

Abstract
The high rate of obesity among adolescents is a global public health problem that has recently expanded to affect middle- and low-income countries. Brazil, which is undergoing a relatively rapid nutrition transition and has inadequate health systems, is currently experiencing the consequences of increasing rates of overweight and obesity concomitantly with the consequences of generations of malnourishment. Given this scenario, Brazil is an ideal context for examining the relationship between family socioeconomic status (SES) and adolescent body mass, as well as how this relationship varies across very different regions within the same country and across the body mass index (BMI) continuum. Guided by a framework that integrates nutrition transition and fundamental cause theories, we use unique nationally representative data with measured height and weight for all household members to conduct quantile regression models. The results suggest that family socioeconomic conditions are important theoretical factors associated with adolescent BMI, but that the way in which family SES impinges on adolescent BMI varies across regions characterized by different locations in the nutrition transition and varying levels of economic development. We also find that family socioeconomic disadvantages operate very differently according to BMI status. The results show that the socioeconomic gradient of adolescent BMI varies by stages of the nutrition transition and economic development and across BMI percentiles.
Introduction
High obesity prevalence among children and adolescents is a global public health problem that has recently expanded to affect middle- and low-income countries, such as Brazil, where obesity among young people is increasing at alarming rates (Ng et al. 2014). Although obesity in such countries has increased among most age groups, its growth among young people has prompted special concern because obesity in childhood and adolescence is associated with a host of negative health and social consequences that can persist throughout the life course (The et al. 2010). The global rise in obesity is widely attributed to the nutrition transition, a shift from a diet composed primarily of grains, fruits, and vegetables to a diet featuring animal-sourced fats and protein, sugars, and high-calorie industrially produced foods (Popkin 2001; Popkin, Lu, and Zhai 2002). The transition and its consequences are also, and increasingly, unevenly distributed. As the nutrition transition proceeds, obesity prevalence tends to increase at a greater rate among the least educated members of society (Dinsa et al. 2012; Popkin 1999), making it likely that obesity is increasingly contributing to growing socioeconomic disparities in health. Given the changes imposed by the nutrition transition, it is also likely that the way in which socioeconomic disparities in body mass index (BMI) emerge and progress among adolescents is heavily dependent on the stage of the nutrition transition and economic development.
Although a growing body of research shows that family SES is associated with offspring BMI (Balistreri and Van Hook 2009; Gordon-Larsen, Adair, and Popkin 2003; Haas et al. 2003; Martin 2008; Martin et al. 2012; Wang 2001; Zhang and Wang 2007), few studies in transitioning countries have examined whether this association is uniform across two important contexts: 1) regions within the same country that are marked by very different stages of the nutrition transition and levels of economic development and 2) the spectrum of BMI statuses, from underweight to obese. Many middle- and low-income countries such as Brazil are marked both by considerable regional variation in the progression of the nutrition transition, in levels of economic development (Monteiro, Conde, and Popkin 2001), and by shifting socioeconomic gradients in BMI as a result of the nutrition transition. In Brazil and other middle- and low-income countries, under-nutrition was relatively common among lower-income populations while obesity was rare and concentrated among the upper and middle classes (Monteiro et al. 1995; Popkin, Lu, and Zhai 2002). As these countries have experienced economic development and the consequent increases in income and the availability of inexpensive, high-calorie foods, obesity rates have increased and shifted from disproportionately afflicting the upper and middle classes to becoming widespread among the poor (Popkin 1993). Such patterns are consistent with fundamental cause theory (Link and Phelan 1995), which emphasizes the emergence and persistence of SES as a fundamental cause of health disparities even when the mechanisms linking SES and health undergo dramatic changes, as in the case of the nutrition transition.
It is therefore important to examine how the association between family SES and adolescent BMI varies across different contexts and across the spectrum of BMI percentiles. A focus on the median or average BMI can be misleading when examining differences in the association between groups in societies in transition, where the BMI distribution is changing rapidly (Beyerlein, Toschke, and von Kries 2010; Classen 2010; Costa-Font, Fabbri, and Gil 2009; Krishna et al. 2015; Ljungvall and Zimmerman 2012), because the mechanisms underlying the association might operate differently across the BMI spectrum. Indeed, even previous research in high-income countries with less variation in BMI has shown that the effects of SES are much stronger for the upper deciles of BMI (Classen 2010; Costa-Font and Gil 2013).
The goal of this paper is to examine how family SES and adolescent BMI intertwine in Brazil, a country that is highly unequal and has significant regional disparities in both economic development and the stage and speed of the nutrition transition. Drawing on nutrition transition and fundamental cause theories, we offer a nuanced theoretical framework for understanding the association between family SES and adolescent BMI in a country in transition. We investigate two research questions: 1) Does the association between family SES and adolescent BMI vary across regions marked by different levels of economic development and stages in the nutrition transition? and 2) Is the association uniform across different BMI statuses? To address these questions, we examine multiple measures of SES and use quantile regression methods and unique nationally representative data that contain information on adolescents’ measured BMI.
This is the first study to our knowledge to anchor heterogeneity in the association between family SES and adolescent BMI in the nutrition transition and economic development in a middle-income country. As such, this work addresses a growing public health concern outside high-income countries and contributes to the literature on adolescent health disparities in at least three key ways: by exploring theoretically informed variation in the effects of family SES on BMI; by analyzing multiple BMI statuses from underweight to obesity, shedding light on socioeconomic disadvantages across the entire spectrum of adolescent BMI statuses; and by applying quantile regression models to a large, nationally representative dataset from Brazil with multiple measures of SES and anthropometric measures of weight and height of all household members. The results offer a nuanced portrait of adolescent BMI in Brazil and serve as an important counterpoint to the current literature, which focuses primarily on the United States and high-income countries.
The Social Patterning of Obesity in Brazil
Since the 1970s, obesity among children and adolescents has increased dramatically in most countries across the world (Ng et al. 2014). In Brazil, the proportion of adolescents (age 10–18) considered obese or overweight grew from 3.7 percent in 1970 to 21.7 percent in 2009 (IBGE 2010). This sharp increase in adolescent obesity is particularly striking, given that malnutrition was widespread in Brazil as recently as the 1970s, when nearly one-fifth of all Brazilian children and adolescents were malnourished (Monteiro et al. 1992) and 37.1 percent were stunted (Monteiro, D’Aquino, and Conde 2010). By comparison, by the mid-2000s, only about 5 percent were malnourished and 7.1 percent were stunted (Monteiro, D’Aquino, and Conde 2010). This shift from a high prevalence of undernutrition to a predominance of overweight and obesity occurred as part of Brazil’s nutrition transition, during which the country experienced large-scale changes in dietary patterns driven primarily by increased consumption of ultra-processed foods high in saturated fat, sodium, and sugar (Monteiro et al. 2000, 2010).
As in many middle- and low-income countries, the nutrition transition in Brazil has taken place during a period of massive socioeconomic development (Monteiro et al. 2002), and its effects have been unequally distributed across the population. Previous research in many middle- and low-income countries has shown that as a country’s gross domestic product increases, the burden of obesity shifts from high-SES to low-SES individuals (Monteiro et al. 2004). There is evidence of a similar trend emerging among Brazilian adults: whereas obesity was once characterized as a disease of the rich, it is now increasingly becoming a burden of the poor (Monteiro, Conde, and Popkin 2007). It remains unclear whether this pattern holds for adolescents when accounting for family social origin rather than individual-level adult SES, as in most prior studies focusing on adults.
Regional Differences: Comparing Northern and Southern Brazil
Throughout the twentieth century, Brazil experienced tremendous but geographically uneven socioeconomic development. Industrialization, agricultural modernization, and urbanization were initially concentrated in the southern regions, and did not occur in the northern regions until much later (Diniz 2002). These large and persistent regional gaps in development and demographic shifts have translated into high levels of socioeconomic inequality and marked geographic variation in the trajectory of the nutrition transition in Brazil.
Malnourishment and stunting were disproportionately concentrated among the poor and, importantly for this paper, were also disproportionately concentrated in the northern regions. In the mid-1970s, more than a quarter of the children in the Northeast were malnourished, compared to only 13 percent of children in the Southeast (Monteiro et al. 1992), and 64 percent of children in the Northeast lived in households with incomes below the poverty line, compared to only 27.7 percent of children in the Southeast (Monteiro et al. 1992). Although levels of malnourishment have declined in recent decades, regional disparities persist. In the South and Southeast, for each malnourished child there are nine children considered overweight or obese. In the North and Northeast,1 in contrast, for each malnourished child there are four children considered overweight or obese (IBGE 2010). These regional disparities suggest that Northern Brazil is behind Southern Brazil in terms of socioeconomic development and the nutrition transition, which are intertwined (Monteiro et al. 1992, 1995, 2010). The nutrition patterns in Southern Brazil resemble those of many high-income countries, with high obesity prevalence and a food environment featuring animal-sourced fats and protein, sugars, and high-calorie industrially produced foods (Dinsa et al. 2012; Popkin 1999). The nutrition patterns in the Northern region, on the other hand, are consistent with patterns at the tail end of the nutrition transition (Monteiro et al. 2010). Such regional variation in the nutrition transition and in socioeconomic development may be associated with geographic differences in the association between family SES and adolescent BMI.
Family SES and Adolescent BMI
We first discuss the overall ways in which family SES is theorized to influence adolescent BMI, drawing on research from other countries to conceptualize family SES as a social determinant of adolescent BMI. In line with the tradition of research examining the association between social position and health, researchers have recently become interested in whether and how family SES is associated with BMI and obesity among children and adolescents (Balistreri and Van Hook 2009; Classen 2010; Costa-Font and Gil 2013; Martin et al. 2012; Pudrovska, Logan, and Richman 2014; Wang 2001; Wang and Zhang 2006). Family SES may directly shape adolescents’ BMI because resources such as family income and parental education likely influence a family’s ability to manage BMI risks among their children, primarily through providing nutritional foods and healthy lifestyles.
However, family income and parental education might influence adolescent BMI in different ways. Family income can affect adolescent BMI by increasing access to healthy foods and exercise habits (Cawley 2004), suggesting a negative association with adolescent BMI. Growing up in a financially stable familial environment (Carr and Umberson 2013) and overall higher SES across generations can lead to better health outcomes. However, family income can also be used to purchase non-healthy goods, leading to a positive association between family income and adolescent BMI. Further, rapid increases in income may be linked with changing consumption patterns, such as indulgent child-feeding practices (Balistreri and Van Hook 2009), where a positive association could reflect rapid upward mobility. Thus, it is perhaps unsurprising that the empirical evidence on the association between family income and adolescent BMI is mixed; researchers have found associations ranging from positive (Haas et al. 2003), to negative (Goodman 1999; Pudrovska, Logan, and Richman 2014), to no association (Goodman, Slap, and Huang 2003; Martin et al. 2012; Zhang and Yang 2007).
In contrast to the mixed evidence regarding family income and adolescent BMI, the evidence regarding parental education and adolescent BMI points to a negative association, at least in high-income countries (Glass, Haas, and Reither 2010; Martin 2008; Martin et al. 2012; Pudrovska, Logan, and Richman 2014). Parents with higher levels of education are more capable of setting and accomplishing health-related goals for their children (Mirowsky and Ross 2003), have greater access to information, skills, and knowledge, and are better able to address children’s health-related behaviors, including regulating food and exercise habits (Ogden et al. 2006).
Most past studies, however, have examined the association between family SES and adolescent BMI in countries already in advanced stages of the nutrition transition and obesity epidemics. Given that Brazil, particularly the Northern region, is at an earlier stage of the nutrition transition than high-income countries, the association between family SES and adolescent BMI might differ from the patterns observed in studies of high-income countries. In early nutrition transition contexts where stunting has only recently declined and obesity is still a relatively new health risk, we might expect positive to negligible associations between family SES and adolescent BMI. A positive or negligible association between family income and adolescent BMI is possible because resources were more commonly used to prevent food insecurity rather than combat obesity. In these settings, food scarcity and patterns of high-energy expenditure are commonly found among the poor, whereas elite groups are capable of obtaining an adequate food supply (Monteiro et al. 2004).
Moreover, a positive or negligible association between parental education and adolescent BMI is possible because individuals might display their status by eating trendy and high-status foods that might be unhealthy (Naccarato and Lebesco 2012). Higher consumption of unhealthy foods among those with higher SES might especially be the case in pre- or early stage nutrition transition contexts, where industrialized foods are new and seen as “high-status,” and where information about the unhealthy consequences of industrialized foods is not yet known. Thus, in the absence of information about unhealthy foods, education in pre- and early stage nutrition transition contexts might serve as a status marker that guides individuals’ dietary choices. These factors imply a positive association between parental education and adolescent BMI. However, because highly educated parents are better able to avoid shifting risks in their children’s environments, once the nutrition transition progresses and awareness about the consequences of such unhealthy foods grows, a negative association between parental education and adolescent BMI emerges, an empirical finding of most studies in the United States.
Previous studies in high-income countries have also tended to analyze samples with more limited variance in BMI. Brazil offers an interesting case to examine variation in the association because it has significant regional variation in both adolescent BMI and socioeconomic and nutrition environments. Given the transitional nature of and significant regional variation in BMI in Brazil, it is also important to examine the association between family SES and adolescent BMI across the whole spectrum of BMI percentiles. When examining societies in transition where body mass is changing rapidly, it is necessary to consider that the effects of family SES on adolescent BMI are potentially different at higher and lower percentiles of the BMI distribution (among the thinnest and heaviest adolescents). This is the case for at least two reasons.
First, the mechanisms determining the association between family SES and adolescent BMI (i.e., family resources that promote healthy foods) likely operate differently across the BMI spectrum. Among underweight adolescents and their families, under-nutrition is highly dependent on food availability; a higher family income likely means providing any food on the table and consequently could be associated with increases in BMI. Among obese adolescents, on the other hand, high family SES might be associated with lower BMI because the operating mechanism might be the ability to purchase healthy foods, because high family SES might also translate into the financial resources and time to promote a healthy lifestyle through diet and exercise (Pudrovska, Logan, and Richman 2014).
The strength of the association between family SES and adolescent BMI may also differ across BMI percentiles (Beyerlein, Toschke, and von Kries 2010; Costa-Font, Fabri, and Gil 2009; Krishna et al. 2015; Ljungvall and Zimmerman 2012). Having higher family SES may be more important for certain groups than for others. For example, obese adolescents may be more susceptible to the negative effects of low family SES than normal-weight adolescents because their families are less likely to have the resources needed to counter the risks of obesogenic food environments. In other words, a higher level of income and parental education may be needed among obese adolescents than among normal-weight adolescents to offset the mechanisms leading to BMI increases. Indeed, recent public health and epidemiological research has found different magnitudes in the associations between several risk factors and BMI at different BMI levels (Beyerlein, Toschke, and von Kries 2010; Costa-Font, Fabbri, and Gil 2009; Krishna et al. 2015; Ljungvall and Zimmerman 2012), including that the association between parental education and BMI is stronger for children with higher BMI values (Beyerlein, Toschke, and von Kries 2010). If risk factors of overweight and obesity disproportionately affect children with high BMI (making them even heavier), incremental exposure to those risk factors would primarily result in more extreme values of BMI in the upper percentiles. The potential for variation in the association between family SES and adolescent BMI across BMI percentiles is likely amplified in countries with changing nutritional environments and large regional variation in BMI, such as Brazil.
Conceptual Framework
We integrate research about the nutrition transition and socioeconomic development in Brazil with research about the association between family SES and adolescent BMI to understand how family SES shapes adolescent BMI in a transitioning country context using a framework that incorporates nutrition transition and fundamental cause theories. The nutrition transition framework guides our thinking about how socioeconomic development and nutritional environments are intertwined and influence BMI (Popkin 1994). In pre-transition and less developed areas, under-nutrition is relatively common, and obesity is relatively rare and concentrated among the upper- and middle-class individuals because they are less likely to be engaged in physical labor and are wealthy enough to purchase higher-calorie foods (Popkin 1994). As economic development occurs and the nutrition transition advances, incomes grow, inexpensive high-caloric foods become more widely available, occupations become much less physically demanding, energy expenditure declines, and individuals shift to much higher fat and more energy-dense diets. As a result, poor nutrition and obesity prevalence increase and obesity shifts from disproportionately afflicting the upper and middle classes to being a burden of the poor (Popkin 1993; Monteiro et al. 1995). For adolescents, these circumstances comprise a context of intergenerational transmission of disadvantage, wherein adolescents from families with low-SES families become the most likely to suffer detrimental BMI outcomes.
To further understand the social patterning of BMI in Brazil as a function of the nutrition transition and socioeconomic development, we use fundamental cause theory (FCT) (Link and Phelan 1995). This perspective views SES as a durable, fundamental cause of health because SES shapes access to resources, knowledge, and skills that make individuals with high SES better equipped to adjust to changes brought about by new diseases. Thus, the emergence of a new health risk may spark or strengthen a negative SES gradient because individuals with low SES have less resources and information about new health risks (Freese and Lutfey 2011; Omran 1971; Phelan and Link 2005; Phelan et al. 2004). In the case of BMI in Brazil, the SES gradient may be flat in regions in the early stages of the nutrition transition because little is known about the risks of obesity. In regions in the later stages of the nutrition transition, when awareness of both the risks of obesity and the resources for preventing it are more widely understood, a negative SES gradient is likely to emerge.
FCT also addresses how the mechanisms linking SES and BMI might change in the face of dramatic shifts in the nutrition environment. For example, we might expect the two primary dimensions of family SES—income and parental education—to vary in their association with adolescent BMI depending on the stage of the nutrition transition. In pre- or early transition contexts in which malnutrition and shortages of food are more common, family income would likely be most important for combating malnutrition and achieving a healthy BMI. However, as the nutrition transition proceeds, and processed foods become more widespread and affordable, education may be the socioeconomic resource most relevant to access information and implement best practices for avoiding behaviors that can lead to unhealthy BMI.
Current Study
We borrow from the nutrition transition framework and FCT to develop a series of hypotheses regarding variation in the association between family SES and adolescent BMI across regions marked by different stages of the nutrition transition and the levels of socioeconomic development and across the spectrum of BMI statuses (table 1).
Table 1.
Study Hypotheses
| Hypothesis 1 | Overall positive association between family SES and adolescent BMI in Brazil but regional differences |
| Hypothesis 1a | Association between family SES and adolescent BMI positive in Northern Brazil |
| Hypothesis 1b | Association between family SES and adolescent BMI negligible or negative in Southern Brazil |
| Hypothesis 2 | Variation in association between family SES and adolescent BMI by BMI status; differences between underweight and overweight and obese adolescents |
| Hypothesis 3 | Among underweight adolescents, positive association between family SES and adolescent BMI; no regional differences |
| Hypothesis 4 | Regional differences among overweight and obese adolescents |
| Hypothesis 4a | Among overweight and obese adolescents, positive association between family SES and BMI in Northern Brazil |
| Hypothesis 4b | Among overweight and obese adolescents, negligible or negative association between family SES and BMI in Southern Brazil |
| Hypothesis 5 | Regional differences less pronounced for parental education than for family income |
Hypothesis 1: Overall Association and Regional Differences
Given that Brazil is still undergoing the nutrition transition, our first hypothesis is that the overall association between family SES and adolescent BMI will be positive; that is, higher levels of parental education and family income will be associated with higher BMI (Hypothesis 1). However, because of the uneven progression of the nutrition transition and socioeconomic development across regions in Brazil, we expect that the associations will differ (in magnitude and possibly in direction) depending on the region examined. We expect that the association will be positive in Northern Brazil, due to its lower levels of economic development and earlier stage of the nutrition transition (Hypothesis 1a), but that the association will be negative or negligible in Southern Brazil (Hypothesis 1b), reflecting the more advanced transitional stage of the nutrition transition, though not yet aligned with high-income countries.
Hypothesis 2: Overall Differences across BMI Percentiles
Because the mechanisms determining the association between family SES and adolescent BMI (i.e., family resources that promote healthy foods) likely operate differently across the BMI spectrum, we hypothesize that the associations between family SES and adolescent BMI will vary for different BMI percentiles because high or low family SES likely implies different dis(advantages) for underweight, normal-weight, overweight, or obese adolescents (Hypothesis 2). We elaborate on the expected direction of these associations in the next set of hypotheses.
Hypotheses 3 and 4: Differences across Regions and BMI Percentiles
We build on the previous hypotheses to examine the association between family SES and adolescent BMI across BMI percentiles separately for Northern and Southern Brazil. We expect to find both similarities and differences between these regions in the associations we examine. In contexts where under-nutrition is highly dependent on food availability (as in Brazil), food scarcity among the families of malnourished adolescents means that low family SES is likely associated with lower adolescent BMI. We hypothesize that such a relationship characterizes both Northern and Southern Brazil because the mechanism underlying the association between family SES and BMI among undernourished adolescents —income to put food on the table—is likely similar (Hypothesis 3).
However, we hypothesize that there will be regional differences in the associations among overweight and obese adolescents (Hypothesis 4). We anticipate a positive association between family SES and adolescent BMI among overweight and obese adolescents in Northern Brazil (Hypothesis 4a), a region in earlier stages of the nutrition transition where processed and out-of-home meals are available primarily to those with higher incomes. In contrast, in regions such as Southern Brazil that are at a later stage in the nutrition transition, the burden of overweight and obesity will likely fall more heavily on the poor, and those with high SES will be less affected. We therefore expect a negligible or negative association between family SES and adolescent BMI among overweight and obese adolescents in Southern Brazil (Hypothesis 4b).
Hypothesis 5: Regional Differences in Effects of Family Income and Parental Education
Finally, while we expect regional differences in the associations between family SES and adolescent BMI (Hypothesis 1a and 1b), we also hypothesize that these differences will be less pronounced for parental education than for financial forms of SES, which highlights the importance of considering multiple forms of family SES (Hypothesis 5). The mechanisms behind the associations between parental education and adolescent BMI are more susceptible to rapid changes in food environments and diet behaviors through the diffusion of innovations that characterize the nutrition transition. Well-educated parents are likely to acquire and use new knowledge about the changing food environments before non-educated parents. Depending on the stage of the nutrition transition, such new knowledge might counteract the harmful effects of the changing food environments, yielding associations that are more similar across regions. The capital available to offspring through family income, on the other hand, likely translates into more dissimilar (dis)advantages for adolescents in regions marked by sharp nutritional differences.
Data and Methods
Data
We use data from the nationally representative Pesquisa de Orçamentos Familiares (Household Expenditure and Income Survey) (POF) conducted in 2002–2003 and 2008–2009. The POF is a household survey conducted by the Brazilian Census Bureau (IBGE). A probability-based, stratified, multistage dataset, the POF has information on 48,470 households and 182,333 individuals in 2002–2003 and 55,970 households and 190,159 in 2008–2009.
The dataset contains demographic and socioeconomic variables as well as indicators of health status, including anthropometric measures of weight and height of every household member, including all children and their parents. Having measured (rather than self-reported) weight and height is a major advantage of the POF data compared to most surveys used to examine BMI in Brazil and in most other countries.2 Another unique feature of the data is the inclusion of BMI of all household members, which allows the use of the desirable but rarely available measure of parental BMI as a control for the intergenerational association in BMI (Costa-Font and Gil 2013). The POF also contains detailed inventories of food availability in households.
Analytic Samples
We used three analytic samples to address the research questions. The first sample included all adolescents who were ages 12–17 in both waves and who were classified as the child of the household head3 (N = 27,123). The second and third samples were composed of 15,539 and 7,903 adolescents living in Northern and Southern Brazil, respectively. We included only one adolescent per household (chosen via random selection using Stata) to eliminate problems of non-independence of observations. We focused on Northern and Southern Brazil because these regions have clearly different patterns and stages of the nutrition transition (Moubarac et al. 2014).4
Measures
The dependent variable was adolescent BMI, calculated as measured weight divided by measured height. Following the literature, we applied a transformation based on the Box-Cox transformation-based semiparametric approach5 to create a BMI z-score that accounts for the strong correlation of BMI with age and sex (Cole and Green 1992; Cole 1988).
While we used BMI z-scores in the models, we conducted multiple sensitivity tests using different calculations of BMI to ensure the robustness of the findings. In models estimated with the log of BMI (original) as the dependent variable, the results remain unchanged, except for the covariates of age and sex, as expected. We also estimated models separately by sex and found that the overall patterns were similar for boys and girls. For descriptive purposes, we also created a categorical BMI status variable based on the standards established by the World Health Organization (WHO 2007). Adolescents were classified into four categories: underweight (z < −2), normal weight (z > = −2 and < = 1), overweight (z > 1), and obese (z > 2).
Our key independent variables included family SES, measured as the log of household income per capita, and whether at least one of the parents has a high school education or more.6 We also used several control variables at the adolescent and family levels. We included controls for age, sex (1 = female), and race (1 = nonwhite). We created an index of food availability in the household using principal components factors (PCF).7. We constructed an index of the availability of food of high nutritional value that includes vegetables, meat, chicken, fish, milk, yogurt, eggs, cheese, fruits, grains, and fibers (Previdelli et al. 2011).
We also included a four-category indicator of parental weight status based on parental BMI, using a BMI of 25–29 and 30 and above as the cutoffs for overweight and obesity, respectively. The final variable was coded 0 if neither parent is obese or overweight, 1 if only the mother is obese or overweight, 2 if only the father is obese or overweight, and 3 if both parents are obese or overweight. Finally, we included urbanicity and, in models for the entire country, region of residence.
Methods
We first examined the association between family SES and adolescent BMI by estimating OLS regression models, as is standard. We next estimated quantile regression models, which assume that the associations between covariates (family SES) and the dependent variable (adolescent BMI) vary according to the percentile of the dependent variable examined (Classen 2010; Koenker and Bassett 1978). Relative to other regression estimates, quantile regression estimates are more robust against outliers in the dependent variable. The main advantage of these models is that they allow us to investigate whether the strength or direction of the association between covariates (SES) and the dependent variable (BMI) varies in different percentile groups along the dependent variable distribution (Classen 2010; Koenker and Bassett 1978; Koenker and Hallock 2001). Quantile regression models account for effects not only in the conditional mean (such as OLS) but also on the lower and upper tails of the BMI distribution, therefore satisfactorily accounting for observed heterogeneity in our dependent variable.
The quantile regression can be written as (Buchinsky 1994)
where X is the independent variables with βα coefficients at each quantile α. Quantα (Y|X) denotes the αth conditional quantile of Y, adolescent BMI, given a set of X independent variables. We estimate simultaneous quantile regression models in which the variance-covariance matrix is estimated via bootstrapping with 1,000 bootstrap replications to obtain the standard deviations. We also run separate models for two regions: North/Northeast and South/Southeast.8
We performed the estimations at the 3th, 50th, 85th, and 97th percentiles of BMI, following the cutoffs used in literature (Beyerlein, Toschke, and von Kries 2010; Classen 2010; Costa-Font, Fabbri, and Gil 2009; Krishna et al. 2015; Ljungvall and Zimmerman 2012; WHO 2007). These percentiles reflect areas in the BMI distribution that are of greatest interest, allowing for relationships to vary in magnitude and direction (Stifel and Averett 2009). The 50th percentile gives the estimation at the median. The 85th percentile is the cutoff for those considered overweight, and the 97th percentile is the cutoff for those considered obese. Because the BMI distribution of the Brazilian population is in transition, we also examined the other extreme of the distribution, that is, in the 3rd percentile, the cutoff for underweight adolescents. We also estimated the quantile regressions in all percentiles of the BMI distribution to create figures showing the associations across the entire distribution.
Results
Table 2 shows the means and proportions of all variables included in the models. In the full sample, parents have completed, on average, 7.19 years of schooling, and the mean per capita household income is US$501.32. These overall statistics mask Brazil’s large regional differences. In Southern Brazil, parental education reaches 8.11 years of schooling, while parents in Northern Brazil have only 5.81 years of schooling. Per capita household income is $636.97 in Southern Brazil and $299.36 in Northern Brazil. There are also large race differences across the two regions—61.59 percent of adolescents in Southern Brazil are white while only 25.03 percent of adolescents are considered white in Northern Brazil. In all three samples, around 93 percent of the respondents are enrolled in school. In terms of parental BMI status, for 26.11 percent of adolescents neither their mother nor their father is considered overweight or obese, while for 28.07 percent of adolescents both parents are considered overweight or obese.
Table 2.
Individual and Family Characteristics of Adolescents Ages 12–17: Brazil, 2002–2003 and 2008–2009
| Brazil | Northern regions (NNE) | Southern regions (SSE) | |
|---|---|---|---|
| Parental education (high school or more) | 30.59 | 22.80 | 35.82 |
| SD | 4.32 | 4.26 | 4.11 |
| Per capita household income | 501.32 | 299.36 | 636.97 |
| SD | 836.34 | 612.02 | 913.30 |
| Sex (% of girls) | 47.32 | 46.66 | 47.58 |
| Age | 14.39 | 14.38 | 14.41 |
| SD | 1.69 | 1.68 | 1.70 |
| Healthy food index | 0.43 | 0.43 | 0.43 |
| SD | 0.32 | 0.32 | 0.32 |
| Attends school? (% yes) | 93.02 | 92.97 | 92.95 |
| Race (% of white) | 46.01 | 25.03 | 61.59 |
| Parental obesity | |||
| None is overweight/obese | 26.11 | 30.75 | 22.78 |
| Only father overweight/obese | 23.43 | 20.34 | 25.26 |
| Only mother overweight/obese | 22.38 | 24.2 | 21.57 |
| Both overweight/obese | 28.07 | 24.71 | 30.39 |
| Region of residence * | |||
| North and Northeast | 39.04 | ||
| South and Southeast | 54.46 | ||
| Midwest | 6.50 | ||
| N | 27,123 | 15,539 | 7,903 |
Source: 2003 and 2008 POF.
The percentage of those in Southern regions is larger than Northern regions due to the use of sample weights.
Table 3 presents summary statistics for each covariate in the multivariate analyses separately by adolescent BMI categories; as in table 2, results are presented separately for each of the three analytical samples. For ease of interpretation, we display BMI in four categories: underweight, normal weight, overweight, and obese. To facilitate comparisons with studies focusing on mean BMI, we also provide mean BMI for all adolescents by parental education level and by the highest and lowest household income quintile. The results in table 3 highlight several interesting regional patterns. In the full sample, parents of overweight and obese adolescents have higher levels of schooling than parents of underweight and normal-weight adolescents (7.96 and 8.14 versus 6.62 and 7.06); this difference occurs in both regions but is smaller in Southern Brazil than in Northern Brazil. In contrast, mean per capita household income is lower for adolescents considered overweight and obese than for those considered underweight and normal weight, although again the difference is starker in Northern than in Southern Brazil. Children of obese or overweight parents are more likely to be considered obese or overweight themselves; this likelihood is even greater when both parents are obese or overweight.
Table 3.
BMI Group per Individual and Household Characteristics of Adolescents Ages 12–17: Brazil, 2003–2004 and 2008–2009
| Brazil |
Northern regions (NNE) |
Southern regions (SSE) |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Underw. |
Normal |
Overw. |
Obese |
Underw. |
Normal |
Overw. |
Obese |
Underw. |
Normal |
Overw. |
Obese |
|
| Column 1 | Column 2 | Column 3 | Column 4 | Column 5 | Column 6 | Column 7 | Column 8 | Column 9 | Column 10 | Column 11 | Column 12 | |
| Total | 2.12 | 82.49 | 12.56 | 2.83 | 2.82 | 85.61 | 9.65 | 1.92 | 1.64 | 80.31 | 14.54 | 3.52 |
|
| ||||||||||||
| Parental education * (HS or more) | 27.41 | 29.06 | 34.78 | 39.76 | 22.09 | 22.12 | 31.01 | 39.56 | 32.64 | 33.76 | 36.45 | 40.58 |
|
| ||||||||||||
| Mean BMI ** | ||||||||||||
|
| ||||||||||||
| (Less than HS) | 19.99 (−0.052) | 19.59 (−0.177) | 20.31 (0.0480) | |||||||||
|
| ||||||||||||
| (HS or more) | 20.50 (0.104) | 20.21 (0.022) | 20.64 (0.143) | |||||||||
|
| ||||||||||||
| Per capita household income | 423.55 | 479.57 | 614.29 | 692.33 | 197.42 | 280.56 | 431.35 | 623.70 | 658.12 | 621.68 | 699.00 | 719.90 |
|
| ||||||||||||
| SD | 941.91 | 819.13 | 891.69 | 925.52 | 238.82 | 559.81 | 863.13 | 1220.70 | 1259.28 | 915.85 | 877.96 | 788.42 |
|
| ||||||||||||
| Mean BMI ** | ||||||||||||
|
| ||||||||||||
| (First quartile) | 19.28 (−0.204) | 19.08 (−0.230) | 19.55 (−0.163) | |||||||||
|
| ||||||||||||
| (Fourth quartile) | 20.81 (0.185) | 20.69 (0.137) | 20.85 (0.200) | |||||||||
|
| ||||||||||||
| Healthy food index | 0.44 | 0.43 | 0.44 | 0.46 | 0.44 | 0.43 | 0.45 | 0.48 | 0.45 | 0.43 | 0.44 | 0.46 |
|
| ||||||||||||
| SD | 0.33 | 0.32 | 0.32 | 0.33 | 0.33 | 0.32 | 0.32 | 0.33 | 0.32 | 0.32 | 0.31 | 0.33 |
|
| ||||||||||||
| Attends school? (% yes) | 94.73 | 93.29 | 91.14 | 92.24 | 96.35 | 93.04 | 90.82 | 95.55 | 93.31 | 93.39 | 90.92 | 91.01 |
|
| ||||||||||||
| Race (% white) | 41.81 | 44.79 | 54.15 | 48.53 | 21.32 | 24.83 | 27.18 | 28.62 | 66.62 | 60.48 | 68.22 | 57.13 |
|
| ||||||||||||
| Parental obesity | ||||||||||||
|
| ||||||||||||
| None overweight/obese | 45.89 | 27.71 | 17.09 | 4.91 | 48.95 | 31.97 | 19.20 | 7.58 | 43.05 | 24.39 | 16.23 | 3.63 |
|
| ||||||||||||
| Only father overweight or obese | 21.10 | 23.67 | 22.29 | 23.31 | 16.35 | 20.78 | 18.88 | 13.88 | 26.36 | 25.46 | 23.65 | 27.02 |
|
| ||||||||||||
| Only mother overweight or obese | 20.44 | 23.26 | 17.97 | 17.78 | 24.35 | 24.34 | 22.60 | 26.02 | 15.61 | 23.02 | 15.80 | 15.02 |
|
| ||||||||||||
| Both overweight/obese | 12.58 | 25.36 | 42.65 | 54.00 | 10.35 | 22.91 | 39.32 | 52.52 | 14.98 | 27.14 | 44.32 | 54.32 |
|
| ||||||||||||
| Poor? (% yes) | 34.28 | 24.16 | 14.48 | 10.87 | 50.70 | 43.21 | 33.41 | 26.73 | 15.57 | 10.46 | 5.33 | 5.04 |
|
| ||||||||||||
| Region of residence * | ||||||||||||
|
| ||||||||||||
| Northern regions | 51.86 | 40.52 | 30.01 | 26.50 | ||||||||
|
| ||||||||||||
| Southern regions | 41.94 | 53.02 | 63.04 | 67.75 | ||||||||
|
| ||||||||||||
| Midwest | 6.20 | 6.46 | 6.95 | 5.75 | ||||||||
|
| ||||||||||||
| N | 641 | 22,638 | 3,171 | 673 | 415 | 13,259 | 1,557 | 308 | 141 | 6,369 | 1,127 | 266 |
Source: Own elaboration based on 2003 and 2008 POF.
Row sum,
Mean BMI and Z-score in parenthesis.
Overall Association and Regional Differences
Table 4 shows regression results for OLS models with adolescent BMI as the dependent variable. These models are comparable to the models implemented in most previous studies that estimate reduced-form equations for the average child (at the conditional mean levels of adolescent BMI). Column 1 shows results for the entire country, while columns 2 and 3 show results for the Northern versus Southern regions, respectively. Higher levels of household per capita income and of parental education are associated with increases in BMI, providing support for Hypothesis 1. Higher levels of household per capita income are also associated with increases in BMI for adolescents in both Northern and Southern Brazil, with coefficients statistically significant at the 0.01 level. The results for household income align with our hypothesis for Northern Brazil, but diverge from our prediction of a negative or negligible association for Southern Brazil, suggesting that the Southern region might be more distant from completing the nutrition transition than we had anticipated. The coefficient representing parental education is also statistically significant and positive for Northern Brazil, suggesting that adolescents with parents with at least a high school education have higher BMI (0.081 significant at the 0.01 level, shown in column 2). The coefficient representing parental education is not statistically significant in Southern Brazil. These findings for parental education provide some support for Hypotheses 1a and 1b in that the associations between parental education and adolescent BMI differ across regions. It is also noteworthy that adolescents with both parents considered overweight or obese have higher BMI levels than those with no overweight or obese parents.
Table 4.
Results from OLS Regression Models of Adolescent BMI Percentiles: Brazil, 2003–2008, 12–17 Years Old, BMI z-Score
| Brazil |
Northern regions (NNE) |
Southern regions (SSE) |
|
|---|---|---|---|
| BMI z-score | Column 1 | Column 2 | Column 3 |
| Log of per capita household income | 0.045*** | 0.042*** | 0.058*** |
| (0.0080) | (0.0104) | (0.0155) | |
|
| |||
| Parental education—high school or more (no omitted) | 0.055*** | 0.081*** | 0.017 |
| (0.0154) | (0.0209) | (0.0273) | |
|
| |||
| Age in years | −0.005 | 0.008* | −0.016** |
| (0.0035) | (0.0046) | (0.0065) | |
|
| |||
| Sex (male omitted) | −0.009 | 0.034** | −0.048** |
| (0.0118) | (0.0154) | (0.0221) | |
|
| |||
| Parental obesity (none is overweight or obese omitted) | |||
|
| |||
| Only father overweight or obese | 0.211*** | 0.197*** | 0.252*** |
| (0.0171) | (0.0224) | (0.0326) | |
|
| |||
| Only mother overweight or obese | 0.228*** | 0.233*** | 0.218*** |
| (0.0167) | (0.0210) | (0.0328) | |
|
| |||
| Both overweight or obese | 0.519*** | 0.494*** | 0.562*** |
| (0.0162) | (0.0211) | (0.0310) | |
|
| |||
| Healthy food index | −0.023 | −0.039 | −0.057 |
| (0.0193) | (0.0251) | (0.0361) | |
|
| |||
| Race (nonwhite omitted) | −0.002 | −0.023 | 0.023 |
| (0.0130) | (0.0178) | (0.0235) | |
|
| |||
| Urban or rural area? (Rural omitted) | −0.023* | −0.019 | −0.029 |
| (0.0135) | (0.0172) | (0.0265) | |
|
| |||
| Year (2003 omitted) | 0.124*** | 0.102*** | 0.176*** |
| (0.0124) | (0.0162) | (0.0231) | |
|
| |||
| Region (Southern regions omitted) | |||
|
| |||
| North and Northeast | −0.127*** | ||
| (0.0146) | |||
|
| |||
| Midwest | −0.016 | ||
| (0.0195) | |||
|
| |||
| Constant | −0.480*** | −0.775*** | −0.433*** |
| (0.0725) | (0.0895) | (0.1387) | |
|
| |||
| N | 27,123 | 15,539 | 7,903 |
Source: 2003 and 2008 POF.
Differences across BMI Percentiles: Overall Country and within Regions
Table 5 shows results from quantile regression models for the whole country and separately by region. We estimated the relationship between family SES and adolescent BMI via quantile regression, which allows for the magnitude of the effect of family SES to vary according to the percentile of the adolescent’s BMI, determining whether the strength of this correlation appears to be largest at lower or higher levels of BMI. Columns 1–4 show results for the entire country, while columns 5–8 show results for the Northern regions and columns 9–12 show results for the Southern regions. The adolescent BMI z-scores range from −7.07 to 4.00. It is important to note that, following the definition presented by the World Health Organization, adolescents can be classified into five categories: severe thinness (z < −3), thinness (z < −2), normal weight (z > = −2 and < = 1), overweight (z > 1), and obese (z > 2).9 This means that to evaluate the impact of a one-unit change in the independent variables, we need to take into account the percentile of BMI we are looking at. We discuss the results in terms of both coefficients and predicted BMI z-scores (presented in table 1a in the appendix).
Table 5.
Results from Quantile Regression Models of Adolescent Ages 12–17, BMI Percentiles by Regions: Brazil, 2003–2008
| Brazil |
Northern regions (NNE) |
Southern regions (SSE) |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| q03 |
q50 |
q85 |
q97 |
q03 |
q50 |
q85 |
q97 |
q03 |
q50 |
q85 |
q97 |
|
| BMI z-score | Column1 | Column2 | Column3 | Column4 | Column5 | Column6 | Column7 | Column8 | Column9 | Column10 | Column11 | Column12 |
| Log of per capita household income | 0.024 | 0.044*** | 0.049*** | 0.065*** | −0.000 | 0.042*** | 0.061*** | 0.077** | 0.137*** | 0.062*** | 0.036 | 0.058 |
| (0.0256) | (0.0086) | (0.0124) | (0.0208) | (0.0286) | (0.0102) | (0.0153) | (0.0310) | (0.0407) | (0.0191) | (0.0250) | (0.0434) | |
|
| ||||||||||||
| Parental education (HS or more) | −0.011 | 0.071*** | 0.059** | 0.021 | −0.003 | 0.098*** | 0.092*** | 0.031 | −0.077 | 0.032 | 0.037 | 0.006 |
| (0.0405) | (0.0191) | (0.0243) | (0.0415) | (0.0636) | (0.0221) | (0.0316) | (0.0639) | (0.0665) | (0.0357) | (0.0446) | (0.0825) | |
|
| ||||||||||||
| Age in years | −0.025*** | 0.001 | −0.003 | 0.001 | −0.001 | 0.014*** | 0.011 | 0.004 | −0.058*** | −0.012 | −0.019* | 0.003 |
| (0.0098) | (0.0041) | (0.0053) | (0.0099) | (0.0133) | (0.0046) | (0.0068) | (0.0131) | (0.0151) | (0.0085) | (0.0097) | (0.0211) | |
|
| ||||||||||||
| Sex (male omitted) | −0.015 | −0.006 | 0.008 | 0.036 | 0.043 | 0.043** | 0.041 | 0.053 | −0.028 | −0.076*** | 0.013 | −0.045 |
| (0.0341) | (0.0139) | (0.0194) | (0.0366) | (0.0486) | (0.0177) | (0.0247) | (0.0516) | (0.0549) | (0.0293) | (0.0334) | (0.0732) | |
|
| ||||||||||||
| Parental obesity (none is overweight or obese omitted) | ||||||||||||
|
| ||||||||||||
| Only father overweight or obese | 0.315*** | 0.166*** | 0.234*** | 0.334*** | 0.322*** | 0.157*** | 0.177*** | 0.249*** | 0.328*** | 0.188*** | 0.335*** | 0.512*** |
| (0.0500) | (0.0200) | (0.0251) | (0.0433) | (0.0686) | (0.0235) | (0.0300) | (0.0624) | (0.0999) | (0.0434) | (0.0491) | (0.0985) | |
|
| ||||||||||||
| Only mother overweight or obese | 0.293*** | 0.194*** | 0.201*** | 0.406*** | 0.250*** | 0.210*** | 0.181*** | 0.379*** | 0.383*** | 0.134*** | 0.230*** | 0.461*** |
| (0.0496) | (0.0195) | (0.0268) | (0.0470) | (0.0697) | (0.0231) | (0.0353) | (0.0609) | (0.0851) | (0.0437) | (0.0528) | (0.1119) | |
|
| ||||||||||||
| Both overweight or obese | 0.574*** | 0.462*** | 0.562*** | 0.753*** | 0.605*** | 0.440*** | 0.498*** | 0.627*** | 0.545*** | 0.481*** | 0.729*** | 0.907*** |
| (0.0468) | (0.0190) | (0.0266) | (0.0465) | (0.0606) | (0.0233) | (0.0342) | (0.0658) | (0.0897) | (0.0374) | (0.0472) | (0.0866) | |
|
| ||||||||||||
| Healthy food index | −0.016 | −0.030 | −0.052* | 0.024 | −0.009 | −0.040 | −0.053 | −0.001 | −0.129 | −0.045 | −0.101* | 0.057 |
| (0.0493) | (0.0245) | (0.0293) | (0.0549) | (0.0722) | (0.0289) | (0.0395) | (0.0730) | (0.0908) | (0.0458) | (0.0586) | (0.1162) | |
|
| ||||||||||||
| Race (nonwhite omitted) | 0.020 | −0.004 | −0.006 | −0.052 | 0.026 | −0.037* | −0.022 | −0.033 | 0.017 | 0.053* | −0.007 | −0.085 |
| (0.0379) | (0.0178) | (0.0227) | (0.0390) | (0.0590) | (0.0207) | (0.0278) | (0.0584) | (0.0631) | (0.0313) | (0.0370) | (0.0817) | |
|
| ||||||||||||
| Urban or rural area? (rural omitted) | −0.116*** | −0.031** | 0.047** | 0.133*** | −0.166*** | −0.013 | 0.040 | 0.172*** | −0.023 | −0.079** | 0.043 | 0.089 |
| (0.0384) | (0.0155) | (0.0203) | (0.0361) | (0.0542) | (0.0192) | (0.0274) | (0.0473) | (0.0690) | (0.0336) | (0.0406) | (0.0792) | |
|
| ||||||||||||
| Year (2003 omitted) | 0.159*** | 0.111*** | 0.107*** | 0.139*** | 0.159*** | 0.097*** | 0.090*** | 0.093** | 0.167*** | 0.166*** | 0.131*** | 0.127* |
| (0.0347) | (0.0154) | (0.0192) | (0.0329) | (0.0485) | (0.0173) | (0.0257) | (0.0464) | (0.0586) | (0.0308) | (0.0355) | (0.0740) | |
|
| ||||||||||||
| Region (Southern regions omitted) | ||||||||||||
|
| ||||||||||||
| Northern regions | −0.109*** | −0.126*** | −0.153*** | −0.176*** | ||||||||
| (0.0406) | (0.0179) | (0.0261) | (0.0434) | |||||||||
|
| ||||||||||||
| Midwest | −0.058 | 0.003 | −0.024 | −0.022 | ||||||||
| (0.0543) | (0.0246) | (0.0326) | (0.0580) | |||||||||
|
| ||||||||||||
| Constant | −1.850*** | −0.536*** | 0.391*** | 0.893*** | −2.132*** | −0.843*** | −0.012 | 0.630** | −2.223*** | −0.453*** | 0.653*** | 0.889** |
| (0.2061) | (0.0800) | (0.1071) | (0.2050) | (0.2813) | (0.0918) | (0.1341) | (0.2635) | (0.3435) | (0.1698) | (0.2041) | (0.4192) | |
|
| ||||||||||||
| N | 27,123 | 27,123 | 27,123 | 27,123 | 15,539 | 15,539 | 15,539 | 15,539 | 7,903 | 7,903 | 7,903 | 7,903 |
Source: 2003 and 2008 POF.
The results for the entire country in table 5 indicate that among adolescents considered normal weight, overweight, and obese, higher levels of income are associated with significantly higher BMI (coefficients of 0.044, 0.049, and 0.065, shown in columns 2–4). The association is statistically insignificant among underweight adolescents. Further results from table 5 also indicate that the association between family SES and BMI differs depending on the percentile examined: having a high school–educated parent is associated with higher BMI among normal-weight and overweight adolescents (coefficients of 0.071 and 0.059, shown in columns 2 and 3), but does not seem to matter for underweight or obese adolescents, as indicated by the lack of statistically significant coefficients for those groups. The predicted probabilities (shown in table 1 in the appendix) also show that the association between parental education and adolescent BMI is positive only until the college level—for adolescents with college-educated parents, the association is negative, suggesting that higher levels of parental education imply lower BMI. Combined, these findings lend support for Hypothesis 2 in that the associations between family SES and BMI differ according to the BMI percentile examined.
A more complex picture emerges when comparing the associations between family SES and adolescent BMI across regions while at the same time considering variation according to the BMI percentile. Among underweight adolescents in Northern Brazil (column 5), family SES (both household income and parental education) is not statistically associated with BMI, with coefficients approaching zero. In Southern Brazil, on the other hand, higher levels of household income are associated with higher BMI (coefficient 0.137 statistically significant at the 0.01 level; column 9) among underweight adolescents, lending partial support to Hypothesis 3.
The regional differences in the associations between family SES and adolescent body weight are stark among overweight and obese adolescents, lending support to Hypothesis 4. Higher levels of income are associated with higher BMI among overweight and obese adolescents in the North (0.061 and 0.077, statistically significant at the 0.01 level, columns 7 and 8), providing support for Hypothesis 4a; in line with Hypothesis 4b, the analogous coefficients for the South are half the magnitude and statistically insignificant (columns 11 and 12). A similar pattern of regional differences emerges when we consider parental education: positive, statistically significant coefficients (0.092, shown in column 7) for the North, and statistically insignificant coefficients approaching for the South (columns 11 and 12). Also worth noting, having obese parents is associated with higher BMI among all adolescents, suggesting the importance of controlling for parental body mass status.
Regional Differences in the Associations between Family Income and Parental Education
Figure 110 portrays the distinct regional patterns of the association between family income and adolescent BMI described above: regional differences are large in percentiles at the extremes of the distribution of BMI, particularly among underweight, overweight, and obese adolescents, but are small in the range considered normal weight. Among underweight adolescents, the association is larger (and statistically significant) in the Southern than in the Northern regions, with a difference in coefficients statistically significant at the 0.01 level. Among the overweight and obese group of adolescents, income has little impact on BMI in the more developed Southern regions, with statistically insignificant coefficients, but is positively and statistically associated with BMI in the less developed Northern regions. These regional differences are masked in the results of the OLS model (also shown in figure 1) and the full-country analysis, both of which obscure important nuances in the association between family SES and adolescent BMI.
Figure 1.
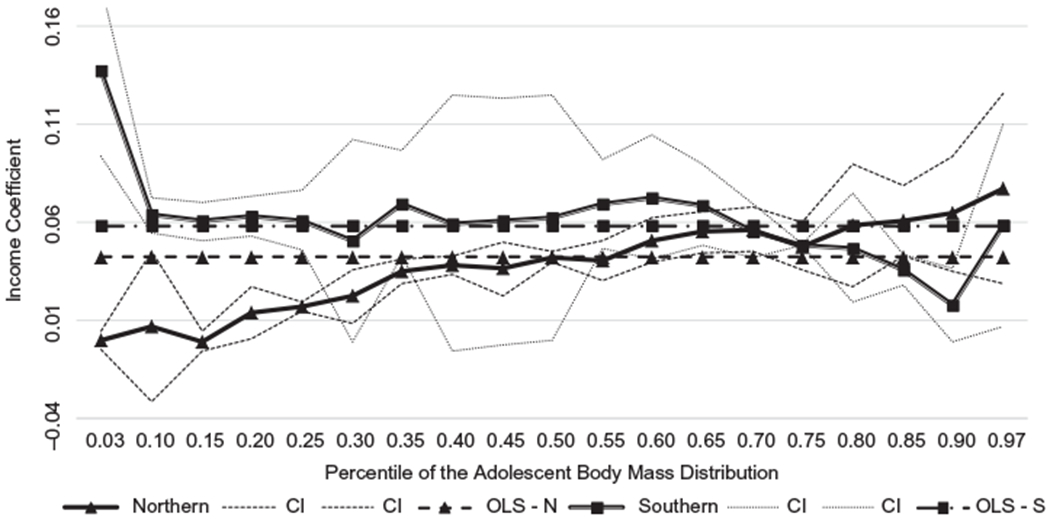
Quantile estimates of per capita family income on adolescent body mass, Brazil’s regions
Figure 2 plots the quantile regression coefficients of parental education for all percentiles of adolescent BMI. While the association between parental education and adolescent BMI follows the same overall pattern in both regions, in the more developed Southern region, the negative association between family SES and adolescent BMI fades in the 97th percentile of the distribution, with the coefficient reaching zero.
Figure 2.
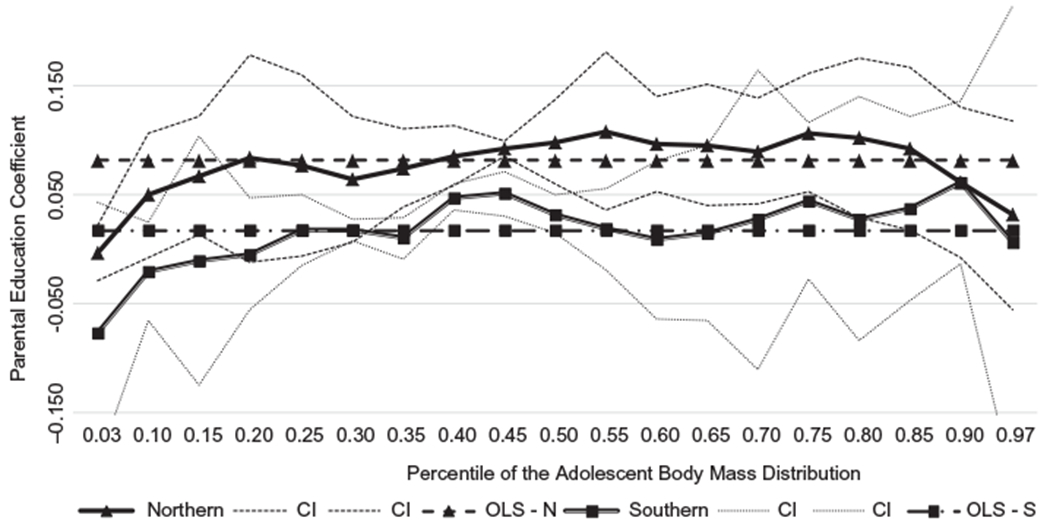
Quantile estimates of parental education on adolescent body mass, Brazil’s regions
The findings described above are in line with Hypothesis 5 in that regional differences in the curves defining the association between parental education and BMI are less pronounced than the regional differences in the curves defining the associations between family income and BMI. The curves representing the associations between family income and BMI in the North and in the South cross when reaching overweight and obese adolescents. The analogous curves representing parental education follow a similar pattern across regions, with differences only in the magnitude of the association. This suggests that it is important to consider multiple forms of family SES.
Additional findings (table 1a) present the predicted estimates of BMI z-scores, and these results highlight one additional important pattern: while parental education is positively associated with BMI for almost all groups of adolescents, the association is negative among adolescents with college-educated parents. In Northern Brazil, with all other controls at the mean, the estimated BMI z-score is 1.9312 for adolescents with high school–educated parents and 1.8313 for adolescents with college-educated parents; the corresponding values for Southern Brazil are 2.0827 and 1.9395.
Discussion and Conclusion
Socioeconomic development and the nutrition transition in Brazil have spawned profound changes that are reshaping both the overall distribution and the social patterning of BMI in the country. Once concentrated among the affluent classes, overweight and obesity are now increasingly becoming a burden of the poor, at least among Brazilian adults (Monteiro, Conde, and Popkin 2001). Despite evidence of an emerging negative SES gradient in BMI among adults, little is known about such patterns for adolescents, a group at risk for enduring the lifelong disadvantages associated with obesity. Regional disparities in this stage of the nutrition transition and levels of socioeconomic development and a changing BMI percentile distribution provide a unique opportunity to examine how the association between family SES and adolescent BMI is unfolding in a developing country still in the midst of its nutrition transition.
The goal of this paper was to examine how family SES and adolescent BMI intertwine in Brazil, a highly unequal country with stark regional disparities in the nutrition transition and socioeconomic development and with shifting SES gradients in BMI. Guided by expectations derived from nutrition transition and fundamental cause theories, we examined how the association between family SES and adolescent BMI is conditioned by regions marked by different levels of economic development and stage of the nutrition transition and by BMI percentile. Using nationally representative data with measured height and weight of all family members in Brazil’s distinct Northern and Southern regions, we conducted OLS and quantile regression models that revealed four key findings about variation in the association between family SES and adolescent BMI by region and by BMI percentile. First, we found that the overall association between family SES and adolescent BMI is positive in Brazil, as might be expected for a country still undergoing the nutrition transition. Second, we showed that the positive association between family income and BMI holds in both Northern and Southern Brazil, but that the association between parental education and family BMI differs across regions, remaining positive in Northern Brazil but losing magnitude and significance in Southern Brazil. Third, we found evidence that the associations between family SES and adolescent BMI vary across the spectrum of BMI percentiles. Fourth, we found that regional differences in the family SES-BMI association were less pronounced for parental education than for family income.
As one of the first studies to provide a detailed portrait of heterogeneity in the association between family SES and adolescent BMI in Brazil, this work makes at least three key conceptual contributions to the literature on socioeconomic inequality and health outcomes everywhere. The first contribution is evidence that the association between family SES and adolescent BMI varies according to contextual environments, that is, by regions marked by differences in the nutrition transition and levels of socioeconomic development. Although the overall association between family SES (both parental education and family income) and adolescent BMI is positive, reflecting Brazil’s status as a country still in the midst of its nutrition transition, the regional differences in this association suggest that SES gradients in adolescent BMI are conditioned by the stage of the nutrition transition and level of socioeconomic development of the regions in which adolescents live.
The second, key contribution is that whereas most prior studies of SES and BMI have focused on obesity, we focused on percentiles in the entire range of the BMI distribution. Findings underscore important differences in the associations between family SES and adolescent body weight related to the BMI percentile examined and emphasize the value of considering that the way in which family SES influences adolescent BMI varies according to the BMI status examined. The results suggest that in some cases, estimates of the determinants of adolescent BMI produced by OLS regression models, which estimate the associations at the mean, can be misleading. For example, the overall OLS estimates in the analysis indicate that both family income and parental education are positively associated with adolescent BMI; however, the quantile regression estimates show that the associations are not always positive or statistically significant for all BMI percentiles.
Moreover, the magnitude of the impact of family SES on BMI can vary significantly according to the BMI percentile, suggesting that the SES gap in BMI varies. This is in line with the idea that the socioeconomic gradients in adolescent BMI vary according to BMI status (Classen 2010; Costa-Font and Gil 2013), supporting our second hypothesis. The positive association between family income and BMI among underweight and normal-weight adolescents in Southern Brazil and the increases in the association at higher BMI percentile cutoffs in Northern Brazil, for example, suggest that the mechanism underlying the association is an increasing ability to purchase food but, importantly, not necessarily nutritious and healthy food. For underweight adolescents in Northern Brazil, family SES in the form of either parental education or family income is not a significant determinant of adolescent BMI, suggesting that income-generating interventions, while important for many adolescent economic and social outcomes, are unlikely to be effective in raising the BMI levels of those at greatest risk of undernutrition. In Southern Brazil, in contrast, the results reveal a significant association between family income and BMI among underweight adolescents (Hypothesis 3).
Findings also point to important regional differences in the associations between family SES and adolescent BMI among overweight and obese adolescents (Hypothesis 4). Our findings show that family SES is associated with higher BMI among overweight and obese adolescents in Northern Brazil, where the nutrition transition is at earlier stages (Hypothesis 4a), but the associations are statistically insignificant in Southern Brazil, where the nutrition transition is more advanced (Hypothesis 4b). However, the finding that income is positively associated with BMI among underweight and normal weight adolescents in Southern Brazil complicates this picture and suggests that even this more socioeconomically developed region of the country is still undergoing the nutrition transition. Overall, these results provide a picture of a society in transition, where family SES is associated with different BMI statuses depending on the context in which such associations are embedded. For example, in Northern regions, the gap in BMI between adolescents in families with higher income and those in families with lower income is more pronounced among overweight and obese adolescents than among underweight or normal weight adolescents. In this part of the country, lower SES “protects” overweight and obese adolescents from BMI increases. In the Southern region, however, there is no socioeconomic gradient (for either family income or parental education) in BMI among overweight and obese adolescents. This pattern suggests that the positive association between SES and BMI among overweight and obese adolescents may fade as regions develop and move along the nutrition transition. With the progression of the nutrition transition and greater socioeconomic development, families with low incomes and low levels of education may become disproportionately exposed and vulnerable to obesogenic environments in which less healthy, low-cost food options are likely the default choice available.
The third main contribution is evidence that region and BMI status influence the relative importance of family income and parental education for predicting adolescent BMI. Among underweight adolescents in Southern Brazil, family income rather than parental education is the key underlying SES factor affecting adolescent BMI. It is likely that the mechanism behind the association in these families is simply the ability to purchase food. Prior studies have found a similar positive association between income and adolescent BMI (Haas et al. 2003). Among overweight and obese adolescents, however, parental education and income are equally important for BMI in Northern Brazil but not in Southern Brazil. The study provides additional evidence that the association between family SES and BMI varies according to whether family SES reflects financial resources or parental education.
Taken together, findings from this study provide an important illustration of the evolution of social position as a fundamental cause of health in a middle-income country undergoing the nutrition transition. The evidence that SES gradients in adolescent BMI differ across regions marked by different stages of the nutrition transition and socioeconomic development and across BMI percentiles points to a potential reshaping of the social patterning of adolescent BMI in Brazil. Our findings do not clearly support FCT, in that we did not find evidence of a negative SES gradient in adolescent BMI (in which lower parental education level and lower family income are associated with higher BMI). However, it is possible, and perhaps even likely, that such a gradient will emerge over time. As the nutrition transition progresses and the risks of overweight and obesity become more common and well known, the burden of these health conditions may begin to fall disproportionately on adolescents from families with low SES who, unlike adolescents from families with high SES, have fewer resources available to combat such risks.
Given that adolescent obesity can carry a host of lifelong negative health and social consequences, monitoring trends in this association in Brazil and in other middle- and low-income countries still undergoing the nutrition transition represents a critical, ongoing task for future research. For such research, our study highlights the utility of fundamental cause framework and a methodological approach that anticipates variations in the SES-BMI association based on macrosocial contexts and BMI percentile, in addition to the dimension of family SES examined. This type of framework and approach would be useful for examining not only the association between SES and BMI or obesity, but also the SES patterning of the uptake of new obesity prevention or reduction interventions, technologies, and behaviors in Brazil and in other low- and middle-income countries. Such work is needed to better elucidate how family SES shapes access and utilization of health resources among adolescents in contexts of high social inequality and undergoing significant nutritional and epidemiological change.
Biographies
Létícia J. Marteleto is Associate Professor of Sociology and Faculty Research Associate of the Population Research Center at the University of Texas at Austin. Research interests include social demography, education and health inequality in an international comparative perspective. Recent work has appeared in Demography, Social Forces, and Research in Social Stratification and Mobility.
Luiz C. D. Gama is a PhD candidate in the Economics Department at the Federal University of Minas Gerais and a lecturer at the Federal Center for Technological Education of Minas Gerais/Brazil. His research focuses on labor economics, applied econometrics, and social mobility.
Molly Dondero is Assistant Professor of Sociology at American University. Research interests include international migration, immigrant integration, race/ethnicity, health, and inequality. Recent publications have appeared in Demography, Population Research and Policy Review, and Social Science and Medicine.
Letisha E. C. Brown is a PhD candidate in the Sociology Department at the University of Texas at Austin. Her research focuses on race, social ties, and food practices. Recent work has appeared in the South African Review of Sociology.
Appendix
Table 1a.
Estimated Adolescent BMI Z-Score by Measures of Family Socioeconomic Status, Brazil and Regions
| Parental education |
Per capita family income |
Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤4 |
>4 & ≤8 |
>8 & ≤11 |
>11 & < = 15 |
>15 |
≤115 |
>115 & ≤200 |
>200 & ≤320 |
>320 & < = 600 |
>600 |
|||
| Column 1 | Column 2 | Column 3 | Column 4 | Column 5 | Column 6 | Column 7 | Column 8 | Column 9 | Column 10 | |||
| Q3 | Brazil | −1.8701 | −1.8146 | −1.8066 | −1.7413 | −1.8680 | −1.9430 | −1.8654 | −1.8249 | −1.7796 | −1.7425 | −1.8296 |
|
| ||||||||||||
| NNE | −1.8871 | −1.8617 | −1.8546 | −1.8203 | −1.9770 | −1.9324 | −1.8885 | −1.8623 | −1.8323 | −1.8311 | −1.8686 | |
|
| ||||||||||||
| SSE | −1.8807 | −1.7740 | −1.7617 | −1.6358 | −1.7625 | −2.0036 | −1.8661 | −1.7979 | −1.7260 | −1.6302 | −1.8021 | |
|
| ||||||||||||
| Q50 | Brazil | −0.1095 | −0.0485 | 0.0446 | 0.1344 | 0.0301 | −0.1767 | −0.0941 | −0.0402 | 0.0205 | 0.1048 | −0.0351 |
|
| ||||||||||||
| NNE | −0.1570 | −0.1118 | −0.0084 | 0.0631 | −0.0367 | −0.2081 | −0.1403 | −0.0943 | −0.0436 | 0.0257 | −0.0904 | |
|
| ||||||||||||
| SSE | −0.0492 | 0.0158 | 0.0804 | 0.1774 | 0.0451 | −0.1248 | −0.0383 | 0.0146 | 0.0756 | 0.1557 | 0.0186 | |
|
| ||||||||||||
| Q85 | Brazil | 0.8541 | 0.9494 | 1.0334 | 1.1348 | 1.0354 | 0.7701 | 0.8758 | 0.9441 | 1.0181 | 1.1158 | 0.9473 |
|
| ||||||||||||
| NNE | 0.7867 | 0.8588 | 0.9751 | 1.0671 | 0.9735 | 0.7200 | 0.8091 | 0.8700 | 0.9369 | 1.0315 | 0.8758 | |
|
| ||||||||||||
| SSE | 0.9474 | 1.0396 | 1.1141 | 1.1870 | 1.0402 | 0.8853 | 0.9761 | 1.0347 | 1.0963 | 1.1575 | 1.0320 | |
|
| ||||||||||||
| Q97 | Brazil | 1.6940 | 1.8225 | 1.9182 | 2.0282 | 1.8908 | 1.5892 | 1.7288 | 1.8144 | 1.9022 | 2.0058 | 1.8111 |
|
| ||||||||||||
| NNE | 1.6313 | 1.7453 | 1.8378 | 1.9312 | 1.8313 | 1.5412 | 1.6658 | 1.7415 | 1.8156 | 1.9107 | 1.7376 | |
|
| ||||||||||||
| SSE | 1.8103 | 1.9242 | 1.9990 | 2.0827 | 1.9395 | 1.7110 | 1.8446 | 1.9179 | 1.9927 | 2.0665 | 1.9091 | |
Footnotes
Hereafter, we refer to North and Northeast Brazil as Northern Brazil, and South and Southeast Brazil as Southern Brazil.
Trained interviewers used calibrated portable scales to obtain weight measurements of respondents wearing light clothes and no shoes. During height measurements, respondents did not wear shoes and their heads were held in the Frankfort plane (Monteiro et al. 2000).
We excluded 401 adolescents with a reported weight lower than 5 kg, because it is implausible. We considered only adolescents with valid information about father or mother’s education, and information about family income. As usual in studies using data from household surveys, only those classified as children of the head of the family are included in the sample.
The Midwest does not present a clear pattern of socioeconomic development or stages of the nutrition transition since it encompasses both the nation’s capital—with one of the country’s highest per capita income, Brasília—and areas that are not as economically developed, as Southern Brazil. Past research has compared Northern and Southern Brazil in a similar way (Monteiro et al. 1995; Marteleto and Souza 2012).
The authors assume an underlying skewed normal distribution of the measurement, so that a suitable power transformation will result in a normally distributed variable. In the method proposed, the distribution at each covariate value is summarized by three parameters—the median, the coefficient of variation, and skewness, the latter expressed as a Box-Cox power. These three parameters are constrained to change smoothly as the covariate changes. The BMI z-score for an individual of sex s and age t is calculated as , where L is the Box-Cox power, M is the median, and S is the coefficient of variation.
We also tested other specifications of parental education, such as years of schooling and highest level of schooling between parents; the overall pattern of results did not change.
In factor analysis, factors are created as hypothetical variables, and they are linear combinations of observed variables that explain the variability of the data. Specifically, PCF, it is expected that most variables are highly correlated to the first factor. Since the first component is the most important, we used it to create our index.
The results support our justification for examining adolescent body mass separately by region: the BMI z-score distributions for the two regions are so different that they never intersect (available upon request).
In our descriptive analyses, we aggregated adolescents considered severely thin and thin in one category, called underweight.
Contributor Information
Letícia J. Marteleto, Associate Professor of Sociology and Faculty Research Associate of the Population Research Center at the University of Texas at Austin
Luiz C. D. Gama, PhD candidate in the Economics Department at the Federal University of Minas Gerais and a lecturer at the Federal Center for Technological Education of Minas Gerais/Brazil
Molly Dondero, Assistant Professor of Sociology at American University.
Letisha E. C. Brown, PhD candidate in the Sociology Department at the University of Texas at Austin
References
- Balistreri KS, and Van Hook J. 2009. “Socioeconomic Status and Body Mass Index Among Hispanic Children of Immigrants and Children of Natives.” American Journal of Public Health 99(12):2238—46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beyerlein A, Toschke AM, and von Kries R. 2010. “Risk Factors for Childhood Overweight: Shift of the Mean Body Mass Index and Shift of the Upper Percentiles: Results from a Cross-Sectional Study.” International Journal of Obesity 34:642–48. [DOI] [PubMed] [Google Scholar]
- Buchinsky M 1994. “Changes in the US wage structure 1963–1987: Application of quantile regression.” Econometrica : Journal of the Econometric Society 62:405–58. [Google Scholar]
- Carr D, and Umberson D. 2013. “The Psychology of Stress, Health and Coping.” In The Handbook of Social Psychology, 2nd ed. edited by Delamater J and Ward A, 465–87. [Google Scholar]
- Cawley J 2004. “The Impact of Obesity in Wages.” Journal of Human Resources 39(2):451–74. [Google Scholar]
- Classen TJ 2010. “Measures of the Intergenerational Transmission of Body Mass Index between Mothers and Their Children in the United States, 1981–2004.” Economic & Human Biology 8(1):30–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole TJ 1988. “Fitting Smoother Centile Curves to Reference Data (with Discussion).” JRSS A 151:385–418. [Google Scholar]
- Cole TJ, and Green PJ. 1992. “Smoothing Reference Centile Curves: The LMS Method and Penalized Likelihood.” Statistical Methodology 11(10):1305–19. [DOI] [PubMed] [Google Scholar]
- Costa-Font J, Fabbri D, and Gil J. 2009. “Decomposing Body Mass Index Gaps between Mediterranean Countries: A Counterfactual Quantile Regression Analysis.” Economics & Human Biology 7(3):351–65. [DOI] [PubMed] [Google Scholar]
- Costa-Font Joan, and Gil Joan. 2013. “Intergenerational and Socioeconomic Gradients of Child Obesity.” Social Science and Medicine 93:29–37. [DOI] [PubMed] [Google Scholar]
- Diniz CC, 2002. “A nova configuração urbano-industrial no Brasil.” In Unidade e fragmentação: a questão regional no Brasil, edited by Kon Anita. São Paulo: Col. Debates. Editora Perspectiva. [Google Scholar]
- Dinsa GD, Goryakin E, Fumagalli E, and Suhrcke M. 2012. “Obesity and Socioeconomic Status in Developing Countries: A Systematic Review.” Obesity Review 13:1067–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freese J, and Lutfey K. 2011. “Fundamental Causality: Challenges of an Animating Concept for Medical Sociology.” In The Handbook of the Sociology of Health, Illness, and Healing, edited by Pescosolido B, Martin J, McLeod J, and Rogers A, 67–81. New York: Springer. [Google Scholar]
- Glass CM, Haas SA, and Reither EN. 2010. “The Skinny on Success: Body Mass, Gender and Occupational Standing across the Life Course.” Social Forces 88(4):1777—806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodman E 1999. “The Role of Socioeconomic Status Gradients in Explaining Differences in US Adolescents’ Health.” American Journal of Public Health 89:1522–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodman E, Slap GB, and Huang Bin. 2003. “The Public Health Impact of Socioeconomic Status on Adolescent Depression and Obesity.” American Journal of Public Health 93(11):1844–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gordon-Larsen P, Adair LS, and Popkin BM. 2003. “The Relationship of Ethnicity, Socioeconomic Factors, and Overweight in U.S. Adolescents.” Obesity Research 11(1):121–29. [DOI] [PubMed] [Google Scholar]
- Haas JS, Lee LB, Kaplan CP, Sonnerborn D, Phillips KA, and Liang Su-Ying. 2003. “The Association of Race, Socioeconomic Status and Health Insurance Status with the Prevalence of Overweight among Children and Adolescents.” American Journal of Public Health 93(12):2105–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- IBGE. 2010. “Antropometria e Estado Nutricional de Crianças, Adolescentes e Adultos no Brasil.” Pesquisa de Orçamentos Domiciliares 2008–2009. [Google Scholar]
- Koenker R, and Bassett Gilbert Jr. 1978. “Regression Quantiles.” Econometrica: Journal of the Econometric Society 46(1):33–50. [Google Scholar]
- Koenker R, and Hallock KF. 2001. “Quantile Regression.” Journal of Economic Perspectives 15(4):143–56. [Google Scholar]
- Krishna A, Razak F, Lebel A, Smith GD, and Subramanian SV. 2015. “Trends in Group Inequalities and Interindividual Inequalities in BMI in the United States, 1993–2012.” American Journal of Clinical Nutrition 101(3):598–605. [DOI] [PubMed] [Google Scholar]
- Link BG, and Phelan J. 1995. “Social Conditions as Fundamental Causes of Disease.” Journal of Health and Social Behavior Spec No:80–94. [PubMed] [Google Scholar]
- Ljungvall A, and Zimmerman FJ. 2012. “Bigger Bodies: Long-Term Trends and Disparities in Obesity and Body-Mass index among U.S. Adults, 1960–2008.” Social Science & Medicine 75(1):109–19. [DOI] [PubMed] [Google Scholar]
- Marteleto L, and Souza L. 2012. “The Impact of Family Size on Children’s Educational Attainment over Time: Assessing the Exogenous Variation in Fertility using Twins in Brazil.” Demography 49(4): 1453–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin MA, 2008. “The Intergenerational Correlation in Weight: How Genetic Resemblance Reveals the Social Role of Families.” American Journal of Sociology 114(Suppl.):S67–S105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin MA, Frisco ML, Nau C, and Burnett K. 2012. “Social Stratification and Adolescent Overweight in the United States: How Income and Educational Resources Matter across Families and Schools.” Social Science and Medicine 74(4):597–606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mirowsky J, and Ross CE. 2003. Education, Social Status, and Health. New York: A. de Gruyter. [Google Scholar]
- Monteiro CA, Benicio MDA, Conde WL, and Popkin BM. 2000. “Shifting obesity trends in Brazil.” European Journal of Clinical Nutrition 54(4):342–6. [DOI] [PubMed] [Google Scholar]
- Monteiro CA, Benicio MH, Iunes R, Gouveia NC, Taddei JA, and Cardoso MA. 1992. “National Status of Brazilian Children: Trends from 1975–1989.” Bulletin of the World Health Organization 70(5): 657–66. [PMC free article] [PubMed] [Google Scholar]
- Monteiro CA, Conde WL, and Popkin BM. 2001. “Independent Effects of Income and Education on the Risk of Obesity in the Brazilian Adult Population.” Journal of Nutrition 131(3):8815–65. [DOI] [PubMed] [Google Scholar]
- ––––––. 2002. “Is obesity replacing or adding to undernutrition? Evidence from different social classes in Brazil.” Public Health Nutrition 5(1A):105–12. [DOI] [PubMed] [Google Scholar]
- ––––––. 2007. “Income-Specific Trends in Obesity in Brazil: 1975–2003.” American Journal of Public Health 97(10)1808–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monteiro CA, D’Aquino MH, Conde WL, et al. 2010. “Narrowing Socioeconomic Inequality in Child Stunting: The Brazilian Experience (1974–2007).” Bulletin of the World Health Organization 88(4): 305–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monteiro CA, Lvey RB, Claro RM, Castor IR, and Cannon G. 2010. “A New Classification of Foods Based on the Extent and Purpose of Their Processing.” Cadernos de Saude Publica 26(11):2039–49. [DOI] [PubMed] [Google Scholar]
- Monteiro CA, Mondini L, de Souza AL, and Popkin BM. 1995. “The Nutrition Transition in Brazil.” European Journal of Clinical Nutrition 49(2):105—13. [PubMed] [Google Scholar]
- Monteiro CA, Moura EC, Conde WL, and Popkin BM. 2004. “Socioeconomic Status and Obesity in Adult Populations of Developing Countries.” Bulletin of the World Health Organization 82(12): 940–46. [PMC free article] [PubMed] [Google Scholar]
- Moubarac JC, Batal M, Martins APB, Claro R, Levy RB, Cannon G, and Monteiro C. 2014. “Processed and ultra-processed food products: consumption trends in Canada from 1938 to 2011.” Canadian Journal of Dietetic Practice and Research 75(1):15–21. [DOI] [PubMed] [Google Scholar]
- Naccarato P, and Lebesco K. 2012. Culinary Capital. New York: Berg. [Google Scholar]
- Ng M, et al. 2014. “Global, Regional, and National Prevalence of Overweight and Obesity in Children during 1980–2013: A Systematic Analysis for the Global Burden of Disease Study.” The Lancet 384 (9945):766–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, and Flegal KM. 2006. “Prevalence of Overweight and Obesity in the United States, 1999–2004.” JAMA: The Journal of the American Medical Association 295:1549–55. [DOI] [PubMed] [Google Scholar]
- Omran AR, 1971. “The Epidemiologic Transition: A Theory of the Epidemiology of Population Change.” Milbank Memorial Fund Quarterly 49:509–38. [PubMed] [Google Scholar]
- Phelan JC, and Link BG. 2005. “Controlling Disease and Creating Disparities: A Fundamental Cause Perspective.” Journal of Gerontology: Psychological Sciences and Social Sciences 60(2):S27–33. [DOI] [PubMed] [Google Scholar]
- Phelan JC, Link BG, Diez-Roux A, Kawachi I, and Levin B. 2004. “Fundamental Causes of Social Inequalities in Mortality: A Test of the Theory.” Journal of Health and Social Behavior 45(3):265–85. [DOI] [PubMed] [Google Scholar]
- Popkin BM 1993. “Nutritional Patterns and Transitions.” Population and Development Review 19: 138–57. [Google Scholar]
- ––––––. 1994. “The nutrition transition in low-income countries: an emerging crisis.” Nutrition Reviews 52(9):285–98. [DOI] [PubMed] [Google Scholar]
- ––––––. 1999. “Urbanization, Lifestyle Changes and the Nutrition Transition.” World Development 27: 1905–16. [Google Scholar]
- Popkin BM 2001. “The nutrition transition and obesity in the developing world.” The Journal of Nutrition 131(3):871S–3S. [DOI] [PubMed] [Google Scholar]
- Popkin BM, Lu B, and Zhai F. 2002. “Understanding the Nutrition Transition: Measuring Rapid Dietary Changes in Transitional Countries.” Public Health Nutrition 4:947–53. [DOI] [PubMed] [Google Scholar]
- Previdelli AN, Caesar de Andrade S, Pires MM, Vivolo SRF, Firberg RM, and Marchioni DM. 2011. “Índice de Qualidade da Dieta Revisado (IQD-R): Desenvolvimento para aplicação na população brasileira.” Cad Saúde Publica 45(4):794–98. [Google Scholar]
- Pudrovska T, Logan E, and Richman A. 2014. “Early-Life Social Origins of Later-Life Body Weight: The Role of Socioeconomic Disadvantage and Body Mass over the Life Course.” Journal of Health and Social Behavior 55(3):283–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stifel D, and Averett S. 2009. “Childhood Overweight in the United States: A Quantile Regression Approach.” Economics in Human Biology 7(3):387–97. [DOI] [PubMed] [Google Scholar]
- Wang Y. 2001. “Cross-National Comparison of Childhood Obesity: The Epidemic and the Relationship between Obesity and Socioeconomic Status.” International Journal of Epidemiology 30(5):1129–36. [DOI] [PubMed] [Google Scholar]
- Wang Y, and Zhang Q. 2006. “Are American Children and Adolescents of Low Socioeconomic Status at Increased Risk of Obesity?” American Journal of Clinical Nutrition 84:707–16. [DOI] [PubMed] [Google Scholar]
- World Health Organization (WHO). 2007. Growth Reference Data for 5–19 Years. Geneva: WHO. [Google Scholar]
- Zhang Q, and Yang Y. 2007. “Using Concentration Index to Study Changes in Socio-Economic Inequality of Overweight among US Adolescents between 1971 and 2002.” International Journal of Epidemiology 36(4):916–25. [DOI] [PubMed] [Google Scholar]