

Abstract
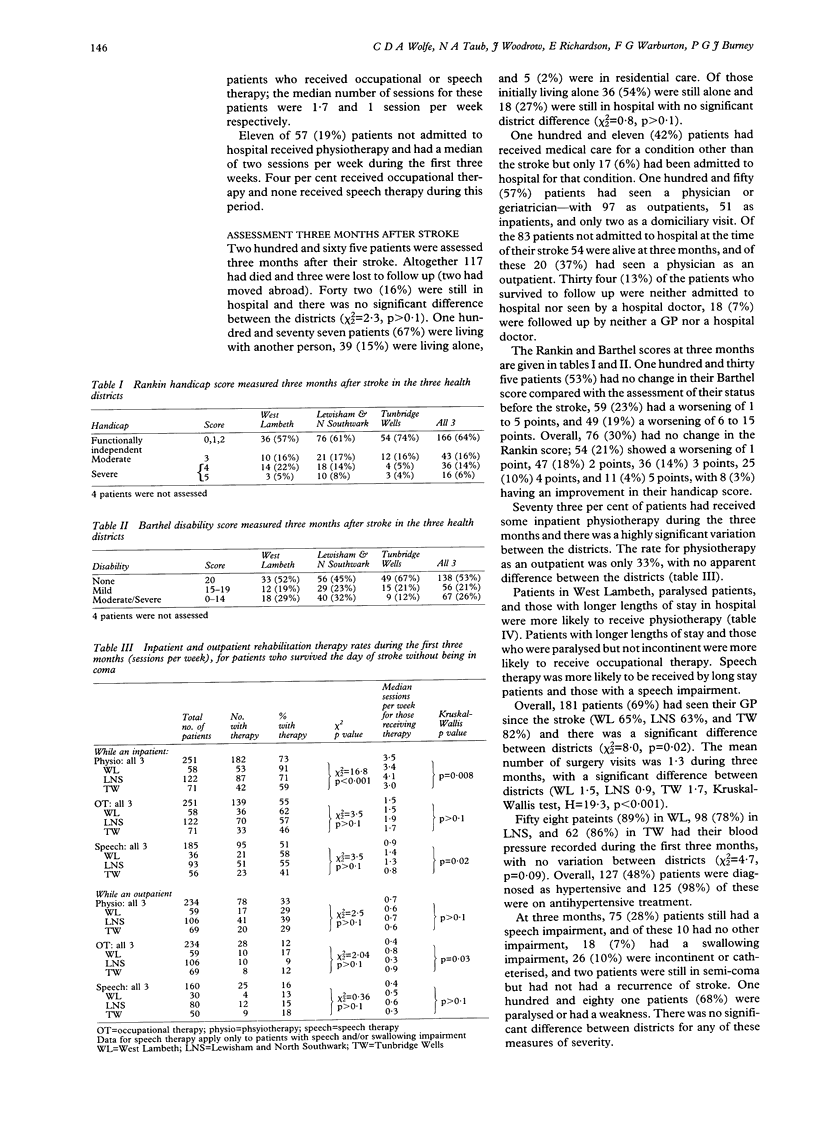
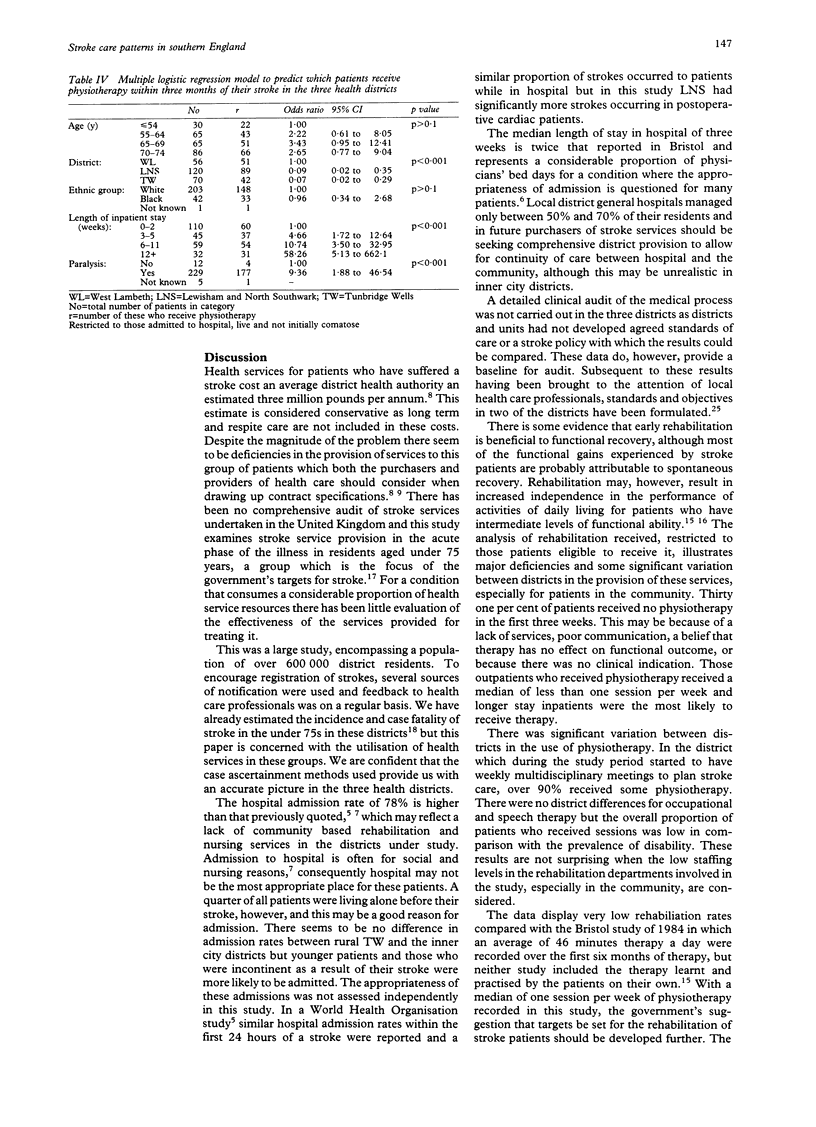
OBJECTIVE--To quantify the use of health care services by acutely ill stroke patients in three district health authorities. DESIGN--A follow up study of all patients recorded in population based registers who had a first ever stroke in three district health authorities, with assessment following the onset and three months after the stroke. SETTING--West Lambeth, Lewisham and North Southwark, and Tunbridge Wells District Health Authorities in south east England. SUBJECTS--All first time stroke patients under the age of 75 years who presented between 15 August 1989 and 14 August 1990. MEASUREMENTS AND MAIN RESULTS--Hospital admission rates, rates of use of rehabilitation services, and contact with medical practitioners together with assessment of disability and handicap were determined. A total of 386 strokes were registered. Seventy eight per cent were treated in hospital and younger and incontinent patients were significantly more likely to be admitted. The median stay was 21 days. Patients in West Lambeth, those paralysed, and those who stayed longer in hospital were more likely to receive physiotherapy. Altogether 265 patients were followed up, 117 having died within three months of the stroke. During the three months, 150 (57%) had seen a hospital physician and 181 (69%) their general practitioner, but 18 (7%) had seen neither. Sixty seven (26%) patients were moderately or severely disabled. Twenty seven per cent of inpatients had received no inpatient physiotherapy and 67% of all patients no outpatient physiotherapy during the three months. CONCLUSIONS--The hospital admission rates were high, with long lengths of stay. There were significant differences in the amount of rehabilitation received in each district. This was low overall, especially for those not admitted to hospital. As expected, patients admitted for long periods were the most likely to receive therapy. Before district policies for admission and management of stroke patients can be drawn up, increased knowledge of which aspects of stroke management are effective is needed. Policies should aim to provide planned, coordinated care between hospital and the community. It is striking that many patients received no form of rehabilitation therapy.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aho K., Harmsen P., Hatano S., Marquardsen J., Smirnov V. E., Strasser T. Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ. 1980;58(1):113–130. [PMC free article] [PubMed] [Google Scholar]
- Bamford J., Sandercock P., Dennis M., Burn J., Warlow C. A prospective study of acute cerebrovascular disease in the community: the Oxfordshire Community Stroke Project--1981-86. 2. Incidence, case fatality rates and overall outcome at one year of cerebral infarction, primary intracerebral and subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry. 1990 Jan;53(1):16–22. doi: 10.1136/jnnp.53.1.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bamford J., Sandercock P., Warlow C., Gray M. Why are patients with acute stroke admitted to hospital? Br Med J (Clin Res Ed) 1986 May 24;292(6532):1369–1372. doi: 10.1136/bmj.292.6532.1369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brocklehurst J. C., Andrews K., Morris P., Richards B. R., Laycock P. L. Why admit stroke patients to hospital? Age Ageing. 1978 May;7(2):100–108. doi: 10.1093/ageing/7.2.100. [DOI] [PubMed] [Google Scholar]
- Brocklehurst J. C., Andrews K., Richards B., Laycock P. J. How much physical therapy for patients with stroke? Br Med J. 1978 May 20;1(6123):1307–1310. doi: 10.1136/bmj.1.6123.1307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garraway W. M., Akhtar A. J., Hockey L., Prescott R. J. Management of acute stroke in the elderly: follow-up of a controlled trial. Br Med J. 1980 Sep 27;281(6244):827–829. doi: 10.1136/bmj.281.6244.827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kurtzke J. F. The current neurologic burden of illness and injury in the United States. Neurology. 1982 Nov;32(11):1207–1214. doi: 10.1212/wnl.32.11.1207. [DOI] [PubMed] [Google Scholar]
- Malmgren R., Bamford J., Warlow C., Sandercock P., Slattery J. Projecting the number of patients with first ever strokes and patients newly handicapped by stroke in England and Wales. BMJ. 1989 Mar 11;298(6674):656–660. doi: 10.1136/bmj.298.6674.656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- RANKIN J. Cerebral vascular accidents in patients over the age of 60. II. Prognosis. Scott Med J. 1957 May;2(5):200–215. doi: 10.1177/003693305700200504. [DOI] [PubMed] [Google Scholar]
- Smith D. S., Goldenberg E., Ashburn A., Kinsella G., Sheikh K., Brennan P. J., Meade T. W., Zutshi D. W., Perry J. D., Reeback J. S. Remedial therapy after stroke: a randomised controlled trial. Br Med J (Clin Res Ed) 1981 Feb 14;282(6263):517–520. doi: 10.1136/bmj.282.6263.517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevens R. S., Ambler N. R., Warren M. D. A randomized controlled trial of a stroke rehabilitation ward. Age Ageing. 1984 Mar;13(2):65–75. doi: 10.1093/ageing/13.2.65. [DOI] [PubMed] [Google Scholar]
- Wade D. T., Hewer R. L., David R. M., Enderby P. M. Aphasia after stroke: natural history and associated deficits. J Neurol Neurosurg Psychiatry. 1986 Jan;49(1):11–16. doi: 10.1136/jnnp.49.1.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wade D. T., Hewer R. L. Functional abilities after stroke: measurement, natural history and prognosis. J Neurol Neurosurg Psychiatry. 1987 Feb;50(2):177–182. doi: 10.1136/jnnp.50.2.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wade D. T., Langton Hewer R. Hospital admission for acute stroke: who, for how long, and to what effect? J Epidemiol Community Health. 1985 Dec;39(4):347–352. doi: 10.1136/jech.39.4.347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wade D. T., Langton-Hewer R., Skilbeck C. E., Bainton D., Burns-Cox C. Controlled trial of a home-care service for acute stroke patients. Lancet. 1985 Feb 9;1(8424):323–326. doi: 10.1016/s0140-6736(85)91091-8. [DOI] [PubMed] [Google Scholar]
- Wade D. T., Skilbeck C. E., Hewer R. L., Wood V. A. Therapy after stroke: amounts, determinants and effects. Int Rehabil Med. 1984;6(3):105–110. doi: 10.3109/03790798409165926. [DOI] [PubMed] [Google Scholar]
- Wolfe C. D., Taub N. A., Woodrow E. J., Burney P. G. Assessment of scales of disability and handicap for stroke patients. Stroke. 1991 Oct;22(10):1242–1244. doi: 10.1161/01.str.22.10.1242. [DOI] [PubMed] [Google Scholar]
- Wolfe C. D., Taub N. A., Woodrow J., Richardson E., Warburton F. G., Burney P. G. Does the incidence, severity, or case fatality of stroke vary in southern England? J Epidemiol Community Health. 1993 Apr;47(2):139–143. doi: 10.1136/jech.47.2.139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Swieten J. C., Koudstaal P. J., Visser M. C., Schouten H. J., van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1988 May;19(5):604–607. doi: 10.1161/01.str.19.5.604. [DOI] [PubMed] [Google Scholar]