

Abstract
Background:
Minimum legal age (MLA) restrictions are a core policy to reduce youth use of tobacco, e-cigarettes, and other substances. We examined trends in perceived ease of access to tobacco and other substances across three countries with differing MLA policies, including the United States (US), which increased the federal MLA for tobacco products from 18 to 21 in 2019.
Methods.
Repeat cross-sectional data were analyzed from seven waves of the International Tobacco Control (ITC) Youth Tobacco and Vaping Survey conducted between 2017 and 2021. Online surveys were conducted with non-probability samples of 91,647 youth aged 16–19 in Canada, England, and the US. Regression models were used to examine differences in perceived ease of accessing each of 7 substances (analyzed as “very easy” or “fairly easy” versus else), and differences between countries and over time (including before and after any MLA changes) for cigarettes, e-cigarettes, cannabis, and alcohol; additional models examined sub-national variation in MLA.
Results.
Perceived access varied by substance and across countries: in August/September 2021, perceived ease of accessing cigarettes and e-cigarettes was greater in Canada where MLA was 18–19 (61.7% cigarettes, 66.4% e-cigarettes) and England where MLA was 18 (66.9%, 69.6%), compared to the US where MLA was 21 (48.0%, 60.9%; p<0.001 for all). Perceived ease of accessing cannabis was greatest in Canada (53.3%), followed by the US (44.1%) and England (34.0%; p<0.001 for all). Following the federal MLA increase for tobacco products in the US, perceived ease of access decreased significantly for cigarettes (65.1% in 2019Aug to 59.7% in 2020Feb; aOR=0.80 (95%CI=0.71–0.89)) and e-cigarettes (72.9% in 2019Aug to 69.4% in 2020Feb; aOR=0.87 (95%CI=0.77–0.98)).
Conclusions.
Higher MLA was strongly associated with fewer youth perceiving easy access to substances: perceived access varied between countries with differing MLA, as well as within-country before and after changes to MLA.
Keywords: tobacco, e-cigarettes, alcohol, cannabis, youth, policy
Minimum legal age (MLA) of sale is a core policy intervention aimed at reducing substance use among youth, including for tobacco, e-cigarettes, and alcohol. Most countries prohibit selling tobacco to minors, typically defined as those below the age of 18, with similar MLA laws for alcohol and e-cigarettes. MLA policies seek to reduce substance use among youth by restricting supply to minors. In addition to reducing direct access through commercial sources, increasing MLA can increase ‘search-time’ costs (i.e., time and effort) associated with finding non-compliant retail or alternative sources, including social sources and proxy purchasers (IOM, 2015).
There is substantial evidence demonstrating that higher MLA for alcohol sales is associated with lower alcohol consumption among young people (DeJong & Blanchette, 2014; Wagenaar & Toomey, 2002). In contrast, a comprehensive evidence review on raising the MLA of sale for tobacco, conducted by the Institute of Medicine (IOM) in 2015, noted limited evidence and mixed findings in this area. However, modelling conducted as part of the report projected that raising the MLA to 21 years in the United States (US) was likely to decrease smoking among adolescents aged 15 to 17 (IOM, 2015). Subsequent studies also suggest a beneficial effect of increased MLA for tobacco products. In England, MLA for cigarettes was increased in 2007 from 16 to 18 years, and long-term trend analysis indicates an association with a greater decline in ‘ever’ smoking among those aged 16–17 compared with those aged 18–24 (Beard et al., 2020). In Canada, analysis of national survey data between 2000 and 2014 found that smoking prevalence was lower among age-restricted youth in Canadian provinces with higher MLA (Callaghan et al., 2018).
Increases in MLA for tobacco have recently been implemented in the US, at the state and federal levels. Between 2016 and 2019, 12 states fully implemented “T21” laws raising the age of access for tobacco and e-cigarettes to 21 years (Marynak et al., 2020; Preventing Tobacco Addiction Foundation, 2022), in addition to over 500 localities (Campaign for Tobacco-Free Kids, n.d.). Several studies have examined state-level MLA increases, finding that “T21” laws were associated with declines in both smoking and e-cigarette use. For example, an analysis of Behavioral Risk Factor Surveillance Survey (BRFSS) data from 2009 to 2019 found that statewide T21 implementation was associated with declines in past 30-day smoking among 18-to-20-year-olds (Bryan et al., 2020). Similarly, analysis of state Youth Risky Behavior Surveys (YRBS) over the same time period found reductions in cigarette and e-cigarette consumption among 18-year-old high school students in states with T21 laws (Bryan et al., 2020). Decreases in tobacco sales in states with T21 laws, compared with those that did not, were also found (Ali et al, 2020). T21 laws have also been associated with lower e-cigarette use: between 2017 and 2019, prevalence of e-cigarette use increased in states without T21 laws, but not in states with T21 laws (Choi et al., 2021).
In addition to reducing objective availability by directly reducing retail access, MLA laws may impact perceived availability among youth (IOM, 2015). Youth access and perceived access to tobacco, alcohol, and illicit drugs is associated with their use (National Center on Addiction and Substance Abuse, 2011), including longitudinal research finding that perceived accessibility to cigarettes increased youth’s risk of future smoking initiation and escalation (Doubeni, 2008). Youth perceptions of access to substances are influenced not just by physical availability (including retail access), but by social availability (which includes social norms, prevalence among peers, and perceived support for use by peers and the community), and other factors such as age and community prevalence (Warren et al, 2015).
While perceived availability is a potentially important indicator of youth access and use of tobacco products, there is limited research examining perceived access and the impact of MLA laws. A study of 19 European countries found a greater decrease in perceived ease of cigarette obtainability in countries enforcing sales to those over the age of 18 (Kuipers et al., 2017). In the US, the Monitoring the Future survey indicates that perceived access to cigarettes has declined over time: in the early 1990s approximately 90% of 10th-graders reported easy access to cigarettes, compared to 50% in 2020 (Johnston et al., 2021). In a California study of their state T21 law, around half of participants under age 21 reported that it was harder to purchase cigarettes (54%) and e-cigarettes (44%) compared to a year earlier, before T21 (Schiff et al., 2021).
As noted in the IOM report, there are challenges with separating the effects of minimum age laws and their enforcement and compliance, and other policy effects (IOM, 2015). While measures of use such as prevalence are affected by numerous other factors, perceived access provides a ‘proximal’ indicator of MLA policy effects on youth access where one would expect any direct impact of MLA policies to be observed. However, little is known about how recent changes to minimum legal age laws and regulatory status have impacted perceptions of access, and the extent to which these changes are consistent across different jurisdictions.
The current study examined perceived ease of access to seven legal and illegal substances most commonly used by youth in in Canada, England, and the US between 2017 and 2021. Variation in the MLA across jurisdictions and substances, as well as recent changes to legal status and MLA for some substances, allows comparisons regarding the potential impact on youths’ perceptions of access (“natural experiments”)—see Table 1 for details. In brief, the US federal MLA for tobacco products and e-cigarettes was raised from 18 to 21 years, effective December 2019 (notwithstanding jurisdictions that had already implemented T21), and the MLA in all US states is 21 for alcohol, as is the case for cannabis in states where it is legally sold. In Canada, MLA depends on the province/territory and substance, and is usually 18 or 19 years. Relevant legislative changes in Canada during the study period include: implementation of the Tobacco and Vaping Products Act (TVPA) in May 2018, which brought e-cigarettes under the same MLA as tobacco; federal legalization of non-medical (“recreational”) cannabis in October 2018; and provincial/territorial increases to MLA in 2020, for tobacco in one province (to 21 years) and two territories (to 19), and for cannabis in one province (to 21). In contrast, the MLA in England is 18 years for tobacco, e-cigarettes, and alcohol, and there is no legal sale of non-medical cannabis. There was no legal access to hallucinogens or ecstasy/MDMA in any of the countries.
Table 1:
Minimum legal age for purchase of various products, by country, 2017–2021
| Canada | England | United States | |
|---|---|---|---|
|
| |||
| Cigarettes | – 18 years: provinces of Alberta (AB), Manitoba (MB), Quebec (QC), Saskatchewan (SK), Northwest Territories (NWT) prior to Mar. 31, 2020, Yukon territory (YT) prior to Mar. 5, 2020 – 19 years: provinces of British Columbia (BC), New Brunswick (NB), Newfoundland & Labrador (NL), Nova Scotia (NS), Ontario (ON), Prince Edward Island (PEI) prior to Mar. 1, 2020, Nunavut (NU), YT as of Mar. 5, 20201, NWT as of Mar. 31, 20202 – 21a years: PEI as of Mar. 1, 20203 |
18 years 4 | – federal: – 18 years: prior to Dec. 20, 2019 – 21 years: as of Dec. 20, 2019 – prior to Dec. 20, 2019, MLA of 21 implemented in 16 states (Arkansasb, California, Connecticut, Delaware, Hawaii, Illinois, Maineb, Maryland, Massachusettsb, New Jersey, New York, Ohio, Oregon, Texasb, Vermont, Virginia) and District of Columbia (DC)5,6 |
| E-cigarettes | As of May 23, 2018, same as cigarettes7,8 | 18 years 9 | As of Aug. 8, 2016, same as cigarettes10 |
| Alcohol | – 18 years: AB, MB, QC11 – 19 years: BC, NB, NL, NS, NU, NWT, ON, PEI, SK, YT11 |
18 years 12 | 21 years 13 |
| Cannabis | As of Oct. 17, 2018:14 – 18 years: AB, QC prior to Jan. 1, 2020 – 19 years: BC, MB, NB, NL, NS, NU, NWT, PEI, ON, SK, YT –21 years: QC as of Jan. 1, 202015 |
N/A (no legal non-medical access) | 21 years in the 18 states (and DC) where nonmedical cannabis is legal16 |
With a 2-year transition period where those who were 19 years of age by March 1, 2020 were still permitted to purchase products
With a transition period where those who were already of age were still permitted to purchase products. See Supplemental File for details.
Government of Yukon. Find out about tobacco and vaping products legislation. https://yukon.ca/en/health-and-wellness/cannabis-and-alcohol/find-out-about-tobacco-and-vaping-products-legislation#whats-new (accessed 10 June 2021)
Government of Northwest Territories. Smoking Control and Reduction Act and Tobacco and Vapour Products Control Act. https://www.hss.gov.nt.ca/en/services/bill-40–41 (accessed 10 June 2021)
Government of Prince Edward Island. 2021.Vaping Laws. https://www.princeedwardisland.ca/en/information/health-and-wellness/vaping-laws (accessed 10 June 2021)
Fidler JA, West R. Changes in smoking prevalence in 16–17-year-old versus older adults following a rise in legal age of sale: findings from an English population study. Addiction. 2010;105:1984–8.
Marynak K, Mahoney M, Williams KS, Tynan MA, Reimels E, King BA. State and Territorial Laws Prohibiting Sales of Tobacco Products to Persons Aged <21 Years – United States, December 20, 2019. MMWR Morb Mortal Wkly Rep. 2020;69(7):189–192. doi: 10.15585/mmwr.mm6907a3.
Preventing Tobacco Addiction Foundation. 2022. Tobacco 21: The Law of the Land [Tobacco 21 State Laws in Order of Enactment and their Date of Implementation]. https://tobacco21.org (accessed 31 March 2022)
Government of Canada. Tobacco and Vaping Products Act. https://www.canada.ca/en/health-canada/services/health-concerns/tobacco/legislation/federal-laws/tobacco-act.html (accessed 10 June 2021)
Government of Canada. Tobacco and Vaping Products Act. S.C. 1997, c. 13. https://laws-lois.justice.gc.ca/PDF/T-11.5.pdf (accessed 10 June 2021)
UK Government. The Nicotine Inhaling Products (Age of Sale and Proxy Purchasing) Regulations 2015. UK Statutory Instruments 2015 No. 895. https://www.legislation.gov.uk/uksi/2015/895/contents/made
Federal Register. May 10, 2016. Deeming Tobacco Products To Be Subject to the Federal Food, Drug, and Cosmetic Act, as Amended by the Family Smoking Prevention and Tobacco Control Act; Restrictions on the Sale and Distribution of Tobacco Products and Required Warning Statements for Tobacco Products. https://www.govinfo.gov/content/pkg/FR-2016-05-10/pdf/2016-10685.pdf (accessed 10 June 2021)
Canadian Centre on Substance Use and Addiction. Policy and Regulations (Alcohol). https://www.ccsa.ca/policy-and-regulations-alcohol (accessed 10 June 2021)
Wagenaar AC, Toomey TL. Effects of minimum drinking age laws: review and analyses of the literature from 1960 to 2000. 2002. Journal of Studies on Alcohol; Suppl 14: 206–225.
U.S. Department of Health & Human Services, Division of Population Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. n.d. [last reviewed Sept 3, 2020]. Age 21 Minimum Legal Drinking Age. https://www.cdc.gov/alcohol/fact-sheets/minimum-legal-drinking-age.htm (accessed 10 June 2021)
Government of Canada. Cannabis in the provinces and territories. 2018. https://www.canada.ca/en/health-canada/services/drugs-medication/cannabis/laws-regulations/provinces-territories.html (accessed 10 June 2021)
Banerjee S. 2019 Dec 31. Quebec raising legal age for cannabis to 21, the strictest in the country. Toronto Star. https://www.thestar.com/news/canada/2019/12/31/quebec-raising-legal-age-for-cannabis-to-21-the-strictest-in-the-country.html (accessed 14 April 2022)
The current study examined trends over time and across jurisdictions to address: 1) whether perceived access varied by substance and country, including between countries with differing MLA; and, 2) whether perceived access to cigarettes, e-cigarettes, cannabis, and alcohol changed over time within and between countries, including before and after any changes in legal status and/or MLA. In addition to national-level comparisons, sub-national comparisons examined differences in state/provincial MLA laws: 1) US-specific analyses examined differences in implementation of state-level T21 laws, as well as differences in perceived access by cannabis legalization; and, 2) Canada-specific analyses examined differences in MLA of 18 versus 19 for tobacco and e-cigarettes, and provincial variation in cannabis MLA laws. Country-specific comparisons also addressed whether any variation in perceived access by MLA differed by age of respondents. Comparisons across countries and states/provinces are particularly important to help account for any effects of the COVID-19 pandemic that would be common across jurisdictions. Substances where there were no changes to legal status and/or MLA (e.g., alcohol) provide context for comparisons.
METHODS
The International Tobacco Control Policy Evaluation Project (ITC) Youth Tobacco and Vaping Survey is a self-completed online survey examining tobacco use and vaping among youth in Canada, England, and the US. Repeat cross-sectional data were analyzed from 91,647 respondents across 7 survey waves: annual surveys conducted around August of 2017, 2018 and 2019 (exact timing varied by year, extending into July or September), and biannual surveys at 6-month intervals (around February and August, with slightly varied timing) in 2020 and 2021. See Table 2 for sample size in each country at each wave.
Table 2:
Sample characteristics, youth aged 16–19 years, by country, weighted %(n)
| Canada (n=29,719) |
England (n=28,541) |
United States (n=33,387) |
|
|---|---|---|---|
|
| |||
| Age (mean; SD) | 17.5 (1.08) | 17.5 (1.03) | 17.5 (1.06) |
| Sexa | |||
| Male | 51.3% (15,235) | 51.4% (14,665) | 51.1% (17,049) |
| Female | 48.7% (14,484) | 48.6% (13,876) | 48.9% (16,339) |
| Race/ethnicityb | |||
| White (only) | 54.5% (16,203) | 75.0% (21,402) | 71.2% (23,779) |
| Mixed/Other/Not stated | 45.5% (13,516) | 25.0% (7,139) | 28.8% (9,608) |
| Survey date | |||
| 2017 – Jul/Aug | 13.6% (4,038) | 14.0% (3,995) | 12.3% (4,095) |
| 2018 – Aug/Sep | 12.9% (3,845) | 13.6% (3,874) | 12.1% (4,034) |
| 2019 – Aug/Sep | 13.9% (4,135) | 12.2% (3,493) | 11.9% (3,981) |
| 2020 – Feb/Mar | 14.2% (4,217) | 15.0% (4,275) | 15.4% (5,132) |
| 2020 – Aug | 14.4% (4,269) | 15.0% (4,290) | 17.9% (5,991) |
| 2021 – Feb/Mar | 15.5% (4,611) | 15.1% (4,298) | 15.8% (5,273) |
| 2021 – Aug/Sep | 15.5% (4,604) | 15.1% (4,316) | 14.6% (4,881) |
Determined by response to “sex at birth” survey item; where sex at birth was missing, inferred from gender if “man” or “woman” selected
Determined by response(s) to a survey item with multiple categories, categorized into those who specified only white/European, or any other response; wording of the Canadian source question changed slightly, from response option “White” in 2017 to “European” in 2018 to “White or European” from 2019 onward
Respondents aged 16 to 19 years were recruited through Nielsen Consumer Insights Global Panel and their partners’ panels, either directly or through their parents. Participants completed a 20-minute online survey, available in English in all countries, as well as in French in Canada. The survey consisted of sociodemographic measures, detailed questions on e-cigarette and tobacco use and perceptions, and additional questions on other health behaviours, including cannabis use. On completion, respondents received remuneration in accordance with their panel’s usual incentive structure, which could include points-based or monetary rewards and/or chances to win monthly prizes.
This study was reviewed and received ethics clearance through a University of Waterloo Research Ethics Committee (ORE#21847/31017) and the King’s College London Psychiatry, Nursing & Midwifery Research Ethics Subcommittee. A full description of the study methods can be found in the Technical Reports (e.g., Hammond et al., 2022).
Measures
Complete versions of the ITC Youth Tobacco and Vaping Surveys—including all measures described below—are publicly available on the project website (http://davidhammond.ca/projects/e-cigarettes/itc-youth-tobacco-ecig/).
Outcomes: perceived ease of accessing substances
All respondents were asked, “How difficult do you think it would be for you to get the following types of substances, if you wanted?” for each of the following: cigarettes; e-cigarette/vaping device/cartridge/e-liquid; alcohol; marijuana or cannabis; ecstasy/MDMA; hallucinogens (LSD, acid, PCP, magic mushrooms, mesc); and, prescription pain killers/opiates (oxycodone/oxycontin, codeine). Response options “Very difficult”, “Fairly difficult”, “Fairly easy”, “Very easy”, and “Don’t know” were collapsed for each substance into binary variables for analysis, “very easy” or “fairly easy” vs. other responses; “Refused” responses were excluded.
Socio-demographic variables
Socio-demographic variables included sex at birth, age, and race/ethnicity. Race/ethnicity was assessed using country-specific racial/ethnic questions with multiple categories, which were recoded to “White (only)” or “Other” (including any other race/ethnicity and not stated) to allow for cross-country comparisons.
Use of cigarettes, e-cigarettes, cannabis, alcohol
Smoking cigarettes and using e-cigarettes/vaping were each assessed, including ever use (“Have you ever tried [cigarette smoking / an e-cigarette/vaped], even one or two puffs?”) and recency of use (“When was the last time you [smoked a cigarette / used an e-cigarette/vaped], even one or two puffs?”). All respondents were asked when they last used cannabis (“When was the last time you used marijuana/cannabis?”). From these items, past 30-day cigarette smoking, vaping, and cannabis use, respectively, were derived. Ever users of alcohol were asked about frequency of alcohol use in the past 12 months; those who indicated “once a month” or more often were categorized as monthly users.
MLA policies
Minimum legal age of sale for cigarettes, e-cigarettes, alcohol and cannabis was documented for each jurisdiction during the time period of 2017–2021: see Table 1 and Supplemental File for all policy implementation dates and coding. For between-country comparisons, country was used as a proxy for national-level MLA policy.
For country-specific analyses examining sub-national policies, indicator variables were created to represent whether respondents were of legal age for sale of a substance, according to their jurisdiction (state/province) at each time point. In the US, a ‘Tobacco 21’ implementation variable was created, based on respondent age and state of residence, as well as the implementation date of the policy to raise MLA for tobacco products to 21 (0=T21 not implemented, 1=T21 implemented for <1 year, 2=T21 implemented 1–2 years, 3=T21 implemented 3+ years; sensitivity analyses also used a version which was the number of months since implementation). In Canada, a minimum legal age variable for tobacco products was created, based on province of residence (0=MLA 18; 1=MLA 19).
Cannabis legalization variables were also created. In the US, this was based on state of residence and date of legalization (0=prohibited, 1=legalized medical only, 2=legalized recreational and medical), since all states that legalized recreational cannabis had a MLA of 21. In Canada, the cannabis policy variable was the same for all provinces prior to federal legalization of recreational cannabis (value of 0), and thereafter based on provincial MLA (1=MLA 18; 2=MLA 19; 3=MLA 21).
Analysis
Post-stratification sample weights were calculated for each country, based on age, sex, geographic region, and race/ethnicity (US only). In addition, subsequent survey waves were calibrated back to wave 1 proportions for student status (student vs. not) and school grades (<70%, don’t know, and refused; 70–79%; 80–89%; 90–100%) and used the National Youth Tobacco Survey (NYTS) in the US and the Canadian Student Tobacco, Alcohol and Drugs Survey (CSTADS) in Canada to calibrate to the trend over time for smoking in the last 30 days. Participants were excluded from the dataset if they failed a data integrity check in which they were asked to select the current month from a list, and were excluded from the analytic sample if not classified for sex, smoking status or vaping status variables.
Weighted estimates with 95% confidence intervals (95% Cis) are reported unless otherwise noted. Descriptive analyses assessed perceived ease of access for each country and substance, over time, as well as by age and use status.
Models comparing substances in the most recent wave
To test differences at the most recent wave (2021Aug), separate logistic regression models were estimated: 1) within each country, within-subjects testing of all pairwise comparisons between each substance (all 7), to examine which substances youth perceive as easier to access than others; and 2) for each substance, testing between countries (all pairwise comparisons), to examine country differences in perceived ease of access for each substance.
Models across waves and countries to examine national policies
To test differences over time and between countries, separate logistic regression models were estimated for perceived ease of access (“very” or “fairly easy” vs. else) for each of cigarettes, e-cigarettes, cannabis, and alcohol. Base models included country (as an indicator for MLA) and survey wave (as a measure of time; categorical), and adjusted for age (categorical), sex, and race/ethnicity [‘White’ (only) vs. else], and contrasts tested wave-to-wave differences (i.e., between each wave and previous wave) within each country and substance. As a second step, the interaction of country and survey wave was added to models for cigarettes, e-cigarettes and cannabis, and the following contrasts were tested: for cigarettes and e-cigarettes, country by wave differences after implementation of T21 in the US (i.e., 2019Aug vs. 2020Feb, 2020Aug, 2021Feb, and 2021Aug), with US as the reference group; for cannabis, country by wave differences after legalization in Canada (2018 vs. 2019, 2020Feb, 2020Aug, 2021Feb, 2021Aug), with Canada as the reference group.
In a subsequent step to examine potential differential effects of policies among users and non-users, past 30-day use status for the substance in question was added to the base model for each substance, as well as the interaction with survey wave; contrasts tested the main effect of use and interaction of ‘use’ variable and survey wave, within each country.
Country-specific models to examine sub-national policies
To examine sub-national policies in the US and Canada for cigarettes, e-cigarettes and cannabis, separate logistic regression models were estimated for perceived ease of access for each substance, and for each country, pooling data across waves. Models adjusted for age (categorical), sex, and race/ethnicity [‘White’ (only) vs. else], and were specified according to the country and substance since policies varied, described below.
In the US, base models for cigarettes and e-cigarettes included an indicator variable for the effect of coverage under state-level policies raising MLA for tobacco products to 21 (individual level, based on respondent age, state, and implementation date for T21, as described above) —categorized as time since T21 implementation (<1 year, 1–2 years, 3+ years) among those of an affected age, and where those who are legally allowed to purchase remain a ‘0’ (i.e., not implemented). Contrasts tested each level of the T21 variable (0 is the referent). As a second step to examine whether the effect of T21 policy implementation differed by age, the interaction of T21 with age was added to each base model, and contrasts examined the simple effect of the T21 variable within each age group, and differences in effects between age groups (vs. age 16).
To examine the effect of cannabis legalization in the US, the base model included an indicator variable for state-level cannabis legalization status (not legal, medical only, or recreational and medical), and contrasts tested each level of the cannabis policy variable. As a second step to examine whether the effect of legalization differed by age, the interaction of legalization status with age was added to each base model, and contrasts examined the simple effect of the legalization variable within each age group, and differences in effect between age groups (vs. age 16).
In Canada, for cigarettes and e-cigarettes, base models included an indicator variable for whether the provincial MLA for tobacco products was 18 or 19. A second step to examine potential differences by age added the interaction for MLA and age, and contrasts examined the simple effect of MLA for each age, as well as differences in effect of MLA between age groups (vs. age 18). For e-cigarettes only, since the implementation of the TVPA in May 2018 was technically the introduction of a national MLA for e-cigarettes, an additional step added time since policy implementation (months; continuous) to the base model (where the pre-TVPA wave in 2017 was coded as 0), and a subsequent step added the interaction of MLA (18/19) and months since policy.
To examine the effects of cannabis legalization and provincial MLA, the base model included a cannabis policy variable, based on province and implementation date of legalization and/or any provincial changes to MLA (18 vs. 19 vs. 21). Contrasts tested each level of the policy variable. As a second step to examine whether the effect of cannabis policy implementation differed by age, the interaction of policy with age was added to each base model, and contrasts examined the simple effect of the policy variable within each age group, and differences in effects between age groups (vs. age 16).
Sensitivity analyses were conducted to adjust for calendar time, by adding a continuous variable for months since first survey (2017Aug) to each Step 1 model (no interaction). In addition, for sub-national models in the US, models were estimated with the indicator variable for ‘state’, to account for state-level differences other than MLA.
RESULTS
Sample
Table 2 presents the characteristics of respondents in each country (N=91,647).
Perceived ease of access between all substances: 2021
Perceived ease of accessing various substances in the most recent wave, August/September 2021, is shown in Figure 1 (see Supplemental Table S1 for all waves). In all countries, the largest proportions of youth perceived alcohol and e-cigarettes as easy to access, followed by cigarettes, cannabis, prescriptions painkillers/opiates, and lastly, ecstasy/MDMA and hallucinogens. Within each country, the percentage of youth who perceived easy access differed between each substance. For example, US youth were less likely to perceive cigarettes as easy to access, compared to e-cigarettes (aOR=0.59, 95%CI 0.54–0.63) or alcohol (aOR=0.74, 95%CI 0.67–0.81). See Supplemental Tables S2 and S3 for all within- and between-country estimates across substances.
Figure 1: Perceived ease of accessing substances among youth aged 16–19, by country, August/September 2021 (n=13,801).
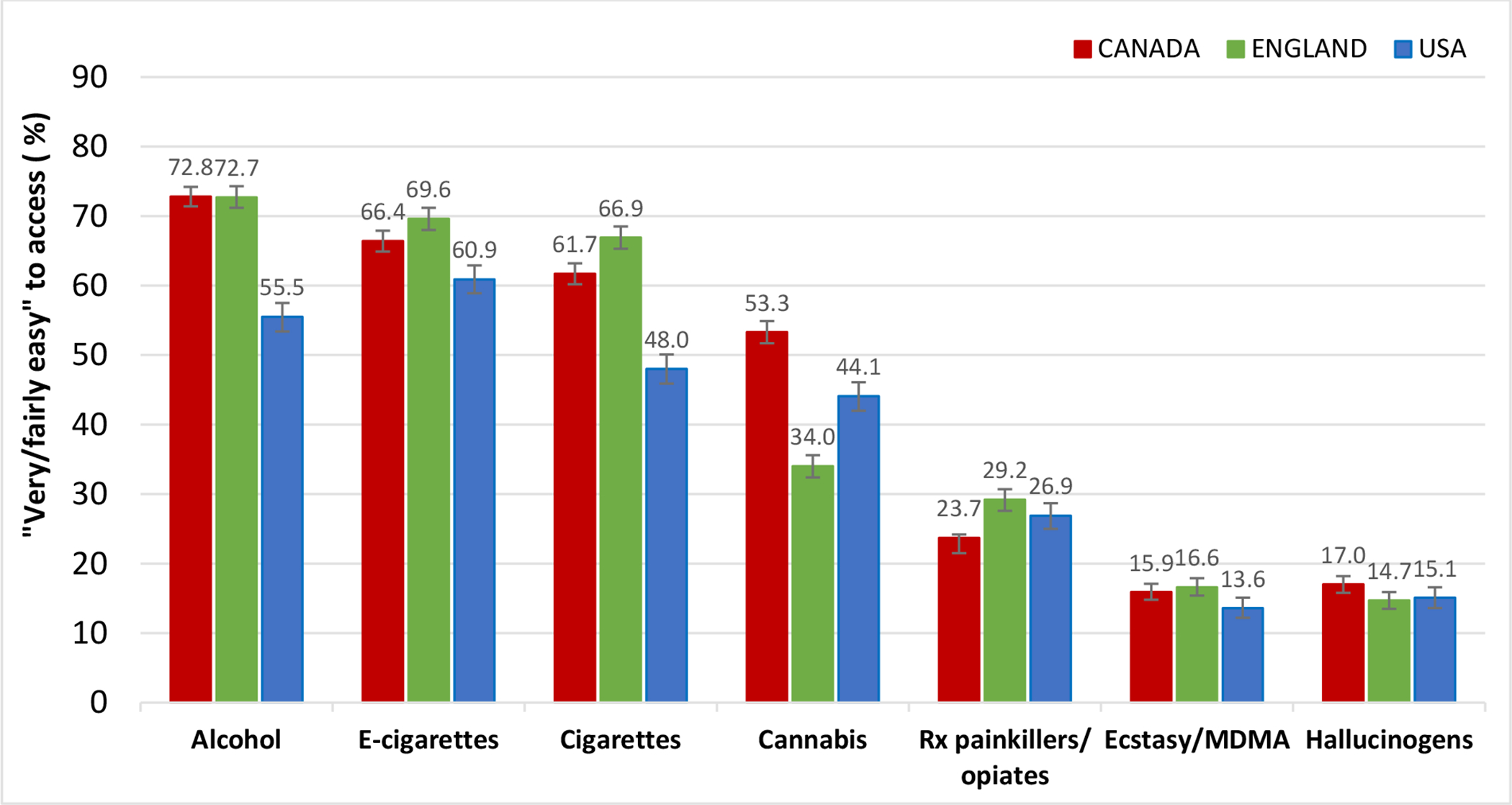
Estimates are weighted % who selected “very easy” or fairly “easy” (vs. else) and 95% confidence intervals.
Trends over time in perceived ease of access: 2017–2021
Figure 2 shows trends over time in perceived ease of access for the four substances that have a minimum legal age and are legal for sale in at least one of the countries: cigarettes, e-cigarettes, cannabis and alcohol. Estimates for other substances—painkillers/opiates, ecstasy/MDMA and hallucinogens—are shown in Supplemental Figure S1.
Figure 2: Perceived ease of accessing substances among youth aged 16–19 and changes in MLA laws by country, 2017–2021 (N=91,647).
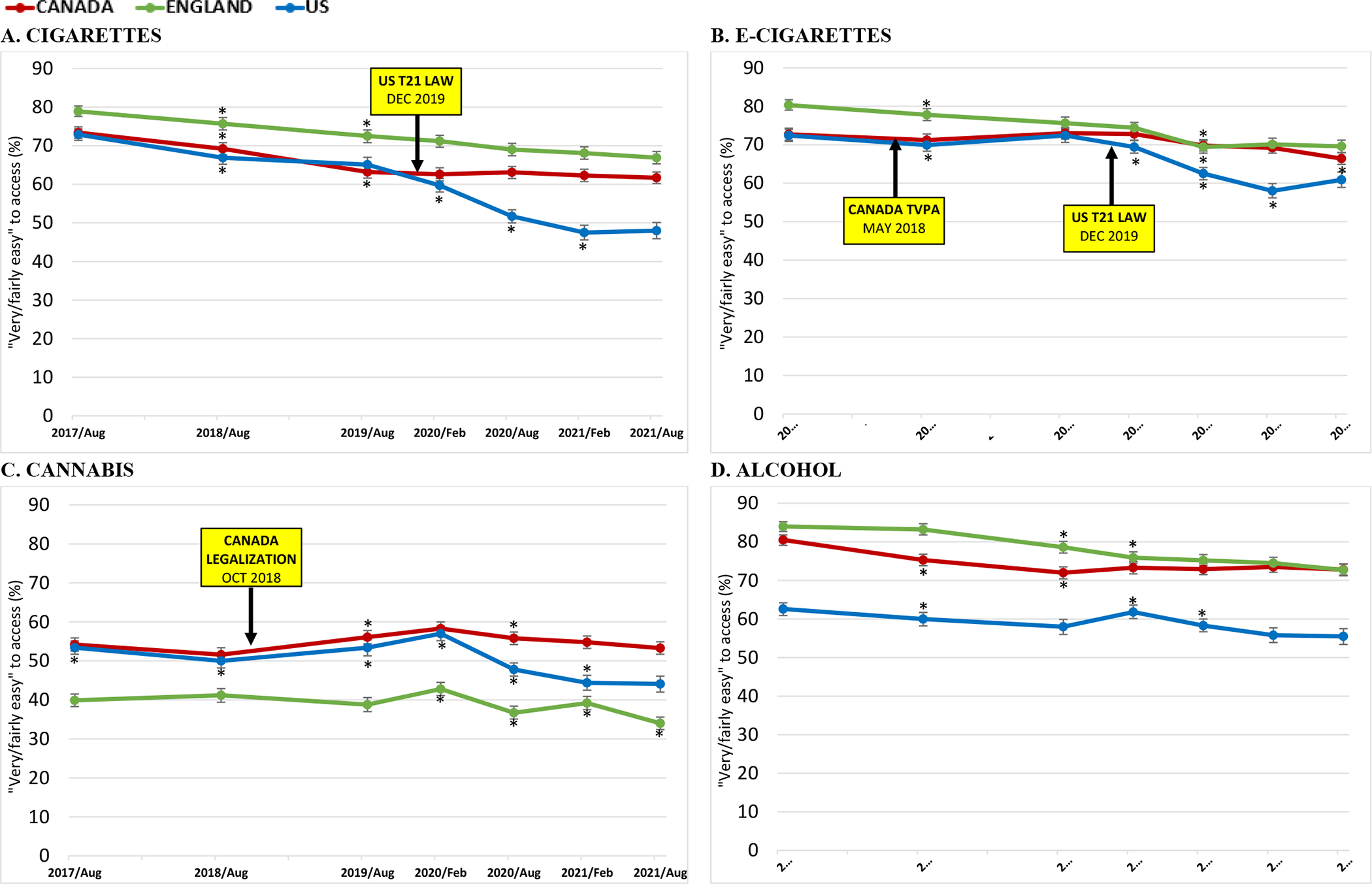
Estimates are weighted % who selected “very easy” or fairly “easy” (vs. else) and 95% confidence intervals
*p<0.05 for between-wave change within country, in model controlling age, sex, race; estimates from all contrasts available in Supplemental Table S4
Perceived ease of accessing cigarettes: differences between countries and over time
In August 2021, youth in the US were less likely to perceive easy access to cigarettes than in Canada (aOR=0.51, 95%CI 0.46–0.57) or England (aOR=0.43, 95%CI 0.39–0.49), while youth in Canada were less likely to perceive easy access to cigarettes than in England (aOR=0.85 95%CI 0.77–0.94). In the US, perceptions that cigarettes were easy to access decreased for three subsequent waves following T21 implementation, before stabilizing in 2021 (2020Feb vs. 2019 aOR=0.80, 95%CI 0.71–0.89; 2020Aug vs. 2020Feb aOR=0.72, 95%CI 0.65–0.80; 2021 Feb vs. 2020Aug aOR=0.85, 95%CI 0.77–0.95; 2021Aug vs. 2021Feb aOR=1.01, 95%CI 0.89–1.13). When the interaction of country and wave was added to the model, perceived ease of access declined to a greater extent in the US between 2019 (pre-implementation) and each subsequent wave after T21 implementation compared to in Canada and England (p<0.01), with the exception of February 2020 in England (p=0.06). See Figure 2 and Supplemental Table S4.
Perceived ease of accessing cigarettes: subnational differences in T21 implementation within the US
A US-specific model examined sub-national T21 policy implementation in the US. Compared to youth in states where T21 was not implemented, youth below the MLA had lower odds of reporting that cigarettes were easy to access when state-level T21 was implemented (p<0.001), including for less than 1 year (aOR=0.57, 95%CI 0.53–0.61), 1 to 2 years (aOR=0.45, 95%CI 0.42–0.48), or 3 or more years (aOR=0.44, 95%CI 0.39–0.50). The interaction term of T21 by age was significant (p<0.001) when added to this model—see Figure 3. Within each age, T21 implementation was associated with lower odds of perceiving easy access to cigarettes compared to when not implemented (p<0.001 for each level); however, the effects were larger among those aged 18 and 19. See Supplemental Table S5.
Figure 3: Perceived ease of accessing tobacco and cannabis among youth aged 16–19, by respondent age and legality/MLA policy, US and Canada, 2017–2021 US – State/federal Tobacco 21 implementation statusa and state-level cannabis legalization status (n=29,719).
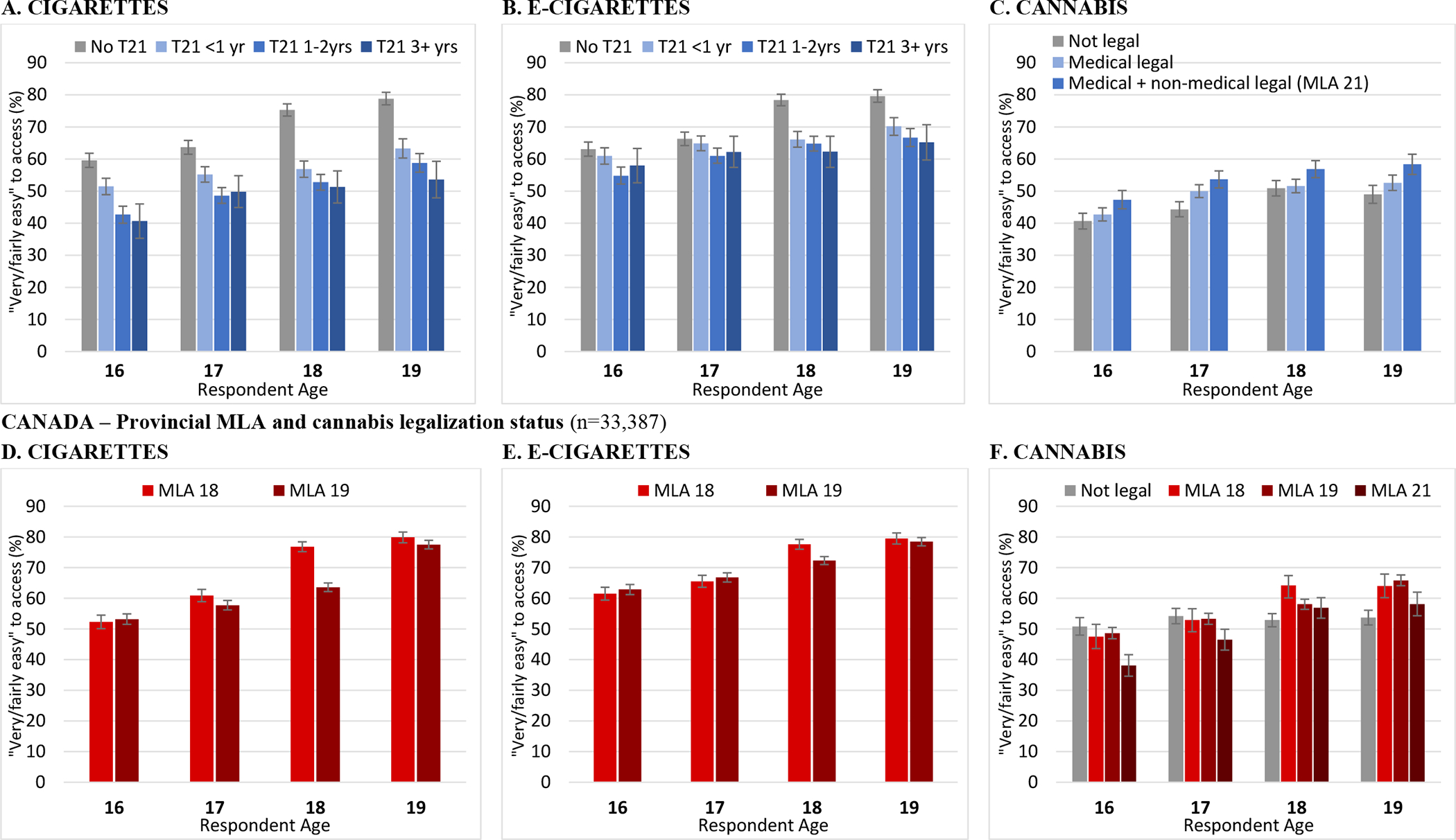
Estimates are weighted % who selected “very easy” or fairly “easy” (vs. else) and 95% confidence intervals
aUS ‘Tobacco 21’ implementation variable applied at individual level based on respondent age, state, and implementation date of the policy to raise MLA for tobacco products to 21: “No T21”=T21 not applied (note: respondents who are legally allowed to purchase stay a ‘0’); “T21 <1yr”=T21 implemented for less than 1 year; “T21 1–2yrs”=T21 implemented for 1–2 years, “T21 3+yrs”=T21 implemented for 3+ years
Estimates from country-specific regression models for each substance available in Supplemental Tables S5 and S6.
Perceived ease of accessing cigarettes: differences between Canadian provinces with different MLA
In a Canada-specific model examining MLA, youth had lower odds of reporting that cigarettes were easy to access in provinces where MLA was 18 versus 19 years of age (aOR=0.84, 95%CI 0.79–0.89; p<0.001). There was a significant interaction of MLA with age (p<0.001) when added to this model: the effect of MLA was significant only for those aged 18 (aOR=0.55, 95%CI 0.49–0.61) as shown in Figure 3. See Supplemental Table S6.
Perceived ease of accessing e-cigarettes: differences between countries and over time
In August 2021, youth in the US were less likely to perceive e-cigarettes as easy to access than in Canada (aOR=0.72, 95%CI 0.65–0.81) or England (aOR=0.67, 95%CI 0.60–0.75). In the US, perceived ease of accessing e-cigarettes decreased in each of the three waves following T21 implementation, before stabilizing in 2021 (2020Feb vs. 2019 aOR=0.87, 95%CI 0.77–0.98; 2020Aug vs. 2020Feb aOR=0.73, 95%CI 0.66–0.82; 2021 Feb vs. 2020Aug aOR=0.84, 95%CI 0.75–0.93; 2021Aug vs. 2021Feb aOR=1.12, 95%CI 0.996–1.26). In Canada, there were no significant between-wave changes in perceived ease of accessing e-cigarettes in the waves immediately following the TVPA implementation in May 2018, although there were significant decreases between 2020Feb and 2020Aug (aOR=0.87, 95%CI 0.78–0.96) and between 2021Feb and 2021Aug (aOR=0.90, 95%CI 0.82–0.995).
When the interaction of country and wave was added to the model to examine differences between the US and other countries after the implementation of T21, the changes between 2019 and February 2020 did not differ between the US and Canada (p=0.13) or England (p=0.39); however, between 2019 and each subsequent wave, declines in perceiving easy access to e-cigarettes were greater in the US than in Canada and England (p<0.01), except for August 2020 in England (p=0.09). See Figure 2 and Supplemental Table S4.
Perceived ease of accessing e-cigarettes: subnational differences in T21 implementation within the US
In a US-specific model examining sub-national T21 policy implementation in the US, compared to youth in states where T21 was not implemented, youth had lower odds of reporting that e-cigarettes were easy to access when state-level T21 was implemented (p<0.001), including for less than 1 year (aOR=0.74, 95%CI 0.69–0.80), 1 to 2 years (aOR=0.64, 95%CI 0.59–0.69), or 3 or more years (aOR=0.67, 95%CI 0.60–0.76). Perceived ease of access within each age by policy implementation is shown in Figure 3. The interaction term of T21 by age was significant (p<0.001): among 18- and 19-year-olds, T21 implementation was associated with lower odds of perceived easy access compared to not implemented (p<0.001 for each level); however, among 16- and 17-year-olds only implementation for 1–2 years (vs. not implemented) was significant. See Supplemental Table S5.
Perceived ease of accessing e-cigarettes: differences between Canadian provinces with different MLA
In a Canada-specific model, there was no overall association between MLA of 18 versus 19 years and youth perceptions that e-cigarettes were easy to access (aOR=1.00, 95%CI 0.94–1.06, p=0.95)—see Figure 3. There was a significant interaction of MLA with age (p<0.001), such that a MLA of 19 (vs. 18) years was associated with decreased odds of perceiving e-cigarettes as easy to access only among 18-year-olds (aOR=0.79, 95%CI 0.70–0.88), while the direction of effect was opposite and of borderline significance among those aged 16 (aOR=1.13, 95%CI 1.01–1.27) and 17 (aOR=1.12, 95%CI 1.004–1.25), and did not make a difference for 19-year-olds (aOR=1.00, 95%CI 0.87–1.14); see Figure 3 and Supplemental Table S6.
Perceived ease of accessing cannabis: differences between countries and over time
In August 2021, youth in Canada were more likely to perceive cannabis as easy to access than in England (aOR=2.43, 95%CI 2.21–2.69) or the US (aOR=1.59, 95%CI 1.43–1.77). Youth in the US were also more likely to perceive cannabis as easy to access than in England (aOR=1.53, 95%CI 1.37–1.71). After legalization in Canada (October 2018), there was a significant increase in perceived ease of accessing cannabis (2019 vs. 2018 aOR=1.17, 95%CI 1.06–1.29), but no changes between subsequent waves, except for a decrease between 2020Aug and 2020Feb (aOR=0.90, 95%CI 0.82–0.99). In the US, perceived ease of accessing cannabis decreased significantly between 2017 and 2018 (aOR=0.87, 95%CI 0.79–0.96), but then increased from 2018 to 2019 (aOR=1.14, 95%CI 1.02–1.27) and from 2019 to 2020Feb (aOR=1.17, 95%CI 1.04–1.30), before again decreasing between 2020Feb and 2020Aug (aOR=0.69, 95%CI 0.63–0.76) and between 2020Aug and 2021Feb (aOR=0.88, 95%CI 0.80–0.98).
In a second step, the interaction of country and wave was added to the model to examine differences between Canada and other countries after cannabis legalization. The changes in Canada between 2018 (pre-legalization) and each subsequent wave (post-legalization) differed significantly (p<0.05) from both England and the US, except that similar increases in perceived ease of access to cannabis were observed in the US between 2018 and both August 2019 (p=0.72) and February 2020 (p=0.60); since then, perceived ease of access to cannabis remained fairly stable in Canada while declining in the US; a more variable but overall declining trend was observed in England. See Figure 2 and Supplemental Table S4.
Perceived ease of accessing cannabis: subnational differences in legalization within the US
In a US-specific model examining sub-national cannabis legalization in the US, perceived ease of accessing cannabis differed significantly by state policy (p<0.001). Compared to youth in states that had not legalized any cannabis use, youth in states that had legalized only medical cannabis use (aOR=1.12, 95%CI 1.05–1.20) or legalized both medical and non-medical use of cannabis (aOR=1.37, 95%CI 1.27–1.48) were more likely to perceive easy access. Youth in states that had legalized both were more likely to perceive easy access than those that legalized only medical use (aOR=1.22, 95%CI 1.14–1.31). When the interaction of state policy and age was added to the base model (including state), there was no significant overall difference in the effect of state policy across ages (p=0.39).
Perceived ease of accessing cannabis: differences between Canadian provinces with different MLA
In a Canada-specific model, there was a significant association between legalization with a MLA of 18 vs. 19 vs. 21 years and youth perceptions that cannabis was easy to access (p<0.001). Compared to when cannabis was not legal, youth in provinces with a MLA of 18 (aOR=1.20, 95%CI 1.10–1.32) or 19 years (aOR=1.18, 95%CI 1.11–1.26) were more likely to perceive cannabis as easy to access, while youth in a province with a MLA of 21 years were less likely (aOR=0.78, 95%CI 0.72–0.86). There was a significant interaction with age (p<0.001): those who were age 16 or 17 were less likely to perceive easy access where MLA was 21 compared to when cannabis was not legal, and those who were age 18 or 19 were more likely to perceive easy access where MLA was 18 or 19 years compared to when cannabis was not legal (see Figure 3).
Perceived ease of accessing alcohol: differences between countries and over time
In August 2021, youth in the US were less likely to perceive alcohol as easy to access than Canada (aOR=0.41, 95%CI 0.37–0.46) or England (aOR=0.45, 95%CI 0.40–0.50). There were few significant between-wave differences (see Figure 2D and Supplemental Table S4).
DISCUSSION
The current paper has three primary findings: 1) youth perceived easy access to a range of substances and perceived access was greater for legal substances, as expected; 2) higher MLA was strongly associated with lower perceived access, including comparisons across countries and different substances within countries; 3) implementation of T21 laws in the US was associated with substantial reductions in perceived ease of accessing cigarettes and e-cigarettes among youth. These findings are discussed in greater detail below.
Youth perceptions of access varied by product and by country, and generally coincided with the legality of substances, with the greatest proportions perceiving easy access to alcohol and tobacco products, and lowest for illicit substances, such as ecstasy/MDMA and hallucinogens. In the case of cannabis, for which legal status differed across countries, perceived access was substantially lower in England, where ‘recreational’ cannabis remains illegal. In sub-national analyses comparing US states with differing cannabis laws, perceived easy access was highest among youth living in states that had legalized recreational cannabis, followed by states that had legalized medical cannabis, with the lowest levels of perceived easy access in states where all cannabis remained illegal. In Canada, changes from pre- to post-legalization of ‘recreational’ cannabis in October 2018 were modest: more youth perceived easy access to cannabis in the period immediately following legalization; however, perceived ease of access returned to pre-legalization levels by 2021. Perceived ease of access for cannabis decreased in all countries after 2020, likely reflecting the onset of the COVID-19 pandemic, which has been associated with reductions in youth cannabis use during its initial stages, possibly due to restricted social interactions and ‘lockdowns’ (NIDA, 2021). However, decreases in perceived access observed in Canada after 2020 were less than those observed in the US and England. In addition, perceived ease of access was lower in Canadian provinces with higher MLAs. Overall, the mixed findings in Canada reflect the widespread availability of cannabis prior to legalization (Wadsworth et al., 2022), and are consistent with the mixed findings to date on differences between US states and perceived access among young people (Brooks-Russell et al., 2019; Harpin et al., 2018; Paschall & Grube, 2020). The impact of legalization on perceived access may also require a longer timeframe to evaluate, given the amount of time for the legal retail market to become established.
We observed a general decline in perceived ease of access for cigarettes in all three countries, although to a greater extent in the US following the implementation of T21 at the federal level (noting that some states had already implemented T21). Prior to the federal T21 law, approximately two-thirds of youth in the US reported it would be fairly or very easy to access cigarettes, compared to less than half in 2021. The current findings are consistent with analyses of state-level T21 policies, which suggested that T21 implementation was associated with declines in smoking among youth below the legal age for tobacco access (Bryan et al., 2020). Given that the federal T21 policy was implemented in close proximity to the onset of COVID-19 pandemic restrictions, the cross-country comparisons in the current study are important for establishing that the decline in the US was greater than other countries which experienced similar pandemic restrictions. The sub-national analyses among US states were also consistent with an effect of T21 laws.
Our findings also suggest that the US T21 law had a similar impact on perceived access to e-cigarettes. As with cigarettes, sub-national differences provided consistent findings: youth living in US states and Canadian provinces with higher MLA reported lower perceived access. Within each of the three countries, more youth perceived easy access to e-cigarettes than to cigarettes, which likely reflects higher prevalence of vaping compared to smoking among youth in the three countries (Hammond et al., 2020). In addition, there was little evidence that perceived access changed in Canada following the federal legislation implemented in May 2018 that liberalized e-cigarette policies and permitted the sale of nicotine containing e-cigarettes without pre-market approval (Government of Canada, 2018). These findings are somewhat surprising, but likely reflect the widespread retail availability and access to e-cigarettes prior to the 2018 legislative change, in which there was little or no enforcement of MLA because no nicotine-containing e-cigarettes were approved for sale (Hammond et al., 2015). Therefore, while the legislation increased the retail availability of e-cigarettes, it was also accompanied by greater enforcement of MLA laws (Health Canada, 2022).
Factors other than MLA changes can also affect perceived access. For example, changes in perceived availability may reflect changes not only in opportunities to obtain tobacco, but also in social norms and demand for tobacco (IOM, 2015). However, the pattern of findings by age suggests that the changes in perceived access observed in the current study are at least partly attributable to MLA laws. In the sub-national analyses that examined perceived access in US states and Canadian provinces with differing MLAs for e-cigarettes, tobacco, and cannabis, the effects were strongest for ages immediately below the MLA. For example, in Canada, the largest differences between youth in provinces with MLA of 18 vs. 19 in perceived easy access to cigarettes and e-cigarettes were observed among youth who were age 18. In addition, while current users (of cigarettes, e-cigarettes and cannabis, respectively) perceived greater ease of access than non-users (see Supplemental Figure S2), patterns over time were similar, suggesting a similar impact of MLA laws on perceived access among users versus non-users.
Limitations
The study has several limitations. Samples were recruited through consumer panels and were not probability-based, although we had large samples in each country and used weighting to increase comparability to national population estimates. The study also used a conservative measure for perceived ease of access, grouping those who said it would be very or fairly easy to access compared to all others, including those who did not know, which may have underestimated the potential effects of policies. In addition, perceived access is a subjective measure, and while it is an important indicator, it does not necessarily indicate actual access to these substances by youth. A variety of factors may drive perceptions of access, including prevalence among friends and family, price and market trends, enforcement, etc., and minimum legal age is just one.
Another factor that may have underestimated potential effects of MLA policies is variation in MLA between bordering jurisdictions (countries or states/provinces); such discrepancies may undermine effects of MLA increases through cross-border purchasing, although cross-border access is less likely to be perceived as “easy”. In addition, as noted, at least 500 US jurisdictions below the state level implemented T21 before the federal date, which may contribute to underestimating the effects of state-level MLA policies. However, differences in perceived access between jurisdictions were observed despite these limitations.
There are some considerations regarding the timing of policy implementation. In the US, subnational T21 policies at the state and local levels in effect before the federal implementation covered approximately half of the US population (Physicians for a Smokefree Canada, 2021). Thus, using the federal T21 implementation date in the between-country comparisons is conservative. In addition, some state-level policies had exemptions for youth who were already of age under the current regulations, so the policy variables were mapped onto current age as closely as possible, but were not exact since respondent birthdates were not available. In Canada, there were changes in 2020 to MLA for tobacco in 2 territories, which were not covered by our survey, and the province of Prince Edward Island (though with an exemption for those who were already 19), which comprises less than 1% of our sample, so we do not expect an impact of these changes on the national estimates.
When examining sub-national differences in the US, existing differences between jurisdictions may have impacted associations between policy variables and perceived access. Sensitivity analyses were conducted to examine including state in each model, yielding the same pattern of results (see Supplemental Table S5), with the exception of cannabis: in the model including state, youth in states that had legalized both medical and non-medical use of cannabis were less likely to perceive easy access than those in states that legalized only medical use or had not legalized any cannabis use, while there was no significant difference for youth in states that had legalized only medical cannabis use.
As noted above, the COVID-19 pandemic occurred shortly after the T21 implementation, and its impact on prevalence of substance use among young people has been documented. However, pandemic impacts are unlikely to account for the observed findings regarding T21 implementation, since perceived ease was already decreasing in early 2020 (pre-pandemic) in the US, and there was not a corresponding drop in perceived access among youth in Canada or England after March 2020. Further, perceived access to other substances such as alcohol or cannabis did not decrease in early 2020 in the US in parallel with cigarettes and e-cigarettes, though decreases for all substances were observed later in 2020, presumably related to the pandemic.
Finally, the study sample included only youth aged 16 to 19 years old, in Canada, England, and the US, so findings cannot be generalized beyond those groups. As demonstrated in the results of the subnational models, associations between MLA and perceived access may differ by age, so patterns may differ among those younger than 16, or those closest to the age affected by MLA changes (e.g., 20-year-olds, for T21 policies).
Conclusions
Minimum legal age was strongly associated with perceived access to substances among youth, and implementation of policies to increase the MLA for cigarettes and e-cigarettes was associated with reductions in perceived access to these products. While the US was the only country in the study to have implemented a national MLA of 21 for tobacco and e-cigarettes, there have been calls to increase the MLA for cigarettes both in Canada (Public Health Agency of Canada, 2020) and in England (Khan, 2022). National surveys in Canada, England and the US indicate support for raising the MLA for tobacco to 21, even among a majority of current and former smokers (Hawkins et al., 2020).
Supplementary Material
Highlights.
Youth’s perceived access to substances examined in Canada, England, US, 2017–2021
Minimum legal age (MLA) was strongly associated with perceived ease of access
Fewer US youth (MLA 21) reported easy access to tobacco vs Canada, England (MLA 18)
Ease of accessing tobacco decreased after minimum legal age increased to 21 in US
Perceived easy access to cannabis greater in Canada vs US and England
Funding sources
This work was supported by the US National Institutes of Health (1P01CA200512). The February/March 2020, February/March 2021, and August 2021 waves of the ITC Youth Tobacco and Vaping Survey were funded by a contribution from Health Canada’s Substance Use and Addictions Program (SUAP). Research reported in this publication was supported by the National Institute on Drug Abuse of the National Institutes of Health and the FDA Center for Tobacco Products (R21DA053614). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the Food and Drug Administration. DH is supported by a Canadian Institutes of Health Research (CIHR)–Public Health Agency of Canada (PHAC) Applied Public Health Research Chair (DH). KE is the recipient of Fellowship funding from the UK Society for the Study of Addiction (SSA). The funders had no role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Footnotes
Declaration of interests
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests:
DH has served as a paid expert witness on behalf of public health authorities in response to legal challenges from tobacco, vaping, and cannabis companies. All other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper
Ethics approval
The authors declare that they have obtained ethics approval from an appropriately constituted ethics committee/institutional review board where the research entailed animal or human participation.
University of Waterloo Research Ethics Committee (ORE#21847/31017) King’s College London Psychiatry, Nursing & Midwifery Research Ethics Subcommittee (RESCM-4113)
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- Ali FRM, Rice K, Fang X, & Xu X (2020). Tobacco 21 policies in California and Hawaii and sales of cigarette packs: a difference-in-differences analysis. Tobacco Control, 29 (50), 588–592. doi: 10.1136/tobaccocontrol-2019-055031. [DOI] [PubMed] [Google Scholar]
- Beard E, Brown J, Jackson S, West R, Anderson W, Arnott D, & Shahab L (2020). Long-term evaluation of the rise in legal age-of-sale of cigarettes from 16 to 18 in England: a trend analysis. BMC Medicine, 18(1), 85. doi: 10.1186/s12916-020-01541-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks-Russell A, Ma M, Levinson AH, Kattari L, Kirchner T, Anderson Goodell EM, & Johnson RM (2019). Adolescent marijuana use, marijuana-related perceptions, and use of other substances before and after initiation of retail marijuana sales in Colorado (2013–2015). Prevention Science, 20, 185–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryan C, Hansen B, McNichols D, & Sabia JJ 2020. (revised April 2021). Do State Tobacco 21 Laws Work? NBER Working Paper 28173. Cambridge, MA: National Bureau of Economic Research. http://www.nber.org/papers/w28173 [Google Scholar]
- Callaghan RC, Sanches M, Gatley J, Cunningham JK, Chaiton MO, Schwartz R, Bondy S, & Benny C (2018). Impacts of Canada’s minimum age for tobacco sales (MATS) laws on youth smoking behaviour, 2000–2014. Tobacco Control, 27, e105–e111. https://tobaccocontrol.bmj.com/content/27/e2/e105 [DOI] [PubMed] [Google Scholar]
- Campaign for Tobacco-Free Kids. (n.d.). States and localities that have raised the minimum legal sale age for tobacco products to 21. https://www.tobaccofreekids.org/assets/content/what_we_do/state_local_issues/sales_21/states_localities_MLSA_21.pdf
- Choi K, Omole T, Wills T, & Merianos AL (2022). E-cigarette-inclusive smoke-free policies, excise taxes, tobacco 21 and changes in youth e-cigarette use: 2017–2019. Tobacco Control, 31, 758–761. doi: 10.1136/tobaccocontrol-2020-056260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dave D, Feng B, & Pesko MF (2019). The effects of e-cigarette minimum legal sale age laws on youth substance use. Health Economics, 28(3), 419–436. 10.1002/hec.3854 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeJong W, & Blanchette J (2014). Case closed: Research evidence on the positive public health impact of the age 21 minimum legal drinking age in the United States. Journal of Studies on Alcohol and Drugs, Supplement, 75, 108–115. doi: 10.15288/jsads.2014.75.108 [DOI] [PubMed] [Google Scholar]
- Doubeni CA, Li W, Fouayzi H, & Difranza JR (2008). Perceived accessibility as a predictor of youth smoking. Annals of Family Medicine, 6(4), 323–330. doi: 10.1370/afm.841 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammond D, Reid JL, Burkhalter R, & Rynard VL (2022). ITC Youth Tobacco and E-Cigarette Survey: Technical Report – Wave 5 (2021 - August). Waterloo, ON: University of Waterloo. http://davidhammond.ca/projects/e-cigarettes/itc-youth-tobacco-ecig/ [Google Scholar]
- Hammond D, Rynard V, & Reid JL (2020). Changes in prevalence of vaping among youth in the United States, Canada, and England, 2017 to 2019. Journal of the American Medical Association – Pediatrics, 174(8), 797–800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammond D, White CM, Czoli CD, Martin CL, Magennis P, & Shiplo S (2015). Retail availability and marketing of e-cigarettes in Canada. Canadian Journal of Public Health, 106(6), e408–e412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harpin SB, Brooks-Russell A, Ma M, James KA, & Levinson AH (2018). Adolescent marijuana use and perceived ease of access before and after recreational marijuana implementation in Colorado. Substance Use & Misuse, 53, 451–56. doi: 10.1080/10826084.2017.1334069 [DOI] [PubMed] [Google Scholar]
- Hawkins SS, Chung-Hall J, Craig L, Fong GT, Borland R, Cummings KM, Levy D, & Hitchman SC (2020). Support for Minimum Legal Sales Age Laws Set to Age 21 Across Australia, Canada, England, and United States: Findings From the 2018 ITC Four Country Smoking and Vaping Survey. Nicotine & Tobacco Research, 22(12),2266–2270. doi: 10.1093/ntr/ntaa119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Health Canada. (2022, March). Vaping compliance and enforcement. https://www.canada.ca/en/health-canada/services/smoking-tobacco/vaping/compliance-enforcement.html
- Institute of Medicine (IOM). (2015). Public health implications of raising the minimum age of legal access to tobacco products. Washington, DC: The National Academies Press. [PubMed] [Google Scholar]
- Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, & Patrick ME (2021). Monitoring the Future national survey results on drug use 1975–2020: Overview, key findings on adolescent drug use. Ann Arbor: Institute for Social Research, University of Michigan. [Google Scholar]
- Khan J (2022, June 9). The Khan review: Making smoking obsolete. Published to GOV.UK [pdf only]. Office for Health Improvement and Disparities. https://www.gov.uk/government/publications/the-khan-review-making-smoking-obsolete [Google Scholar]
- Kuipers MAG, Brandhof SD, Monshouwer K, Stronks K, & Kunst AE (2017).. Impact of laws restricting the sale of tobacco to minors on adolescent smoking and perceived obtainability of cigarettes: an intervention–control pre–post study of 19 European Union countries. Addiction, 11(2): 320–329. 10.1111/add.13605 [DOI] [PubMed] [Google Scholar]
- Marynak K, Mahoney M, Williams KS, Tynan MA, Reimels E, & King BA (2019). State and Territorial Laws Prohibiting Sales of Tobacco Products to Persons Aged <21 Years - United States, December 20, 2019. Morbidity and Mortality Weekly Report, 69(7), 189–192. doi: 10.15585/mmwr.mm6907a3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. (2012). Preventing Tobacco Use Among Youth and Young Adults: A Report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention (US). https://www.cdc.gov/tobacco/sgr/2012/index.htm [PubMed] [Google Scholar]
- National Center on Addiction and Substance Abuse. (2011). Adolescent Substance Use: America’s #1 Public Health Problem. New York, NY: CASA. https://eric.ed.gov/?id=ED521379 [Google Scholar]
- National Institute on Drug Abuse (NIDA). (2021, December 15). Percentage of adolescents reporting drug use decreased significantly in 2021 as the COVID-19 pandemic endured. https://nida.nih.gov/newsevents/news-releases/2021/12/percentage-of-adolescents-reporting-drug-use-decreased-significantly-in-2021-as-the-covid-19-pandemic-endured [Google Scholar]
- Paschall MJ, & Grube JW (2020). Recreational marijuana availability in Oregon and use among adolescents. American Journal of Preventive Medicine, 58, e63–e9. doi: 10.1016/j.amepre.2019.09.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Physicians for a Smoke-Free Canada. (2021, April 12). Tobacco 21 – More evidence on the benefits of raising the minimum legal age. http://smoke-free.ca/SUAP/2021/tobacco%2021.pdf [Google Scholar]
- Preventing Tobacco Addiction Foundation. (2022). Tobacco 21: The Law of the Land [Tobacco 21 State Laws in Order of Enactment and their Date of Implementation]. Retrieved 31 March, 2022 from https://tobacco21.org [Google Scholar]
- Public Health Agency of Canada. (2020, January 22). Statement from the Council of Chief Medical Officers of Health on Nicotine Vaping in Canada. https://www.canada.ca/en/public-health/news/2020/01/statement-from-the-council-of-chief-medical-officers-of-health-on-nicotine-vaping-in-canada.html [Google Scholar]
- Schiff S, Liu F, Boley Cruz T, Unger JB, Cwalina S, Leventhal A, McConnell R, & Barrington-Trimis J (2021). E-cigarette and cigarette purchasing among young adults before and after implementation of California’s tobacco 21 policy. Tobacco Control, 30(2), 206–211. doi: 10.1136/tobaccocontrol-2019-055417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van der Eijk Y & Chen J I-P. (2022). Case for raising the minimum legal age of tobacco sale to 25. Tobacco Control, 31, 487–492. https://tobaccocontrol.bmj.com/content/31/3/487 [DOI] [PubMed] [Google Scholar]
- Wadsworth E, Driezen P, Chan G, Hall W, & Hammond D (2022). Perceived access to cannabis and ease of purchasing cannabis in retail stores in Canada immediately before and one year after legalization. American Journal of Drug and Alcohol Abuse, 48(2), 195–205. [DOI] [PubMed] [Google Scholar]
- Wagenaar AC, & Toomey TL (2002). Effects of minimum drinking age laws: Review and analyses of the literature from 1960 to 2000. Journal of Studies on Alcohol, 63(Suppl 14), 206–225. doi: 10.15288/jsas.2002.s14.206 [DOI] [PubMed] [Google Scholar]
- Warren JC, Smalley KB, & Barefoot KN (2015). Perceived ease of access to alcohol, tobacco and other substances in rural and urban US students. Rural Remote Health, 15(4), 3397. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.