

Abstract
The genetic features of a series of 227 patients with hereditary motor and sensory neuropathy (HMSN) have been analysed. The series comprised 119 index cases from 110 families in which 108 affected relatives were identified. The cases were classified as having type I or type II HMSN on the basis of nerve conduction studies. Inheritance in the type I cases was autosomal dominant in 139 (45 families) and autosomal recessive in eight (four families) with 26 single cases. For the type II cases, 35 (17 families) were autosomal dominant and three (two families) autosomal recessive with 16 single cases. A significant excess of males was present in the combined single and recessive type I cases and in the type I index cases. No X linked pedigrees were identified.
The correlation coefficients for motor nerve conduction velocity between the index cases and their relatives suggested further genetic heterogeneity in the type I cases. Parent-offspring and sib-sib correlation coefficients for age of onset in the dominantly inherited type I cases were less than 0·5. There was therefore no strong suggestion of genetic heterogeneity in terms of age of onset.
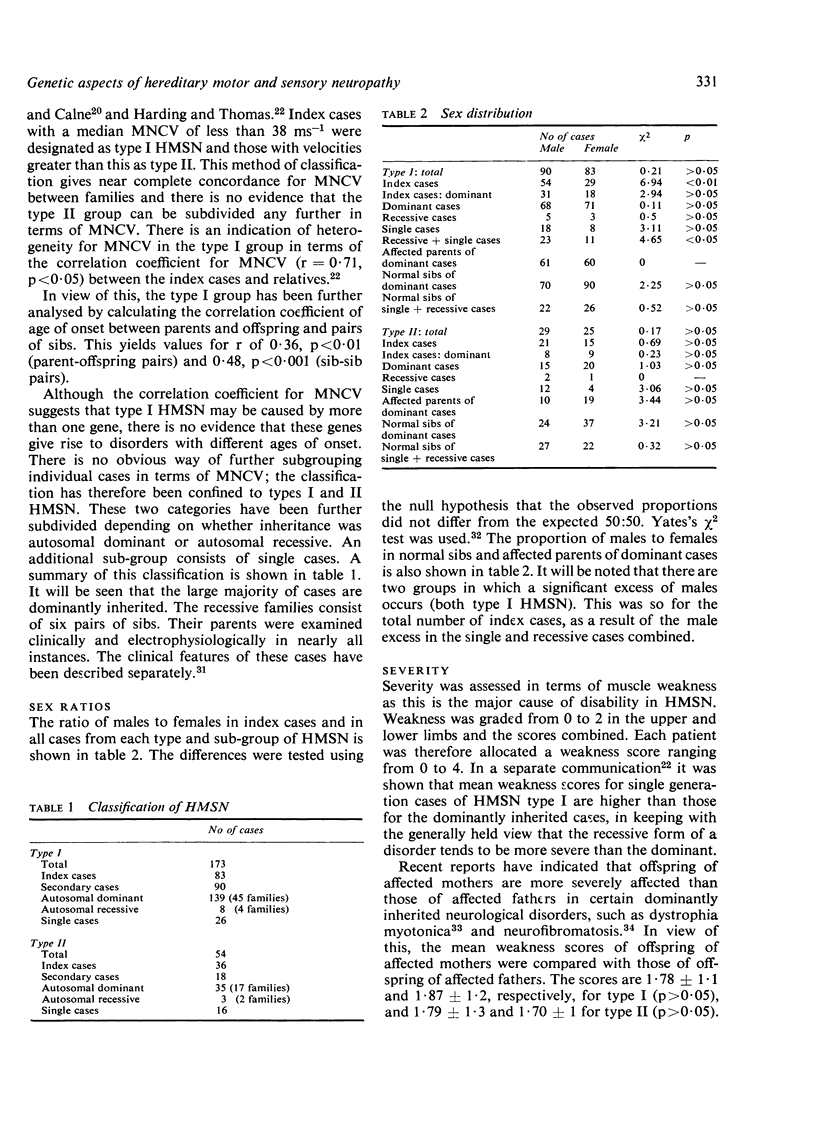
The severity of muscle weakness did not differ between the dominantly inherited type I and type II cases. In both types males had higher weakness scores than females, but there was no difference for either type in relation to the sex of the affected parent.
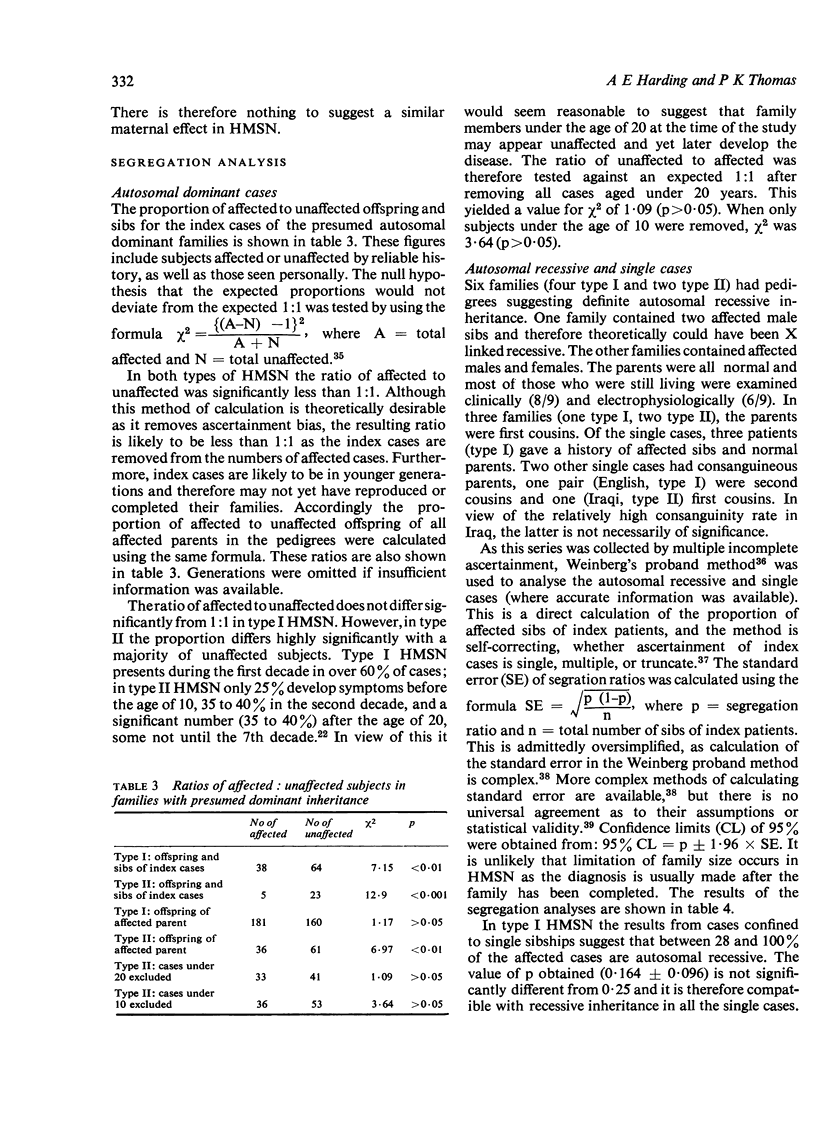
Segration analysis suggested that approximately 70% of the single generation type I cases were of autosomal recessive inheritance, whereas only about 25% of the single generation type II cases were recessive. Biological fitness was reduced in type II HMSN, which would support a higher proportion of new dominant mutations among the single cases of this type than in type I. Despite the excess of males in the type I single case/recessive category, a contribution of cases with X linked recessive inheritance is improbable. Single cases of HMSN, especially the type II form in view of its later onset, are likely to be unrecognised clinically and will be classified as `cryptogenic' neuropathy. As in many affected subjects the degree of disability is minimal, a careful scrutiny of the relatives is merited in such instances.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- AUSTIN J. H. Observations on the syndrome of hypertrophic neuritis (the hypertrophic interstitial radiculo-neuropathies). Medicine (Baltimore) 1956 Sep;35(3):187–237. doi: 10.1097/00005792-195609000-00002. [DOI] [PubMed] [Google Scholar]
- Brust J. C., Lovelace R. E., Devi S. Clinical and electrodiagnostic features of Charcot-Marie-Tooth syndrome. Acta Neurol Scand Suppl. 1978;68:1–142. [PubMed] [Google Scholar]
- Davis C. J., Bradley W. G., Madrid R. The peroneal muscular atrophy syndrome: clinical, genetic, electrophysiological and nerve biopsy studies. I. Clinical, genetic and electrophysiological findings and classification. J Genet Hum. 1978 Dec;26(4):311–349. [PubMed] [Google Scholar]
- Dyck P. J., Lambert E. H. Lower motor and primary sensory neuron diseases with peroneal muscular atrophy. I. Neurologic, genetic, and electrophysiologic findings in hereditary polyneuropathies. Arch Neurol. 1968 Jun;18(6):603–618. doi: 10.1001/archneur.1968.00470360025002. [DOI] [PubMed] [Google Scholar]
- Dyck P. J., Lambert E. H. Lower motor and primary sensory neuron diseases with peroneal muscular atrophy. II. Neurologic, genetic, and electrophysiologic findings in various neuronal degenerations. Arch Neurol. 1968 Jun;18(6):619–625. doi: 10.1001/archneur.1968.00470360041003. [DOI] [PubMed] [Google Scholar]
- GILLIATT R. W., THOMAS P. K. Extreme slowing of nerve conduction in peroneal muscular atrophy. Ann Phys Med. 1957 Aug;4(3):104–106. doi: 10.1093/rheumatology/4.3.104. [DOI] [PubMed] [Google Scholar]
- Harding A. E., Thomas P. K. Hereditary distal spinal muscular atrophy. A report on 34 cases and a review of the literature. J Neurol Sci. 1980 Mar;45(2-3):337–348. doi: 10.1016/0022-510x(80)90177-x. [DOI] [PubMed] [Google Scholar]
- Harper P. S., Dyken P. R. Early-onset dystrophia myotonica. Evidence supporting a maternal environmental factor. Lancet. 1972 Jul 8;2(7767):53–55. doi: 10.1016/s0140-6736(72)91548-6. [DOI] [PubMed] [Google Scholar]
- Humberstone P. M. Nerve conduction studies in Charcot-Marie-Tooth disease. Acta Neurol Scand. 1972;48(2):176–190. doi: 10.1111/j.1600-0404.1972.tb07539.x. [DOI] [PubMed] [Google Scholar]
- Lapresle J., Salisachs P., Kremlin-Bicêtre L. Onion bulbs in a nerve biopsy specimen from an original case of Roussy-Lévy disease. Arch Neurol. 1973 Nov;29(5):346–348. doi: 10.1001/archneur.1973.00490290086013. [DOI] [PubMed] [Google Scholar]
- Mahloudji M. A recessively inherited mixed polyneuropathy of early onset. J Med Genet. 1969 Dec;6(4):411–412. doi: 10.1136/jmg.6.4.411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meadows J. C., Marsden C. D. A distal form of chronic spinal muscular atrophy. Neurology. 1969 Jan;19(1):53–58. doi: 10.1212/wnl.19.1.53. [DOI] [PubMed] [Google Scholar]
- Miller M., Hall J. G. Possible maternal effect on severity of neurofibromatosis. Lancet. 1978 Nov 18;2(8099):1071–1073. doi: 10.1016/s0140-6736(78)91804-4. [DOI] [PubMed] [Google Scholar]
- Salisachs P. Wide spectrum of motor conduction velocity in Charcot-Marie-Tooth disease. An anatomico-physiological interpretation. J Neurol Sci. 1974 Sep;23(1):25–31. doi: 10.1016/0022-510x(74)90138-5. [DOI] [PubMed] [Google Scholar]
- Skre H. Genetic and clinical aspects of Charcot-Marie-Tooth's disease. Clin Genet. 1974;6(2):98–118. doi: 10.1111/j.1399-0004.1974.tb00638.x. [DOI] [PubMed] [Google Scholar]
- Sumner D., Crawfurd M. D., Harriman D. G. Distal muscular dystrophy in an English family. Brain. 1971;94(1):51–60. doi: 10.1093/brain/94.1.51. [DOI] [PubMed] [Google Scholar]
- Thomas P. K., Calne D. B. Motor nerve conduction velocity in peroneal muscular atrophy: evidence for genetic heterogeneity. J Neurol Neurosurg Psychiatry. 1974 Jan;37(1):68–75. doi: 10.1136/jnnp.37.1.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas P. K., Calne D. B., Stewart G. Hereditary motor and sensory polyneuropathy (peroneal muscular atrophy). Ann Hum Genet. 1974 Oct;38(2):111–153. doi: 10.1111/j.1469-1809.1974.tb01945.x. [DOI] [PubMed] [Google Scholar]
- de Weerdt C. J. Linkage relations of locus for X-borne type of Charcot-Marie-Tooth muscular atrophy and that for Xg blood groups. J Med Genet. 1976 Oct;13(5):399–399. doi: 10.1136/jmg.13.5.399. [DOI] [PMC free article] [PubMed] [Google Scholar]