

Abstract
Objective
We present a case of intraprocedural device malfunction related to the JET 7 Xtra Flex reperfusion catheter during mechanical thrombectomy.
Case Presentation
A 92-year-old man presented with sudden right hemiparesis with a National Institutes of Health Stroke Scale score of 22. His left middle cerebral artery (M1) was occluded, and emergency mechanical thrombectomy was performed. After partial recanalization was achieved, angiography through a JET 7 Xtra Flex was attempted. After manual injection of contrast media via a 10-mL syringe through the JET 7 Xtra Flex, the catheter moved, jumping forward, and the distal tip of the catheter expanded and ruptured. This resulted in intracranial vessel damage and subsequent patient death.
Conclusion
Contrast media must not be injected through the JET 7 Xtra Flex. If contrast media needs to be injected for angiography during mechanical thrombectomy with a reperfusion catheter, it should always be through the guide catheter.
Keywords: acute ischemic stroke, mechanical thrombectomy, JET 7, complication, combined technique
Introduction
Mechanical thrombectomy for emergent large vessel occlusion rapidly became common after its efficacy was demonstrated by several randomized controlled studies in 2015.1) To quickly recanalize occluded vessels, the advancement of therapeutic devices for mechanical thrombectomy is essential, for which device manufacturers have newly developed many stent retrievers with different diameters, lengths, and structures. On the other hand, many large-bore reperfusion catheters with excellence in guidance have recently been developed and become used at clinical settings. JET 7 Xtra Flex (Penumbra, Alameda, CA, USA) is a new reperfusion catheter launched in Japan since January 2020. Although it has a large lumen diameter of 0.072 inches, it is excellent for guidance and easily reaches intracranial occluded vessels, being launched as a new device capable of rapidly acquiring recanalization.
We report a case of intraprocedural device malfunction related to the JET 7 Xtra Flex reperfusion catheter. The catheter tip ruptured after partial balloon-like expansion when angiography was performed through the JET 7 Xtra Flex placed in the intracranial internal carotid artery. As the event resulted in rupture of a vessel and caused serious complications, we present the case to provide information to neuroendovascular therapists.
Case Presentation
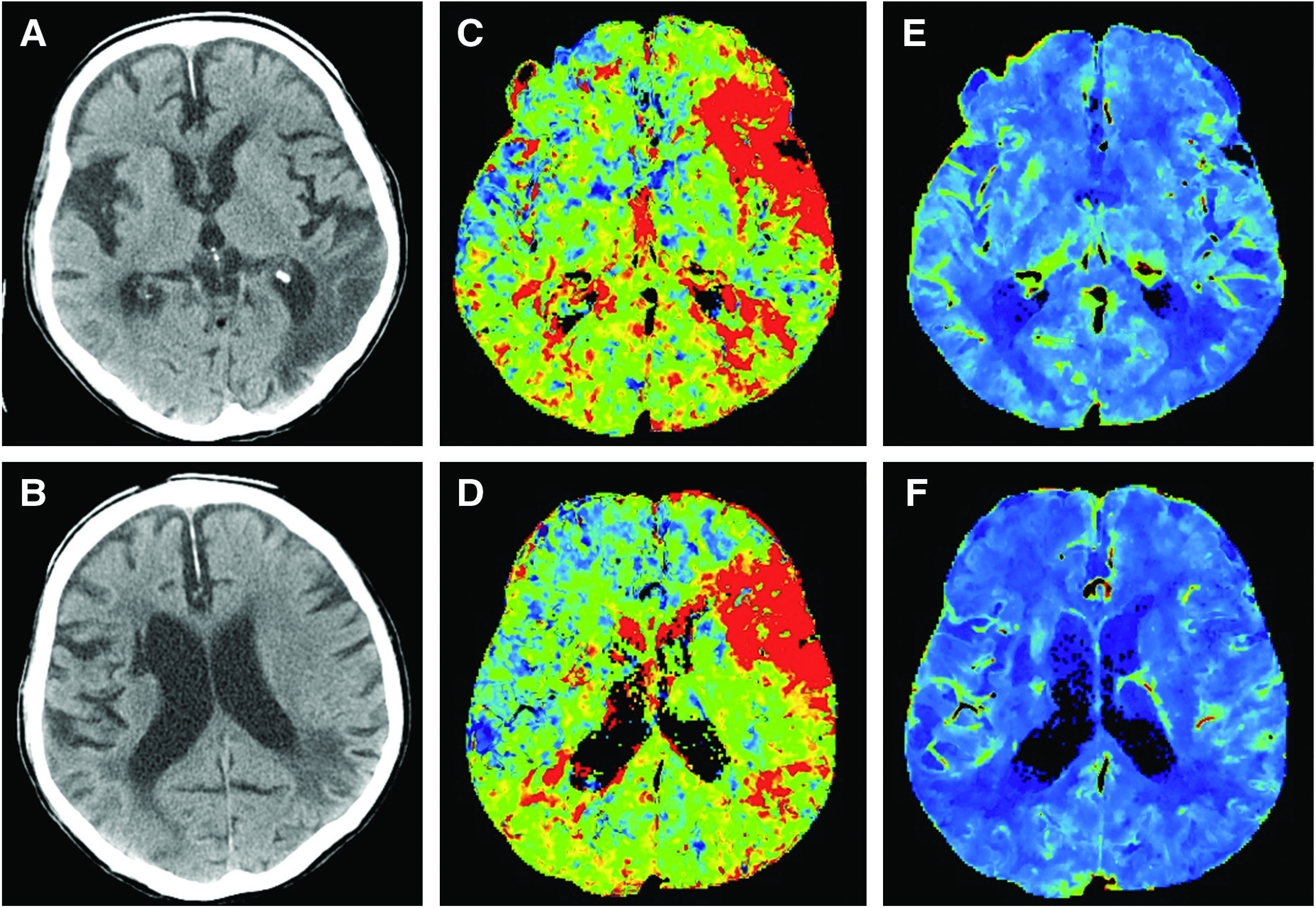
A 92-year-old man presented with sudden disturbance of consciousness, aphasia, and right hemiparesis with a National Institutes of Health Stroke Scale score of 22. His past medical history was significant for atrial fibrillation, hypertension, and cerebral infarction. On plain CT, old cerebral infarction was noted in the left parietotemporal lobe. On CT perfusion, delay of time-to-maximum of residue function (Tmax) was observed in the left middle cerebral artery territory without a decrease in the cerebral blood volume (CBV) in this area (Fig. 1). Immediate mechanical thrombectomy was decided to perform because a penumbra region was present in the left middle cerebral artery territory.
Fig. 1 . On plain CT (A and B), old cerebral infarction was present in the left parietotemporal lobe. On CT perfusion, delayed Tmax (C and D) was noted in the left middle cerebral artery territory but no decrease in CBV (E and F) was noted in the same area. CBV: cerebral blood volume; Tmax: time-to-maximum of residue function.
Endovascular treatment
Under local anesthesia, a 9-Fr 90-cm Branchor (Asahi Intecc, Aichi, Japan) was guided to the left internal carotid artery through the right femoral arterial approach. Angiography was performed, and occlusion of the left middle cerebral artery (distal M1) was confirmed (Fig. 2A and 2B). When the JET 7 Xtra Flex was advanced to the occluded region over a microcatheter (Velocity; Penumbra) and 0.014-inch micro guide wire (CHIKAI; Asahi Intecc), it reached the thrombus and thrombectomy by direct aspiration using a suction pump (Penumbra ENGINE; Penumbra) was performed. Partial recanalization was noted on angiography performed later, but residual occlusion was present in the M2 superior branch of the left middle cerebral artery, for which a stent retriever (Trevo ProVue 3 × 20 mm; Stryker, Kalamazoo, MI, USA) was applied to the thrombus in the M2 superior branch. During aspiration through the JET 7 Xtra Flex with the ENGINE, the Trevo ProVue stent retriever was retrieved without resistance by pulling it into the JET 7 Xtra Flex. Angiography was then performed through the JET 7 Xtra Flex placed in the intracranial left internal carotid artery, but complete recanalization was not noted and an avascular area remained in the frontal lobe over the parietal lobe (Fig. 2C and 2D). After investigation of continuation of the procedure for partial recanalization, secondary angiography through the JET 7 Xtra Flex positioned in the left carotid siphon was decided. Angiography was performed after confirming back flow of blood into a 10-cc syringe connected to the JET 7 Xtra Flex, but contrast medium did not flow out from the tip. The JET 7 Xtra Flex tip instead exhibited jump-like movement, followed by ballooning of the catheter and rupture (Fig. 3). Immediately after rupture, blood flow in the cervical left internal carotid artery was temporarily occluded by a balloon of the guiding catheter and heparin was simultaneously neutralized. The patient became comatose and his breathing weakened, for which anesthetic management with tracheal intubation and a ventilator was performed. Cone-beam CT was performed after vital signs stabilized, and the presence of extensive subarachnoid hemorrhage was confirmed. It was considered that the left internal carotid artery over the middle cerebral artery (M1) ruptured due to the abnormal expansion of the JET 7 Xtra Flex. To stop the bleeding from the injured vascular region, a microcatheter, SL-10 (Stryker) was guided to M1 using a CHIKAI micro wire, but it was difficult because the lumen structure of the JET 7 Xtra Flex was broken. The SL-10 microcatheter was guided to M1 by passing through the broken side wall of the JET 7 Xtra Flex (Fig. 4A), and its presence in M1 was confirmed by angiography through the SL-10 microcatheter. M1 over the intracranial internal carotid artery was filled with Target coils (Stryker) backward, with which the broken JET 7 Xtra Flex was also pulled back little by little. There was resistance, but it was able to be removed and retrieved from the body. After stopping bleeding from the hemorrhagic region with detachable coils and the absence of bleeding from the guiding catheter was confirmed by left internal carotid artery angiography, the procedure was completed (Fig. 4B and 4C). On postoperative CT, diffuse subarachnoid hemorrhage, intraventricular hematoma, and ventricular enlargement were observed (Fig. 4D). The retrieved JET 7 Xtra Flex was broken by 25 mm at a site 5 mm from the tip toward the proximal side, the outer layer polymer was torn in a 20-mm range, and the coil wind was fully stretched and popped out (Fig. 5). Ventricular drainage was performed on the same day and whole-body management was performed thereafter, but the patient died on the 10th hospital day.
Fig. 2 . Angiography (A and B) at initiation of the procedure. The distal M1 of the left middle cerebral artery was occluded. Angiography (C and D) immediately before the accident. A residual avascular area was present in the left frontal lobe over the parietal lobe on angiography through the JET 7 Xtra Flex positioned at the left carotid siphon.

Fig. 3 . Angiography (frontal view: A–D, lateral view: E–H) at rupture of the JET 7 Xtra Flex. The JET 7 Xtra Flex tip was positioned at the left carotid siphon. When contrast medium was injected, it did not flow out from the catheter tip (A and E). The JET 7 Xtra Flex tip instead exhibited jump-like movement, and then expanded like a balloon (B, C, F, and G) and ruptured (D and H). White arrows: JET 7 Xtra Flex tip.
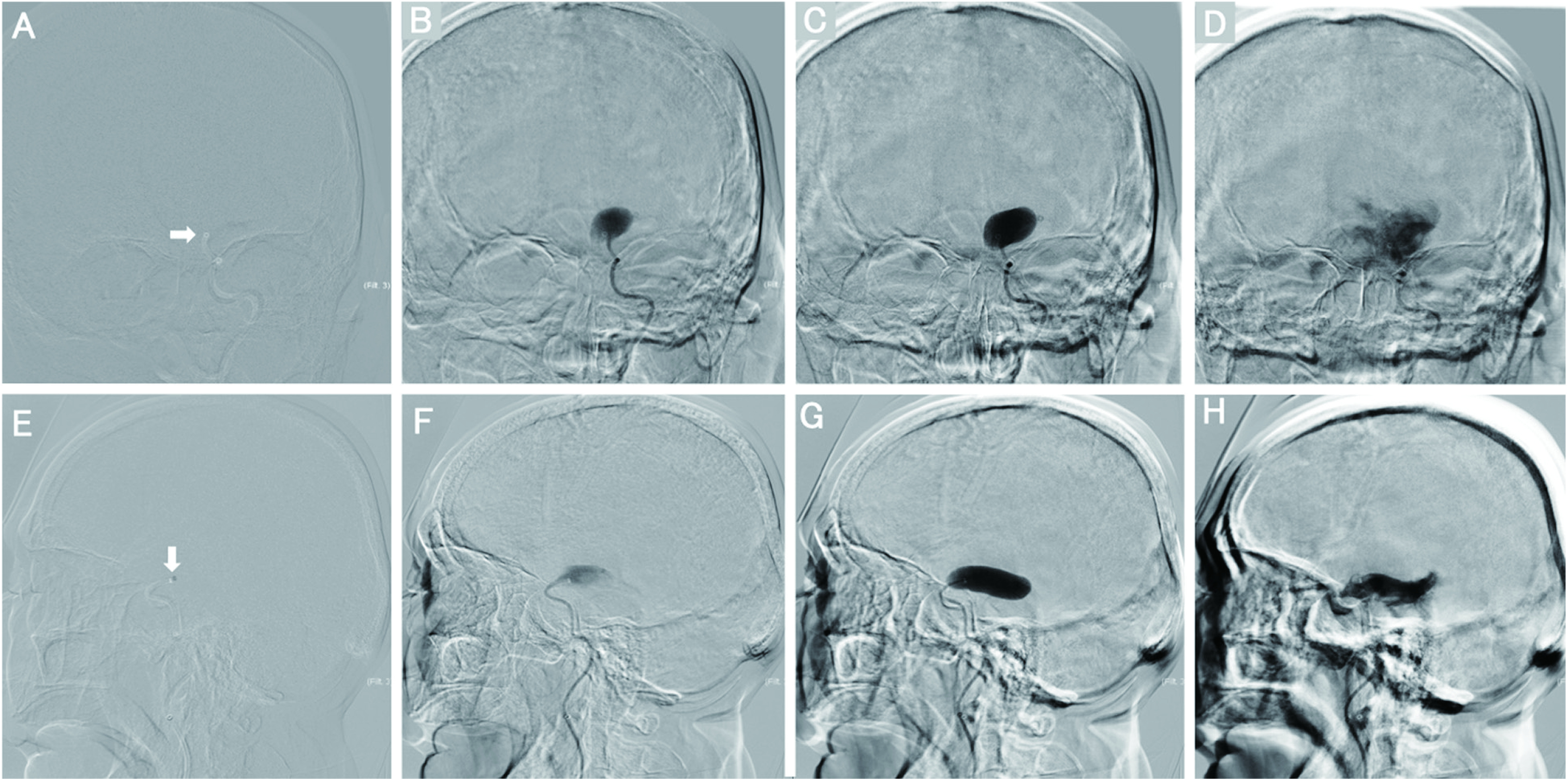
Fig. 4 . (A) An SL-10 microcatheter passed through the broken side wall of the JET 7 Xtra Flex and it was guided to the left middle cerebral artery (M1). (B) Internal trapping by detachable coils from the left middle cerebral artery (M1) to the left internal carotid artery. (C) Angiography of the left internal carotid artery at the end of procedure: No extravasation from the injured vessel was noted. (D) Head CT immediately after endovascular surgery: Diffuse subarachnoid hemorrhage, intraventricular hematoma, and ventricular enlargement were observed. White arrow: JET 7 Xtra Flex tip.
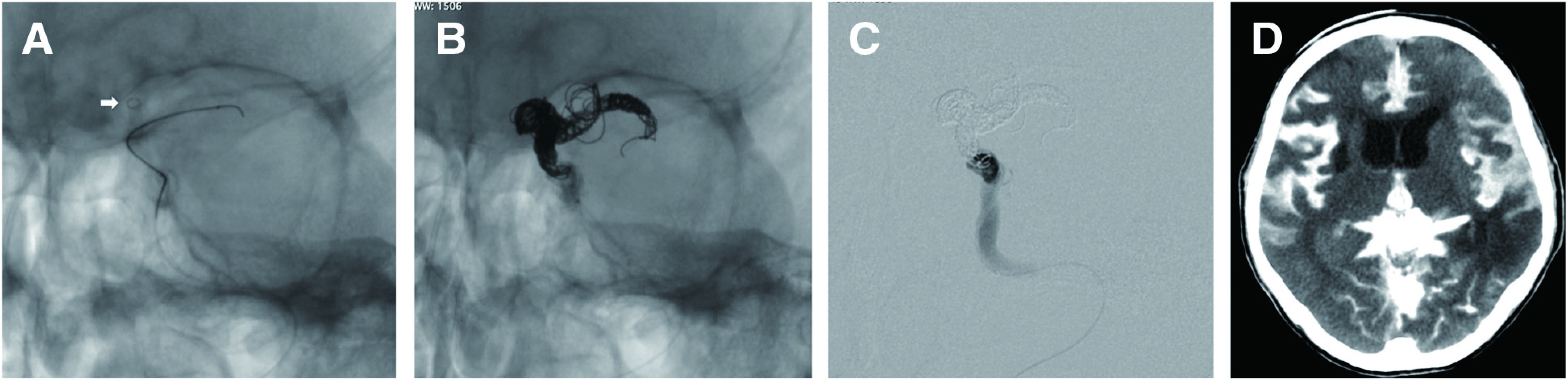
Fig. 5 . Damaged JET 7 Xtra Flex. The JET 7 Xtra Flex was broken at a site 5 mm from the tip by 25 mm toward the proximal side, the outer layer polymer was torn in a 20-mm range, and the coil wind was fully stretched and popped out.

Discussion
The JET 7 Xtra Flex became reimbursed by health insurance on January 1, 2020, and was launched on January 6, 2020 in Japan. It is a new reperfusion catheter with a large bore diameter of 0.072 inches. Regarding the structure, in addition to a helical coil wind made of stainless steel and nitinol, and a full-length polytetrafluoroethylene (PTFE) liner of the tip over the hand region, a new flexible polymer was adopted for the catheter tip, which enabled retention of the lumen while being flexible. This was the first case of a disruptive accident after its launch in Japan. As of June 2020, serious accidents in which ballooning of the JET 7 Xtra Flex occurred and the catheter ruptured have been reported in 3 cases (all died) in Japan and 8 cases in other countries. Thus, the domestic agent, Medico’s Hirata Inc. (Osaka, Japan), voluntarily suspended shipment in Japan from June 18, 2020. As disruptive accidents continued to be reported in the US, Penumbra Inc. issued the following notification approved by the US Food and Drug Administration on July 27, 2020.2) The main content was as follows: 1) Please do not inject contrast medium using a syringe through the JET 7 Xtra Flex and 2) please do not use stent devices of other companies because the safety and efficacy have not been confirmed. It remained as a notification to users, and its sale continued. Adverse events due to abnormal expansion have been reported thereafter3,4) and recall information was posted on the home page of the manufacturer, Penumbra Inc., that the JET 7 Xtra Flex may expand like a balloon and rupture on December 15, 2020, in the US, and the product was urgently recalled.5) According to the announcement by Penumbra Inc., the company confirmed 17 cases (0.056%) of adverse events due to expansion or rupture of the catheter tip and 14 cases (0.046%) of death out of more than 30000 cases of the use of the JET 7 Xtra Flex.
Regarding the cause of catheter tip expansion, an interview with the manufacturer and operator, and investigation by the Internal Accident Investigation Committee were performed. Penumbra Inc. stated in an online conference with our hospital that although similar cases at clinical settings have been confirmed, the cause was unclear. However, they mentioned the following possible cause: In this event, the inner liner of the catheter was damaged at some point during the procedure and the condition became pressurized at the time of contrast medium injection, which may cause catheter expansion. Pulling the stent retriever into a JET 7 Xtra Flex may cause damage, but the event may occur even if no stent retriever is used, i.e., the event may occur even when the procedure is performed using only a reperfusion catheter. Furthermore, abnormal events are common at the time of contrast medium injection and when the inner liner is damaged, and may occur at the time of injection of liquid other than contrast medium (blood or saline). The operator in the present case was a resident, but he had already experienced dozens of cases of mechanical thrombectomy and was familiar with handling the devices, including reperfusion catheters. In the interview with the operator, backflow of blood was confirmed and subsequent contrast medium injection by pushing by hand was sensed as usual without resistance. Therefore, no abnormality, such as pressure on the hand, was noted in this event, suggesting that the catheter readily expanded due to an abnormality without sensing resistance. The time from expansion, which was generated in the catheter and enabled it to rupture, was 4 frames or approximately 1 second; therefore, it may be difficult to avoid rupture even if the abnormality is noticed when expansion starts. For safety, a method confirming patency of the catheter, for example, 1) confirmation of backflow of blood and 2) injection of a small volume of contrast medium from the tip, may enable safe angiography. On the other hand, occurrence of a similar event has been reported even though patency of the lumen of JET 7 Xtra Flex was confirmed by these methods; thus, these are not effective means to confirm the safety. In the present case, it is possible that vulnerability of the catheter itself was involved and it was difficult for the operator to avoid this complication. At our hospital, the Internal Accident Investigation Committee was established immediately after the accident, aiming at investigation of the cause and recurrence prevention measures, and performed the investigation. Based on the online conference with Penumbra Inc. and accident investigation, the operation at the time of accident was standard and damage beyond expectation may have occurred. The catheter used in this case at our hospital was the JET 7 Xtra Flex, in which the material at the catheter tip was different from the initial model, JET 7 Standard Tip, sold in other countries, and only JET 7 Xtra Flex was introduced in Japan. According to the report from Penumbra Inc., the device for which rupture accidents have been reported is only JET 7 Xtra Flex and no similar case has occurred in the preceding model, JET 7 Standard Tip or the earlier generation model ACE68 (Penumbra), suggesting that the rupture accident in the present case was a characteristic phenomenon of the JET 7 Xtra Flex and it was presumed to be due to vulnerability of the structure of the catheter tip.
At present, a combined technique concomitantly using a reperfusion catheter and a stent retriever in mechanical thrombectomy has widely spread,6–8) but this complication was an accident highlighting the risk of device damage by the combined technique and angiography through the reperfusion catheter. When the combined technique is used, the possibility of damaging the lining membrane of the reperfusion catheter by friction of pulling a stent retriever into the catheter is always present, and the risk may increase as the frequency of pulling back increases. In addition, each device company uses the latest technology to retain flexibility and lumen of reperfusion catheters with a large bore, but the tip may become vulnerable and damaged due to such a large bore. As the size and location of the thrombus are confirmed by this combined technique, angiography through a reperfusion catheter and microcatheter, i.e., the sandwich angiography technique, is becoming an accepted practice at clinical settings, and contrast medium injection through the reperfusion catheter guided into the intracranial vessels has become increasingly performed because the time of the procedure is shorter and angiography is clear. Therefore, as manual angiography through the reperfusion catheter is often performed at clinical settings, each manufacturer has set a pressure resistance limit to be endured in manual angiography as a criterion. However, these are results of in vitro experiments and no lumen damage related to the procedure was expected. Therefore, it cannot be said that there is no risk of expansion or rupture of reperfusion catheter products of other companies other than JET 7 Xtra Flex.
During investigation of the medical accident, first, regarding the combined technique, as the safety of and caution for concomitant use are not described in the package insert of each device, the combined technique is regarded as a treatment method independently judged by physicians, although it is conventional, and evidence for the safety and efficacy is not established. Indeed, the manufacturer commented that co-treatment with a stent retriever from other company is not recommended. Moreover, regarding angiography in cases using a reperfusion catheter, the package insert states to perform angiography through the guiding catheter after removing the reperfusion catheter, injection with a high pressure by an automatic injector is the only contraindication, and manual angiography through the reperfusion catheter is not recommended, although it is not contraindicated. Accordingly, the manufacturer commented that angiography through the reperfusion catheter is not recommended because the JET 7 Xtra Flex acquired pharmaceutical approval for its specific use for thrombus suction; i.e., when a medical accident occurs, even though the procedure is a conventional treatment method frequently described in reports and academic meetings, it may be regarded as performed based on the independent judgment made by a physician as off-label use, to which attention should be paid. It was also necessary in the present case to perform confirmation angiography after thrombectomy through the guiding catheter as a procedure recommended in the package insert.
The combined technique is roughly divided into 2 types: The stent retriever is not pulled back into the reperfusion catheter and it is retrieved as a unit, such as in the continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE) method6) and stent retriever assisted vacuum-locked extraction (SAVE) method,7) and the a stent-retrieving into an aspiration catheter with proximal balloon technique (ASAP) method8) in which the stent retriever is pulled back into the reperfusion catheter and the reperfusion catheter is left in the intracranial vessels. The present adverse event was caused by angiography after the stent retriever was pulled into the JET 7 Xtra Flex and retrieved. The reperfusion catheter was not removed from the body and left in the intracranial vessels in consideration of the next procedure being able to be promptly performed in case recanalization cannot be achieved. However, based on this accident, the combined technique of leaving the reperfusion catheter in the intracranial vessels cannot be recommended, i.e., there are some points that require attention, such as that angiography must not be performed through the reperfusion catheter and damage of the reperfusion catheter cannot be confirmed after pulling the stent retriever into the catheter. Therefore, at present, we choose the procedure for the combined technique in which the stent retriever is not pulled back into the reperfusion catheter and angiography is performed through the guiding catheter as a unit after retrieval.
We reported an unexpected adverse event, expansion of the JET 7 Xtra Flex. The Internal Accident Investigation Committee presumed that it was a complication characteristic to the JET 7 Xtra Flex, but many harmful accidents have occurred before the product was recalled. It is necessary to prevent similar accidents by making this case well known, and we want to emphasize the following 2 points: Angiography must not be performed through a JET 7 Xtra Flex and angiography should be performed through the guiding catheter in cases using a reperfusion catheter other than a JET 7 Xtra Flex.
Conclusion
We reported an unexpected disruptive accident that is considered characteristic to the JET 7 Xtra Flex. Angiography must not be performed through a JET 7 Xtra Flex. In treatment using the combined technique, attention should be sufficiently paid to damage of the devices and angiography should be performed through the guiding catheter when a reperfusion catheter is used.
Disclosure Statement
The authors declare no conflicts of interest.
References
- 1). Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta- analysis of individual patient data from five randomised trials. Lancet 2016; 387: 1723–1731. [DOI] [PubMed] [Google Scholar]
- 2). Penumbra Inc . Notification to healthcare providers; 2020, Available: http://www.penumbrainc.com/wp-content/uploads/2020/07/FINAL-Notification-to-Healthcare-Providers-27Jul20202.pdf. (Accessed: March 31, 2021)
- 3). Pearly Ti J, Yeo L, Anil G. Can a stent retriever damage the JET 7 reperfusion catheter? AJNR Am J Neuroradiol 2020; 41: 2317–2319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4). Majidi S, Bageac DV, Fayed I, et al. JET 7 XTRA Flex reperfusion catheter related complications during endovascular thrombectomy. J Neurointerv Surg 2021; 13: 352–356. [DOI] [PubMed] [Google Scholar]
- 5). Penumbra Inc . Urgent voluntary medical device recall notification immediate action required; 2020, Available: https://www.penumbrainc.com/wp-content/uploads/2020/12/JET-7XF-15Dec20.pdf. (Accessed: March 31, 2021)
- 6). McTaggart RA, Tung EL, Yaghi S, et al. Continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE): a technique which improves outcomes. J Neurointerv Surg 2017; 9: 1154–1159. [DOI] [PubMed] [Google Scholar]
- 7). Maus V, Behme D, Kabbasch C, et al. Maximizing first-pass complete reperfusion with SAVE. Clin Neuroradiol 2018; 28: 327–338. [DOI] [PubMed] [Google Scholar]
- 8). Goto S, Ohshima T, Ishikawa K, et al. A stent-retrieving into an aspiration catheter with proximal balloon (ASAP) technique: a technique of mechanical thrombectomy. World Neurosurg 2018; 109: e468–e475. [DOI] [PubMed] [Google Scholar]