

Abstract
Objectives:
Computer workstations are considered a potential workplace hazard. This study sought to evaluate computer workstation ergonomics in a university office environment, and to determine its relationship with musculoskeletal (MS) and visual symptoms reported by employees.
Material and Methods:
This was a cross-sectional observational study. A total of 231 university employees were recruited using a stratified random sampling technique. By means of direct observation, computer workstations were evaluated using the Occupational Safety and Health Administration (OSHA) Ergonomic Computer Workstation Evaluation Checklist. In addition, the participants reported MS and visual symptoms during the past week and 12 months by completing questionnaires.
Results:
Several ergonomic deficiencies in computer workstations were identified. Seating, working area, and keyboard and input devices had the most documented deficits. A significant proportion of employees reported various MS symptoms during the past 12 months. The most affected body parts were the shoulders (37%), the lower back (34%), and the neck (29%). The most prevalent visual symptom was tired eyes (68%). Logistic regression analysis indicated that MS symptoms, such as ache, pain and discomfort, were significantly associated with the total scores on the OSHA components. Deficits in monitor ergonomics and its placement, particularly the presence of glare reflected on the screen, were also associated with reported visual symptoms. Independent variables, such as gender, age, employment duration, job type, daily computer work hours, and work pattern, reliably predicted the participants’ reported experience of various MS and visual symptoms.
Conclusions:
Both MS and visual symptoms are associated with deficits in computer workstation ergonomics. Appropriate strategies, work practices, and preventive measures are needed to eliminate occupational hazards associated with computer workstations. Int J Occup Med Environ Health. 2022;35(2):141 – 56
Keywords: Jordan, ergonomics, workplace safety, musculoskeletal symptoms, computer workstations, visual symptoms
INTRODUCTION
The use of computer and visual display terminals (VDTs) is common in many workplaces, particularly in offices. These devices have become an essential part of daily office work due to their positive effects on accuracy, efficiency, and the achievement of desired organizational outcomes. However, the prolonged use of such devices, along with the inappropriate adherence to health and safety requirements of workstations, has been associated with various potential health problems.
Several studies have been conducted to examine ergonomic standards, deficiencies, and human factors in office work environments. Whereas most of these studies have focused on assessing the ergonomic needs of industrial office workers, few studies were designed to specifically report the major ergonomic issues which university employees encounter while working at computer workstations. University teachers were found to suffer from different types of musculoskeletal (MS) disorders, mainly lower back and neck pains. This could be attributed to an inappropriate ergonomic design of workstations [1].
In fact, MS problems in the neck, shoulders, elbows, wrists, and back regions are highly prevalent among computer users. For example, the prevalence rates of pain symptoms in different body parts range 20.3–56.1% [2]. This pain has been associated with various factors, such as input devices or computer mouse time use [3], employment duration, and increased work demand [2]. In addition, a significant correlation exists between work style factors, insufficient work breaks, pain symptoms, and a loss of productivity [4]. Finally, work behaviors are significant predictors of MS symptoms. Working with heightened muscle tension and mental fatigue were significantly associated with MS symptoms [5].
Ergonomic deficiencies in the university computer workstation design included monitor alignment [6], and furniture dimension and anthropometric measurement mismatch [1]. Other identified deficiencies in other settings included physical design, workstation layout, employment posture, work practices, and training programs. Moreover, the use of unadjustable chairs, bent and unsupported back postures, and office tables for computers were also documented [7].
According to the American Optometric Association, most adult workers (58%) experience digital eye strain or computer vision syndrome from overexposure to computers [8]. Office workers experience somatic visual symptoms, such as tired eyes, dry eyes, and eye discomfort, which are associated with computer-related work and increased work hours [9]. Visual symptoms could be due to problems with equipment, work stations, office environment, and job design or a combination of these factors [10].
An adequate assessment of occupational health problems seems to be helpful in identifying and reducing work-related risk factors, providing an opportunity for early intervention. Furthermore, when workplace demands are fitted appropriately to match the capabilities of workers and accommodate their health needs, a safer and healthier work environment is created to reduce work-related problems among workers [11]. To the best of the authors’ knowledge, no published study has assessed ergonomics among VDT users in Jordan, and this study is the first to evaluate computer workstation ergonomics, and MS and visual symptoms among workers in a university office environment. Specifically, this study answered the following research questions:
-
–
What are the computer workstation ergonomics deficiencies?
-
–
What are the variables that predict the participants’ reported MS and visual symptoms?
MATERIAL AND METHODS
Design
An observational descriptive cross-sectional study design was used. This design was used to investigate the association between independent variables (gender, age, job type, employment duration, computer workstation-related work pattern [continuous vs. intermittent], number of computer-related work hours per day [in and out of the office], hours spent in a typical week on performing vigorous physical activities) and scores on the Occupational Safety and Health Administration (OSHA) Ergonomic Computer Workstation Evaluation Checklist, as well as deficits in monitor design with its orientation and reported MS and visual symptoms.
Setting
The study was conducted in a large public university in Jordan, where employees work with VDTs as part of their job. Both academic and administrative staff were invited to participate in the study with the following inclusion criteria: age 20–59 years, employment duration of >6 months in the current job, and full-time work status. Additionally, an assessment was made of the participants’ medical history of MS conditions causing symptoms, without any existing diagnosis of eye diseases or conditions causing ocular symptoms or affecting the ability to focus clearly on close objects. Exclusion criteria included contact lens use and current pregnancy.
Study participants
Stratified cluster sampling was used in this study. The 2-step sampling process included:
random cluster selection of faculties and centers at the university,
random stratified selection from each cluster.
The final study sample included a total of 231 participants (89 academic staff and 142 administrative staff).
Instruments
Four instruments were used for this study:
-
–
a descriptive data questionnaire to collect data on demographics and other work-related data,
-
–
a questionnaire on visual symptoms arising from computer workstation/VDT use [12],
-
–
the Nordic Musculoskeletal Questionnaire (NMQ) [13],
-
–
the OSHA Ergonomic Computer Workstation Evaluation Checklist [14].
Nine visual symptoms, including watery eyes, dry eyes, itchy eyes, pain behind the eyes, aching eyes, sore eyes, tired eyes, blurred vision, and double vision, were assessed based on the degree of ocular discomfort experienced by the participants. The symptoms were assessed on a Likert scale ranging from 0 (no symptom) to 3 (se vere symptom). Cronbach’s α for the 9 visual symptoms was 0.85, which denotes high reliability [12].
To screen MS symptoms, the NMQ was used. The questionnaire has been used in various occupational groups to evaluate MS problems. This questionnaire, which was selfadministered, consists of structured, forced, and binary or multiple choices. The first basic part of the questionnaire assessed the anatomical region of the MS symptoms (neck, shoulders, elbow, wrist, hand, and upper and lower back), as well as an additional classification of symptoms based on the timing of the occurrence within the past 12 months and 7 days. The second part of the questionnaire included additional questions regarding the symptoms for each anatomical region, functional influence, and durability, as well as the MS symptoms during the past 7 days [13]. The validity and reliability of the screening tool were established. The validity was tested by a comparison with the participants’ clinical history; the findings revealed that the unmatched results ranged 0–20%. Acceptable psychometric properties for the NMQ in the screening and surveillance of MS problems were reported in previous studies [15].
The OSHA Ergonomic Computer Workstation Evaluation Checklist has been used to evaluate various VDT workstations. It has several ergonomic components, and each one contains multiple items concerning workstations, such as seating, keyboard and input devices, monitor, mobile devices, accessories, and general concepts. Each item on the checklist was answered on a binary basis (yes or no) [14].
Ethics
The study approval was obtained from the university administration and the ethics committee for scientific research (ID: I7-886). Additionally, written informed consent was obtained from each participant. The participants were informed about the voluntary nature of the study and about the fact that they could refuse to participate or withdraw at any time during the study without any consequences. The participants were assured of the confidentiality and anonymity of their data. All data were deidentified.
Pilot study
A pilot testing of the adapted NMQ was conducted. First, the questionnaire items were independently translated into the Arabic language by 2 certified translators, and a final version was generated based on consensus. Second, 2 other professionals performed a reverse-translation independent of each other. Then, the translated version of the questionnaire was reviewed by a panel of experts. This panel comprised 3 content experts, a specialist in the area of instrument development, and a research expert.
To verify the questionnaire’s psychometric properties after translation, copies were distributed to 44 randomly selected full-time university employees. They were asked to complete the NMQ for the second time after 1 week of the first administration. This sample of employees was not included in the main study. The estimated agreement between the identified MS symptoms for different body parts was assessed to ensure test-retest reliability. The calculated κ correlation coefficient was excellent, ranging 0.83–0.96. The calculated Cronbach’s α coefficient for internal consistency on all items of the questionnaire was 0.87.
Data collection procedure
Data collection proceeded after ethical approval was obtained. The researcher obtained an appointment via e-mail or phone call, and approached each selected participant personally in his/her workplace. The participants provided written informed consent, and completed the descriptive data questionnaire, the questionnaire on visual symptoms arising from computer workstation/VDT use, and NMQ. An appointment was made to observe each participant on a usual working day to complete the OSHA Ergonomic Computer Workstation Evaluation Checklist. One of the researchers was available for any clarification or question. Each participant completed the questionnaires in approx. 30–40 min.
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows v. 20.0. Descriptive statistics were analyzed to describe the participants’ demographics, which included gender, job type, employment duration, the educational level, the computer workstation-related work pattern (continuous vs. intermittent), and the number of computer-related work hours per day. Each item on the OSHA checklist had 2 possible outcomes (0 – no and 1 – yes). The total score for each ergonomics component of the checklist was scored by summing the points of items within each component that received a “yes” response. The study outcome (dependent variables) of the presence of MS or visual symptoms in the past 12 months of work was dummy-coded. Binary logistic regression was used to assess variables, and to reliably predict MS and visual symptoms among university employees. Statistical significance was determined by a p < 0.05.
RESULTS
Sample description
The total sample size was 231 participants with a 92% response rate. Most participants were female (65.8%, N = 152), administrative staff (61%, N =142), worked on the computer for 3–5 h/day (40.7%, N = 94). Over half (54.1%) of the participants had a continuous computer workstation-related work pattern. Only 26 (11.3%) of the participants used “over the office” lighting, whereas the rest used general room lighting (ceiling light) (88.7%). None of the participants used “over task” lighting. Descriptive statistics are presented in Table 1.
Table 1.
Characteristics of the university employees involved in the study on evaluating computer workstation ergonomics, Jordan, September 2019–January 2020
| Variable | Participants (N = 231) | |
|---|---|---|
| n | % | |
| Gender | ||
| female | 152 | 65.8 |
| male | 79 | 34.2 |
| Age | ||
| 20–29 years | 46 | 19.9 |
| 30–39 years | 93 | 40.3 |
| 40–49 years | 54 | 23.4 |
| 50–59 years | 38 | 16.5 |
| Job type | ||
| academic | 89 | 38.5 |
| administrative | 142 | 61.5 |
| Employment duration | ||
| 1–5 years | 59 | 25.5 |
| 6–10 years | 84 | 36.4 |
| 11–15 years | 52 | 22.5 |
| ≥16 years | 36 | 15.6 |
| Level of education | ||
| secondary | 3 | 1.3 |
| diploma | 57 | 24.7 |
| bachelor | 79 | 34.2 |
| master | 39 | 16.9 |
| doctor | 53 | 22.9 |
| Computer workstation-related work pattern | ||
| intermittent | 106 | 45.9 |
| continuous | 125 | 54.1 |
| Computer-related work in the office | ||
| <1 h/day | 25 | 10.8 |
| 1–2 h/day | 38 | 16.5 |
| 3–5 h/day | 94 | 40.7 |
| >5 h/day | 74 | 32.0 |
| out of the office | ||
| <1 h/day | 76 | 32.9 |
| 1–3 h/day | 95 | 41.1 |
| >3 h/day | 60 | 26.0 |
| Type of light(s) | ||
| general lightening in the room (ceiling) | 205 | 88.7 |
| over the office lightening | 26 | 11.3 |
| over task lightening | 0 | 0.00 |
| Office light intensity | ||
| very bright | 37 | 16.0 |
| moderate brightness | 185 | 80.1 |
| mild brightness | 9 | 3.9 |
| Screen glare | ||
| yes | 159 | 68.8 |
| no | 72 | 31.2 |
Computer workstation ergonomic deficiencies
Most ergonomic workstation deficiency hazards in this study were related to seating, working area, keyboard and input devices, and monitors. Table 2 illustrates the most commonly assessed ergonomic deficiencies. In general, administrative employees had more deficiencies in the working stations, seating, and working posture than academic staff whereas academic staff had more keyboard and input device-related deficiencies.
Table 2.
The highest assessed computer workstation ergonomic deficiencies using the OSHA Ergonomic Computer Workstation Evaluation Checklist [14] for the university employees involved in the study on evaluating computer workstation ergonomics, Jordan, September 2019–January 2020
| Ergonomic deficiency | Participants (N = 231) | |
|---|---|---|
| n | % | |
| Workstation | ||
| the thighs are not parallel to the floor and the lower legs are not perpendicular to the floor | 171 | 74.0 |
| the feet do not rest on the floor nor are they supported by a stable footrest | 170 | 73.9 |
| insufficient places (trapped thighs) | 121 | 52.3 |
| the legs and the feet do not have sufficient space | 119 | 51.5 |
| insufficient forward clearance for the legs and the feet | 119 | 51.5 |
| the head and the neck are not in an upright position | 40 | 17.3 |
| the trunk is not perpendicular to the floor | 40 | 17.3 |
| the shoulders and the upper arms are not relaxed (elevated or stretched) | 26 | 11.2 |
| the upper arm and the elbows are not close to the body (extended outward) | 25 | 10.8 |
| the wrists and the hands are not straight (bent up/down or sideways to the little fingers) | 24 | 10.4 |
| the forearms, wrists and hands are not straight in line | 21 | 9.0 |
| Seating | ||
| the seat has no cushioning and is not rounded | 168 | 72.7 |
| the seat width and depth are not accommodated to the worker’s size | 155 | 67.1 |
| the seat front presses against the back of the knee and the lower legs | 147 | 63.6 |
| the backrest does not support the lower back | 136 | 58.9 |
| Keyboard and input devices | ||
| the input devices are not easily activated (size and shape hand fits) | 180 | 77.9 |
| the wrists and the hands are rested on sharp or hard edges | 92 | 39.8 |
| Accessories | ||
| the telephone cannot be used with the head upright (not bent) and the shoulders relaxed (not elevated) if computer tasks done at the same time | 190 | 82.3 |
| the telephone is not positioned close to the work to avoid excessive reaches generally, within 45–50 cm | 182 | 78.8 |
| General ergonomics | ||
| insufficient adjustability of the workstation and equipment | 154 | 66.7 |
| inadequate maintenance for computer workstations | 49 | 21.2 |
| computer tasks are not organized in a way that allows workers to take a break | 45 | 19.5 |
| Monitor | ||
| light reflection from the screen to the user’s eyes | 153 | 66.2 |
| the top of the screen is not at the eye level | 149 | 64.5 |
| the monitor is not directly in front of the user, so the user needs to twist his/her head and trunk | 67 | 29.0 |
| the monitor distance does not allow the user to read without leaning his/her head, neck or trunk forward or backward | 55 | 23.8 |
MS symptoms
The participants reported MS symptoms for the past 12 months and 7 days. For the 12-month period, most MS symptoms were reported in the shoulders (32.0%). Figure 1 shows the proportion of reported MS symptoms at different anatomical regions.
Figure 1.
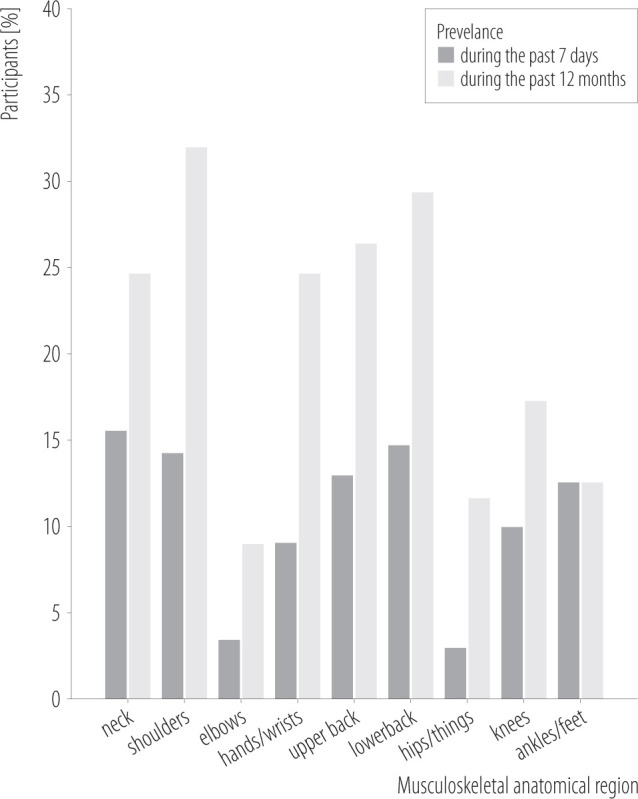
The musculoskeletal symptoms reported by 231 university employees involved in the study on evaluating computer workstation ergonomics, Jordan, September 2019–January 2020
Visual symptoms
One hundred and sixty-six (71.9%) participants reported that they had ≥1 visual symptom. The most severe visual symptoms reported by the participants were tired eyes (11%), dry eyes (8%), and itchy eyes (7%). Table 3 presents data on the frequencies of visual symptoms according to the severity level experienced by the participants.
Table 3.
The visual symptoms reported by 231 university employees involved in the study on evaluating computer workstation ergonomics, Jordan, September 2019–January 2020
| Visual symptom | Participants (N = 231) [n (%)] | |||
|---|---|---|---|---|
| no symptoms | mild symptoms | moderate symptoms | severe symptoms | |
| Teary eyes | 110 (47.6) | 84 (36.4) | 25 (13) | 8 (3.5) |
| Dry eyes | 114 (49.4) | 65 (28.1) | 33 (14.3) | 19 (8.2) |
| Itchy eyes | 93 (40.3) | 83 (35.9) | 40 (17.3) | 15 (6.5) |
| Pain behind the eyes | 138 (59.7) | 49 (21.2) | 34 (14.7) | 10 (4.3) |
| Pain in the eyes | 116 (50.2) | 60 (26.0) | 47 (20.3) | 8 (3.5) |
| Sore eyes | 173 (74.9) | 34 (14.7) | 18 (7.8) | 6 (2.6) |
| Tired eyes | 66 (28.2) | 75 (32.5) | 66 (28.6) | 24 (10.4) |
| Unclear vision | 117 (50.6) | 62 (26.8) | 40 (17.3) | 12 (5.2) |
| Double vision | 175 (75.8) | 30 (13.0) | 20 (8.7) | 6 (2.6) |
Relationship between computer workstation ergonomics and MS symptoms
Table 4 shows the results of logistic regression analysis investigating the associations between OHSA checklist ergonomics components and reported MS symptoms in different anatomical regions. Generally, a higher total score on the checklist components seems to have a “protective” effect, with regard to the experience of MS symptoms. As illustrated in Table 4, a significant association existed between workstations and accessories, and reported symptoms in the neck, shoulders, hands/wrists, and upper and lower back (p < 0.05). Likewise, the total score on the general ergonomic concept on the OSHA checklist was significantly related to reported symptoms in the previous anatomical regions, except for the lower back. The likelihood of experiencing wrist/hand symptoms was positively associated with a lower score on keyboard/input device items (p < 0.05).
Table 4.
The summary of logistic regression analysis for the total scores on the OSHA Ergonomic Computer Workstation Evaluation Checklist and reported musculoskeletal symptoms among university employees (N = 231), Jordan, September 2019–January 2020
| Variable | Logistic regression for musculoskeletal anatomical region | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| neck | shoulders | hands/wrists | upper back | lower back | ||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Workstations | 0.85** | 0.76–0.95 | 0.88* | 0.78–0.98 | 0.83** | 0.74–0.94 | 0.87* | 0.77–0.98 | 0.81*** | 0.73–0.91 |
| Seating | 0.96 | 0.82–1.14 | 0.85 | 0.71–1.01 | 0.97 | 0.75–1.09 | 0.82* | 0.70–0.97 | 0.80* | 0.69–0.95 |
| Keyboard/input device | 0.84 | 0.86–1.04 | 0.92 | 0.76–1.12 | 0.72** | 0.59–0.89 | 0.96 | 0.79–1.17 | 0.99 | 0.83–1.19 |
| Monitor | 0.79* | 0.65–0.95 | 0.83* | 0.68–0.98 | 0.97 | 0.80–1.18 | 0.86 | 0.71–1.04 | 0.97 | 0.82–1.16 |
| Accessories | 0.81* | 0.67–0.99 | 0.76** | 0.62–0.93 | 0.72** | 0.56 0.91 | 0.77* | 0.62–0.97 | 0.78* | 0.65–0.95 |
| General ergonomics | 0.78* | 0.62–0.96 | 0.70* | 0.55–0.90 | 0.70** | 0.54–0.92 | 0.77* | 0.59–0.96 | 0.89 | 0.71–1.13 |
p < 0.05;
p < 0.01;
p < 0.001.
Relationship between monitor ergonomics and visual symptoms
The experience of most commonly reported visual symptoms (tired eyes, itchy eyes, and teary eyes) had a statistically significant association with monitor ergonomic deficiencies. The findings indicate that the presence of a glare from windows or lights and inappropriate monitor screen distance are significant predictors of reported tired eyes, itchy eyes, and teary eyes (p < 0.05). Additionally, an insufficient adjustment of the screen was found to be associated with higher odds of experiencing itchy eyes (p < 0.05) (Table 5).
Table 5.
Logistic regression results for the most commonly reported visual symptoms and monitor ergonomics among university employees (N = 231), Jordan, September 2019–January 2020
| Monitor ergonomics/placement | Logistic regression for visual symptom | |||||
|---|---|---|---|---|---|---|
| tired eyes | itchy eyes | teary eyes | ||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Glare (from windows, lights) is not reflected on the screen | ||||||
| yes | 1 | 1 | 1 | |||
| no | 4.36*** | 2.27–8.45 | 2.71** | 1.46–5.03 | 2.10* | 1.17–3.67 |
| The top of the screen is at or below the eye level so the user can read it without bending his/her head or neck down/back | ||||||
| yes | 1 | 1 | 1 | |||
| no | 1.84 | 0.79–4.3 | 2.87* | 1.29–6.39 | 1.51 | 0.77–2.95 |
| Monitor position is directly in front of the user, so the user does not have to twist his/her head or neck | ||||||
| yes | 1 | 1 | 1 | |||
| no | 1.45 | 0.53–3.91 | 1.32 | 0.56–3.14 | 1.30 | 0.60–2.85 |
| Monitor distance (generally arm length) allows the user to read without leaning his/her head, neck or trunk forward or backward | ||||||
| yes | 1 | 1 | 1 | |||
| no | 3.88** | 1.4–10.5 | 5.12*** | 2.28–8.68 | 2.37* | 1.05–5.37 |
p < 0.05;
p < 0.01;
p < 0.001.
Relationship between individual variables and symptoms
Musculoskeletal symptoms
The predictor variables for the development of MS symptoms among university employees in this study were gender, job type, age, employment duration, daily computer-related work hours (in/out of the office), work pattern, and hours spent during a week on performing vigorous physical activities. The analyses of the variables that reliably predict those participants having any MS symptoms do not indicate that the predictors model provides more statistically significant improvement than the constant-only model (χ2 = 80.48, df = 8, N = 231, p < 0.001).
According to Table 6, gender is a statistically significant predictor of MS symptoms reported in the neck, shoulders, hands/wrists, and upper and lower back. For instance, male employees seemed to be approx. 2.5 times less likely to develop MS symptoms in the neck (OR = 0.42) and the lower back (OR = 0.40) than their female counterparts. Employment duration of 11–15 years was associated with higher odds of experiencing neck symptoms. An employee who had been working for 11–15 years seemed to be 2 times more likely to experience neck pain. Moreover, employment duration of ≥16 years was associated with higher odds of experiencing neck, shoulder, hands/wrists, and upper and lower back symptoms. Employees with ≥16 years of work experience were approx. 3 times more likely than employees with shorter employment duration to experience MS symptoms.
Table 6.
The summary of logistic regression analysis for variables predicting the experience of musculoskeletal and visual symptoms, among university employees (N = 231), Jordan, September 2019–January 2020
| Variable | Logistic regression | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| musculoskeletal anatomical region | visual symptom | |||||||||||||||
| neck | shoulders | hands/wrists | upper back | lower back | tired eyes | itchy eyes | teary eyes | |||||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Gender | ||||||||||||||||
| female | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| male | 0.42*** | 0.08–0.38 | 0.37** | 0.18–0.77 | 0.35 * | 0.15–0.79 | 0.32** | 0.15–0.68 | 0.40* | 0.23–0.73 | 0.63 | 0.34–1.17 | 0.45* | 0.23–0.86 | 0.76 | 0.41–1.40 |
| Job type | ||||||||||||||||
| academic | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| administrative | 2.29* | 1.13–4.63 | 1.45 | 0.76–2.78 | 1.29 | 0.63–2.63 | 1.5 | 0.74–3.10 | 2.7* | 1.27–5.86 | 1.21 | 0.66–2.25 | 1.26 | 0.64–2.48 | 1.58 | 0.85–2.99 |
| Age | ||||||||||||||||
| 20–29 years | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| 30–39 years | 1.63 | 0.70–3.81 | 1.23 | 0.54–2.77 | 1.9 | 0.77–4.81 | 1.16 | 0.45–3.02 | 1.12 | 0.54–2.50 | 1.10 | 0.3–3.97 | 1.17 | 0.40–3.43 | 1.35 | 0.71–2.87 |
| 40–49 years | 1.95 | 0.77–4.96 | 1.79 | 0.74–4.34 | 2.78 | 0.94–6.80 | 1.39 | 0.60–3.25 | 1.86 | 0.80–3.56 | 2.38 | 0.77–5.38 | 1.45 | 0.52–3.78 | 1.7 | 0.88–3.27 |
| 50–59 years | 5.68** | 1.75–8.52 | 4.88* | 1.63–8.67 | 5.82* | 1.75–9.35 | 3.58* | 1.11–7.50 | 4.34* | 2.01–9.09 | 3.65* | 1.41–7.68 | 2.78** | 1.8–7.73 | 2.67* | 1.20–6.70 |
| Employment duration | ||||||||||||||||
| 1–5 years | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| 6–10 years | 1.37 | 0.56–3.34 | 0.99 | 0.48–2.46 | 0.67 | 0.51–1.61 | 0.44 | 0.20–1.17 | 0.92 | 0.40–2.21 | 0.61 | 0.39–1.32 | 0.86 | 0.41–1.82 | 0.80 | 0.33–1.85 |
| 11–15 years | 2.09* | 1.06–4.10 | 1.21 | 0.55–2.65 | 1.83 | 0.77–4.34 | 1.36 | 0.66–2.85 | 0.82 | 0.37–1.79 | 1.22 | 0.69–2.37 | 1.63 | 0.84–3.17 | 1.31 | 0.67–2.55 |
| ≥16 years | 3.2* | 1.29–7.14 | 2.89* | 1.18–5.35 | 2.86* | 1.14–5.04 | *2.46 | 1.03–5.86 | 2.68* | 1.12–4.86 | 2.77* | 1.16–6.64 | 2.96* | 1.12–5.83 | 1.66 | 0.71–3.86 |
| Computer workstation-related work pattern | ||||||||||||||||
| intermittent | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| continuous | 2.32* | 1.16–4.61 | 2.34* | 1.13–4.84 | 2.31* | 1.17–4.99 | 1.27 | 0.59–2.74 | 1.10 | 0.5–2.24 | 1.93* | 1.08–3.47 | 1.37 | 0.72–2.60 | 2.3* | 1.11–4.76 |
| Computer-related work | ||||||||||||||||
| in the office | ||||||||||||||||
| <1 h/day | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| 1–2 h/day | 1.28 | 0.3–5.06 | 1.10 | 0.24–4.78 | 1.10 | 0.4–3.97 | 1.15 | 0.44–2.99 | 1.21 | 0.67–2.71 | 1.17 | 0.40–3.34 | 2.20 | 0.84–7.09 | 1.11 | 0.55–2.33 |
| 3–5 h/day | 1.88 | 0.51–6.90 | 1.18 | 0.27–5.16 | 2.38 | 0.77–7.38 | 1.29 | 0.26–4.50 | 2.79* | 1.12–5.03 | 1.45 | 0.52–3.78 | 2.44 | 0.89–5.35 | 1.58 | 0.70–3.55 |
| >5 h/day | 4.39* | 1.24–7.74 | 1.60 | 0.38–6.61 | 3.65* | 1.14–9.68 | 3.08 | 0.67–6.19 | 5.6** | 1.76–9.16 | 2.78* | 1.8–5.37 | 3.59** | 1.51–8.55 | 3.53* | 1.27–6.88 |
| out of the office | ||||||||||||||||
| <1 h/day | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| 1–3 h/day | 0.80 | 0.43–1.84 | 1.39 | 0.63–3.05 | 2.42* | 1.21–6.29 | 1.43 | 0.69–2.98 | 2.49* | 1.16–4.43 | 2.03* | 1.17–4.66 | 1.59 | 0.81–3.14 | 1.42 | 0.66–3.05 |
| >3 h/day | 2.20* | 1.18–4.64 | 2.37* | 1.13–4.46 | 2.76* | 1.15–5.40 | 1.48 | 0.72–3.03 | 2.63* | 1.22–5.35 | 2.34* | 1.05–3.92 | 2.30* | 1.20–4.44 | 1.49 | 0.68–3.25 |
| Hours spent in a typical week on performing vigorous physical activities | ||||||||||||||||
| none | 1 | 1 | 1 | 1 | 1 | |||||||||||
| 1–3 h/week | 0.67 | 0.4–1.61 | 1.53 | 0.76–3.06 | 0.51 | 0.20–1.36 | 1.39 | 0.7–2.77 | 1.28 | 0.62–2.63 | ||||||
| 4–6 h/week | 1.83 | 0.77–4.34 | 2.60* | 1.10–5.43 | 1.28 | 0.62–2.63 | 1.37 | 0.60–3.13 | 2.03* | 1.17–3.92 | ||||||
| >6 h/week | 2.86* | 1.14–5.04 | 3.28** | 1.41–6.70 | 1.53 | 0.70–3.33 | 2.35* | 1.05–5.27 | 2.34* | 1.17–4.66 | ||||||
p < 0.05;
p < 0.01;
p < 0.001.
The increased odds ratio indicates that when all the other predictors remain constant, those university employees who had been working continuously were approx. 2 times more likely to develop MS symptoms in the neck, shoulders, hands and wrists than those who had been working intermittently. The odds ratio for the job type suggests that an administrative employee is 2 times more likely to experience neck symptoms, and 3 times more likely to experience lower back symptoms, than an academic employee. Likewise, university employees aged 50–59 years have an increased risk of MS symptoms in the neck, shoulders, hands/wrists, and upper and lower back. Moreover, the odds of experiencing MS symptoms, as compared to no symptoms, were increased among those employees who had been working on computer workstations at the office for >5 h/day. For instance, they were 4 times more likely to experience neck and hand/wrist symptoms, and 5 times more likely to experience lower back symptoms. Likewise, the employees who had been working on computer workstations outside the office for 1–3 h were more likely to develop hand/wrist and lower back symptoms. Moreover, the time spent working on a computer outside the office, reaching >3 h/day, was significantly associated with an increased risk of having all MS symptoms, except for upper back pain.
The likelihood of experiencing neck, shoulder, and upper and lower back pain was positively associated with increased hours of performing vigorous physical activity. The participants who performed vigorous physical activities for >6 h/week were approx. 3 times more likely to experience shoulder and neck pain than the participants who did not perform such vigorous physical activities (Table 6).
Visual symptoms
The results of logistic regression analysis indicate that the 7 predictors model (gender, job type, age, employment duration, work pattern, daily computer-related work hours [in/out of the office]) provides more statistically significant improvement than the constant-only model (χ2 = 116.29, df = 8, N = 231, p < 0.001). Table 6 suggests that female employees had 2 times higher odds of experiencing itchy eye symptoms. Likewise, an employee performing computer-related work for >5 h/day in the office was 3.5 times more likely to experience itchy and teary eyes, with the odds being as high as they were for an employee working for <1 h/day in front of a computer. Likewise, the employees who had been working outside the office in front of a computer for 1–3 h/day were 2 times more likely to experience tired eyes than those who had been working for <1 h/day in front of a computer. Those employees who had been working for >3 h in front of a computer outside the office were 2 times more likely to experience itchy eyes than those who had been doing so for <1 h/day. Employment duration of ≥16 years was associated with higher odds of experiencing visual symptoms. Those employed for ≥16 years were approx. 3 times more likely to experience tired and itchy eyes than those who had employment duration of 1–5 years. However, a given job type had no statistically significant association with reported visual symptoms. Similarly, working for <5 h/day had no statistically significant association with reported visual symptoms.
DISCUSSION
This study employed observational and self-administered questionnaire methods to describe ergonomic deficiencies in the computer workstation, and to evaluate the prevalence of visual and MS symptoms experienced by university employees. Additionally, it investigated the association between the reported MS and visual symptoms, and predictor variables.
Occupational health problems are continuously increasing as a result of the daily use of VDTs. An early identification of occupational health problems would be helpful to identify and reduce work-related risk factors and to provide early interventions when needed. Human wellbeing should be the main focus in working areas, and all other factors should be designed to help workers work effectively and safely [16].
Major deficiencies identified in this study were related to seating, working area, keyboard and input devices, general computer tasks, monitor, and working posture. Seating deficiency was more prevalent among academic employees than among administrative employees. The presence of such deficiencies indicates that regular office stations are inadequately designed to meet employees’ physical and task needs. Serious ergonomic deficiencies in the computer design, layout, and usage were also previously reported [7]. The most documented deficiencies in computer workstations for administrative staff were related to the working area, which is not optimized for computer-related tasks. Likewise, thighs, legs, and feet had insufficient space, and employees needed much effort to access keyboards and input devices to accomplish required tasks. These findings could be attributed to the use of regular office tables for computer-related work, despite recommendations that necessitate the use of ergonomically-designed tables for computer workstations [17].
The results show that the reported percentages of MS symptoms experienced in the past 12 months were higher than those of the same symptoms in the past 7 days. Regarding the anatomical regions of MS symptoms, most symptoms were reported in the shoulders. This high prevalence of MS symptoms in the shoulders could be partly explained by the lack of ergonomically designed seating and an absence of document holders, which increase neck and back bending, and thus also muscle load. Similar results were previously reported in which the prevalence of neck, shoulders, and upper and lower back symptoms were higher among VDT employees [18].
The prevalence of upper and lower MS problems was higher among administrative employees, and was associated with their computer workstation-related work pattern and poor ergonomically designed chairs and tables. A continuous work pattern is described as longer periods of computer-related work. Whereas academic employees were less likely to experience lower back pain, administrative employees were 2.5 times more likely to have lower back pain. A possible explanation could be attributed to the nature of work and other work-related aspects that allow academic employees to take more postural breaks from computer-related work. Academic employees had some liberty to determine when various tasks had to be performed. In addition, administrative employees had higher percentages of ergonomic deficiencies in seating, in which case more than two-thirds of backrests could not support the lower back.
The results indicate that gender, age, job type, work pattern, employment duration, daily computer-related work hours (in/out of the office), and hours spent during a week on performing vigorous physical activity reliably predict the participants’ experience of MS symptoms. Generally, women complain more of work-related MS problems than men, with an increase specifically in injuries related to the upper extremities and the neck [19]. Gender differences in control strategies used during task performance may explain the increased vulnerability to developing MS disorders, when performing repetitive work involving the upper extremities for sustained periods in occupational life [20].
Other variables acting as significant predictors of reported MS symptoms were job type, age, work pattern, and OSHA scores. These results suggest that administrative staff are 2 times more likely to have MS symptoms than academic staff, while controlling for other independent variables. Moreover, the employees who had a continuous computer workstation-related work pattern were 3.5 times more likely to report MS symptoms than the employees who worked intermittently. The continuity of work has been significantly associated with upper extremity MS symptoms [18]. With regard to age as a predictor of MS symptoms, results suggest that with increasing age, the likelihood of experiencing MS symptoms increases. Similarly, the youngest participants less frequently reported MS symptoms, especially pain in the shoulder, than their elderly counterparts [2]. Higher scores on different components of the OSHA Ergonomic Computer Workstation Evaluation Checklist seem to have a “protective” effect, and were strongly associated with various reported MS symptoms.
The association between daily work hours and reported MS symptoms was found to be statistically significant. These findings were similar to other study findings, in which a significant association was reported between the prevalence of MS symptoms in the wrists/hands and increased computer-related work hours [21].
A significant proportion of the participants involved in this study experienced visual symptoms, with tired eyes being the most frequently reported by the participants. Similar complaints were documented by computer users [22]. Double vision was reported as the least common visual symptom among the participants, which is consistent with the least frequent visual symptom reported in other studies among VTD users [12]. Experiencing eye and vision problems has been linked to reduced productivity at work [23], and negatively affects the quality of life of a computer user [24].
Independent variables, such as age, employment duration, work pattern, computer-related work hours (both in/out of the office), and monitor ergonomics with its orientation, and especially the presence of deficits in monitor distance or glare reflection on the screen, reliably predict the reported visual symptoms. In this study, aging was a significant predictor of tired, itchy, and teary eyes. However, in some studies, age was not associated with computer vision syndrome [25].
Working on a computer for ≥5 h in a continuous manner seems to increase the odds of having visual symptoms. This finding is consistent with that of previous studies in which mean daily computer usage and increased continuous screen time were found to be significantly correlated with the prevalence of computer vision syndrome [26]. The presence of bright lighting and glare in the working environment leads to eye strain and difficulty in seeing objects on computer screens [9]. This could explain the significant association, as was found in this study, between poor monitor design and the presence of glare on the screen, on the one hand, and the reported visual symptoms, on the other. Similarly, a previous study found that visual symptoms were attributed to average computer-related work hours per day, and visual problems were higher with increased light glaring in computer workstation areas [27]. However, job type was not associated with reported visual symptoms in this study.
Generally speaking, MS and visual health problems related to workstations are complex and multifactorial. The findings presented in this study can inform further studies with comparable outcomes in occupational health, addressing the issue of ergonomics in computer workstations. Future studies are needed to examine the causal relationship between MS and visual symptoms, and to assess different interventions for reducing the burden of these symptoms with concomitant evaluation of desired outcomes.
Limitations
This study had some limitations. First, data were collected from a single institution; therefore, this could limit the generalizability of the findings drawn from this study to all university institutions. Multiple-site investigations are needed in the future to improve the external validity and to increase the generalizability of research findings. Second, the use of self-administered questionnaires to report MS and visual symptoms was prone to certain biases, such as the recall bias and the responder bias, which could lead to over- or underestimation of the obtained responses.
Implications
Computer workstations should be designed on the basis of ergonomic standards and recommendations (e.g., OSHA computer workstation ergonomic standards). Ergonomic interventions should be implemented in the following 3 categories of activities: corrective ergonomics (correcting the past ergonomic issues), preventive ergonomics (working on present issues, e.g., design), and prospective ergonomics (anticipating future ergonomic needs) [28]. The development and implementation of work practices are needed to eliminate occupational hazards. Computer workstation users should be provided with information regarding good working practices to increase their awareness of ergonomic issues in computer workstations (e.g., healthy posture). Additionally, they need to be provided with sufficient training and motivation in the ergonomic layout of computer workstations (e.g., how to prevent window-screen light reflections).
A careful MS and eye examination should be conducted regularly for all employees working on computer workstations to ensure an early referral for treatment and to reduce the severity of symptoms. Preventive measures should be implemented in university workplaces. These include offering breaks from work to avoid sitting or staring at monitors for long hours. Reminders adopted to prevent long work durations without breaks could be helpful. Additionally, preventive measures need to be adequately applied to lessen the visual symptoms, particularly tired eyes, dry eyes, and itchy eyes. Performing eye muscle exercises and a frequent use of wetting eye drops are recommended [29].
CONCLUSIONS
This study revealed that computer workstations have serious deficiencies in their design, layout, and usage. Unfortunately, the parameters of computer workstation ergonomics were unsatisfactory, especially those related to seating, chairs, working area, glare problems resulting from the reflection of light from computer screens, and a lack of document holders. The results revealed that a significant proportion of university employees, who work on computer workstations, experienced MS and visual symptoms.
In this study, several independent variables were significantly associated with reported MS and visual symptoms. Female gender, age, employment duration, computer-related work hours (in/out of the office), job type, work pattern, hours spent during a week on performing vigorous physical activity, and ergonomic deficiencies reliably predict the participant’s experience of MS symptoms. Additionally, age, employment duration, work patterns, computer-related work hours, and the presence of deficits in monitor design or glare reflection on the screen were significantly associated with reported visual symptoms.
ACKNOWLEDGMENTS
The authors would like to acknowledge the university employees who participated in this study.
REFERENCES
- 1.Kibria M, Rafiquzzaman M.. Ergonomic computer workstation design for university teachers in bangladesh. Jordan J Mech Ind Eng. 2019;13(2):91–103. [Google Scholar]
- 2.Kaliniene G, Ustinaviciene R, Skemiene L, Vaiciulis V, Vasilavicius P.. Associations between musculoskeletal pain and work-related factors among public service sector computer workers in Kaunas County, Lithuania. BMC Musculoskelet Disord. 2016;17(1):420, 10.1186/s12891-016-1281-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mikkelsen S, Funch Lassen C, Vilstrup I, Kryger A, Brandt L, Thomsen J, et al. Does computer use affect the incidence of distal arm pain? A one-year prospective study using objective measures of computer use. Int Arch Occup Environ Health. 2011;85:139–52, 10.1007/s00420-011-0648-1. [DOI] [PubMed] [Google Scholar]
- 4.Sharan D, Parijat P, Sasidharan AP, Ranganathan R, Mohandoss M, Jose J.. Workstyle risk factors for work related musculoskeletal symptoms among computer professionals in India. J Occup Rehabil. 2011;21(4):520–5, 10.1007/s10926-011-9294-4. [DOI] [PubMed] [Google Scholar]
- 5.Griffiths KL, Mackey MG, Adamson BJ.. Behavioral and psychophysiological responses to job demands and association with musculoskeletal symptoms in computer work. J Occup Rehabil. 2011;21(4):482–92, 10.1007/s10926-010-9263-3. [DOI] [PubMed] [Google Scholar]
- 6.Chowdhury N, Aghazadeh F, Amini M.. Ergonomic assessment of working postures for the design of university computer workstations. Occup Ergon. 2017;13(S1):37–46, 10.3233/OER-170252. [DOI] [Google Scholar]
- 7.Shikdar AA, Al-Kindi MA.. Office ergonomics: Deficiencies in computer workstation design. Int J Occup Saf Ergon. 2007;13(2):215–23, 10.1080/10803548.2007.11076722. [DOI] [PubMed] [Google Scholar]
- 8.American Optometric Association [Internet]. St. Louis: The Association; 2016. [cited 2019 Jul 17]. Most Americans experience digital eye strain from overexposure to computers according to survey. Available from: https://www.aoa.org/newsroom/most-americans-experience-digital-eye-strain-from-overexposure-to-computers-according-to-survey. [Google Scholar]
- 9.Sheppard AL, Wolffsohn JS.. Digital eye strain: Prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3(1):e000146, 10.1136/bmjophth-2018-000146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Richter HO, Zetterlund C, Lundqvist LO.. Eye-neck interactions triggered by visually deficient computer work. Work. 2011;39(1):67–78, 10.3233/wor-2011-1152. [DOI] [PubMed] [Google Scholar]
- 11.Crawford JO, Berkovic D, Erwin J, Copsey SM, Davis A, Giagloglou E, et al. Musculoskeletal health in the workplace. Best Pract Res Clin Rheumatol. 2020;34(5):101558, 10.1016/j.berh.2020.101558. [DOI] [PubMed] [Google Scholar]
- 12.Shrestha G, Mohamed F, Shah D.. Visual problems among video display terminal (VDT) users in Nepal J Optom. 2011;4: 56–62, 10.1016/S1888-4296(11)70042-5. [DOI] [Google Scholar]
- 13.Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–7, 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 14.United States Department of Labor Occupational Safety and Health Administration (OSHA) [Internet]. Washington, DC: The Department; 2019. [cited 2019 Jul 16]. Computer workstations eTool. Available from: https://www.osha.gov/SLTC/etools/computerworkstations/index.html. [Google Scholar]
- 15.Kahraman T, Genç A, Göz E.. The Nordic Musculoskeletal Questionnaire: cross-cultural adaptation into Turkish assessing its psychometric properties. Disabil Rehabil. 2016; 38(21): 2153–60, 10.3109/09638288.2015.1114034. [DOI] [PubMed] [Google Scholar]
- 16.Schulte P, Vainio H.. Well-being at work – overview and perspective. Scand J Work Environ Health. 2010;36(5):422–9, 10.5271/sjweh.3076. [DOI] [PubMed] [Google Scholar]
- 17.Woo EH, White P, Lai CW.. Ergonomics standards and guidelines for computer workstation design and the impact on users’ health – a review. Ergonomics. 2016;59(3): 464–75, 10.1080/00140139.2015.1076528. [DOI] [PubMed] [Google Scholar]
- 18.Ardahan M, Simsek H.. Analyzing musculoskeletal system discomforts and risk factors in computer-using office workers. Pak J Med Sci. 2016;32(6):1425–9, 10.12669/pjms.326.11436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Nordander C, Hansson G-Å, Ohlsson K, Arvidsson I, Balogh I, Strömberg U, et al. Exposure–response relationships for work-related neck and shoulder musculoskeletal disorders – Analyses of pooled uniform data sets. Appl Ergon. 2016;55:70–84, 10.1016/j.apergo.2016.01.010. [DOI] [PubMed] [Google Scholar]
- 20.Srinivasan D, Sinden KE, Mathiassen SE, Côté JN.. Gender differences in fatigability and muscle activity responses to a short-cycle repetitive task. Eur J Appl Physiol. 2016;116(11):2357–65, 10.1007/s00421-016-3487-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Griffiths KL, Mackey MG, Adamson BJ, Pepper KL.. Prevalence and risk factors for musculoskeletal symptoms with computer based work across occupations. Work. 2012;42(4):533–41, 10.3233/wor-2012-1396. [DOI] [PubMed] [Google Scholar]
- 22.Portello JK, Rosenfield M, Bababekova Y, Estrada JM, Leon A.. Computer-related visual symptoms in office workers. Ophthalmic Physiol Opt. 2012;32(5):375–82, 10.1111/j.1475-1313.2012.00925.x. [DOI] [PubMed] [Google Scholar]
- 23.Yamada M, Mizuno Y, Shigeyasu C.. Impact of dry eye on work productivity. Clinicoecon Outcomes Res. 2012;4: 307–12, 10.2147/CEOR.S36352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Uchino M, Schaumberg DA.. Dry eye disease: Impact on quality of life and vision. Curr Ophthalmol Rep. 2013;1(2):51–7, 10.1007/s40135-013-0009-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.de Paiva CS. Effects of aging in dry Eye. Int Ophthalmol Clin. 2017;57(2):47–64, 10.1097/IIO.0000000000000170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ranasinghe P, Wathurapatha WS, Perera YS, Lamabadusuriya DA, Kulatunga S, Jayawardana N, et al. Computer vision syndrome among computer office workers in a developing country: an evaluation of prevalence and risk factors. BMC Res Notes. 2016;9:150, 10.1186/s13104-016-1962-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sánchez-Brau M, Domenech-Amigot B, Brocal-Fernández F, Quesada-Rico JA, Seguí-Crespo M.. Prevalence of computer vision syndrome and its relationship with ergonomic and individual factors in presbyopic VDT workers using progressive addition lenses. Int J Environ Res Public Health. 2020;17(3), 10.3390/ijerph17031003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Brangier É, Robert J-M.. Prospective ergonomics: The foundations and issues. Trav Hum. 2014;77(1):1–20, 10.3917/th.771.0001. [DOI] [Google Scholar]
- 29.Lertwisuttipaiboon S, Pumpaibool T, Neeser KJ, Kasetsuwan N.. Effectiveness of a participatory eye care program in reducing eye strain among staff computer users in Thailand. Risk Manag Healthc Policy. 2017;10:71–80, 10.2147/RMHP.S134940. [DOI] [PMC free article] [PubMed] [Google Scholar]