

Abstract
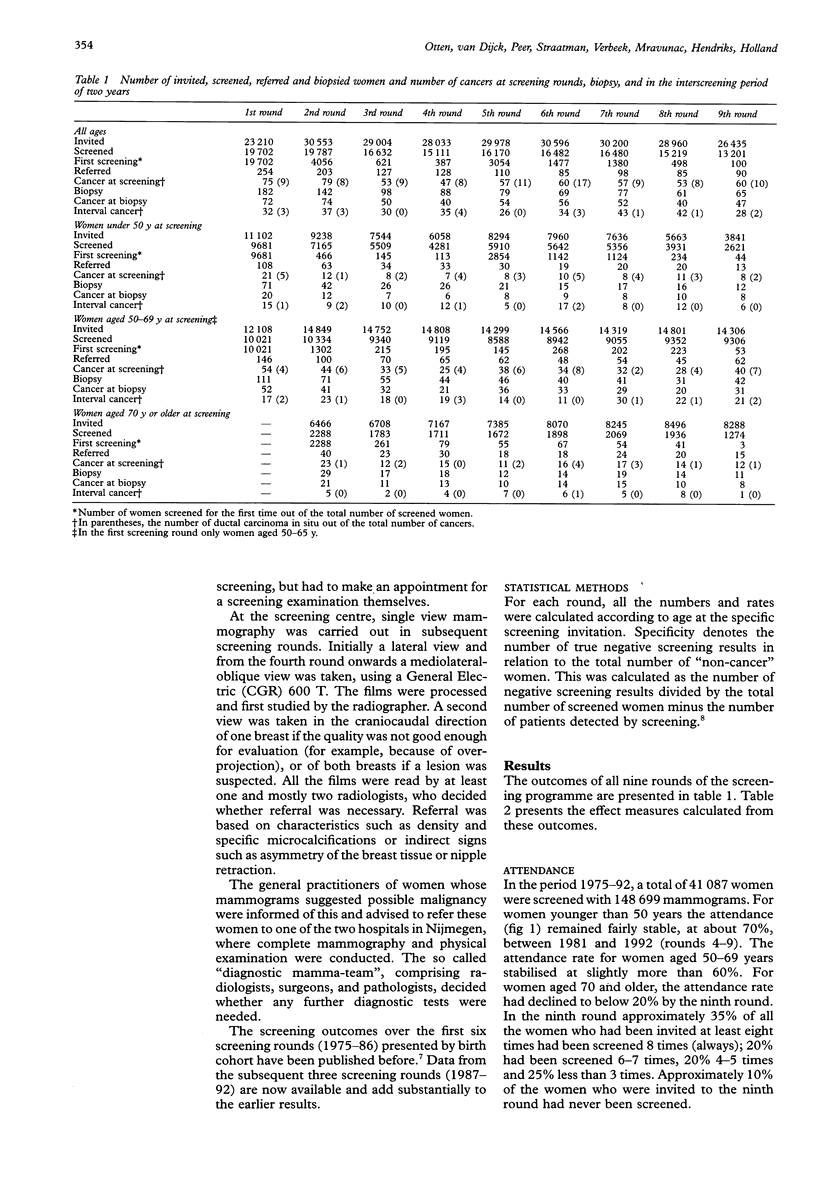
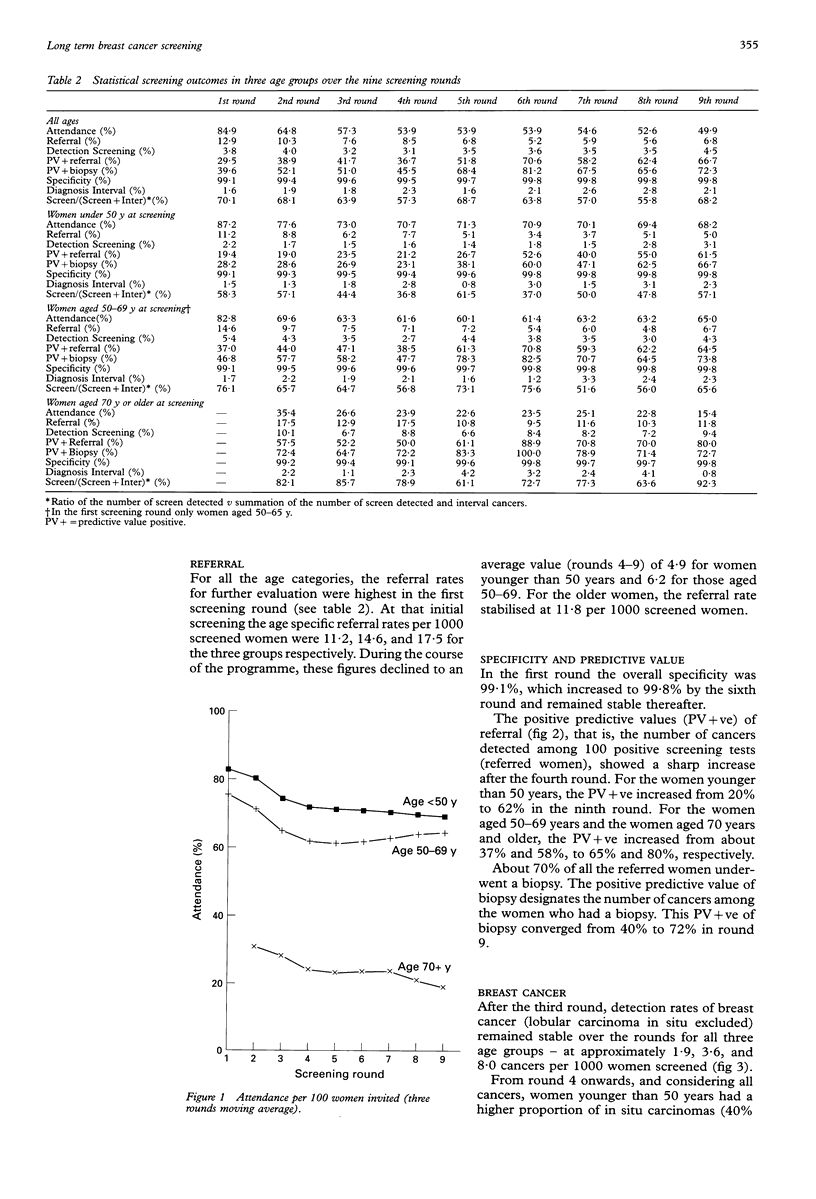
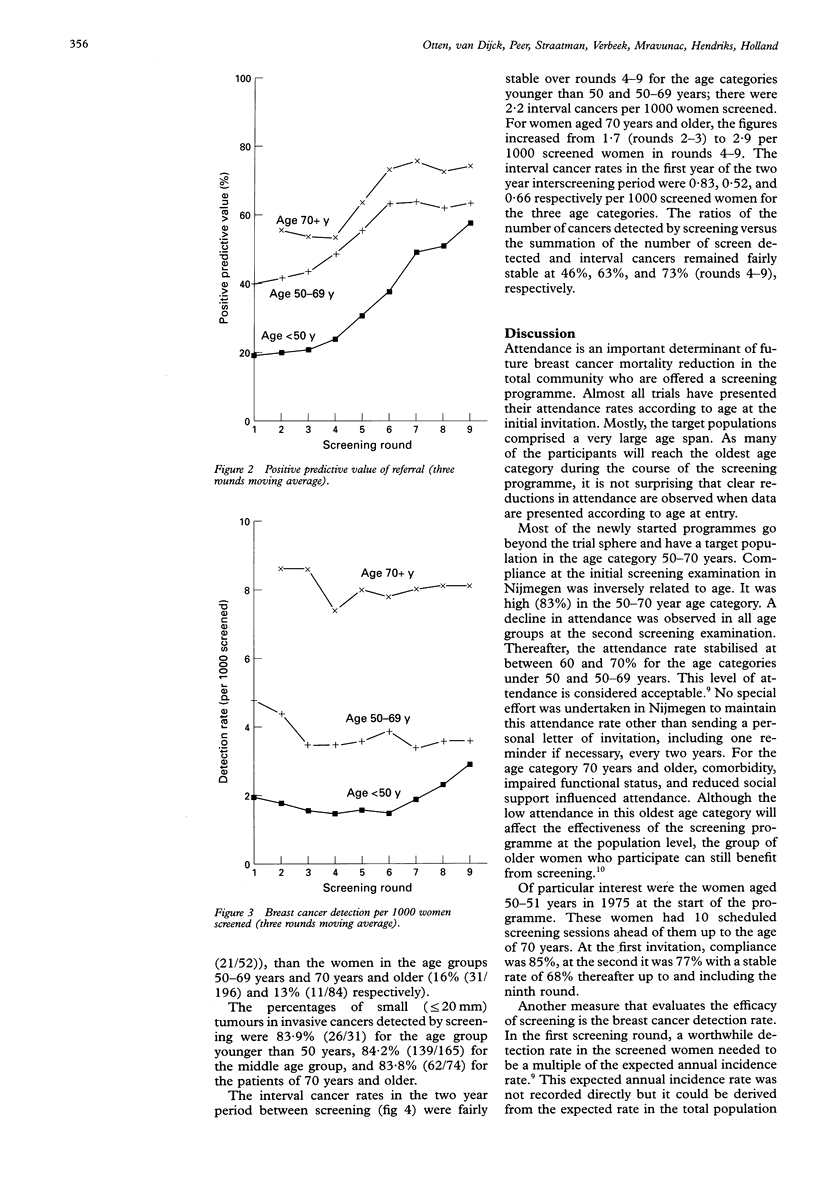
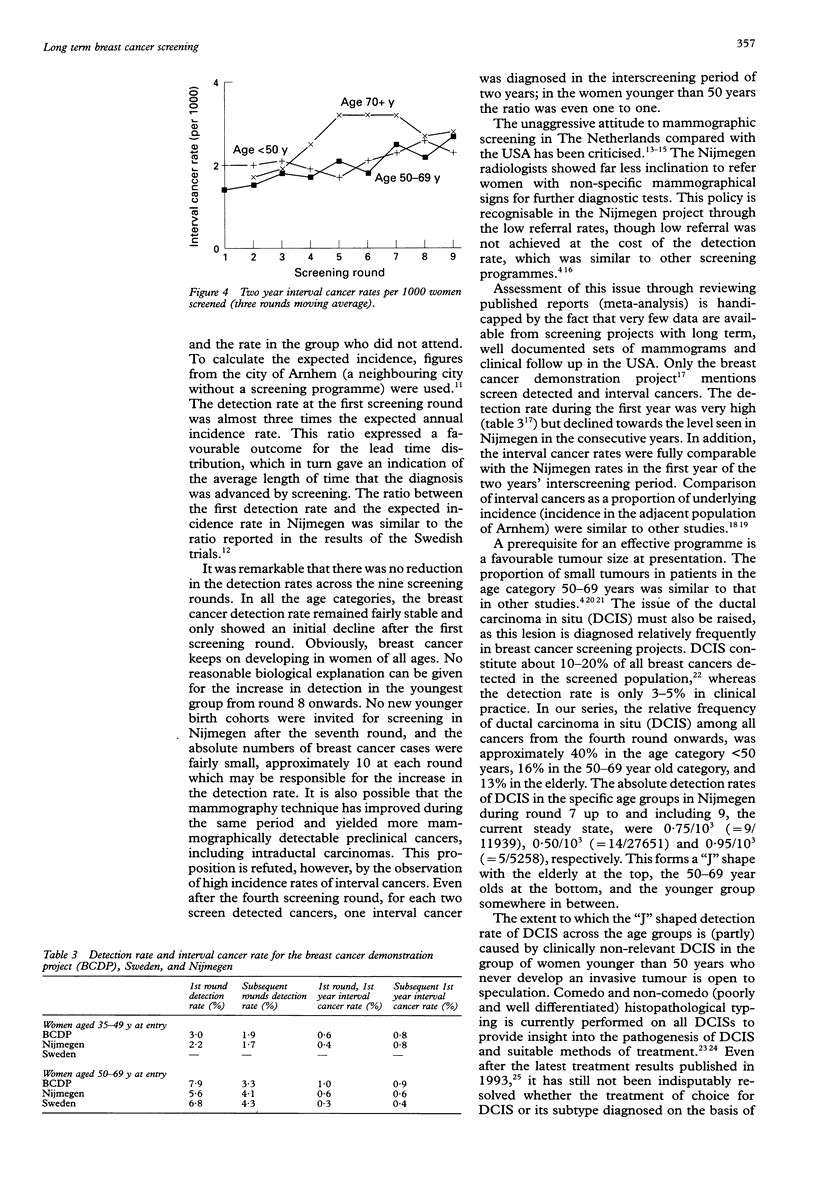
STUDY OBJECTIVE: To assess the performance of breast cancer screening in different age categories over two decades. DESIGN: Important determinants of reduced breast cancer mortality such as attendance, mammography performance, cancer detection, and disease stage were recorded. SETTING: Nijmegen, The Netherlands, 1975-92. SUBJECTS: Since 1975 more than 40,000 women aged 35 years and older have been invited biennially for breast screening in a population based project in Nijmegen. MAIN RESULTS: Rates of attendance, referral, detection, and disease stage were calculated, as well as the specificity of screening mammography and the predictive value of referral and biopsy. From round 3 onwards, the attendance rate of women younger than 50 years stabilised at 70%, in women of 50-69 years it was 62%, and in women aged 70 and over it was 22%. In these three age categories, the referral rates of a positive screening mammography per 1000 screened women were 4.9, 6.2, and 11.8, respectively. Specificity rates were between 99% and 100%. Current predictive values of referral were high: in the specific age categories 39%, 59%, and 68% of the referred women had cancer. Detection rates remained fairly stable over the rounds 4-9, at 1.9, 3.6, and 8.0 cancers per 1000 screened women. In the two year period between screening the numbers of interval cancers per 1000 screened women were 2.2, 2.2, and 2.9, for the three age categories respectively. With regard to invasive cancers detected during screening, the percentage of small tumours (< or = 20 mm on the mammogram) was 84% in each age category. For women younger than 50 years, the proportion of intraductal carcinoma in all the cancers detected at screening was 40%, while it was 15% in the other age categories. CONCLUSION: Throughout the nine rounds, the screening outcomes were found to be adequate, particularly considering the high specificity rate and the predictive value of referral without the interference of a low detection rate. Although the occurrence of interval cancers seemed high, it was similar to other screening programmes. Despite a relatively low referral rate, the ratios of screen detected versus interval cancer cases were favourable. Well organised screening programmes can achieve good mammography results without too many false positives. It is important that women continue to participate in a screening programme because cancer can still be detected even after several successive negative screening examinations.
Full text
PDF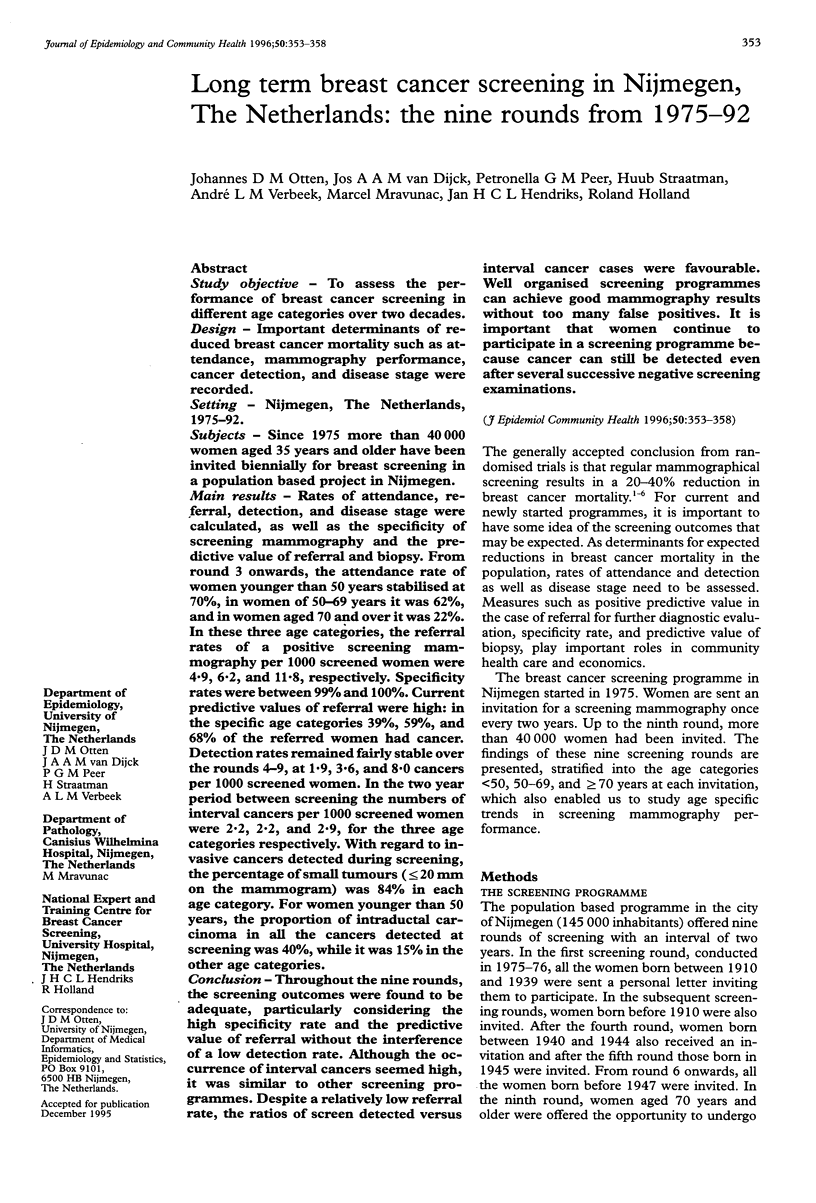
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson T. J., Lamb J., Donnan P., Alexander F. E., Huggins A., Muir B. B., Kirkpatrick A. E., Chetty U., Hepburn W., Smith A. Comparative pathology of breast cancer in a randomised trial of screening. Br J Cancer. 1991 Jul;64(1):108–113. doi: 10.1038/bjc.1991.251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brecht J. G., Robra B. P. A graphic method of estimating the specificity of screening programmes from incomplete follow-up data. Methods Inf Med. 1987 Jan;26(1):53–58. [PubMed] [Google Scholar]
- Chamberlain J., Moss S. M., Kirkpatrick A. E., Michell M., Johns L. National Health Service breast screening programme results for 1991-2. BMJ. 1993 Aug 7;307(6900):353–356. doi: 10.1136/bmj.307.6900.353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Day N. E., Williams D. R., Khaw K. T. Breast cancer screening programmes: the development of a monitoring and evaluation system. Br J Cancer. 1989 Jun;59(6):954–958. doi: 10.1038/bjc.1989.203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher B., Costantino J., Redmond C., Fisher E., Margolese R., Dimitrov N., Wolmark N., Wickerham D. L., Deutsch M., Ore L. Lumpectomy compared with lumpectomy and radiation therapy for the treatment of intraductal breast cancer. N Engl J Med. 1993 Jun 3;328(22):1581–1586. doi: 10.1056/NEJM199306033282201. [DOI] [PubMed] [Google Scholar]
- Fletcher S. W., Black W., Harris R., Rimer B. K., Shapiro S. Report of the International Workshop on Screening for Breast Cancer. J Natl Cancer Inst. 1993 Oct 20;85(20):1644–1656. doi: 10.1093/jnci/85.20.1644. [DOI] [PubMed] [Google Scholar]
- Holland R., Connolly J. L., Gelman R., Mravunac M., Hendriks J. H., Verbeek A. L., Schnitt S. J., Silver B., Boyages J., Harris J. R. The presence of an extensive intraductal component following a limited excision correlates with prominent residual disease in the remainder of the breast. J Clin Oncol. 1990 Jan;8(1):113–118. doi: 10.1200/JCO.1990.8.1.113. [DOI] [PubMed] [Google Scholar]
- Holland R., Peterse J. L., Millis R. R., Eusebi V., Faverly D., van de Vijver M. J., Zafrani B. Ductal carcinoma in situ: a proposal for a new classification. Semin Diagn Pathol. 1994 Aug;11(3):167–180. [PubMed] [Google Scholar]
- Kopans D. B. Mammography screening for breast cancer. Cancer. 1993 Sep 15;72(6):1809–1812. doi: 10.1002/1097-0142(19930915)72:6<1809::aid-cncr2820720603>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- Moskowitz M. Breast cancer: age-specific growth rates and screening strategies. Radiology. 1986 Oct;161(1):37–41. doi: 10.1148/radiology.161.1.3532183. [DOI] [PubMed] [Google Scholar]
- Nyström L., Rutqvist L. E., Wall S., Lindgren A., Lindqvist M., Rydén S., Andersson I., Bjurstam N., Fagerberg G., Frisell J. Breast cancer screening with mammography: overview of Swedish randomised trials. Lancet. 1993 Apr 17;341(8851):973–978. doi: 10.1016/0140-6736(93)91067-v. [DOI] [PubMed] [Google Scholar]
- Paci E., Ciatto S., Buiatti E., Cecchini S., Palli D., Rosselli del Turco M. Early indicators of efficacy of breast cancer screening programmes. Results of the Florence District Programme. Int J Cancer. 1990 Aug 15;46(2):198–202. doi: 10.1002/ijc.2910460209. [DOI] [PubMed] [Google Scholar]
- Peeters P. H., Verbeek A. L., Hendriks J. H., van Bon M. J. Screening for breast cancer in Nijmegen. Report of 6 screening rounds, 1975-1986. Int J Cancer. 1989 Feb 15;43(2):226–230. doi: 10.1002/ijc.2910430209. [DOI] [PubMed] [Google Scholar]
- Peeters P. H., Verbeek A. L., Zielhuis G. A., Vooijs G. P., Hendriks J. H., Mravunac M. Breast cancer screening in women over age 50. A critical appraisal. Acta Radiol. 1990 May;31(3):225–231. [PubMed] [Google Scholar]
- Rutqvist L. E., Miller A. B., Andersson I., Hakama M., Hakulinen T., Sigfússon B. F., Tabár L. Reduced breast-cancer mortality with mammography screening--an assessment of currently available data. Int J Cancer Suppl. 1990;5:76–84. doi: 10.1002/ijc.2910460711. [DOI] [PubMed] [Google Scholar]
- Tabàr L., Fagerberg G., Duffy S. W., Day N. E., Gad A., Gröntoft O. Update of the Swedish two-county program of mammographic screening for breast cancer. Radiol Clin North Am. 1992 Jan;30(1):187–210. [PubMed] [Google Scholar]
- Verbeek A. L., Hendriks J. H., Holland R., Mravunac M., Sturmans F., Day N. E. Reduction of breast cancer mortality through mass screening with modern mammography. First results of the Nijmegen project, 1975-1981. Lancet. 1984 Jun 2;1(8388):1222–1224. doi: 10.1016/s0140-6736(84)91703-3. [DOI] [PubMed] [Google Scholar]
- Wald N., Frost C., Cuckle H. Breast cancer screening: the current position. BMJ. 1991 Apr 6;302(6780):845–846. doi: 10.1136/bmj.302.6780.845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woodman C. B., Threlfall A. G., Boggis C. R., Prior P. Is the three year breast screening interval too long? Occurrence of interval cancers in NHS breast screening programme's north western region. BMJ. 1995 Jan 28;310(6974):224–226. doi: 10.1136/bmj.310.6974.224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Dijck J. A., Holland R., Verbeek A. L., Hendriks J. H., Mravunac M. Efficacy of mammographic screening of the elderly: a case-referent study in the Nijmegen program in The Netherlands. J Natl Cancer Inst. 1994 Jun 15;86(12):934–938. doi: 10.1093/jnci/86.12.934. [DOI] [PubMed] [Google Scholar]
- van Dijck J. A., Verbeek A. L., Hendriks J. H., Holland R. The current detectability of breast cancer in a mammographic screening program. A review of the previous mammograms of interval and screen-detected cancers. Cancer. 1993 Sep 15;72(6):1933–1938. doi: 10.1002/1097-0142(19930915)72:6<1933::aid-cncr2820720623>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]