

Key Points
-
•
In MDS, HRQoL was worse for vulnerable participants and those with worse prognosis.
-
•
Lower-risk MDS was associated with better HRQoL, but this relationship was lost among the vulnerable.
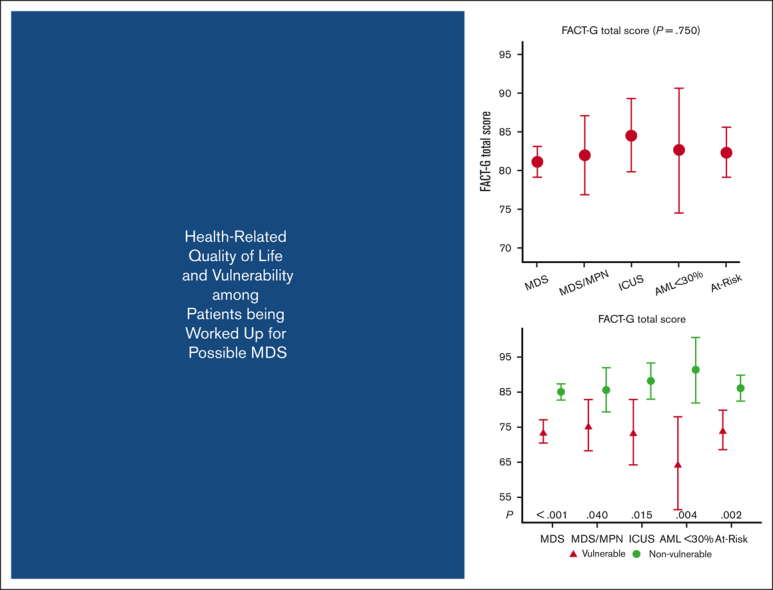
Visual Abstract
Abstract
Health-related quality of life (HRQoL) and vulnerability are variably affected in patients with myelodysplastic syndromes (MDS) and other cytopenic states; however, the heterogeneity of these diseases has limited our understanding of these domains. The National Heart, Lung, and Blood Institute-sponsored MDS Natural History Study is a prospective cohort enrolling patients undergoing workup for suspected MDS in the setting of cytopenias. Untreated patients undergo bone marrow assessment with central histopathology review for assignment as MDS, MDS/myeloproliferative neoplasm (MPN), idiopathic cytopenia of undetermined significance (ICUS), acute myeloid leukemia (AML) with <30% blasts, or “At-Risk.” HRQoL data are collected at enrollment, including the MDS-specific Quality of Life in Myelodysplasia Scale (QUALMS). Vulnerability is assessed with the Vulnerable Elders Survey. Baseline HRQoL scores from 449 patients with MDS, MDS/MPN, AML <30%, ICUS or At-Risk were similar among diagnoses. In MDS, HRQoL was worse for vulnerable participants (eg, mean Patent-Reported Outcomes Management Information Systems [PROMIS] Fatigue of 56.0 vs 49.5; P < .001) and those with worse prognosis (eg, mean Euroqol-5 Dimension-5 Level [EQ-5D-5L] of 73.4, 72.7, and 64.1 for low, intermediate, and high-risk disease; P = .005). Among vulnerable MDS participants, most had difficulty with prolonged physical activity (88%), such as walking a quarter mile (74%). These data suggest that cytopenias leading to MDS evaluation are associated with similar HRQoL, regardless of eventual diagnosis, but with worse HRQoL among the vulnerable. Among those with MDS, lower-risk disease was associated with better HRQoL, but the relationship was lost among the vulnerable, showing for the first time that vulnerability trumps disease risk in affecting HRQoL. This study is registered at www.clinicaltrials.gov as NCT02775383.
Introduction
The myelodysplastic syndromes (MDS) are hematologic malignancies characterized by abnormal blood counts that can progress to acute myeloid leukemia (AML). The median age at diagnosis is in the early 70s.1,2 The International Prognostic Scoring System (IPSS),3 and its update, the IPSS-revised (IPSS-R),4 are used to assess prognostic risk based on bone marrow findings and laboratory results. Although combination therapies, targeted treatments, and even stem cell transplantation for higher-risk disease are explored for these disorders, most patients are of advanced age and considered incurable at diagnosis. Thus, much of MDS management focuses on improving health-related quality of life (HRQoL) and function in addition to survival. Such patient-reported outcomes are variably affected, but the heterogeneous composition of disease states grouped together as “MDS” increases the difficulty of rigorously assessing them.
Given that older adults often have other reasons for cytopenias, patients with suspected MDS should have a baseline bone marrow assessment with cytogenetic and next-generation sequencing analyses to confirm their diagnosis and subtype and to aid in prognostic assessment and treatment selection.5 Unfortunately, many patients carry the diagnosis without ever having had a marrow assessment.6 In addition to confirming the diagnosis and understanding patients’ current HRQoL, a careful assessment of functional status is essential to determining whether potentially frail7 older patients with MDS can achieve the same benefits and safety of treatments studied in younger, generally more robust populations.
Although the in-person comprehensive geriatric assessment (CGA), a multidimensional clinical evaluation featuring evaluation of comorbid conditions, activities of daily living, and physical and cognitive function, has been recommended by organizations such as the American Society of Clinical Oncology to complement or replace the traditional 4-level performance status to assess functional status for older adults,8 resources for such evaluation in the contemporary oncology clinic are sparse. Although in no way a substitute for the CGA, a patient-administered questionnaire such as the Vulnerable Elders Survey (VES-13) can provide insight as to those who are “vulnerable,” defined by the creators as older persons at risk for health deterioration.9 The VES-13 has been successfully used in several hematologic oncology populations10 to provide screening for vulnerability, including non-Hodgkin lymphoma11 and patients in need of stem cell transplantation.12
Emerging evidence suggests significant associations between underlying cancer diagnoses, vulnerability, and HRQoL,13, 14, 15, 16 but the prevalence of vulnerability among patients with confirmed MDS is not known. It is also not known if vulnerability is associated with worse HRQoL or which aspect is the most affected (eg, impaired physical activity vs instrumental activities of daily living). Indeed, impairments in HRQoL that are most common in patients with MDS, such as fatigue due to anemia, patient-reported outcomes experienced as a patient with cancer, MDS-specific symptoms such as physical and emotional burden of the syndromes, and changes in life utilities, may all be associated with underlying MDS vulnerability and/or disease risk. If found, such relationships could lead to routine measurement and intervention for both vulnerability and HRQoL in this population.
We leveraged a prospective study of patients with centrally confirmed MDS and other cytopenic disorders to characterize potential HRQoL differences for patients with and without biopsy-proven MDS. We also analyzed HRQoL among MDS risk groups, hypothesizing that higher-risk diseases would be associated with worse HRQoL. Finally, we assessed the prevalence of vulnerability in all groups, factors contributing to vulnerability for those with MDS, and the potential relationship between vulnerability, HRQoL, and disease subtype.
Methods
Study design and population
The National Heart, Lung, and Blood Institute MDS Natural History Study (NCT02775383) is a prospective cohort study initiated in June 2016 enrolling patients undergoing diagnostic workup for suspected MDS or MDS/myeloproliferative neoplasms (MPNs) in the setting of cytopenias. The protocol is approved through the NCI Central Institutional Review Board, and informed consent was obtained from all patients before participation. Eligible participants are either currently undergoing diagnostic workup for suspicion of MDS or have been diagnosed with de novo or therapy-related MDS within 12 months of enrollment, have not received hematopoietic growth factors in the past 6-months, and have not received any other therapy for MDS. Untreated participants undergo bone marrow assessment with centralized histopathology review at enrollment for assignment into diagnostic subgroups for longitudinal follow-up, including MDS, MDS/MPN, idiopathic cytopenia of undetermined significance (ICUS), AML with <30% blasts not including core-binding factor mutations (chromosomal rearrangements between chromosomes 8 and 21, and within chromosome 16), as well as acute promyelocytic leukemia (including chromosomal rearrangements between chromosomes 15 and 17), or, otherwise “at-risk” (pathology assessment of dysplasia in baseline bone marrow aspirate, or any clonal abnormality by conventional karyotype), or genetic mutations meeting minimally acceptable criteria for allelic variant presence (variant allele frequency ≥2%; clonal cytopenia of undetermined significance). Participants assigned to other diagnoses (AML ≥30% blasts, nonmyeloid malignancies or other cytopenia or cancers) are enrolled into a cross-sectional cohort with no further follow-up.17 Although patients classified as ICUS or “at-risk” do not meet the minimal criteria for MDS at diagnosis, a subpopulation of these patients might acquire additional somatic gene mutations and/or cytogenetic aberrations during follow-up and/or may progress and develop definite morphologic evidence of the disease, which can provide valuable insight into associated differences in vulnerability and quality of life. Study enrollment was paused from 27 March 2020 to 18 May 2020 because of the COVID-19 pandemic.
HRQoL and vulnerability assessment
HRQoL and vulnerability data are collected at enrollment (baseline; before receipt of biopsy results) for all enrolled and at subsequent visits for longitudinal participants (HRQoL only); for this current analysis, we present only baseline results. HRQoL instruments include the MDS-specific 38-item Quality of Life in Myelodysplasia Scale (QUALMS),18 the 27-item Functional Assessment of Cancer Therapy-General form (FACT-G),19 the 7-item Patient Reported Outcomes Measurement Information System (PROMIS) Short Form-Fatigue,20 and the 5-item Euroqol EQ-5D-5L.21 The 13-item VES-139 was used to measure vulnerability.
To avoid potential effects on HRQoL due to the beginning of the COVID-19 pandemic, baseline HRQoL scores were analyzed for participants enrolled before 27 March 2020, who had available VES-13 data and who were classified as having MDS, MDS/MPN, AML <30% blasts, ICUS, or at-risk. Mean (QUALMS) or total (FACT-G, PROMIS) scores were obtained from the item-specific scores of the respective instruments. Higher values on the QUALMS mean score, FACT-G total score, and EQ-5D-5L single index score indicate better HRQoL; lower PROMIS Fatigue T-scores represent improved symptoms of fatigue. A score of 3 or more on the VES-13 total score is considered vulnerable. Additional details regarding the HRQoL instruments and scoring of the VES-13 are provided in supplemental Table 1. HRQoL scores were also analyzed by vulnerability status (vulnerable vs not vulnerable) and by MDS prognosis, grouped into very low/low, intermediate, or high/very high strata defined according to IPSS-R.4
Statistical analyses
The frequencies and proportions of discrete demographic factors, including sex, race, ethnicity, and transfusion needs, were compared between diagnostic categories using Fisher's exact test. An analysis of variance was used for comparing mean baseline characteristics, including age, body mass index, and blast percentage, between diagnostic groups. Estimates of mean HRQoL scores with 95% confidence intervals (95% CIs) were obtained from age–adjusted linear regression models of each HRQoL measure on the diagnostic categories. Age-adjusted models of the HRQoL measures, with added covariates for vulnerability status and its interaction with diagnostic category, were used to assess the effect of vulnerability on HRQoL scores.
An assessment of the linear trend of HRQoL with worsening MDS risk categories was conducted in MDS participants using linear regression models of each HRQoL score on IPSS-R strata, adjusted for age, and repeated within each vulnerability subgroup to evaluate any vulnerability impact on trend. F tests were obtained from the above regression models to test for overall differences between diagnostic categories and for overall trends in HRQoL and MDS prognosis. T tests from the above regression models were obtained to test for pairwise differences between diagnostic categories or vulnerability subgroups. The P values reported in each diagnostic category for a given HRQoL were adjusted for multiple comparisons using the Hochberg procedure, with unadjusted CIs reported. Statistical tests for different HRQoL instruments were left unadjusted because of the exploratory aim of these comparisons. A two-sided alpha of 0.05 was applied for all tests. Of the 480 participants available for analysis, only 6% (n = 31) lacked HRQoL and vulnerability data. Complete-case analysis was used for each HRQoL instrument such that only participants with available data contributed to the analysis for the given HRQoL instrument. All analyses were conducted using SAS version 9.4.
Results
Baseline characteristics
In total, 94% of registered participants (N = 449/480) enrolled for longitudinal follow-up had HRQoL and vulnerability data available. Comparing participants with and without HRQoL and vulnerability data available, there were no significant differences in any baseline characteristics, including age, body mass index, sex, race, blast percentage, and IPSS-R (within MDS and MDS/MPN). The mean (standard deviation [SD]) age was 72 (10) years, and most participants were male (68%), White (93%), and non-Hispanic or Latino (95%; Table 1). Participants were classified as having MDS (55%), MDS/MPN (9%), AML<30% blasts (3%), ICUS (11%), or at-risk (22%). Over half of MDS and MDS/MPN participants (57%) were categorized as lower-risk IPSS-R, compared with 21% intermediate- and 22% higher-risk. No patients had severe thrombocytopenia (platelets <50); patients with MDS and AML were more likely to have severe neutropenia (Absolute Neutrophil Count (ANC)<800) and anemia (Hb<8).
Table 1.
Summary of baseline characteristics by disease subgroup
| Characteristic | Statistic | MDS (N = 248) | MDS/MPN (N = 40) | ICUS (N = 48) | AML<30% (N = 15) | At-risk (N = 98) | All (N = 449) | P value |
|---|---|---|---|---|---|---|---|---|
| Age | Mean ± SD | 71.8 ± 10.1 | 76.5 ± 7.4 | 69.9 ± 12.4 | 73.1 ± 7.8 | 71.9 ± 10.6 | 72.1 ± 10.2 | .039 |
| Sex | Female, n (%) | 86 (35%) | 6 (15%) | 17 (35%) | 4 (27%) | 31 (32%) | 144 (32%) | .139 |
| Male, n (%) | 162 (65%) | 34 (85%) | 31 (65%) | 11 (73%) | 67 (68%) | 305 (68%) | ||
| Race | American Indian/Alaska Native, n (%) | 2 (1%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (0%) | .002 |
| Asian, n (%) | 1 (0%) | 0 (0%) | 2 (4%) | 1 (7%) | 4 (4%) | 8 (2%) | ||
| Black, n (%) | 5 (2%) | 2 (5%) | 5 (10%) | 1 (7%) | 1 (1%) | 14 (3%) | ||
| Native Hawaiian/Pacific Islander, n (%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | ||
| White, n (%) | 235 (95%) | 38 (95%) | 37 (77%) | 13 (87%) | 93 (95%) | 416 (93%) | ||
| More than 1 race, n (%) | 0 (0%) | 0 (0%) | 1 (2%) | 0 (0%) | 0 (0%) | 1 (0%) | ||
| Unknown/not reported, n (%) | 5 (2%) | 0 (0%) | 3 (6%) | 0 (0%) | 0 (0%) | 8 (2%) | ||
| Ethnicity | Hispanic or Latino, n (%) | 4 (2%) | 2 (5%) | 4 (8%) | 1 (7%) | 1 (1%) | 12 (3%) | .069 |
| Not Hispanic or Latino, n (%) | 237 (96%) | 38 (95%) | 44 (92%) | 13 (87%) | 95 (97%) | 427 (95%) | ||
| Unknown/not reported, n (%) | 7 (3%) | 0 (0%) | 0 (0%) | 1 (7%) | 2 (2%) | 10 (2%) | ||
| BMI | Mean ± SD | 29.1 ± 6.3 | 27.4 ± 5.7 | 27.8 ± 4.7 | 30.4 ± 3.2 | 28.9 ± 5.7 | 28.8 ± 5.9 | .257 |
| Blast % | Mean ± SD | 4.1 ± 4.7 | 3.6 ± 4.5 | 1.5 ± 4.3 | 22.2 ± 2.5 | 1.0 ± 1.1 | 3.8 ± 6.3 | <.001 |
| Hemoglobin (g/dL) | <8, n (%) | 42 (17%) | 5 (13%) | 1 (2%) | 1 (7%) | 7 (7%) | 56 (12%) | <.001 |
| 8-10, n (%) | 90 (36%) | 12 (30%) | 10 (21%) | 8 (53%) | 13 (13%) | 133 (30%) | ||
| >10, n (%) | 116 (47%) | 23 (58%) | 37 (77%) | 6 (40%) | 78 (80%) | 260 (58%) | ||
| Platelets (10⁹/L) | <50, n(%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| ≥50, n (%) | 248 (100%) | 40 (100%) | 48 (100%) | 15 (100%) | 98 (100%) | 449 (100%) | ||
| Absolute Neutrophil Count (106/L) | <800, n (%) | 44 (18%) | 4 (10%) | 1 (2%) | 12 (80%) | 4 (4%) | 65 (14%) | <.001 |
| ≥800, n (%) | 198 (80%) | 35 (88%) | 45 (94%) | 3 (20%) | 91 (93%) | 372 (83%) | ||
| Missing, n (%) | 6 (2%) | 1 (3%) | 2 (4%) | 0 (0%) | 3 (3%) | 12 (3%) | ||
| Vulnerable∗ | Vulnerable, n (%) | 84 (34%) | 18 (45%) | 12 (25%) | 5 (33%) | 30 (31%) | 149 (33%) | .370 |
| IPSS-R | Very low, n (%) | 56 (23%) | 5 (13%) | — | — | — | — | — |
| Low, n (%) | 72 (29%) | 16 (40%) | — | — | — | — | ||
| Intermediate, n (%) | 46 (19%) | 8 (20%) | — | — | — | — | ||
| High, n (%) | 28 (11%) | 1 (3%) | — | — | — | — | ||
| Very high, n (%) | 29 (12%) | 0 (0%) | — | — | — | — | ||
| Not calculated, n (%) | 17 (7%) | 10 (25%) | — | — | — | — |
Fisher exact test used for comparing proportions of demographic factors between disease groups. An ANOVA used for comparing means of demographic factors between disease groups.
ANOVA, analysis of variance; BMI, body mass index; N, number of participants in each disease category.
Vulnerable participants are those with VES-13 ≥3.
Comparing across diagnostic categories, age differed significantly (P = .039), with the MDS/MPN group being the oldest on average [mean (SD) = 77 (7) years] and the ICUS group being the youngest [mean (SD) = 70 (12) years]. A smaller proportion of participants were White in the ICUS group compared with other diagnostic categories (77% vs 87%-95%, P = .002). Mean blast percentage was higher among AML <30% than other groups (22.2% vs 1%-4%, P < .001).
HRQoL and disease category
Comparing mean baseline HRQoL scores across all cytopenia diagnostic categories, no significant differences were found (Figure 1). No significant differences were found between MDS and the other diagnostic categories (Table 2). AML <30% blasts tended to have lower HRQoL scores (eg, mean EQ-5D-5L score of 64.3 [95% CI, 54.5-74.1]) than other diagnostic categories, but differences were not statistically significant (eg, mean EQ-5D-5L scores of 70.3 [95% CI, 67.8-72.7; P = .996] in MDS; 74.3 [95% CI, 68.3-80.4; P = .727] in MDS/MPN overlap; 74.3 [95% CI, 68.7-79.9; P = .727] in ICUS; and 73.4 [95% CI, 69.5-77.3; P = .727] in at-risk).
Figure 1.

Summary of HRQoL scores by disease group. Number of participants (N) in each disease subgroup with a QOL score and vulnerability data: MDS (N = 248), MDS/MPN (N = 40), ICUS (N = 48), AML<30% (N = 15), at-risk (N = 98). Mean estimates and P values based on analysis of covariance (ANCOVA) adjusted for age.
Table 2.
Summary of baseline HRQoL scores by disease group
| QOL measure | Statistic | MDS (N = 248) | MDS/MPN (N = 40) | ICUS (N = 48) | AML<30% (N = 15) | At-risk (N = 98) |
|---|---|---|---|---|---|---|
| QUALMS mean score | Mean (95% CI) | 69.7 (68.0-71.4) | 71.7 (67.3-76.1) | 73.5 (69.5-77.4) | 65.7 (58.5-72.9) | 73.2 (70.4-76.0) |
| P value (vs MDS) | - | .923 | .606 | .923 | .349 | |
| QUALMS physical burden | Mean (95% CI) | 67.1 (64.9-69.3) | 69.6 (64.0-75.2) | 69.0 (64.0-74.1) | 67.4 (58.1-76.7) | 72.0 (68.4-75.6) |
| P value (vs MDS) | - | .944 | .944 | .944 | .223 | |
| QUALMS benefit finding | Mean (95% CI) | 59.1 (55.9-62.3) | 56.5 (48.6-64.5) | 59.0 (51.8-66.3) | 55.4 (42.2-68.5) | 54.0 (49.0-59.1) |
| P value (vs MDS) | - | .987 | .987 | .987 | .963 | |
| QUALMS emotional | Mean (95% CI) | 71.0 (68.7-73.3) | 72.9 (67.0-78.9) | 78.0 (72.6-83.4) | 63.6 (53.8-73.4) | 75.3 (71.5-79.1) |
| P value (vs MDS) | - | .549 | .172 | .549 | .407 | |
| FACT-G total score | Mean (95% CI) | 81.1 (79.1-83.2) | 82.0 (76.9-87.1) | 84.6 (79.9-89.3) | 82.6 (74.5-90.7) | 82.4 (79.2-85.7) |
| P value (vs MDS) | - | .964 | .964 | .964 | .964 | |
| FACT-G physical well-being | Mean (95% CI) | 22.4 (21.8-23.0) | 22.8 (21.3-24.3) | 22.7 (21.4-24.1) | 22.4 (20.0-24.9) | 23.2 (22.2-24.2) |
| P value (vs MDS) | - | .985 | .985 | .985 | .985 | |
| FACT-G social well-being | Mean (95% CI) | 22.5 (21.8-23.2) | 22.4 (20.6-24.3) | 22.4 (20.7-24.0) | 23.6 (20.6-26.5) | 21.8 (20.7-23.0) |
| P value (vs MDS) | - | .955 | .955 | .955 | .955 | |
| FACT-G emotional well-being | Mean (95% CI) | 18.1 (17.6-18.7) | 17.5 (16.2-18.9) | 18.7 (17.4-19.9) | 17.5 (15.3-19.7) | 18.4 (17.5-19.3) |
| P value (vs MDS) | - | .984 | .984 | .984 | .984 | |
| FACT-G functional well-being | Mean (95% CI) | 18.3 (17.5-19.1) | 18.9 (16.9-21.0) | 20.2 (18.4-22.1) | 19.1 (15.8-22.3) | 19.5 (18.2-20.8) |
| P value (vs MDS) | - | .949 | .629 | .949 | .949 | |
| EQ-5D-5L total score | Mean (95% CI) | 70.3 (67.8-72.7) | 74.3 (68.3-80.4) | 74.3 (68.7-79.9) | 64.3 (54.5-74.1) | 73.4 (69.5-77.3) |
| P value (vs MDS) | - | .996 | .996 | .996 | .996 | |
| PROMIS Fatigue mean T-score | Mean (95% CI) | 51.7 (50.7-52.7) | 50.0 (47.4-52.5) | 51.8 (49.5-54.1) | 50.0 (45.9-54.1) | 51.1 (49.5-52.7) |
| P value (vs MDS) | - | .973 | .973 | .973 | .973 |
Estimates based on ANCOVA model adjusted for age. P values for pairwise comparisons adjusted using the Hochberg procedure. P values for overall F test for comparison of scores between diagnostic categories: QUALMS mean (P = .082), physical burden (P = .242), benefit finding (P = .539), emotional (P = .028), FACT-G total (P = .750), physical well-being (P = .748), social well-being (P = .818), emotional well-being (P = .700), functional well-being (P = .293), EQ-5D-5L (P = .214), PROMIS Fatigue (P = .681).
ANCOVA, analysis of covariance; N, number of participants in each disease group with an observed QOL score and vulnerability data.
Vulnerability and disease category
Based on the VES-13, 149 participants (33%) were considered vulnerable (Table 1), and vulnerability rates were similar between diagnostic categories. For vulnerable participants with MDS (n = 84, Table 3), most were age ≥75 years (63%), rated their health as poor or fair (65%), and had difficulty with prolonged physical activity (88%), such as walking a quarter mile (74%) or doing heavy housework (68%). A smaller percentage of vulnerable MDS participants required help with instrumental activities of daily living, such as shopping (33%) or managing money (15%). Compared with nonvulnerable MDS participants, vulnerable participants tended to be older, have lower hemoglobin levels, and a smaller proportion with low ANC (supplemental Table 2).
Table 3.
Characteristics of participants in the vulnerability subgroup
| Reason vulnerable | Vulnerability subgroup |
|||||
|---|---|---|---|---|---|---|
| MDS (N = 84) | MDS/MPN (N = 18) | ICUS (N = 12) | AML<30% (N = 5) | At-risk (N = 30) | Total (N = 149) | |
| Age | ||||||
| ≥75, n (%) | 53 (63%) | 15 (83%) | 6 (50%) | 2 (40%) | 20 (67%) | 96 (64%) |
| 75-84, n (%) | 29 (35%) | 11 (61%) | 3 (25%) | 1 (20%) | 13 (43%) | 57 (38%) |
| ≥85, n (%) | 24 (29%) | 4 (22%) | 3 (25%) | 1 (20%) | 7 (23%) | 39 (26%) |
| General health | ||||||
| Health rating of poor or fair, n (%) | 55 (65%) | 8 (44%) | 8 (67%) | 4 (80%) | 15 (50%) | 90 (60%) |
| Average difficulty with physical activities | ||||||
| Any activity, n (%) | 74 (88%) | 18 (100%) | 10 (83%) | 5 (100%) | 27 (90%) | 134 (90%) |
| Walking quarter-mile, n (%) | 62 (74%) | 15 (83%) | 6 (50%) | 5 (100%) | 21 (70%) | 109 (73%) |
| Heavy housework, n (%) | 57 (68%) | 15 (83%) | 8 (67%) | 5 (100%) | 21 (70%) | 106 (71%) |
| Stooping, crouching, kneeling, n (%) | 49 (58%) | 13 (72%) | 4 (33%) | 4 (80%) | 19 (63%) | 89 (60%) |
| Lifting objects 10 lbs or more, n (%) | 28 (33%) | 3 (17%) | 4 (33%) | 3 (60%) | 11 (37%) | 49 (33%) |
| Reaching or extending arms above shoulder, n (%) | 21 (25%) | 0 (0%) | 4 (33%) | 2 (40%) | 8 (27%) | 35 (23%) |
| Writing or grasping small objects, n (%) | 10 (12%) | 0 (0%) | 0 (0%) | 2 (40%) | 4 (13%) | 16 (11%) |
| Walking across room, n (%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Doing light housework, n (%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Difficulty/require assistance with activities because of health | ||||||
| Any activity, n (%) | 35 (42%) | 6 (33%) | 5 (42%) | 2 (40%) | 15 (50%) | 63 (42%) |
| Shopping, n (%) | 28 (33%) | 3 (17%) | 4 (33%) | 2 (40%) | 13 (43%) | 50 (34%) |
| Managing money, n (%) | 13 (15%) | 4 (22%) | 4 (33%) | 0 (0%) | 5 (17%) | 26 (17%) |
| Bathing or showering, n (%) | 15 (18%) | 2 (11%) | 0 (0%) | 0 (0%) | 5 (17%) | 22 (15%) |
Bold values indicate frequencies and percent vulnerable within a VES-13 domain. The same participant may meet several characteristics. Therefore, the number of participants meeting an individual characteristic within a domain may not sum to total the number of participants who meet any characteristic for the given domain.
N, number of participants in each disease group with an observed QOL score and who are vulnerable based on whether VES-13 ≥3.
In the overall cohort, vulnerable participants had significantly worse HRQoL on all measures except PROMIS Fatigue for MDS/MPN, ICUS, AML<30% blasts, and at-risk, both when pooled over all diagnostic categories (supplemental Figure 1) and within each diagnostic category (Figure 2; supplemental Table 3). Only vulnerable participants with MDS scored significantly lower than nonvulnerable MDS participants on the PROMIS Fatigue (means of 56.0 [95% CI, 54.3-57.6] vs 49.5 [95% CI, 48.3-50.7]; P < .001).
Figure 2.

Summary of HRQoL overall scores by vulnerability subgroup among and disease subgroup. Number of participants (N) in each disease and vulnerability: vulnerable MDS (N = 84), MDS/MPN (N = 18), ICUS (N = 12), AML<30% (N = 5), at-risk (N = 30), nonvulnerable MDS (N = 164), MDS/MPN (N = 22), ICUS (N = 36), AML<30% (N = 10), at-risk (N = 68). Estimates based on ANCOVA model adjusted for age. P values for pairwise comparisons adjusted using the Hochberg procedure. Vulnerable defined as VES-13 ≥ 3.
HRQoL, vulnerability, and MDS disease risk
Except for FACT-G and PROMIS Fatigue, a significant trend of worsening HRQoL with worse MDS or MDS/MPN disease prognosis was identified for all overall HRQoL scores, with decreasing EQ-5D-5L mean scores of 73.4 (95% CI, 70.2-76.5), 72.7 (95% CI, 67.5-77.8), and 64.1 (95% CI, 59.1-69.1) for low-, intermediate-, and high-risk MDS or MDS/MPN, respectively (P = .005, Figure 3; supplemental Table 4). Based on subscales (supplemental Table 4; supplemental Figures 4 and 5), HRQoL significantly worsened over the risk groups for the overall QUALMS (P = .046), QUALMS-P (P = .020), and QUALMS-BF (P = .039). Accounting for vulnerability, however, these trends on the HRQoL measures were significant only among nonvulnerable MDS or MDS/MPN participants for QUALMS-P, FACT-G Physical Well-Being, and EQ-5D-5L (supplemental Table 5). In addition, vulnerable MDS or MDS/MPN participants had significantly worsening HRQoL for increasing disease risk for QUALMS Benefit Finding (P = .030) and FACT-G Emotional Well-Being (P = .036).
Figure 3.

Summary of HRQoL overall scores by IPSS-R score in MDS or MDS/MPN overlap. Number of participants (N) with MDS or MDS/MPN overlap in each IPSS-R strata: very low/low (N = 149), intermediate (N=54), high/very high (N = 58). Estimates based on ANCOVA model adjusted for age. Estimates and P value based on linear regression of QOL score and IPSS-R score adjusted for age.
Discussion
MDS and related hematologic conditions tend to affect adults of advanced age, are associated with cytopenias, and consequently negatively affect quality of life and survival. In this large, prospective cohort of older adults being evaluated for suspicion of MDS with rigorous hematologic assessment, including bone marrow biopsy, baseline HRQoL (assessed before patient receipt of bone marrow biopsy results) was affected but did not appear to differ between those ultimately found to have MDS vs ICUS, AML, or those categorized as at-risk.
A large proportion of our patients being worked up for cytopenias were found to be vulnerable on the VES-13 (33.2%), with worse HRQoL among those who were vulnerable. Moreover, among those with biopsy-confirmed MDS, very low/low-risk disease on the IPSS-R was associated with better HRQoL than higher-risk disease, as initially hypothesized. Interestingly, this relationship was observed primarily among the nonvulnerable, suggesting that HRQoL can be difficult to disentangle or improve in the context of underlying vulnerability in this patient population.
Unexpectedly, baseline HRQoL was not worse among patients who truly had MDS vs those who had other reasons for cytopenias. This finding was likely due to HRQoL being driven by symptoms related to abnormal blood counts, which occurred in all patients being evaluated for “possible MDS.” Our data suggest that baseline HRQoL cannot be used to distinguish true MDS among patients being worked up for cytopenias and should not factor into the decision of whether to obtain a diagnostic bone marrow assessment. Although such assessment is an essential part of the work up for MDS, in a study of the Surveillance, Epidemiology, and End Results Program (SEER)-Medicare database of the National Cancer Institute, only 82% of patients who carried the diagnosis had a claim for a bone marrow biopsy, and even fewer (74%) had claims for cytogenetic testing at diagnosis.6 This may be because clinicians sometimes use gestalt quality of life assessment as a proxy for potential MDS risk, and thus forgo biopsy for those patients with cytopenias who report feeling well. Our data suggest that clinicians may not be able to rely on these informal assessments to detect true MDS.
In contrast, among patients with true MDS, HRQoL was modestly impaired with increasing IPSS-R risk stratum; for example, scores on the QUALMS-P and EQ-5D-5L total scores were better for those in the very low/low-risk IPSS-R group (P = .020 and .005, respectively). This finding may be related to progressively worsening blood counts and cytokine-mediated symptoms associated with excess blasts and may point to the need for increased symptom support for these patients by engaging palliative care. It is provocative in the context of prior data suggesting that HRQoL can be added to IPSS-R data to further improve risk stratification 2.22 In an international study of patients with higher-risk MDS, in multivariable models for survival including the IPSS-R, patient-reported fatigue was an independent prognostic factor (hazard ratio, 1.13 [1.06-1.19]; P = .0002). Those data and ours suggest that a formal HRQoL assessment, including fatigue, should be a routine part of the MDS clinical evaluation.
Indeed, we found that for participants with biopsy-confirmed MDS, HRQoL impairment was similar to that routinely seen in solid malignancies; for example, the mean total FACT-G score was 81.1, similar to localized breast cancer (82.4) and localized colorectal cancer (79.6).23 This finding provides an HRQoL argument that patients with MDS have lived experiences that are more similar to those of early-stage patients with cancer than people without cancer. Our finding is also consistent with a study assessing EQ-5D at initial diagnosis for lower-risk patients from the European LeukemiaNet MDS Registry.24 Compared with age- and sex-matched people without cancer, a significantly higher proportion of patients with MDS reported moderate/severe pain/discomfort, impaired mobility, anxiety/depression, and impaired daily activities, even though this was a lower-risk cohort and thus “far away” from AML.
Over one-third of our MDS cohort was vulnerable, per the VES-13. Although vulnerability and the related concept of frailty in MDS have been studied using general measures,25 until recently none have been MDS-specific. In 2020, a group using the Canadian MDS registry (n = 644) developed a frailty index for patients with MDS (the “MDS-FI”) 226; the tool was subsequently reduced to 15 variables for increased administration time efficiency.27 Such an instrument could be easily administered as part of the baseline MDS assessment. Moreover, our finding that patients with MDS who are vulnerable most often have difficulty with prolonged physical activity (88%), such as walking a quarter mile (74%), or doing heavy housework (68%), argues that it may make sense to specifically query these domains in clinic and refer to social work and physical therapy as needed.
Although the literature is sparse regarding the interaction between vulnerability and HRQoL in patients with hematologic malignancies, there is some evidence suggesting that relationships exist between frailty and HRQoL variables in patients with cancer. Frailty and vulnerability are distinct concepts, but they are highly correlated. Indeed, a Dutch study of patients with and without cancer (n = 7493)15 found that those who were frail reported significantly lower HRQoL. In addition, patients with cancer reported a significantly higher level of frailty and lower HRQoL as compared with patients without cancer; however, when mutually adjusting for frailty and cancer diagnosis, frailty had a stronger association with HRQoL, suggesting that increasing frailty may be the more important factor, as compared with the cancer diagnosis itself, toward lower HRQoL. Our finding that patients with MDS who were vulnerable largely did not experience differences in HRQoL by increasing MDS risk suggests that a similar relationship may hold for the syndromes: being vulnerable may erase differences in HRQoL associated with the otherwise “known group” of underlying disease risk.18
Increasing evidence suggests that clonal cytopenia of undetermined significance has similar clinical characteristics and potential for disease progression when compared with lower-risk MDS.28, 29, 30, 31 To our knowledge, we report some of the first data on HRQoL and vulnerability for patients with ICUS, finding that HRQoL (ostensibly driven by cytopenias) was similar and vulnerability a bit less common (25% vs 36% for patients with MDS). Further analysis of the ICUS cohort and the “at-risk” cohort as they mature will be essential to determine if changes in HRQoL or vulnerability are seen with subsequent MDS-defining events.
Our work has limitations. First, our collection of HRQoL and vulnerability data was incomplete; however, similar baseline characteristics were observed between those with and without available survey data, suggesting our results were not affected by selection bias. Second, we had a high percentage of White patients overall (93%) and in the MDS cohort (95%), which may limit the generalizability of our results to other populations. Third, we were limited to the use of the VES-13 survey, and our vulnerability results may have been different if our patients underwent a gold standard CGA8 for frailty. We also note that the survey instruments used here may differ in their sensitivity for measuring HRQoL. Indeed, recent findings32 suggest the QUALMS-P may be even more sensitive than the overall QUALMS to changes in lived experiences among patients with MDS. Finally, our study focused on baseline HRQoL results among participants enrolled before the COVID-19 suspension; future analyses are planned to evaluate HRQoL longitudinally and compare HRQoL before vs after suspension.
In conclusion, we found that among patients suspected of having MDS, disease-specific and general HRQoL did not distinguish those having a true MDS diagnosis, although HRQoL was different among different risk groups for those who ultimately had the disease. Vulnerability was prevalent, often associated with physical impairment, and overshadowed our ability to assess quality of life differences in MDS subgroups, showing for the first time that vulnerability trumps disease risk in affecting the HRQoL of these patients. Our analyses affirm the need for a baseline marrow assessment to diagnose MDS, even among patients with suspected disease who feel well, and suggest that both HRQoL and several specific questions about physical function be routinely assessed as well.
Conflict-of-interest disclosure: D.R. reports membership on a board or advisory committee at and holds stock in NanoString Technologies, Inc. R.K. received honoraria from Novartis, Geron, and Acceleron; and received honoraria from and is on the speakers bureau at Agios, Abbvie, JAZZ, and Bristol Myers Squibb. T.A.B. holds stock in and reports membership on a board or advisory committee at Bristol Myers Squibb; holds stock in AstraZeneca, Epizyme, and Heron Therapeutics; and reports membership on a board or advisory committee at Morphosys, Karyopharm, and Cardinal Health. E.P. received research funding from Bristol Myers Squibb, Kura, and Incyte; and received honoraria from Taiho and Blueprint. A.D. reports consultancy, membership on a board, or advisory committee at Taiho, Novartis, and Bristol Myers Squibb; and reports membership on a board or advisory committee at Takeda. M.A.S. reports membership on a board or advisory committee at Novartis, Takeda/Millenium, and Bristol Myers Squibb. The remaining authors declare no competing financial interests.
Acknowledgments
This study was conducted on behalf of the investigators of the National Heart, Lung, and Blood Institute National MDS Natural History Study. The National MDS Natural History Study has been supported by US Federal Government contracts HHSN268201400003I and HHSN268201400002I from the National Heart, Lung, and Blood Institute and additional funding by the National Cancer Institute to NCORP and the participating clinical centers.
The content is solely the responsibility of the authors and does not represent the policy of the National Institutes of Health or the Department of Health and Human Services.
Authorship
Contribution: G.A.A. designed the study and wrote the manuscript; D.H. and M.O. performed the statistical analyses; G.A.A., D.H., C.L., M.A.S., and S.W. contributed to the study design and interpretation of the data; and all authors contributed to interpretation of the data, preparation of the manuscript, and approved its content.
Footnotes
Data are available on request from the corresponding author, Gregory A. Abel (gregory_abel@dfci.harvard.edu).
The full-text version of this article contains a data supplement.
Supplementary Material
References
- 1.Aguiar APN, Mendonca PDS, Ribeiro-Junior HL, et al. Myelodysplastic syndromes: an analysis of non-hematological prognostic factors and its relationship to age. J Geriatr Oncol. 2020;11(1):125–127. doi: 10.1016/j.jgo.2019.06.021. [DOI] [PubMed] [Google Scholar]
- 2.Ma X, Does M, Raza A, Mayne ST. Myelodysplastic syndromes: incidence and survival in the United States. Cancer. 2007;109(8):1536–1542. doi: 10.1002/cncr.22570. [DOI] [PubMed] [Google Scholar]
- 3.Greenberg P, Cox C, LeBeau MM, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89(6):2079–2088. [PubMed] [Google Scholar]
- 4.Greenberg PL, Tuechler H, Schanz J, et al. Revised International Prognostic Scoring System for myelodysplastic syndromes. Blood. 2012;120(12):2454–2465. doi: 10.1182/blood-2012-03-420489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Greenberg PL, Stone RM, Bejar R, et al. Myelodysplastic syndromes, version 2.2015. J Natl Compr Canc Netw. 2015;13(3):261–272. doi: 10.6004/jnccn.2015.0038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Abel GA, Cronin AM, Odejide OO, Uno H, Stone RM, Steensma DP. Influence of patient and provider characteristics on quality of care for the myelodysplastic syndromes. Br J Haematol. 2016;173(5):713–721. doi: 10.1111/bjh.13987. [DOI] [PubMed] [Google Scholar]
- 7.Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–1375. doi: 10.1016/S0140-6736(19)31786-6. [DOI] [PubMed] [Google Scholar]
- 8.Mohile SG, Dale W, Somerfield MR, et al. Practical assessment and management of vulnerabilities in older patients receiving chemotherapy: ASCO guideline for geriatric oncology. J Clin Oncol. 2018;36(22):2326–2347. doi: 10.1200/JCO.2018.78.8687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Saliba D, Elliott M, Rubenstein LZ, et al. The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community. J Am Geriatr Soc. 2001;49(12):1691–1699. doi: 10.1046/j.1532-5415.2001.49281.x. [DOI] [PubMed] [Google Scholar]
- 10.Luciani A, Ascione G, Bertuzzi C, et al. Detecting disabilities in older patients with cancer: comparison between Comprehensive Geriatric Assessment and Vulnerable Elders Survey-13. J Clin Oncol. 2010;28(12):2046–2050. doi: 10.1200/JCO.2009.25.9978. [DOI] [PubMed] [Google Scholar]
- 11.Fama A, Martin P, Allmer C, et al. Vulnerable Elders Survey-13 (VES-13) predicts 1-year mortality risk in newly diagnosed non-Hodgkin lymphoma (NHL) Blood. 2019;134(suppl 1):69. [Google Scholar]
- 12.Holmes HM, Des Bordes JK, Kebriaei P, et al. Optimal screening for geriatric assessment in older allogeneic hematopoietic cell transplantation candidates. J Geriatr Oncol. 2014;5(4):422–430. doi: 10.1016/j.jgo.2014.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chehrehgosha M, Alizadeh-Khoei M, Behnampour N, Sharifi F, Fadaye Vatan R, Aminalroaya R. Diagnosis of frailty in geriatric patients: is the pictorial fit frail scale an appropriate screening tool in hospital settings? Caspian J Intern Med. 2021;12(3):307–314. doi: 10.22088/cjim.12.3.307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chehrehgosha M, Vatan RF, Alizadeh Khoei M, et al. Role of frailty in prediction of hospitalized older adult patients outcomes: a prospective study. Turk J Med Sci. 2021;51(5):2324–2333. doi: 10.3906/sag-2012-332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Geessink N, Schoon Y, van Goor H, Olde Rikkert M, Melis R, TOPICS-MDS consortium Frailty and quality of life among older people with and without a cancer diagnosis: findings from TOPICS-MDS. PLoS One. 2017;12(12):e0189648. doi: 10.1371/journal.pone.0189648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Amitai I, Geddes M, Zhu N, et al. Patient-reported fatigue refines prognosis in higher-risk myelodysplastic syndromes (MDS): a MDS-CAN study. Br J Haematol. 2021;194(2):319–324. doi: 10.1111/bjh.17537. [DOI] [PubMed] [Google Scholar]
- 17.Sekeres MA, Gore SD, Stablein DM, et al. The National MDS Natural History Study: design of an integrated data and sample biorepository to promote research studies in myelodysplastic syndromes. Leuk Lymphoma. 2019;60(13):3161–3171. doi: 10.1080/10428194.2019.1616186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Abel GA, Efficace F, Buckstein RJ, et al. Prospective international validation of the Quality of Life in Myelodysplasia Scale (QUALMS) Haematologica. 2016;101(6):781–788. doi: 10.3324/haematol.2015.140335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cella DF, Tulsky DS, Gray G, et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol. 1993;11(3):570–579. doi: 10.1200/JCO.1993.11.3.570. [DOI] [PubMed] [Google Scholar]
- 20.Cella D, Riley W, Stone A, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005-2008. J Clin Epidemiol. 2010;63(11):1179–1194. doi: 10.1016/j.jclinepi.2010.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L) Qual Life Res. 2011;20(10):1727–1736. doi: 10.1007/s11136-011-9903-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Efficace F, Gaidano G, Breccia M, et al. Prognostic value of self-reported fatigue on overall survival in patients with myelodysplastic syndromes: a multicentre, prospective, observational, cohort study. Lancet Oncol. 2015;16(15):1506–1514. doi: 10.1016/S1470-2045(15)00206-5. [DOI] [PubMed] [Google Scholar]
- 23.Pearman T, Yanez B, Peipert J, Wortman K, Beaumont J, Cella D. Ambulatory cancer and US general population reference values and cutoff scores for the Functional Assessment of Cancer Therapy. Cancer. 2014;120(18):2902–2909. doi: 10.1002/cncr.28758. [DOI] [PubMed] [Google Scholar]
- 24.Stauder R, Yu G, Koinig KA, et al. Health-related quality of life in lower-risk MDS patients compared with age- and sex-matched reference populations: a European LeukemiaNet study. Leukemia. 2018;32(6):1380–1392. doi: 10.1038/s41375-018-0089-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Abel GA, Klepin HD. Frailty and the management of hematologic malignancies. Blood. 2018;131(5):515–524. doi: 10.1182/blood-2017-09-746420. [DOI] [PubMed] [Google Scholar]
- 26.Starkman R, Alibhai S, Wells RA, et al. An MDS-specific frailty index based on cumulative deficits adds independent prognostic information to clinical prognostic scoring. Leukemia. 2020;34(5):1394–1406. doi: 10.1038/s41375-019-0666-7. [DOI] [PubMed] [Google Scholar]
- 27.Wan BA, Nazha A, Starkman R, et al. Revised 15-item MDS-specific frailty scale maintains prognostic potential. Leukemia. 2020;34(12):3434–3438. doi: 10.1038/s41375-020-01026-y. [DOI] [PubMed] [Google Scholar]
- 28.Galli A, Todisco G, Catamo E, et al. Relationship between clone metrics and clinical outcome in clonal cytopenia. Blood. 2021;138(11):965–976. doi: 10.1182/blood.2021011323. [DOI] [PubMed] [Google Scholar]
- 29.Valent P, Orazi A, Steensma DP, et al. Proposed minimal diagnostic criteria for myelodysplastic syndromes (MDS) and potential pre-MDS conditions. Oncotarget. 2017;8(43):73483–73500. doi: 10.18632/oncotarget.19008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Malcovati L, Galli A, Travaglino E, et al. Clinical significance of somatic mutation in unexplained blood cytopenia. Blood. 2017;129(25):3371–3378. doi: 10.1182/blood-2017-01-763425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Gondek LP, DeZern AE. Assessing clonal haematopoiesis: clinical burdens and benefits of diagnosing myelodysplastic syndrome precursor states. Lancet Haematol. 2020;7(1):e73–e81. doi: 10.1016/S2352-3026(19)30211-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Efficace F, Koinig K, Cottone F, et al. Raising the standards of patient-centered outcomes research in myelodysplastic syndromes: Clinical utility and validation of the subscales of the QUALMS from the MDS-RIGHT project. Cancer Med. 2023;12(6):7529–7539. doi: 10.1002/cam4.5487. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.