

Abstract
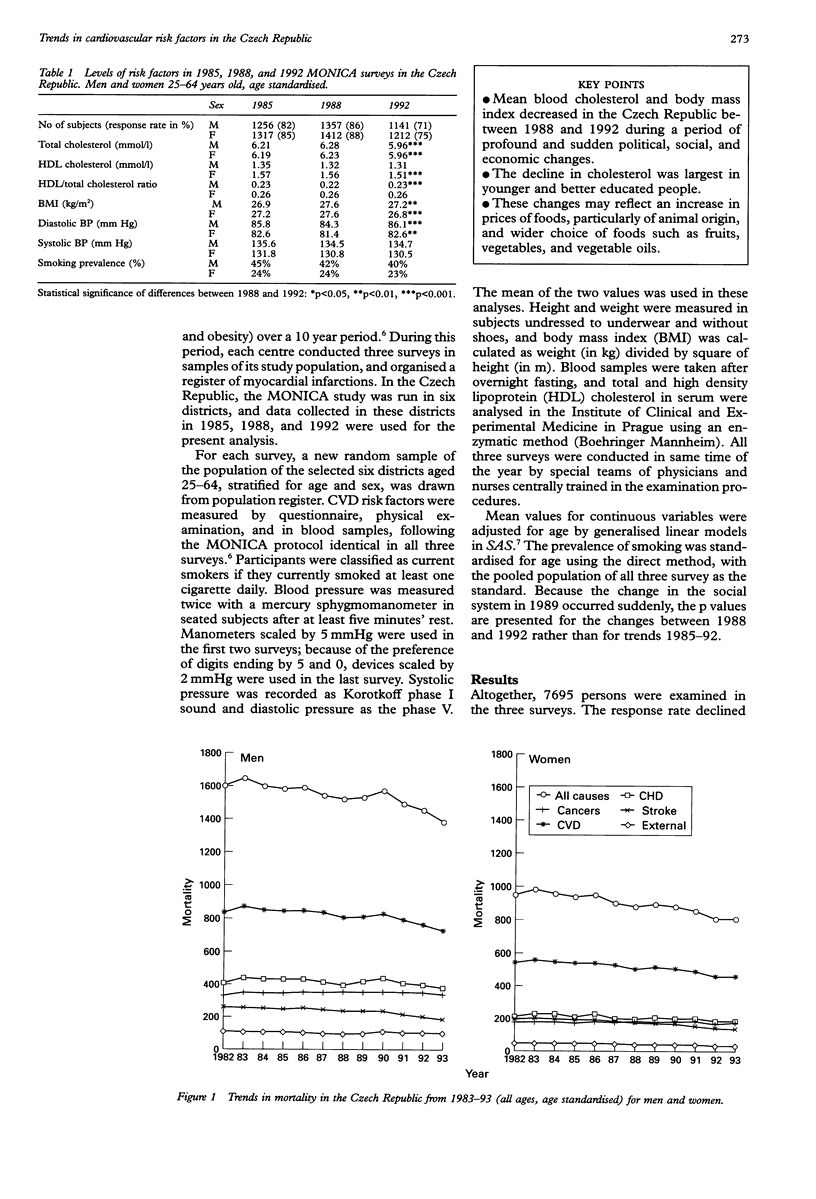
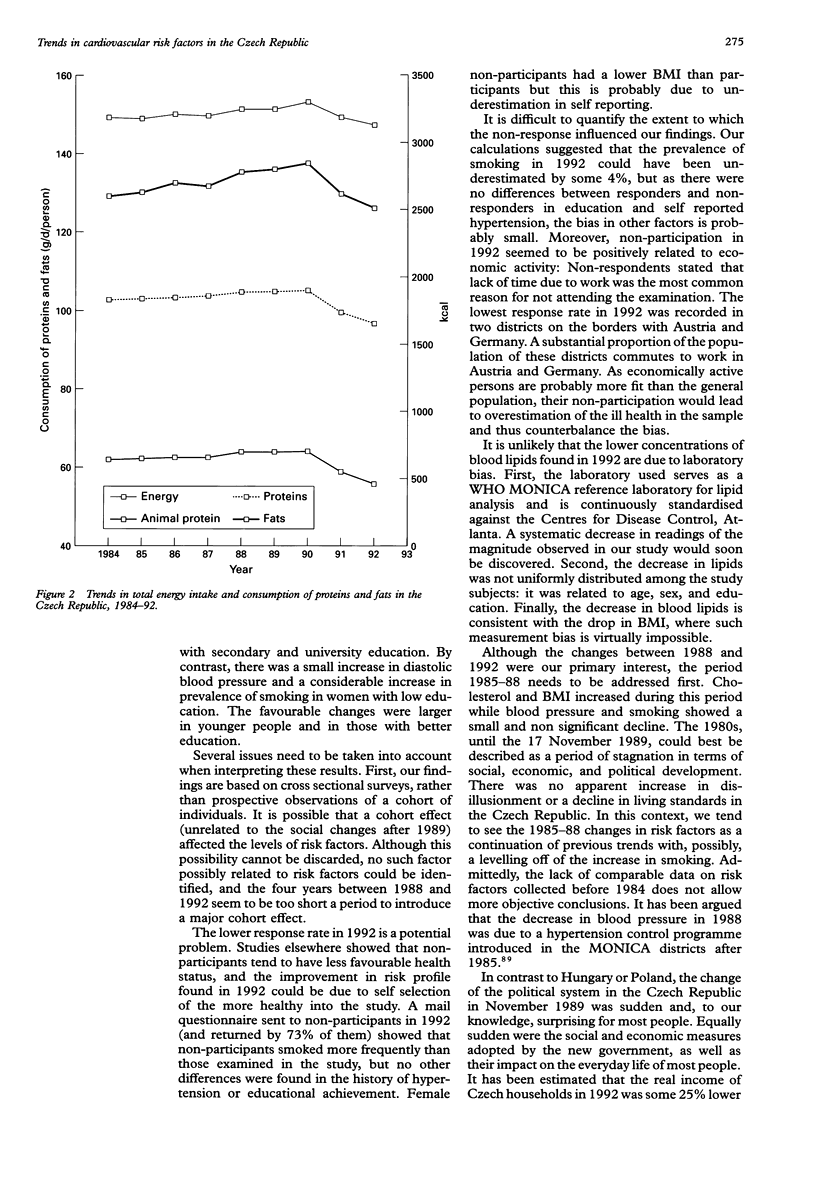
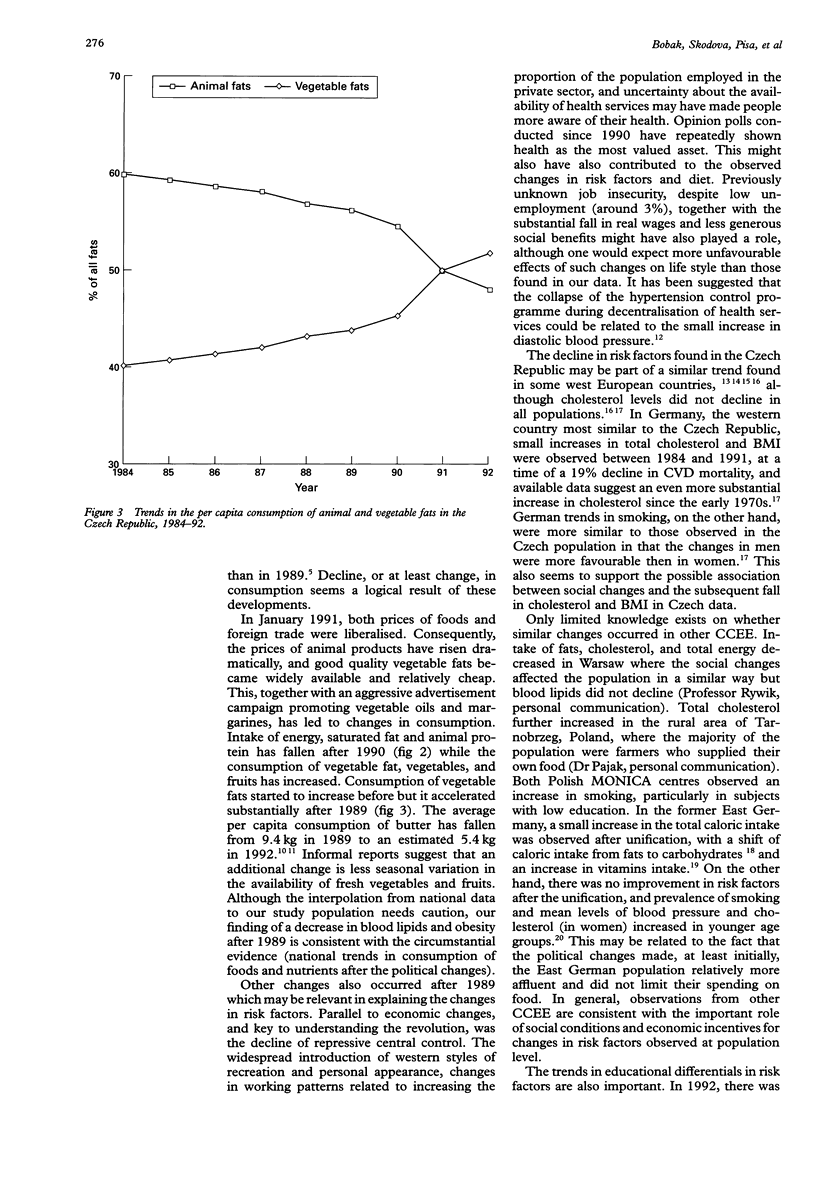
BACKGROUND: Mortality from cardiovascular diseases is substantially higher in central and eastern Europe than in the west. After the fall of communism, these countries have undergone radical changes in their political, social, and economic environments but little is known about the impact of these changes on health behaviours or risk factors. Data from the Czech Republic, a country whose mortality rates from cardiovascular diseases are among the highest, were analysed in this report. OBJECTIVES: To examine the trends in cardiovascular risk factors in Czech population over the last decade during which a major and sudden change of the political and social system occurred in 1989, and whether the trends differed in relation to age and educational group. DESIGN AND SETTING: Data from three cross sectional surveys conducted in 1985, 1988, and 1992 as a part of the MONICA project were analysed. The surveys examined random samples of men and women aged 25-64 in six Czech districts and measured the following risk factors: smoking, blood pressure, body mass index (BMI), and total and high density lipoprotein (HDL) cholesterol. RESULTS: The numbers of subjects (response rate) examined were 2573 (84%) in 1985, 2769 (87%) in 1988, and 2353 (73%) in 1992. Total cholesterol and body mass index increased between 1985 and 1988 and decreased between 1988 and 1992. The prevalence of smoking was declining slightly in men between 1985 and 1992 but remained stable in women. There were only small changes in blood pressure. The decline in cholesterol and BMI in 1988-92 may be related to changes in foods consumption after the price deregulation in 1991. An improvement in risk profile was more pronounced in younger age groups, and the declines in cholesterol and obesity were substantially larger in men and women with higher education. By contrast, there was an increase in smoking in women educated only to primary level. CONCLUSION: Substantial changes in cholesterol, obesity, and women's smoking occurred in the Czech population after the political changes in 1989. Although a causal association cannot be claimed, national trends in foods consumption are consistent with changes in blood lipids and obesity. Further monitoring of trends is required to confirm these trends.
Full text
PDF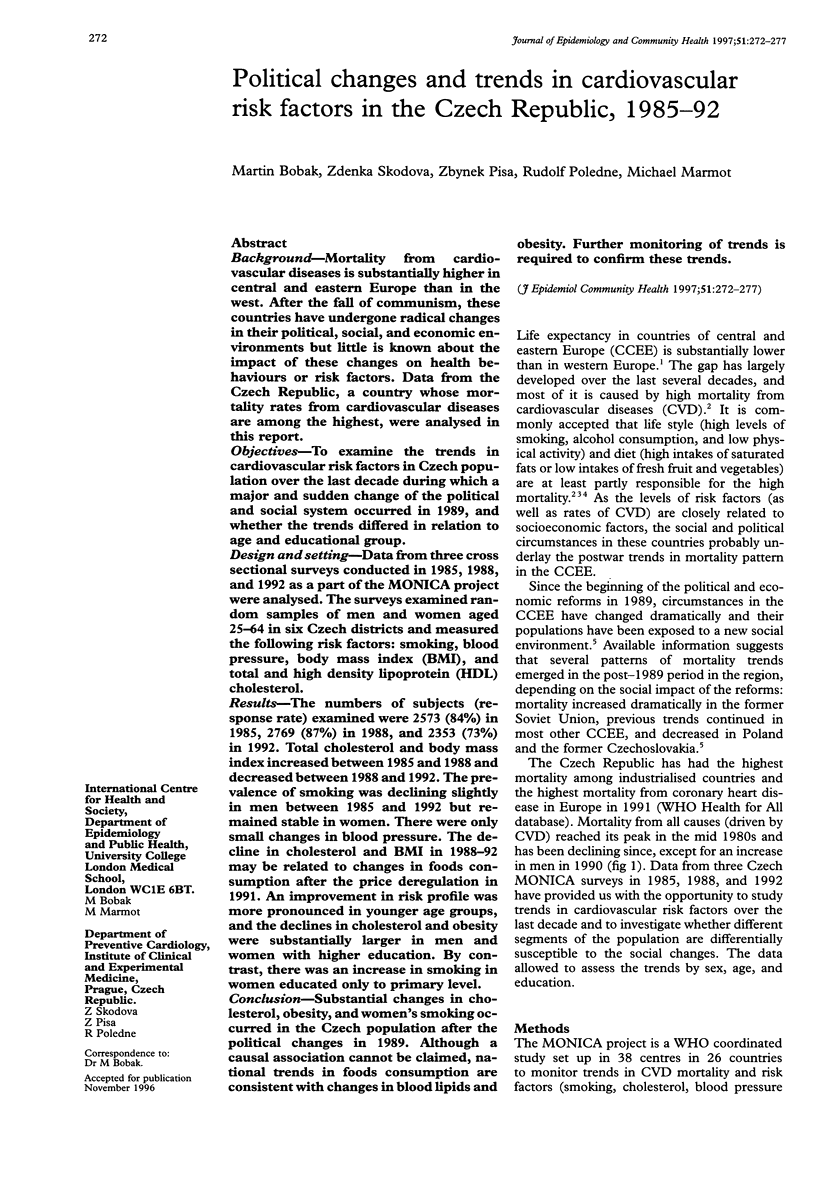

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bobak M., Marmot M. East-West mortality divide and its potential explanations: proposed research agenda. BMJ. 1996 Feb 17;312(7028):421–425. doi: 10.1136/bmj.312.7028.421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feachem R. Health decline in eastern Europe. Nature. 1994 Jan 27;367(6461):313–314. doi: 10.1038/367313a0. [DOI] [PubMed] [Google Scholar]
- Heinemann L., Barth W., Hoffmeister H. Trend of cardiovascular risk factors in the East German population 1968-1992. J Clin Epidemiol. 1995 Jun;48(6):787–795. doi: 10.1016/0895-4356(94)00179-t. [DOI] [PubMed] [Google Scholar]
- Hoffmeister H., Mensink G. B., Stolzenberg H. National trends in risk factors for cardiovascular disease in Germany. Prev Med. 1994 Mar;23(2):197–205. doi: 10.1006/pmed.1994.1027. [DOI] [PubMed] [Google Scholar]
- Kesteloot H. Nutrition and health. Eur Heart J. 1992 Jan;13(1):120–128. doi: 10.1093/oxfordjournals.eurheartj.a060031. [DOI] [PubMed] [Google Scholar]
- Law M. R., Wald N. J., Thompson S. G. By how much and how quickly does reduction in serum cholesterol concentration lower risk of ischaemic heart disease? BMJ. 1994 Feb 5;308(6925):367–372. doi: 10.1136/bmj.308.6925.367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menotti A., Scanga M. Trends in coronary risk factors in Italy. Responsible Investigators of the RF2, OB43 and MICOL Research Groups. Int J Epidemiol. 1992 Oct;21(5):883–892. doi: 10.1093/ije/21.5.883. [DOI] [PubMed] [Google Scholar]
- Peto R., Lopez A. D., Boreham J., Thun M., Heath C., Jr Mortality from tobacco in developed countries: indirect estimation from national vital statistics. Lancet. 1992 May 23;339(8804):1268–1278. doi: 10.1016/0140-6736(92)91600-d. [DOI] [PubMed] [Google Scholar]
- Sigfusson N., Sigvaldason H., Steingrimsdottir L., Gudmundsdottir I. I., Stefansdottir I., Thorsteinsson T., Sigurdsson G. Decline in ischaemic heart disease in Iceland and change in risk factor levels. BMJ. 1991 Jun 8;302(6789):1371–1375. doi: 10.1136/bmj.302.6789.1371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sjøl A., Grunnet K., Schroll M. Secular trends in serum cholesterol, high density lipoproteins and triglycerides 1964-1987. Int J Epidemiol. 1991 Mar;20(1):105–113. doi: 10.1093/ije/20.1.105. [DOI] [PubMed] [Google Scholar]
- Skodová Z., Písa Z., Pikhartová J., Cícha Z., Vojtísek P., Emrová R., Berka L., Hoke M., Wiesner E., Valenta Z. Development of the cardiovascular risk in the population of the Czech Republic. Cor Vasa. 1993;35(5):178–182. [PubMed] [Google Scholar]
- Vartiainen E., Puska P., Jousilahti P., Korhonen H. J., Tuomilehto J., Nissinen A. Twenty-year trends in coronary risk factors in north Karelia and in other areas of Finland. Int J Epidemiol. 1994 Jun;23(3):495–504. doi: 10.1093/ije/23.3.495. [DOI] [PubMed] [Google Scholar]