

Abstract
Background
Otitis media with effusion (OME) is an accumulation of fluid in the middle ear cavity, common amongst young children. The fluid may cause hearing loss. When persistent, it may lead to behavioural problems and a delay in expressive language skills. Management of OME includes watchful waiting, medical, surgical and mechanical treatment. Autoinflation is a self‐administered technique, which aims to ventilate the middle ear and encourage middle ear fluid clearance by providing a positive pressure of air in the nose and nasopharynx (using a nasal balloon or other handheld device). This positive pressure (sometimes combined with simultaneous swallow) encourages opening of the Eustachian tube and may help ventilate the middle ear.
Objectives
To assess the efficacy (benefits and harms) of autoinflation for the treatment of otitis media with effusion in children.
Search methods
The Cochrane ENT Information Specialist searched the Cochrane ENT Register; Central Register of Controlled Trials (CENTRAL); Ovid MEDLINE; Ovid Embase; Web of Science; ClinicalTrials.gov; ICTRP and additional sources for published and unpublished trials. The date of the search was 20 January 2023.
Selection criteria
We included randomised controlled trials (RCTs) and quasi‐randomised trials in children aged 6 months to 12 years with unilateral or bilateral OME. We included studies that compared autoinflation with either watchful waiting (no treatment), non‐surgical treatment or ventilation tubes.
Data collection and analysis
We used standard Cochrane methods. Our primary outcomes were determined following a multi‐stakeholder prioritisation exercise and were: 1) hearing, 2) OME‐specific quality of life and 3) pain and distress. Secondary outcomes were: 1) persistence of OME, 2) other adverse effects (including eardrum perforation), 3) compliance or adherence to treatment, 4) receptive language skills, 5) speech development, 6) cognitive development, 7) psychosocial skills, 8) listening skills, 9) generic health‐related quality of life, 10) parental stress, 11) vestibular function and 12) episodes of acute otitis media. We used GRADE to assess the certainty of evidence for each outcome.
Although we included all measures of hearing assessment, the proportion of children who returned to normal hearing was our preferred method to assess hearing, due to challenges in interpreting the results of mean hearing thresholds.
Main results
We identified 11 completed studies that met our inclusion criteria (1036 participants). The majority of studies included children aged between 3 and 11 years. Most were carried out in Europe or North America, and they were conducted in both hospital and community settings. All compared autoinflation (using a variety of different methods and devices) to no treatment. Most studies required children to carry out autoinflation two to three times per day, for between 2 and 12 weeks. The outcomes were predominantly assessed just after the treatment phase had been completed. Here we report the effects at the longest follow‐up for our main outcome measures.
Return to normal hearing
The evidence was very uncertain regarding the effect of autoinflation on the return to normal hearing. The longest duration of follow‐up was 11 weeks. At this time point, the risk ratio was 2.67 in favour of autoinflation (95% confidence interval (CI) 1.73 to 4.12; 85% versus 32%; number needed to treat to benefit (NNTB) 2; 1 study, 94 participants), but the certainty of the evidence was very low.
Disease‐specific quality of life
Autoinflation may result in a moderate improvement in quality of life (related to otitis media) after short‐term follow‐up. One study assessed quality of life using the Otitis Media Questionnaire‐14 (OMQ‐14) at three months of follow‐up. Results were reported as the number of standard deviations above or below zero difference, with a range from ‐3 (better) to +3 (worse). The mean difference was ‐0.42 lower (better) for those who received autoinflation (95% CI ‐0.62 to ‐0.22; 1 study, 247 participants; low‐certainty evidence; the authors report a change of 0.3 as clinically meaningful).
Pain and distress caused by the procedure
Autoinflation may result in an increased risk of ear pain, but the evidence was very uncertain. One study assessed this outcome, and identified a risk ratio of 3.50 for otalgia in those who received autoinflation, although the overall occurrence of pain was low (95% CI 0.74 to 16.59; 4.4% versus 1.3%; number needed to treat to harm (NNTH) 32; 1 study, 320 participants; very low‐certainty evidence).
Persistence of OME
The evidence suggests that autoinflation may slightly reduce the persistence of OME at three months. Four studies were included, and the risk ratio for persistence of OME was 0.88 for those receiving autoinflation (95% CI 0.80 to 0.97; 4 studies, 483 participants; absolute reduction of 89 people per 1000 with persistent OME; NNTB 12; low‐certainty evidence).
Authors' conclusions
All the evidence we identified was of low or very low certainty, meaning that we have little confidence in the estimated effects. However, the data suggest that autoinflation may have a beneficial effect on OME‐specific quality of life and persistence of OME in the short term, but the effect is uncertain for return to normal hearing and adverse effects. The potential benefits should be weighed against the inconvenience of regularly carrying out autoinflation, and the possible risk of ear pain.
Keywords: Child; Child, Preschool; Humans; Cognition; Drug-Related Side Effects and Adverse Reactions; Epistaxis; Otitis Media with Effusion; Otitis Media with Effusion/therapy; Pain
Plain language summary
Autoinflation for otitis media with effusion (OME or 'glue ear') in children
Key messages
Due to a lack of robust evidence, we are uncertain whether autoinflation has any effect on hearing. Using autoinflation two to three times per day may slightly reduce the number of children with OME after three months follow‐up. Scores on a questionnaire that looked at quality of life for people with OME were also better for children who carried out autoinflation. However, some children may experience pain when using autoinflation.
What is OME?
Otitis media with effusion (OME, sometimes called 'glue ear') is a common condition affecting young children. Fluid collects in the middle ear, causing hearing impairment. As a result of their poor hearing, children may have behavioural difficulties and delays in their speech development.
How is OME treated?
Most of the time, OME does not need any treatment and the symptoms will get better with time. In children with persistent OME, different treatments have been explored, including medications or surgery. Autoinflation is a technique where children blow air out of their nose against a pressure device (such as a balloon). This forces air back through the Eustachian tube, which connects the back of the nose to the middle ear. Opening of this tube may allow the middle ear fluid to drain away.
What did we want to find out?
We wanted to identify whether autoinflation was better than no treatment, medical treatment or surgical treatment for children with OME.
We also wanted to see if there were any unwanted effects associated with autoinflation.
What did we do?
We searched for studies that compared autoinflation with no treatment or other treatments in children with OME. We compared and summarised the study results, and rated our confidence in the evidence, based on factors such as study methods and sizes.
What did we find?
We found 11 studies that involved 1036 children with OME. Most of the studies were in children aged over three years old, and only lasted for up to three months. They compared autoinflation (carried out two to three times per day) with no treatment.
We are uncertain whether autoinflation has any effect on hearing, as there was very little evidence about this.
Autoinflation may slightly reduce the number of children who still have OME after three months of follow‐up, and may result in an improvement in quality of life.
Children who use autoinflation may experience more ear pain than those who do not receive any treatment, but only one study assessed this, and the number of children with pain was small (4.4% compared to 1.3% in those who did not have treatment).
What are the limitations of the evidence?
We have very little information about the longer‐term effects of autoinflation. A variety of different techniques and devices are available for autoinflation, and we do not know if some of these are more effective than others.
How up‐to‐date is this evidence?
The evidence is up‐to‐date to January 2023.
Summary of findings
Summary of findings 1. Autoinflation compared to no treatment for otitis media with effusion (OME) in children.
| Autoinflation compared to no treatment for otitis media with effusion (OME) in children | ||||||
| Patient or population: otitis media with effusion (OME) in children aged 6 months to 12 years Setting: outpatient Intervention: autoinflation Comparison: no treatment | ||||||
| Outcomes | Relative effect (95% CI) | Anticipated absolute effects* (95% CI) | Certainty of the evidence (GRADE) | What happens | ||
| Without autoinflation | With autoinflation | Difference | ||||
| Proportion of children whose hearing is normal Follow‐up: up to 3 months № of participants: 94 (1 RCT) |
RR 2.67 (1.73 to 4.12) | 31.9% | 85.2% (55.2 to 100) | 53.3% more (23.3 more to 68.1more) | ⊕⊝⊝⊝ Very low1,2,3 | The evidence is very uncertain about the effect of autoinflation on return to normal hearing at 3 months. |
| Disease‐specific quality of life Mean difference in standardised OMQ‐14 scores (lower score is favourable) Follow‐up: 3 months (short‐term) № of participants: 247 (1 RCT) |
— | — | — | MD 0.42 lower (0.62 lower to 0.22 lower) | ⊕⊕⊝⊝ Low1,4 | The evidence suggests that autoinflation may improve disease‐specific quality of life at 3 months. The study authors reported a change of 0.3 as clinically meaningful. |
| Pain and distress related to the procedure: otalgia Follow‐up: 3 months (short‐term) № of participants: 320 (1 RCT) |
RR 3.50 (0.74 to 16.59) | 1.3% | 4.4% (1 to 22.6) |
3.1% more (0.3% fewer to 19.5% more) | ⊕⊝⊝⊝ Very low1,5 | Autoinflation may slightly increase the risk of ear pain (otalgia), but the evidence is very uncertain. |
| Persistence of OME Follow‐up: 3 months (short‐term) № of participants: 483 (4 RCTs) |
RR 0.88 (0.80 to 0.97) | 74.1% | 65.2% (59.3 to 71.9) | 8.9% fewer (14.8 fewer to 2.2 fewer) | ⊕⊕⊝⊝ Low1,6 | The evidence suggests that autoinflation may slightly reduce persistence of OME at 3 months. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OME: otitis media with effusion; OMQ‐14: Otitis Media Questionnaire‐14; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded by one level for a risk of performance bias.
2Downgraded by one level for indirectness, as no description of 'normal hearing' was provided.
3Downgraded by one level for imprecision, as the optimal information size (OIS) was not reached (< 300 events).
4Downgraded by one level for imprecision, as the OIS was not reached (< 400 participants).
5Downgraded by two levels for imprecision, as the OIS was not reached (< 300 events) and the confidence interval crosses two decision thresholds (RR 0.8 and 1.25).
6Downgraded by one level for a risk of detection bias.
Background
Description of the condition
Otitis media with effusion (OME) is a common condition in early childhood. The condition, also known as 'glue ear' and serous otitis media, is defined as "the presence of fluid in the middle ear without signs or symptoms of acute infection" (Rosenfeld 2016).
A key clinical feature of OME is hearing loss, due to decreased mobility of the tympanic membrane and consequent loss of sound conduction (Rosenfeld 2016). When hearing loss persists, this may affect speech and language development, and lead to behavioural problems in some children (NICE 2008). Other symptoms that may be attributable to OME include balance (vestibular) problems and ear discomfort (Rosenfeld 2016). When symptoms persist, they may lead to poor school performance and affect a child's daily activities, social interactions and emotions, possibly leading to a poorer quality of life for the child (Rosenfeld 2000).
It is thought that up to 80% of children have had OME by the age of four years, but a decline in prevalence is observed for children beyond six years of age (Williamson 2011). Most episodes of OME in children resolve spontaneously within three months, however approximately 35% of children will have more than one episode of OME and, furthermore, 5% to 10% of episodes will last for more than a year (Rosenfeld 2016). Children with OME following an episode of untreated acute otitis media have a 59% rate of resolution by one month rising to 74% by three months, while children with newly diagnosed OME of unknown duration demonstrate a resolution rate of 28% by three months and up to 42% by six months (Rosenfeld 2003). The condition is more prevalent in children with craniofacial syndromes, such as Down syndrome or cleft palate (Flynn 2009 [https://revman.cochrane.org/#/767321080313575379/dashboard/htmlView/current?revertEnabled=false&versionWithProductionChanges=false#REF‐Flynn‐2009]; Maris 2014 [https://revman.cochrane.org/#/767321080313575379/dashboard/htmlView/current?revertEnabled=false&versionWithProductionChanges=false#REF‐Maris‐2014]). Atopy has been considered a potential risk factor for OME in children (Kreiner‐Møller 2012; Marseglia 2008; Zernotti 2017), as have parental smoking, attendance at day care and low socioeconomic status (Dewey 2000; Marx 1995; Rovers 2006).
Diagnosis of OME is typically by clinical examination including (pneumatic) otoscopy and/or tympanometry in primary care. Following diagnosis, there will often be a period of active observation for at least three months. During the observation period the care provider may offer a non‐surgical intervention such as hearing aids or autoinflation. The National Institute for Health and Care Excellence (NICE) and the American Academy of Otolaryngology–Head and Neck Surgery (AAO‐HNS) do not currently recommend the use of antibiotics, antihistamines, decongestants or corticosteroids for OME as there is insufficient evidence to suggest they are effective treatments (NICE 2008; Rosenfeld 2016). If OME has not resolved within the three‐month observation period, the child may be referred for further management/active intervention. This may include hearing aid provision or review by an ENT surgeon for consideration for myringotomy, ventilation tubes insertion and/or adenoidectomy. The choice of active intervention varies considerably. Earlier active intervention may be considered for children at increased risk of developmental difficulties (see Rosenfeld 2016 for a list of 'at‐risk' factors).
This Cochrane Review focusses on autoinflation as a treatment for OME in children. This review forms part of a suite of five reviews of OME treatment, which will address those interventions identified in a prioritisation exercise as being most important and in need of up‐to‐date Cochrane Reviews, namely myringotomy and insertion of ventilation tubes, adenoidectomy with or without ventilation tubes, topical and oral steroids, autoinflation and antibiotics (Cochrane ENT 2020).
Description of the intervention
Autoinflation is a technique that forces the Eustachian tube to open by raising intranasal pressure. Its main goal is to aerate the middle ear cavity and equalise pressures in both sides of the tympanic membrane. Autoinflation can be achieved in a number of ways: forced exhalation with mouth and nose closed, for example the Valsalva manoeuvre; blowing up of a balloon through each nostril (demonstrated here); or use of a device that utilises Politzeration, which involves blowing air up the nose while the patient swallows. There are commercial devices available, such as the Otovent nasal balloon device, and the air‐pump EarPopper device (RACGP 2016). Given the manipulation required for successful autoinflation, it is considered suitable for children aged four years and over (Williamson 2015). It is a low‐cost intervention that can be used during an active observation period post‐diagnosis and may avoid the need for a surgical intervention (NICE 2016).
How the intervention might work
The aim of autoinflation is to introduce air into the middle ear, via the Eustachian tube, thus equalising the pressures either side of the tympanic membrane, and promoting drainage of fluid (Perera 2013). Each time the procedure is repeated, it promotes aeration of the middle ear, thereby mitigating any abnormal Eustachian tube function until normal functioning returns (Berkman 2013).
Why it is important to do this review
A Cochrane Review assessing the effects of autoinflation on OME for adults and children was published in 2013 (Perera 2013), updating a review originally published in 2006. Searches were run to 2013 and the review included eight studies. The studies were small and had a short follow‐up. The review authors concluded that "it is reasonable to consider autoinflation whilst awaiting natural resolution of otitis media with effusion".
A scoping search undertaken in 2020 identified seven abstracts published since 2013, including five publications assessing the EarPopper device and two publications relating to nasal balloon autoinflation with the Otovent device. Searches also identified two clinical trial registrations relating to a Swedish study of the Otovent device (Ejnell 2015a; Ejnell 2015b). A prioritisation exercise undertaken in 2020 identified a review of autoinflation for OME as a top priority (Cochrane ENT 2020). Given the number of relevant studies published in recent years, it is timely to update the evidence.
This review has been produced as part of a suite of reviews, which also inform a NICE guideline on the management of OME in children (NICE 2023). The population of interest was therefore confined to children for consistency across the suite of reviews, and to align with the NICE guideline update.
Objectives
To assess the effects (benefits and harms) of autoinflation for otitis media with effusion (OME) in children.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) and quasi‐randomised trials (where studies were designed as RCTs, but the sequence generation for allocation of treatment used methods such as alternative allocation, birth dates and alphabetical order).
Types of participants
The population of interest was children aged 6 months to 12 years with unilateral or bilateral otitis media with effusion (OME). If a study included children aged younger than 6 months and older than 12 years, we planned to only include the study if the majority of children fit our inclusion criteria, or if the study authors presented outcome data according to age group. We included all children regardless of any comorbidity such as Down syndrome or cleft palate. Clinical diagnosis of OME was confirmed by oto(micro)scopy or tympanometry, or both.
Types of interventions
Intervention
Autoinflation by any method.
Comparator
We planned to assess the following comparisons:
autoinflation versus watchful waiting;
autoinflation versus non‐surgical treatment;
autoinflation versus ventilation tubes.
If study participants had received other treatments (for example, intranasal steroids, oral steroids, antibiotics, mucolytics or decongestants), we included the study if both arms received identical treatments.
Types of outcome measures
We analysed the following outcomes in the review, but we did not use them as a basis for including or excluding studies. We assessed all outcomes at very short term (< 6 weeks), short term (> 6 weeks to ≤ 3 months), medium term (> 3 months to ≤ 1 year) and long term > 1 year.
Primary outcomes
-
Hearing:
Proportion of children whose hearing has returned to normal, with normal hearing defined as 20 dB HL or less (assessed using age‐appropriate tests).
Hearing threshold.
It was anticipated that study data for these outcomes may be derived from a variety of assessment methods. To avoid loss of important evidence, we extracted all such data for analysis. However, we gave consideration to the appropriateness of pooling different types of data in meta‐analysis. Our selection of primary outcomes is based principally upon clinical importance, but also permits applicability across a variety of age‐appropriate assessment methods and considers the types of outcome data that are most likely to be available. Accordingly, we regard the proportion of participants whose hearing has returned to normal as the most important measure of hearing impact. We consider medium‐ and long‐term outcome data as the most clinically important.
-
Disease‐specific quality of life measured using a validated instrument, for example:
OM8‐30 (Haggard 2003);
Otitis Media‐6 (Rosenfeld 1997).
Adverse events ‐ pain and distress caused by the procedure, including otalgia.
Secondary outcomes
Presence/persistence of OME.
-
Adverse events ‐ measured by the number of participants affected:
eardrum perforation.
Compliance.
-
Receptive language skills, measured using a validated scale, for example:
Peabody Picture Vocabulary Test ‐ Revised (Dunn 2007);
Reynell Developmental Language Scales (relevant domains) (Reynell 1985);
Preschool Language Scale (PLS) (relevant domains) (Zimmerman 1992);
Sequenced Inventory of Communication (SCID) (relevant domains) (Hedrick 1984).
-
Speech development, or expressive language skills, measured using a validated scale, for example:
Schlichting test (Schlichting 2010);
Lexi list (Schlichting 2007);
Reynell Developmental Language Scales (relevant domains) (Reynell 1985);
PLS (relevant domains) (Zimmerman 1992);
SCID (relevant domains) (Hedrick 1984).
-
Cognitive development, measured using a validated scale, for example:
Griffiths Mental Development Scales (Griffiths 1996);
McCarthy General Cognitive Index (McCarthy 1972);
Bayley Scales of Infant and Toddler Development (Bayley 2006).
-
Psychosocial outcomes, measured using a validated scale, for example:
Social Skills Scale of the Social Skills Rating System (Gresham 1990);
Child Behaviour Checklist (Achenbach 2011);
Strengths and Difficulties Questionnaire (Goodman 1997);
Pediatric Symptom Checklist (Jellinek 1988).
Listening skills, for example listening to stories and instructions effectively. Given that there are few validated scales to assess listening skills in children with OME, we included any methods used by trialists.
-
Generic health‐related quality of life assessed using a validated instrument, for example:
EQ‐5D (Rabin 2001);
TNO AZL Children’s QoL (TACQOL) (Verrips 1998);
TNO AZL Pre‐school children QoL (TAPQOL) (Fekkes 2000);
TNO AZL Infant Quality of Life (TAIQOL) (TNO 1997);
Infant Toddler Quality of Life Questionnaire (ITQOL) (Landgraf 1994);
Child Health Questionnaire (CHQ) (Landgraf 1996).
Parental stress, measured using a validated scale, for example: Parenting Stress Index (Abidin 1995).
-
Vestibular function:
balance;
co‐ordination.
Number of doctor‐diagnosed acute otitis media (AOM) episodes within a specified time frame.
These outcomes were identified as the most important in two studies that aimed to develop a core outcome set for children with OME (Bruce 2015; Liu 2020). As this review forms part of a suite of reviews of interventions for OME, not all outcomes will be relevant for all reviews.
Search methods for identification of studies
The Cochrane ENT Information Specialist conducted systematic searches for randomised controlled trials and controlled clinical trials. There were no language, publication year or publication status restrictions. We contacted original authors for clarification and further data if trial reports were unclear, and we arranged translations of papers where necessary. The date of the search was 20 January 2023.
Electronic searches
The Information Specialist searched:
the Cochrane ENT Register (searched via the Cochrane Register of Studies to 20 January 2023);
the Cochrane Central Register of Controlled Trials (CENTRAL 2023, Issue 1) (searched via the Cochrane Register of Studies to 20 January 2023);
Ovid MEDLINE(R) Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R) (1946 to 20 January 2023);
Ovid EMBASE (1974 to 20 January 2023);
Web of Science (1945 to 20 January 2023);
-
ClinicalTrials.gov, www.clinicaltrials.gov:
searched via the Cochrane Register of Studies to 20 January 2023;
searched via www.clinicaltrials.gov to 20 January 2023;
-
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP), https://apps.who.int/trialsearch/:
searched via the Cochrane Register of Studies to 20 January 2023;
searched via https://apps.who.int/trialsearch/ to 20 January 2023.
The Information Specialist modelled subject strategies for databases on the search strategy designed for CENTRAL. The search strategies were designed to identify all relevant studies for a suite of reviews on various interventions for OME. Where appropriate, they were combined with subject strategy adaptations of the highly sensitive search strategy designed by Cochrane for identifying randomised controlled trials and controlled clinical trials (as described in the Technical Supplement to Chapter 4 of the Cochrane Handbook for Systematic Reviews of Interventions version 6.1) (Lefebvre 2020). Search strategies for major databases including CENTRAL are provided in Appendix 1.
Searching other resources
We scanned the reference lists of identified publications for additional trials and contacted trial authors where necessary. The Information Specialist also ran non‐systematic searches of Google Scholar to retrieve grey literature and other sources of potential trials.
We did not perform a separate search for adverse effects. We considered adverse effects described in included studies only.
Data collection and analysis
Selection of studies
The Cochrane ENT Information Specialist used Cochrane's Screen4Me workflow to help assess the search results. Screen4Me comprises three components:
Known assessments – a service that matches records in the search results to records that have already been screened in Cochrane Crowd and been labelled as 'a RCT' or as 'not a RCT'.
The machine learning classifier (RCT model) (Wallace 2017), available in the Cochrane Register of Studies (CRS‐Web), which assigns a probability of being a true RCT (from 0 to 100) to each citation. Citations that are assigned a probability score below the cut‐point at a recall of 99% are assumed be non‐RCTs. For those that scored on or above the cut‐point we either manually dual screened these results or sent them to Cochrane Crowd for screening.
Cochrane Crowd is Cochrane's citizen science platform where the Crowd help to identify and describe health evidence. For more information about Screen4Me and the evaluations that have been done, please go to the Screen4Me website on the Cochrane Information Specialist's portal and see Marshall 2018; McDonald 2017; Noel‐Storr 2018; Thomas 2017.
Two review authors (KG, CM) independently screened the remaining titles and abstracts to identify potentially relevant studies. At least two review authors (of KG, SM, CM and KW) then independently evaluated the full text of each potentially relevant study to determine whether it met the inclusion/exclusion criteria for this review. Any differences were resolved by discussion and consensus, with the involvement of a third author where necessary.
Screening eligible studies for trustworthiness
Two review authors (of KG, CM, MR, KW) used the screening tool developed by Cochrane Pregnancy and Childbirth to assess the trustworthiness of the included studies. This tool includes specified criteria to identify studies that are considered sufficiently trustworthy to be included in the review (see Appendix 2). The process is outlined in Figure 1. We had planned to exclude studies from the main analysis if there were concerns when using this tool.
1.
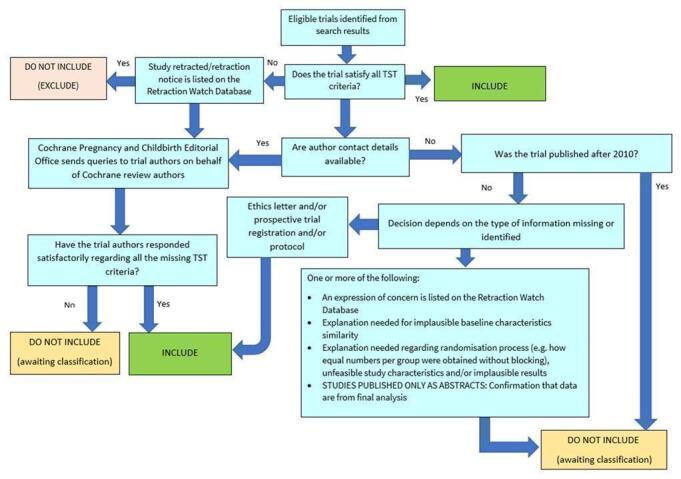
The Cochrane Pregnancy and Childbirth Trustworthiness Screening Tool
However, for this review we identified some concerns with many of the studies that were assessed as suitable for inclusion. Issues that arose included a lack of prospective trial registration for studies published after 2010 (Banigo 2016; Bidarian‐Moniri 2014; Scadding 2014), equal numbers allocated to the control and intervention groups without the use of blocked randomisation (Arick 2005; Banigo 2016; Ercan 2005; Stangerup 1992), and one study where the results on change in hearing were considered implausible (Arick 2005). In addition, some studies failed to describe the baseline characteristics of participants adequately, therefore we were unable to establish whether there was excessive similarity between the groups (Arick 2005; Brooker 1992; Ercan 2005; Stangerup 1992). Only three of the included studies had no concerns when using this tool: Chan 1989, Williamson 2015a and Williamson 2015b.
We attempted to clarify these issues with the authors, where possible, but were not able to obtain additional information. However, we are uncertain whether the concerns highlighted by the trustworthiness tool represent genuine issues with the reliability of the data, or whether the tool may be highly sensitive to trial features that may or may not represent untrustworthy data. We note that this tool, and other tools used for the same purpose, have not yet been validated for use.
We therefore took the decision to include all of these studies in the main analyses for this review. We have undertaken a sensitivity analysis where relevant, to exclude studies that failed to meet the criteria for this tool.
Data extraction and management
At least two review authors (of KG, CM, MR, KW) independently extracted outcome data from each study using a standardised data collection form. Where a study had more than one publication, we retrieved all publications to ensure complete extraction of data. Any discrepancies in the data extracted by the two authors were checked against the original reports, and differences were resolved through discussion and consensus, with recourse to a third author where necessary. If required, we contacted the study authors for clarification. We included key characteristics of the studies, such as the study design, setting, sample size, population and the methods for defining or collecting outcome data in the studies.
We extracted data on study findings according to treatment assignment, irrespective of whether study participants complied with treatment or received the treatment to which they were randomised.
In addition to extracting pre‐specified information about study characteristics and aspects of methodology relevant to risk of bias, we extracted the following summary statistics for each study and outcome:
For continuous data: the mean values, standard deviation and number of patients for each treatment group at the different time points for outcome measurement. Where endpoint data were not available, we extracted the values for change‐from‐baseline data instead. If values for the individual treatment groups were not reported, where possible we extracted summary statistics (e.g. mean difference) from the studies.
For binary data: we extracted information on the number of participants experiencing an event, and the number of participants assessed at that time point. If values for the individual treatment groups were not reported, where possible we extracted summary statistics (e.g. risk ratio) from the studies.
For ordinal scale data: we did not include any data from an ordinal scale in this review.
We pre‐specified time points of interest for the outcomes in this review. Where studies reported data at multiple time points, we took the longest available follow‐up point within each of the specific time frames. For example, if a study reported an outcome at 4 months, 8 months and 12 months of follow‐up then we included the 12‐month data for the time point > 3 months to ≤ 1 year. For adverse events, it was anticipated that some studies may report frequency data for events and it may not be possible to determine whether these events occurred in one patient on one occasion or more than one occasion. In such circumstances we reported the data narratively.
Assessment of risk of bias in included studies
At least two authors (of KG, CM, MR, KW) undertook assessment of the risk of bias of the included studies independently, with the following taken into consideration, as guided by the Cochrane Handbook for Systematic Reviews of Interventions (Handbook 2011):
sequence generation;
allocation concealment;
blinding;
incomplete outcome data;
selective outcome reporting; and
other sources of bias.
We used the Cochrane risk of bias tool in RevMan 5.3 (RevMan 2014), which involves describing each of these domains as reported in the study and then assigning a judgement about the adequacy of each entry: 'low', 'high' or 'unclear' risk of bias.
Measures of treatment effect
We summarised dichotomous data, such as presence of OME, as risk ratios (RR) and 95% confidence intervals (CI) and we summarised continuous data as a mean difference (MD) and 95% CI. For the outcomes presented in the summary of findings tables, we provide both the relative and absolute measures of effect.
Unit of analysis issues
We planned to include studies that randomised by participant or by cluster, but no cluster‐randomised studies were identified as part of this review. We did include cross‐over studies, but used data from the first phase of the trial only, prior to cross‐over.
For this review we anticipated that the unit of analysis would be the child. However, some studies reported findings by ear and therefore we have used both the child and ear as the unit of analysis.
All studies randomised participants to autoinflation or no treatment (watchful waiting) at the level of the child ‐ as this is an intervention that affects both ears. Some studies in this review included children with bilateral OME ‐ either exclusively (Bidarian‐Moniri 2014; Blanshard 1993), or as a proportion of included participants (Arick 2005; Brooker 1992; Chan 1989; Ercan 2005; Stangerup 1992; Williamson 2015a). This gave rise to a number of issues regarding the unit of analysis, as some studies reported outcomes (particularly the persistence of OME) for each ear.
We considered that outcomes for ears within the same individual were likely to be correlated ‐ for example, if a child had resolution of OME in one ear, they may be more likely to experience resolution in the contralateral ear. There is not complete independence between ears of the same individual. Standard meta‐analysis techniques assume that all data are independent. Therefore inclusion of the raw data (for the number of ears) is likely to overestimate the precision of any effect, and result in an excessively narrow confidence interval.
To account for this correlation, we used the suggested methods in the Cochrane Handbook for Systematic Reviews of Interventions (Handbook 2011), which are more commonly employed in the analysis of cluster‐randomised trials. We treated individuals who contributed two ears to the analysis (all of those with bilateral disease) as a 'cluster' of two data points. We then attempted to account for the correlation in these clusters, by assuming a certain correlation between ears of the same individual. We could not identify a figure for this correlation in the published literature, so we used an estimated correlation of 0.5 in the main analysis, but conducted sensitivity analyses using correlations of 0 and 1, to test the limits of this assumption. We then reduced the effective size of the trials by the 'design effect' ‐ which accounts for correlation between ears, and the average cluster size (which would be 2 for trials where all children had bilateral disease, and less than 2 if trials included a mixture of children with bilateral and unilateral disease).
Some trials also reported data both as a 'per ear' analysis, and as a 'per child' analysis ‐ where persistence was regarded as the presence of OME in either at least one ear, or all affected ears for children with bilateral disease. Where possible, we included these data as part of a sensitivity analysis, to assess whether the overall results were substantially altered.
Dealing with missing data
We attempted to contact study authors by email where data on an outcome of interest to the review were not reported but the methods described in the paper suggest that the outcome was assessed, or if not all data required for meta‐analysis were reported.
Assessment of heterogeneity
We assessed clinical heterogeneity by examining the included studies for potential differences between them in the types of participants recruited, interventions or controls used, and the outcomes measured. We assessed statistical heterogeneity by considering both the I² statistic, which calculates the percentage of variability that is due to heterogeneity rather than chance (with values over 50% suggesting substantial heterogeneity), and the P value from the Chi² test (Higgins 2021).
Assessment of reporting biases
We assessed reporting bias as within‐study outcome reporting bias and between‐study publication bias.
Outcome reporting bias (within‐study reporting bias)
We assessed within‐study reporting bias by comparing the outcomes reported in the published report against the study protocol or trial registry, whenever this could be obtained. If the protocol or trial registry entry was not available, we compared the outcomes reported to those listed in the methods section. If results are mentioned but not reported adequately in a way that allows analysis (e.g. the report only mentions whether the results were statistically significant or not), bias in a meta‐analysis is likely to occur. We then sought further information from the study authors. If no further information could be found, we noted this as being a 'high' risk of bias when the risk of bias tool was used. If there was insufficient information to judge the risk of bias we noted this as an 'unclear' risk of bias (Handbook 2011).
Publication bias (between‐study reporting bias)
If we were able to pool 10 or more studies in a single analysis, we planned to produce a funnel plot to explore possible publication biases. We planned to test for asymmetry using Egger's test (Egger 1997). However, we did not perform this test due to the paucity of data available for meta‐analysis.
Data synthesis
Where two or more studies reported the same outcome we performed a meta‐analysis using Review Manager 5 (RevMan 2014). We reported pooled effect measures for dichotomous outcomes as a risk ratio (RR) using the Mantel‐Haenszel methods. For continuous outcomes measured using the same scales we reported the mean difference (MD). We used a random‐effects model.
Where it was not possible to pool the findings from studies in a meta‐analysis, we present the results of each study and provide a narrative synthesis of findings.
Subgroup analysis and investigation of heterogeneity
We proposed the following subgroup analyses if sufficient data were available in study reports:
children with mild hearing loss versus moderate or worse;
children with allergy versus those without (using the trialists own definition);
children aged six years and younger versus children older than six years;
different types of autoinflation device;
children with previous ventilation tubes versus those without ventilation tubes;
children with cleft palate versus children without;
children with Down syndrome versus children without.
However, we did not find any data suitable for conducting these subgroup analyses. No studies provided subgroup data for children with different features (for example, for those with mild hearing loss, compared to those with moderate or worse hearing loss). Many of the trials did not provide sufficient background information (for example, on hearing level) for us to conduct subgroup analysis at the level of the individual study. Where data were provided, trials often recruited a mixed population that encompassed all subgroups (for example, most trials recruited children aged 3 to 10 years, not specifically children aged ≤ 6 years, or older than 6 years).
We did have information on the different types of autoinflation device used in the trials. However, as many studies included custom‐made devices, we were unable to group these in a meaningful way to compare devices in a subgroup analysis. Therefore we took the decision to present only the summary effect.
Sensitivity analysis
We planned to carry out the following sensitivity analyses to assess whether our findings were robust to decisions made regarding analyses and inclusion of studies:
Impact of model chosen: we compared the results using a random‐effects versus a fixed‐effect model.
Inclusion of studies at high risk of bias: we planned to compare the results including all studies versus excluding studies at overall high risk of bias, that is four or more of the seven domains of bias are rated as high risk (see Assessment of risk of bias in included studies). However, no study was rated at high risk of bias for four or more domains, therefore we did not conduct this analysis.
Exclusion of studies with concerns over trustworthiness, as assessed by the Trustworthiness Screening Tool (Figure 1).
Summary of findings and assessment of the certainty of the evidence
At least two authors (KG, CM, KW) independently used the GRADE approach to rate the overall certainty of evidence using GRADEpro GDT (gradepro.org/). The certainty of evidence reflects the extent to which we are confident that an estimate of effect is correct, and we have applied this in the interpretation of results. There are four possible ratings: high, moderate, low and very low. A rating of high certainty of evidence implies that we are confident in our estimate of effect and that further research is very unlikely to change our confidence in the estimate of effect. A rating of very low certainty implies that any estimate of effect obtained is very uncertain.
The GRADE approach rates evidence from RCTs that do not have serious limitations as high certainty. However, several factors can lead to the downgrading of the evidence to moderate, low or very low. The degree of downgrading is determined by the seriousness of these factors:
study limitations (risk of bias);
inconsistency;
indirectness of evidence;
imprecision; and
publication bias.
We include a summary of findings table, constructed according to the recommendations described in Chapter 10 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2021), for the following comparison(s):
autoinflation versus watchful waiting;
autoinflation versus non‐surgical treatment;
autoinflation versus ventilation tubes.
We include the following outcomes in the summary of findings table:
hearing;
disease‐specific quality of life;
adverse events ‐ pain and distress caused by the procedure (otalgia);
presence/persistence of OME.
We prioritised data from the longest available time point for presentation in the summary of findings tables.
Results
Description of studies
Results of the search
The searches (September 2021 and January 2023) retrieved a total of 7441 records. This reduced to 4157 after the removal of duplicates. The Cochrane ENT Information Specialist sent all 4157 records to the Screen4Me workflow. The Screen4Me workflow identified 84 records as having previously been assessed: 50 had been rejected as not RCTs and 34 had been assessed as possible RCTs. The remaining 4073 references were sent to the RCT classifier, which rejected an additional 1514 records as not RCTs (with 99% sensitivity). The Cochrane Crowd assessed 2443 of the remaining references, rejecting 1313 as not RCTs and identifying 1130 as possible RCTs. Following this process, the Screen4Me workflow had rejected 2877 records and identified 1280 possible RCTs for title and abstract screening (see Table 2).
1. RCTs identified through Cochrane Crowd and the RCT classifier.
| Possible RCTs | Rejected | |
| Known assessments | 34 | 50 |
| RCT classifier | 2559 | 1514 |
| Cochrane Crowd | 1130 | 1313 |
| Total | 1280 | 2877 |
RCT: randomised controlled trial
We identified 76 additional duplicates. We screened the titles and abstracts of the remaining 1204 records. We discarded 886 records and assessed 318 full‐text records. We subsequently discarded an additional 266 records and identified an additional five duplicates.
We excluded 25 records with reasons recorded in the review (see Excluded studies and Characteristics of excluded studies).
We included 11 studies (15 records) where results were available (Arick 2005; Banigo 2016; Bidarian‐Moniri 2014; Blanshard 1993; Brooker 1992; Chan 1989; Ercan 2005; Scadding 2014; Stangerup 1992; Williamson 2015a; Williamson 2015b). See Characteristics of included studies.
We identified five ongoing studies (six records). See Characteristics of ongoing studies for further details of these studies.
One study is awaiting classification as we were unable to obtain the full text for assessment (Tawfik 2002).
A flow chart of study retrieval and selection is provided in Figure 2.
2.

Included studies
We included 11 completed RCTs (Arick 2005; Banigo 2016; Bidarian‐Moniri 2014; Blanshard 1993; Brooker 1992; Chan 1989; Ercan 2005; Scadding 2014; Stangerup 1992; Williamson 2015a; Williamson 2015b). One RCT, Williamson 2015b, was a pilot trial for another included RCT (Williamson 2015a).
A summary of key participant characteristics, interventions, outcomes measured and follow‐up time is provided in Table 3.
2. Key characteristics of studies and participants.
| Study | Participants and ears randomised (N) | Autoinflation method | Age (years) and whether unilateral or bilateral (if stated) | Outcomes assessed by study | Final follow‐up |
| Arick 2005 | 94 174 ears |
Modified Politzer device, used twice daily for 7 weeks | 4 to 11 Minimum 2‐month history of middle ear effusion |
|
11 weeks |
| Banigo 2016 | 30 | EarPopper device, used twice daily for 7 weeks | 4 to 11 3‐month history of persistent OME |
|
7 weeks |
| Bidarian‐Moniri 2014 | 45 | New autoinflation device consisting of an inflatable facemask, a T‐shaped junction tube connecting at one end to the facemask, another end to a balloon and the third end to a handheld pump covered by a teddy bear to improve compliance Used twice daily for 4 weeks |
2 to 8 All bilateral Persistent OME with a duration of at least 3 months |
|
4 weeks (Additional data at 1‐year follow‐up, but not relevant for this review) |
| Blanshard 1993 | 85 | Otovent device, used 3 times daily for 3 months | 3 to 10 Bilateral Confirmation of type B or C2 tympanograms on 2 occasions separated by ≥ 3 months |
|
3 months |
| Brooker 1992 | 40 78 ears |
Device comprised of a toy balloon attached to a carnival blower mouthpiece; used 3 times daily for 3 weeks | < 10 years Unilateral or bilateral |
|
3 weeks |
| Chan 1989 | 41 | Modified Valsalva techniques ‐ a disposable anaesthesia mask attached to a floating ball‐type flowmeter. Child instructed to exhale through the nose through the mask (with mouth closed), as the pressure increased the ball in the flowmeter was propelled upwards. Used 3 times daily for 2 weeks. | 3 to 18 Unilateral or bilateral Aimed to include those that had persistence for ≥ 3 months (although this was not everyone) |
|
2 weeks |
| Ercan 2005 | 60 93 ears |
Otovent, used 3 times daily for 6 weeks | Unilateral and bilateral Chronic OME for 3 months |
|
3 months |
| Scadding 2014 | 200 | Otovent, used 3 times daily for 4 to 5 weeks | 4 to 8 With ≥ 3 months of glue ear or > 2 episodes in the past 6 months |
|
2 years |
| Stangerup 1992 | 100 | Tube designed by the author, with a balloon on the end, inserted in one nostril and blown up whilst occluding the other. Used 3 times daily for 2 to 4 weeks. | 3 to 10 Unilateral and bilateral Secretory OM for ≥ 3 months |
|
3 months |
| Williamson 2015a | 320 | Otovent, used 3 times daily for between 1 and 3 months | 4 to 11 Unilateral and bilateral Parental concern with report of ≥ 1 relevant symptom/concern associated with OME in previous 3 months |
|
3 months |
| Williamson 2015b | 21 | Otovent, used 3 times daily for between 1 and 3 months | 4 to 11 Unilateral and bilateral Parental concern with report of ≥ 1 relevant symptom/concern associated with OME in previous 3 months |
|
3 months |
OME: otitis media with effusion; RTI: respiratory tract infection; SD: standard deviation; URTI: upper respiratory tract infection
Study design
All included trials were RCTs; one was a cross‐over trial so we only used data from the first stage of the trial, prior to cross‐over (Bidarian‐Moniri 2014). While all studies recruited children, eight presented some findings by ear (Arick 2005; Bidarian‐Moniri 2014; Blanshard 1993; Brooker 1992; Chan 1989; Ercan 2005; Stangerup 1992; Williamson 2015a). The majority of studies followed participants for three months. The shortest follow‐up time was two weeks (Chan 1989) and the longest was two years (Scadding 2014).
Participants
A total of 1036 participants were included. The majority of studies aimed to recruit children aged approximately 3 to 11 years old. Chan 1989 recruited children up to the age of 18 years, although most were aged three to six years. Most studies recruited children with at least a three‐month history of OME (Banigo 2016; Bidarian‐Moniri 2014; Blanshard 1993; Chan 1989; Scadding 2014; Stangerup 1992; Williamson 2015a; Williamson 2015b). Ercan 2005 recruited children with a four‐week history of OME, Arick 2005 recruited children with a two‐month history of OME, and Brooker 1992 did not report the duration of OME. Some studies included children with bilateral disease, whilst others recruited participants with either bilateral or unilateral OME.
Interventions and comparisons
We identified studies that assessed two of our three comparisons of interest.
Comparison 1: autoinflation versus no treatment (watchful waiting)
Eleven completed RCTs assessed this comparison:
Arick 2005 (94 participants, 174 ears)
Banigo 2016 (30 participants)
Bidarian‐Moniri 2014 (45 participants)
Blanshard 1993 (85 participants)
Brooker 1992 (40 participants, 78 ears)
Chan 1989 (41 participants)
Ercan 2005 (60 participants, 93 ears)
Scadding 2014 (200 participants)
Stangerup 1992 (100 participants)
Williamson 2015a (320 participants)
Williamson 2015b (21 participants)
All provided data we could use in this review except for Scadding 2014, which did not provide data for any of our outcomes of interest.
Of these 11 trials, five used an Otovent as the autoinflation intervention (Blanshard 1993; Ercan 2005; Scadding 2014; Williamson 2015a; Williamson 2015b), one used an EarPopper (Banigo 2016), and one used a modified Politzer device (Arick 2005). Three trials used devices designed by the trial authors (Bidarian‐Moniri 2014; Brooker 1992; Stangerup 1992) and one used a modified Valsalva technique (Chan 1989).
In nine trials, the comparison group received no treatment (Arick 2005; Banigo 2016; Bidarian‐Moniri 2014; Blanshard 1993; Brooker 1992; Chan 1989; Stangerup 1992; Williamson 2015a; Williamson 2015b). In one trial, both the intervention and control group were treated with nasal saline irrigation three times a day for six weeks (Ercan 2005), and in the trial Scadding 2014 there were four treatment arms including autoinflation, autoinflation and nasal steroids, nasal steroids and placebo.
Three ongoing studies are investigating this comparison but provide no usable data for this current review (INFLATE (ACTRN12617001652369); NCT00393159; NCT05324696). INFLATE (ACTRN12617001652369) uses Otovent as the intervention and the comparison is usual care, while NCT02038400 uses EarPopper and the comparison is no treatment. NCT05324696 uses a custom‐made device (based on the one used by Bidarian‐Moniri 2014), and will compare this to the use of a sham device.
Comparison 2: autoinflation versus ventilation tubes
Two ongoing studies will assess this comparison but do not provide any data we could use (NCT02038400; NCT02546518). For one trial, autoinflation is achieved using a Kinetube, and the other will use a custom‐made device, similar to that used by Bidarian‐Moniri 2014.
Outcomes
Hearing
Assessment of hearing varied across the studies. Two studies considered the proportion of children whose hearing returned to normal. Normal hearing was defined in one study as a hearing threshold of < 20 dB HL (Bidarian‐Moniri 2014), and simply stated as 'normal hearing' with no definition by Arick 2005. Three other studies measured the mean hearing level using pure tone audiometry and reported this as a pure tone average, or as separate values for the different frequencies.
Three studies provided some data related to hearing, which we could not use in our analyses. Banigo 2016 reported on the number of children who were no longer listed for ventilation tube insertion, as their hearing had improved, and they failed to meet the criteria for ventilation tube insertion. However, the threshold used for this appeared to be a hearing threshold of < 25 dB HL, which may not be regarded as 'normal hearing'. In addition, other factors were taken into account when assessing whether ventilation tubes should be fitted. Therefore we considered that these data could not be used as a surrogate measure for 'children with normal hearing'. Brooker 1992 reported on the number of children with improvement in hearing (10 dB HL in the pure tone audiogram frequencies from 250 Hz to 2000 Hz) and who developed a peak in a previously flat tympanogram. As this only considers 'improvement', these data will not include all children with normal hearing at the end of follow‐up, therefore they were not included. Scadding 2014 reported a composite outcome of the proportion of children who had persistent hearing loss ≥ 30 dB HL, or grommet insertion, by the time of follow‐up.
Disease‐specific health‐related quality of life
This was reported by only one of the included studies, using the Otitis Media Questionnaire‐14 (OMQ‐14) (Williamson 2015a).
Pain and distress at the time of the procedure
This broad outcome measure was not reported by any of the included studies. However, we considered that 'otalgia' should be viewed as part of this outcome measure. One study did report on the presence of otalgia in both groups (Williamson 2015a).
Presence/persistence of OME
Trial authors often described "resolution" of OME (rather than persistence), and this was frequently assessed by tympanometry. For example, Williamson 2015a defined resolution of OME as "a change from at least one type B (fluid) to A/C1 (clear) tympanogram". Where studies reported resolution we took the inverse data to assess presence or persistence of OME.
Adverse events
Five studies reported some information regarding adverse events (Banigo 2016; Bidarian‐Moniri 2014; Chan 1989; Scadding 2014; Williamson 2015a).
Compliance
A number of studies gave a narrative report of the levels of compliance with the intervention.
Receptive language skills
Williamson 2015a was the only included study to assess developmental outcomes, in this case receptive language skills. However, due to problems with the website‐based assessment and late ethics permission, insufficient numbers of children completed this follow‐up test, and the data were not reported.
Number of doctor‐diagnosed episodes of acute otitis media
Four studies provided some information for this outcome, over different durations of follow‐up.
Our other outcomes of interest were not reported by any of the included studies. This included speech development, cognitive development, psychosocial outcomes, listening skills, generic health‐related quality of life, parental stress and vestibular function.
Excluded studies
We excluded 25 studies from this review for the following reasons:
Eleven studies were not randomised controlled trials (Bidarian‐Moniri 2016; Gibson 1996; Head 1992; Iino 1989; Li 2021; Paradise 1997; Parlea 2012; Shubich 1996; Silman 2005; Stenstrom 2005; Tham 2018).
Two studies included an incorrect population ‐ one included adult participants and one included children with recurrent acute otitis media, not OME (Ferrara 2005; Li 2020).
Ten studies considered an intervention that was not relevant for this review (Ardehali 2008; ChiCTR2000035008; Choung 2008; De Nobili 2008; El Hachem 2012; Endo 1997; Heaf 1991; Marchisio 1998; Rohail 2006; Starcevic 2011). Some of these studies are included in other reviews in this suite.
One study included an incorrect comparison. Autoinflation was used before and after adenoidectomy, and compared to adenoidectomy alone (Leunig 1995).
Finally, one study was withdrawn before any data were available (NCT03534219).
Risk of bias in included studies
The risk of bias in the included studies shows a mixed picture of low, unclear and high‐risk ratings. See Figure 3 for the risk of bias graph (our judgements about each risk of bias item presented as percentages across all included studies) and Figure 4 for the risk of bias summary (our judgements about each risk of bias item for each included study).
3.

Risk of bias graph (our judgements about each risk of bias item presented as percentages across all included studies).
4.

Risk of bias summary (our judgements about each risk of bias item for each included study).
Allocation
We rated seven of the studies at low risk of bias when assessing random sequence generation (Banigo 2016; Bidarian‐Moniri 2014; Blanshard 1993; Chan 1989; Scadding 2014; Williamson 2015a; Williamson 2015b), but we rated the risk as unclear for the remaining five studies. We rated only three studies at low risk of bias for allocation concealment (Scadding 2014; Williamson 2015a; Williamson 2015b); we rated the remaining six at unclear risk, due to insufficient information.
Blinding
We rated all 11 studies to be at high risk of performance bias as it was not possible to blind study participants and personnel to treatment group.
We rated six studies at high risk of detection bias (Blanshard 1993; Brooker 1992; Chan 1989; Ercan 2005; Scadding 2014; Stangerup 1992). These studies did not state that outcome assessors were blinded, therefore we considered that it is unlikely that they were. We rated Arick 2005 as unclear and the remaining studies as at low risk of detection bias.
Incomplete outcome data
We rated eight studies at low risk of attrition bias. We rated Scadding 2014 and Stangerup 1992 as high risk. Scadding 2014 reported an attrition rate of 38% and Stangerup 1992 reported many results as a 'per protocol' analysis ‐ only for those who successfully carried out autoinflation. We rated Williamson 2015a at unclear risk of attrition bias: although loss to follow‐up was similar across the groups, sensitivity analyses from the main publication indicated that imputation for missing data resulted in a loss of the significant difference between the two groups for some outcome measures.
Selective reporting
We rated two studies at low risk of reporting bias as we found a published protocol for the trials (Williamson 2015a; Williamson 2015b). We rated the remaining nine trials at unclear risk of reporting bias as we could not locate protocols for these trials.
Other potential sources of bias
We rated seven trials at low risk of other bias. We rated Banigo 2016, Bidarian‐Moniri 2014, Brooker 1992 and Chan 1989 at unclear risk of other bias due to a short follow‐up period that did not allow sufficient time for changes in the control (no treatment) groups.
Effects of interventions
See: Table 1
Comparison 1: Autoinflation versus no treatment
See Table 1 for details of the primary outcome measures.
Hearing
Proportion of children whose hearing is normal
Very short‐term follow‐up (< 6 weeks)
One study provided data for this outcome (Bidarian‐Moniri 2014). As Bidarian‐Moniri 2014 reported this outcome by ear, we adjusted the data using a correlation coefficient of 0.5, to account for correlation between ears of the same participant. The mean difference in the likelihood of achieving a hearing threshold of < 20 dB HL using autoinflation was 4.45 (95% confidence interval (CI) 2.14 to 9.27; 86% versus 19%; 1 study, 45 participants; Analysis 1.1; very low‐certainty evidence). Sensitivity analyses using different correlation coefficients of either 1 (Analysis 1.10) or 0 (Analysis 1.11) produced little change in the findings.
1.1. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 1: Proportion of children whose hearing is normal (very short‐term, < 6 weeks)
1.10. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 10: Sensitivity analysis: Proportion of children whose hearing is normal (very short‐term, < 6 weeks). Per ear data (ICC of 1, complete correlation between ears)
1.11. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 11: Sensitivity analysis: Proportion of children whose hearing is normal (very short‐term, < 6 weeks). Per ear data (ICC of 0, no correlation between ears)
Short‐term follow‐up (6 weeks to 3 months)
Arick 2005 provided data for this outcome (Analysis 1.2). Arick 2005 used a modified Politzer method for autoinflation and reported a risk ratio of 2.67 for the return to normal hearing (in at least one ear) in those who received autoinflation (95% CI 1.73 to 4.12; 85% versus 32%; 1 study, 94 participants; Analysis 1.2; very low‐certainty evidence).
1.2. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 2: Proportion of children whose hearing is normal (short‐term, > 6 weeks to ≤ 3 months)
Medium‐term follow‐up (> 3 months to ≤ 1 year)
This outcome was not assessed at this time point by any of the included studies.
Hearing threshold
Very short‐term follow‐up (< 6 weeks)
A single study reported this outcome at this time point. The change from baseline in average pure‐tone air conduction threshold was estimated to be ‐5.00 dB HL lower in those who received autoinflation compared to those who received no intervention (95% CI ‐10.1 to 0.1; 1 study, 45 participants; Analysis 1.3; very low‐certainty evidence). These data were reported in the original text with a mean value, median value and full range, therefore we used the reported mean values, and estimated the standard deviation using the methods given by Wan 2014.
1.3. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 3: Hearing threshold (very short‐term, < 6 weeks)
Short‐term follow‐up (6 weeks to 3 months)
Two studies reported this outcome. Data in both studies were reported separately for four different frequencies. We were unable to pool these data (and estimate the pure tone average) due to insufficient information regarding the correlation between hearing at different frequencies. Therefore, we have presented the data separately for the four frequencies assessed. At each frequency the direction of effect was in favour of autoinflation (mean differences between groups ranging from ‐9.04 to ‐12.88 dB HL, 95% CI ranging from ‐2.83 to ‐17.85; 2 studies, 113 participants; I2 from 0% to 57%; Analysis 1.4; low‐certainty evidence). One study reported data separately for the left and right ear. We used data from the right ears for the main analysis, but sensitivity analysis showed little difference when using data from the left ears (Analysis 1.13).
1.4. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 4: Hearing threshold (short‐term, > 6 weeks to ≤ 3 months)
1.13. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 13: Sensitivity analysis: Hearing threshold (short‐term, > 6 weeks to ≤ 3 months). Left ear data
Additional data were reported by Blanshard 1993. After three months of follow‐up, the mean change in hearing threshold (as assessed with pure tone audiometry) was reported for those who had high adherence with the use of Otovent, those with low adherence and those in the control group. The mean change overall for the Otovent group (38 ears) was an increase (worsening) of hearing threshold by 0.98 dB HL, although outcomes were better for those with high adherence (an improvement of ‐2.13 dB HL in 19 ears) than those with low adherence (a worsening of 4.08 dB HL in 19 ears). This compared to a worsening of 0.52 dB HL in the control group (34 ears). As no standard deviations were reported, we were unable to include these data in the meta‐analysis, although they are suggestive of a trivial difference between the groups.
Disease‐specific quality of life
Short‐term follow‐up
A single study reported this outcome (Williamson 2015a). The authors used a standardised version of the OMQ‐14, measured with a 14‐item scale. Total raw scores are then converted using a weighted scoring system into a standardised score. The range of this score is not explicit, but appears to be between approximately ‐3 and +3, with lower scores reflecting better quality of life. The mean difference was adjusted for potential confounders, including sex, age, centre (primary care trust), baseline values and baseline severity of disease. The adjusted mean difference was ‐0.42 for those who received autoinflation (95% CI ‐0.62 to ‐0.22; 1 study, 247 participants; Analysis 1.5; low‐certainty evidence). The authors report that a change of 0.3 on this scale would be regarded as clinically meaningful, indicating that this would represent a moderate improvement in quality of life.
1.5. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 5: Disease‐specific quality of life (short‐term, > 6 weeks to ≤ 3 months)
Pain and distress at the time of the procedure
This broad outcome measure was not reported by any of the included studies. However, one study did report specifically on otalgia, and the results of this analysis are presented here.
Otalgia
A single study reported on otalgia as a complication of treatment. No definition of otalgia was given. The risk ratio was 3.50 for those who carried out autoinflation (95% CI 0.74 to 16.59; absolute risk 7/160 participants in the autoinflation group, compared to 2/160 in the no treatment group; 1 study, 320 participants; Analysis 1.6; very low‐certainty evidence).
1.6. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 6: Adverse events ‐ pain and distress caused by the procedure (otalgia)
Persistence of OME
Please see Unit of analysis issues for further details on how these analyses were conducted.
Very short‐term follow‐up (< 6 weeks)
Seven studies reported this outcome at between two weeks and six weeks of follow‐up.
Overall, a risk ratio of 0.86 was found for the persistence of OME at < 6 weeks in children who received autoinflation (95% CI 0.72 to 1.04; 67% versus 78%; 7 studies, 688 participants; I2 = 74%; Analysis 1.7; very low‐certainty evidence). It should be noted that there is considerable inconsistency in this analysis, with one study appearing to favour no intervention, and two studies showing little difference between the two groups. As described above, most data were reported 'per ear', therefore to account for correlation between ears of the same individual we have carried out some adjustment of the data. Imputing different correlation coefficients, and the use of 'per child' rather than 'per ear' data where reported, made little difference to the overall result (Analysis 1.14; Analysis 1.15; Analysis 1.16).
1.7. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 7: Persistence of OME (very short‐term, < 6 weeks)
1.14. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 14: Sensitivity analysis: Persistence of OME (very short‐term, < 6 weeks). Per ear data (ICC of 0)
1.15. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 15: Sensitivity analysis: Persistence of OME (very short‐term, < 6 weeks). Per ear data (ICC of 1)
1.16. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 16: Sensitivity analysis: Persistence of OME (very short‐term, < 6 weeks). Per child data, where available
Short‐term follow‐up (> 6 weeks to ≤ 3 months)
Four studies also reported at this time point. The risk ratio of 0.88 was similar to that seen at earlier time points (95% CI 0.80 to 0.97; 65% versus 74%; 4 studies, 483 participants; I2 = 0%; Analysis 1.8; low‐certainty evidence). Again, adjustment using different correlation coefficients, or assessing 'per child' data made very little difference to the overall effect estimate (Analysis 1.17; Analysis 1.18; Analysis 1.19).
1.8. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 8: Persistence of OME (short‐term, > 6 weeks to ≤ 3 months)
1.17. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 17: Sensitivity analysis: Persistence of OME (short‐term, > 6 weeks to ≤ 3 months). Per ear data (ICC of 0)
1.18. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 18: Sensitivity analysis: Persistence of OME (short‐term, > 6 weeks to ≤ 3 months). Per ear data (ICC of 1)
1.19. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 19: Sensitivity analysis: Persistence of OME (short‐term, > 6 weeks to ≤ 3 months). Per child data, where available
The study Banigo 2016 also reported the number of children who "still had hearing loss and met the criteria set by NICE (including history, otoscopic examination, tympanometry and audiometry findings) so they had ventilation tubes inserted" after seven weeks of follow‐up. However, we considered that some children with a persistent effusion may not meet the criteria required for surgery, and would not be included, therefore this could not be used as a proxy for 'persistence of OME'.
Adverse events
Perforation of the tympanic membrane
This was not described in any of the studies. As described below, for some studies we are unsure if this is because no tympanic membrane perforations occurred, or because this outcome was not fully assessed or reported.
Other adverse events
Five studies provided very limited information on adverse events:
Banigo 2016 reported, "The most common complaint from the children in treatment group was ear discomfort and a blocked sensation in the ears immediately following its use, which was short‐lived and did not affect compliance".
Bidarian‐Moniri 2014 reported, "No adverse effects were observed".
Chan 1989 reported, "Of the 40 subjects who returned for the two‐week visit, none reported any untoward side effects related to performing autoinflation during the study period". It is not clear whether the side effects prioritised in this review were specifically assessed.
Scadding 2014 reported that no adverse events were seen in their trial. The authors state that "Minor adverse events were recorded, but none was of sufficient severity to cause cessation of the treatment or withdrawal from the trial. The commonest was minor epistaxis which occurred in fewer than 10% of subjects."
Williamson 2015b reported that one child experienced nosebleeds while using autoinflation. The parent reported that the child had suffered from previous recurrent nosebleeds, but chose to continue with the study anyway.
Six studies did not report any information on adverse events. It is not clear whether this was because no events occurred, or because they were not assessed or reported (Arick 2005; Blanshard 1993; Brooker 1992; Ercan 2005; Stangerup 1992; Williamson 2015a).
Compliance
Details on compliance of study participants with autoinflation are provided in Table 4. Overall, most trials that reported compliance seemed to rate this as satisfactory or good.
3. Compliance with autoinflation.
| Study | Treatment requirements | Compliance monitoring and definition | Age | Compliance |
| Arick 2005 | Twice a day, alternating nostrils with each treatment for 7 weeks | Daily log to track compliance | 4 to 11 years | Complete compliance in 46 of 47 experimental patients (97.9%), moderate compliance in remaining patient |
| Banigo 2016 | Use twice a day and on each occasion to be used twice in each nostril for 7 weeks | Diary card, no definition | Treatment Mean 5.94 years (range 4.36 to 8.19) Control Mean 5.55 (range 3.96 to 7.79) |
94% on average |
| Bidarian‐Moniri 2014 | Use the device twice a day to perform 20 inflations at each session (approximately 5 to 10 minutes) for 4 weeks | Diary and full compliance was defined as using the device twice a day to perform 20 inflations at each session (approximately 5 to 10 minutes) during a period of 4 weeks | Treatment: 68 months Control: 53 months |
All children from 2 years and 9 months of age were able to use the device after demonstration by a doctor or nurse. In one case, the compliance was not satisfactory to complete the 4‐week treatment. The overall compliance for the total treatment time was satisfactory. |
| Blanshard 1993 | One nostril 3 times a day | Compliance was measured as the number of times the device was used as a percentage of the maximum possible | Treatment HC (high compliance) n = 19 Mean 62.7 months (SD 17.5) LC (low compliance) n = 23 Mean 52.8 months (SD 8.9) Control n = 41 Mean 59.9 months (SD 18.3) |
Of 42 children in the treatment group, 19 (45%) used it as prescribed (> 70%), 18 (43%) used it irregularly and 5 (12%) were unable to use it at all. Treatment group was divided into those with a high compliance (HC) of greater than 70%, (n = 19) and those with a low compliance (LC) of < 70% (n = 23). In the LC group compliance deteriorated from 45% to 29% over the course of the treatment. See table 1 in Blanshard 1993 for further information |
| Brooker 1992 | Inflate balloon nasally 3 times a day for 3 weeks | No information on compliance | Age 3 to 10 years, mean 5.7 | No information on compliance |
| Chan 1989 | 3 times daily for 2 weeks | Participants stratified according to their ability of tubal opening during autoinflation Parents asked to record number of exercise cycles completed each day and to hand in a score card at the end of the 2‐week study as a method to monitor patient compliance Ability to autoinflate Autoinflation No 4 (21.1) Yes 15 (78.9) Control No 5 (22.7) Yes 17 (77.3) |
Age between 3 and 18 years of age Autoinflation 3 to 6 years: 14 (73.6) 7 to 11 years: 4 (21.1) > 12 years: 1 (5.3) Control 3 to 6 years: 13 (59.1) 7 to 11 years: 7 (31.8) > 12 years: 2 (9.2) |
No further details on compliance |
| Ercan 2005 | Autoinflation 3 times a day for 6 weeks | — | Mean age 6.2 years (range 4 to 10 years) | “The compliance of the children to the autoinflation was satisfactory and the autoinflation was somehow amusing for the children” |
| Scadding 2014 | Otovent 3 times daily for approximately 4 to 5 weeks | Compliance assessed by questioning child and parent/guardian and by number of bottles used. Those who reported spray use on at least 3 days a week remained in the study. | Aged between 4 and 8 years Treatment 5.7 (SD 1.3) Placebo 5.7 years (SD 1.3) |
Those who reported spray use on at least 3 days a week remained in the study |
| Stangerup 1992 | 3 times a day for 2 weeks | At second visit the use of the nose balloon was scored: 0 not used, 1 used a few times, 2 used as prescribed | Aged 3 to 10 years “some children younger than 3 years of age had difficulty performing autoinflation” Median age 5.3 years |
3 children had not performed autoinflation, 10 only once, 33 had followed instructions |
| Williamson 2015a | Otovent 3 times per day for 1 to 3 months | Weekly diary of compliance, sticker book | Autoinflation group: mean 5.4 years (SD 1.24) Control group: mean 5.4 years (SD 1.04) |
89% (116/130) used ‘most’ or ‘all of the time’ in the first month 80% in months 2 and 3 (68/85, 805) See table 22 in Williamson 2015a for more information |
| Williamson 2015b | Otovent 3 times per day for 1 to 3 months | Recorded using a daily sticker reward chart | Age: Autoinflation group: 4 to 5 years: 3 5 to 6 years: 4 6 to 10 years: 0 7 to 11 years: 2 Control group: 4 to 5 years: 2 5 to 6 years: 8 6 to 10 years: 0 7 to 11 years: 0 |
Compliance described as “excellent” and pilot study answered major unknown issue about “whether or not children were able to perform the technique and achieve sufficient compliance over 1 month in a primary care setting” See table 4 in Williamson 2015a for more information |
SD: standard deviation
Episodes of acute otitis media
Two studies assessed the occurrence of acute otitis media during short‐term follow‐up. The risk ratio was 0.82 for those who carried out autoinflation, although the confidence intervals were wide (95% CI 0.49 to 1.36; 2 studies, 403 participants; I2 = 0%; Analysis 1.9; very low‐certainty evidence).
1.9. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 9: Episodes of acute otitis media (short‐term, > 6 weeks to ≤ 3 months)
Two further studies reported this outcome. However, we were not able to include the data in the meta‐analysis:
Stangerup 1992 used a 'per protocol' analysis ‐ data were only reported for participants who regularly underwent autoinflation, not for the whole group of individuals who were allocated to autoinflation. Therefore, these data were not included in the review.
Banigo 2016 provided a narrative report, stating "There was no report of an acute otitis media during EarPopper use". No details are provided regarding whether any episodes occurred in the control group, therefore we were unable to provide an accurate comparison of the two groups.
See Table 5 for the results of the sensitivity analyses conducted as part of this review.
4. Sensitivity analyses.
| Outcome | Main analysis result | Sensitivity analysis | Sensitivity analysis result |
| 1.5.1 Hearing threshold (short‐term, > 6 weeks to ≤ 3 months): 0.5 kHz | MD ‐9.13 (‐15.14 to ‐3.13) | Fixed‐effect model | MD ‐10.17 (‐13.63 to ‐6.71) |
| 1.5.2 Hearing threshold (short‐term, > 6 weeks to ≤ 3 months): 1 kHz | MD ‐10.34 (‐17.85 to ‐2.83) | Fixed‐effect model | MD ‐11.77 (‐15.73 to ‐7.82) |
| 1.5.3 Hearing threshold (short‐term, > 6 weeks to ≤ 3 months): 2 kHz | MD ‐9.04 (‐14.84 to ‐3.25) | Fixed‐effect model | MD ‐9.85 (‐13.61 to ‐6.10) |
| 1.5.4 Hearing threshold (short‐term, > 6 weeks to ≤ 3 months): 4 kHz | MD ‐12.88 (‐17.01 to ‐8.75) | Fixed‐effect model | MD ‐12.88 (‐17.01 to ‐8.75) |
| 1.7 Persistence of OME (very short‐term, < 6 weeks) | RR 0.86 (0.72 to 1.04) | Fixed‐effect model | RR 0.83 (0.76 to 0.92) |
| 1.7 Persistence of OME (very short‐term, < 6 weeks) | RR 0.86 (0.72 to 1.04) | Excluding studies at high risk using the trustworthiness tool | RR 0.94 (0.81 to 1.09) |
| 1.8 Persistence of OME (short‐term, > 6 weeks to ≤ 3 months) | RR 0.88 (0.80 to 0.97) | Fixed‐effect model | RR 0.86 (0.77 to 0.97) |
| 1.8 Persistence of OME (short‐term, > 6 weeks to ≤ 3 months) | RR 0.88 (0.80 to 0.97) | Excluding studies at high risk using the trustworthiness tool | RR 0.88 (0.74 to 1.04) |
| 1.9 Episodes of acute otitis media (short‐term, > 6 weeks to ≤ 3 months) | RR 0.82 (0.49 to 1.36) | Fixed‐effect model | RR 0.85 (0.51 to 1.41) |
| 1.9 Episodes of acute otitis media (short‐term, > 6 weeks to ≤ 3 months) | RR 0.82 (0.49 to 1.36) | Excluding studies at high risk using the trustworthiness tool | RR 1.25 (0.34 to 4.57) |
MD: mean difference; OME: otitis media with effusion; RR: risk ratio
Numbers in brackets represent 95% confidence intervals.
Discussion
It should be noted that most of the studies included in this review lasted up to three months, and required children to perform autoinflation two to three times per day. Furthermore, outcomes were reported just after treatment had been completed. Therefore, we are uncertain whether any effects of autoinflation persist into the longer term. As we did not assess the proportion of children who went on to receive medical or surgical treatment for OME, we do not know whether the use of autoinflation has any impact on this. It may simply hasten recovery for children in whom OME would have resolved anyway.
Summary of main results
Short‐term effects (up to three months)
Overall, autoinflation may slightly increase the proportion of children whose hearing returns to normal at up to three months follow‐up, but the evidence was very uncertain. We are uncertain whether mean hearing threshold is an appropriate method of assessing hearing in this condition (see below). Nonetheless, at less than six weeks there appeared to be little difference in the mean hearing threshold between those who received autoinflation and no treatment, but the evidence was very uncertain. After six weeks to three months of follow‐up, autoinflation may result in a small improvement in hearing threshold. It may also result in an improvement in quality of life.
Autoinflation may also result in a reduction in the proportion of children with persistent OME at six weeks to three months of follow‐up, although the evidence at the earlier time point (less than six weeks) was very uncertain. After three months of follow‐up, there may be a very slight reduction in the proportion of children who experience acute otitis media, but the evidence was very uncertain. The evidence about ear pain was also very uncertain, but the occurrence of pain may increase with the use of autoinflation.
We did not identify any evidence on generic quality of life, expressive or receptive language skills, cognitive development, psychosocial outcomes, listening skills, parental stress or vestibular function.
Longer‐term effects (over three months)
We did not identify evidence for any outcomes over this time frame.
Overall completeness and applicability of evidence
Most of the studies included recruited children aged over three years. Autoinflation may be difficult for children in younger age groups to perform, therefore we considered that this was an appropriate population. However, it should be noted that few studies provide any evidence regarding the use of autoinflation in children aged less than three years.
We intended to include studies where children had craniofacial anomalies, or conditions such as Down syndrome. However, a number of studies specifically excluded children with these conditions (Bidarian‐Moniri 2014; Blanshard 1993; Chan 1989; Ercan 2005; Scadding 2014; Williamson 2015a; Williamson 2015b). The remaining studies did not state that children with these conditions were excluded, but none specifically recruited children with these high‐risk conditions. Therefore, we do not know whether the efficacy of autoinflation may differ for these children.
Many of the studies included in this review enrolled children who had OME for at least three months, however children with a shorter duration of disease were also included. It is not clear whether the efficacy of the intervention may vary depending on the duration of the disease, or perhaps according to prior treatment. Further information is required to identify whether this intervention may be more suitable for use in a primary care setting, as an early intervention for OME, or whether it is better suited to use in secondary care, for children with persistent or treatment‐resistant disease.
A variety of devices and techniques were used to carry out autoinflation, ranging from custom‐made devices to commercially available products such as Otovent. We did not have enough data to consider this as part of a subgroup analysis, so cannot say if one method works better than another.
The data obtained as part of this review on adherence to treatment were encouraging, showing moderate or good adherence when using autoinflation devices. However, we note that a substantial proportion of studies did not assess compliance. In addition, the studies that did provide an assessment of compliance used different measures to assess this. We are aware that compliance may differ in routine clinical practice, as compared to a trial setting. As highlighted in the review, autoinflation may be associated with an increase in ear pain, and the willingness of children to engage with the procedure may wane over time, which may impact on efficacy.
We have concerns that assessment of hearing using the mean difference in final hearing threshold (or mean change in hearing threshold) may not be the most appropriate way to assess hearing. OME has a high spontaneous resolution rate. Consequently, we would anticipate that the change in hearing threshold for most children will be similar across the groups – as many children will improve with or without treatment. Therefore, even if a subset of children had substantial benefit from the intervention, the overall mean difference between the two groups would appear to be small. When assessed using the mean difference, the marked benefit seen in a subgroup of participants is ‘diluted’ by the children who get better regardless of treatment. Therefore, an apparently small mean difference between the two groups may actually be consistent with a substantial change in the number of children in whom hearing returns to normal. It should be noted that persistence (or resolution) of OME is always expressed as a proportion. Most children included in these studies would be expected to have a return to normal hearing alongside resolution of OME. In the absence of our preferred outcome measure of proportion of children with return to normal hearing it may be that presence (and resolution) of OME provides a better or more useful estimate of effect on hearing in these studies.
Finally, we did not assess the number of children who received further treatment for OME (including medical or surgical interventions) as part of this review. Therefore, we do not have data to show whether this intervention prevents children from ultimately receiving surgery and ventilation tube insertion as a treatment for OME. However, this is likely to be an important consideration when deciding on a treatment strategy for OME.
Quality of the evidence
We rated the evidence included in this review as low‐ or very low‐certainty. This was due to a number of issues. Firstly, many of the outcomes were affected by the potential for bias in the individual studies. We rated all the studies at high risk of performance bias, as participants and study personnel were aware of the group allocation. Some studies also had additional problems, including detection bias (where outcome assessors were also aware of the group allocation for participants), loss to follow‐up or extremely short follow‐up times.
As well as the potential for bias, the effect estimates for many of the outcomes had confidence intervals that crossed from a threshold of potential benefit or harm to a trivial effect, leading to uncertainty in the overall effect estimates. For some analyses very few participants were included, which resulted in extremely wide confidence intervals and more uncertainty in the overall result.
Potential biases in the review process
As part of the development of this review we conducted comprehensive searches, and made significant efforts to locate and include all relevant studies on this topic. Not all of our outcomes of interest were reported by every study. If these outcome data were assessed but not reported, then there is a risk of bias in the meta‐analysis results.
We acknowledge that there is little consensus on the definition of 'normal hearing'. Consequently, our selection of a hearing threshold of ≤ 20 dB HL as 'normal' was based on discussion between the author team, review of earlier studies and a pragmatic choice of outcome measure. However, we were as inclusive as possible with this outcome measure, and have included data where authors provided an alternative definition of normal hearing. If we had rigidly used a definition of ≤ 20 dB HL then the data included in this review would have been even more sparse.
During the preparation of this review, we had to consider the definition of autoinflation. We originally included one study that utilised nose‐blowing as an autoinflation technique (Heaf 1991). However, in response to comments from our peer reviewers, we subsequently excluded this study from the review. Different definitions of 'autoinflation' could therefore lead to inclusion of different studies, and potentially impact on the findings of the review.
Agreements and disagreements with other studies or reviews
The previous Cochrane Review on this topic included eight studies, with a total of 702 participants (Perera 2013). The review authors concluded that autoinflation has a beneficial effect on resolution of OME. However, the authors noted that none of the included studies were rated as high quality, and many of the effect estimates had wide confidence intervals and failed to reach conventional statistical significance. This review differs slightly, as we have used the GRADE approach to formally assess the certainty of the evidence for each outcome. Given some concerns over the potential for bias in the included studies, and the imprecision in some effect estimates, the overall certainty of the evidence is therefore rated as low or very low. In addition, the outcome measures used for the original review and this updated review differ slightly. However, despite these differences, the summary of both reviews is similar ‐ that there may be some small benefit from autoinflation for some outcomes, but that longer follow‐up is required, including an assessment of quality of life and developmental outcomes.
Authors' conclusions
Implications for practice.
There may be some small benefit from the use of autoinflation for otitis media with effusion (OME) with regard to persistence of OME and quality of life, although whether this benefit persists in the long term is unclear. The evidence is uncertain regarding return to normal hearing and adverse events. We are also unable to identify whether one type of autoinflation device is more effective than another.
We did not look for evidence regarding the need for additional treatment in children with OME, and the data on longer‐term follow‐up were sparse. Therefore, we do not know whether the use of autoinflation has any impact on the requirement for medical treatment (such as antibiotics or steroids), or any effect on the number of children who require surgery for OME.
Implications for research.
We identified a number of trials in this area, including a total of 1036 participants. Nonetheless, the evidence available for this intervention remains low‐ or very low‐certainty. Further consideration should be given to which children may be most likely to benefit from this intervention before embarking on large‐scale trials. This review forms part of a suite of five reviews, which consider interventions for OME (Galbraith 2022; MacKeith 2022a; MacKeith 2022b; Mulvaney 2022a; Mulvaney 2022b). Here we present implications for research in this field, which are shared across the suite of reviews:
As OME is a fluctuating condition with high rates of resolution and recurrence, and a highly variable impact on children, clinical trials (and, in particular, randomised controlled trials) may not be the research design of choice. Instead, evidence may be better obtained from surgical or clinical registries (for example, see Schmalbach 2021) or prospective cohort studies, with the use of 'big data'. These data sets may also be used to help identify subgroups of children who are at greater risk of persistent disease or long‐term consequences of OME. A clearer understanding of possible subgroups of children is needed to better target interventions to those who need them most, whilst avoiding over‐treatment for those in whom spontaneous resolution is anticipated.
Adverse effects of interventions are important, and should always be assessed. However, randomised controlled trials are also not the best method to consider these ‐ especially when events are rare. Observational studies with longer follow‐up and larger numbers of participants are needed to provide more robust evidence on the frequency of side effects. It is important to note that the protocol, inclusion criteria and search strategy used for this review would have excluded these types of studies. It is therefore possible that evidence of this type may exist. With this in mind, we would advocate a review of observational data, to assess whether evidence regarding longer‐term outcomes and adverse events is already available. This may be particularly important when assessing harms from serious but rare adverse events.
It is encouraging that a core outcome set has been developed in this field (Bruce 2015; Liu 2020). Guidance on how to measure the different outcomes would also be helpful for future research.
Comparison of mean hearing thresholds is widely used in research to assess the impact of different interventions on hearing. However, this outcome measure risks underestimating the potential impact of interventions on hearing. Small changes in mean hearing thresholds may be consistent with a substantial improvement in the number of children whose hearing returns to normal ‐ particularly in a condition with a high spontaneous resolution rate. We would encourage researchers to assess hearing with the proportion of children in whom hearing returns to normal, in preference to mean hearing thresholds.
History
Protocol first published: Issue 4, 2022
Acknowledgements
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to Cochrane ENT. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
The authors are grateful to Anne Littlewood, Information Specialist with Cochrane Oral Health, for providing peer review comments on the draft search methods. We are also grateful to Dr Richard Rosenfeld for providing editorial sign‐off of the protocol.
We are grateful to the 20 Cochrane Crowd screeners for screening 2443 records to identify 1130 possible RCTs, and reject 1313 references as not RCTs. We are particularly grateful to Bernardo Costa, Stefanie Rosumeck, Nikolaos Sideris, Susanna Wisniewski, Anna Resolver, Lai Ogunsola, Shammas Mohammed, Sarah Moore, Brian Duncan, Mohammad Aloulou, Ana‐Marija Ljubenković, Vighnesh D, Ahlam Jamal Alhemedi, Neetu Bhadra, Amin Sharifan, Abu Emmil Qawarizmi Bin Abu Sofian, Helen Ramsay, Dinah Amoah, Maike Scherhans and Natalya Clark for screening more than 200 records each.
Finally, our grateful thanks to Jenny Bellorini, Managing Editor, and Samantha Cox, Information Specialist, from Cochrane ENT, without whom the development of these reviews would not have been possible.
Editorial and peer reviewer contributions
Cochrane ENT supported the authors in the development of this review.
The following people conducted the editorial process for this article:
Sign‐off Editor (final editorial decision): Adrian James, Department of Otolaryngology ‐ Head and Neck Surgery, Hospital for Sick Children, Toronto, Canada
Managing Editor (selected peer reviewers, provided editorial guidance to authors, edited the article): Liz Bickerdike, Cochrane Central Editorial Service
Editorial Assistant (conducted editorial policy checks, collated peer reviewer comments and supported editorial team): Leticia Rodrigues, Cochrane Central Editorial Service
Copy Editor (copy editing and production): Jenny Bellorini, Cochrane Central Production Service
Peer reviewers: Nuala Livingstone, Cochrane Evidence Production and Methods Directorate (methods); Jo Platt, Central Executive Information Specialist (search); Hannah E Cooper, UCL Ear Institute (clinical); Jonathan Walsh, Johns Hopkins School of Medicine Department of Otolaryngology ‐ Head and Neck Surgery (clinical); Carolyn M Jenks, MD, Johns Hopkins University School of Medicine Department of Otolaryngology ‐ Head and Neck Surgery (clinical); Dr Jessica Scaife, Surgical Intervention Trials Unit, Nuffield Department of Surgical Sciences, University of Oxford (consumer)
Appendices
Appendix 1. Search strategies
The search strategies were designed to identify all relevant studies for a suite of reviews on various interventions for otitis media with effusion.
| CENTRAL (CRS) | Cochrane ENT Register (CRS) | MEDLINE (Ovid) |
| 1 MESH DESCRIPTOR Otitis Media with Effusion EXPLODE ALL AND CENTRAL:TARGET 2 ("otitis media" adj6 effusion):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 3 (OME):TI,TO AND CENTRAL:TARGET 4 (Secretory otitis media):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 5 (Serous otitis media):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 6 (Middle‐ear effusion):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 7 (glue ear):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 8 (middle‐ear perfusion):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 9 MESH DESCRIPTOR Otitis Media AND CENTRAL:TARGET 10 (otitis media):TI,TO AND CENTRAL:TARGET 11 #9 OR #10 AND CENTRAL:TARGET 12 (((effusion or Recurrent or persistent or serous or secretory or perfusion) adj3 otitis)):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 13 #11 AND #12 AND CENTRAL:TARGET 14 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #13 AND CENTRAL:TARGET |
1 MESH DESCRIPTOR Otitis Media EXPLODE ALL AND INREGISTER 2 ("otitis media" OR OME OR "glue ear" OR middle‐ear effusion OR middle‐ear perfusion):AB,EH,KW,KY,MC,MH,TI,TO AND INREGISTER 3 #1 OR #2 4 (effusion or Recurrent or persistent or serous or secretory or perfusion):AB,EH,KW,KY,MC,MH,TI,TO AND INREGISTER 5 #3 AND #4 |
1 exp Otitis Media with Effusion/ 2 ("otitis media" adj6 effusion).ab,ti. 3 OME.ti. 4 Secretory otitis media.ab,ti. 5 Serous otitis media.ab,ti. 6 Middle‐ear effusion.ab,ti. 7 Glue ear.ab,ti. 8 middle‐ear perfusion.ab,ti. 9 Otitis Media/ 10 otitis media.ti. 11 9 or 10 12 ((effusion or Recurrent or persistent or serous or secretory or perfusion) adj3 otitis).ab,ti. 13 11 and 12 14 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 13 15 randomized controlled trial.pt. 16 controlled clinical trial.pt. 17 randomized.ab. 18 placebo.ab. 19 drug therapy.fs. 20 randomly.ab. 21 trial.ab. 22 groups.ab. 23 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 24 exp animals/ not humans.sh. 25 23 not 24 26 14 and 25 |
| Embase (Ovid) | Web of Science (Web of knowledge) | Trial registries (CRS) |
| 1 exp secretory otitis media/ 2 ("otitis media" adj6 effusion).ab,ti. 3 OME.ti. 4 Secretory otitis media.ab,ti. 5 Serous otitis media.ab,ti. 6 Middle‐ear effusion.ab,ti. 7 glue ear.ab,ti. 8 middle‐ear perfusion.ab,ti. 9 otitis media/ 10 otitis media.ti. 11 9 or 10 12 ((effusion or Recurrent or persistent or serous or secretory or perfusion) adj3 otitis).ab,ti. 13 11 and 12 14 1 or 2 or 4 or 5 or 6 or 7 or 8 or 13 15 (random* or factorial* or placebo* or assign* or allocat* or crossover*).tw. 16 (control* adj group*).tw. 17 (trial* and (control* or comparative)).tw. 18 ((blind* or mask*) and (single or double or triple or treble)).tw. 19 (treatment adj arm*).tw. 20 (control* adj group*).tw. 21 (phase adj (III or three)).tw. 22 (versus or vs).tw. 23 rct.tw. 24 crossover procedure/ 25 double blind procedure/ 26 single blind procedure/ 27 randomization/ 28 placebo/ 29 exp clinical trial/ 30 parallel design/ 31 Latin square design/ 32 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 33 exp ANIMAL/ or exp NONHUMAN/ or exp ANIMAL EXPERIMENT/ or exp ANIMAL MODEL/ 34 exp human/ 35 33 not 34 36 32 not 35 37 14 and 36 |
11 #10 AND #9 Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 10 #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1 Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 9 TS=(randomised OR randomized OR randomisation OR randomisation OR placebo* OR (random* AND (allocat* OR assign*) ) OR (blind* AND (single OR double OR treble OR triple) )) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 8 (TI=(otitis media) ) AND TS=((effusion or Recurrent or persistent or serous or secretory or perfusion) NEAR/3 otitis) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 7 TOPIC: ((middle‐ear perfusion) ) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 6 TOPIC: ((glue ear) ) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 5 TOPIC: ((Middle‐ear effusion) ) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 4 TOPIC: ((Serous otitis media) ) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 3 TOPIC: ((Secretory otitis media) ) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 2 TITLE: (OME) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years 1 TOPIC: ("otitis media" NEAR/6 effusion) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years |
1 ("otitis media" OR OME OR "glue ear" OR middle‐ear effusion OR middle‐ear perfusion):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 2 (effusion or Recurrent or persistent or serous or secretory or perfusion):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 3 #1 AND #2 4 http*:SO AND CENTRAL:TARGET 5 (NCT0* or ACTRN* or ChiCTR* or DRKS* or EUCTR* or eudract* or IRCT* or ISRCTN* or JapicCTI* or JPRN* or NTR0* or NTR1* or NTR2* or NTR3* or NTR4* or NTR5* or NTR6* or NTR7* or NTR8* or NTR9* or SRCTN* or UMIN0*):AU AND CENTRAL:TARGET 6 #4 OR #5 7 #3 AND #6 |
| ClinicalTrials.gov | ICTRP | |
| (EXPAND[Concept] "otitis media" OR EXPAND[Concept] "glue ear" OR middle‐ear ) AND (effusion OR Recurrent OR persistent OR serous OR secretory OR perfusion ) | Interventional Studies | (otitis media AND effusion) OR glue ear OR middle‐ear effusion OR middle‐ear perfusion |
Appendix 2. Tool for screening eligible studies for scientific integrity/trustworthiness
This screening tool has been developed by Cochrane Pregnancy and Childbirth. It includes a set of predefined criteria to select studies which, based on available information, are deemed to be sufficiently trustworthy to be included in the analysis.
| Criteria questions | Assessment | Comments and concerns | |
| High risk | Low risk | ||
| Research governance | |||
| Are there any retraction notices or expressions of concern listed on the Retraction Watch Database relating to this study? | Yes | No | |
| Was the study prospectively registered (for those studies published after 2010) If not, was there a plausible reason? | No | Yes | |
| When requested, did the trial authors provide/share the protocol and/or ethics approval letter? | No | Yes | |
| Did the trial authors engage in communication with the Cochrane Review authors within the agreed timelines? | No | Yes | |
| Did the trial authors provide IPD data upon request? If not, was there a plausible reason? | No | Yes | |
| Baseline characteristics | |||
| Is the study free from characteristics of the study participants that appear too similar? (e.g. distribution of the mean (SD) excessively narrow or excessively wide, as noted by Carlisle 2017) |
No | Yes | |
| Feasibility | |||
| Is the study free from characteristics that could be implausible? (e.g. large numbers of women with a rare condition (such as severe cholestasis in pregnancy) recruited within 12 months) | No | Yes | |
| In cases with (close to) zero losses to follow‐up, is there a plausible explanation? | No | Yes | |
| Results | |||
| Is the study free from results that could be implausible? (e.g. massive risk reduction for main outcomes with small sample size)? | No | Yes | |
| Do the numbers randomised to each group suggest that adequate randomisation methods were used (e.g. is the study free from issues such as unexpectedly even numbers of women ‘randomised’ including a mismatch between the numbers and the methods, if the authors say ‘no blocking was used’ but still end up with equal numbers, or if the authors say they used ‘blocks of 4’ but the final numbers differ by 6)? | No | Yes | |
| For abstracts only: | |||
| Have the study authors confirmed in writing that the data to be included in the review have come from the final analysis and will not change? | No | Yes | |
Data and analyses
Comparison 1. Autoinflation versus watchful waiting/no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Proportion of children whose hearing is normal (very short‐term, < 6 weeks) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.2 Proportion of children whose hearing is normal (short‐term, > 6 weeks to ≤ 3 months) | 1 | 94 | Risk Ratio (M‐H, Random, 95% CI) | 2.67 [1.73, 4.12] |
| 1.3 Hearing threshold (very short‐term, < 6 weeks) | 1 | 45 | Mean Difference (IV, Random, 95% CI) | ‐5.00 [‐10.10, 0.10] |
| 1.4 Hearing threshold (short‐term, > 6 weeks to ≤ 3 months) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.4.1 0.5 kHz | 2 | 113 | Mean Difference (IV, Random, 95% CI) | ‐9.13 [‐15.14, ‐3.13] |
| 1.4.2 1.0 kHz | 2 | 113 | Mean Difference (IV, Random, 95% CI) | ‐10.34 [‐17.85, ‐2.83] |
| 1.4.3 2.0 kHz | 2 | 113 | Mean Difference (IV, Random, 95% CI) | ‐9.04 [‐14.84, ‐3.25] |
| 1.4.4 4.0 kHz | 2 | 113 | Mean Difference (IV, Random, 95% CI) | ‐12.88 [‐17.01, ‐8.75] |
| 1.5 Disease‐specific quality of life (short‐term, > 6 weeks to ≤ 3 months) | 1 | 247 | Mean Difference (IV, Random, 95% CI) | ‐0.42 [‐0.62, ‐0.22] |
| 1.6 Adverse events ‐ pain and distress caused by the procedure (otalgia) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.6.1 Otalgia | 1 | 320 | Risk Ratio (M‐H, Random, 95% CI) | 3.50 [0.74, 16.59] |
| 1.7 Persistence of OME (very short‐term, < 6 weeks) | 7 | 688 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.72, 1.04] |
| 1.7.1 Per ear data | 6 | 670 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.69, 1.04] |
| 1.7.2 Per child data | 1 | 18 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.72, 1.39] |
| 1.8 Persistence of OME (short‐term, > 6 weeks to ≤ 3 months) | 4 | 483 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.80, 0.97] |
| 1.8.1 Per ear data | 3 | 466 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.79, 0.96] |
| 1.8.2 Per child data | 1 | 17 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.61, 2.07] |
| 1.9 Episodes of acute otitis media (short‐term, > 6 weeks to ≤ 3 months) | 2 | 403 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.49, 1.36] |
| 1.10 Sensitivity analysis: Proportion of children whose hearing is normal (very short‐term, < 6 weeks). Per ear data (ICC of 1, complete correlation between ears) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.11 Sensitivity analysis: Proportion of children whose hearing is normal (very short‐term, < 6 weeks). Per ear data (ICC of 0, no correlation between ears) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.12 Sensitivity analysis: Hearing threshold (short‐term, > 6 weeks to ≤ 3 months). Right ear data | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.12.1 0.5 kHz | 2 | 117 | Mean Difference (IV, Random, 95% CI) | ‐9.13 [‐15.35, ‐2.92] |
| 1.12.2 1.0 kHz | 2 | 117 | Mean Difference (IV, Random, 95% CI) | ‐10.91 [‐20.07, ‐1.76] |
| 1.12.3 2.0 kHz | 2 | 117 | Mean Difference (IV, Random, 95% CI) | ‐9.59 [‐17.74, ‐1.44] |
| 1.12.4 4.0 kHz | 2 | 117 | Mean Difference (IV, Random, 95% CI) | ‐13.37 [‐20.66, ‐6.08] |
| 1.13 Sensitivity analysis: Hearing threshold (short‐term, > 6 weeks to ≤ 3 months). Left ear data | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.13.1 0.5 kHz | 2 | 115 | Mean Difference (IV, Random, 95% CI) | ‐8.97 [‐14.88, ‐3.06] |
| 1.13.2 1.0 kHz | 2 | 115 | Mean Difference (IV, Random, 95% CI) | ‐9.64 [‐15.50, ‐3.78] |
| 1.13.3 2.0 kHz | 2 | 115 | Mean Difference (IV, Random, 95% CI) | ‐8.06 [‐12.16, ‐3.97] |
| 1.13.4 4.0 kHz | 2 | 115 | Mean Difference (IV, Random, 95% CI) | ‐10.92 [‐15.42, ‐6.41] |
| 1.14 Sensitivity analysis: Persistence of OME (very short‐term, < 6 weeks). Per ear data (ICC of 0) | 6 | 862 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.68, 1.04] |
| 1.15 Sensitivity analysis: Persistence of OME (very short‐term, < 6 weeks). Per ear data (ICC of 1) | 6 | 551 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.70, 1.03] |
| 1.16 Sensitivity analysis: Persistence of OME (very short‐term, < 6 weeks). Per child data, where available | 7 | 621 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.68, 1.04] |
| 1.16.1 Per ear data, adjusted for correlation for those with bilateral disease | 4 | 300 | Risk Ratio (M‐H, Random, 95% CI) | 0.79 [0.55, 1.12] |
| 1.16.2 Per child data: persistence in any affected ear | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.88, 1.25] |
| 1.16.3 Per child data: persistence in all affected ears | 2 | 281 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.68, 1.00] |
| 1.17 Sensitivity analysis: Persistence of OME (short‐term, > 6 weeks to ≤ 3 months). Per ear data (ICC of 0) | 4 | 617 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.82, 0.97] |
| 1.17.1 Per ear data | 3 | 600 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.82, 0.97] |
| 1.17.2 Per child data | 1 | 17 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.61, 2.07] |
| 1.18 Sensitivity analysis: Persistence of OME (short‐term, > 6 weeks to ≤ 3 months). Per ear data (ICC of 1) | 4 | 402 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.81, 1.00] |
| 1.18.1 Per ear data | 3 | 385 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.80, 1.00] |
| 1.18.2 Per child data | 1 | 17 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.61, 2.07] |
| 1.19 Sensitivity analysis: Persistence of OME (short‐term, > 6 weeks to ≤ 3 months). Per child data, where available | 4 | 441 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.78, 0.96] |
| 1.19.1 Per ear data | 2 | 179 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.68, 1.06] |
| 1.19.2 Per child data | 2 | 262 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.66, 1.02] |
1.12. Analysis.

Comparison 1: Autoinflation versus watchful waiting/no treatment, Outcome 12: Sensitivity analysis: Hearing threshold (short‐term, > 6 weeks to ≤ 3 months). Right ear data
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Arick 2005.
| Study characteristics | ||
| Methods | Two‐arm, parallel‐group, randomised controlled trial with 7 weeks treatment and 11 weeks follow‐up | |
| Participants |
Setting: Single‐centre, conducted in ENT outpatients setting in the USA. Study dates are not reported. Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 4 to 11 years Minimum of a 2‐month history of middle ear effusion and associated hearing loss as documented by a physician Pure tone air conduction thresholds of 20 dB HL or more at 3 frequencies between 500 Hz and 4000 Hz with air‐bone gaps of 15 dB or more at these frequencies or pure tone air conduction thresholds of 25 dB HL or more at 2 frequencies between 500 Hz and 4000 Hz with air‐bone gaps of 15 dB or more at these frequencies at the final pretest A tympanometric peak pressure of ‐100 daPa or less at the final pretest Otologic diagnosis of middle ear effusion at the final pretest Exclusion criteria: Enlarged adenoids, acute otitis media and other ear abnormalities at the final pretest otologic examination |
|
| Interventions |
Autoinflation group (n = 47 (88 ears) randomised) Modified Politzer device. Hand‐held, battery‐operated. A probe tip is inserted into the nostril, while compressing the other nostril with a finger. Child holds a small amount of water in the mouth without swallowing. The device is turned on to introduce air flow into the nostril. After 1 to 2 seconds of air flow the child swallows the water. Air pressure was initially 5.2 psi. This was reduced to 2.5 over the course of the study due to some discomfort. The protocol was then changed to 2.5 psi for children ≤ 7 years and increased if tolerated. Pressure could be lowered if needed due to discomfort. Used twice a day for 7 weeks Control group (n = 47 (86 ears) randomised) No treatment |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review: None Other outcomes reported in the study: Tympanic membrane motility, only for those ears that had achieved normal hearing Tympanometric peak pressure |
|
| Funding sources | This research was supported by a grant (No. 5R44DC0036 I3‐03) from the Small Business Innovation Research Program, National Institute on Deafness and Other Communication Disorders, National Institutes of Health to Arisil Instruments | |
| Declarations of interest | No declaration made, but note that the principal investigators appear to own a business to develop this instrument (Arisil Instruments) | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: “Of this group, 47 patients (88 ears) were randomly assigned to the experimental group and 47 patients (86 ears) were assigned to the control group”. Comment: no further information. |
| Allocation concealment (selection bias) | Unclear risk | No details provided. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: “Audiologists were blinded to each patient's otologic findings, and otolaryngologists were blinded to each patient's audiometric findings. At the posttest, audiologists and otolaryngologists were blinded to each patient's disease status. The statistician was blinded as to whether test results were obtained before or after therapy and to the disease status of each patient.” (page 57) Comment: blinding of outcome assessors is not described, although outcome assessors (audiologists and ENT surgeons) were independent of each other. It is not clear if outcomes assessors were blinded to treatment allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data are available for almost all randomised participants. |
| Selective reporting (reporting bias) | Unclear risk | No protocol has been found to enable assessment of selective reporting. |
| Other bias | Low risk | No other concerns identified. |
Banigo 2016.
| Study characteristics | ||
| Methods | Two‐arm, single‐blind, parallel‐group, randomised controlled trial with 7 weeks of treatment and follow‐up | |
| Participants |
Setting: Single‐centre, conducted in an outpatient hospital clinic in the UK between September 2008 and March 2013 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 4 to 11 years with hearing loss from persistent OME over a 3‐month period and an average air conduction of 25 dB HL or worse in the better ear across 0.5, 1.0, 2.0 and 4.0 kHz were considered eligible for the trial Children who were placed on a waiting list for VT insertion and had a wait of > 7 weeks Exclusion criteria:
|
|
| Interventions |
Autoinflation group (n = 15 randomised, n = 15 completed) Use of EarPopper® device. Used twice a day, twice in each nostril. Device used on low‐pressure settings (level I) for 7 weeks. Control group (n = 15 randomised, n = 14 completed) No details given but presumably nothing done/no placebo |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
Other outcomes reported in the study: Number of patients requiring ventilation tubes at longer‐term follow‐up |
|
| Funding sources | Not reported | |
| Declarations of interest | None reported | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “children were allocated to treatment or control groups using a randomly allocated computer‐generated code”. Comment: computer‐generated randomisation. |
| Allocation concealment (selection bias) | Unclear risk | No information on concealment of allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: “The audiologists performing the final audiogram at 7 weeks were blinded to which group each child belonged to”. Comment: outcomes assessed by blinded personnel. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Only one dropout in the trial and this is unlikely to influence results. |
| Selective reporting (reporting bias) | Unclear risk | No protocol was identified. |
| Other bias | High risk | Follow‐up is 7 weeks and therefore this is insufficient time for follow‐up of no treatment. |
Bidarian‐Moniri 2014.
| Study characteristics | ||
| Methods | Two‐arm, randomised, controlled, cross‐over, with follow‐up at 4 weeks and 1 year Data from the first phase of the study were used in this review |
|
| Participants |
Setting: Multicentre study, conducted in hospitals in Sweden and Portugal between May 2010 and June 2012 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 2 to 8 years with history of persistent bilateral otitis media with effusion with a duration of disease of at least 3 months and history of subjective hearing loss, waiting for grommet surgery Children underwent otomicroscopy, tympanometry and audiometry. Those with bilateral OME with type C2 or B tympanogram. Exclusion criteria:
|
|
| Interventions |
Autoinflation group (n = 22 randomised first) A new autoinflation device consisting of an inflatable facemask, a T‐shaped junction tube connecting at one end to the facemask, another end to a balloon and the third end to a handheld pump. The pump was covered by a teddy bear in order to improve compliance in young children. Three different balloons with the respective opening pressures of 20 ± 3, 40 ± 2 and 60 ± 5 cm H2O were used. Children used the device twice a day to perform 20 inflations at each session (approximately 5 to 10 minutes) during a period of 4 weeks Control group (n = 23 randomised first) No treatment |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
Other outcomes reported in the study:
|
|
| Funding sources | This work was partially financed by grants from the Rune and Ulla Amlöv Foundation for Neurological, Rheumatological and Audiological Research, Sweden | |
| Declarations of interest | None reported | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “Computer‐generated, independent allocation sequences were used for randomisation. To avoid disproportionate numbers of patients in each group, randomisation was performed in blocks of six subjects (three allocated to the treatment and three to the control group).” Comment: computer‐generated. |
| Allocation concealment (selection bias) | Unclear risk | Quote: “Computer‐generated, independent allocation sequences were used for randomisation. To avoid disproportionate numbers of patients in each group, randomisation was performed in blocks of six subjects (three allocated to the treatment and three to the control group). The children were enrolled by a secretary and assigned to group A or B by one of the authors.” Comment: with a relatively small block size in this unblinded study, it may be possible to predict the next allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: “Pure tone air conduction thresholds for each ear or sound field audiometry for both ears were performed by an experienced audiologist who was blinded to the group allocation of the child.” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There do not appear to be any missing outcome data. |
| Selective reporting (reporting bias) | Unclear risk | No protocol or trial registration was found. |
| Other bias | High risk | Follow‐up is at 1 month ‐ this is insufficient time for follow‐up of no treatment. |
Blanshard 1993.
| Study characteristics | ||
| Methods | Two‐arm, parallel‐group, randomised controlled trial, with 3 months of treatment and follow‐up | |
| Participants |
Setting: Single‐centre, conducted in an ENT clinic in the UK from July to December 1991 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 3 to 10 years with confirmation of bilateral type B or C2 tympanograms on 2 occasions separated by at least 3 months and on the waiting list for grommets Exclusion criteria:
|
|
| Interventions |
Autoinflation group (n = 42 completed) The Otovent device is a rounded plastic nose piece with a balloon attached. Used once through each nostril 3 times a day. Balloon changed every 3 days. Not to be used during the first few days of an URTI, or an episode of otalgia Control group (n = 41 completed) No intervention |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
|
|
| Funding sources | Not reported | |
| Declarations of interest | None reported | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “They were allocated to either the treatment or to the control group by computer generated random numbers”. Comment: computer‐generated method of randomisation. |
| Allocation concealment (selection bias) | Unclear risk | No information on allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No information is provided regarding whether outcome assessors were blinded. It is likely they were unblinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There was minimal dropout. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available. Most analyses are conducted according to a per protocol analysis of those with high compliance versus control, rather than the entire treatment group. |
| Other bias | Low risk | No other concerns. |
Brooker 1992.
| Study characteristics | ||
| Methods | Two‐arm, parallel‐group, randomised controlled trial of 3 weeks treatment and follow‐up | |
| Participants |
Setting: Single‐centre, conducted in a hospital audiology clinic in the UK. Study dates were not reported. Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Children aged less than 10 years referred to audiology clinic with unilateral or bilateral glue ears diagnosed by otoscopy, audiogram and tympanogram. The children had to be able to inflate a carnival blower nasally. Exclusion criteria: Not reported |
|
| Interventions |
Autoinflation group (n = 21 (41 ears) randomised) Three times daily for 3 weeks. Device comprised of a toy balloon attached to a carnival blower mouthpiece. Pressure required to inflate was in the range 35 to 40 mmHg then settled to 20 to 23 mmHg once the balloon had started to inflate. Children were taught how to do it initially. Control group (n = 19 (37 ears) randomised) No treatment |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
|
|
| Funding sources | Not reported | |
| Declarations of interest | None reported | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The children so selected were, with the informed consent of their parents, allocated at random into two groups.” Comment: insufficient information to judge random sequence generation. |
| Allocation concealment (selection bias) | Unclear risk | No description of allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | There is no statement to indicate that outcome assessors were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing outcome data. |
| Selective reporting (reporting bias) | Unclear risk | No protocol was identified. |
| Other bias | High risk | Follow‐up was for 3 weeks ‐ this is insufficient time for as assessment of the 'no treatment' group, as they would not be expected to have improved during this time frame. |
Chan 1989.
| Study characteristics | ||
| Methods | Two‐arm, parallel‐group, randomised controlled trial with 2 weeks of treatment and follow‐up | |
| Participants |
Setting: Single‐centre, conducted in the USA between February 1986 and February 1987 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 3 to 18 years with chronic otitis media with effusion. The aim was to include those that had persistence for at least 3 months (although this was not everyone). Failed to respond to conventional antimicrobial treatment. Exclusion criteria:
|
|
| Interventions |
Autoinflation group (n = 19 randomised) Modified Valsalva techniques ‐ a disposable anaesthesia mask attached to a floating ball‐type flowmeter with 2 plastic ring adaptors. Children were instructed to exhale through the nose through the mask (with the mouth closed); as the pressure increased, the ball in the flowmeter was propelled upwards. To be performed 3 times daily for 2 weeks Control group (n = 22 randomised) No treatment |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
Other outcomes reported in the study: Bilateral versus unilateral disease outcomes in control vs autoinflation groups |
|
| Funding sources | NIH grants | |
| Declarations of interest | None reported | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Within in each stratification, subjects were randomly assigned to either the autoinflation or the control group by the use of a set of random numbers”. Comment: random numbers were used for randomisation. |
| Allocation concealment (selection bias) | Unclear risk | No information on concealment of allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | There is no description of whether the outcome assessors were blinded. It is likely that they were unblinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Only 1 participant was missing from follow‐up. |
| Selective reporting (reporting bias) | Unclear risk | No protocol was identified. |
| Other bias | High risk | Follow‐up is 2 weeks and therefore this is insufficient time for follow‐up of no treatment. |
Ercan 2005.
| Study characteristics | ||
| Methods | Two‐arm, parallel‐group randomised controlled trial with 6 weeks of treatment and follow‐up at 3 and 9 months | |
| Participants |
Setting: Single‐centre, conducted in an outpatient setting in Turkey between January 2002 and April 2004 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Children with middle ear effusion and free of signs of otitis media for at least a 4‐week period (ear ache, ear discharge etc.) Diagnosis of chronic otitis media with effusion was established by the typical appearance (fluid level or air bubbles in middle ear, white opacification in the tympanic membrane, vascularisation of the tympanic membrane without erythema, lack of mobility of the tympanic membrane in ventilation of the external ear canal, etc.) of the tympanic membrane at the pneumatic otoscopic examination and type B tympanogram at the end of the 3 months follow‐up Exclusion criteria:
|
|
| Interventions |
Autoinflation group (n = 30 randomised (48 ears)) Otovent 3 times a day for 6 weeks, with nasal saline irrigation 3 times a day for 6 weeks Control group (n = 30 randomised (45 ears)) Treated with nasal saline irrigation 3 times a day for 6 weeks Information on treatment used before entry into the trial Amoxicillin for 3 weeks, antihistamines (in case of allergy) and nasal saline irrigation |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
|
|
| Funding sources | Not reported | |
| Declarations of interest | None reported | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: “The patients were randomly divided into two groups”. Comment: no information provided to indicate how the random sequence was generated. |
| Allocation concealment (selection bias) | Unclear risk | Quote: “The patients were randomly divided into two groups”. Comment: no information provided to indicate how allocation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | This was an open‐label trial, with no mention of blinding, therefore the outcome assessors were unlikely to be blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There do not appear to be any missing outcome data. |
| Selective reporting (reporting bias) | Unclear risk | No protocol or trial registration was found. |
| Other bias | Low risk | No concerns. |
Scadding 2014.
| Study characteristics | ||
| Methods | Four‐arm, parallel‐group, randomised controlled trial with up to 2 years of treatment and follow‐up | |
| Participants |
Setting: Single‐centre, conducted in a specialist glue ear clinic in a hospital in the UK between 1994 and 2003 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 4 to 8 years with at least 3 months of glue ear or more than 2 episodes in the past 6 months, and a type B or C tympanogram Exclusion criteria:
|
|
| Interventions |
Nasal steroids group (n = 52 randomised; n = 32 completed) 50 µg per spray, 1 puff per nostril twice daily for 2 weeks (2 puffs per nostril twice daily for children over 35 kg), i.e. total daily dose 200 µg (or 400 µg) initially Then reduced to 1 puff per nostril (100 µg) once daily. “The children were asked to use this on a regular basis”. “Those who reported spray use on at least 3 days a week remained in the study” Autoinflation group (n = 52 randomised; n = 30 completed) Otovent autoinflation device. Used 3 times daily for the first box of balloons (i.e. 4 to 5 weeks) then stopped if hearing was not troublesome. Use was re‐established if glue ear re‐presented, especially after a cold. Autoinflation and nasal steroids group (n = 48 randomised; n = 31 completed) Otovent as above and nasal steroids as above Placebo group (n = 48 randomised; n = 30 completed) Matching placebo |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
Other outcomes reported in the study:
|
|
| Funding sources | Glaxo Smith Kline, Inphormed and Merck | |
| Declarations of interest | This study was conceived by Glenis Scadding and funded by Glaxo Smith Kline (including the salary of Abhijeet Parikh as a PhD student) together with Inphormed who provided Otovent devices free of charge. Merck Sharp and Dohme provided funding for further independent statistical analysis since this was advised by a referee when the paper was originally submitted. Glenis Scadding has received funding from GSK and MSD for other trials, serves on an advisory panel and has lectured for them at meetings. Helen Tate has worked as an independent statistical consultant for Merck, Sharp and Dohme. At the time of the study, DR was a full‐time employee of GlaxoSmithKline R&D. None of the other authors has any interests to declare. | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Subjects were randomised to receive FP or matching placebo in a 1:1 ratio according to a computer‐generated randomisation schedule using a block size of 8.” “In addition those children entering the trial with an odd number were also given the Otovent device; this part of the study was open.” Comment: computer‐generated randomisation. |
| Allocation concealment (selection bias) | Low risk | Quote: “…computer‐generated randomisation schedule using a block size of 8. This was held in the pharmacy, and both subjects and observers were blind as to the nature of this treatment.” Comment: third party conducted randomisation and allocation. Even though personnel would know that an odd number is allocation to Otovent, it is unlikely that allocation could be interfered with. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "both subjects and observers were blind as to the nature of this treatment. In addition those children entering the trial with an odd number were also given the Otovent device; this part of the study was open." It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "both subjects and observers were blind as to the nature of this treatment.” Comment: the above statement may refer to the steroid intervention, but it is likely that outcome assessors are not blinded to autoinflation allocation. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 38% loss to follow‐up; this may substantially impact results. |
| Selective reporting (reporting bias) | Unclear risk | No protocol found, so it was not possible to assess selective reporting bias. |
| Other bias | Low risk | No other concerns. |
Stangerup 1992.
| Study characteristics | ||
| Methods | Two‐arm, parallel‐group, randomised controlled trial with 2 weeks of treatment and 3 months of follow‐up | |
| Participants |
Setting: Single‐centre, conducted in a university ENT Department in China between June 2009 and March 2011 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 3 to 10 years, unilateral or bilateral secretory otitis media for at least 3 months as verified by tympanometry and otomicroscopy Exclusion criteria: None reported |
|
| Interventions |
Autoinflation group (n = 46 completed) Tube designed by the author, with a balloon on the end, inserted in one nostril and blown up whilst occluding the other Three times per day for 2 weeks. If a type C2 or a type B tympanogram persisted after 2 weeks, the children where instructed to carry on for a further 2 weeks. To cease if they acquired a common cold or purulent rhinitis Control group (n = 47 completed) No treatment |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
|
|
| Funding sources | Not reported | |
| Declarations of interest | None reported | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: “One hundred children were consecutively randomized to undergo either autoinflation, using a new device, or placed in a control group.” “The patients were randomized to either a group performing autoinflation for 2 weeks or to a group being observed without treatment for 2 weeks.” Comment: no information on how the random sequence was generated. |
| Allocation concealment (selection bias) | Unclear risk | Quote: “One hundred children were consecutively randomized to undergo either autoinflation, using a new device, or placed in a control group.” “The patients were randomized to either a group performing autoinflation for 2 weeks or to a group being observed without treatment for 2 weeks.” Comment: no information on how allocation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It is not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | It is unlikely that outcome assessors were blind to treatment allocation. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Many results are reported as a per protocol analysis only for those who successfully carried out autoinflation. |
| Selective reporting (reporting bias) | Unclear risk | No protocol or trial registration was found. |
| Other bias | Low risk | No concerns. |
Williamson 2015a.
| Study characteristics | ||
| Methods | Two‐arm, parallel‐group, randomised controlled trial with 3 months of follow‐up | |
| Participants |
Setting: Multicentre, conducted in 43 general practices in the UK between January 2012 and February 2013 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 4 to 11 years and attending school. At least one ear with a type B tympanogram in one or both ears and middle ear pressure of ‐400 with a flat trace, based on the modified Jerger classification, and fulfilled one of these 3 criteria:
Exclusion criteria:
|
|
| Interventions |
Autoinflation group (n = 160 randomised, n = 125 followed up at 3 months) Otovent was used. Children were required to inflate a purpose‐manufactured balloon by blowing through each nostril into a connecting nozzle 3 times per day for 1 to 3 months. Children were shown the procedure, and a website with an instruction video was available for back‐up. Children still showing a type B tympanogram in either ear at 1 month were advised to continue for a further 2 months. Control group (n = 160 randomised, n = 120 followed up at 3 months) No treatment Background intervention common to both groups Routine care was given to both groups as normal |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
Other outcomes reported in the study: Parents were asked to complete a weekly diary recording the number of days (0 to 7) of their child’s main symptoms of hearing loss, earache, difficulty concentrating, pain relief, disturbed sleep and absence from school. None of these are relevant outcomes. In addition, a second diary of items was included to systematically record a number of other symptoms including nosebleeds, clumsiness/off‐balance, systemic illness, nasal discharge and nasal congestion/snoring. Not relevant outcomes. Those that we have listed as adverse events are recorded separately. Hearing disability was evaluated at baseline and at 1 month for all children using the TADAST web‐based test. TADAST is a forced‐choice test, originally developed in primary care, which evaluates hearing disability associated with glue ear. Only accounts for disability related to hearing, not an objective measure of hearing loss as required for our primary outcome. Not presented in text therefore cannot be used for hearing disability, due to few people completing questionnaire. Health economic analysis Qualitative outcomes Diary card of symptoms |
|
| Funding sources | Funded by the HTA programme. Project number 09/01/27. | |
| Declarations of interest | One author is a member of the NIHR Editorial Board | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “An independent external agency provided a centralised web‐based randomisation system (www.sealedenvelope.com) for nurses to access while recruiting children to the study”. “The randomisation used an algorithm with minimisation based on three potential effect modifiers/confounders: age (< 6.5 years vs. > 6.5 years), sex and baseline severity of OME (one vs. two baseline type B tympanograms)”. Comment: computer‐generated randomisation. |
| Allocation concealment (selection bias) | Low risk | Quote: “An independent external agency provided a centralised web‐based randomisation system (www.sealedenvelope.com) for nurses to access while recruiting children to the study”. Comment: adequate concealment of allocation by third party. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: “Owing to the nature of the intervention, use of placebo was not possible and therefore nurses, children and families were not masked to treatment allocation.” Comment: no blinding was possible. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: “Tympanometry […] provides a reasonably objective outcome measure that can also be assessed blind to allocation arm. Two members of the trial team, trained in tympanometry, independently reviewed anonymised tympanometry printouts”. Comment: outcome assessors were blinded to allocated group. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing outcome data were balanced across groups, with similar reasons in each group, however it is unclear whether the proportion of missing outcomes is likely to introduce significant bias in the effect direction or magnitude. Sensitivity analysis with multiple imputation to account for missing data resulted in similar effect size, but the difference between groups was then non‐significant. Per protocol analysis reduced the effect size further. |
| Selective reporting (reporting bias) | Low risk | Study protocol is published, and all outcome measures are reported according to the pre‐specified plan. |
| Other bias | Low risk | No other concerns. |
Williamson 2015b.
| Study characteristics | ||
| Methods | Two‐arm, parallel‐group randomised controlled trial with 3 months of follow‐up These are pilot data from the same publication as Williamson 2015a |
|
| Participants |
Setting: Multicentre, conducted in 4 general practices in the UK between January 2010 and May 2010 Sample size:
Participant (baseline) characteristics:
Inclusion criteria: Aged 4 to 11 years and attending school. At least one ear with a type B tympanogram in one or both ears and middle ear pressure of ‐400 with a flat trace, based on the modified Jerger classification, and fulfilled one of the these 3 criteria:
Exclusion criteria:
|
|
| Interventions |
Autoinflation group (n = 11 randomised, n = 9 followed up at 3 months) Otovent was used. Children were required to inflate a purpose‐manufactured balloon by blowing through each nostril into a connecting nozzle 3 times per day for 1 to 3 months. Children were shown the procedure, and a website with an instruction video was available for back‐up. Children still showing a type B tympanogram in either ear at 1 month were advised to continue for a further 2 months. Control group (n = 10 randomised, n = 8 followed up at 3 months) No treatment Background intervention common to both groups Routine care was given to both groups as normal |
|
| Outcomes |
Primary outcomes relevant to this review:
Secondary outcomes relevant to this review:
|
|
| Funding sources | Not reported | |
| Declarations of interest | None reported | |
| Notes |
Research integrity checklist
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Eligible children were individually randomised to autoinflation plus routine care or routine care alone via a telephone dial‐in service" "The randomisation method used an algorithm with minimisation based on three previously found key variables: age, sex and baseline severity of OME." Comment: third party randomisation with the use of a minimisation algorithm implies computer‐generated randomisation method. |
| Allocation concealment (selection bias) | Low risk | Quote: "Eligible children were individually randomised to autoinflation plus routine care or routine care alone via a telephone dial‐in service" Comment: likely to be adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Given the nature of the intervention it was not possible to blind participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Tympanometric outcomes were assessed blind to intervention group by the chief investigator." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4/21 (19%) loss to follow‐up at 3 months. |
| Selective reporting (reporting bias) | Low risk | All outcomes are reported according to the pre‐specified plan. |
| Other bias | Low risk | No other concerns identified. |
AOM: acute otitis media; dB: decibels; dB HL: decibels hearing level; ENT: ear, nose and throat; HTA: health technology assessment; kg: kilogram; µg: microgram; MEE: middle ear effusion; n/a: not applicable; NIH: National Institutes of Health; OME: otitis media with effusion; OMQ‐14: Otitis Media Questionnaire‐14; RTI: respiratory tract infection; SD: standard deviation; URTI: upper respiratory tract infection; VT: ventilation tube
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ardehali 2008 | INTERVENTION: treatment with antibiotics, and is relevant for another review in this suite (Mulvaney 2022a) |
| Bidarian‐Moniri 2016 | ALLOCATION: not randomised |
| ChiCTR2000035008 | INTERVENTION: wrong intervention |
| Choung 2008 | INTERVENTION: treatment with steroids, and is relevant for another review in this suite (Mulvaney 2022b) |
| De Nobili 2008 | INTERVENTION: included nasal decongestants |
| El Hachem 2012 | INTERVENTION: no intervention of interest |
| Endo 1997 | INTERVENTION: treatment with antibiotics, and is relevant for another review in this suite (Mulvaney 2022a) |
| Ferrara 2005 | PARTICIPANTS: had recurrent acute otitis media |
| Gibson 1996 | ALLOCATION: not randomised |
| Head 1992 | STUDY DESIGN: commentary article, not an RCT |
| Heaf 1991 | INTERVENTION: not an intervention of interest (nose blowing, not autoinflation) |
| Iino 1989 | ALLOCATION: not randomised |
| Leunig 1995 | COMPARISON: not a comparison of interest |
| Li 2020 | PARTICIPANTS: adult patients |
| Li 2021 | ALLOCATION: not randomised |
| Marchisio 1998 | INTERVENTION: treatment with antibiotics, and is relevant for another review in this suite (Mulvaney 2022a) |
| NCT03534219 | OTHER: study withdrawn/terminated |
| Paradise 1997 | ALLOCATION: not randomised |
| Parlea 2012 | ALLOCATION: not randomised |
| Rohail 2006 | INTERVENTION: not a relevant intervention (no autoinflation) |
| Shubich 1996 | ALLOCATION: not randomised |
| Silman 2005 | ALLOCATION: not randomised |
| Starcevic 2011 | INTERVENTION: treatment with ventilation tubes, and is relevant for another review in this suite (MacKeith 2022a) |
| Stenstrom 2005 | ALLOCATION: not randomised |
| Tham 2018 | ALLOCATION: not randomised |
RCT: randomised controlled trial
Characteristics of studies awaiting classification [ordered by study ID]
Tawfik 2002.
| Methods | — |
| Participants | — |
| Interventions | — |
| Outcomes | — |
| Notes | Unable to obtain full text |
Characteristics of ongoing studies [ordered by study ID]
INFLATE (ACTRN12617001652369).
| Study name | 'INFLATE: a protocol for a randomised controlled trial comparing nasal balloon autoinflation to no nasal balloon autoinflation for otitis media with effusion in Aboriginal and Torres Strait Islander children' |
| Methods | Multicentre, open‐label, parallel‐group randomised controlled trial |
| Participants | Aboriginal and Torres Strait Islander children aged 3 to 16 years old with unilateral or bilateral OME Estimated enrolment 400 participants |
| Interventions | Nasal balloon autoinflation using the Otovent device (2 times per day for 1 to 3 months) compared to no treatment |
| Outcomes |
|
| Starting date | December 2017 |
| Contact information | P.Abbott@westernsydney.edu.au |
| Notes | — |
NCT00393159.
| Study name | 'The influence of the Ear Popper on serous otitis media and on the accompanying conductive hearing loss in children' |
| Methods | Single‐centre, parallel‐group, open‐label randomised controlled trial with 7 weeks duration of intervention and follow‐up at a maximum of 12 weeks |
| Participants | Children aged 3 to 18 years with OME for at least 3 months, a conductive hearing loss of more than 15 dB, and type B or C tympanogram |
| Interventions | Use of Ear Popper device (frequency of use not stated) compared to no treatment |
| Outcomes |
|
| Starting date | Trial registered in October 2006. No details on starting date. |
| Contact information | dkyo@barak‐online.net.il |
| Notes | We presume that this trial has been discontinued, due to the duration of time that has elapsed since the trial registration, however we have been unable to verify this |
NCT02038400.
| Study name | 'Efficacy of KNT® (KINETUBE) in recurrent chronic otitis media in children' |
| Methods | Parallel‐group, open‐label RCT |
| Participants | Children aged 7 to 15 years old with recurrent otitis media with effusion, or atelectasis, with presence of fluid behind the eardrum, and conductive hearing loss ≥ 30 dB NB: it is not clear if this study will recruit children with OME or only recurrent acute otitis media |
| Interventions | Use of the Kinetube compared to ventilation tube insertion Frequency and duration of treatment are not stated |
| Outcomes | Hearing threshold in dB HL measured with pure tone audiometry at up to 12 months |
| Starting date | Trial registration January 2014 |
| Contact information | Loic Mondoloni, Assistance Publique Hopitaux De Marseille |
| Notes | It is not clear if this trial is ongoing, or was discontinued |
NCT02546518.
| Study name | 'A comparison of surgical and a new non‐surgical treatment methods for secretory otitis media in children' |
| Methods | Single‐centre, parallel‐group randomised controlled trial |
| Participants | Children aged 30 months to 7 years with unilateral or bilateral OME for 3 months or longer |
| Interventions | The use of a custom‐made autoinflation device (as described in Bidarian‐Moniri 2014) for 5 minutes, twice a day for 1 month will be compared to the insertion of a tympanostomy tube |
| Outcomes |
|
| Starting date | September 2015 Estimated completion date December 2017 |
| Contact information | mohammed.al‐azzawe@vgregion.se hasse.ejnell@vgregion.se |
| Notes | Unable to locate any publication arising from this trial registration |
NCT05324696.
| Study name | 'Autoinflation: alternative in the treatment of otitis media with effusion' |
| Methods | Parallel‐group randomised controlled trial, conducted in Portugal |
| Participants | Children aged 3 to 8 years with unilateral or bilateral OME, as diagnosed with otomicroscopy and tympanometry (type B or C2), audiogram with hearing loss ≥ 20 dB or air‐bone gap Estimated enrolment 50 participants |
| Interventions | Autoinflation device (based on that used by Bidarian‐Moniri 2014) compared to a sham device that does not generate pressure No details on frequency |
| Outcomes | Resolution of OME, assessed after 3 years of follow‐up |
| Starting date | November 2020. Estimated completion December 2023. |
| Contact information | Joao Lino, Instituto de Ciências Biomédicas Abel Salazar |
| Notes | — |
dB HL: decibels hearing level; OME: otitis media with effusion; OMQ‐14: Otitis Media Questionnaire‐14; RCT: randomised controlled trial
Differences between protocol and review
We noted some overlap in the outcomes related to adverse events that were specified in our protocol (Galbraith 2022). The original list of primary and secondary outcomes was as follows:
Primary outcomes
Hearing
Disease‐specific quality of life
Adverse events ‐ pain and distress caused by the procedure
Secondary outcomes
Presence/persistence of OME
-
Adverse events:
Eardrum perforation
Middle ear infection
Otalgia
Acute otitis media (AOM)
Compliance
Receptive language skills
Speech development
Cognitive development
Psychosocial outcomes
Listening skills
Generic health‐related quality of life
Parental stress
Vestibular function
Number of doctor‐diagnosed AOM episodes within a specified time frame
However, when we came to extract outcome data from the studies, we noted that there was some duplication in this list:
Our primary outcome of 'pain and distress caused by the procedure' overlapped with the outcome 'otalgia', listed as a secondary outcome.
Our secondary outcomes of middle ear infection and acute otitis media (listed under adverse events) overlapped with the outcome 'number of doctor diagnosed AOM episodes within a specified time frame'.
No studies reported specifically on 'pain and distress caused by the procedure'. However, some studies gave information on the number of children experiencing otalgia. We considered that this should be assessed within this primary outcome, rather than as a separate, secondary outcome. Therefore, data on otalgia have been included under this outcome in the summary of findings table, and are reported in the abstract.
Due to the overlap in outcomes considering infection, we have only reported on the 'number of doctor diagnosed AOM episodes within a specified time frame'.
In our protocol we planned to use the Trustworthiness Tool developed by Cochrane Pregnancy and Childbirth to determine which studies would be included in the main analyses. As described in the text, we used this tool to assess the studies, but did not use it to determine whether a study should be included in the main analysis.
Contributions of authors
Katie Webster: screened the search results and selected studies, conducted data extraction and carried out statistical analyses. Drafted the text of the review.
Caroline A Mulvaney: drafted the protocol. Screened the search results and selected studies, conducted data extraction, carried out statistical analyses and GRADE assessment. Drafted the text of the review.
Kevin Galbraith: drafted the protocol. Screened the search results and selected studies, conducted data extraction, carried out statistical analyses and GRADE assessment. Drafted the text of the review.
Mridul Rana: conducted data extraction. Reviewed the analyses and reviewed and edited the text of the review.
Tal Marom: reviewed the protocol. Reviewed the analyses and reviewed and edited the text of the review.
Mat Daniel: reviewed the protocol. Reviewed the analyses and reviewed and edited the text of the review.
Roderick P Venekamp: co‐wrote and edited the protocol. Reviewed the analyses and reviewed and edited the text of the review.
Anne GM Schilder: co‐wrote and edited the protocol. Reviewed the analyses and reviewed and edited the text of the review.
Samuel MacKeith: drafted the protocol. Screened the search results and selected studies. Reviewed the analyses and reviewed and edited the text of the review.
Sources of support
Internal sources
No sources of support provided
External sources
-
National Institute for Health Research, UK
Infrastructure funding for Cochrane ENT
Declarations of interest
Katie Webster: none known.
Caroline A Mulvaney: none known.
Kevin Galbraith: none known.
Mridul Rana: none known.
Samuel MacKeith: treats patients with OME in his NHS and private practice and is Assistant Co‐ordinating Editor of Cochrane ENT but has not been involved in the editorial process for this review.
Tal Marom: treats patients with OME in his public sector and private practice.
Mat Daniel: treats patients with OME in his NHS practice. He has a financial interest in Aventamed, a company that produces a ventilation tube insertion device.
Roderick P Venekamp: is an Editor for Cochrane Acute Respiratory Infections and Cochrane ENT, but had no role in the editorial process for this review.
Anne GM Schilder: Professor Anne Schilder was joint Co‐ordinating Editor of Cochrane ENT until April 2020, but had no role in the editorial process for this review. She treats patients with OME in her NHS practice. Her evidENT team at the UCL Ear Institute is supported by the National Institute of Health Research (NIHR) University College London Hospitals (UCLH) Biomedical Research Centre (BRC), with research projects being supported by the NIHR, Wellcome Trust, RNiD, ENT UK and industry. She is the National Specialty Lead for the NIHR Clinical Research Network ENT and Surgical Specialty Lead for ENT for the Royal College of Surgeons of England's Clinical Research Initiative. In her role as director of the NIHR UCLH BRC Deafness and Hearing Problems Theme, she advises CRO, biotech and pharma companies in the hearing field on clinical trial design and delivery.
New
References
References to studies included in this review
Arick 2005 {published data only}
- Arick D, Silman S. Nonsurgical home treatment of middle ear effusion and associated hearing loss in children. Part I: clinical trial. Ear, Nose, & Throat Journal 2005;84(9):567-8, 570-4, 576 passim. [CENTRAL: CN-00552768] [EMBASE: 41864684] [PMID: ] [PubMed] [Google Scholar]
Banigo 2016 {published data only}
- Banigo A, Hunt A, Rourke T, Whiteside O, Aldren C. Does the Earpopper(®) device improve hearing outcomes in children with persistent otitis media with effusion? A randomised single-blinded controlled trial. Clinical Otolaryngology 2016;41(1):59-65. [CENTRAL: CN-01078433] [EMBASE: 607683212] [PMID: ] [DOI] [PubMed] [Google Scholar]
Bidarian‐Moniri 2014 {published data only}
- Bidarian-Moniri A, Ramos MJ, Ejnell H. Autoinflation for treatment of persistent otitis media with effusion in children: a cross-over study with a 12-month follow-up. International Journal of Pediatric Otorhinolaryngology 2014;78(8):1298-305. [CENTRAL: CN-00994829] [EMBASE: 2014464001] [PMID: ] [DOI] [PubMed] [Google Scholar]
Blanshard 1993 {published data only}
- Blanshard J, Maw A, Bawden R. The treatment of otitis media with effusion in children by autoinflation. In: 2nd European Congress of Oto-Rhino-Laryngology and Cervico-facial Surgery. 1992:31-7. [CENTRAL: CN-01165327]
- Blanshard JD, Maw AR, Bawden R. Conservative treatment of otitis-media with effusion by autoinflation of the middle-ear. Clinical Otolaryngology 1993;18(3):188-92. [CENTRAL: CN-02472342] [DOI] [PubMed] [Google Scholar]
Brooker 1992 {published data only}
- Brooker DS, McNeice A. Autoinflation in the treatment of glue ear in children. Clinical Otolaryngology and Allied Sciences 1992;17(4):289-90. [CENTRAL: CN-00262418] [PMID: ] [DOI] [PubMed] [Google Scholar]
Chan 1989 {published data only}
- Chan KH, Bluestone CD. Lack of efficacy of middle-ear inflation: treatment of otitis media with effusion in children. Otolaryngology--Head and Neck Surgery 1989;100(4):317-23. [CENTRAL: CN-00060254] [PMID: ] [DOI] [PubMed] [Google Scholar]
Ercan 2005 {published data only}
- Ercan I, Cakir BC, Kayaoglu S, Turgut S. Long term effect of autoinflation in the treatment of otitis media with effusion. Elektronik Kulak Buran Bogaz ve Bas Boyun Cerrahisi Dergisi [Electronic Journal of Otolalryngology - Head and Neck Surgery] 2005;4(4):166-70. [CENTRAL: CN-00849154] [Google Scholar]
Scadding 2014 {published data only}
- Scadding G, Rajput K, Parikh A, Hilss S, Jansz J A, Darby YC, et al. Double blind, placebo-controlled study of Flixonase with and without Otovent in the treatment of otitis media with effusion. In: 8th International Congress of Paediatric Otorhinolaryngology (ESPO); 2002 Sep 11-14; Oxford, UK. 2002:92-3. [ABSTRACT NUMBER: 21.04] [CENTRAL: CN-00431597]
- Scadding GK, Darby YC, Jansz AJ, Richards D, Tate H, Hills S, et al. Double-blind, placebo controlled randomised trial of medical therapy in otitis media with effusion. Advances in Life Sciences and Health 2014;1(2):1-11. [CENTRAL: CN-01043521] [Google Scholar]
Stangerup 1992 {published data only}
- Stangerup S, Tos M. Autoinflation in the treatment of Eustachian tube dysfunction, secretory otitis media and its sequelae. In: Mogi G (editor), editors(s). Recent Advances in Otitis Media. Amsterdam/New York: Kugler Publications, 1994:759-63. [CENTRAL: CN-01214464] [Google Scholar]
- Stangerup SE, Sederberg-Olsen J, Balle V. Autoinflation as a treatment of secretory otitis media. A randomized controlled study. Archives of Otolaryngology--Head & Neck Surgery 1992;118(2):149-52. [CENTRAL: CN-00082084] [PMID: ] [DOI] [PubMed] [Google Scholar]
Williamson 2015a {published data only}ISRCTN55208702
- ISRCTN55208702. An open randomised study of autoinflation in 4-11 year old school children with otitis media with effusion (OME) in primary care [Study of autoinflation in 4-11 year old school children with glue ear]. https://www.isrctn.com/ISRCTN55208702 (first received 16 June 2011). [CENTRAL: CN-01012774]
- Williamson I, Vennik J, Harnden A, Voysey M, Perera R, Breen M, et al. An open randomised study of autoinflation in 4- to 11-year-old school children with otitis media with effusion in primary care. Health Technology Assessment (Winchester, England) 2015;19(72):1-150. [CENTRAL: CN-01098789] [EMBASE: 606141685] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williamson I, Vennik J, Harnden A, Voysey M, Perera R, Kelly S, et al. Effect of nasal balloon autoinflation in children with otitis media with effusion in primary care: an open randomized controlled trial. CMAJ: Canadian Medical Association Journal 2015;187(13):961-9. [CENTRAL: CN-01078404] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Williamson 2015b {published data only}
- Williamson I, Vennik J, Harnden A, Voysey M, Perera R, Breen M, et al. An open randomised study of autoinflation in 4- to 11-year-old school children with otitis media with effusion in primary care. Health Technology Assessment (Winchester, England) 2015;19(72):1-150. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Ardehali 2008 {published data only}
- Ardehali MM, Seraj JM, Asiabar MK, Adibi H. The possible role of gastroesophageal reflux disease in children suffering from chronic otitis media with effusion. Acta Medica Iranica 2008;46(1):33-7. [CENTRAL: CN-00708224] [EMBASE: 351792703] [Google Scholar]
Bidarian‐Moniri 2016 {published data only}
- Bidarian-Moniri A. Autoinflation reduces middle ear effusion in children with otitis media with effusion. Evidence Based Medicine 2016;21(2):65-5. [CENTRAL: CN-02197786] [DOI] [PMC free article] [PubMed] [Google Scholar]
ChiCTR2000035008 {published data only}
- ChiCTR2000035008. Multicenter randomized controlled study of APONSTEM eustachian tube balloon as a treatment for children with recurrent chronic secretory otitis media. http://www.who.int/trialsearch/Trial2.aspx?TrialID=ChiCTR2000035008 (first received 2020). [CENTRAL: CN-02184651]
Choung 2008 {published data only}
- Choung YH, Shin YR, Choi SJ, Park K, Park HY, Lee JB, et al. Management for the children with otitis media with effusion in the tertiary hospital. Clinical and Experimental Otorhinolaryngology 2008;1(4):201-5. [CENTRAL: CN-00671567] [DOI] [PMC free article] [PubMed] [Google Scholar]
De Nobili 2008 {published data only}
- De Nobili E, Bellomo A, De Nobili E, Bellomo A. Comparative evaluation of efficacy of crenotherapeutic Politzer with sulphurous water versus crenotherapeutic Politzer and autoinsufflation (Otovent) in patients with tubaric dysfunction and secretory otitis media [Studio comparativo dell’efficacia del Politzer crenoterapico con acqua sulfurea versus Politzer crenoterapico e autoinsufflazione domiciliare (metodo Otovent®) in pazienti affetti da disfunzione tubarica e otite media secretiva]. Medicina Clinica e Termale 2008;20(64):30-4. [CENTRAL: CN-00675975] [Google Scholar]
El Hachem 2012 {published data only}
- El Hachem N, Halimi M. New technique for the passive opening of the Eustachian tube. Tympanometry assessment of the effect of a new manipulation technique on the opening of the Eustachian tube in children less than six years with otitis media with or without effusion [Nouvelle technique passive d'ouverture de la trompe d'Eustache. Evaluation par tympanometrie de l'effet d'une nouvelle manipulation sur l'ouverture de la trompe d'Eustache chez les enfants de moins de six ans atteints d'une otite moyenne avec ou sans effusion]. Kinesitherapie 2012;132:25-33. [Google Scholar]
Endo 1997 {published data only}
- Endo LH, Antunes AB, Vidolin C, Bilecki MM, Magalhaes KVB. Secretory media otitis: clinical treatment vs placebo [Otite media secretora: tratamento clinco versus placebo]. Revista Brasileira de Otorrinolaringologia 1997;63(2):116-9. [CENTRAL: CN-00187118] [EMBASE: 27225833] [Google Scholar]
Ferrara 2005 {published data only}
- Ferrara S, Sammartano D, Ferrara P. Long-term management of recurrent otitis media with effusion in children. In: XVIII International Federation of Otorhinolaryngology Societies (IFOS) World Congress 2005 Jun 25-30; Rome (Italy). 2005. [CENTRAL: CN-00526409]
Gibson 1996 {published data only}
- Gibson PG, Stuart JE, Wlodarczyk J, Olson LG, Hensley MJ. Nasal inflammation and chronic ear disease in Australian Aboriginal children. Journal of Paediatrics and Child Health 1996;32(2):143-7. [CENTRAL: CN-00131589] [PMID: ] [DOI] [PubMed] [Google Scholar]
Head 1992 {published data only}
- Head M. Does nose blowing help hearing in glue ear? Nursing Times 1992;88(3):53. [CENTRAL: CN-00081595] [PMID: ] [PubMed] [Google Scholar]
Heaf 1991 {published data only}
- Heaf M, Hutchings S, Bunch K. Does nose blowing improve hearing in serous otitis? A community study. British Journal of General Practice 1991;41(350):377-9. [CENTRAL: CN-00612450] [PMID: ] [PMC free article] [PubMed] [Google Scholar]
Iino 1989 {published data only}
- Iino Y, Ishitoya J, Ikeda M, Ito Y, Usami M, Kawashiro N, et al. Factors on delayed recovery of otitis media with effusion in children--clinical and bacteriological study. Nihon Jibiinkoka Gakkai Kaiho 1989;92(8):1183-91. [CENTRAL: CN-00063873] [PMID: ] [DOI] [PubMed] [Google Scholar]
Leunig 1995 {published data only}
- Leunig A, Mees K. Autoinflation of the middle ear with Otovent [Mittelohrbeluftung mit dem otovent-latexmembran-system]. Laryngo- Rhino- Otologie 1995;74(6):352-4. [CENTRAL: CN-00392275] [EMBASE: 25203663] [DOI] [PubMed] [Google Scholar]
Li 2020 {published data only}
- Li H, Zhou Y, Huang J, Zhang L, Lou Z. Treatment of secretory otitis media with balloon dilation and tympanostomy tube insertion: a randomized controlled trial. Basic & Clinical Pharmacology & Toxicology 2020;127(Suppl 1):292-3. [CENTRAL: CN-02230226] [EMBASE: 633830686] [Google Scholar]
Li 2021 {published data only}
- Li SN, Huang YY, Hou SL, Wu Y, Shen JL, Wang L, et al. Effect of autoflation on the prognosis of otitis media with effusion in children. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke za Zhi [Chinese Journal of Otorhinolaryngology Head and Neck Surgery] 2021;56(6):573-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Marchisio 1998 {published data only}
- Marchisio P, Principi N, Passali D, Salpietro DC, Boschi G, Chetri G, et al. Epidemiology and treatment of otitis media with effusion in children in the first year of primary school. Acta Oto-laryngologica 1998;118(4):557-62. [CENTRAL: CN-00154484] [EMBASE: 1998254893] [PMID: ] [DOI] [PubMed] [Google Scholar]
NCT03534219 {published data only}
- NCT03534219. Efficacy of the Earpopper device in children with recurrent otitis media [Efficacy of the Earpopper device in children with recurrent otitis media: a randomized controlled trial]. https://clinicaltrials.gov/show/nct03534219 (first received 11 May 2018). [CENTRAL: CN-01601566]
Paradise 1997 {published data only}
- Paradise J, Campbell T, Dollaghan C, Feldman H, Bernard B, Colborn K, et al. Receptive vocabulary, cognition, and parent-rated behavior at age 3 years in relation to otitis media in the first 3 years of life. In: Abstract Book of the Association of Health Service Research. Vol. 14. 1997:350-1. [CENTRAL: CN-00452820]
Parlea 2012 {published data only}
- Parlea E, Georgescu M, Calarasu R. Tympanometry as a predictor factor in the evolution of otitis media with effusion. Journal of Medicine and Life 2012;5(4):452-4. [CENTRAL: CN-00850240] [EMBASE: 369159817] [PMID: ] [PMC free article] [PubMed] [Google Scholar]
Rohail 2006 {published data only}
- Rohail A, Gill ZI, Butt MR. A comparison of medical treatment versus surgical treatment for the management of otitis media with effusion. Annals of King Edward Medical College 2006;12(1):64-7. [CENTRAL: CN-00597368] [Google Scholar]
Shubich 1996 {published data only}
- Shubich I. Otitis media with effusion and allergy control in children: a prospective study. In: Sixth International Symposium on Otitis Media; 1996; Fort Lauderdale (FL). 1996:173-4. [CENTRAL: CN-00452904]
Silman 2005 {published data only}
- Silman S, Arick DS, Emmer MB. Nonsurgical home treatment of middle ear effusion and associated hearing loss in children. Part II: validation study. Ear Nose & Throat Journal 2005;84(10):646-50. [CENTRAL: CN-00597170] [PMID: ] [PubMed] [Google Scholar]
Starcevic 2011 {published data only}
- Velepic M, Starcevic R, Bonifacic M, Ticac R, Kujundzic M, Udovic DS, et al. The clinical status of the eardrum: an inclusion criterion for the treatment of chronic secretory otitis media in children. International Journal of Pediatric Otorhinolaryngology 2011;75(5):686-90. [CENTRAL: CN-00784332] [EMBASE: 51315541] [PMID: ] [DOI] [PubMed] [Google Scholar]
Stenstrom 2005 {published data only}
- Stenstrom R, Pless IB, Bernard P. Hearing thresholds and tympanic membrane sequelae in children managed medically or surgically for otitis media with effusion. Archives of Pediatrics & Adolescent Medicine 2005;159(12):1151-6. [CENTRAL: CN-00532329] [PMID: ] [DOI] [PubMed] [Google Scholar]
Tham 2018 {published data only}
- Tham T, Rahman L, Costantino P. Efficacy of a non-invasive middle ear aeration device in children with recurrent otitis media: a randomized controlled trial protocol. Contemporary Clinical Trials Communications 2018;12:92-7. [CENTRAL: CN-01652639] [EMBASE: 2001167167] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
Tawfik 2002 {published data only}
- Tawfik S, Belal A, Sorour W. A comparative study of the different treatment modalities of otitis media with effusion in children. In: 8th International Congress of Paediatric Otorhinolaryngology (ESPO). Oxford, UK, 11-14 September, 2002. 2002:151. [ABSTRACT NUMBER: P2.26] [CENTRAL: CN-00508402]
References to ongoing studies
INFLATE (ACTRN12617001652369) {published data only}
- ACTRN12617001652369. Autoinflation for Aboriginal and Torres Strait Islander children with bilateral OME (middle ear infection) [A multi-centre randomised controlled trial to compare the efficacy of nasal balloon autoinflation versus no nasal balloon autoinflation for bilateral otitis media with effusion in Aboriginal and Torres Strait Islander children]. http://www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12617001652369 (first received 2017). [CENTRAL: CN-01896354]
- Walsh R, Reath J, Gunasekera H, Leach A, Kong K, Askew D, et al. INFLATE: a protocol for a randomised controlled trial comparing nasal balloon autoinflation to no nasal balloon autoinflation for otitis media with effusion in Aboriginal and Torres Strait Islander children. Trials 2022;23(1):309. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT00393159 {published data only}
- NCT00393159. The influence of The Ear Popper on serous otitis media and on the accompanying conductive hearing loss in children. https://clinicaltrials.gov/show/NCT00393159 (first received 26 October 2006). Accessed 15/01/2023. [CENTRAL: CN-01038104]
NCT02038400 {published data only}
- NCT02038400. Evaluation of the efficiency of KINETUBE® in the recurrent chronic tubal ear otitis care (otitis media with effusion, atelectatic otitis or retraction) in children with an age range of 7-15 years. https://clinicaltrials.gov/show/NCT02038400 (first received 16 January 2014). Accessed 15/01/2023. [CENTRAL: CN-00921546]
NCT02546518 {published data only}
- NCT02546518. A comparison of surgical and a new non-surgical treatment methods for secretory otitis media in children- hearing and socioeconomic aspects. https://clinicaltrials.gov/show/nct02546518 (first received 11 September 2015). Accessed 15/01/2023. [CENTRAL: CN-01102072]
NCT05324696 {published data only}
- NCT05324696. Autoinflation: alternative in the treatment of otitis media with effusion (OME). https://clinicaltrials.gov/show/NCT05324696 (first received 12 April 2022). Accessed 15/01/2023.
Additional references
Abidin 1995
- Abidin RR. Parenting Stress Index: Professional Manual. Third edition. Odessa, FL: Psychological Assessment Resources, 1995. [Google Scholar]
Achenbach 2011
- Achenbach TM. Child Behavior Checklist. In: Kreutzer JS, DeLuca J, Caplan B, editors(s). Encyclopedia of Clinical Neuropsychology. New York, NY: Springer, 2011. [DOI: 10.1007/978-0-387-79948-3_1529] [DOI] [Google Scholar]
Bayley 2006
- Bayley N. Bayley Scales of Infant and Toddler Development. 3rd edition. San Antonio, TX: Harcourt Assessment, Inc, 2006. [Google Scholar]
Berkman 2013
- Berkman ND, Wallace IF, Steiner MJ, Harrison M, Greenblatt AM, Lohr KN, et al. Otitis media with effusion: comparative effectiveness of treatments [Internet]. Report No.: 13-EHC091-EF edition. Vol. 1. Rockville (MD): Agency for Healthcare Research and Quality (US), 2013. [PubMed] [Google Scholar]
Bruce 2015
- Bruce I, Harman N, Williamson P, Tierney S, Callery P, Mohiuddin S, et al. The management of Otitis Media with Effusion in children with cleft palate (mOMEnt): a feasibility study and economic evaluation. Health Technology Assessment 2015;19(68):1-374. [DOI: 10.3310/hta19680] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cochrane ENT 2020
- Cochrane ENT. Otitis media with effusion: a project to prioritise Cochrane systematic reviews. https://ent.cochrane.org/otitis-media-effusion-ome-glue-ear 2020 (accessed 3 November 2021).
Dewey 2000
- Dewey C, Midgeley E, Maw R. The relationship between otitis media with effusion and contact with other children in a british cohort studied from 8 months to 3 1/2 years. The ALSPAC Study Team. Avon Longitudinal Study of Pregnancy and Childhood. International Journal of Pediatric Otorhinolaryngology 2000;55(1):33-45. [DOI] [PubMed] [Google Scholar]
Dunn 2007
- Dunn LM, Dunn DM. Peabody Picture Vocabulary Test, Fourth Edition (PPVT™-4). Pearson Education, 2007. [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315(7109):629-34. [DOI: 10.1136/bmj.315.7109.629] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ejnell 2015a
- Ejnell H. A comparison of surgical and a new non-surgical treatment methods for secretory otitis media in children- hearing and socioeconomic aspects. https://clinicaltrials.gov/show/nct02546518 (first received 11 September 2015).
Ejnell 2015b
- Ejnell H. The effect of early non-surgical treatment of children with middle ear effusion on the hearing level and the health economics. https://clinicaltrials.gov/show/nct02549612 (first received 15 September 2015).
Fekkes 2000
- Fekkes M, Theunissen NC, Brugman E, Veen S, Verrips EG, Koopman HM, et al. Development and psychometric evaluation of the TAPQOL: a health-related quality of life instrument for 1–5-year-old children. Quality of Life Research 2000;9:961-72. [DOI: 10.1023/a:1008981603178] [DOI] [PubMed] [Google Scholar]
Goodman 1997
- Goodman R. The Strengths and Difficulties Questionnaire: a research note. Journal of Child Psychology and Psychiatry 1997;38:581-6. [DOI: 10.1111/j.1469-7610.1997.tb01545.x] [DOI] [PubMed] [Google Scholar]
Gresham 1990
- Gresham FM, Elliott SN. Social Skills Rating System. Circle Pines, MN: American Guidance Service, 1990. [Google Scholar]
Griffiths 1996
- Griffiths R. The Griffiths Mental Development Scales from Birth to Two Years, manual, the 1996 revision. Henley: Association for Research in Infant and Child Development, Test Agency, 1996. [Google Scholar]
Haggard 2003
- Haggard MP, Smith SC, Nicholls EE. Quality of life and child behaviour. In: Rosenfeld RM, Bluestone CD, editors(s). Evidence-based Otitis Media. 2nd edition. Hamilton, Ontario: BC Decker Inc, 2003:401-29. [https://researchonline.lshtm.ac.uk/id/eprint/15108] [Google Scholar]
Handbook 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org.
Hedrick 1984
- Hedrick DL, Prather EM, Tobin AR. Sequenced Inventory of Communication Development. Seattle, WA: University of Washington Press, 1984. [Google Scholar]
Higgins 2021
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook. [DOI] [PMC free article] [PubMed]
Jellinek 1988
- Jellinek MS, Murphy JM, Robinson J, Feins A, Lamb S, Fenton T. Pediatric Symptom Checklist: screening school-age children for psychosocial dysfunction. Journal of Pediatrics 1988;112(2):201-9. [DOI: 10.1016/s0022-3476(88)80056-8] [DOI] [PubMed] [Google Scholar]
Kreiner‐Møller 2012
- Kreiner-Møller E, Chawes BL, Caye-Thomasen P, Bønnelykke K, Bisgaard H. Allergic rhinitis is associated with otitis media with effusion: a birth cohort study. Clinical and Experimental Allergy 2012;42(11):1615-20. [DOI: 10.1111/j.1365-2222.2012.04038.x] [DOI] [PubMed] [Google Scholar]
Landgraf 1994
- Landgraf JM. The Infant/Toddler Child Health Questionnaire: conceptual framework, logic content, and preliminary psychometric results. Boston: Health Act, 1994. [Google Scholar]
Landgraf 1996
- Landgraf JL, Abetz L, Ware JE. The CHQ User’s Manual. Boston: The Health Institute, New England Medical Center, 1996. [Google Scholar]
Lefebvre 2020
- Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf M-I, et al. Chapter 4: Searching for and selecting studies. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook.
Liu 2020
- Liu PZ, Ismail-Koch H, Stephenson K, Donne AJ, Fergie N, Derry J, et al. A core outcome set for research on the management of otitis media with effusion in otherwise-healthy children. International Journal of Pediatric Otorhinolaryngology 2020;134:110029. [DOI: 10.1016/j.ijporl.2020] [DOI] [PubMed] [Google Scholar]
MacKeith 2022a
- MacKeith S, Mulvaney CA, Galbraith K, Marom T, Daniel M, Venekamp RP, et al. Ventilation tubes (grommets) for otitis media with effusion (OME) in children. Cochrane Database of Systematic Reviews 2022, Issue 3. Art. No: CD015215. [DOI: 10.1002/14651858.CD015215] [DOI] [PMC free article] [PubMed] [Google Scholar]
MacKeith 2022b
- MacKeith S, Mulvaney CA, Galbraith K, Marom T, Daniel M, Venekamp RP, et al. Adenoidectomy for otitis media with effusion (OME) in children. Cochrane Database of Systematic Reviews 2022, Issue 4. Art. No: CD015252. [DOI: 10.1002/14651858.CD015252] [DOI] [PMC free article] [PubMed] [Google Scholar]
Marseglia 2008
- Marseglia GL, Pagella F, Caimmi D, Caimmi S, Castellazzi AM, Poddighe D, et al. Increased risk of otitis media with effusion in allergic children presenting with adenoiditis. Otolaryngology – Head and Neck Surgery 2008;138(5):572-5. [DOI: 10.1016/j.otohns.2008.01.020] [DOI] [PubMed] [Google Scholar]
Marshall 2018
- Marshall J, Noel-Storr AH, Kuiper J, Thomas J, Wallace BC. Machine learning for identifying randomized controlled trials: an evaluation and practitioner's guide. Research Synthesis Methods 2018;9(4):602-14. [DOI: 10.1002/jrsm.1287] [DOI] [PMC free article] [PubMed] [Google Scholar]
Marx 1995
- Marx J, Osguthorpe JD, Parsons G. Day care and the incidence of otitis media in young children. Otolaryngology Head and Neck Surgery 1995;112(6):695-9. [DOI] [PubMed] [Google Scholar]
McCarthy 1972
- McCarthy D. Manual for the McCarthy Scales of Children's Abilities. New York: Psychological Corp, 1972. [Google Scholar]
McDonald 2017
- McDonald S, Noel-Storr AH, Thomas J. Harnessing the efficiencies of machine learning and Cochrane Crowd to identify randomised trials for individual Cochrane reviews. In: Global Evidence Summit; 2017 Sep 13-17; Cape Town, South Africa. 2017.
Mulvaney 2022a
- Mulvaney CA, Galbraith K, MacKeith S, Marom T, Daniel M, Venekamp RP, et al. Antibiotics for otitis media with effusion (OME) in children. Cochrane Database of Systematic Reviews 2022, Issue 4. Art. No: CD015254. [DOI: 10.1002/14651858.CD015254] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mulvaney 2022b
- Mulvaney CA, Galbraith K, MacKeith S, Marom T, Daniel M, Venekamp RP, et al. Topical and oral steroids for otitis media with effusion (OME) in children. Cochrane Database of Systematic Reviews 2022, Issue 4. Art. No: CD015255. [DOI: 10.1002/14651858.CD015255] [DOI] [PMC free article] [PubMed] [Google Scholar]
NICE 2008
- NICE. Otitis media with effusion in under 12s: Otitis media with effusion in under 12s: surgery (CG60). Available at: https://www.nice.org.uk/guidance/cg60 2008 (accessed 3 November 2021).
NICE 2016
- National Institute for Health and Care Excellence. Otovent nasal balloon for otitis media with effusion. https://www.nice.org.uk/advice/mib59/resources/otovent-nasal-balloon-for-otitis-media-with-effusion-pdf-63499234925509 2016 (accessed 3 November 2021).
NICE 2023
- National Institute for Health and Care Excellence. Otitis media with effusion in under 12s. NICE guideline [NG233]; August 2023. https://www.nice.org.uk/guidance/ng233. [PubMed]
Noel‐Storr 2018
- Noel-Storr AH. Cochrane Crowd: new ways of working together to produce health evidence. In: Evidence Live; 2018 Jun 18-20; Oxford, UK. 2018.
Perera 2013
- Perera R, Glasziou P, Heneghan CJ, McLellan J, Williamson I. Autoinflation for hearing loss associated with otitis media with effusion. Cochrane Database of Systematic Reviews 2013, Issue 5. Art. No: CD006285. [DOI: 10.1002/14651858.CD006285.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rabin 2001
- Rabin R, Charro F. EQ-5D: a measure of health status from the EuroQol Group. Annals of Medicine 2001;33(5):337-43. [DOI: 10.3109/07853890109002087] [DOI] [PubMed] [Google Scholar]
RACGP 2016
- The Royal Australian College of General Practitioners. Autoinflation: glue ear. https://www.racgp.org.au/getattachment/14295770-1083-475d-b7ae-8d43d7ecfb69/Autoinflation-for-glue-ear-in-children.aspx 2016 (accessed 3 November 2021).
RevMan 2014 [Computer program]
- Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Reynell 1985
- Reynell JH. Reynell Development Language Scales Manual. 2nd edition. Windsor, UK: NFER-Nelson, 1985. [Google Scholar]
Rosenfeld 1997
- Rosenfeld RM, Goldsmith AJ, Tetlus L, Balzano A. Quality of life for children with otitis media. Archives of Otolaryngology - Head & Neck surgery 1997;123:1049-54. [DOI: 10.1001/archotol.1997.01900100019002] [DOI] [PubMed] [Google Scholar]
Rosenfeld 2000
- Rosenfeld RM, Bhaya MH, Bower CM, Brookhouser PE, Casselbrant ML, Chan KH, et al. Impact of tympanostomy tubes on child quality of life. Archives of Otolaryngology - Head & Neck Surgery 2000;126:585-92. [DOI: 10.1001/archotol.126.5.585] [DOI] [PubMed] [Google Scholar]
Rosenfeld 2003
- Rosenfeld RM, Kay D. Natural history of untreated otitis media. Laryngoscope 2003;113:1645-57. [DOI] [PubMed] [Google Scholar]
Rosenfeld 2016
- Rosenfeld RM, Shin JJ, Schwartz SR, Coggins R, Gagnon L, Hackell JM, et al. Clinical practice guideline: otitis media with effusion (update). Otolaryngology - Head & Neck Surgery 2016;154:S1-S41. [DOI: 10.1177/0194599815623467] [DOI] [PubMed] [Google Scholar]
Rovers 2006
- Rovers MM, Kok IM, Schilder AG. Risk factors for otitis media: an international perspective. International Journal of Pediatric Otorhinolaryngology 2006;70(7):1251-6. [DOI] [PubMed] [Google Scholar]
Schlichting 2007
- Schlichting JEPT, Lutje Spelberg HC. Lexilijst Begrip: An instrument to investigate language comprehension in children aged 15-25 months in the context of early identification. Amsterdam: Pearson Assessment & Information BV, 2007. [Google Scholar]
Schlichting 2010
- Schlichting JEPT, Lutje Spelberg HC. Schlichting Test for Language Comprehension; Instruction manual. Wooden: Bohn Stafleu van Loghum, 2010. [Google Scholar]
Schmalbach 2021
- Schmalbach CE, Brereton J, Bowman C, Denneny JC. American Academy of Otolaryngology–Head and Neck Surgery/Foundation Reg-ent Registry: Purpose, Properties, and Priorities. Otolaryngology – Head and Neck Surgery 2021;164(5):964-71. [DOI] [PubMed] [Google Scholar]
Thomas 2017
- Thomas J, Noel-Storr AH, Marshall I, Wallace B, McDonald S, Mavergames C, et al, Living Systematic Review Network. Living systematic reviews 2: combining human and machine effort. Journal of Clinical Epidemiology 2017;91:31-7. [DOI] [PubMed] [Google Scholar]
TNO 1997
- TNO—Prevention and Health/LUMC. TAIQOL—Questionnaire for parents of children aged 1—5 years. Leiden, The Netherlands: Leiden University Medical Center, 1997. [Google Scholar]
Verrips 1998
- Verrips GH, Vogels AGC, Verloove-Vanhorick SP, Fekkes M, Koopman HM, Kamphuis RP, et al. Health-related quality of life measure for children - the TACQOL. Journal of Applied Therapeutics 1998;1(4):357-60. [Google Scholar]
Wallace 2017
- Wallace BC, Noel-Storr A, Marshall IJ, Cohen AM, Smalheiser NR, Thomas J. Identifying reports of randomized controlled trials (RCTs) via a hybrid machine learning and crowdsourcing approach. Journal of the American Medical Informatics Association 2017;24(6):1165-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wan 2014
- Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Medical Research Methodology 2014;14:135. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Williamson 2011
- Williamson I. Otitis media with effusion in children. BMJ Clinical Evidence 2011;2011:0502. [PMID: ] [PMC free article] [PubMed] [Google Scholar]
Williamson 2015
- Williamson I, Vennik J, Harnden A, Voysey M, Perera R, Kelly S, et al. Effect of nasal balloon autoinflation in children with otitis media with effusion in primary care: an open randomized controlled trial. Canadian Medical Association Journal 2015;187(13):961-9. [DOI: 10.1503/ cmaj.141608] [DOI] [PMC free article] [PubMed] [Google Scholar]
Zernotti 2017
- Zernotti ME, Pawankar R, Ansotegui I, Badellino H, Croce JS, Hossny E, et al. Otitis media with effusion and atopy: is there a causal relationship? World Allergy Organization Journal 2017;10(1):37. [DOI: 10.1186/s40413-017-0168-x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Zimmerman 1992
- Zimmerman IL, Steiner VG, Pond RE. Preschool Language Scale-3. San Antonio, TX: The Psychological Corporation, 1992. [Google Scholar]
References to other published versions of this review
Galbraith 2022
- Galbraith K, Mulvaney CA, MacKeith S, Marom T, Daniel M, Venekamp RP, et al. Autoinflation for otitis media with effusion (OME) in children. Cochrane Database of Systematic Reviews 2022, Issue 4. Art. No: CD015253. [DOI: 10.1002/14651858.CD015253] [DOI] [PMC free article] [PubMed] [Google Scholar]