

BACKGROUND
Relationships between systemic social injustices, adverse social conditions, and poor health outcomes are not new.1–6 However, a push to value-based care7–9 along with societal inequities that the COVID-19 pandemic has both highlighted and exacerbated10–13 have prompted the U.S. healthcare sector to refocus attention on patients’ social contexts. Recent years have seen a proliferation in the number of U.S. healthcare organizations endeavoring to improve patients’ health by screening for individual-level social needs (e.g., housing instability, food insecurity, a lack of reliable transportation) and referring those who indicate wanting help to relevant resources, like community-based organizations (CBOs).14–17
A key consideration regarding social needs screening and referral interventions is how to successfully embed these new practices within already cramped clinical workflows.18,19 Several qualitative studies, for example, have found that healthcare professionals express concern about having enough time to conscientiously both identify and respond to patients’ social needs within the scope of a clinical visit.20–23 Remote screening (e.g., via phone calls or text messages) outside of clinical visits might offer a promising alternative to in-person screening, both for time and accessibility reasons. For instance, telehealth could facilitate with the identification of social needs among those facing chronic barriers to in-person healthcare, including a lack of reliable transportation, mobility issues, or competing priorities such as work or childcare.24,25 Also, by potentially mitigating some of the power dynamics that accompany clinical spaces,25,26 some patients may find remote interventions to be more comfortable. However, remote screening and referral for social needs could be both alienating and restricting for patients who prefer in-person healthcare interactions,27,28 those with less technological literacy or access,29,30 or those with limited English proficiency.31 Regardless, many healthcare organizations necessarily shifted from in-person to remote interventions for social needs during the COVID-19 pandemic32–34 and now must consider the merits of continuing with that approach versus returning to in-person strategies when it comes to working collaboratively with patients to address the social needs that they disclose.
Therefore, having a better understanding for the impacts of in-person versus remote social needs screening and referral on addressing patients’ social needs is critical. An important first step to potentially resolve patients’ social needs is whether those who screen positive for social needs are willing to accept healthcare-based assistance to connect with corresponding resources.35 Multiple studies have reported discrepancies between the proportions of patients who screen positive for social needs versus those who are interested in help.35 Of course, there is nothing wrong with patients declining assistance with social needs, in and of itself. A patient may not view a social need as an immediate concern, may already be receiving help elsewhere, or may simply not want help with social needs from their healthcare provider.36 However, inequities could be exacerbated if there are systematic differences between those who are willing to accept versus decline support by screening mode.
This study made use of data from a social needs screening and referral intervention across diverse outpatient healthcare settings that spanned the start of the COVID-19 pandemic. We assessed whether in-person versus remote screening modified associations between patients’ total number of self-reported social needs and their willingness to accept help with social needs.
METHODS
This cross-sectional study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines37 and used data from the Accountable Health Communities (AHC) Model. The institutional review board of Oregon Health & Science University (OHSU) approved the study and all participants provided verbal informed consent (STUDY00018168).
The Accountable Health Communities (AHC) Model
The AHC Model was developed by the Centers for Medicare & Medicaid Services Innovation Center to test whether systematically identifying and addressing Medicare and Medicaid beneficiaries’ social needs impacts healthcare costs and utilization.17 Community-dwelling beneficiaries who consent to participate are screened for 5 social needs—housing stability and quality, utility needs, food insecurity, transportation needs beyond medical transportation, and interpersonal safety—using the AHC Health-Related Social Needs Screening Tool.38,39 Those who screen positive for ≥1 social need(s) and ≥2 self-reported emergency department visits within the previous 12 months are offered navigation services to facilitate community resource connections. Nationally, thirty-two “bridge organizations” across 25 states were originally selected to implement the AHC Model.40
The AHC Model in Oregon
Oregon’s bridge organization for the AHC Model was the Oregon Rural-Practice-based Research Network (ORPRN)41 at OHSU. Responsibilities of ORPRN included identifying and collaborating with clinical delivery sites to adopt the AHC Model and aligning partners to optimize the capacity of local communities to address beneficiaries’ social needs. Clinical delivery sites spanned 24 of Oregon’s 36 counties and represented a wide range of organizations and settings, including federally qualified health centers, private practices, emergency departments, and health departments.
The onset of the COVID-19 pandemic in the spring of 2020 had an immediate impact on healthcare delivery in Oregon.42 It also affected AHC Model implementation in three primary ways. First, several clinical delivery sites that had been screening participants in person were no longer able to participate due to reduced staff and competing priorities. Second, some sites switched from in-person to remote screening. Finally, health systems that were not participating pre-pandemic asked to join the study via remote screening, only. In response to these COVID-related contextual changes, ORPRN centralized efforts for the remote screening by hiring and training health sciences students to contact beneficiaries by phone or text message, describe the AHC Model, and screen consenting beneficiaries for social needs. For eligible beneficiaries, students offered referrals to a resource navigator (e.g., community health worker, social worker) for additional follow up, as part of the navigation requirement for the AHC Model. Across all of the participating healthcare settings, the frequency and consistency of screening varied based upon their capacity and internal workflows.
Study Participants
Study participants were community-dwelling Medicare and Medicaid beneficiaries who participated in the AHC Model in Oregon between October 17, 2018 and December 31, 2020. The study focused on those who consented to participate and who were eligible for resource navigation assistance due to both disclosing ≥1 social need(s) and self-reporting ≥2 emergency department visits within the previous year. We excluded those without complete data for either the outcome measure or covariates from the final study sample and analyses. Participants were also excluded from analyses if they came from clinical delivery sites in which there were <10 participants or in which 100% of participants were either willing or unwilling to accept navigation assistance (see Appendix 1 for demographics of included versus excluded beneficiaries). By December 31, 2020, 14,691 Medicare and Medicaid beneficiaries had participated in the AHC Model in Oregon and 2,929 (20%) had qualified for resource navigation assistance. Analyses included 1,504 participants with complete data for all variables of interest, of which 653 (43%) were screened for social needs in person and 851 (57%) were screened remotely (Figure). Participants originated from 28 clinical delivery sites.
Figure.
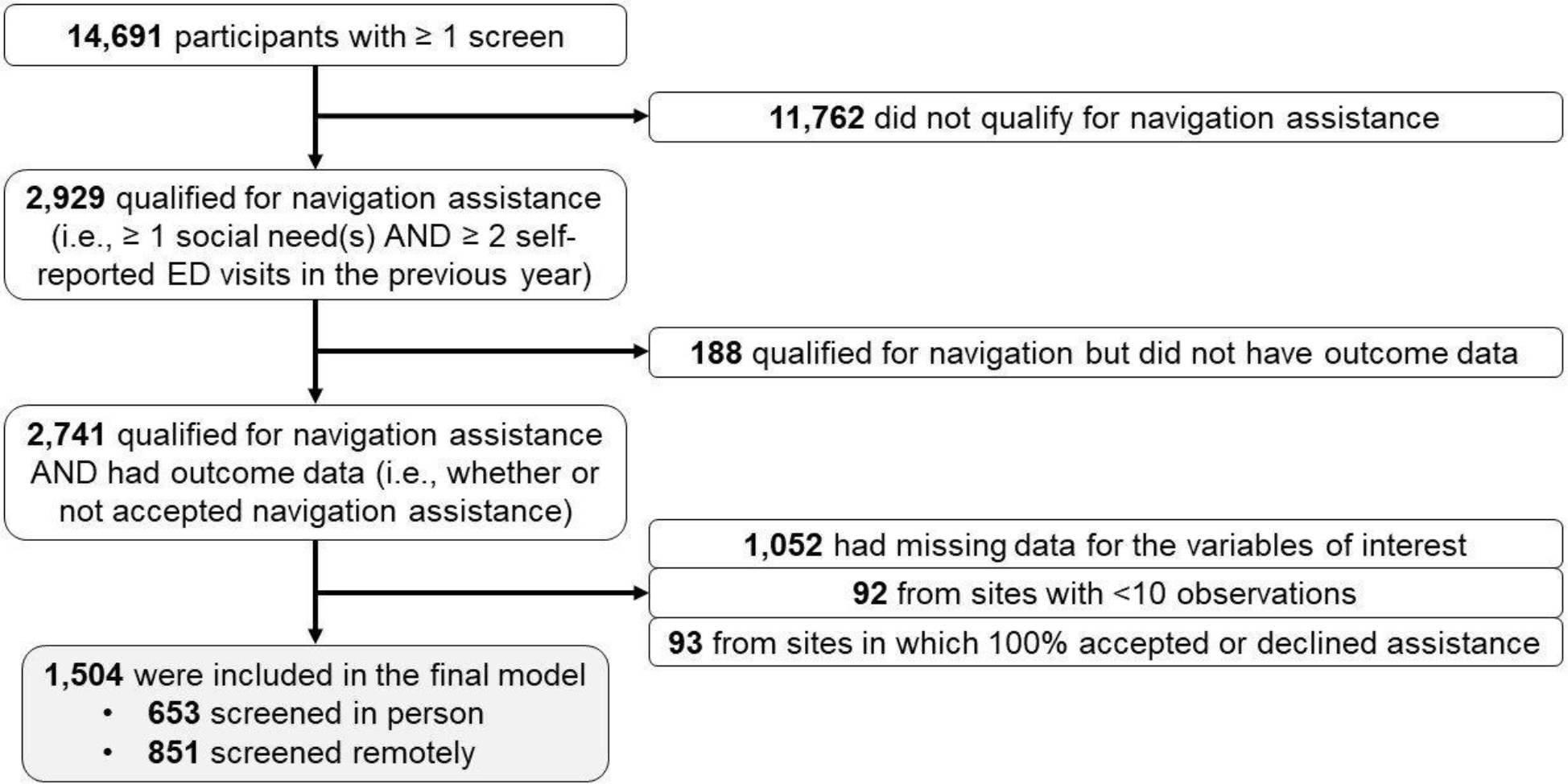
Study sample flow diagram
Study Measures
The primary, binary outcome measure was whether participants were willing to accept resource navigation assistance with their social needs. Participants responded “yes” or “no” to the following question: “You are eligible to receive extra help by a staff person called a navigator who can assist you with accessing resources. Would you like to receive help from a navigator?” The ordinal predictor variable – participants’ total number of social needs (based on a scale of 1–5) – originated from participants’ responses to the AHC Model screening questions. We acquired the screening mode (in-person; remote) of the clinical delivery sites from ORPRN AHC Model team members who inputted screening mode into a spreadsheet. Most covariates also came from participants’ responses to the screening questions. These included categorical variables of participants’ race,43 ethnicity, sex, household income, and for whom participants answered the screening questions.38,44 Birth year and zip code came from participants’ electronic health records to construct categorical variables for beneficiaries’ age and rurality, respectively. We constructed age as a 3-category variable (≤17; 18–64; ≥65) due to reasons corresponding to both Medicare qualification and mandatory reporting requirements in Oregon.45,46 Rurality designations came from the Oregon Office of Rural Health (urban; rural or frontier).47
Statistical Analysis
We used chi-square tests of independence to compare demographic characteristics of those screened for social needs in-person versus remotely. We conducted a multivariable logistic regression analysis to assess whether the screening mode (in-person; remote) modified associations between patients’ total number of social needs (predictor variable) and their willingness to accept help with social needs (outcome variable). Specifically, we created an interaction term (screening mode + total number of social needs) to test for the presence of effect modification.48 The model included clinical delivery site fixed effects and clustered standard errors at the site level. We selected confounders based on a priori assumptions and review of the literature regarding factors that are likely to affect both patients’ total number of social needs and interest in receiving healthcare-based assistance with social needs.49,50 In particular, both a participant’s acuity of need and whether they have reason to trust or mistrust health systems are likely to impact their interest in accepting assistance. For instance, we viewed the “race” variable as a proxy for racism. Racism affects acuity of need due to its impact on the unequal and unjust distribution of resources in society.51–53 It also can affect mistrust of healthcare systems due to historical and ongoing healthcare-based discrimination faced by those who are Black, Indigenous, and People of Color.54,55 While we conducted complete-case analyses, we also carried out sensitivity analyses with missing indicators (Appendix 2). We completed analyses using Stata/IC 15.1 from January 1 to December 10, 2021.
RESULTS
Participant Demographics
Participants’ social needs and demographic characteristics—including for the subgroups of those screened in person versus remotely—are available in Table 1. As anticipated, the majority of those screened in person participated prior to Oregon’s COVID-19 social distancing mandate,56 which went into effect on March 23, 2020 (n=599; 92%); and the majority of those screened remotely participated after the executive order (n=825; 97%). Likewise, there were significant differences between the in-person and remote subgroups regarding nearly all social need and demographic variables. For example, 61% of in-person versus 74% of remote participants endorsed ≥2 social needs (p<0.001). Among all participants, the most frequently reported social need was food insecurity (77%), followed by housing instability and quality (60%), transportation needs (45%), utility needs (33%), and interpersonal safety (12%).
Table 1.
Participant demographics, including those screened in person and those screened remotely (n=1,504)*
| Full Model (n=1,504) | In Person (n=653) | Remote (n=851) | P value† | |
|---|---|---|---|---|
| Total # of social needs disclosed | ||||
| 1 | 475 (32) | 253 (39) | 222 (26) | <.001 |
| 2 | 443 (29) | 183 (28) | 260 (31) | |
| 3 | 340 (23) | 132 (20) | 208 (24) | |
| 4 | 193 (13) | 68 (10) | 125 (15) | |
| 5 | 53 (4) | 17 (3) | 36 (4) | |
| Types of social needs disclosed | ||||
| Food | 1,160 (77) | 501 (77) | 659 (77) | .74 |
| Housing | 903 (60) | 351 (54) | 552 (65) | <.001 |
| Transportation | 673 (45) | 258 (40) | 415 (49) | <.001 |
| Utilities | 497 (33) | 197 (30) | 300 (35) | .04 |
| Safety | 185 (12) | 65 (10) | 120 (14) | .02 |
| “Are you Hispanic, Latino/a, or Spanish Origin?” | ||||
| Yes | 205 (14) | 76 (12) | 129 (15) | .05 |
| “Which one or more of the following would you say is your race?” ‡ | ||||
| AIAN | 121 (8) | 56 (9) | 65 (8) | <.001 |
| Asian | 19 (1) | 6 (1) | 13 (2) | |
| Black or African American | 155 (10) | 52 (8) | 103 (12) | |
| NHOPI | 17 (1) | 4 (1) | 13 (2) | |
| Other | 89 (6) | 25 (4) | 64 (8) | |
| White | 1,054 (70) | 496 (76) | 558 (66) | |
| Multiple | 49 (3) | 14 (2) | 35 (4) | |
| Sex | ||||
| Male | 533 (35) | 211 (32) | 322 (38) | .03 |
| Rurality | ||||
| Rural or Frontier | 490 (33) | 353 (54) | 137 (16) | <.001 |
| Age | ||||
| ≤17 | 180 (12) | 65 (10) | 115 (14) | <.001 |
| 18–64 | 1,164 (77) | 490 (75) | 674 (79) | |
| ≥65 | 160 (11) | 98 (15) | 62 (7) | |
| Mean Age | 41 | 43 | 40 | <.01 |
| “I am answering this survey about…” | ||||
| Myself | 1,293 (86) | 577 (88) | 716 (84) | <.01 |
| My child | 163 (11) | 55 (8) | 108 (13) | |
| Another adult | 34 (2) | 11 (2) | 23 (3) | |
| Other | 14 (1) | 10 (2) | 4 (0) | |
| “What is your annual household income from all sources?” | ||||
| <$10,000 | 596 (40) | 264 (40) | 332 (39) | <.001 |
| $10,000 to <$15,000 | 216 (14) | 90 (14) | 126 (15) | |
| $15,000 to <$20,000 | 176 (12) | 101 (15) | 75 (9) | |
| $20,000 to <$25,000 | 112 (7) | 36 (6) | 76 (9) | |
| $25,000 to <$35,000 | 182 (12) | 87 (13) | 95 (11) | |
| $35,000 to <$50,000 | 137 (9) | 47 (7) | 90 (11) | |
| $50,000 to <$75,000 | 56 (4) | 20 (3) | 36 (4) | |
| ≥$75,000 | 29 (2) | 8 (1) | 21 (2) | |
| Oregon’s “Stay Home, Save Lives” COVID-19 executive order (3/23/2020) | ||||
| Screened After Executive Order | 879 (58) | 54 (8) | 825 (97) | <.001 |
| Willing to accept navigation assistance | ||||
| Yes | 1,069 (71) | 413 (63) | 656 (77) | <.001 |
The data for this analysis was collected from October 17, 2018 through December 31, 2020.
P values based on chi-square tests of independence for those screened in person vs. remotely.
Participants who selected White and an additional race category were grouped with the non-White category they selected. We made this decision due to the variable “race” serving as a proxy for racism.43
Fifteen percent of remote versus 12% of in-person participants responded “Yes” to the question, “Are you Hispanic, Latino/a, or Spanish Origin?” (p=0.05). Participants’ responses about race were also significantly different across the two subgroups (p<0.001). Higher proportions of remote compared to in-person participants selected the categories of “Asian,” “Black or African American,” and “Native Hawaiian or Pacific Islander.” The in-person subgroup, however, included higher proportions of those who selected the categories “American Indian or Alaska Native” and “White.” Fifty-four percent of in-person versus 16% of remote participants had a rural or frontier address (p<0.001). Additionally, the in-person subgroup had a lower proportion of males (32% versus 38%; p=0.03), a higher proportion of those who took the screening on behalf of themselves (88% versus 84%; p<0.01), and a higher mean age (43 versus 40) (p<0.01).
Willingness to Accept Navigation
Seventy-one percent (n=1,069) of participants were willing to accept help with social needs, overall. A higher proportion of those screened remotely (77%) versus in person (63%) were willing to accept navigation assistance (p<0.001) (Table 1).
Multivariable Logistic Regression Analysis
In the multivariable logistic regression analysis presented in Table 2, there were significant associations between a higher number of social needs and a willingness to accept navigation assistance. Participants reporting 3 social needs (aOR,57 2.9, 95% CI, 1.6–5.0, p<0.001), 4 social needs (aOR, 3.2, 95% CI, 1.4–7.0, p<0.01), and 5 social needs (aOR, 5.2, 95% CI, 2.8–10, p<0.001) were significantly more likely to be willing to accept help compared to those reporting 1 social need. In the full model, neither screening mode (in-person; remote) nor the interaction term (screening mode + total number of social needs) were significantly associated with a willingness to accept help with social needs. This remained true in a sensitivity analysis in which missing indicators were included for all variables with missing data (Appendix 2). Regarding the remainder of covariates in the model, those selecting the race category “American Indian or Alaska Native” were significantly less likely to be willing to accept navigation assistance compared to those selecting the race category “White”, only (aOR, 0.6, 95% CI, .5-.8, p<0.01). In addition, participants who selected an income of $35,000 to $50,000 were significantly less likely to be willing to accept assistance compared to those who selected an income of <$10,000 (aOR, 0.6, 95% CI, .4-.9, p=0.02). No other covariates were significant.
Table 2.
Multivariable logistic regression results (n=1,504)
| Variable | aOR (95% CI) | P value |
|---|---|---|
| Total # of social needs disclosed | ||
| 1 | 1 [Reference] | NA |
| 2 | 1.4 (.7 – 2.7) | .30 |
| 3 | 2.9 (1.6 – 5.0) | <.001 |
| 4 | 3.2 (1.4 – 7.0) | <.01 |
| 5 | 5.2 (2.8 – 10.0) | <.001 |
| Screening method | ||
| In Person | 1 [Reference] | NA |
| Remote | 1.3 (.6 – 2.9) | .50 |
| Interaction Term (Total # of social needs * Screening method) | ||
| 1 need * remote | 1 [Reference] | NA |
| 2 needs * remote | .9 (.5 – 1.7) | .78 |
| 3 needs * remote | .5 (.3 – 1.0) | .06 |
| 4 needs * remote | 1.3 (.5 – 3.4) | .60 |
| 5 needs * remote | .4 (.16 – 1.2) | .10 |
| “Are you Hispanic, Latino/a, or Spanish Origin?” | ||
| No | 1 [Reference] | NA |
| Yes | 1.3 (.9 – 1.8) | .24 |
| “Which one or more of the following would you say is your race?”* | ||
| White | 1 [Reference] | NA |
| AIAN | .6 (.5 – .8) | <.01 |
| Asian | 1.4 (.6 – 3.5) | .41 |
| Black or African American | 1.4 (.8 – 2.3) | .26 |
| NHOPI | 1.6 (.3 – 9.6) | .60 |
| Other | 1.4 (.9 – 2.2) | .12 |
| Multiple | 1.4 (.7 – 2.7) | .33 |
| Sex | ||
| Female | 1 [Reference] | NA |
| Male | .9 (.8 – 1.8) | .37 |
| Rurality | ||
| Urban | 1 [Reference] | NA |
| Rural or Frontier | .9 (.6 – 1.2) | .46 |
| Age | ||
| ≤17 | 1.7 (.7 – 4.0) | .20 |
| 18–64 | 1 [Reference] | NA |
| ≥65 | 1.1 (.7 – 1.7) | .52 |
| “I am answering this survey about…” | ||
| Myself | 1 [Reference] | NA |
| My child | .6 (.3 – 1.3) | .21 |
| Another adult | .7 (.3 – 1.7) | .47 |
| Other | .8 (.3 – 2.2) | .70 |
| “What is your annual household income from all sources?” | ||
| <$10,000 | 1 [Reference] | NA |
| $10,000 to <$15,000 | 1.2 (1.0 – 1.5) | .11 |
| $15,000 to <$20,000 | 1.3 (.7 – 2.4) | .32 |
| $20,000 to <$25,000 | .9 (.6 – 1.4) | .80 |
| $25,000 to <$35,000 | .9 (.7 – 1.3) | .70 |
| $35,000 to <$50,000 | .6 (.4 – .9) | .02 |
| $50,000 to <$75,000 | .6 (.3 – 1.3) | .19 |
| ≥$75,000 | 1.0 (.3 – 3.3) | .97 |
We used the category “White” as the comparator because it was the largest group in our sample.
DISCUSSION
In this cross-sectional multisite study of the AHC Model in Oregon, our multivariable logistic regression analysis did not find that screening mode was an effect modifier for participants’ total number of social needs and their willingness to accept help with social needs. In other words, our results suggest that for individuals presenting with the same number of social needs, their likelihood of being willing to accept navigation may not be significantly impacted by whether they are screened for social needs in person or remotely. As with previous studies, we also found strong associations between a higher number of social needs and a willingness to accept resource navigation assistance.49,50
Overall, roughly 71% of eligible Medicare and Medicaid beneficiaries were willing to accept resource navigation assistance. While the proportion of those who were willing to accept navigation was significantly higher in the remote (77%) versus in-person (63%) subgroups, this difference was likely due to a higher number and acuity of social needs among remote participants (see Table 1) in light of the COVID-19 pandemic.58 Nonetheless, whether remote or in person, the proportion of patients who were willing to accept assistance both fell within the higher end of what previous studies have reported,35 and is an important finding given the potential impact of the AHC Model on healthcare-based social needs screening and referral interventions nationally. Although it was not an objective of our analysis, future evaluation of the AHC Model should consider whether and why patients’ willingness to accept navigation may vary across both states and bridge organizations.
We included race as a proxy for racism in our analysis because we anticipated that the impact of racism could differentially affect distinct groups’ willingness to accept navigation. It is important to note that our AIAN sample was significantly less willing to accept navigation compared to our White sample. However, since this was not the primary focus of our research study, we feel it is inappropriate to draw conclusions about this result without further investigation. In particular – mirroring the sentiments of other researchers59 – we recommend future studies use community-engaged methods to meaningfully examine potential differences across racial and ethnic groups regarding interest in social needs navigation, along with many other aspects of social needs screening and referral interventions.
As healthcare organizations consider how to integrate social needs screening and referral interventions into their clinical workflow, our study provides evidence that screening for social needs remotely may be justifiable in terms of patients’ willingness to accept help with the social needs that they disclose. Remote screening, particularly through low-tech telephone calls or text messages, could also be advantageous in terms of reaching patients who face barriers to in-person visits or videoconferencing.60–62 Of course, findings from the present study could be more reflective of how ORPRN implemented remote screening for social needs versus the remote aspect, by itself. For example, something about how ORPRN trained the health sciences students to conduct the screening may have been important (e.g., placing emphasis on trauma informed engagement). In a recent qualitative study on the AHC Model in Oregon, our team identified screener techniques that appeared to garner positive patient experiences, including demonstrating respect for patient autonomy, a kind demeanor, a genuine intention to help, and attentiveness and responsiveness to patients’ situations.63 More research is needed to better understand the ways in which those conducting screening for social needs, both in-person and remotely, can effectively foster patient engagement when discussing patients’ social contexts. For instance, future research could examine differences in AHC Model implementation across bridge organizations to assess how varying approaches to performing screening affected patients’ willingness to accept help.
Limitations
The study had a few notable limitations, especially regarding data availability. First, there were likely unmeasured drop-off points in patient engagement that resulted in nonresponse bias. For example, it was not possible to report on the total number nor the demographics of beneficiaries who declined participation in the AHC Model in Oregon during the study period. While results indicated that a high percentage of eligible beneficiaries were willing to accept navigation assistance, it is likely that otherwise eligible beneficiaries were never offered assistance because they declined to participate at the outset.64,65 Further, other studies have found that patients may request help with social needs, even after screening negatively for the same social needs on a questionnaire.66,67 Participants in the AHC Model were only offered assistance if they screened positively for ≥1 social need. But patients may have been reluctant to share such information with the clinical delivery sites, especially if they had concerns regarding how their data would be used.20 The study also lacked certain variables that may be important for patient engagement, like participants’ primary language or country of origin.68 Another principal limitation was that detailed information about how clinical delivery sites implemented the AHC Model in Oregon was not available. For instance, for the in-person screening sites, there was not reliable data about how the screening was administered (e.g., paper form, tablet) or by whom (e.g., staff- versus participant-administered). These implementation differences during in-person screening may have also influenced patients’ interest in accepting help with social needs, and future research should collect and analyze such information in greater detail.
Conclusions
Our study of the AHC Model in Oregon provides evidence that, among patients presenting with a similar number of social needs, the type of screening mode (in-person; remote) may not adversely affect the proportion of patients who are willing to accept help with resource navigation. For both healthcare organizations considering a return to in-person social needs screening following the COVID-19 pandemic and those weighing the merits of in-person versus remote approaches, our results indicate a consideration for the benefits of remote screening outside of a clinical visit, especially for populations with inequitable access to in-person healthcare. However, it is important that remote screening approaches be contextually tailored to promote health equity in terms of technological access, literacy, and appropriate language options for the populations being served. Whether screening for social needs is conducted in person or remotely, more research is needed to better understand what approaches best garner patient trust and authentic collaboration, especially among those who may benefit from resource navigation assistance.
Supplementary Material
Acknowledgements:
We thank all of the healthcare settings and Medicare and Medicaid beneficiaries who participated in the AHC Model in Oregon and contributed to this study.
Funding statement:
This project was supported by the Centers for Medicare and Medicaid Services (CMS) and the Agency for Healthcare Research and Quality of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $1,218,898 with 28 percent funded by CMS/HHS and $42,978 with 72 percent funded by AHRQ/HHS (Project Number 1R36HS027707-01). The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, CMS/HHS, AHRQ/HHS, or the U.S. Government. The research presented here was conducted by the awardee. Findings may not be consistent with or confirmed by the findings of the independent evaluation contractor.
Footnotes
Conflicting and competing interests: The authors have no conflicts of interest to disclose.
REFERENCES
- 1.Beauchamp DE. Public health as social justice. Inquiry. 1976;13(1):3–14. [PubMed] [Google Scholar]
- 2.Krieger N, Rowley DL, Herman AA, Avery B, Phillips MT. Racism, sexism, and social class: implications for studies of health, disease, and well-being. Am J Prev Med. 1993;9(6):82–122. [PubMed] [Google Scholar]
- 3.Link BG, Phelan J. Social conditions as fundamental causes of disease. J Health Soc Behav. 1995:80–94. [PubMed] [Google Scholar]
- 4.Krieger N, Birn A-E. A vision of social justice as the foundation of public health: commemorating 150 years of the spirit of 1848. Am J Public Health. 1998;88(11):1603–1606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Williams DR, Collins C. Racial residential segregation: a fundamental cause of racial disparities in health. Public Health Rep. 2001;116(5) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yearby R Structural racism and health disparities: Reconfiguring the social determinants of health framework to include the root cause. The Journal of Law, Medicine & Ethics. 2020;48(3):518–526. [DOI] [PubMed] [Google Scholar]
- 7.Fraze T, Lewis VA, Rodriguez HP, Fisher ES. Housing, transportation, and food: how ACOs seek to improve population health by addressing nonmedical needs of patients. Health Aff (Millwood). 2016;35(11):2109–2115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Buehler JW, Snyder RL, Freeman SL, Carson SR, Ortega AN. It’s not just insurance: the Affordable Care Act and population health. Public Health Rep. 2018;133(1):34–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sullivan HR. Hospitals’ obligations to address social determinants of health. AMA journal of ethics. 2019;21(3):248–258. [DOI] [PubMed] [Google Scholar]
- 10.Sandhu S, Lemmon ME, Eisenson H, Crowder C, Bettger JP. Addressing the social determinants of health during the COVID-19 pandemic: ensuring equity, quality, and sustainability. Fam Community Health. 2021;44(2):78–80. [DOI] [PubMed] [Google Scholar]
- 11.Metzl JM, Maybank A, De Maio F. Responding to the COVID-19 pandemic: the need for a structurally competent health care system. JAMA. 2020;324(3):231–232. [DOI] [PubMed] [Google Scholar]
- 12.Fortuna LR, Tolou-Shams M, Robles-Ramamurthy B, Porche MV. Inequity and the disproportionate impact of COVID-19 on communities of color in the United States: The need for a trauma-informed social justice response. Psychological Trauma: Theory, Research, Practice, and Policy. 2020;12(5):443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Horse AJY, Yang T-C, Huyser KR. Structural inequalities established the architecture for COVID-19 pandemic among native Americans in Arizona: a geographically weighted regression perspective. Journal of Racial and Ethnic Health Disparities. 2021:1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Garg A, Marino M, Vikani AR, Solomon BS. Addressing families’ unmet social needs within pediatric primary care: the health leads model. Clin Pediatr (Phila). 2012;51(12):1191–1193. [DOI] [PubMed] [Google Scholar]
- 15.Page-Reeves J, Kaufman W, Bleecker M, et al. Addressing social determinants of health in a clinic setting: the WellRx pilot in Albuquerque, New Mexico. The Journal of the American Board of Family Medicine. 2016;29(3):414–418. [DOI] [PubMed] [Google Scholar]
- 16.Sundar KR. Universal screening for social needs in a primary care clinic: a quality improvement approach using the your current life situation survey. The Permanente Journal. 2018;22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Alley DE, Asomugha CN, Conway PH, Sanghavi DM. Accountable health communities — addressing social needs through Medicare and Medicaid. N Engl J Med. 2016;374(1):8–11. [DOI] [PubMed] [Google Scholar]
- 18.Butler ED, Morgan AU, Kangovi S. Screening for unmet social needs: Patient engagement or alienation? NEJM Catalyst Innovations in Care Delivery. 2020;1(4) [Google Scholar]
- 19.LaForge K, Gold R, Cottrell E, et al. How 6 organizations developed tools and processes for social determinants of health screening in primary care: an overview. The Journal of ambulatory care management. 2018;41(1):2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Herrera C-N, Brochier A, Pellicer M, Garg A, Drainoni M-L. Implementing social determinants of health screening at community health centers: clinician and staff perspectives. J Prim Care Community Health. 2019;10:2150132719887260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Berry C, Paul M, Massar R, Marcello RK, Krauskopf M. Social Needs Screening and Referral Program at a Large US Public Hospital System, 2017. Am J Public Health. 2020;110(S2):S211–S214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Browne J, Mccurley JL, Fung V, Levy DE, Clark CR, Thorndike AN. Addressing social determinants of health identified by systematic screening in a medicaid accountable care organization: a qualitative study. J Prim Care Community Health. 2021;12:2150132721993651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kostelanetz S, Pettapiece-Phillips M, Weems J, et al. Health care professionals’ perspectives on universal screening of social determinants of health: a mixed-methods study. Population Health Management. 2021; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Powell RE, Henstenburg JM, Cooper G, Hollander JE, Rising KL. Patient perceptions of telehealth primary care video visits. The Annals of Family Medicine. 2017;15(3):225–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Access Kaplan B., Equity, and Neutral Space: Telehealth Beyond the Pandemic. The Annals of Family Medicine. 2021;19(1):75–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Duane J-N, Blanch-Hartigan D, Sanders JJ, et al. Environmental Considerations for Effective Telehealth Encounters: A Narrative Review and Implications for Best Practice. Telemedicine and e-Health. 2021;(00):1–8. [DOI] [PubMed] [Google Scholar]
- 27.Gordon HS, Solanki P, Bokhour BG, Gopal RK. “I’m not feeling like I’m part of the conversation” Patients’ perspectives on communicating in clinical video telehealth visits. J Gen Intern Med. 2020;35(6):1751–1758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Predmore ZS, Roth E, Breslau J, Fischer SH, Uscher-Pines L. Assessment of Patient Preferences for Telehealth in Post-COVID-19 Pandemic Health Care. JAMA Netw Open. Dec 1 2021;4(12):e2136405. doi: 10.1001/jamanetworkopen.2021.36405 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bailey SC, O’conor R, Bojarski EA, et al. Literacy disparities in patient access and health-related use of Internet and mobile technologies. Health Expect. 2015;18(6):3079–3087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Curtis ME, Clingan SE, Guo H, Zhu Y, Mooney LJ, Hser YI. Disparities in digital access among American rural and urban households and implications for telemedicine-based services. The Journal of Rural Health. 2021; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rodriguez JA, Saadi A, Schwamm LH, Bates DW, Samal L. Disparities In Telehealth Use Among California Patients With Limited English Proficiency: Study examines disparities in telehealth use among California patients with limited English proficiency. Health Aff (Millwood). 2021;40(3):487–495. [DOI] [PubMed] [Google Scholar]
- 32.Koonin LM, Hoots B, Tsang CA, et al. Trends in the use of telehealth during the emergence of the COVID-19 pandemic—United States, January–March 2020. Morbidity and Mortality Weekly Report. 2020;69(43):1595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Murray E, Roosevelt GE, Vogel JA. Screening for health-related social needs in the emergency department: Adaptability and fidelity during the COVID-19 pandemic. The American Journal of Emergency Medicine. 2021; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gottlieb LM, Pantell MS, Solomon LS. The National Academy of Medicine Social Care Framework and COVID-19 Care Innovations. J Gen Intern Med. 2021;36(5):1411–1414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.De Marchis EH, Alderwick H, Gottlieb LM. Do patients want help addressing social risks? The Journal of the American Board of Family Medicine. 2020;33(2):170–175. [DOI] [PubMed] [Google Scholar]
- 36.Sinding C, Wiernikowski J. Treatment decision making and its discontents. Soc Work Health Care. 2009;48(6):614–634. [DOI] [PubMed] [Google Scholar]
- 37.Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Bull World Health Organ. 2007;85:867–872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Centers for Medicare & Medicaid Services. The Accountable Health Communities Health-Related Social Needs Screening Tool. https://innovation.cms.gov/files/worksheets/ahcm-screeningtool.pdf
- 39.Billioux A, Verlander K, Anthony S, Alley D. Standardized screening for health-related social needs in clinical settings: The accountable health communities screening tool. NAM Perspectives. 2017; [Google Scholar]
- 40.Centers for Medicare & Medicaid Services (CMS). Accountable Health Communities Model. Updated October 20, 2021. Accessed December 8, 2021, https://innovation.cms.gov/innovation-models/ahcm
- 41.Oregon Rural Practice-based Research Network. About Us. Accessed January 21, 2022, https://www.ohsu.edu/oregon-rural-practice-based-research-network/about-us
- 42.Steeves-Reece AL, Elder NC, Graham TA, et al. Rapid Deployment of a Statewide COVID-19 ECHO Program for Frontline Clinicians: Early Results and Lessons Learned. The Journal of Rural Health. 2021;37(1):227–230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Data Standards for the Identification and Monitoring of Systemic Racism. 2017. https://files.ontario.ca/solgen_data-standards-en.pdf [Google Scholar]
- 44.Department of Health US and Human Services. HHS Implementation Guidance on Data Collection Standards for Race, Ethnicity, Sex, Primary Language, and Disability Status. https://aspe.hhs.gov/reports/hhs-implementation-guidance-data-collection-standards-race-ethnicity-sex-primary-language-disability-0 [Google Scholar]
- 45.Oregon State University. FAQs: Reporting Child Abuse & Neglect at OSU. https://youth.oregonstate.edu/abuse/faq
- 46.Oregon Department of Human Services. Elderly and Vulnerable Adult Rights and Abuse Prevention. https://www.oregon.gov/DHS/seniors-disabilities/SUA/Pages/Adult-Abuse-Prevention.aspx
- 47.Oregon Office of Rural Health. Oregon Office of Rural Health Geographic Definitions. Accessed December 30, 2021, https://www.ohsu.edu/oregon-office-of-rural-health/about-rural-and-frontier-data
- 48.Wang R, Ware JH. Detecting moderator effects using subgroup analyses. Prevention science. 2013;14(2):111–120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.De Marchis EH, Hessler D, Fichtenberg C, et al. Assessment of social risk factors and interest in receiving health care–based social assistance among adult patients and adult caregivers of pediatric patients. JAMA Network Open. 2020;3(10):e2021201–e2021201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.McQueen A, Kreuter MW, Herrick CJ, Li L, Brown DS, Haire-Joshu D. Associations among social needs, health and healthcare utilization, and desire for navigation services among US Medicaid beneficiaries with type 2 diabetes. Health & Social Care in the Community. 2021; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Jones CP. Levels of racism: a theoretic framework and a gardener’s tale. Am J Public Health. 2000;90(8):1212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Phelan JC, Link BG. Is racism a fundamental cause of inequalities in health? Annu Rev Sociol. 2015;41:311–330. [Google Scholar]
- 53.Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. The Lancet. 2017;389(10077):1453–1463. [DOI] [PubMed] [Google Scholar]
- 54.Jaiswal J, Halkitis PN. Towards a more inclusive and dynamic understanding of medical mistrust informed by science. Behav Med. 2019;45(2):79–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Quinn SC, Andrasik MP. Addressing vaccine hesitancy in BIPOC Communities—Toward trustworthiness, partnership, and reciprocity. N Engl J Med. 2021; [DOI] [PubMed] [Google Scholar]
- 56.Rogoway M Oregon governor issues ‘stay home’ order to enforce coronavirus restrictions. The Oregonian. [Google Scholar]
- 57.Ranganathan P, Aggarwal R, Pramesh C. Common pitfalls in statistical analysis: Odds versus risk. Perspect Clin Res. 2015;6(4):222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Kreuter M, Garg R, Javed I, Golla B, Wolff J, Charles C. 3.5 million social needs requests during COVID-19: What can we learn from 2–1-1? Health Affairs Blog. 2020; [Google Scholar]
- 59.Gottlieb LM, Lindau ST, Peek ME. Why Add “Abolition” to the National Academies of Sciences, Engineering, and Medicine’s Social Care Framework? AMA Journal of Ethics. 2022;24(3):170–180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Baras Shreibati J When low tech wins. N Engl J Med. 2021;385(7):581–583. [DOI] [PubMed] [Google Scholar]
- 61.Chen J, Li KY, Andino J, et al. Predictors of Audio-Only Versus Video Telehealth Visits During the COVID-19 Pandemic. J Gen Intern Med. 2021:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Gilson SF, Umscheid CA, Laiteerapong N, Ossey G, Nunes KJ, Shah SD. Growth of ambulatory virtual visits and differential use by patient sociodemographics at one urban Academic Medical Center during the COVID-19 pandemic: retrospective analysis. JMIR Medical Informatics. 2020;8(12):e24544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Steeves-Reece AL, Nicolaidis C, Richardson DM, et al. “It Made Me Feel like Things Are Starting to Change in Society:” A Qualitative Study to Foster Positive Patient Experiences during Phone-Based Social Needs Interventions. Int J Environ Res Public Health. 2022;19(19):12668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Schickedanz A, Sharp A, Hu YR, et al. Impact of social needs navigation on utilization among high utilizers in a large integrated health system: a quasi-experimental study. J Gen Intern Med. 2019;34(11):2382–2389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Chagin K, Choate F, Cook K, Fuehrer S, Misak JE, Sehgal AR. A Framework for Evaluating Social Determinants of Health Screening and Referrals for Assistance. J Prim Care Community Health. 2021;12:21501327211052204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Ray KN, Gitz KM, Hu A, Davis AA, Miller E. Nonresponse to Health-Related Social Needs Screening Questions. Pediatrics. 2020;146(3) [DOI] [PubMed] [Google Scholar]
- 67.Hassan A, Scherer EA, Pikcilingis A, et al. Improving social determinants of health: effectiveness of a web-based intervention. Am J Prev Med. 2015;49(6):822–831. [DOI] [PubMed] [Google Scholar]
- 68.Uwemedimo OT, May H. Disparities in utilization of social determinants of health referrals among children in immigrant families. Frontiers in pediatrics. 2018;6:207. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.