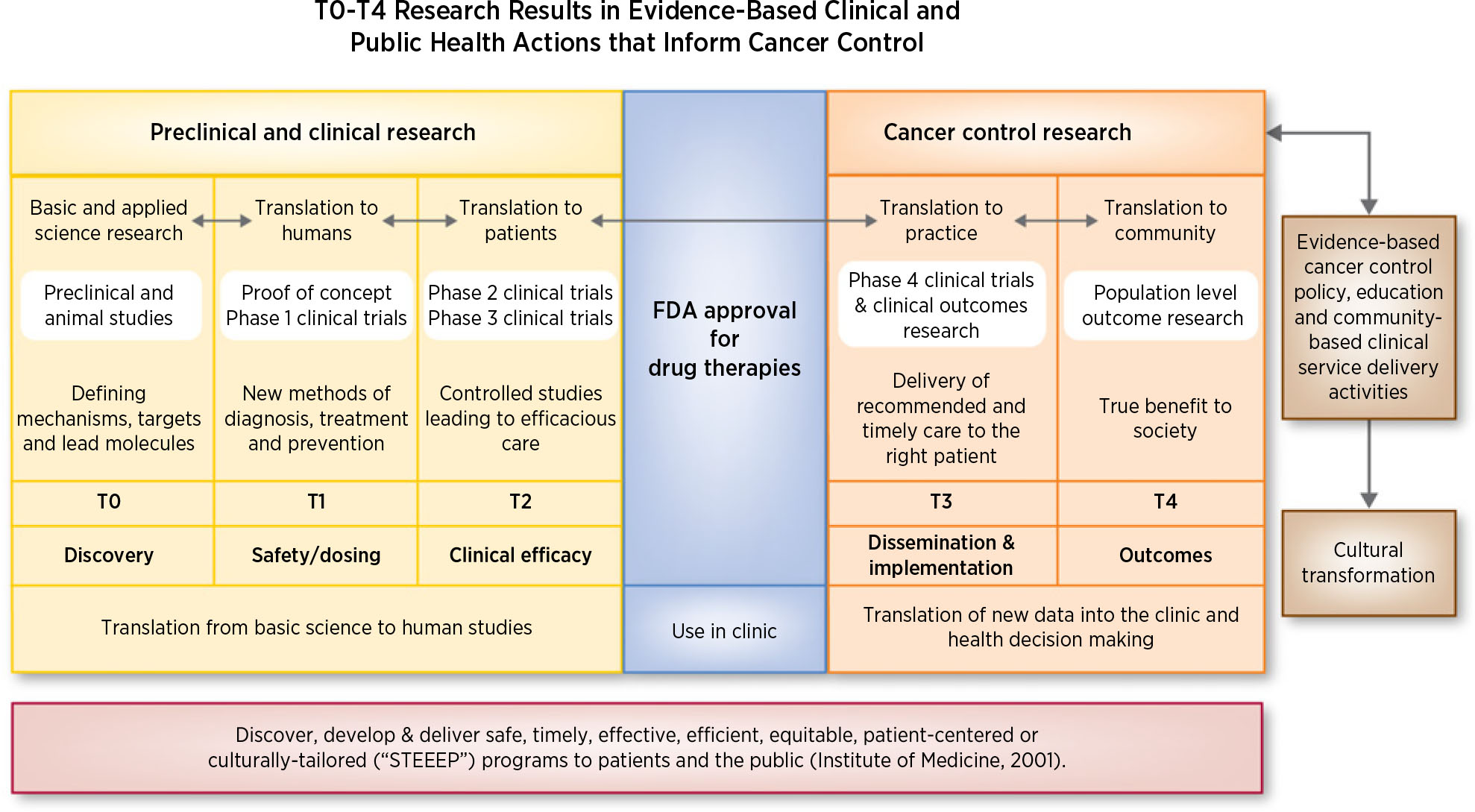
Translational research phases resulting in evidence-based clinical and public health actions to result in impactful cancer control.
Following FDA approval, preventive interventions must be proven safe, potent, and cost effective in the general population over longer durations through implementation-oriented, phase IV clinical trials. These trials gather data on a much broader scope than the clinical trials in T3 research. Phase IV trials query the optimal populations, practitioners, methods, and metrics to establish delivery protocols and understand the range of expected outcomes. The products of such research are incorporated into evidence-based reviews, curricula, best-practice algorithms, guidelines, practice incentives, and quality/outcome measures. Through such evidence-based standards, implementation of preventive measures is optimized across the entire population in T4.
Thus, the process by which evidence is developed to support a novel preventive device or intervention is now relatively clear. Development of such evidence is a growing priority for federal and private funding agencies. The National Cancer Institute, Food and Drug Administration, Agency for Healthcare Research and Quality, Patient-Centered Outcomes Research Institute, Centers for Disease Prevention and Control, Centers for Medicare and Medicaid, and most recently, Stand Up To Cancer (SU2C) all have initiatives designed to advance this research and its subsequent incorporation into evidence-based actions. For example, a national commitment to eradicate cancer by accelerating high-priority research, including in prevention, early detection, and disparities science, was launched in 2016 with the creation of the Cancer Moonshot initiative, signed into law as part of the 21st Century Cures Act (17).
The T0-T4 research process encompasses discovery science, clinical/translational science, and population science, illustrates the challenges and opportunities in cancer prevention and lies upstream of the discipline of cancer control. This field involves discovering, testing, validating, implementation, dissemination, and evaluation of prevention strategies in domains spanning public policy, public and professional education, and community-based clinical and public health services. The cancer control discipline aims to serve public health, with special attention being given to addressing health disparities. Agencies involved in cancer control activities range from large to small and public to private, including government-based social policy, clinical, and public health agencies at the city, county, state, national, and international levels; employers; insurers; health and public health delivery organizations; educational organizations at all levels; private foundations; professional and scientific organizations; and the faith-based community. The latter can by illustrated by the Fe en Acción–Church-based intervention, which was effective in increasing physical activity and decreasing body mass index among Latina women (18).
Launched in 2014, the NCI Community Oncology Research Program (NCORP) is a national network of institutions, replacing NCI’s previously supported community networks, and created to ensure that people have access to clinical trials and the benefits of the latest research, regardless of where they live. In late 2015, the NCI Division of Cancer Prevention (DCP) convened a cancer prevention think tank chaired by Dr. Scott M. Lippman to review the current state of cancer prevention research, identify key prevention research priorities and trials that could be conducted within NCORP, which has a major prevention focus within the DCP (in contrast to NCI’s NCTN). Priorities that emerged include, a pre-cancer genome atlas (PreTCGA), HPV vaccines, immune prevention of noninfectious origins, and overdiagnosis (19).
Given the diversity of evidence-based interventions that can prevent cancer and promote health and wellness across an entire population, as well as the variety and number of institutions involved, we cannot catalog all ongoing initiatives. The individual and cumulative impact of such initiatives is difficult to quantify, as are the gaps in intervention delivery. Cancer control efforts are further complicated if responsibility is broadly distributed, as in the United States, and no leader or single funding agency has emerged. Finally, some cancer control actions may prioritize societal over individual needs, resulting in inadequate support for individuals from adopting evidence-based cancer control actions.
Multi-omic, immune, and stem cell precancer biology
Multi-omic and immune profiling.
The rate-limiting step in cancer prevention has been our limited in-depth study and understanding of the biology of cancer risk (e.g., obesity) and precancer progression, in striking contrast to the extensive study of cancer biology, driving breakthrough advances in precision and immune therapy over the last approximately 5–10 years.. The recent development and application of engineered models, single-cell technologies, and computational tools to study precancer biology is beginning to uncover the immense tumor heterogeneity, elucidate and map pathways and mechanisms that drive neoplastic transformation, and identify molecular subgroups, launching a new era of precision and immune prevention and interception. Large-scale longitudinal and systematic mapping is critical to PCA initiatives. Further complexity is the finding of prevalent driver mutations in completely benign conditions, such as BRAF mutations in benign nevi (20), and age-related early premalignancy (such as clonal hematopoiesis), and esophageal epithelium from older people.
To implement feasible early detection and interception strategies, it is imperative to understand the basis of neoplastic progression and clearly delineate the underlying biology of histologic lesions/conditions that predate cancer, as well as the putative timelines from their initiation to the onset of invasive neoplasia. For example, in certain cancers like glioblastomas and small-cell lung cancers, the absence of well-defined precursor lesions makes preventive strategies particularly challenging (21), while even in lethal cancers like pancreatic ductal adenocarcinoma (PDAC), one can at least envision such a roadmap because of the existence of two well-established precursors and pathways (22, 23) to PDAC – the most common (~80%) involves microscopic precursor lesions known as pancreatic intraepithelial neoplasia or PanIN, and the other major subtype (~10%) involves macroscopic (cystic; principally mucinous) or intraductal papillary mucinous neoplasms (IPMN)–precursor lesions, principally of mucinous cysts of the pancreas. The cell of origin for both precursor types is different (24), although both harbor oncogenic point mutations of KRAS as the common defining genetic alteration, but PanINs acquire subsequent p16 or p53 loss, while IPMNs also harbor “hotspot” oncogenic mutations of GNAS that encodes for the alpha subunit of a stimulatory G-protein. The recent development of genetically engineered models of IPMN provides a unique opportunity to test these paradigms of immune prevention in systems that phenocopy the human disease (25, 26).
Multiple studies have shown that even “apparently sporadic” cancers can occur on the backdrop of unsuspected germline mutations (27–30). As a result, the National Comprehensive Cancer Network recommends genetic testing for all cases of ovarian cancer and is now pivoting toward universal germline genetic testing for pancreatic cancer with the intent of “cascade testing” first-degree relatives who might also harbor unsuspected germline mutations and thus, be candidates for screening and cancer interception. Further rationale for this approach in pancreatic cancer is the devastating outcome and recent signals of benefit from surveillance (31, 32).
Elucidating molecular and cellular drivers of precancers is critical to developing precision and immune prevention. The complexity, diversity and pathways of precancer development and transformation causes great intra- and inter-tumor heterogeneity and individual variation. Emerging molecular and cellular studies exploiting advanced bigdata approaches are beginning map this complexity (33). Recent studies of colorectal and myeloproliferative neoplasia highlighted below have identified premalignant genomic subgroups, critical to refining preventive screening, risk stratification, and target identification (34). Precision prevention may account for disease heterogeneity (35, 36) with interventions tailored to precancer biologic subgroups (37). Current data suggest that cancer develops as a consequence of progressive genomic and epigenomic alterations (38, 39), which can drive immune escape and occur in the context of an inflammatory microenvironment. Recently, HCC precursor progression was mechanistically linked to defects in innate and adaptive immunity (40–43). Macrophage PI3Kγ drives PanIN progression (44). Single-cell transcriptomic analysis of IPMNs demonstrated progressive alterations in the immune microenvironment from low-grade dysplasia to invasive cancer (45). Unraveling the mechanisms of innate and adaptive immune downregulation in inflammatory subsets of lung premalignancy is already identifying potential immune/inflammatory prevention targets such as interleukin-1β inhibition, recently been shown to reduce lung and other cancer incidence (46–49). Furthermore, metformin alleviates tumor inflammation by reducing the expression of inflammatory cytokines including IL-1β as well as infiltration and M2 polarization of tumor-associated macrophages (TAMs) in vitro and in vivo (48). Canakinumab targeting the interleukin-1β innate immunity pathway, significantly increased the rate of fatal infections and sepsis, but the striking difference in lung cancer rates drew immediate attention and set in motion plans by Novartis for a follow-up phase I study of the combination of canakinumab and a programmed cell death protein 1 (PD-1) inhibitor in patients with non-small cell lung cancer (www.clinicaltrials.gov). The relationship between inflammation and cancer is complicated, with features of inflammation that range from adaptive to maladaptive (49). In general, chronic inflammation has long been implicated in the genesis and promotion of tumors following inflammatory lung, bowel, and liver disease. A specific role for IL-1β is suggested by preclinical studies. In mice, IL-1β decreases tumor invasion, growth, and metastases (50). IL-1β also stimulates production of IL-6, a well–established mediator of tumor growth in experimental systems. The anti–IL-6 antibody siltuximab has not produced benefit in multiple myeloma but is FDA-approved for the treatment of idiopathic multicentric Castleman disease (51). Anti–inflammatory drugs might have the opposite effect of dampening the immune response to tumors, and this consideration, in fact, prompted the investigators in the lung trial to record data on cancer incidence and death as a secondary aim of the trial (46). Specifically, a proinflammatory infiltrate comprised of cytotoxic T cells, Th cells, and dendritic cells was progressively depleted and replaced with an immunosuppressive myeloid-derived suppressor cell infiltrate during neoplastic progression. Such studies suggest that immune interventions are more effective in the setting of inherent immunity to driver signals (e.g., see SOX2 below), to boost host immune response. Such studies suggest that immune-based intervention may have value when applied in a preventive context, potentially “normalizing” the immune suppressive milieu back to one where the neoplastic cells are “rejected” by a productive immune infiltrate. In preclinical models, vaccination against aberrantly expressed or mutated self-proteins prevented inflammation-induced colon cancer (52), ductal carcinoma in situ and HER2+/ER− breast cancer (53), and progression of (PanIN; ref. 54). Vaccination has also been shown to block tumor development in transgenic animal models that develop spontaneous tumors (55).
Commensal microbiota can influence cancer initiation and progression in tissues such as the colon that are in direct contact with gut microbiota (56), as well as in other tissues without such contact (57). Recent computational studies have identified microbiome genomic signatures associated with NASH progression (58). The pancreatic microbiome promotes oncogenesis in preinvasive spontaneous and engineered mouse models by induction of innate and adaptive immune suppression. Specific strains of gut and intratumoral bacteria induce an immunosuppressive microenvironment favoring oncogenic progression (59). Ablation of the microbiome with antibiotics reshapes the tumor microenvironment (TME), inducing T-cell activation, improving immune surveillance, and increasing sensitivity to immune interception (60, 61) while depletion of the gut microbiome promoted the efficacy of immunotherapy in established tumor models (62). Age-associated changes in gut commensal microbes may be a mechanism of the age-related cancer (63). Recent computational studies have identified microbiome genomic signatures associated with precancer progression and germline influence on shaping the somatic and immune landscape (64, 65).
The use of liquid biopsies for cancer detection and monitoring is rapidly changing standards of care, and technical advances improving sensitivity can detect low levels circulating tumor DNA among patients with early-stage cancer, in the post resection adjuvant setting and even isolated precancer cases (66), suggesting the potential of blood-based molecular screening for early, preinvasive stages of neoplasia from a variety of tissues. The process by which molecules carrying precancer mutations may be transmitted into the circulation are unclear but may include both cell-free DNA and membrane-bound extracellular vesicles, including exosomes (67, 68). Detection of precancerous traces of diverse cancers in the blood represents a growing area of research, although it needs to be balanced with the concerns for overdiagnosis of indolent precursor lesions or the release of mutant DNA from clonal hematopoiesis or aging tissues (69). The latter is illustrated by ultra-deep NGS detection of tiny “premalignant” clones in the blood of up to 95% of healthy women in their 50s (70). Methylation and proteomic marker panels have produced promising early detection results (71, 72). Remarkably, it was very recently demonstrated that methylation patterns on circulating tumor DNA could further implicate the site at which the tumor was developing (73).
Stem cell signals in cancer development and interception.
In addition to breakthrough advances in omic and immune precancer biology, recent studies identified stem cell/progenitor signals and reprogramming that drive oncogenesis (74) and revealed the potential of targeting stem cell pathways to prevent malignant transformation. Musashi (Msi) is a key stem cell signal upregulated during pancreas oncogenesis and genetic loss or blockade of Msi can inhibit tumor growth and propagation. Msi knock-in reporter mice allowed functional and image-based tracking/mapping of stem cell signals, revealing that Msi was a key driver of PanIN progression (75).
Elegant studies of luminal stem/progenitor cell biology have created a transformative potential to prevent/delay BRCA1-associated breast cancer, a disease for which the best current preventive option is prophylactic surgery. A highly proliferative subset of luminal progenitor cells give rise to basal-like breast cancer, which constitutively express RANK and are hyper-responsive to RANK-L (produced by mature luminal cells that express PR), a key mediator of progestin-driven mammary tumorigenesis, before transitioning to a hormone-independent (e.g., NFκB activated) state. RANK-L/RANK signaling also can influence innate and adaptive immunity. Pharmacologic RANK-L inhibition (or RANK deletion) in mouse models inhibits Brca1-driven mammary tumorigenesis (76–78). Targeting RANKL directly is more selective and less toxic than targeting ER or NFκB to prevent mammary cancer in the BRCA1-mutation setting. Denosumab (a RANK-L mAb inhibitor FDA approved in 2010 for treating postmenopausal osteoporosis and preventing skeletal events) is in development for breast cancer prevention trial in BRCA1-mutation carriers, based on the above research and recent clinical data indicating that risk-reducing salpingo-oophorectomy is ineffective in this setting.
Studies of stem cell biology in hematologic neoplasia also identified stem cell targets for interception. Recent data in the leukemic precursors myeloproliferative neoplasms (MPN) have identified distinct genomic subgroups, defined by genetic driver mutations (e.g., in JAK2, CALR, and MPL) that predict leukemic transformation (79). Inflammatory cytokine-mediated activation of JAK2/STAT signaling enhances expression of an RNA editing enzyme adenosine deaminase acting on RNA (ADAR1), and deregulated ADAR1 activity leads to hyperediting of tumor suppressors that are associated with preleukemia stem cell transformation (80). JAK2 inhibition blocks ADAR1 transcriptional activation, which could prevent oncogenic transformation of preleukemic progenitors into self-renewing leukemia stem cell in MPNs. MPN studies also uncovered germline–somatic interactions driving premalignant progression (81, 82). ADAR1 editase activity can also drive epithelial oncogenesis (83). Stemness has also been reported to mediate high-fat diet–induced intestinal tumorigenesis (84). Search for shared targets of immune response led to the finding that T cells against stem cell antigens (such as SOX2) are particularly enriched in myeloma precursors (versus multiple myeloma). Prospective data demonstrate that baseline SOX2-specific T-cell immunity correlates with reduced rates of progression and transformation to multiple myeloma in patients with asymptomatic myeloma precursor states (85).
Colorectal adenoma–carcinoma model.
Studies in this setting illustrate many of the advances in elucidating precancer omic, germline, immune, and stem cell biology. It has taken almost three decades to obtain a detailed annotation of the genomic events initially described in the seminal multistep genetic model by Vogelstein and Fearon (86). Until recently, most of the studies conducted in colorectal precancers interrogated restricted numbers of lesions and genomic aberrations. Deployment of next-generation sequencing (NGS) technologies has transformed our understanding of the genomic landscape of precancers (87). Whole-exome sequencing analyses of small adenomas from patients with familial adenomatous polyposis (FAP) have established a catalog of >200 somatic hits; hints of clonal selection and mutational rate that overlapped with early-stage carcinomas. In fact, 25% of the mutational load present in adenomas (all passenger mutations) was already present in normal samples, providing direct evidence that a substantial proportion of the genomic variation present in colorectal cancers is present prior to the acquisition of a driver event in at-risk tissues, probably secondary to the self-renewal process generated by stem cells. IL-1β may promote colon tumor invasion through activation of cancer stem cell self-renewal and epithelial-mesenchymal transition, and Zeb1 plays a critical role in these two processes. Thus, IL-1β and Zeb1 might be new therapeutic targets against colon cancer stem cells. Host/microbiome interactions are important in premalignant biology and add another layer of TME complexity. Studies in genetically engineered mouse models have found that APC loss disrupts the intestinal epithelial barrier, facilitating invasion of microbes and microbial nucleic acids that activate adenoma-associated macrophages to produce IL-23, which then stimulates IL-17 production by T cells, accelerating adenoma development and progression. Bacterial translocation can activate toll-like receptors that can upregulate other inflammatory elements. These barrier defects drive an environment of innate inflammation that leads to adenoma proliferation in a background of an immunosuppressive TME (88). Additional studies have been published subsequently annotating unique sets of samples with growth rates assessed by CT colonography and profiled from paraffin (89) or analyzed by orthogonal analyses integrating mutation, copy number, and methylation data (90).
The available data on the genomic annotation of intestinal carcinogenesis and precancers has come mainly from hereditary colorectal cancer syndromes, which recapitulate the two major pathways in sporadic colorectal cancer: chromosomal instability (non-hypermutant) and mismatch repair deficiency (hypermutant). Advantages of studying precancer biology in hereditary cancer syndromes includes: (i) accelerated pace of carcinogenesis, (ii) relative abundance of tissue to perform analysis, and (iii) frequent and close surveillance. FAP, a very severe and rare disease caused by a germline mutation in APC, is a molecular model for the most common (85%) sporadic colorectal cancer characterized by chromosomal instability (91). Colorectal carcinogenesis is accelerated in FAP due to faster acquisition of somatic APC hits; subsequent somatic driver mutations (e.g., KRAS/BRAF and TP53) occur at a normal pace (92). In fact, the initial descriptions in 2016 of the genomic landscape of colorectal precancers using NGS technologies leveraged biorepositories of FAP samples (93). These studies provided a catalog of the somatic variation cooperating with APC in colorectal carcinogenesis. The central role of the gut microbiome in FAP is shown by the interplay between enterotoxigenic Bacteroides fragilis and IL17 in the adenoma to carcinoma transition (59). The other major oncogenic pathway is illustrated by Lynch syndrome, caused by germline DNA mismatch repair (MMR) defect, which induces a fundamentally distinct APC mutation (frameshift), a model for 12% of sporadic hypermutant colorectal cancers. Lynch syndrome accounts for ~4% of CRC diagnoses and has a lifetime CRC risk of ~6% (94). The incremental 5-yearrisks of CRC are age-dependent, ranging from 0.5–1.0% in people age >50 years old. Defects in DNA repair generate exponential accumulation of point mutations at microsatellites tracts, generating neoantigens and accelerating carcinogenesis (92, 95). Whole-genome transcriptomics in Lynch syndrome premalignancy found activation of CD4 T cells and immune checkpoints (LAG-3 and PD-1), independent of the acquisition of hypermutation, likely linked to the neoantigen repertoire derived from MMR deficiency (96). Prior reports have cataloged the neoantigen repertoire displayed by MMR-deficient carcinomas (97), immunogenicity elicited by such neoantigens in T cells, and novel mechanisms of immune escape in Lynch syndrome carriers (98, 99). Refinement of bioinformatic tools coupled with NGS technologies will allow a more precise definition of the neoantigen repertoire presented in premalignancy by both MHC-I and II to guide the personalized vaccine development for cancer interception (100, 101).
Recent translation of hereditary to sporadic precancers applied the colorectal cancer–specific consensus molecular subclassification (CMS; ref. 96). The CMS has changed the prognostic landscape of colorectal cancer (102), describing four transcriptomically distinct subgroups: CMS-1, which recapitulates MMR-deficient tumors and CMS-2, -3, and -4, subdividing the broad molecularly diverse chromosome-instable group. Chromosome-unstable colorectal cancers depend on WNT activation (CMS-2), metabolic (e.g., fructose, glutamine, and fatty acid) pathway deregulation (CMS-3), and epithelial–mesenchymal transition (CMS-4). CMS-1 and -2 were the main subgroups identified in colorectal precancers with small (<5%), but biologically relevant CMS-3 and -4 subtypes. CMS-1 lesions tend to display a serrated appearance with activation of immune pathways (PD-1 activation and immune signals) and BRAF mutations. Subsequent studies will have to link this classification to samples from prospective cohorts with long-term follow-up to connect CMS subtypes with colorectal cancer risk and adapt the CMS classifier to premalignant biology and the transcriptomic signals that drive transformation.
Preventive agent trials in the colorectal adenoma-carcinoma model have produced major advances. Aspirin is an example of a repurposed preventive compound with consistent 20% to 30% reductions in colorectal adenoma incidence and colorectal cancer risk and mortality in a large array of observational and experimental studies. Clinical benefit has been established in RCTs in the sporadic and Lynch syndrome setting. Regular aspirin use may also complement the benefits of screening. Prospective cohort studies suggest that the aspirin’s reduction of colorectal cancer risk could be mediated in part by prostaglandin catabolism, MYC, PIK3CA mutations, and immune response in the TME. Cohort and preclinical data suggest interactions between aspirin use, germline variants, and somatic mutations on colorectal cancer risk (103), illustrating the potential of predictive biomarkers and precision prevention. The USPSTF has recommended aspirin in individuals ages 50–59 and a 10% 10-year risk for cardiovascular events, noting additional benefits of reductions in colorectal cancer with long-term use. The balance of benefits and harms may change substantially with age, because the risk of major bleeding risk increases with age. For that reason, the USPSTF rated the evidence “Insufficient” (I) for adults age 70 or older. In the future, recommendations for use may be refined according to germline genotypes, phenotypic biomarkers, or specific clinical situations.
The clinical impact of prevention agent combinations is illustrated by the breakthrough trial sulindac and erlotinib, which reduced the occurrence of duodenal adenomas (104–106). Recent transcriptomic and other correlative science studies from this landmark-positive randomized trial in FAP identified molecular targets and innate immune pathways mediating sulindac–erlotinib suppression of duodenal polyposis; and Kras mutations attenuated sulindac efficacy in mouse models, with implications for precision prevention (107).
Paradigm-changing work in Lynch syndrome has led to universal tumor testing for microsatellite instable (MSI)-positive as a screen for Lynch syndrome, recommended for all colorectal cancers by multiple professional organizations, including the American College of Gastroenterology, the U.S. Multi-Society Taskforce on Colorectal Cancer, and the NCCN. The Society for Gynecologic Oncology and the American College of Obstetrics and Gynecology have likewise recommended universal testing of all endometrial cancers for MSI-positive as a screen for Lynch syndrome. Despite these recommendations, implementation of universal tumor screening has been challenging. A recent study found that <30% of colorectal cancers were screened for Lynch syndrome at the time of diagnosis. The recent clinical impact and FDA approval of a PD-1 inhibitor in all metastatic MSI-positive cancers will likely increase tumor testing in this setting. New data indicate the value of up front NGS tumor testing to potentially replace immunohistochemical staining for MSI, when the cost and turnaround time of such testing improve (108).
Given the great impact of PD-1 inhibitors in MSI-positive advanced cancers (both Lynch syndrome and sporadic MSI-positive; ref. 109), immune interception is beginning to be studied in Lynch syndrome. Translating immune therapy to cancer interception strategies in LS carriers is attractive based on 2 factors: healthy (no precancers or cancers) Lynch syndrome carriers are at higher cancer risk than the general population (with 5-year cancer rates of 5–14%; ref. 110), and have evidence of host T-cell immunity (which predicts benefit from interventions to boost host immunity). More complex biologic and ethical issues and concerns exist with translating the PD-1 inhibitor Lynch syndrome therapeutic success to the prevention setting, due to the need to balance the unknown long-term risks (e.g., autoimmune serious adverse effects) with the potential for cancer prevention. In MLH1 & MSH2 mutation carriers, the risk of colorectal cancers plus adenomas is ~30% within five years after the original surgery, and 50% within 15 years. In the same Lynch syndrome carriers, prior colorectal cancer resection increases 5-year risk to ~48–58% (all figures are age dependent). These issues are illustrated by a cutting edge ongoing immune interception trial (NCT03631641) of PD1 blockade in a 2–3 fold higher-risk Lynch syndrome colorectal cancer survivor population (prior resected colorectal cancer at least one year before trial eligible, and higher risk MMR gene defects, MLH1 or MLH2 carriers). An international trial is testing a cancer vaccine in healthy Lynch syndrome carriers. It is well-known that African Americans suffer the highest burden from colorectal cancer of all race–ethnicities in the U.S. However, familial risk of colorectal cancer has not been well-studied among African Americans. A relatively large study characterized the mutation spectrum and colorectal cancer risk among 51 African American families with the Lynch syndrome. The authors reported that among African Americans, the predominant phenotype was MLH1 (61%) followed by MSH2 (21%), whereas among Caucasians with Lynch syndrome in the literature, the predominant phenotype is MSH2 followed by MLH1 (111).
Primary prevention
Primary prevention is focused on reducing cancer incidence by avoiding carcinogen exposure. Interventions are intended to remove, avoid, or increase resistance to a risk factor or carcinogenic exposure. Interventions include those for use in apparently healthy individuals to prevent initiation of carcinogenesis, for example, preventing smoking initiation and avoiding UV exposure. A striking example of a molecular prevention intervention is immune interception with HPV vaccination. Nonetheless, the use and definition of molecular prevention is currently evolving. Molecular prevention may also be applied in a secondary context (Fig. 3) to slow further progression. Study of cancer genomic landscapes, imprinted during the process of cancer development, has revealed >30 distinct mutational signatures (cancer.sanger.ac.uk/cosmic/signatures), indicative of exposure to preventable carcinogens (e.g., tobacco, UV light, and aflatoxin), and identifying previously unknown carcinogens (112, 113). The application of NGS to tumors has major and unexpected implications for primary prevention, as highlighted by a recent study of aristolochic acid (AA), a compound found in certain traditional herbal medicines. A provocative recent study utilizing this technology and approach on established cancers identified AA, a very potent human carcinogen commonly found in certain plants and herbs, to cause 78% of liver cancer in Taiwan and 47% of liver cancer in China. The Singapore team that led this study received the recent AACR team-science award. Especially in light of the wide availability of AA-containing plants and herbs, education and public awareness are paramount for primary prevention. For instance, research on AA revealed a potential role for AA exposure in the development of liver cancer. This finding both increased public awareness of the risks of AA exposure and led regulatory agencies to announce stricter policies on use of AA-containing plants. For example, the same research team identified major genetic abnormalities in stomach cancers, a leading cause of global cancer death, and were able to translate these findings into clinical trials targeting these abnormalities. They also showed how parts of DNA affected by carcinogens can be used as screening tools to identify previously undetected carcinogen exposures (114).
Figure 3.
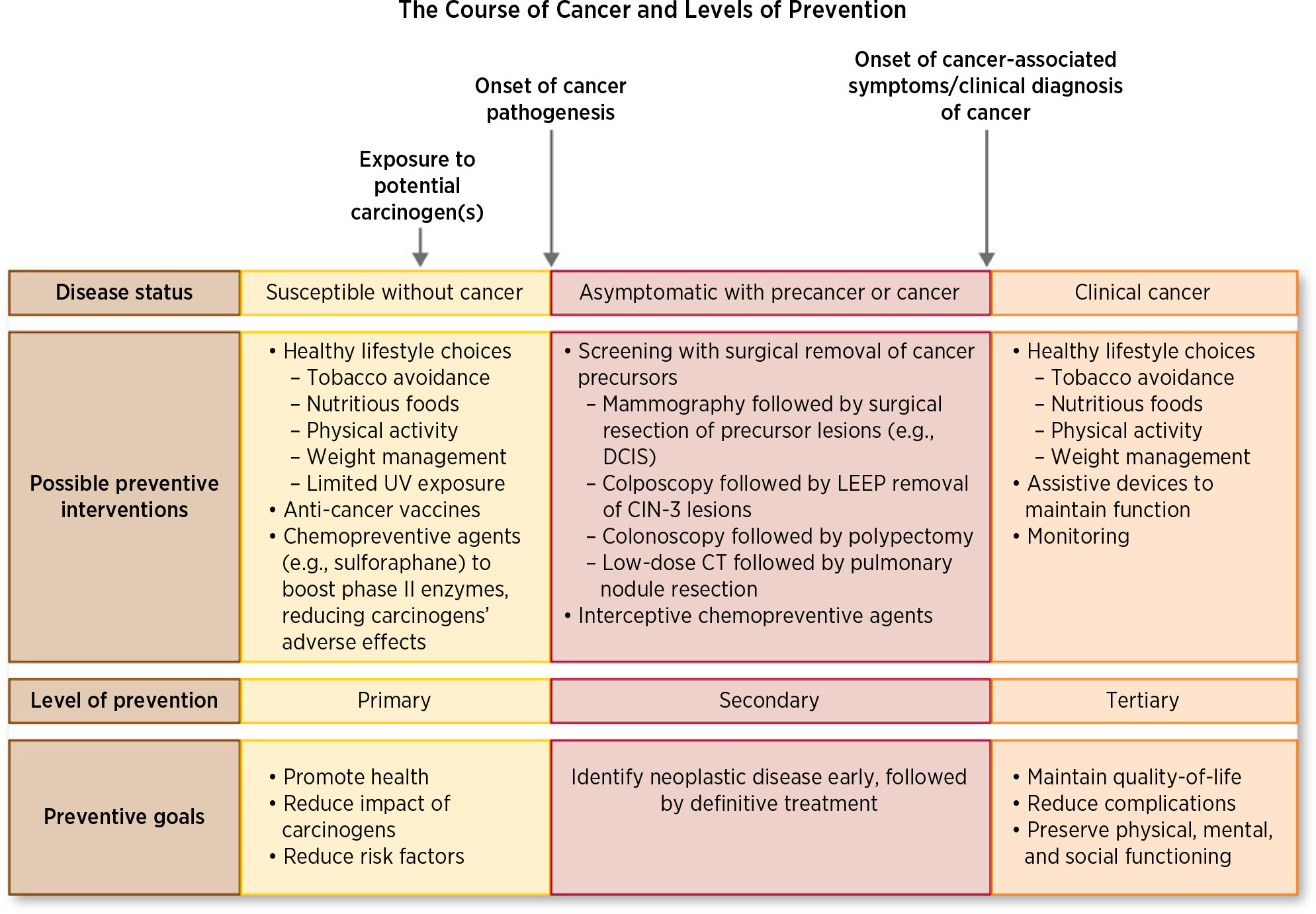
The course of cancer and levels of prevention.
Lifestyle-related and environmental exposures contribute to and, in some cases, drive the bulk of cancer incidence and cancer-related deaths worldwide (5). Many of these factors are modifiable through actions that may be taken to reduce exposures to noncritical levels at the individual and/or population levels (Table 1). In the context of tobacco, primary prevention at the individual level would be avoidance of tobacco use, whereas primary prevention at the population level would be implementation of a tobacco control program consisting of policy changes, education, and delivery of cessation services to reduce exposure broadly (115).
Table 1.
Prevalence of factors that modify the risk of cancer in the United States along with relevant cancer preventive actions at the personal and population levels
| Risk modifier | Average national prevalence | States with highest and lowest prevalence |
Related evidence-based personal actionsa | Related USPSTF/ACIP recommendation | Related evidence-based cancer control actionsb |
||
|---|---|---|---|---|---|---|---|
| Highest | Lowest | For the community | For the clinic | ||||
|
| |||||||
| Cigarette smoking | Avoid or eliminate tobacco use | Clinicians ask about tobacco use, advise to stop, & provide behavioral interventions & FDA-approved pharmacotherapy for cessation (the 5A’s model) | Increasing the unit price of tobacco products Mass media campaigns when combined with other interventions |
Provider reminders when used alone or with provider education (cessation) | |||
| Adult | 15.1 (2014) | West Virginia, 26.7 | Utah, 9.7 | Primary care clinicians provide interventions, including education or brief counseling, to prevent initiation of tobacco use among school-aged children & adolescents | Smoke-free policies Mass-reach health communication interventions (cessation) |
||
| Youth (high school students) | 10.8 (2014) | West Virginia, 18.8 | Utah, 4.4 | Mobile phone-based interventions (cessation) Quitline interventions Reducing client out-of-pocket costs for cessation therapies Community mobilization with additional interventions (restricting minors’ access) Incentives & competitions to increase smoking cessation combined with additional interventions (among workers) |
|||
|
| |||||||
| Heavy drinking | |||||||
| Adult | 5.9 (2015) | D.C., 9.1 | West Virginia, 3.5 | Men: No more than 2 drinks per day | Clinicians screen adults ≥18 & provide behavioral counseling interventions for alcohol misuse | Increasing alcohol taxes | Electronic screening and brief interventions (may be used in various community settings as well) |
| Youth (high school students) | 17.7 (2015) | Montana, 20.7 | Virginia, 11.0 | Women: No more than 1 drink per day | Dram shop liability Regulation of alcohol outlet density Maintaining limits on days & hours of sale Enhanced enforcement of laws prohibiting sales to minors Privatization of retail alcohol sales (recommended against) |
||
|
| |||||||
| BMI ≥ 30 | |||||||
| Adult | 29.8 (2014) | Louisiana, 36.2 | Colorado, 20.2 | Be as lean as possible throughout life without being underweight Avoid excess weight gain at all ages |
Clinicians screen adults & children ≥6 for obesity & offer or refer to intensive, multicomponent behavioral interventions | Behavioral interventions to reduce recreational, sedentary screen time (children <13 years old) | |
| Youth (high school students) | 13.9 (2015) | Mississippi, 13.9 | 10.3, Montana | For those who are overweight or obese, losing even a small amount of weight has health benefits and is a good place to start Get regular physical activity and limit intake of high- calorie foods and drinks as keys to help maintain a healthy weight |
Worksite programs Multicomponent coaching/ counseling interventions to reduce weight & to maintain weight loss Multicomponent interventions to increase availability of healthier foods and beverages in schools Meal and fruit and vegetable snack interventions to increase healthier foods and beverages provided by schools |
||
|
| |||||||
| Lack of physical activity | 22.1 (2014) | Mississippi, 31.4 | Colorado, 16.4 | Adults: at least 150 min of moderate intensity or 75 min of vigorous intensity activity/wk Children: at least 1 hr of moderate or vigorous- intensity activity/d, with vigorous activity on at least 3 d/wk Limit sedentary behavior such as sitting, lying down, watching TV, and other forms of screen- based entertainment Doing some physical activity above usual activities, no matter what one’s level of activity, can have many health benefits |
Family-based interventions Health communication and social marketing: campaigns that include mass media and health-related product distribution Community-wide campaigns Individually adapted health behavior change programs Social support interventions in community settings Enhanced school-based physical education Community-scale urban design and land use policies Built environments Creating or improving places for physical activity Point-of-decision prompts to encourage use of stairs |
||
|
| |||||||
| Fruit intake (≥2 cups/d) | 13.1 (2013) | California, 17.7 | Tennessee, 7.5 | Eat a healthy diet, with an emphasis on plant-based foods | |||
| Moore et al, MMWR 2015:64:709–25 | Eat at least 2½ cups of fruit and vegetables each day Limit how much red & processed meat you eat Choose whole grains instead of refined grain products |
||||||
|
| |||||||
| Vegetable intake (2.5–3 cups/d) | 8.9 (2013) | California, 13.0 | Mississippi, 5.5 | Eat a healthy diet, with an emphasis on plant-based foods | |||
| Moore et al, MMWR 2015:64:709–25 | Eat at least 2½ cups of fruit and vegetables each day Limit how much red & processed meat you eat Choose whole grains instead of refined grain products |
||||||
|
| |||||||
| ≥1 sunburn in previous year (high school students) | 55.8 (2015) | N/A | N/A | Avoid excessive UV exposure | Clinicians counsel children, adolescents, & young adults aged 10 to 24 who have fair skin about minimizing UV exposure | Education & policy approaches in primary & middle school settings and in outdoor recreational & occupational settings Multicomponent communitywide interventions |
|
|
| |||||||
| Use of indoor tanning bed (high school students) | 7.3 (2015) | N/A | N/A | Do not use tanning beds | Clinicians counsel children, adolescents, & young adults aged 10 to 24 who have fair skin about minimizing UV exposure | ||
|
| |||||||
| Screening for colon cancer | 66.4 (2014) | Massachusetts, 76.5 | Wyoming, 56.9 | Know your family history | Screening for colorectal cancer starting at age 50 & continuing until age 75 | Multicomponent interventions | Provider assessment & feedback |
| Mammography | 73.0 (2014) | Massachusetts, 88.0 | Idaho, 62.5 | Follow a cancer screening program | Biennial mammography for women ages 50 to 74 | Client reminders | Provider reminder & recall systems |
| Pap test | 82.6 (2014) | Massachusetts, 88.0 |
Idaho, 76.2 | Screening for cervical cancer in women ages 21 to 65 with Pap smear every 3 years or, for women ages 30 to 65 who want to lengthen the screening interval, screening with a combo of Pap smear & HPV testing every 5 years | Small media One-on-one education Group education (breast only) Reducing client out-of-pocket costs (breast only) Reducing structural barriers (breast & colon only) |
||
|
| |||||||
| HPV vaccination | Girls: 41.9 | Girls: Rhode Island, 68.0 | Girls: Mississippi, 24.4 | Use preventive medicines & vaccines | Vaccination at 11 or 12 years old, can begin as early as 9 years old | Home visits to increase vaccination rates | Health care system-based interventions implemented in combination |
| Reagan-Steiner et al, MMWR 2016;65:850–58 | Boys: 28.1 (2015) | Boys: Rhode Island, 58.1 | Boys: Tennessee, 16.0 | doses 6 mo apart for those aged <15 doses at 0,1–2 mo, 6 mo for those aged ≥15 |
Reducing client out-of-pocket costs Vaccination programs in schools & organized child care centers |
Immunization information systems Provider assessment & feedback |
|
| HBV vaccination Hill et al, MMWR 2015;64:889–96 | 72.4 (2014) | North Dakota, 88.4 | Vermont, 48.4 | Use preventive medicines & vaccines | Universal vaccination of infants; vaccination is recommended for all children & adolescents aged <19 Hepatitis B vaccination is recommended for all unvaccinated adults at risk for HBV infection & for all adults requesting protection from HBV infection Screen for HBV infection in persons at high risk for infection & at the first prenatal visit for pregnant women |
Vaccination programs in WIC settings Client or family incentive rewards Client reminder & recall systems Vaccination requirements for child care, school, & college attendance Community-based interventions implemented in combination |
Provider reminders Standing orders when used alone |
|
| |||||||
| Hepatitis C (reported cases of acute infection) | 0.7 per 100,000 | 0.1, Missouri, Nebraska & South Carolina | West Virginia, 3.4 | Use preventive medicines & vaccines | Screen for HCV infection in persons at elevated risk for infection & offer one-time screening to adults born 1945– 1965 | ||
NOTE. All data from the CDC’s 2015 National Health Interview Survey, Behavioral Risk Factor Surveillance System, Youth Risk Behavior Surveillance System, or their Division of Viral Hepatitis Statistics and Surveillance System, unless otherwise noted.
Abbreviations: ACIP, Advisory Committee on Immunization Practices; USPSTF, United States Preventive Services Task Force; UV, ultraviolet.
On the basis of established cancer prevention recommendations from the American Cancer Society and the American Institute for Cancer Research/World Cancer Research Fund.
Actions taken from the Guide to Community Preventive Services (the Community Guide) https://www.thecommunityguide.org/. Modified from refs. 2, 4.
To capture the status and opportunities related to primary prevention, five areas are analyzed in the information to follow.
Tobacco.
Use of conventional tobacco products remains the leading cause of preventable cancer mortality, accounting for nearly one-third of all cancer-related deaths (116). Tobacco use is associated with a variety of chronic diseases as well as with cancer development in as many as 18 different organ sites (115). Global estimates of tobacco use have identified 1.25 billion active smokers, with numbers still rising in Asia.
Despite these statistics, much progress has been made over the last 50 years. Strategies for reducing overall tobacco use have included evidence-based public policies, such as taxation, clean air laws, advertising and marketing restrictions, and health warnings on packaging, as well as public awareness and education campaigns, and community-based cessation services that offer important approaches to tobacco control. In the United States, these efforts have resulted in a reduction in tobacco use (115), correlating with a reduction in lung cancer incidence and mortality (117). A 62% reduction in lung cancer mortality is associated with smoking cessation by age 50 (118).
Although these statistics are encouraging, cigarette smoking remains the leading cause of cancer-related deaths in the United States (119) and reductions in tobacco use have not been evenly distributed across populations. Higher rates of tobacco use characterize certain racial/ethnic subgroups, lower socioeconomic status groups, rural populations, and individuals with comorbid mental illness (115). Such trends highlight the need for continued prioritization of tobacco control efforts in at-risk populations.
Obesity, energy imbalance, and physical inactivity.
Recent figures are striking, with 120 million obese children and adolescents and 640 million adults estimated worldwide. Approximately 20% to 33% of cancer-related deaths in Western populations are attributed to obesity, poor diet, or sedentary lifestyles (120). An absence of excess body fat lowers the risk of cancer at 13 organ sites (121). Recommendations are to be as lean as possible, without becoming underweight (122). Nonetheless, if current trends in reducing tobacco use continue, energy imbalance and obesity will soon become the dominant, modifiable cancer risk factor in the United States, as roughly two-thirds of adults (120) and 32% of youth in the United States are overweight or obese (123). More than half of adults (124) and 30% of children ages 6 to 11 do not participate in the recommended levels of physical activity (125). Because increased physical activity can reduce the risk of cancer (126), the U.S. Surgeon General has called for action involving evidence-based strategies for increasing individual physical activity. Current recommendations suggest 30 minutes of moderate-intensity physical activity at least five days per week, 20 minutes of vigorous-intensity activity at least three days per week, or some combination of the two (127). NCI scientists found that leisure-time physical activity was associated with lower risks of 13 cancer types (esophageal adenocarcinoma, liver, lung, kidney, gastric cardia, endometrial, myeloid leukemia, myeloma, colon, head and neck, rectal, bladder, and breast). Most of these associations were evident regardless of body mass index or smoking history. These findings confirm and extend the evidence for a benefit of physical activity on cancer risk and support its role as a key component of population-wide cancer prevention. An NCI-funded international study demonstrated that people exposed to activity-supportive neighborhoods were far more likely to participate in physical activity than people exposed to less supportive neighborhoods, and estimated that two million lives could be saved annually worldwide with a focus on building environments designed for people to move. This is a challenge, because most cities are designed for cars, not for people to move. Globally, this work has contributed to initiatives by the WHO and others to guide policies promoting active environments. Nationally, this work was cited as part of the CDC’s guide to community preventive services endorsement of built environment strategies for promoting health (128).
Dietary changes may also reduce cancer risk. Seventy-six percent of adults in the United States do not meet government recommendations for daily fruit intake, and 87% do not meet vegetable intake recommendations (129), behaviors that are particularly disproportionate in racial and ethnic minorities and low socioeconomic status groups.
Evidence-based recommendations indicate that optimal energy balance requires (i) limited portion sizes, (ii) consumption of a variety of fruits, vegetables, beans, and whole grains, (iii) limited consumption of energy-dense foods as well as red and processed meats, (iv) avoidance of sugary drinks, (v) and limited consumption of alcoholic beverages (120, 130).
Ultraviolet radiation exposure.
Excessive ultraviolet (UV) light from both the sun and artificial devices, such as tanning beds, is believed to contribute to the approximately 5 million cases of skin cancer reported annually in the United States (131). Personal actions to reduce skin cancer risks include limiting sun exposure, using sunscreen, wearing protective clothing and hats, and avoiding exposure to artificial tanning devices.
Population-wide actions, such as public policies that restrict or ban indoor tanning and public educational campaigns, can reduce skin cancer occurrence (131). To date, 13 U.S. states, in addition to Washington, D.C., have enacted legislation that restricts minors’ access to tanning beds. Additional states are considering similar action. Australia represents an outstanding example of population-based skin cancer control that has reduced melanoma incidence (132, 133).
Cancer-associated microbial infections.
Pathogenic infections contribute to an estimated 16% of cancers worldwide, with more than 90% of these cancers being associated with four pathogens:
- Helicobacter pylori (H. pylori)
- Associated with gastric cancer and mucosa-associated lymphoid tissue.
- Effectively treated with a short-course combination of antibiotics and proton-pump inhibitors.
- Hepatitis B virus (HBV)
- Contributes to cirrhosis and liver cancers.
- Effective vaccines developed for HBV-associated proteins have reduced hepatocellular carcinoma incidence (134).
- Hepatitis C virus (HCV)
- Contributes to cirrhosis and liver cancers.
- May be detected by blood-based screening (as recommended by the CDC for those born between 1946 and 1964) and treated with a combination of effective although expensive antiviral agents.
- Human papillomavirus (HPV)
- Associated with cancers of the anus, cervix, oropharynx, penis, vagina, and vulva.
- There are 3 HPV vaccines for the prevention of HPV-related cancers including Cervarix (types 16, 18), Gardasil (types 6, 11, 16, 18), and Gardasil 9 (types 6, 11, 16, 18, 31, 33, 45, 52, 58).
Unfortunately, despite the availability of effective preventive interventions for the previously listed pathogenic infections, limitations remain. High infection rates continue to persist in racial and ethnic minorities as well as in low socioeconomic status groups. In addition, HCV infections are often left undiagnosed and untreated, despite effective agents (135, 136). Overall, HPV vaccine uptake has been low, and HBV vaccination is variable in the United States and abroad. Thus, missed opportunities for cancer prevention persist (137, 138).
Environmental risk factors.
Causality has been shown between various cancers and the following environmental factors:
Bladder cancer: Consumption of water contaminated with arsenic.
Liver cancer: Aflatoxin exposure.
Lung cancer: Radon gas exposure.
Mesothelioma: Asbestos exposure.
Respiratory cancers: Exposure to outdoor air pollution due to motor vehicles, industrial processes, power generation, or indoor air pollution due to the burning of solid fuels for heating or cooking.
There is a dearth of research regarding other environmental risk factors and their links to cancer development and progression (139). This is a growing area of AACR interest, with future initiatives currently under development with environmental and occupational health experts.
Summary.
Primary prevention shows that personal and population-level actions to limit exposure to or influence of carcinogenic lifestyles and environmental factors can reduce associated cancers. There is no more dramatic or convincing example of this than efforts in tobacco control in the United States over the last 50 years that have reduced lung cancer rates first among men and more recently in women (115). However, change depends on implementing sustained, evidence-based personal actions to promote healthy lifestyle options, as well as population-based actions in public policy, public and professional education, and community-based service delivery, particularly among groups and regions with the greatest burden. The six Institute of Medicine measures of quality programs apply to such population-based initiatives. That is, such interventions are optimally: safe, timely, effective, efficient, equitably distributed, patient-/population-centered, and sustainable (STEEEPS). Any interventions must be effectively disseminated to those living in low-resource settings and to those who are geographically, linguistically, culturally, or socially isolated. As former NCI Director Sam Broder once remarked, “Poverty is a carcinogen.” (140).
Secondary prevention
Secondary prevention refers to efforts taken to limit the progression or impact of a disease process that has already begun. Most often, this occurs through the application of risk-directed assessments followed by preventive interventions that can mitigate risks or interrupt progression. Such interventions include screening and the use of surgical interventions and/or molecular preventive agents designed to interrupt an established disease process (Fig. 3).
Risk evaluation and screening.
Secondary prevention is most often oriented toward the identification of higher-than-average-risk individuals from the general population via screens in asymptomatic populations for the presence of subclinical precancer or cancer. These cancer-related markers may include:
Aberrant radiographic images (e.g., masses or ground-glass opacities in spiral CT scans of the lungs; breast masses or calcifications in mammograms).
Cancer-related infections (e.g., HPV DNA in secretions or cellular collections; hepatitis B proteins or hepatitis C antibodies in the blood).
Cellular/protein aberrations [e.g., abnormal concentrations of CA125, carcinoembryonic antigen (CEA) prostate-specific antigen (PSA), etc.].
Molecular changes or hemoglobin in stool.
Visual identification of precancers, for example, visual inspection with acetic acid to detect abnormal cells of the cervix; optical imaging of oral dysplasia (141); and histopathologic examination of atypical cells in cytologic scrapings of the cervix or dysplasia in biopsies of skin, mouth, cervix, breast, prostate.
Screening and early detection techniques possess clinical efficacy as they allow for early identification of neoplastic processes, earlier and more precise treatment interventions, and improved outcomes. The National Lung Screening Trial, a randomized controlled trial (RCT) of >53,000 current and former heavy smokers ages 55 to 74, compared the effects of two screening procedures for lung cancer, low-dose helical CT and standard chest X-ray, on lung cancer mortality and found 20% fewer lung cancer–related deaths among trial participants screened with low-dose helical CT (142). A bronchial genomic classifier improved the sensitivity of bronchoscopy for lung cancer detection (143). Screening and early detection also come with potential risks, however, including anxiety, invasive testing, and the possibility of false-positive or false-negative results. Tests with low sensitivity and specificity may lead to additional diagnostic testing, which may be more invasive, expensive, and associated with intrinsic harms including infection, bleeding, or organ perforation. Conversely, some screening tests are associated with overdiagnosis, defined as the detection of lesions that would not have become clinically evident in the patient’s lifespan had it not been for the screening test, which may result in unnecessary morbidity from treatment. Therefore, there is a need for the development of refined and validated risk models across all cancers. We are also beginning to see the application of artificial intelligence and machine learning algorithms to radiology, which has the potential to reduce both false negatives (especially minute early lesions that could be missed by the human eye) and false positives, to facilitate precancer and early cancer diagnosis on imaging (144).
Genomic technologies support detection strategies with greater sensitivity as well as improved risk stratification of lesions and patients. The development of a clinically acceptable diagnostic test for cancer screening, early detection, and diagnosis is challenging and expensive, however, requiring extensive testing to define sampling strategies, target population identification, and clinical use context. Returns on investment arising from successful screening or diagnostic tests have been limited, thus diminishing the private sector’s interest in developing such technologies.
Population-based cancer screening requires that:
The test be acceptable to patients and providers;
The test accurately identifies asymptomatic precancer or cancer, which disregarding normal conditions; and
The process of receiving a positive test result and undergoing a subsequent diagnostic evaluation and intervention decreases a person’s chance of dying from that cancer.
Thus, cancer screening is part of a larger continuum of care to ensure that diagnostic tests, which may identify a precancer or cancer for which there is no effective treatment, are not rendered useless and potentially harmful. Evidence of benefit is important when asking large numbers of asymptomatic people to undergo a screening test. The risk of applying a screening test followed by potential surgical or medical interventions to mitigate identified risks in asymptomatic individuals must be weighed against the risk of developing a symptomatic and typically later-stage cancer. Currently, the United States Preventive Services Task Force (USPSTF) recommends screening for breast, cervical, colon, and lung cancers based on age (and smoking history, in the case of lung cancer screening). Unfortunately, the number of screening strategies available and universally agreed upon remains relatively small. Interpretations of some tests, such as PSA screenings for prostate cancer (145), are changing as more long-term outcome data emerge, highlighting the need to develop more sensitive screening tests.
Cancer interception.
Preventive interventions following identification of an individual at high risk of developing cancer may involve surgical removal of precancers or entire organs or administration of “interceptive” agents intended to reduce or eliminate existing precancers or prevent their progression to invasive disease (3). Cancer chemopreventive agents applied to prevent progression of precancers in a secondary preventive context are referred to as “cancer-interceptive” agents. Such interventions may reduce the risk of cancer incidence, the development of advanced stage cancers, and cancer mortality, but may also be expensive, present with toxicities, require invasive diagnostic testing, and result in overdiagnosis and overtreatment of preneoplastic lesions. HPV vaccine is a great example of successful cancer immune interception.
Some of the greatest progress in cancer prevention has resulted from effective cancer screening tests followed by surgical preventive interventions. Evidence-based cancer screening tests have been established for the identification of precancers and cancers in at least four organs including the cervix, breast, colon, and lung. In most cases, clinical recommendations are based on long-term outcomes from RCTs involving the sequence of a screening test, diagnostic confirmation, and subsequent surgical interventions in “screen-positive” individuals. Follow-up studies gather data on cancer-related mortality endpoints as well as data on unintended morbidities of the screening test, the diagnostic test, and subsequent surgical interventions. Some tests, such as the Pap test for cervical cancer, have achieved their “recommended” status based on results found in comparison with nonscreened populations in population-based observational studies of reduced cancer incidence and mortality.
Existing controversies in cancer screening.
Despite cancer screening efficacy, debate persists on the usefulness of some screens. PSA screening for prostate cancer, especially when followed by diagnostic biopsy and surgical prostatectomy, can lead to posttreatment anxiety, urinary incontinence, and sexual dysfunction. An additional harm is the detection of prostate cancers that would have never caused symptoms or come to medical attention during the patient’s natural lifespan had the cancer not been detected by screening. Such situations are referred to as overdiagnosis. Thus, PSA screening is recommended by some healthcare professionals but discouraged by others due to differing perspectives regarding clinical risks and benefits, as well as divergent interpretations of available data. The consideration of PSA screening followed by diagnostic confirmation and deferred intervention, commonly described as “watchful waiting,” in “screen positives” with precancerous lesions and/or early-stage cancer provides an increasingly attractive option (145).
Despite controversies, there are proven examples of effective cancer screening techniques. Colorectal cancer screening followed by surgical interception, most often, endoscopic polypectomy, is associated with a substantial reduction in colorectal cancer–associated mortality (146). Cervical cancer screening followed by surgical interception by excisional biopsy, conization, or loop electrosurgical excision procedure, results in a 70% to 80% cervical cancer–related mortality reduction (147). Mammographic screening followed by lumpectomy also results in reduced breast cancer mortality (148). Lung cancer screening with low-dose CT has reduced mortality by 20% (149) in current or previous (within 15 years) smokers with a 30-pack-year history (a “pack-year” is smoking an average of 1 pack of cigarettes per day for 1 year) who underwent invasive biopsy and surgical resection.
Cancer chemoprevention.
In 1976, Sporn originally described cancer chemoprevention as the application of drugs or natural compounds to reverse, block, or prevent the development of cancer, with efficacy assessments most often based on changes in the number, size, or histopathologic grade of precursor lesions (150). Definitive RCTs have been largely negative (and some even harmful; refs. 151, 152), including a very recent RCT of a high-vegetable diet to prevent progression in patients with prostate cancer on active surveillance and even “positive” RCTs meeting their primary efficacy endpoint have complex secondary endpoint/disease trade-offs, challenging clinical translation. For example, results of the Prostate Cancer Prevention Trial, testing the effectiveness of finasteride to prevent the disease, had met its primary endpoint of 25% fewer prostate cancer diagnoses than men on the placebo. There was a cautionary note, however, that men who developed prostate cancer on the finasteride arm were more likely to have high-grade lethal tumors (153). However, despite the higher rate of high-grade disease, recent long-term (18-year) follow-up, found no significant survival differences (154). Long-term RCT results showed that raloxifene, a common osteoporosis drug, prevented breast cancer to the same degree, but with fewer serious side-effects than tamoxifen, which is FDA approved in this setting. Raloxifene retained 76% of tamoxifen’s efficacy in preventing invasive disease and incidence curves approached that of tamoxifen in preventing noninvasive disease—all with significantly less endometrial cancer with raloxifene use (155, 156). There have been a number of FDA-approved agents carrying labeled indications to treat precancerous lesions or reduce cancer risks (Table 2). Chemopreventive agents have been considered for applications in a primary context to reduce the biologic impact of carcinogens or cancer-associated pathogens in the general population and in a secondary context to treat precancers and mitigate cancer risks in high-risk populations. Potential uses are being refined with more specific terminology. For example, immune prevention efforts, such as the administration of vaccines directed against HPV or hepatitis B are most effective applied in unexposed children and young people, as they are directed at preventing the initial infection. The use of ledipasvir/sofosbuvir to treat hepatitis C (136), and therefore prevent the development of liver cancer, represents chemoprevention applied in a secondary preventive setting, as ledipasvir/sofosbuvir does not prevent the initial infection, but rather intercepts and prevents further carcinogenic progression. The use of preventive agents in high-risk cohorts and in other secondary preventive contexts to intercept the carcinogenic progression of established precancers (3) underscores a trend toward more precise molecular targeting and greater personalization of cancer interventions. Changes to an airway genomic signature associated with PI3K activity were associated with a preventive agent response in smokers with bronchial dysplasia (157). In lung cancer, upregulation of the PI3K (phosphoinositide 3-kinase) pathway is an early event that contributes to cell proliferation, survival, and tissue invasion, and upregulation of this pathway was associated with enrichment of the lower airways with bacteria (158).
Table 2.
Approved agents for the treatment of precancerous lesions or cancer risk reduction
| Agent | Targeted cohort | indication |
|---|---|---|
|
| ||
| Tamoxifen | • Women with DCIS following breast surgery and radiation • Women at high risk for breast cancer (“high risk” defined as women at least 35 years of age with a 5-year predicted risk of breast cancer >/= 1.67%, as calculated by the Gail Model) |
Reduce the risk of invasive breast cancer Reduce the incidence of breast cancer |
|
| ||
| Raloxifene | • Postmenopausal women at high risk for invasive breast cancer (“high risk” defined as at least one breast biopsy showing lobular CIS or atypical hyperplasia, one or more first-degree relatives with breast cancer, or a 5-year predicted risk of breast cancer >/= 1.66% (based on the modified Gail model). | Reduction in risk of invasive breast cancer (Note: Raloxifene does not eliminate the risk of breast cancer. Patients should have breast exams and mammograms before starting raloxifene and should continue regular breast exams and mammograms in keeping with good medical practice after beginning treatment with raloxifene) |
|
| ||
| Cervarix | • Females 9 through 25 years of age | The prevention of the following diseases caused by oncogenic HPV types 16 and 18: • Cervical cancer • CIN grade 2 or worse and adenocarcinoma in situ • CIN grade 1 |
|
| ||
| Gardasil 9 | Girls and women 9 through 26 years of age | The prevention of the following diseases caused by HPV types included in the vaccine: • Cervical, vulvar, vaginal, and anal cancer caused by HPV types 16, 18, 31, 33, 45, 52, and 58 And the following precancerous or dysplastic lesions caused by HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58: • CIN grade 2/3 and cervical AIS • CIN grade 1 • VIN grade 2 and grade 3 • VaIN grade 2 and grade 3 • AIN grades 1, 2, and 3 |
| Boys and men 9 through 26 years of age | The prevention of the following diseases caused by HPV types included in the vaccine: • Anal cancer caused by HPV types 16,18, 31, 33, 45, 52, and 58 And the following precancerous or dysplastic lesions caused by HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58: • AIN grades 1, 2, and 3 |
|
|
| ||
| PDT with Photofrin | Males and females with high-grade dysplasia in BE | Ablation of HGD in patients with BE who do not undergo esophagectomy |
|
| ||
| Celecoxiba | Males and females >18 years old with FAP | Reduction in the number of adenomatous colorectal polyps in FAP, as an adjunct of usual care (e.g., endoscopic surveillance, surgery) |
|
| ||
| BCG | Males and females with CIS of the urinary bladder | Intravesical use in the treatment and prophylaxis of CIS of the urinary bladder and for the prophylaxis of primary or recurrent stage Ta and/or T1 papillary tumors following TUR |
|
| ||
| Valrubicin | Males and females with BCG-refractory CIS | Intravesical therapy of BCG-refractory CIS of the urinary bladder in patients for whom immediate cystectomy would be associated with unacceptable morbidity or mortality. |
|
| ||
| Fluorouracil | Males and females with multiple actinic or solar keratosis | Topical treatment of multiple actinic or solar keratosis |
|
| ||
| Diclofenac sodium | Males and females with actinic keratosis | Topical treatment of actinic keratosis |
|
| ||
| PDT with 5- aminolevulinic acid | Males and females with actinic keratosis of the face or scalp | Topical treatment of minimally to moderately thick actinic keratosis of the face or scalp |
|
| ||
| Masoprocolb | Males and females with actinic (solar) keratosis | Topical treatment of actinic keratosis |
|
| ||
| Imiquimod | Immunocompetent adults | Topical treatment of clinically typical, nonhyperkeratotic, nonhypertrophic, actinic keratosis on the face or scalp |
|
| ||
| Ingenol mebutate | Males and females with actinic keratosis on the face, scalp, trunk and extremities | Topical treatment of actinic keratosis |
Abbreviations: AIN, anal intraepithelial neoplasia; AIS, adenocarcinoma in situ; BE, Barrett’s esophagus; BCG, Bacillus-Calmette-Guerin; CIN, cervical intraepithelial neoplasia; CIS, carcinoma in situ; DCIS, ductal carcinoma in situ; FAP, familial adenomatous polyposis; HGD, high-grade dysplasia; HPV, human papillomavirus; PDT, photodynamic therapy; VaIN, vaginal intraepithelial neoplasia; TUR, transurethral resection; VIN, vulvar intraepithelial neoplasia.
FDA labeling voluntarily withdrawn by Pfizer, February 2011.
Withdrawn from U.S. market, June 1996..
Cancer-interceptive agents under consideration include food-based chemopreventives (e.g., green tea, curcumin, broccoli, sprouts) as well as drugs with better defined molecular targets (e.g., tamoxifen, raloxifene, aspirin, NSAIDs). Experiences with 5-fluorouracil, eflornithine, and EGFR inhibitors suggest that interventions currently known as chemotherapeutics may prove efficacious in a preventive context (159–163). Systematic evaluation of such opportunities will continue as newer, more targeted cancer therapies arise. Such work may be advanced through enrollment of study subjects with the potential of lifelong follow-up and greater use of electronic health records with standardized surveillance guidelines and recording of secondary precancers and cancers. Recent precision prevention is illustrated by RCT results of targeting the FXR–FGF axis, which will likely lead to the first preventive agent to reverse the HCC precursor NASH (164).
Chemoprevention combinations.
One promising area in cancer prevention is the potential of agent combinations for high-risk patient populations. For example, the combination of sulindac and eflornithine in patients with colorectal adenomas resulted in a 70% reduction in recurrent adenomas and a 90% reduction in advanced and multiple adenomas over a 3-year interval (159). See above for FAP combination trials. Experimental chemoprevention combinations involving metformin have shown promise based on preclinical and epidemiologic data. Experimental clinical studies are ongoing to evaluate whether insulin-lowering effects are key to metformin’s efficacy or related drugs also have direct anticancer effects on mTOR or YAP signaling (165, 166).
Tertiary prevention
Tertiary prevention focuses on alleviating disability resulting from a cancer diagnosis and its treatment by taking measures to improve the overall quality of life and long-term outcomes of patients with cancer, following treatment (Fig. 3). Typically, such efforts involve individuals at higher-than-average risk due to the baseline risks that led to their primary cancers, as well as additional risks for treatment-related toxicities and treatment-related cancer incidence. Preventive work at this level is referred to as “survivorship” in the continuum of cancer care.
Survivorship includes assessments and interventions to reduce the risk of recurrence, reduce occurrence of new primary cancers, maximize quality of life, and assist in psychosocial adjustment following cancer treatment. As part of this, it is vital to provide accurate and reliable information on health behaviors with appropriate timing and in a manner that survivors can understand and apply. Included among evidence-based interventions with impact and importance to survivors are:
Tobacco reduction programs that can improve treatment efficacy, overall health, and outcomes (167).
Dietary programs prioritizing energy balance, obesity prevention, and provocative circadian fasting schedules (171, 172).
Outpatient rehabilitation programs to assist patients with returning to optimal levels of functioning (173).
Programs tailored to the needs and challenges of various cancer health disparities (174).
State of cancer prevention science: summary.
The process through which evidence is developed for a novel preventive device or intervention technique of relevance to large populations is now clear, and is a growing priority for federal and private funding agencies.
The design and application of optimal preventive interventions will benefit from assessing precancers from a multidisciplinary perspective to better characterize the hallmarks of premalignant disease, permitting the implementation of cancer interception techniques to reverse or prevent aberrations in as many cancer hallmarks as possible.
Mechanistic links between dominant cancer risk factors and molecular aberrations capable of contributing to cancer are variably established.
Developing, refining, and validating cancer risk models.
Lifestyle and environmental exposures contribute to the bulk of cancer incidence and deaths worldwide. However, many of these factors are modifiable through actions that can reduce risks to noncritical levels at the individual and/or population levels, including tobacco control, weight management and physical activity, avoidance of UV radiation, prevention and treatment of cancer-associated microbial infections, and protection from known environmental carcinogens such as asbestos, radon gas, and the burning of solid fuels.
Implementation and dissemination of effective prevention strategies is critical to reducing the cancer burden. Individuals living in low-resource settings and in other underserved population segments require added attention.
The six Institute of Medicine measures of quality care apply to prevention and population-based initiatives as well as to clinical therapeutics: safe, timely, effective, efficient, equitable, and patient-centered/culturally tailored. Sustainability over time is an additional parameter important to prevention measures.
Cancer screening has been shown to be effective in reducing cancer mortality for some common cancers. Mammographic screening reduces breast cancer mortality, colon screening reduces colon cancer mortality, cervical screening reduces cervical cancer mortality by 70% to 80%, and low-dose CT lung screening reduces lung cancer mortality by 20%.
Emerging genomic technologies are allowing for improved detection strategies as well as improved stratification of precancerous lesions and high-risk patient populations.
“Cancer interception” is defined as the administration of preventive treatment modalities in high-risk cohorts to interrupt the carcinogenic process and supports progress toward the development of precision targeted and immune cancer prevention interventions.
Evidence-based cancer prevention interventions with impact and importance to survivors include tobacco treatment programs, energetics and exercise interventions, dietary programs that prioritize energy balance, outpatient rehabilitation, and attention to cancer health disparities.
Current Limitations and Obstacles in Cancer Prevention
Development of prevention as a dominant strategy to reduce the burden of cancer faces barriers. Even though research supports the use of evidence-based prevention strategies (4, 175), implementation varies around the globe as well as within the United States.
Conceptual challenges
The simple term cancer prevention belies its complexity. Prevention describes many different goals, interventions, and participants, causing confusion in communications within and beyond the field. Definitions and standards for classification of prevention strategies and tactics lack consistency and clarity. For example, the term chemoprevention can be applied in several different contexts. Chemoprevention is often intended as a primary preventive strategy to reduce the impact of carcinogens. However, it may also refer to a secondary goal of eliminating or reducing the number, size, or distribution of precancerous lesions. Introduction of the term interception relating to the latter application may help distinguish secondary from primary preventive applications. The clarity is welcomed by the field, especially by researchers and those in industry pursuing preventive drug development (176). Terminology can also obscure health disparities that are cancer risk factors. Among these are age, gender, race, population density (i.e., urban, suburban, rural, frontier), geography, socioeconomic status, insurance status, access to screening or care, language/acculturation, etc.
With a progressive disease comes the challenge of defining the moment when the disease is worthy of identification and intervention. A focus on disease process rather than endpoint requires identifying a disease stage that is early enough for the patient to benefit from early detection and prevention. The disease stage must be modifiable and interventions must be clinically effective. Technological advances are driving earlier identification of stages in the carcinogenic process, and the “development-to-application” cycle time is growing shorter. Cancer prevention must move beyond the description of molecular aberrations in the form of cellular atypia, histopathologic dysplasia, or even cancer, to accurate forecasting of the prognosis for a preneoplastic lesion, the status of the organ in which it resided, and competing causes of morbidity and mortality. Unfortunately, such prognoses are difficult, especially at the earlier stages of neoplasia, which may arise and regress in an unpredictable, multidirectional manner.
Clinical application of prevention techniques can be varied and inconsistent. Select examples or extreme cases may be used to argue a course of action, without attention to the range of variation. With experience, caregivers gain understanding of all available screening and treatment options. Fundamentally, patients must be evaluated over time to determine their personal preferences and to gain a better understanding of the risks and benefits associated with any cancer intervention.
Procedural challenges
Cancer prevention efforts can suffer from misplaced or limited focus, lack of engagement, ineffective communication, limited investment, critical variations, systemic fragmentation, and insufficiencies. Molecular biologists’ lack of sufficient engagement in cancer prevention research has contributed to a paucity of data regarding the key molecular derangements underlying the biology of early neoplasia, as well as the sequence, timing, and reversibility of these changes. There has been no systemic characterization of molecular aberrations in early neoplasia, like what has occurred in advanced cancers via The Cancer Genome Atlas (TCGA). Although some insight into the biology of precancers has been gained, too often the focus is on data collection rather than translational applications of those data. An area needing attention is identification of molecular drivers of premalignancy (177).
Cancer prevention research and development has not garnered much interest from the pharmaceutical industry, possibly due to the temporal and fiscal challenges inherent in preventive device and drug development (178). Most progress has resulted from public funding, which is limited due to competing priorities in basic cancer science and treatment. As a result, few well-funded investigators are vested in prevention and screening research. However, a recent article (176) clarifies the pharmaceutical industry’s perspective on the field and its potential. This article highlights the three major concerns within the field listed in the information to follow. Because of these challenges, most pivotal cancer prevention trials must rely on clinical outcomes and take an extremely long time to complete, dissuading private investment.
Lack of validated preventive targets.
Insufficient diagnostics associated with identifying those at-risk populations most likely to respond to molecular preventive interventions.
Lack of sufficiently validated surrogate endpoints to define at-risk populations, prioritize key mechanisms, and accelerate developmental timelines.
Private investment in prevention needs efficient validation and approval processes for molecularly based clinical assays and accurate, reliable and predictive intermediate markers of efficacy. Additional concerns include regulatory agencies’ reluctance to approve drugs based on surrogate efficacy endpoints and the notion that preventive agents lack profitability. Drugs for long-term, systemic use with their attendant need for few side effects may be unnecessary, as short-term, intermittent, localized, and/or low-dose therapies are now possible. Hait and Lebowitz cite examples wherein some of these challenges have been overcome and call for a greater sense of urgency to address these challenges, accelerate progress, and attract greater public and industry investment. A major recent step in this context was launched this year – a five-year translational research alliance with Boston University and Johnson & Johnson Innovation LLC (JJI) aimed at intercepting lung cancer, the leading cause of cancer deaths worldwide. The first project involves a translational research consortium that was established by the U.S. Department of Defense seven years ago and is now co-funded by the NCI and Janssen. The alliance will develop a precancer genome atlas (PCA) in collaboration with a Stand Up To Cancer multidisciplinary lung cancer interception dream team last year. This can serve as a model how research university can collaborate with a large corporate partner. This new alliance with JJI, and its focus on intercepting lung cancer, comes at a time when cancer researchers and physicians are expressing renewed optimism over recent breakthroughs and new technologies that are enabling translation to cancer interception.
Interdisciplinary communication can be challenging and ineffective. Care of patients at risk for cancer often involves a wide array of clinical practitioners including primary care providers (e.g., nurse practitioners, physician assistants, general internists, family medicine physicians), screening or diagnostic specialists (e.g., gastroenterologists, radiologists, pathologists), and intervention specialists (e.g., surgeons, oncologists, infectious disease physicians). Success of preventive clinical care depends on timely and accurate communication among these providers regarding risk evaluations, interventions, and outcomes.
In stage T2-T4 research, data systems are often insufficient to measure status and progress at the level and frequency needed to assess foundational needs, guide strategy, or evaluate outcomes following interventions. Many commercial electronic health records are incapable of providing the necessary data for T2-T4 research or monitoring clinical service delivery or outcomes. Relevant outcomes from cancer screening or early detection are often invisible to the diverse array of investigators, clinicians, and public health planners involved in caring for at-risk populations. For example, most state-based cancer registries do not require reporting of precancers, a practice based on outdated data whereby precancers were considered biologically independent of invasive cancers (e.g., “benign” vs. “malignant” tumors) and irrelevant to subsequent cancer risk. Collectively, these efforts require further engagement of statisticians and quantitative scientists.
Fragmented health care delivery and population health systems are unable to provide comprehensive prevention and screening services in a manner consistent with recommended, evidence-based guidelines. Prevention and screening services are insufficiently reimbursed and prioritized, despite improvements following implementation of the Affordable Care Act. Screening adherence across cancer sites continues to be a challenge as well. For example, of women eligible for breast, cervical, and colon cancer screening, only 8% to 43% underwent screening for all three cancers (179). In some cases, especially for colorectal cancer screening, this lack of screening may be attributed to insufficient clinical capacity. More than 24 million American adults will require colorectal cancer screening to reach the aspirational goal of 80% population screening coverage by 2018. The provision of effective tobacco cessation services beyond state-funded tobacco quitlines is similarly challenging. Thus, fragmentation as well as variation in availability, quality, and costs ofclinical preventive services prevents comprehensive implementation of healthy life-style interventions (180).
Cancer biology challenges
For decades, research into the biology of early neoplastic development has generated insights through use of in vitro mechanistic studies, in vivo models, and various clinical studies of precancerous lesions. Despite great progress, additional focus and effort is needed.
Progressive mutations in genes regulating cellular identity, fate, growth control, and genomic integrity, can drive transformation from healthy colorectal mucosa to adenoma and then to colorectal cancer (181). The model has far too often been discussed as a linear evolutionary progression, however, which can lead to an inaccurate impression given the importance of the dynamic and varied nature of precancerous lesions (182). Data suggest a much more complex biology with substantial tumor heterogeneity in precancers (183, 184) creating genetically distinct and competing subclones, which may either regress, remain dormant, or progress to invasive cancer (see detailed discussion above). The substantial tumor heterogeneity between and within such precancer lesions and between and within individuals is (185) not well investigated or established in precancers (186). Given the range of molecular aberrations in precancers that have been identified thus far, such lesions are expected to harbor less heterogeneity than more advanced lesions, which could translate into greater responsiveness to targeted or immune-based interception agents. In addition to the heterogeneity found within organs or between individuals, there are added layers of complexity between target organs, within different organ-based signaling pathways, and with molecular abnormalities capable of demonstrating opposite effects in different organs (187).
Hanahan and Weinberg’s model of six to eight key functional derangements with two enabling characteristics and the related groups of genes and pathways regulating cancer development and progression have complemented earlier insights by providing a functional lexicon of aberrations important in the process (188, 189). The order, timing, and prevalence of these “hallmark” insults during the earliest stages of neoplastic development are under active study. Provocative genetic, epigenetic, and immunologic precancer data have the potential to be translated into molecular targets for cancer interception. Emerging over the last couple years, the vast scope, complexity, and impact of early mutational drivers and pathways, germline-somatic interactions, stem cell and immune signals in premalignant progression and early detection research, are briefly highlighted as follows:
PDAC development: Kras mutation diverges with p16 or p53 inactivation to PanINs; and GNAS mutation to IPMN pathway (26).
PanIN pathway: early Kras mutation and inflammation drive IL17 signaling to induce stemness and progression to PDAC (190); highlighting the potential of repurposing IL17 inhibitors.
Colorectal adenoma–carcinoma sequence: APC inactivation or loss drives chromosome instability pathway (in FAP and sporadic); while MMR defect (in Lynch syndrome and sporadic MLH1 methylation) induces a highly immunogenic “frameshift” mutations in APC and other genes.
Early ontogeny of BRCA-1 related breast cancer discovered hormone-responsive progenitors supports repurposing an FDA-approved RANK-pathway inhibitor
Breast cancer in BRCA1 carriers: normal stem cells that acquire PTEN mutation driving basal pathway; while p53 mutation drives luminal pathway results; in both pathways, BRCA1 loss is a late event (191).
MPN comprehensive molecular subclassification: JAK2–TET2 mutation order profoundly affects stem/progenitor cell biology, age and drug sensitivity (192, 193).
Inherited variation and somatic mutation of JAK2, SH2B3, TET2, and CHEK2 contribute to V617F age-related clonal hematopoiesis and/or MPN development (81).
Acquired ASXL1 mutations are common in patients with inherited GATA2 mutations and correlate with myeloid transformation to MDS/AML.
Germline RUNX1 mutation carriers develop detectable clonal hematopoiesis with a cumulative risk of >80% by age 50 years.
Genome-wide computational studies shape where, when, and how tumors develop and inherited variation and antigen presentation pathways (64, 65).
A breakthrough early detection research report established plasma cell-free DNA methylation patterns that implicate the site of tumor development (194).
Targeted single-cell sequencing can elucidate the order of mutation acquisition in T-ALL multipotent progenitor cells (195). Potentially divergent BRAF or KRAS pathways and immune dysregulation in the pathogenesis of atypical adenomatous hyperplasia and progression to lung adenocarcinoma (196). Drivers of squamous precancers are also being uncovered in actinic keratosis. A landmark RNA-seq study of lung dysplasia identified distinct molecular subgroups, including downregulation of IFNγ signaling, M1 macrophage polarity and T-cell–mediated immunity associated with high-grade lesion progression (197). The immune subtype identified in oral precancer showed that a macrophage signature predicted oral cancer free survival. Comprehensive study of proteomic alterations in airway epithelium uncovered dramatic metabolic reprogramming happening early in the pathogenesis of this lethal disease (198). Provocative new data discovered NOTCH1 mutations as early events in lung premalignancy and aging normal esophagus; Notch is also involved in tumor morphogenesis and patterning of the TME (199). NOTCH1 mutations were remarkably found at high prevalence in aging normal esophagus (200, 201), analogous to incidental findings of age-related, AML-cancer-associated driver mutations in asymptomatic clonal hematopoiesis, which although incidental findings, are clearly clinically relevant since they harbor much higher transformation rates to AML (ultrasensitive NGS has remarkably found tiny clones with the same AML-driver mutations in >95% of micro-CHIP patients; ref. 70). Thus, there is an urgent need to define the molecular, antigenic, and immunologic repertoire of “preneoplasia” through a PCA that includes the study of preclinical models and longitudinal cohorts conducive to rigorous assessment of the effects of spatial expansion and temporal evolution of preneoplasia-associated genetic alterations. Most solid tumor precancer studies are cross-sectional, including tissue adjacent to cancer or precancer tissue without clinical follow up. Increasing spatial and temporal sampling in combination with multi-omic approaches will be critical to fully understand the relationships between precancer and cancer. The importance of longitudinal study is illustrated by Barrett to esophageal adenocarcinoma. Recent Barrett study with 9-year follow-up detected p53 mutations (before the onset of dysplasia or copy number changes) associated with progression to high-grade disease or cancer (202), challenging the prevailing view from cross-sectional studies of tumor/precancer pairs (including two high-profile papers in Nature Genet, September 2015) that p53 mutations occur late, at the time of high-grade dysplasia (HGD) or esophageal adenocarcinoma, and underscore the potential of genomic profiling as an early indicator of progression risk, informing screening guidelines.
Primary prevention
Current obstacles to addressing the dominant cancer risk factors relevant to the U.S. population relate to poor implementation and dissemination of existing evidence-based interventions, particularly for tobacco, UV exposure, and HPV vaccination. The advent of e-cigarettes presents a challenge to tobacco control efforts, while outstanding research questions and measurement issues related to obesity, energy imbalance, and physical inactivity limit our ability to design and implement effective risk-reducing interventions.
Tobacco.
The reduction in tobacco use in the U.S. population over the last 50+ years is a notable, albeit limited success with recent rates of adult tobacco use averaging 17% nationally. Remaining challenges relate to the high rate of tobacco use in certain sectors of the population, particularly among individuals who are homeless (among whom tobacco use rates are 75%), are affected by mental health issues (use rates 40%–45%), or live in states with fewer evidence-based public health actions to reduce tobacco consumption, including taxes, comprehensive smoke-free air laws, and mass media public education programs (203). Although effective drugs and counseling strategies have been developed, defining the optimal regimen for various population subsets remains an active area of investigation. Optimizing delivery of effective regimens to those in greatest need has proven challenging, despite the progress offered by including tobacco cessation services as a billable option without financial barriers. Although data suggest that most smokers are keen to quit, most find it challenging to quit on their own. Quitline services now offered in every state are helpful. For example, disparities implementation and dissemination work (204) is illustrated by the Asian language quitline to improve access. Tobacco control disparities research identified serious concerns, including that Hispanic adolescent never-users of tobacco products were significantly more susceptible to future use of a tobacco product than non-Hispanic whites (205, 206). Similarly, cessation guidelines have been developed and promulgated (207), but too few primary care or oncology clinicians prioritize their delivery as an essential part of care (167). As such, challenges remain regarding how best to help patients overcome nicotine addiction, how to implement those practices in the clinic and population, how to disseminate state-of-the-art practices broadly, and how to reach at-risk populations.
New tobacco-derived products (e.g., e-cigarettes, hookah) have entered the U.S. market in abundance and without attention to product standardization, testing, regulatory guidance, or oversight. Research on these products has been challenging due to lack of standardization and the unlikelihood of securing an investigational new drug application. Debate continues on the value of these devices in assisting with cessation or harm reduction. In addition to cessation efforts, preventing smoking “initiation” has resulted in profound reduction in lung cancer mortality (208).
The growing use of nicotine delivery devices among younger populations is concerning, in terms of both absolute risks and relative to traditional burned tobacco products (209). Restricting youth exposure to smoking ads and access to cigarettes reduces smoking initiation and subsequent lung cancer mortality. Utilizing data from 10,989 never smokers age 12 to 24, receptivity to e-cigarette ads was associated with 1.6-fold increased risk of conventional smoking, suggesting that e-cigarette ads threaten one of the great public health successes of the last 50 years (210).
Obesity, energy imbalance, and physical inactivity.
Nutrition is a determinant of cancer risk. Changes in cancer incidence follow immigrants’ acculturation and population subgroups with different lifelong dietary patterns showing reduced cancer risk (e.g., Seventh-Day Adventists’ vegetarian diets versus the U.S. population’s average diet; ref. 211). International Agency for Research on Cancer (IARC) now classifies numerous cancers as preventable by avoiding weight gain (121). Challenges in obesity research include insufficient mechanistic insights into the condition’s relationship with cancer, limited evaluation measures, lack of insight regarding which measures are most associated with risk of cancer, and lack of effective, long-term interventions.
Various hypotheses underlying the obesity–cancer link have been advanced, including chronic inflammation, alterations in obesity-related metabolic hormones (e.g., leptin, incretin, insulin, glucagon, insulin-binding growth factor), hormonal responses, and behavioral addictions (212). According to the recent IARC working group, evidence for the role of sex hormone metabolism and chronic inflammation in mediating the obesity–cancer relationship is strong, whereas evidence for the role of insulin and IGF signaling is moderate (121).
Obesity’s relationship to cancer has mostly been described in associative terms, yet the relationship is believed to be causal for 13 cancer types. This number might be higher were it not for limitations and variability in measurement techniques, especially at the population level. Studies have variously used weight, BMI, waist circumference, or waist-to-hip ratio to measure obesity, although it remains unclear what measurement is the most relevant. Furthermore, calculations such as BMI remain poor indicators of an individual’s personal risk for developing cancer, cardiovascular disease, or type II diabetes mellitus. Some studies suggest that “metabolic obesity” can occur in healthy-weight individuals, but may be underdiagnosed, resulting in a lost opportunity to intervene and reduce disease risk (213, 214).
The ideal body weight, diet, level of physical activity, and combination of these components for cancer prevention is ill-defined and largely based on population-level associative data, rather than clinical trials. When clinical trials have been conducted to query the impact of dietary adjustments in preventing cancer, answers have been inconclusive, likely due to the short duration (3–5 years) of the intervention versus the longer time necessary to develop cancer, as well as the difficulty of modifying eating and exercise behaviors across time. General recommendations related to diet and physical activity continue to be defined and supported by several foundations and professional organizations, such as ACS, ACSM, AICR, and ASCO (120, 122, 168, 171). Several groups are also engaged in clinical trials aimed at better defining the details of physical activity in terms of types, level of intensity, duration, frequency, and end goals (i.e., a particular BMI, heart rate, level of fitness, etc.) in an attempt to identify opportunities for targeted cancer prevention.
UV radiation exposure.
Sun safety and UV protection are associated with increased risks for a variety of skin cancers including basal cell carcinoma, squamous cell carcinoma, and melanoma. Skin cancer is the most common malignancy in the U.S. population, accounting for nearly 5 million cases annually (131). Intense and early exposures during childhood are associated with increased risk for melanoma, with children exposed to intense levels of UV radiation (i.e., resulting in sunburns), exhibiting an elevated melanoma risk of 60% to 90% (131). Cumulative lifetime UV exposure also raises an individual’s proportional risk of developing basal cell carcinoma and squamous cell carcinoma, associated with profound elevations of tumor mutational burden, and tend to occur at advanced ages (131).
Remaining challenges related to sun safety and UV protection include defining the pathophysiologic role of UV exposure in cancer development. The typical C-to-T transversions induced by UV do not explain the range of genetic mutations identified in skin cancers. The role of sunscreens in reducing skin cancer risk, particularly regarding their mechanisms of action, optimal doses, as well as frequency and duration of use to achieve preventive efficacy, also remains undefined (131).
Cancer-associated microbial infections.
The microbial genesis of several types of cancer (e.g., HPV and cancers of the cervix, anus, genital tract, and oropharynx; hepatitis B and C and hepatocellular carcinoma; H. pylori and gastric cancer; human immunodeficiency virus and AIDS-defining malignancies; etc.) have been identified. Thus, cancer prevention can focus on behavioral actions that reduce the risk of exposure, such as vaccination against the offending organism and promptly identifying and treating infections. Challenges related to microbial-based prevention relate to the lack of knowledge of whether other unrecognized infectious causes of cancer exist and the role of the host microbiome in cancer development or progression. Beyond discovery science, questions remain regarding implementation and dissemination of screens for infectious causes of cancer as well as implementation of vaccinations or treatments for chronic infections associated with cancer. Approximately 79 million people in the United States are infected with HPV, according to CDC statistics, with an estimated 14 million new infections occur annually. These include several high-risk types that are responsible for about 39,000 new HPV-associated cancers each year. However, even routine HPV vaccination has been challenging, despite the vaccinations’ efficacy (137). An obstacle in HPV vaccine uptake has been the “negative” public and social media reports, including regarding HPV vaccine safety. These inaccurate reports and the larger antivaccination movement will need to be counteracted to improve vaccination rates and the use of immune prevention measures in all populations. Increased efforts are also needed to educate physicians so that they may better communicate the benefits of vaccination to their patients. Finally, additional research is needed to develop a screening test for HPV-related precancers and cancers at other, noncervical sites, such as the anus and oropharynx. The NCI-sponsored Costa Rica Vaccine Trial was designed to assess the efficacy of Cervarix in a community-based setting, finding that two doses of the HPV vaccine Cervarix were as effective as the current standard three-dose regimen after 4 years of follow-up (215). HPV vaccine dosing continues to be a major focus to enhance vaccine adherence/uptake. An ongoing randomized noninferiority study in Costa Rica is comparing one versus two vaccine dose effects on persistent infection, and plans for a randomized “immune-bridging” study in the United States to evaluate whether one and two doses achieve stable antibody levels associated with protection from persistent infection in the Costa Rica study. Although a definitive RCT of the prophylactic HPV vaccine to prevent oropharyngeal cancer is unlikely to be conducted, the vaccine has been shown to protect against oral HPV infection, suggesting an additional benefit of vaccination programs for both women and men. AACR, ASCO, and other major organizations are promoting an international educational public health campaigns to increase HPV vaccine uptake, including AACR’s February 1, 2016 Catalyst “Call to Action” and ASCO’s Statement in May 2016 (216), and NCI-designated cancer center consensus statement, identifying the roadmap to increased vaccination uptake, with intense focus on shifting emphasis from behavior associated with infection to preventing major cancers and further study of 1 versus 3 doses. Vaccine uptake is much lower in boys, Hispanics and African Americans. In January 2017, the 69 NCI-designated cancer centers endorsed the CDC’s revised guideline that calls for administration of the HPV vaccine, and highlighted the need for physician advocacy.
Environmental risk factors.
Environmental risk factors can cause cancer, and there are numerous historical examples largely arising from occupational exposures. Included in the roster are links between exposures to chimney soot and scrotal cancer, benzene and hematologic malignancies, and asbestos and mesothelioma. Environmental and workplace protections enacted to reduce or eliminate exposures have resulted in substantial reductions in cancer risk and incidence.
Ongoing challenges regarding environmental risk factors include consideration of which, if any, remaining exposures may be associated with cancer risk, at what doses, durations, and frequencies of exposure, and who may be at greatest risk due to either exposure or individual metabolic susceptibility (217). Of special importance is elucidating how early life exposures to environmental agents may transiently or permanently affect subsequent cancer risk. A key issue in such work is the need to build the scientific case against a potentially carcinogenic exposure with non-experimental investigations including observational studies of exposed versus unexposed humans, supplemented by studies in cell and animal-based models. Development of tools to better assess the range of environmental carcinogens and the characterization of their mutational signatures will help guide priorities. Identification of plausible biologic mechanisms is needed to validate claims in the absence of direct experimental data. Given innumerable potential agents and exposures that may be carcinogenic, prioritization is challenging. Such exposures are expected to be uncommon in the United States in 2018 and beyond as highlighted in recent reviews that estimate population-level risks of environmental exposures at <1% to >60% for different cancers and instead highlighted the importance of early detection and interception in reducing overall cancer burden (218). Communication of results and implications of such studies to all stakeholders remains challenging as well (14).
Secondary prevention
Secondary prevention typically involves two steps. First, a screening test is applied to a group drawn from the general population to identify a subset of individuals at increased risk due to:
Prior risk-inducing exposures and behaviors.
Inherent susceptibilities (e.g., differences in carcinogen metabolism or protective functions).
Neoplastic hallmarks such as increased proliferation, reduced apoptosis, genetic mutations, inflammation, and/or reduced immune surveillance in one or more tissues.
Presence of subclinical precancerous lesions such as incidentally discovered (asymptomatic) mucinous pancreatic cysts.
Next, an intervention involving lifestyle changes, surgery, and/or medications is applied to reduce the adverse effects of carcinogen exposure or to treat precancerous lesions and, thereby, reduce cancer risks.
Risk evaluation and screening.
Even tumors that look histologically similar can vary in biology and progression. Such heterogeneity combined with the dearth of data regarding early stages of the disease add complexity to identification of preventive agents as well as design and implementation of clinical trials.
Many cancer risk models do not address biologic variability. A lack of longitudinal data and precancer samples from patients following treatment weakens modeling of the progression or regression of precancerous lesions and prediction of long-term outcomes. There is also a compelling need to progress beyond association studies to better understand the mechanisms that cause disease. Large genomic databases and less expensive molecular testing platforms enhance the opportunity for large-scale genomic and risk stratification studies, which have been invaluable for understanding advanced cancers (219). Many experts argue that “truncal” mutations identified in such analyses may also identify the earlier mutations most relevant to precancer biology, providing insights to the timing and sequence of such alterations in cancer progression (220). Analyses of advanced cancers may never fully reveal the biology of early neoplastic development, which is likely to be irregular, as evident by the ability of precancers to progress, lie dormant, or regress entirely.
Studies with sufficient scientific rigor that do not disrupt the natural progression of cancer are difficult. For example, laboratory studies of precancer biology often require an intervention (such as a biopsy to provide tissues for analysis) that inherently alters the natural history of the precancer. Thus, the integration of molecular biomarker data with longitudinal clinical outcomes data in the presence and/or absence of preventive interventions remains limited for precancers.
Hereditary syndromes that predispose to cancer offer opportunities to analyze precancerous states, and the development of such high-risk patient cohorts are critical to inform research, providing insights relevant to the broader population (e.g., the recent launch of GENERATE). For example, individuals with family history of pancreatic cancer or germline alterations who undergo pancreatic surgery on screening have a higher rate of multifocal PanIN and cystic lesions (221).
Bias can limit the usefulness of tests designed to identify precancers. For instance, screening tests are better at identifying slow-growing than fast-growing precancerous lesions. Lead-time bias may accelerate the time to identify precancers and cancer without improving survival, and populations willing to participate in screening often live in a healthier manner than those less interested in screening tests, causing a “healthy person” bias.
The prevalence of risk factors differs by populations and can invalidate a screening test. For example, screening will not reduce all-cause mortality if only a minority (e.g., 2%–3%) of those with the cancer die because of the malignancy. Even if screening is successful, oftentimes less than 1% are saved. This explains why the number of lives saved by screening is typically small. Finally, there are rigorous criteria for any screening tests prior to implementation (e.g., disease significance, acceptable test, effective and differential treatments for those with vs. without risk factors or lesions, a tangible difference in outcomes in those screened vs. those not screened). Unless all components are aligned, screening tests are often uninformative. More sensitive (e.g., metabolic) screening tests are needed.
Just as great is the need to understand the biology of identified lesions and to predict the fate of detected tumors. Patients present with few reliable intermediate surrogate biomarkers for health outcomes after screening. As a result, researchers rely on mortality data, which is often difficult to capture and may change because of any number of factors involved in data collection and interpretation. Such factors include tissue sampling, the type and amount of biospecimen, biopsy or collection technique, initial preparation and processing, assay, data analysis, and data interpretation. Identifying biomarkers is challenging, which is why so few screening and early detection markers have been developed, validated, clinically tested, and commercialized – cervix, colon and most recently, lung (222). Standardization of techniques as well as better molecular characterization of precancerous conditions may help overcome these challenges.
New tests require validation on a population level. Without such analysis, there is a risk for “overdiagnosis,” which involves the detection and, in many cases, treatment of individuals with precancers or cancers that may never have harmed the individual. Many screen-detected lesions including low-grade PanIN and ductal carcinoma in situ may not progress to lethal cancers, but rather trigger treatment and possibly overtreatment because it is difficult to determine whether a lesion will become progressive or life-threatening. In such instances, survival rates and cure rates may improve without ever actually improving cancer-related or overall mortality, as has already been shown regarding melanoma, thyroid, prostate, and kidney cancer.
Risk detection strategies that guide clinical decision making are often based in image data rather than molecular data. Imaging permits insights into risk with minimal disturbance to the tissues. Mammography, CT colonography and abbreviated liver MRI are typically applied in a screening context, although they may be used later in a more diagnostic context. These early-detection tests often depend on highly skilled operators or relatively expensive technologies, rendering them vulnerable to variability and less accessible to large cohorts of patients. Biomarkers may be employed along with imaging to improve outcomes and limit risks, although challenges of limited access and quality control across providers remain in many instances.
Cancer interception.
Identification and development of preventive interventions faces long-standing challenges. First is the lack of well-established developmental strategies that have generated strong returns on investment. Although there are now more than ten FDA-approved agents for the treatment of precancers or reduction of risk in above-average-risk individuals (Table 2), the developmental paths for each have been varied, challenging, and in many cases, expensive in terms of time, study subjects, and cost (223). Thus, drug development for cancer prevention or precancer interception is largely publicly funded, with only a limited number of new experimental agents available for testing (176). The most cutting-edge new cancer interception agents are actually repurposed FDA-approved for different indications, which in theory should accelerate the preventive drug development process.
A chief concern is the lack of clinically meaningful and predictive intermediate efficacy markers tied to cancer biology that could guide phase II prevention trials, prioritize agents for entry into phase III trials, and accelerate the developmental process. Preventive agent development often requires protracted timelines between application of an agent and assessment of its clinical benefit. For example, HPV vaccines were FDA approved on the basis of their effects against precancers of the cervix, vulvovaginal, and anus in women and not their effects to prevent invasive cancers. Beyond the initial FDA approval as a preventive vaccine, it would now be useful to understand the vaccine’s effect on HPV viral persistence to better inform screening algorithms.
While it is clear that HPV causes a subset of oropharyngeal cancers in men, cancers that are rising in incidence, to date there has not been a phase III trial dedicated to testing the efficacy of HPV vaccines against this endpoint in male populations, and at this point, given its widespread recommendations for girls and boys, a phase III trial in this setting is unlikely. Oral HPV infection is being used as a surrogate endpoint in this context, and cohort data will also likely provide important insights into this issue.
Identification of high-risk individuals most likely to benefit from a preventive intervention remains challenging, as risks are an amalgam of lifetime exposures to carcinogenic influences. It is unclear how we can quickly and accurately identify at-risk individuals based on their full spectrum of genetic susceptibilities, lifestyle choices, and cumulative exposures. Models exist for specific exposures (e.g., “pack-years” re: tobacco exposures), genetic risks (e.g., family history, germline mutations, BRCA-PRO), commonly involved organs (e.g., Gail or Tyrer–Cuzick models), precancers (e.g., Zauber/CISNET re: adenomas and colorectal cancer risk), or several aspects of lifestyle choices (“Your Disease Risk” model at Washington University, St. Louis, MO). Short-term risks in different germline settings are critical to trial designs and available on the ask2me.org website. However, an ideal model predictive of both risks and benefits following preventive interventions remains to be developed.
In some cases, preventive medicines and medical interventions are most effective when combined with behavioral interventions. For example, tobacco cessation is most effective when nicotine replacement (e.g., varenicline, or buproprion) is combined with behavioral counseling (224). Success rates for such combinatorial programs are as high as 35% to 45% versus average quit rates of <5% with self-treatment, or <10% with assistance from state quitlines as described below regarding the Asian Smokers Quitline.
Treating cancer-associated microbial infections is another method of cancer interception. For example, hepatitis B vaccination is effective in the short term on hepatitis B infection (225) and in the long term on rates of chronic hepatitis, cirrhosis, as well as hepatocellular cancer in vaccinated versus unvaccinated populations (226). HPV vaccination has similar effects on the rates of HPV-related (e.g., oral) infections and precancers, and likely similar effect on development of cancers, cancer-associated morbidities, and cancer-associated mortality over time in populations with good vaccination rates. A recent Australian cost analysis proved that changing from Pap testing every 2 years to primary HPV testing every 5 years with partial genotyping saves lives, is more cost effective, and reduces disease incidence (227). Finally, although hepatitis C screening and treatment is recommended by the CDC and others (see above), disease incidence in underserved populations of the United States with high rates of needle sharing or sexual exposures, combined with high medication costs, have made implementation of recommended screening and drug delivery challenging. It is currently estimated that 50% of HCV infection is occult, with an estimated 3.5 million infected. Only 16% of this number receive HCV treatment, and 9% achieve sustained virologic response (228). Overall, implementation of screening and drug delivery for cancer prevention in the United States is often limited by practical concerns of dissemination related to socioeconomic status, underscreening, and costs.
The role of immunity and immune modulation in the development, progression, and treatment of precancers remains unknown for cancer interception. One clinical pathway would be immunization of patients with precursor or high-risk lesions to eradicate noninvasive tumors, or to prevent their progression to invasive malignancy. Unfortunately, even in preinvasive and high-risk lesions, complex modifications are occurring in the TME that may limit the generation of effective vaccine-induced immunity. For example, single-cell RNA-sequencing analyses of IPMNs found progressive depletion of cytotoxic and Th cells and dendritic cells at the expense of immunosuppressive myeloid-derived suppressor cells (45). Furthermore, even early mutations may drive immunosuppressive mechanisms as illustrated by KRAS mutations in early pancreatic precancers, inducing the secretion of GM-CSF and IL-6, which recruits myeloid cells that drive a proinflammatory microenvironment, thereby enhancing tumor growth and limiting the development of adaptive immunity (229, 230). This phenomenon has also been shown for Ras-mutated lung precancer and is associated with a poor prognosis (231). Elevated levels of myeloid-derived suppressor cells, potent suppressors of type I immune responses, are present in patients with colonic adenomas, preventing successful immunization with a MUC1 vaccine designed to prevent progression to invasive colorectal cancer (232).
Tertiary prevention
Challenges related to cancer prevention extend to the tertiary setting as well. Lifestyle elements can improve quality of life and survivorship. As in other areas of prevention, implementation and dissemination of effective strategies are likely to be uneven across the U.S. population. Most clinical datasets and studies are limited in their racial and ethnic diversity. Few studies collect data on risk, geographic, and socioeconomic factors important to outcomes, missing an opportunity to address compelling questions related to cancer survivorship.
Cancer treatment summaries required by the American College of Surgeons’ Commission on Cancer to ease care transitions between providers include limited information on health behaviors. There is no clinical or population-based infrastructure to support recommended health behavior changes or to assess their uptake by individuals or populations. We must move beyond periodic dietary self-assessments to more robust assessments and biomarkers for cancer risk. Implementation of exercise and weight management into cancer survivorship care plans has been limited by a lack of reimbursement for these services. One solution may be to include exercise programming as part of outpatient cancer rehabilitation services.
Current limitations and obstacles in cancer prevention: summary.
- Barriers to the further development of cancer prevention as a strategy to reduce the cancer burden are numerous, varied, and include the:
- Overall breadth of the prevention field;
- Definition of disease worthy of identification and intervention;
- Consideration of the relative impact of a preventive versus therapeutic strategy;
- Lack of private funding;
- Challenges in interdisciplinary communication;
- Fragmented health care systems unable to provide evidence-based and comprehensive prevention and screening services.
Accurate and comprehensive forecasting regarding the prognosis of a lesion, the organ in which it is contained, and competing causes of morbidity and mortality are the collective goals of cancer risk assessment and intervention.
The extent and implications of precancer heterogeneity are just now beginning to be elucidated. As recently demonstrated in the context of pancreatic cancers, multistep progression can occur over a span of many years, and ancestral clones of cells harboring driver mutations can migrate through the ductal system, colonizing topographically distinct areas of the parenchyma (23). Similar findings were reported years earlier in the context of a single p53-mutant clone colonizing the respiratory tree in a patient with widespread squamous dysplasia but no overt carcinoma (233). These data on “field cancerization” by mutant clones underscore the challenges of screening individuals for initial or subsequent cancers, and suggest that screening might be a lifelong consequence in certain contexts.
Additional studies are needed to define the role of the microbiome in the development, progression, and prevention of precancers. The recent identification of high quality neoantigens in long-term survivors of pancreatic cancer that demonstrate molecular mimicry with bacterial antigens suggests that the host microbiome is likely to impact the natural history of pancreatic cancer development through multiple mechanisms, both cell intrinsic and extrinsic (234).
The molecular complexity and heterogeneity of tumor biology and the limited existing data regarding the earliest stages of disease progression challenge preventive agent identification, trial design, and the ability to enroll molecularly similar patients in target-driven prevention trials.
The biology of early neoplastic development is dynamic, reflecting precancers that progress, lie dormant, or regress entirely.
Fourteen agents have received FDA approval for the treatment of precancers or reduction of risk in above-average risk populations.
- Preventive drug development challenges include:
- Lack of established developmental algorithms or strategies to generate significant returns on investment;
- Limited knowledge of the molecular mechanisms of the earliest stages of precancer development;
- Lack of valid and predictive intermediate efficacy markers tied to cancer biology;
Little is known regarding the role of immunology and immune modulation in the development, progression, and treatment of precancers for cancer interception.
Current clinical studies and datasets are limited in racial and ethnic diversity; few collect data on risk, geographic, and socioeconomic factors important to cancer outcomes.
Future Opportunities in Cancer Prevention
Advances in technology and bioinformatics provide unprecedented opportunities to better identify, characterize, and detect preneoplasia and associated molecular aberrations. Highly sensitive and specific assessments of susceptibility and cancer risk, together with tailored preventive interventions, underlie the concepts of precision cancer prevention and molecularly targeted prevention (37, 235). Biomarker-based tests are already available for cancer detection, but their utility is often limited to early detection in high-risk populations. Molecule-based screening assays have the potential for both under- and overdiagnosis, requiring thoughtful interpretation well as confirmatory diagnostic testing and/or treatment.
Conceptual/procedural
Greater public and professional awareness of precancer development and progression will drive the public’s appreciation of the duration and complexity of carcinogenesis (236). Concordantly, ongoing research must be advanced to evaluate the best methods to educate the public and health professionals regarding screening trade-offs and how to evaluate screening tests’ value.
New technologies will help advance our understanding and practice of risk prediction and cancer prevention. Sorely needed are surrogate intermediate endpoints that can be quantified, tested by investigators through the existing preventive biomarker developmental paradigm (237), considered and approved by regulators, and applied as a focus for reimbursement by payors (176). Summit attendees suggested the need to create a “Roadmap for Precision Molecular Diagnostics” in collaboration with NCI, FDA, and other stakeholder organizations to clarify and standardize the regulatory pathway for preneoplasia assay development. Such insights may help render clinical trials smaller, shorter, more predictive of long-term benefits and risks, and less expensive. A more rapid and successful pipeline (e.g., using repurposed drugs) from research to the clinic will aid public interest in prevention and encourage investment from the private sector.
Cancer biology
A top scientific priority is to investigate the biology of premalignancy by better characterizing the molecular aberrations and pathways that regulate the earliest steps in precancer initiation and progression prior to invasion, as well as the biologic processes that sustain normalcy and nonprogression (i.e., the PCA). The summit recommended a national concerted effort to create a PCA, integrating multiomics, stem cell, and immune oncology—basic tenets of the neoplastic process—to interrogate, target, and intercept events that drive oncogenesis (6, 8, 34, 238). Suitable cancers to study include breast, colorectal, lung, pancreatic, and skin cancers. The project would include specimens from nonneoplastic tissues, nonprogressive precancers, and progressive precancers to gain broad molecular insights into current biology, as well as the selective forces that shape the evolution of cancer from its inception through potential paths of dormancy, regression, or progression to an invasive state. Both epithelial tissues as well as the surrounding TME should be studied. Cancers for which we have banked tissues, or for which tissues can be easily and serially accessed (e.g., skin nevi, colorectal polyps, oral precancerous lesions) may represent an opportunity to pilot studies on how biomarkers change with disease development. Such sampling should include representation from all subpopulations, including underserved and underrepresented constituencies.
Analyses of biospecimens should be technically comprehensive and cover the spectrum of neoplastic initiation, development, and fate. Genomic, epigenomic, and proteomic analyses of normal, preinvasive (progressive, dormant, and regressive), and high-risk lesions should be conducted to understand the linkage between genotype and phenotype. Such analyses may also result in the identification of useful immunogenic targets and provide clinicians the ability to explore immunologic alterations in tissues that may prevent successful immunization.
These analyses should assume a systems biology computational approach to optimize integration and data interpretation across multiomic and immune profiling in longitudinal samples collected over time. Insights might include:
Processes underlying germline deterioration via clonal expansion of somatic alterations in healthy tissues during aging;
Identification of markers from TCGA and PCA data for progression and early intervention of premalignant lesions;
Integration of high-throughput data from various platforms with clinical data;
Integration of genetic and environmental risk stratification models for targeted screening and prevention;
Biomarker identification for early detection and for use as surrogate endpoints for chemoprevention trials;
Better methods for analyzing metadata and combining data using methods such as network meta-analysis, and;
New ideas, such as the use of wearable devices and self-enrollment into prevention studies.
A systems biology approach should be used to inform the development of preclinical model systems that are critical to progress (especially for exposures that cannot be tested in humans), as well as to determine which preclinical systems might be best suited to analyze prevention. Imaging should become better integrated into precancer research. For example, the importance of liver fat in NASH progression was established with new imaging technology called MRI Proton Density Fat Fraction [see “Cancer Chemoprevention” subsection; opportunities for serial measurement and assessments across time and individuals should be leveraged, using imaging and “omics”-based assays of easily accessible cancer or surrogate tissues (e.g., blood, buccal mucosa, skin] that have already been used for epidemiologic analyses.
Little is known about how the microbiome influences immunity and neoplastic initiation and progression, and much remains to be determined, including:
Do specific microbiota protect against, or stimulate cancer initiation and progression?
Does the microbiome contribute independently to cancer risk?
How may microbiota be manipulated to reduce the risks of cancer and/or other chronic diseases?
The human microbiome may profoundly influence the immune response to cancer, which underscores the need for complete characterization of the oral, gut, and genitourinary flora and their relationship to immunity. Further characterization of the microbiome in the presence and absence of cancer will be essential to understanding how best to leverage the microbiome to detect and treat cancer.
Primary prevention
Several opportunities relating to primary prevention or interventions designed to reduce cancer risks or exposures are relevant to the average-risk, general population. Epidemiologic or environmental transitions in precancer or cancer incidence or mortality (e.g., concomitant increases in liver cancer incidence/mortality in the United States with reductions in Asia; reductions in lung cancer incidence/mortality in the United States with increases in Asia, etc.) provide opportunities to study cancer etiology. Better data are needed, however, on population-wide behaviors relevant to cancer and precancer initiation and development. In addition, development and application of exposome technologies could improve understanding of environmental etiologies and mechanisms of carcinogenesis.
Tobacco.
Progress in reducing the prevalence of tobacco use over the last 50 years has been notable, but not equitably distributed across all population subgroups. The prevalence of tobacco use remains high among those with mental health conditions, those with a high school education or less, those living below the poverty level, and among Native Americans and other vulnerable populations. Further progress will depend on reducing the rates through control efforts tailored to these groups (115).
Electronic nicotine delivery systems (ENDS) or e-cigarettes present a new challenge and threaten to undo the half-century of progress made in tobacco control. Although some experts advocate use of ENDS for tobacco cessation and harm reduction, the December 2016 Surgeon General’s Report affirms a strong association between the use of e-cigarettes and use of conventional tobacco products (209). Particularly concerning is that e-cigarettes are now the most commonly used form of tobacco among youth. According to the CDC, approximately 16% of high school students and 5% of middle school students reported current e-cigarette use in 2015, compared with 1.5% and 0.6% in 2011, respectively (239). This is concerning not merely because of the potential for subsequent traditional tobacco use, but because ENDS are designed to deliver nicotine, a highly addictive substance that is unsafe in any form for youth. Additional concerns surround the aerosol that ENDS emit. The Surgeon General’s Report states that it is not a harmless vapor as some have suggested, but rather that it contains several known carcinogens. In 2016, the FDA deemed ENDS subject to their regulation, allowing the FDA to regulate the manufacture, import, packaging, labeling, advertising, promotion, sale, and distribution of ENDS, although regulations have not been promulgated to date.
Opportunities to prevent and reduce e-cigarette use and associated harms include:
Raising and enforcing the minimum legal age of purchase for all tobacco products;
Including e-cigarettes in new and existing smoke-free policies;
Regulating e-cigarette marketing;
Educating youth on the dangers of e-cigarette use, and;
Expanding and improving research related to e-cigarettes.
Obesity, energy imbalance, and physical inactivity.
Obesity is fast becoming a dominant cancer risk factor in the United States and other Western populations, suggesting its importance as an opportunity for cancer prevention research and evidence-based cancer control actions (240). In response to this growing area of concern, key recommendations were outlined:
Apply lessons learned from tobacco use control to other macro-associated risks such as obesity, physical inactivity, and high-sugar beverages;
Promote preclinical and clinical studies of “metabolic obesity” in rodent models and/or healthy-weight individuals;
Investigate how weight loss during adulthood influences cancer risk associated with lifetime obesity;
Develop greater insight into which mechanisms link obesity to cancer;
Evaluate exercise as a systemic intervention.
Summit participants raised numerous questions related to obesity, including:
Should DEXA scans to assess body composition become a part of routine clinical care of normal size individuals to complement and extend the insights provided by BMI?
Can clinical interventions improve adipose-related chronic inflammation, reduce insulin resistance, induce weight loss via medications, and/or modify the microbiome?
Given metformin’s promise as a possible preventive agent, how does it work to reduce cancer risks, is it efficacious in clinical testing in various populations and settings, and what are its effects on the microbiome or on cancer vaccine efficacy?
Are biguanides effective at controlling blood sugar and/or cancer initiation and development?
Can weight management reduce cancer risks in clinical trials, and if so, at which sites and over what time course?
If weight loss or increased physical activity reduce cancer risks, how might we best incentivize these actions across the population?
UV radiation exposure.
There are many evidence-based opportunities for actions to reduce exposure to harmful UV radiation, from both natural and artificial sources. At the policy level, 13 states plus Washington, D.C., have passed legislation banning minors from the use of tanning beds, with more states considering similar legislation. In 2013, Texas banned those under age 18 from using tanning beds; by 2016, most indoor-tanning facilities within the state complied with the ban (241). Policy changes at the institutional level could help but are as yet limited. For example, schools might provide more shade structures to cover playgrounds or institute policies permitting the application of sunscreen or requiring hats to be worn by children when outdoors. In addition to policy changes, greater awareness of the harmful effects of UV exposure in all forms is needed. Several research-tested intervention programs designed to increase awareness and promote sun-protective behaviors, particularly among children, are now publicly available through NCI’s Research-Tested-Intervention-Programs website. Key remaining questions include how best to implement and disseminate such programs tailored to the needs of high-risk populations and high-risk regions of the country.
Cancer-associated microbial infections.
Opportunities in this area relate to improving the implementation and dissemination of evidence-based interventions, such as increasing rates of HPV vaccination and HCV screening. Within the United States, HPV vaccine uptake can be accelerated by:
Reducing missed clinical opportunities to recommend and administer the vaccine;
Strengthening providers’ recommendations to parents;
Ensuring the consistency of vaccine messaging;
Increasing acceptance of the vaccine among parents, adolescents, and caregivers, and;
Maximizing access to vaccine services (137).
A mixture of actions from across policy, education, and clinical service domains will be required to fully leverage these opportunities. To spur vaccine uptake globally, the United States must continue to collaborate with and support GAVI, The Vaccine Alliance as well as low- and middle-income countries in their efforts to develop and implement cancer control plans and registries (137). The cancer-preventive benefits of the HPV vaccine include randomized trials of single-dose schedules (215) and cohort studies assessing vaccine efficacy for oropharyngeal cancer development.
Opportunities to prevent liver cancer due to HCV relate to better identification of infected individuals with subsequent linkage to treatment. Because a screening strategy based on risk alone missed more than 50% of HCV infections, and because those born between 1946 to 1964 accounted for three fourths of all HCV infections, the CDC recommended one-time birth cohort screening in 2012, to complement continued risk-based screening (242). Few data exist at the moment regarding the one-time birth cohort screening strategy. Current studies are testing various interventions to identify those who should be screened (243). A 2014 modeling study showed that expansion of one-time birth-cohort screening to one-time universal screening would identify an additional 446,700 HCV cases over a decade. If treatment capacity were unlimited, this result could reduce adverse long-term outcomes, leading to 96,300 (40%) fewer HCC cases between 2014 and 2050 (244). Thus, we have an opportunity to improve HCV case identification and long-term HCV outcomes, including liver cancer, through more aggressive screening recommendations and expanded treatment capacity. The Extension of Community Healthcare Outcomes project, begun by hepatologist, Dr. Sanjeev Arora at the University of New Mexico (Albuquerque, NM), shows potential to increase treatment capacity by improving access to care for poor and underserved populations at risk of HCV infection (245).
Environmental risk factors.
As noted in the 2010 President’s Cancer Panel report, there are innumerable opportunities to explore various environmental risk factors and cancer (217). The President’s Cancer Panel identified several classes of agents linked with various cancers, but details regarding dose, duration, and frequency of exposures required to cause cancer are needed, as well as how risks of exposure might be best mitigated.
For the future of primary cancer prevention, we must prioritize prevention, as well as personalize precisely delivered assessments of risk, exposures, and individualized interventions. Delivery should reach outside of clinical settings. As wearable sensor technologies become more commonplace, precise and individualized health interventions may replace generic public health recommendations.
Secondary prevention
Opportunities to direct preventive interventions or interception toward at-risk individuals abound. Furthermore, precision cancer prevention continues to attract attention from cancer researchers operating in basic, translational, population, and clinical sciences, as well as in private industry, as the identification of high-risk cohorts and target-directed interventions both involve molecularly informed analyses.
Risk evaluation and screening.
Risk evaluation for secondary prevention typically involves identifying individuals at greater than average risk from a larger population. Identification depends on questionnaires or clinically based parameters, such as assessment of past exposure to cancer risk factors or a personal or family history of precancer or cancer. Many risk models based on such data are already in place and applied clinically. Such instruments guide approved interventions and identify high-risk individuals for entry into prevention trials. It is unknown whether germline or environmental exposures have already altered tissue biology in a manner that would result in increased cancer risks due to aberrancy in molecular pathways or functional hallmarks of cancer. On a population level, application of such molecular assays for risk stratification may provide mechanistic insight into associations between exposures and cancer risk via pharmacogenomics and/or pharmacometabolomics.
Biospecimen collection could generate valuable resources. For example, genomic assessment might arise from DNA obtained from an accessible site unlikely to have been affected, such as blood, buccal mucosa, or skin, as opposed to sampling from exposed and possibly affected tissues or associated fluids, such as from the colon or lung, which may exhibit “field cancerization” effects (246). Assessments would survey not only the germline and potentially affected tissue genomes but also the metabolome, proteome, microbiome, and tissue microenvironment(s). Analyses would be cross-integrated. Results might permit comparisons across the spectrum of neoplastic development and progression including normal, precancers, and cancer, as well as across a population of individual lesions within and across individuals to gain insight into the uniformity or heterogeneity of molecular aberrations or precancers.
Applications of such molecular knowledge could assist risk identification and stratification on the context of cancer prevention. For example, such information could distinguish patients with indolent lesions from those with aggressive lesions, thus distinguishing those who may be able to avoid invasive procedures from those who should undergo additional testing. Molecular markers can also help identify which therapies might be best suited to which patients and to distinguish those likely to respond from those unlikely to respond. With such tailored prognostic information, recommendations for preventive and surveillance strategies can be personalized.
These data lay the groundwork for individually focused, precision approaches to cancer screening, diagnosis, and prevention. Individuals with the most immediate risk could be identified. The process of cancer development could be better understood. At the moment, such markers would most likely be derived from biospecimens and tissue samples and processed for molecular markers. In the future, use of systemic markers (e.g., circulating tumor cells) or molecularly informed imaging may be possible. Easily accessed markers or noninvasive imaging could also reduce the need for invasive procedures and help overcome difficulties associated with accurately measuring processes without disrupting them.
Improved biomarkers or imaging bring opportunities to better define the natural history of precancers and increase our ability to screen and provide preventive interventions. Integrated analysis of biostatistics, bioinformatics, and genetic epidemiology is required to predict which precancers are most likely to remain stable, regress, or progress and become of clinical concern. More understanding of precancer biology combined with more quantitative statistical analysis will help refine screening algorithms, reduce the invasiveness of risk assessment, and reduce overtreatment through better identification of individuals most likely to benefit from screening.
Expanded biomarker characterization and research will also inform implementation and dissemination research related to neoplastic screening and risk assessment. Implementation and dissemination research carries over from clinical efficacy trials to cancer control, identifying actions that could with reasonable assurance realize the promise of prevention research across populations. Research on the optimal implementation of screening tests has distinguished effective from ineffective screening tests, protecting patients from unnecessary harm and reducing unproductive diversion of health care resources.
Cancer interception.
Prevention can benefit greater-than-average-risk individuals in the context of cancer interception in many ways. Recent discoveries of mutation type, order and landscape, germline-somatic interactions, and immune signals are having profound implications on cancer interception (also listed above):
PCA: Molecular characterization of precancerous lesions will illuminate the process of cancer initiation and progression, clarifying “field effects” and the timing and role of heterogeneity in early lesions. A “3-D Atlas” of preneoplasia will also provide insights into the immune and stromal perturbations that accompany multistep progression, including putative neoantigens that might evoke a productive effector T-cell response and the dynamics of immune editing in preneoplasia. Combined with preclinical, in vivo safety, and efficacy data, insights may guide selection of agents for early-phase clinical testing. Selection criteria should take into account molecular targets and the fate or progression of precancers. Interactions between gender, anatomic site, risk-relevant behaviors, and host–pathogen interactions will need to be accounted for. Molecularly targeted agents: Insight into the molecular biology of precancer should facilitate the identification of targets, the molecular agents that can interact with those targets, and the testing of such agents in relevant populations. Molecularly targeted agents have revolutionized cancer therapeutics by reducing toxicity and improving responses in individuals whose tumors are driven by relevant mutations. Imatinib and BCR-Abl tyrosine kinase inhibitors have been very successful in treating patients with chronic myeloid leukemia. A breakthrough trial in patients with very high-risk precancer, such as FAP, with devastating development of duodenal adenomas, ethically justified an aggressive and more toxic approach (supported by strong biologic probability) and reported highly-significant clinical benefit after a 6-month intervention of erlotinib and sulindac (104). This seminal cancer prevention trial also highlighted the importance of exploiting repurposed drugs (erlotinib for lung cancer and sulindac for arthritis) to test new scientific hypotheses.
Microbial infection: The success of vaccines against cancer-associated microbes such as HPV and its related precancers, such as cervical, vulvovaginal, and anal precancers (247), suggests that prevention of microbial infection through vaccination (a primary prevention strategy) can reduce cancer risk at susceptible sites. Eradication of established microbial infection by treatment (a secondary prevention strategy), as with treatment of hepatitis C, should also safely reduce cancer risk. Data related to treatment of HCV and reduced risk of HCC are less mature as a report of veterans cured of HCV suggests that HCC may still occur (248). Timing of microbial eradication may influence preventive effectiveness. Nevertheless, even a reduction of risk could prove significant given how difficult HCC is to screen for, diagnose at an early stage, and treat.
Biomarkers: Biomarkers for the precancerous state are in short supply and are desperately needed to accelerate agent identification, testing, and approval. One example is oral HPV infection (especially in boys) as a surrogate vaccine endpoint informing potential impact on oropharyngeal cancer. Sustained virologic response, which has been used to identify drugs useful for hepatitis C treatment and for gauging clinical response. Future progress will depend on clinical trials designed to follow an intervention through to long-term and clinically valued outcomes. One example pertains to the prospective trials of circulating tumor DNA using ultrasensitive NGS technologies that are being pursued in apparently asymptomatic populations like adult women undergoing mammography. These prospective studies have the potential to realize both the promise of early detection and cancer interception, as well as the potential perils of overdiagnosis from detection of indolent precancers.
Thorough analysis of interception regimens: All aspects of an interception regimen, including the dose, route, duration, and frequency of administration, should be analyzed. Prevention has been thought to require daily, lifelong agent administration, but data now suggest that a daily regimen may not be required, especially with short-term immune interception approaches with PD-1 inhibitors in very high-risk groups, and cancer vaccines which may only require 1–3 doses to stimulation immune memory.
Interactions between interception and genetic variation. The host genome may influence where, when, and how (mutational landscape) cancer develops (64, 65). Key genetic polymorphism may interact with molecularly targeted or immune-directed agents, as well as other interceptive agents.
Precision cancer prevention may soon be possible. We must educate everyone about successes to date and the potential of this field to make a positive contribution to cancer management. This potential is neatly illustrated in the example of cervical cancer, where the most effective and widely implemented strategy is almost entirely premised upon screening, early detection, vaccination, and early precancer management. Cancer treatment is still required, but for fewer individuals as more progress occurs in implementation and dissemination of evidence-based screening and prevention programs.
Tertiary prevention
The future of tertiary prevention will depend on improved infrastructure to support behavioral interventions among survivors. Although lifestyle changes can mitigate risks of subsequent secondary cancers, lifestyle changes bring challenges as well. A triage system for exercise versus rehabilitation that is realistic and can be disseminated in the current oncology clinical care environment is urgently needed. Overall, the evidence base for cancer rehabilitation must be established. Research is needed to determine the effects of survivorship care on lifestyle behaviors. Research on energetics and cancer is needed. In addition, the field must prioritize individualized and population-based interventions that are capable of being implemented on a broad scale. Training and education supported by the NIH in the Trans-Disciplinary Research on Energetics and Cancer (TREC) initiative has supported progress in this area. For example, diet and weight loss trials in cancer survivors include the largest NCI-funded, multicenter weight loss trial in overweight or obese breast cancer survivors. At 12 months, the mean weight loss was 6.0% in the intervention group versus 1.5% in the control group (P < 0.001; ref. 249). Analyses of NHANES data found that the frequency and timing of meals influenced breast cancer risk biomarkers in (250) TREC-funded proactive preclinical and a Women’s Healthy Eating and Living (WHEL) cohort studies (172), which found a highly significant benefit of time-restricted feeding (independent of total caloric intake) in breast cancer survivors. A sedentary lifestyle in breast cancer survivors in the WHEL study was related to a 22% increased risk of breast cancer mortality (251).
Future opportunities in cancer prevention: summary.
Sensitive assessments of cancer susceptibility and risk together with tailored preventive interventions will enable precise molecularly targeted cancer prevention. With the decreasing cost of germline genetic testing (both physician ordered and direct to consumer panels), we will increasingly identify those at inherited predisposition to various cancers, providing a population ripe for cancer interception (252). Hereditary cancer predisposition germline mutations can be identified accurately from cell-free DNA (253).
Promotion of greater public and professional awareness of the evolution and risk of preneoplasia development and progression will improve understanding of cancer development and the time course and complexity of carcinogenesis. Short-term risks in different germline settings are critical to trial designs and available on the ask2me.org website.
Research should focus on the biology of premalignancy, the molecular aberrations and pathways of precancer initiation and progression to invasion, and the biologic processes that sustain normalcy and nonprogression.
Epidemiology of precancer, cancer, and cancer-related mortality provides clinicians with an opportunity to understand cancer etiologies, although data on population-wide behaviors relevant to cancer initiation and development are rarely collected.
Exposome technologies can be applied to better understand environmental causes and mechanisms of carcinogenesis.
Primary cancer prevention can be improved through use of evidence-based interventions developed in a manner concordant with the Institute of Medicine’s STEEEP criteria.
A PCA involving molecular characterization of precancerous lesions will illuminate the process of cancer initiation and preinvasive progression, elucidating “field effects” and the timing and role of heterogeneity in early lesions. The Beau Biden Moonshot has funded such PCA efforts in lung, colon, breast, melanoma, and in hematologic malignancies (clonal hematopoiesis) and this will undoubtedly lead to important insights.
Established therapeutic agents can be repurposed and directed against precancers, advancing interception. Agents so identified include tamoxifen, raloxifene, aromatase inhibitors, and 5-fluorouracil.
Tertiary prevention will depend on enhanced infrastructure in support of behavioral interventions among survivors, including the lifestyle changes that may mitigate risk of secondary cancers.
Cross-Cutting Issues in Cancer Prevention
Cancer health disparities were identified as among the most pressing issues in cancer prevention. Disparities influence every aspect of the cancer care continuum, from prevention and screening, through diagnosis and treatment, and to survivorship and end-of-life care (254, 255). Racial and ethnic minority groups continue to be underrepresented in biomedical research and clinical trials, and malignancies that disproportionately affect these groups remain understudied. Disparities may be exacerbated by uneven access to scientific and technological advancements. For example, the burden of head and neck cancer is greater for blacks than for whites, driven by a striking interaction between oropharyngeal cancer, race, and HPV (256). HCC is the second most common cause of cancer-related death in U.S. Hispanic men, who also have the highest rate of HCC precursor (NASH) lesions; the burden of hepatic neoplasia in Hispanics is tightly linked to obesity. In the national Hispanic Community Health Study/Study of Latinos focusing solely on Hispanics, the strongest predictor of moderate and extreme obesity was length of residency in mainland US, rather than acculturation (257).
According to the NCI, disparities are “adverse differences in cancer incidence, prevalence, death, survivorship, and burden of cancer or related health conditions that exist among specific population groups in the United States.” The Institute of Medicine distinguishes a disparity from a difference, stating that “a disparity is not just a difference in outcomes, but an inequity in outcomes that results from inequitable distribution of or access to resources that promote good health . . . a difference may become a disparity” (258). Successfully addressing disparities will require proportional resource distribution founded on baseline need to ensure greater equity.
Disparities exist in cancer incidence, mortality, and survival when populations groups are compared by gender, race, ethnicity, and socioeconomic status, disability, geographic location, and sexual identity. However, too often disparities are viewed through a limited set of only these variables, which limits our understanding and consideration of potential solutions. For example, overemphasis solely on race and ethnicity as determinants of cancer health disparities without considering other important measures provides an incomplete picture. An emerging concept, termed social determinants of health, considers conditions in the places where individuals live, learn, work, and play as determinants of health risks and outcomes. An excellent and detailed model for considering disparities in cancer development, care, and outcomes has been put forth by Warnecke and colleagues (254). The model considers the social determinants of health, as well as individual demographics, risk behaviors, and biological factors. This and other similar models that consider social determinants of health have the potential to improve health outcomes at the individual and population level as well as improve health equity. For example, an individual’s zip code has been proposed as an essential new “vital sign,” as residential location can be a strong determinant of cancer risk and outcomes (259). A virtuous cycle of research and cancer control actions relevant across diverse countries and contexts could enable more rapid, efficient, and cost-effective discoveries and implementation strategies in multiple settings.
To address disparities, we must improve the delivery of evidence-based interventions that follow the IOM’s STEEEPS criteria for quality care (i.e., care that is safe, timely, efficacious, efficient, equitably distributed, patient-centered, and sustainable; ref. 260). STEEEPS criteria should pertain to all interventions within all population subsets.
Cancer prevention and screening efforts have improved but have not been equitably distributed; many groups have been left behind. Although it is reassuring that cancer health disparities are part of the National Cancer Moonshot plan, there are still many actions that the federal government needs to implement to address cancer health disparities. Such actions include creating a national cancer control plan, appointing a national leader to organize and coordinate committed partners, and increasing funding of both prevention research and evidence-based cancer control actions. In addition, prioritizing research funding to address cancer disparities by utilizing the Cancer Moonshot initiative as a model should be considered (1). Prevention of any disease can occur at two basic levels: (i) avoiding or reducing risk factors coupled with increases in protective factors (primary prevention) and (ii) detection and intervention early in the course of disease evolution (in the cancer field is referred to as cancer interception).
Top Five Priority Recommendations
At the conclusion of the Summit and in response to a challenge advanced by the AACR President-Elect, Dr. Nancy E. Davidson and the NCI Director (ad interim), Dr. Douglas R. Lowy, the participants advanced five priority recommendations based on the prior two days of presentations and discussions. These priorities included four aspects of prevention research and the endorsement of population-wide cancer control, as follows:
Prevention research
Precancer Atlas;
Obesity research to develop interventions and understand cancer-related mechanisms;
Preventive applications of immune- and targeted therapies; and
Development of approaches to overcome inequities and reach all populations in need.
Evidence-based cancer control actions
Implementation of comprehensive, evidence-based interventions to advance the delivery of preventive and screening services, public and professional education, health behavior interventions, and public policies in the general population and high-risk subsets, including cancer survivors. Such actions must overcome inequities.
The hope is that these five recommendations will provide an organizing framework for the field of cancer prevention. This roadmap can unify a field that consists of, and is influenced by, numerous disciplines. Population, basic and clinical contexts now enable an enhanced focus on prevention research. Vogelstein’s recent “Policy Forum” piece in Science elegantly articulated the major global impact of cancer prevention and the challenges, discussed above, and included the predominant disconnect between the critical importance of cancer prevention to reduce mortality, yet this field receives limited support, estimated to be <10% of global cancer research funding. Connecting epidemiologic and molecular perspectives is critical to inform cancer research and prevention strategies (261). For example, obesity is increasing globally at alarming rates, yet we have limited understanding of what drives the obesity-cancer connection. Adipose tissue is a source of mesenchymal stem cells, create suppressive microenvironmental effects, and may promote cancer development by influencing gene expression through reversible epigenetic mechanisms. High-protein diet can reduce beneficial microbiota and metabolites, downregulating immune protection. High-fat diet was found to induce intestinal progenitor cells to adopt a more stem cell-like fate, increasing tumor incidence, caused by certain fatty acids in the diet. In contrast, calorie restriction has the opposite effect, associated with reduced tumor initiation. GWAS data first identified the critical importance of the 1p31.3 locus, which brought attention to the IL-23/IL-17 axis and ultimately led to development of several FDA-approved psoriasis drugs that specifically target IL-17 critical to cancer development and prevention, including microbiome-induced colorectal cancer. Another example of the value of connecting epidemiologic and molecular prespectives is illustrated by the empiric observation that African Americans have poorer response to interferon-based strategies for hepatitis C – only later, with the identification of polymorphisms in interleukin (IL)-28B, was the mechanistic basis for this observation clarified.
The generation of mutations in ostensibly healthy cells from eyelid to esophageal normal epithelia could be important in the pathogenesis of other chronic diseases of aging, such as diabetes, heart disease, and neurodegenerative disorders. This phenomena has been observed in some other sites (e.g., skin, BRAF-mutant moles), where clones are to a point where they become stable, until epigenetic reprogramming or some other event promotes transformation. The NOTCH1 mutation data in this context is striking and suggests the predominance in normal tissue may be due to tissue context (e.g., mutation order, and basic mechanisms that underlie differences in mutational and clonal expansion rates) or perhaps the normal cells acquire NOTCH 1 mutations to protect/prevent transformation possibly via mutation-induced immunity.
In the last five years, the AACR has begun to emphasize the importance of cancer control, supporting initiatives in the policy arena. The AACR has subcommittees on health policy, tobacco and cancer (e.g., AACR’s Tobacco and Cancer Subcommittee special report, a comprehensive statement urging immediate action to reduce tobacco use), and supports public education with the production of Cancer Today. The AACR is poised to continue, expand and accelerate advances related to all five of the priority recommendations both nationally and globally.
Acknowledgments
The authors wish to thank Michael J. Powell, PhD, Leona Flores, PhD, and Jocelyn V. Wainwright, MS for their significant contributions to the creation of this manuscript.
Footnotes
Disclosure of Potential Conflicts of Interest
M.L. Disis reports receiving commercial research grants from EpiThany, Celgene, Seattle Genetics, Silverback Therapeutics, EMD Serono, Pfizer, and Janssen Research & Development, LLC and has ownership interest in EpiThany and the University of Washington. R.N. DuBois is a consultant/advisory board member for SU2C, Robert J. Kleberg, Jr. and Helen C. Kleberg Foundation, AACR, and the German Cancer Research Center (DKFZ). A.R. Giuliano reports that her primary employer (Moffit Cancer Center) receives commercial research grant support from Merck & Co.; she receives honoraria from and serves as a consultant/advisory board member for the same. P. Limburg serves as co-Chief Medical Officer for Exact Sciences through a contracted services agreement with Mayo Clinic; he and Mayo Clinic receive royalties from Exact Sciences through this agreement. E. Vilar-Sanchez is a consultant/advisory board member for Janssen Research & Development, LLC. No potential conflicts of interest were disclosed by the other authors.
References
- 1.Martínez ME, Paskett ED. Using the Cancer Moonshot to Conquer Cancer Disparities: A Model for Action. JAMA Oncol 2018;4:624–25. [DOI] [PubMed] [Google Scholar]
- 2.Polite BN, Adams-Campbell LL, Brawley OW, Bickell N, Carethers JM, Flowers CR, et al. Charting the Future of Cancer Health Disparities Research: A Position Statement from the American Association for Cancer Research, the American Cancer Society, the American Society of Clinical Oncology, and the National Cancer Institute. Cancer Res 2017;77:4548–55. [DOI] [PubMed] [Google Scholar]
- 3.Blackburn EH. Cancer interception. Cancer Prev Res 2011;4:787–92. [DOI] [PubMed] [Google Scholar]
- 4.Emmons KM, Colditz GA. Realizing the potential of cancer prevention - the role of implementation science. N Engl J Med 2017;376:986–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Colditz GA, Wolin KY, Gehlert S. Applying what we know to accelerate cancer prevention. Sci Transl Med 2012; 4:127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jaffee EM, Dang CV, Agus DB, Alexander BM, Anderson KC, Ashworth A, et al. Future cancer research priorities in the USA: a Lancet Oncology Commission. Lancet Oncol 2017;18:e653–e706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Doll R, Peto R. The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. J Natl Cancer Inst 1981;66:1191–308. [PubMed] [Google Scholar]
- 8.Spira A, Yurgelun MB, Alexandrov L, Rao A, Bejar R, Polyak K, et al. Precancer atlas to drive precision prevention trials. Cancer Res 2017;77:1510–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Edwards BK,Howe HL, Ries LA,Thun MJ, Rosenberg HM, Yancik R, et al. Annual report to the nation on the status of cancer, 1973–1999, featuring implications of age and aging on U.S. cancer burden. Cancer 2002;94:2766–92. [DOI] [PubMed] [Google Scholar]
- 10.Kerr J, Anderson C, Lippman SM. Physical activity, sedentary behaviour, diet, and cancer: an update and emerging new evidence. Lancet Oncol 2017;18:e457–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Diehl AM, Day C. Cause, pathogenesis, and treatment of nonalcoholic steatohepatitis. N Engl J Med 2017;377: 2063–72. [DOI] [PubMed] [Google Scholar]
- 12.Koh HK, Sebelius KG. Promoting prevention through the Affordable Care Act. N Engl J Med 2010;363:1296–9. [DOI] [PubMed] [Google Scholar]
- 13.Kelloff GJ, Lippman SM, Dannenberg AJ, Sigman CC, Pearce HL, Reid BJ, et al. Progress in chemoprevention drug development: the promise of molecular biomarkers for prevention of intraepithelial neoplasia and cancer–a plan to move forward. Clin Cancer Res 2006;12:3661–97. [DOI] [PubMed] [Google Scholar]
- 14.Colditz GA, Taylor PR. Prevention trials: their place in how we understand the value of prevention strategies. Annu Rev Public Health 2010;31:105–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Khoury MJ, Gwinn M, Yoon PW, Dowling N, Moore CA, Bradley L. The continuum of translation research in genomic medicine: how can we accelerate the appropriate integration of human genome discoveries into health care and disease prevention? Genet Med 2007;9:665–74. [DOI] [PubMed] [Google Scholar]
- 16.Blumberg RS, Dittel B, Hafler D, von Herrath M, Nestle FO. Unraveling the autoimmune translational research process layer by layer. Nat Med 2012;18:35–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hudson KL, Collins FS. The 21st Century Cures Act - A View from the NIH. N Engl J Med 2017;376:111–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Arredondo EM, Elder JP, Haughton J, Slymen DJ, Sallis JF, Perez LG, et al. Fe en acción: promoting physical activity among churchgoing latinas. Am J Public Health 2017;107: 1109–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McCaskill-Stevens W, Pearson DC, Kramer BS, Ford LG, Lippman SM. Identifying and creating the next generation of community-based cancer prevention studies: summary of a National Cancer Institute Think Tank. Cancer Prev Res 2017; 10:99–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kato S, Lippman SM, Flaherty KT, Kurzrock R. The conundrum of genetic “drivers” in benign conditions. J Natl Cancer Inst 2016;108:djw036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Herbst RS, Heymach JV, Lippman SM. Lung cancer. N Engl J Med2008;359:1367–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Maitra A, Hruban RH. Pancreatic cancer. Annu Rev Pathol2008;3:157–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Makohon-Moore AP, Matsukuma K, Zhang M, Reiter JG, Gerold JM, Jiao Y, et al. Precancerous neoplastic cells can move through the pancreatic ductal system. Nature 2018;561:201–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kopp JL, Dubois CL, Schaeffer DF, Samani A, Taghizadeh F, Cowan RW, et al. Loss of Pten and activation of Kras synergistically induce formation of intraductal papillary mucinous neoplasia from pancreatic ductal cells in mice. Gastroenterology 23–154:1509;2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Patra KC, Kato Y, Mizukami Y, Widholz S, Boukhali M, Revenco I, et al. Mutant GNAS drives pancreatic tumourigenesis by inducing PKA-mediated SIK suppression and reprogramming lipid metabolism. Nat Cell Biol 2018;20:811–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ideno N, Yamaguchi H, Ghosh B, Gupta S, Okumura T, Steffen DJ, et al. GNASR201C induces pancreatic cystic neoplasms in mice that express activated KRAS by inhibiting YAP1 signaling. Gastroenterology 2018;155:1593–607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hu C, Hart SN, Polley EC, Gnanaolivu R, Shimelis H, Lee KY, et al. Association between inherited germline mutations in cancer predisposition genes and risk of pancreatic cancer. JAMA 2018;319:2401–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yurgelun MB, Chittenden AB, Morales-Oyarvide V, Rubinson DA, Dunne RF, Kozak MM, et al. Germline cancer susceptibility gene variants, somatic second hits, and survival outcomes in patients with resected pancreatic cancer. Genet Med 2018. Jul 2. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Shindo K, Yu J, Suenaga M,Fesharakizadeh S, Cho C, Macgregor-Das A, et al. Deleterious germline mutations in patients with apparently sporadic pancreatic adenocarcinoma. J Clin Oncol 2017;35:3382–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bannon SA, Montiel MF, Goldstein JB, Dong W, Mork ME, Borras E, et al. High prevalence of hereditary cancer syndromes and outcomes in adults with early-onset pancreatic cancer. Cancer Prev Res 2018;11:679–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Syngal S, Furniss CS. Germline genetic testing for pancreatic ductal adenocarcinoma at time of diagnosis. JAMA 2018;319: 2383–5. [DOI] [PubMed] [Google Scholar]
- 32.Stoffel EM, McKernin SE, Brand R, Canto M, Goggins M, Moravek C, et al. Evaluating Susceptibility to Pancreatic Cancer: ASCO Provisional Clinical Opinion. J Clin Oncol 2018. Nov 20: JCO1801489. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 33.Beane J, Campbell JD, Lel J, Vick J, Spira A. Genomic approaches to accelerate cancer interception. Lancet Oncol 2017;18:e494–e502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Yurgelun MB, Chenevix-Trench G, Lippman SM. Translating germline cancer risk into precision prevention. Cell 2017;168: 566–70. [DOI] [PubMed] [Google Scholar]
- 35.Liao X, Lochhead P, Nishihara R, Morikawa T, Kuchiba A, Yamauchi M, et al. Aspirin use, tumor PIK3CA mutation, and colorectal-cancer survival. N Engl J Med 2012;367:1596–606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Liu W, Poole EM, Ulrich CM, Kulmacz RJ. Decreased cyclooxygenase inhibition by aspirin in polymorphic variants of human prostaglandin H synthase-1. Pharmacogenet Genomics 2012; 22:525–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rebbeck TR. Precision prevention of cancer. Cancer Epidemiol Biomarkers Prev 2014;23:2713–5. [DOI] [PubMed] [Google Scholar]
- 38.Davoli T, Uno H, Wooten EC, Elledge SJ. Tumor aneuploidy correlates with markers of immune evasion and with reduced response to immunotherapy. Science 2017;355:6322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Li X, Paulson TG, Galipeau PC, Sanchez CA, Liu K, Kuhner MK, et al. Assessment of esophageal adenocarcinoma risk using somatic chromosome alterations in longitudinal samples in barrett’s esophagus. Cancer Prev Res 2015;8:845–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Maricic I, Marrero I, Eguchi A, Nakamura R, Johnson CD, Dasgupta S, et al. Differential activation of hepatic invariant NKT cell subsets plays a key role in progression of nonalcoholic steatohepatitis. J Immunol 2018;201:3017–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ma C, Kesarwala AH, Eggert T, Medina-Echeverz J, Kleiner DE, Jin P, et al. NAFLD causes selective CD4(+) T lymphocyte loss and promotes hepatocarcinogenesis. Nature 2016;531: 253–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Shalapour S, Lin XJ, Bastian IN, Brain J, Burt AD, Aksenov AA, et al. Inflammation-induced IgA+ cells dismantle anti-liver cancer immunity. Nature 2017;551:340–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lee J, Liao R, Wang G, Yang BH, Luo X, Varki NM, et al. Preventive inhibition of liver tumorigenesis by systemic activation of innate immune functions. Cell Rep 2017;21: 1870–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kaneda MM, Cappello P, Nguyen AV, Ralainirina N, Hardamon CR, Foubert P, et al. Macrophage PI3Kγ drives pancreatic ductal adenocarcinoma progression. Cancer Discov 2016;6:870–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bernard V, Semaan A, Huang J, San Lucas FA, Mulu FC, Stephens BM, et al. Single cell transcriptomics of pancreatic cancer precursors demonstrates epithelial and microenvironmental heterogeneity as an early event in neoplastic progression. Clin Cancer Res 2018. Nov 1 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ridker PM, MacFadyen JG, Thuren T, Everett BM, Libby P, Glynn RJ et al. Effect of interleukin-1binhibition with canakinumab on incident lung cancer in patients with atherosclerosis: exploratory results from a randomised, double-blind, placebo-controlled trial. Lancet 2017;390:1833–42. [DOI] [PubMed] [Google Scholar]
- 47.Lee CH, Chang JS, Syu SH, Wong TS, Chan JY, Tang YC, et al. IL-1β promotes malignant transformation and tumor aggressiveness in oral cancer. J Cell Physiol 2015;230:875–84. [DOI] [PubMed] [Google Scholar]
- 48.Incio J, Suboj P, Chin SM, Vardam-Kaur T, Liu H, Hato T, et al. Metformin Reduces Desmoplasia in Pancreatic Cancer by Reprogramming Stellate Cells and Tumor-Associated Macrophages. PLoS One 2015;10:e0141392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mantovani A The inflammation - cancer connection FEBS J 2018;285:638–640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Guo B, Fu S, Zhang J, Liu B, Li Z. Targeting inflammasome/IL-1 pathways for cancer immunotherapy. Sci Rep 2016;6:36107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kurzrock R, Voorhees PM, Casper C, Furman RR, Fayad L, Lonial S, et al. A phase I, open-label study of siltuximab, an anti-IL-6 monoclonal antibody, in patients with B-cell non-Hodgkin lymphoma, multiple myeloma, or Castleman disease. Clin Cancer Res 2013;19:3659–70. [DOI] [PubMed] [Google Scholar]
- 52.Beatty PL, Narayanan S, Gariépy J, Ranganathan S, Finn OJ. Vaccine against MUC1 antigen expressed in inflammatory bowel disease and cancer lessens colonic inflammation and prevents progression to colitis-associated colon cancer. Cancer Prev Res 2010;3:438–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Disis ML, Gad E, Herendeen DR, Lai VP, Park KH, Cecil DL, et al. A multiantigen vaccine targeting neu, IGFBP-2, and IGF-IR prevents tumor progression in mice with preinvasive breast disease. Cancer Prev Res (Phila) 2013;6:1273–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Keenan BP, Saenger Y, Kafrouni MI, Leubner A, Lauer P, Maitra A, et al. A Listeria vaccine and depletion of T-regulatory cells activate immunity against early stage pancreatic intraepithelial neoplasms and prolong survival of mice. Gastroenterology 2014;146:1784–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Marquez JP, Stanton SE, Disis ML. The antigenic repertoire of premalignant and high-risk lesions. Cancer Prev Res 2015; 8:266–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Loo TM, Kamachi F, Watanabe Y, Yoshimoto S, Kanda H, Arai Y, et al. Gut microbiota promotes obesity-associated liver cancer through PGE2-Mediated suppression of antitumor immunity. Cancer Discov 2017;7:522–38. [DOI] [PubMed] [Google Scholar]
- 57.Rajagopala SV, Vashee S, Oldfield LM, Suzuki Y, Venter JC, Telenti A, et al. The human microbiome and cancer. Cancer Prev Res 2017;10:226–34. [DOI] [PubMed] [Google Scholar]
- 58.Loomba R, Seguritan V, Li W, Long T, Klitgord N, Bhatt A, et al. Gut microbiome-based metagenomic signature for non-invasive detection of advanced fibrosis in human nonalcoholic fatty liver disease. Cell Metab 2017;25:1054–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Dejea CM, Fathi P, Craig JM, Boleij A, Taddese R, Geis AL, et al. Patients with familial adenomatous polyposis harbor colonic biofilms containing tumorigenic bacteria. Science 2018;359: 592–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Pushalkar S, Hundeyin M, Daley D, Zambirinis CP, Kurz E, Mishra A, et al. The pancreatic cancer microbiome promotes oncogenesis by induction of innate and adaptive immune suppression. Cancer Discov 2018;8:403–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Thaiss CA, Zmora N, Levy M, Elinav E. The microbiome and innate immunity. Nature 2016;535:65–74. [DOI] [PubMed] [Google Scholar]
- 62.Sethi V, Kurtom S, Tarique M, Lavania S, Malchiodi Z, Hellmund L, et al. Gut microbiota promotes tumor growth in mice by modulating immune response. Gastroenterology 2018;155:33–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Biragyn A, Ferrucci L. Gut dysbiosis: a potential link between increased cancer risk in ageing and inflammaging. Lancet Oncol 2018;19:e295–e304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Marty R, Thompson WK, Salem RM, Zanetti M, Carter H. Evolutionary pressure against MHC class II binding cancer mutations. Cell 2018;175:416–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Marty R, Kaabinejadian S, Rossell D, Slifker MJ, van de Haar J, Engin HB, et al. MHC-I Genotype restricts the oncogenic mutational landscape. Cell 2017;171:1272–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Izumchenko E, Chang X, Brait M, Fertig E, Kagohara LT, Bedi A, et al. Targeted sequencing reveals clonal genetic changes in the progression of early lung neoplasms and paired circulating DNA. Nat Commun 2015;6:8258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Corcoran RB, Chabner BA. Application of cell-free DNA analysis to cancer treatment. N Engl J Med 2018;379:1754–65. [DOI] [PubMed] [Google Scholar]
- 68.Rahbari M, Rahbari N, Reissfelder C, Weitz J, Kahlert C. Exosomes: novel implications in diagnosis and treatment of gastrointestinal cancer. Langenbecks Arch Surg 2016;401: 1097–110. [DOI] [PubMed] [Google Scholar]
- 69.Heitzer E, Perakis S, Geigl JB, Speicher MR. The potential of liquid biopsies for the early detection of cancer. NPJ Precis Oncol 2017;1:36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Young AL, Challen GA, Birmann BM, Druley TE. Clonal haematopoiesis harbouring AML-associated mutations is ubiquitous in healthy adults. Nat Commun 2016;7:12484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Cohen JD, Li L, Wang Y, Thoburn C, Afsari B, Danilova L, et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018;359:926–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Xu RH, Wei W, Krawczyk M, Wang W, Luo H, Flagg K, et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat Mater 2017;16: 1155–61. [DOI] [PubMed] [Google Scholar]
- 73.Shen SY, Singhania R, Fehringer G, Chakravarthy A, Roehrl MHA, Chadwick D, et al. Sensitive tumour detection and classification using plasma cell-free DNA methylomes. Nature 2018;563:579–83. [DOI] [PubMed] [Google Scholar]
- 74.Kaufman CK, Mosimann C, Fan ZP, Yang S, Thomas AJ, Ablain J, et al. A zebrafish melanoma model reveals emergence of neural crest identity during melanoma initiation. Science 2016;351: aad2197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Fox RG, Lytle NK, Jaquish DV, Park FD, Ito T, Bajaj J, et al. Image-based detection and targeting of therapy resistance in pancreatic adenocarcinoma. Nature 2016;534:407–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Nolan E, Vaillant F, Branstetter D, Pal B, Giner G, Whitehead L, et al. RANK ligand as a potential target for breast cancer prevention in BRCA1- mutation carriers. Nat Med 2016;22: 933–9. [DOI] [PubMed] [Google Scholar]
- 77.Sau A, Lau R, Cabrita MA, Nolan E, Crooks PA, Visvader JE, et al. Persistent activation of NF-kappaB in BRCA1-deficient mammary progenitors drives aberrant proliferation and accumulation of DNA damage. Cell Stem Cell 2016;19:52–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Nolan E, Lindeman GJ, Visvader JE. Out-RANKing BRCA1 in mutation carriers. Cancer Res 2017;77:595–600. [DOI] [PubMed] [Google Scholar]
- 79.Grinfeld J, Nangalia J, Baxter EJ, Wedge DC, Angelopoulos N, Cantrill R, et al. Classification and personalized prognosis in myeloproliferative neoplasms. N Engl J Med 2018;379: 1416–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Zipeto MA, Court AC, Sadarangani A, Delos Santos NP, Balaian L, Chun HJ, et al. ADAR1 activation drives leukemia stem cell self-renewal by impairing Let-7 biogenesis. Cell Stem Cell 2016;19:177–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Hinds DA, Barnholt KE, Mesa RA, Kiefer AK, Do CB, Eriksson N, et al. Germ line variants predispose to both JAK2 V617F clonal hematopoiesis and myeloproliferative neoplasms. Blood 2016; 128:1121–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Churpek JE, Pyrtel K, Kanchi KL, Shao J, Koboldt D, Miller CA, et al. Genomic analysis of germ line and somatic variants in familial myelo- dysplasia/acute myeloid leukemia. Blood 2015;126:2484–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Chen L, Li Y, Lin CH, Chan TH, Chow RK, Song Y, et al. Recoding RNA editing of AZIN1 predisposes to hepatocellular carcinoma. Nat Med 2013;19:209–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Beyaz S, Mana MD, Roper J, Kedrin D, Saadatpour A, Hong SJ, et al. High-fat diet enhances stemness and tumorigenicity of intestinal pro- genitors. Nature 2016;531:53–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Dhodapkar MV, Sexton R, Das R, Dhodapkar KM, Zhang L, Sundaram R, et al. Prospective analysis of antigen-specific immunity, stem-cell antigens, and immune checkpoints in monoclonal gammopathy. Blood 2015;126:2475–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Vogelstein B, Fearon ER, Hamilton SR, Kern SE, Preisinger AC, Leppert M, et al. Genetic alterations during colorectal-tumor development. N Engl J Med 1988;319:525–32. [DOI] [PubMed] [Google Scholar]
- 87.Borras E, San Lucas FA, Chang K, Zhou R, Masand G, Fowler J, et al. Genomic landscape of colorectal mucosa and adenomas. Cancer Prev Res 2016;9:417–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Zeuner A, Todaro M, Stassi G,DeMaria R. Colorectal cancer stem cells: from the crypt to the clinic. Cell Stem Cell 2014;15: 692–705. [DOI] [PubMed] [Google Scholar]
- 89.Sievers CK, Zou LS, Pickhardt PJ, Matkowskyj KA, Albrecht DM, Clipson L, et al. Subclonal diversity arises early even in small colorectal tumours and contributes to differential growth fates. Gut 2017;66:2132–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Druliner BR, Wang P, Bae T, Baheti S, Slettedahl S, Mahoney D, et al. Molecular characterization of colorectal adenomas with and without malignancy reveals distinguishing genome, transcriptome and methylome alterations. Sci Rep 2018;8:3161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Jasperson KW, Tuohy TM, Neklason DW, Burt RW. Hereditary and familial colon cancer. Gastroenterology 2010;138: 2044–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Fearon ER. Molecular genetics of colorectal cancer. Annu Rev Pathol 2011;6:479–507 [DOI] [PubMed] [Google Scholar]
- 93.Rashid M, Fischer A, Wilson CH, Tiffen J, Rust AG, Stevens P, et al. Adenoma development in familial adenomatous polyposis and MUTYH-associated polyposis: somatic landscape and driver genes. J Pathol 2016;238:98–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Katona BW, Yurgelun MB, Garber JE, Offit K, Domchek SM, Robson ME, et al. A counseling framework for moderate-penetrance colorectal cancer susceptibility genes. Genet Med 2018. Mar 1. Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 95.Vilar E, Tabernero J. Molecular dissection of microsatellite instable colorectal cancer. Cancer Discov 2013;3:502–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Chang K, Willis JA, Reumers J, Taggart MW, San Lucas FA, Thirumurthi S, et al. Colorectal premalignancy is associated with consensus molecular subtypes 1 and 2. Ann Oncol 2018; 29:2061–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Woerner SM, Yuan YP, Benner A, Korff S, von Knebel Doeberitz M, Bork P. SelTarbase, a database of human mononucleotide-microsatellite mutations and their potential impact to tumorigenesis and immunology. Nucleic Acids Res 2010;38(Database issue):D682–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Schwitalle Y, Kloor M, Eiermann S, Linnebacher M, Kienle P, Knaebel HP, et al. Immune response against frameshift-induced neopeptides in HNPCC patients and healthy HNPCC mutation carriers. Gastroenterology 2008;134:988–97. [DOI] [PubMed] [Google Scholar]
- 99.Echterdiek F, Janikovits J, Staffa L, Muller M, Lahrmann B, Fruhschutz M, et al. Low density of FOXP3-positive T cells in normal colonic mucosa is related to the presence of beta2-micro- globulin mutations in Lynch syndrome-associated colorectal cancer. Oncoimmunology 2016;5:e1075692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Kloor M, von Knebel Doeberitz M. The immune biology of microsatellite-unstable cancer. Trends Cancer 2016;2:121–33. [DOI] [PubMed] [Google Scholar]
- 101.Leoni G, D’Alise AM, Cotugno G, Mori F, Catanese MT, Langone F, et al. (Abstract) A viral vectored vaccine based on shared tumor neoantigens for prevention and treatment of microsatellite instable (MSI) cancers. J Immunother Cancer 2017;5:86. [Google Scholar]
- 102.Guinney J, Dienstmann R, Wang X, de Reyniès A, Schlicker A, Soneson C, et al. The consensus molecular subtypes of colorectal of cancer. Nat Med 2015;21:1350–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Drew DA, Cao Y, Chan AT. Aspirin and colorectal cancer: the promise of precision chemoprevention. Nat Rev Cancer 2016; 16:173–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Samadder NJ, Neklason DW, Boucher KM, Byrne KR, Kanth P, Samowitz W, et al. Effect of sulindac and erlotinib vs placebo on duodenal neoplasia in familial adenomatous polyposis: a randomized clinical trial. JAMA 2016;315:1266–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Lynch PM, Burke CA, Phillips R, Morris JS, Slack R, Wang X, et al. An international randomised trial of celecoxib versus celecoxib plus difluoromethylornithine in patients with familial adenomatous polyposis. Gut 2016;65:286–95. [DOI] [PubMed] [Google Scholar]
- 106.Delker DA, Wood AC, Snow AK, Samadder NJ, Samowitz WS, Affolter KE, et al. Chemoprevention with cyclooxygenase and epidermal growth factor receptor inhibitors in familial adenomatous polyposis patients: mRNA signatures of duodenal neoplasia. Cancer Prev Res 2018;11:4–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Rice PFS, Ehrichs KG, Jones MS, Chen H, Hsu CH, Abril ER, et al. Does Mutated K-RAS Oncogene Attenuate the Effect of Sulindac in Colon Cancer Chemoprevention? Cancer Prev Res 2018;11: 16–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Hampel H, Pearlman R, Beightol M, Zhao W, Jones D, Frankel WL, et al. Assessment of Tumor Sequencing as a Replacement for Lynch Syndrome Screening and Current Molecular Tests for Patients With Colorectal Cancer. JAMA Oncol 2018;4:806–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Le DT, Durham JN, Smith KN, Wang H, Bartlett BR, Aulakh LK, et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017;357:409–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Jenkins MA, Dowty JG, Ait Ouakrim D, Mathews JD, Hopper JL, Drouet Y, et al. Short-term risk of colorectal cancer in individuals with lynch syndrome: a meta-analysis. J Clin Oncol 2015;33: 326–31. [DOI] [PubMed] [Google Scholar]
- 111.Guindalini RS, Win AK, Gulden C, Lindor NM, Newcomb PA, Haile RW, et al. Mutation spectrum and risk of colorectal cancer in African American families with Lynch syndrome. Gastroenterology 2015;149:1446–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SA, Behjati S, Biankin AV, et al. Signatures of mutational processes in human cancer. Nature 2013;500:415–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Alexandrov LB, Ju YS, Haase K, Van Loo P, Martincorena I, Nik-Zainal S, et al. Mutational signatures associated with tobacco smoking in human cancer. Science 2016;354:618–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Ng AWT, Poon SL, Huang MN, Lim JQ, Boot A, Yu W, et al. Aristolochic acids and their derivatives are widely implicated in liver cancers in Taiwan and throughout Asia. Sci Transl Med 2017;9:eaan6446. [DOI] [PubMed] [Google Scholar]
- 115.U.S. Department of Health and Human Services. The Health Consequences of Smoking: 50 Years of Progress. A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and 2946 Human Services; 2014. Available from: https://www.surgeongeneral.gov/library/reports/50-years-of-progress/full-report.pdf. [Google Scholar]
- 116.Eriksen M, Mackay J, Ross H. The Tobacco Atlas, 4th Ed. Atlanta, GA: The American Cancer Society; 2012. [Google Scholar]
- 117.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018;68:7–30. [DOI] [PubMed] [Google Scholar]
- 118.Koh HK, Sebelius KG. Ending the tobacco epidemic. JAMA 2012;308:767–8. [DOI] [PubMed] [Google Scholar]
- 119.Islami F, Goding Sauer A, Miller KD, Siegel RL, Fedewa SA, Jacobs EJ, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin 2018;68:31–54. [DOI] [PubMed] [Google Scholar]
- 120.Kushi L, Doyle C, McCullough M,Rock CL, Demark-Wahnefried W, Bandera EV, et al. American Cancer Society Guidelines on nutrition and physical activity for cancer prevention: reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin 2012;62:30–67. [DOI] [PubMed] [Google Scholar]
- 121.Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K, et al. Body fatness and cancer- viewpoint of the IARC working group. N Engl J Med 2016;375:794–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.AICR/WCRF. Policy Report and Continuous Update Project Reports. Washington, D.C.: AICR/WCRF. Available from: http://www.aicr.org/continuous-update-project/reports/colorectal-cancer-2017-report.pdf. [Google Scholar]
- 123.Ogden C, Carroll M, Kit B, Flegal K. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014;311: 806–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Schoenborn CA, Adams PF, Peregoy JA. Health behaviors of adults: United States, 2008–2010. Vital Health Stat 10; 2013. p. 1–184. [PubMed] [Google Scholar]
- 125.Fakhouri TH, Hughes JP, Brody DJ, Kit BK, Ogden CL. Physical activity and screen-time viewing among elementary school-aged children in the United States from 2009 to 2010. JAMA Pediatr 2013;167:223–9. [DOI] [PubMed] [Google Scholar]
- 126.Moore SC, Lee IM, Weiderpass E, Campbell PT, Sampson JN, Kitahara CM, et al. Association of leisure-time physical activity with risk of 26 types of cancer in 1.44 million adults. JAMA Intern Med 2016;176:816–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 2011; 43:1334–59. [DOI] [PubMed] [Google Scholar]
- 128.Sallis JF, Cerin E, Conway TL, Adams MA, Frank LD, Pratt M, et al. Physical activity in relation to urban environments in 14 cities worldwide: a cross-sectional study. Lancet 2016; 387: 2207–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Moore L, Thompson F. Adults Meeting Fruit and Vegetable Intake Recommendations - United States, 2013. MMWR Morb Mortal Wkly Rep 2015;64:709–13. [PMC free article] [PubMed] [Google Scholar]
- 130.WCRF/AICR. Food, nutrition, physical activity, and the prevention of cancer: a global perspective. Washington DC: AICR; 2007. [Google Scholar]
- 131.U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent Skin Cancer. Washington D.C.:U.S. Department of Health and Human Services; 2014. [Google Scholar]
- 132.Marks R Skin cancer control in the1990’s, from Slip! Slop! Slap! to sun smart. Australas J Dermatol 1990;31:1–4. [DOI] [PubMed] [Google Scholar]
- 133.Iannacone MR, Youlden DR, Baade PD, Aitken JF, Green AC. Melanoma incidence trends and survival in adolescents and young adults in Queensland, Australia. Int J Cancer 2015; 136:603–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Chang MH, Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS, et al. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N Engl J Med 1997;336:1855–9. [DOI] [PubMed] [Google Scholar]
- 135.Denniston MM, Klevens RM, McQuillan GM, Jiles RB. Awareness of infection, knowledge of hepatitis C, and medical follow-up among individuals testing positive for hepatitis C: National Health and Nutrition Examination Survey 2001–2008. Hepatology 2012;55:1652–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Afdhal N, Zeuzem S, Kwo P, Chojkier M, Gitlin N, Puoti M, et al. Ledipasvir and sofosbuvir for untreated HCV genotype 1 infection. N Engl J Med 2014;370:1889–98. [DOI] [PubMed] [Google Scholar]
- 137.President’s Cancer Panel. Accelerating HPV Vaccine Uptake: Urgency for Action to Prevent Cancer: A Report to the President of the United States from the President’s Cancer Panel. Bethesda, MD: National Cancer Institute; 2014. Available from: https://deainfo.nci.nih.gov/advisory/ncab/0214/2Rimer.pdf. [Google Scholar]
- 138.Hill HA, Elam-Evans LD, Yankey D, Singleton JA, Kolasa M. National, state, and selected local area vaccination coverage among children aged 19–35 months - United States, 2014. MMWR Morb Mortal Wkly Rep 2015;64:889–96. [DOI] [PubMed] [Google Scholar]
- 139.Hollstein M, Alexandrov LB, Wild CP, Ardin M, Zavadil J. Base changes in tumour DNA have the power to reveal the causes and evolution of cancer. Oncogene 2017;36:158–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Lichtenfeld JL. Cancer Facts and Figures, 2011: poverty is a carcinogen. does anyone care? Dr. Len’s blog: expert perspective, insight and discussion; 2011. Available from: http://blogs.cancer.org/drlen/2011/06/17/cancer-facts-and-figures-2011-poverty-is-a-carcinogen-does-anyone-care/ [Google Scholar]
- 141.Yang EC, Schwarz RA, Lang AK, Bass N, Badaoui H, Vohra IS, et al. In vivo multimodal optical imaging: improved detection of oral dysplasia in low-risk oral mucosal lesions. Cancer Prev Res 2018;11:465–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.National Lung Screening Trial Research Team, Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011;365:395–409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Silvestri GA, Vachani A, Whitney D, Elashoff M, Porta Smith K, Ferguson JS, et al. A bronchial genomic classifier for the diagnostic evaluation of lung cancer. N Engl J Med 2015; 373:243–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Lehman CD, Yala A, Schuster T, Dontchos B, Bahl M, Swanson K, et al. Mammographic breast density assessment using deep learning: clinical implementation. Radiology 2018;16:180694. [DOI] [PubMed] [Google Scholar]
- 145.U.S. Preventive Services Task Force. Draft recommendation statement: prostate cancer: screening. Available from: www.uspreventiveservicestaskforce.org/Page/Document/RecommendationsStatementDraft/prostate-cancer-screening1.
- 146.Lin JS, Piper MA, Perdue LA, Rutter C, Webber EM, O’Connor E, et al. Screening for colorectal cancer: a systematic review for the U.S. Preventive Services Task Force [Internet]. Rockville, MD: Agency for Healthcare Research and Quality (US); 2016. Available from: https://www.ncbi.nlm.nih.gov/books/NBK373584/. [PubMed] [Google Scholar]
- 147.Vesco KK, Whitlock EP, Eder M, Lin J, Burda BU, Senger CA, et al. Screening for cervical cancer: a systematic evidence review for the U.S. Preventive Services Task Force [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2011. Available from: https://www.ncbi.nlm.nih.gov/books/NBK66096/. [PubMed] [Google Scholar]
- 148.Nelson H, Cantor A, Humphrey L, Fu R, Pappas M, Daeges M, et al. Screening for breast cancer: a systematic review to update the 2009 U.S. Preventive Services Task Force Recommendation. Evidence Synthesis No. 124. Rockville, MD: Agency for Healthcare Research and Quality; 2016. [PubMed] [Google Scholar]
- 149.Humphrey L, Deffebach M, Pappas M, Baumann C, Artis K, Mitchell JP, et al. Screening for lung cancer: systematic review to update the U.S. Preventive Services Task Force Recommendation. Evidence Synthesis No. 105. Rockville, MD: Agency for Healthcare Research and Quality. Ann Intern Med; 2013;159:411–20. [PubMed] [Google Scholar]
- 150.Sporn MB. Approaches to prevention of epithelial cancer during the preneoplastic period. Cancer Res 1976;36:2699–702. [PubMed] [Google Scholar]
- 151.The Alpha-Tocopherol Beta Carotene Cancer Prevention Study Group. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. N Engl J Med 1994;330:1029–35. [DOI] [PubMed] [Google Scholar]
- 152.Lippman SM, Klein EA, Goodman PJ, Lucia MS, Thompson IM, Ford LG, et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2009;301:39–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Thompson IM, Goodman PJ, Tangen CM, Lucia MS, Miller GJ, Ford LG, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003;349:215–24. [DOI] [PubMed] [Google Scholar]
- 154.Thompson IM Jr, Goodman PJ, Tangen CM, Parnes HL, Minasian LM, Godley PA, et al. Long-term survival of participants in the prostate cancer prevention trial. N Engl J Med 2013;369: 603–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Vogel VG, Costantino JP, Wickerham DL, Cronin WM, Cecchini RS, Atkins JN, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes: the NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 trial. JAMA 2006;295:2727–41. [DOI] [PubMed] [Google Scholar]
- 156.Vogel VG, Costantino JP, Wickerham DL, Cronin WM, Cecchini RS, Atkins JN, et al. Update of the National Surgical Adjuvant Breast and Bowel Project Study of Tamoxifen and Raloxifene (STAR) P-2 Trial: Preventing breast cancer. Cancer Prev Res 2010;3:696–706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Tsay JJ, Wu BG. Airway Microbiota Is Associated with Upregulation of the PI3K Pathway in Lung Cancer. Am J Respir Crit Care Med 2018;198:1188–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Lam S, Mandrekar SJ, Gesthalter Y, Allen Ziegler KL, Seisler DK, Midthun DE, et al. A Randomized Phase IIb Trial of myoInositol in Smokers with Bronchial Dysplasia. Cancer Prev Res 2016;9:906–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Meyskens FL, McLaren CE, Pelot D, Fujikawa-Brooks S, Carpenter PM, Hawk E, et al. Difluoromethylornithine plus sulindac for the prevention of sporadic colorectal adenomas: a randomized placebo-controlled, double-blind trial. Cancer Prev Res 2008;1:32–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Bondi EE, Clark WH, Elder D, Guerry D, Greene MH. Topical chemotherapy of dysplastic melanocytic nevi with 5% fluorouracil. Arch Dermatol 1981;117:89–92. [PubMed] [Google Scholar]
- 161.Itoh H, Iida M, Mibu R, Terasaka R, Ohsato K. Local chemotherapy for rectal polyposis: intraluminal administration of 5-fluorouracil for postoperative control of adenomas in the retained rectum in familial polyposis. J Clin Gastroenterol 1989;11:645–9. [PubMed] [Google Scholar]
- 162.William WN Jr, Papadimitrakopoulou V, Lee JJ, Mao L, Cohen EE, Lin HY, et al. Erlotinib and the risk of oral cancer: the Erlotinib Prevention of Oral Cancer (EPOC) Randomized Clinical Trial. JAMA Oncol 2016;2:209–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Bauman JE, Grandis J. Oral cancer chemoprevention–the end of EPOC, the beginning of an epoch of molecular selection. JAMA Oncol 2016;2:178–9. [DOI] [PubMed] [Google Scholar]
- 164.Harrison SA, Rinella ME, Abdelmalek MF, Trotter JF, Paredes AH, Arnold HL, et al. NGM282 for treatment of non-alcoholic steatohepatitis: a multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2018;391:1174–85. [DOI] [PubMed] [Google Scholar]
- 165.Day TA, Shirai K, O’Brien PE, Matheus MG, Godwin KB, Sood AJ, et al. Inhibition of mTOR signaling and clinical activity of rapamycin in head and neck cancer in a window of opportunity trial. Clin Cancer Res 2018Nov 12 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Martin D, Degese MS, Vitale-Cross L, Iglesias-Bartolome R, Valera JLC, Wang Z, et al. Assembly and activation of the Hippo signalome by FAT1 tumor suppressor. Nat Commun 2018;9: 2372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167.Toll BA, Brandon TH, Gritz ER,Warren GW, Herbst RS. Assessing tobacco use by cancer patients and facilitating cessation: an American Association for Cancer Research policy statement. Clin Cancer Res 2013;19:1941–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168.Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvão DA, Pinto BM, et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc 2010;42:1409–26. [DOI] [PubMed] [Google Scholar]
- 169.Speck RM, Courneya KS, Mâsse LC, Duval S, Schmitz KH. An update of controlled physical activity trials in cancer survivors: a systematic review and meta-analysis. J Cancer Surviv 2010;4: 87–100. [DOI] [PubMed] [Google Scholar]
- 170.Friedenreich CM, Neilson HK, Farris MS, Courneya KS. Physical activity and cancer outcomes: a precision medicine approach. Clin Cancer Res 2016;22:4766–75. [DOI] [PubMed] [Google Scholar]
- 171.Rock CL, Doyle C, Demark-Wahnefried W, Meyerhardt J, Courneya KS, Schwartz AL, et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J Clin 2012;62: 243–74. [DOI] [PubMed] [Google Scholar]
- 172.Marinac CR, Nelson SH, Breen CI, Hartman SJ, Natarajan L, Pierce JP, et al. Prolonged nightly fasting and breast cancer prognosis. JAMA Oncol 2016;2:1049–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.Silver JK, Baima J, Mayer RS. Impairment-driven cancer rehabilitation: an essential component of quality care and survivorship. CA Cancer J Clin 2013;63:295–317. [DOI] [PubMed] [Google Scholar]
- 174.Schmitz KH, Neuhouser ML, Agurs-Collins T, Zanetti KA, Cadmus-Bertram L, Dean LT, et al. Impact of obesity on cancer survivorship and the potential relevance of race and ethnicity. J Natl Cancer Inst 2013;105:1344–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175.Walling EB, Benzoni N, Dornfeld J, Bhandari R, Sisk BA, Garbutt J, et al. Interventions to improve HPV vaccine uptake: a systematic review. Pediatrics 2016;138. [DOI] [PubMed] [Google Scholar]
- 176.Hait WN, Lebowitz PF. Disease interception: myths, mountains, and mole hills. Cancer Prev Res 2016;9:635–7. [DOI] [PubMed] [Google Scholar]
- 177.Saintigny P, William WN Jr, Foy JP, Papadimitrakopoulou V, Lang W, Zhang L, et al. Met receptor tyrosine kinase and chemoprevention of oral cancer. J Natl Cancer Inst 2018; 110:250–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Meyskens FL, Curt GA, Brenner DE, Gordon G, Herberman RB, Finn O, et al. Regulatory approval of cancer risk-reducing (chemopreventive) drugs: moving what we have learned into the clinic. Cancer Prev Res 2011;4:311–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.Mema SC,Yang H, Vaska M,Elnitsky S, Jiang Z. Integrated cancer screening performance indicators: a systematic review. PLoS One 2016;11: e0161187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180.Kohler LN, Garcia DO, Harris RB, Oren E, Roe DJ, Jacobs ET. Adherence to diet and physical activity cancer prevention guidelines and cancer outcomes: a systematic review. Cancer Epidemiol Biomarkers Prev 2016;25:1018–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell 1990;61:759–67. [DOI] [PubMed] [Google Scholar]
- 182.Maley CC, Galipeau PC, Finley JC, Wongsurawat VJ, Li X, Sanchez CA, et al. Genetic clonal diversity predicts progression to esophageal adenocarcinoma. Nat Genet 2006;38:468–73. [DOI] [PubMed] [Google Scholar]
- 183.Casasent AK, Schalck A, Gao R, Sei E, Long A, Pangburn W, et al. Multiclonal invasion in breast tumors identified by topographic single cell sequencing. Cell 2018;172:205–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184.Gausachs M, Borras E, Chang K, Gonzalez S, Azuara D, Delgado Amador A, et al. Mutational heterogeneity in APC and KRAS arises at the crypt level and leads to polyclonality in early colorectal tumorigenesis. Clin Cancer Res 2017;23:5936–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185.Vogelstein B, Papadopoulos N, Velculescu VE, Zhou S, Diaz LA Jr, Kinzler KW. Cancer genome landscapes. Science 2013;339: 1546–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 186.Abbosh C, Venkatesan S, Janes S, Fitzgerald RC, Swanton C. Evolutionary dynamics in pre-invasive neoplasia. Curr Opin Syst Biol 2017;2:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 187.Nowell CS, Radtke F. Notch as a tumour suppressor. Nat Rev Cancer 2017;17:145–59. [DOI] [PubMed] [Google Scholar]
- 188.Hanahan D, Weinberg RA. The hallmarks of cancer. Cell 2000;100:57–70. [DOI] [PubMed] [Google Scholar]
- 189.Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell 2011;144:646–74. [DOI] [PubMed] [Google Scholar]
- 190.Riquelme E, Maitra A, McAllister F. Immunotherapy for Pancreatic Cancer: More Than Just a Gut Feeling. Cancer Discov 2018;8:386–88. [DOI] [PubMed] [Google Scholar]
- 191.Martins FC, De S, Almendro V, Gönen M, Park SY, Blum JL, et al. Evolutionary pathways in BRCA1-associated breast tumors. Cancer Discov 2012;2:503–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192.Ortmann CA, Kent DG, Nangalia J, Silber Y, Wedge DC, Grinfeld J, et al. Effect of mutation order on myeloproliferative neoplasms. N Engl J Med 2015;372:601–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 193.Nangalia J, Nice FL, Wedge DC, Godfrey AL, Grinfeld J, Thakker C, et al. DNMT3A mutations occur early or late in patients with myeloproliferative neoplasms and mutation order influences phenotype. Haematologica 2015;100:e438–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.Shen SY, Singhania R, Fehringer G, Chakravarthy A, Roehrl MHA, Chadwick D, et al. Sensitive tumour detection and classification using plasma cell-free DNA methylomes. Nature 2018;563:579–83. [DOI] [PubMed] [Google Scholar]
- 195.De Bie J, Demeyer S, Alberti-Servera L, Geerdens E, Segers H, Broux M, et al. Single-cell sequencing reveals the origin and the order of mutation acquisition in T-cell acute lymphoblastic leukemia. Leukemia 2018;32:1358–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 196.Sivakumar S, Lucas FAS, McDowell TL, Lang W, Xu L, Fujimoto J, et al. Genomic landscape of atypical adenomatous hyperplasia reveals divergent modes to lung adenocarcinoma. Cancer Res 2017;77:6119–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197.Chitsazzadeh V, Coarfa C, Drummond JA, Nguyen T, Joseph A, Chilukuri S, et al. Cross-species identification of genomic drivers of squamous cell carcinoma development across preneoplastic intermediates. Nat Commun 2016;7:12601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Rahman SM, Ji X, Zimmerman LJ, Li M, Harris BK, Hoeksema MD, et al. The airway epithelium undergoes metabolic reprogramming in individuals at high risk for lung cancer. JCI Insight 2016;1:e88814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199.Shen Q, Cohen B, Zheng W, Rahbar R, Martin B, Murakami K, et al. Notch Shapes the Innate Immunophenotype in Breast Cancer. Cancer Discov 2017;7:1320–35. [DOI] [PubMed] [Google Scholar]
- 200.Martincorena I, Fowler JC, Wabik A, Lawson ARJ, Abascal F, Hall MWJ, et al. Somatic mutant clones colonize the human esophagus with age. Science 2018;362:911–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 201.Campbell JD, Zhang X, Perdomo C, Mazzilli S, Geshalter Y, Dhillon SS, et al. Genomic characterization of premalignant lung squamous cell carcinoma lesions [abstract]. In: Proceedings of the American Association for Cancer Research Annual Meeting 2018; Cancer Res 2018;78(13 Suppl):Abstract nr 3248. [Google Scholar]
- 202.Stachler MD,Camarda ND,Deitrick C, Kim A, Agoston AT, Odze RD, et al. Detection of Mutations in Barrett’s Esophagus Before Progression to High-Grade Dysplasia or Adenocarcinoma. Gastroenterology 2018;155:156–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 203.Centers for Disease Prevention and Control (CDC). Best practices for comprehensive tobacco control programs - 2014. Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014. Available from: http://www.cdc.gov/tobacco/stateandcommunity/best_practices/pdfs/2014/comprehensive.pdf. [Google Scholar]
- 204.Cummins SE, Wong S, Bonnevie E, Lee HR, Goto CJ, McCree Carrington J, et al. A multistate asian-language tobacco quitline: addressing a disparity in access to care. Am J Public Health 2015;105:2150–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 205.Vidrine JI, Shete S, Cao Y, Harmonson P, Sharp B, Miles L, et al. Ask-Advise-Connect: a new approach to smoking treatment delivery in health care settings. JAMA Intern Med 2013;173: 458–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 206.Trinidad DR, Pierce JP, Sargent JD, White MM, Strong DR, Portnoy DB, et al. Susceptibility to tobacco product use among youth in wave 1 of the population Assessment of tobacco and health (PATH) study. Prev Med 2017;101:8–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 207.Fiore MC, Jaén CR, Baker TB. Treating tobacco use and dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: Department of Health and Human Services. Public Health Service; 2008. [Google Scholar]
- 208.Pierce JP, Shi Y, McMenamin SB, Benmarhnia T, Trinidad DR, Strong DR, et al. Trends in lung cancer and cigarette smoking: California compared to the rest of the United States. Cancer Prev Res 2018. Oct 10 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 209.U.S. Department of Health and Human Services. E-cigarettes use among youth and young adults: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2016. Available from: https://www.cdc.gov/tobacco/data_statistics/sgr/e-cigarettes/pdfs/2016_sgr_entire_report_508.pdf. [Google Scholar]
- 210.Pierce JP, Sargent JD, Portnoy DB, White M, Noble M, Kealey S, et al. Association between receptivity to tobacco advertising and progression to tobacco use in youth and young adults in the PATH Study. JAMA Pediatr 2018;172:444–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 211.Phillips RL. Role of life-style and dietary habits in risk of cancer among seventh-day adventists. Cancer Res 1975;35:3513–22. [PubMed] [Google Scholar]
- 212.Iyengar NM, Hudis CA, AJ D. Obesity and cancer: local and systemic mechanisms. Ann Rev Med 2015;66:297–309. [DOI] [PubMed] [Google Scholar]
- 213.Iyengar NM, Brown KA, Zhou XK, Gucalp A, Subbaramaiah K, Giri DD, et al. Metabolic obesity, adipose inflammation and elevated breast aromatase in women with normal body mass index. Cancer Prev Res 2017;10:235–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 214.Mainous AG, Tanner RJ, Jo A, Anton SD. Prevalence of prediabetes and abdominal obesity among healthy-weight adults: 18-Year Trend. Ann Fam Med 2016;14:304–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 215.Safaeian M, Porras C, Pan Y, Kreimer A, Schiller JT, Gonzalez P,et al. Durable antibody responses following one dose of the bivalent human papillomavirus L1 virus-like particle vaccine in the Costa Rica Vaccine Trial. Cancer Prev Res 2013;6:1242–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 216.Bailey HH, Chuang LT, duPont NC, Eng C, Foxhall LE, Merrill JK, et al. American Society of Clinical Oncology Statement: human papillomavirus vaccination for cancer prevention. J Clin Oncol 2016;34:1803–12. [DOI] [PubMed] [Google Scholar]
- 217.President’s Cancer Panel. Reducing environmental cancer risk: what we can do now: U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute; 2008–9. [Google Scholar]
- 218.Tomasetti C, Li L, Vogelstein B. Stem cell divisions, somatic mutations, cancer etiology, and cancer prevention. Science 2017;355:1330–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 219.Tomczak K, Czerwińska P, Wiznerowicz M. The Cancer Genome Atlas (TCGA): an immeasurable source of knowledge. Contemp Oncol 2015;19:A68–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 220.Swanton C Intratumor heterogeneity: evolution through space and time. Cancer Res 2012;72:4875–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 221.Brune K, Abe T, Canto M, O’Malley L, Klein AP, Maitra A, et al. Multifocal neoplastic precursor lesions associated with lobular atrophy of the pancreas in patients having a strong family history of pancreatic cancer. Am J Surg Pathol 2006; 30:1067–76. [PMC free article] [PubMed] [Google Scholar]
- 222.Poste G, Compton CC, Barker AD. The national biomarker development alliance: confronting the poor productivity of biomarker research and development. Expert Rev Mol Diagn 2015;15:211–8. [DOI] [PubMed] [Google Scholar]
- 223.Vioxx Horton R., the implosion of Merck, and aftershocks at the FDA. Lancet 2004;364:1995–6. [DOI] [PubMed] [Google Scholar]
- 224.Zhu SH, Cummins SE, Wong S, Gamst AC, Tedeschi GJ, Reyes-Nocon J. The effects of a multilingual telephone quitline for Asian smokers: a randomized controlled trial. J Natl Cancer Inst 2012;104:299–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 225.Chen HL, Chang MH, Ni YH, Hsu HY, Lee PI, Lee CY, et al. Seroepidemiology of hepatitis B virus infection in children: ten years of mass vaccination in Taiwan. JAMA 1996;276:906–8. [PubMed] [Google Scholar]
- 226.Chiang CJ, Yang YW, You SL, Lai MS, Chen CJ. Thirty-year outcomes of the national hepatitis B immunization program in Taiwan. JAMA 2013;310:974–6. [DOI] [PubMed] [Google Scholar]
- 227.Lew J-B, Simms K, Smith M, Hall M, Kang YJ, Xu XM, et al. Primary HPV testing versus cytology-based cervical screening in women in Australia vaccinated for HPV and unvaccinated: effectiveness and economic assessment for the National Cervical Screening Program. Lancet Public Health 2017;2: e96–e107. [DOI] [PubMed] [Google Scholar]
- 228.Yehia BR, Schranz AJ, Umscheid CA, Lo Re V. The treatment cascade for chronic hepatitis C virus infection in the United States: a systematic review and meta-analysis. PLoS One 2014;9: e101554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 229.Pylayeva-Gupta Y, Lee KE, Hajdu CH, Miller G, Bar-Sagi D. Oncogenic Kras-induced GM-CSF production promotes the development of pancreatic neoplasia. Cancer Cell 2012;21: 836–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 230.Zhang Y, Yan W, Collins MA, Bednar F, Rakshit S, Zetter BR, et al. Interleukin-6 is required for pancreatic cancer progression by promoting MAPK signaling activation and oxidative stress resistance. Cancer Res 2013;73:6359–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 231.Sunaga N, Kaira K, Tomizawa Y, Shimizu K, Imai H, Takahashi G, et al. Clinicopathological and prognostic significance of interleukin-8 expression and its relationship to KRAS mutation in lung adenocarcinoma. Br J Cancer 2014;110: 2047–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 232.Kimura T, McKolanis JR, Dzubinski LA, Islam K, Potter DM, Salazar AM, et al. MUC1 vaccine for individuals with advanced adenoma of the colon: a cancer immunoprevention feasibility study. Cancer Prev Res 2013;6:18–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 233.Franklin WA, Gazdar AF, Haney J, Wistuba II, La Rosa FG, Kennedy T, et al. Widely dispersed p53 mutation in respiratory epithelium. A novel mechanism for field carcinogenesis. J Clin Invest 1997;100:2133–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 234.Balachandran VP, èuksza M, Zhao JN, Makarov V, Moral JA, Remark R, et al. Identification of unique neoantigen qualities in long-term survivors of pancreatic cancer. Nature 2017; 551:512–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 235.Kensler TW, Spira A, Garber JE, Szabo E, Lee JJ, Dong Z, et al. Transforming cancer prevention through precision medicine and immune-oncology. Cancer Prev Res 2016;9:2–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 236.Campbell JD, Mazzilli SA, Reid ME, Dhillon SS, Platero S, Beane J, et al. The case for a Pre-Cancer Genome Atlas (PCGA). Cancer Prev Res 2016;9:119–24. [DOI] [PubMed] [Google Scholar]
- 237.Pepe MS, Etzioni R, Feng Z, Potter JD, Thompson ML, Thornquist M, et al. Phases of biomarker development for early detection of cancer. J Natl Cancer Inst 2001;93: 1054–61. [DOI] [PubMed] [Google Scholar]
- 238.Spira A, Disis ML, Schiller JT, Vilar E, Rebbeck TR, Bejar R, et al. Leveraging premalignant biology for immune-based cancer prevention. Proc Natl Acad Sci U S A 2016;113: 10750–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 239.Singh T, Arrazola RA, Corey CG, Husten CG, Neff LJ, Homa DM, et al. Tobacco use among middle and high school students– United States, 2011–2015. MMWR Morb Mortal Wkly Rep 2016;65:361–7. [DOI] [PubMed] [Google Scholar]
- 240.Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Moodie ML, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet 2011;378:804–14. [DOI] [PubMed] [Google Scholar]
- 241.Tripp MK, Gershenwald JE, Davies MA, Garcia J, Gritz ER, Hawk ET, et al. Assessment of compliance with texas legislation banning indoor UV tanning by minors. JAMA Dermatol 2016;153:228–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 242.American Association for the Study of Liver Diseases. Recommendations for testing, managing and treating Hepatitis C. Available from: www.hcvguidelines.org.
- 243.Ona M, Papafragkakis H, Pan C. Hepatitis C Screening in the United States: current models and challenges. Am J Digest Dis 2015;2:29–40. [Google Scholar]
- 244.Kabiri M, Jazwinski AB, Roberts MS, Schaefer AJ, Chhatwal J. The changing burden of hepatitis C virus infection in the United States: model-based predictions. Ann Intern Med 2014;161: 170–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 245.Arora S, Thornton K, Murata G, Deming P, Kalishman S, Dion D, et al. Outcomes of treatment for hepatitis C virus infection by primary care providers. N Engl J Med 2011;364: 2199–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 246.Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer 1953;6:963–8. [DOI] [PubMed] [Google Scholar]
- 247.Brotherton JM, Gertig DM, May C, Chappell G, Saville M. HPV vaccine impact in Australian women: ready for an HPV-based screening program. Med J Aust 2016;204:184–184e181. [DOI] [PubMed] [Google Scholar]
- 248.El-Serag HB, Kanwal F, Richardson P, Kramer J. Risk of hepatocellular carcinoma after sustained virological response in Veterans with hepatitis C virus infection. Hepatology 2016;64: 130–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 249.Rock CL, Flatt SW, Byers TE, Colditz GA, Demark-Wahnefried W, Ganz PA, et al. Results of the Exercise and Nutrition to Enhance Recovery and Good Health for You (ENERGY) Trial: A Behavioral Weight Loss Intervention in Overweight or Obese Breast Cancer Survivors. J Clin Oncol 2015;33:3169–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 250.Patterson RE, Laughlin GA, LaCroix AZ, Hartman SJ, Natarajan L, Senger CM, et al. Intermittent Fasting and Human Metabolic Health. J Acad Nutr Diet 2015;115:1203–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 251.Nelson SH, Marinac CR, Patterson RE, Nechuta SJ, Flatt SW, Caan BJ, et al. Impact of very low physical activity, BMI, and comorbidities on mortality among breast cancer survivors. Breast Cancer Res Treat 2016;155:551–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 252.Hampel H, Pearlman R, Beightol M, Zhao W, Jones D, Frankel WL, et al. Assessment of Tumor Sequencing as a Replacement for Lynch Syndrome Screening and Current Molecular Tests for Patients With Colorectal Cancer. JAMA Oncol 2018;4: 806–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 253.Slavin TP, Banks KC, Chudova D, Oxnard GR, Odegaard JI, Nagy RJ, et al. Identification of Incidental Germline Mutations in Patients With Advanced Solid Tumors Who Underwent Cell-Free Circulating Tumor DNA Sequencing. J Clin Oncol 2018: JCO1800328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 254.Warnecke RB, Oh A, Breen N, Gehlert S, Paskett E, Tucker KL, et al. Approaching health disparities from a population perspective: the National Institutes of Health Centers for Population Health and Health Disparities. Am J Public Health 2008;98:1608–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 255.Gehlert S, Colditz GA. Cancer disparities: unmet challenges in the elimination of disparities. Cancer Epidemiol Biomarkers Prev 2011;20:1809–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 256.Settle K, Posner MR, Schumaker LM, Tan M, Suntharalingam M, Goloubeva O, et al. Racial survival disparity in head and neck cancer results from low prevalence of human papillomavirus infection in black oropharyngeal cancer patients. Cancer Prev Res 2009;2:776–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 257.Merchant G, Buelna C, Castañeda SF, Arredondo EM, Marshall SJ, Strizich G, et al. Accelerometer-measured sedentary time among Hispanic adults: Results from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Prev Med Rep 2015;2:845–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 258.Institute of Medicine (IOM). Unequal treatment: confronting racial and ethnic disparities in health care: The National Academy of Sciences; 2002. [Google Scholar]
- 259.Paskett ED. The New Vital Sign: Where Do You Live? Cancer Epidemiol Biomarkers Prev 2016;25:581–2. [DOI] [PubMed] [Google Scholar]
- 260.Institute of Medicine (IOM). Crossing the quality chasm: a new health system for the 21st century. Washington, D.C.: The National Academy of Sciences; 2001. [Google Scholar]
- 261.Song M, Vogelstein B, Giovannucci EL, Willett WC, Tomasetti C. Cancer prevention: Molecular and epidemiologic consensus. Science 2018;361:1317–8. [DOI] [PMC free article] [PubMed] [Google Scholar]