

Key Points
Question
What is the impact of dietary sodium intake on blood pressure in middle-aged to elderly individuals?
Findings
In this prospectively allocated diet order crossover study of 213 individuals, 1 week of a low-sodium diet resulted in an average 8–mm Hg reduction in systolic blood pressure vs a high-sodium diet, with few adverse events. The low-sodium diet lowered systolic blood pressure in nearly 75% of individuals compared with the high-sodium diet.
Meaning
In this trial, the blood pressure–lowering effect of dietary sodium reduction was comparable with a commonly used first-line antihypertensive medication.
Abstract
Importance
Dietary sodium recommendations are debated partly due to variable blood pressure (BP) response to sodium intake. Furthermore, the BP effect of dietary sodium among individuals taking antihypertensive medications is understudied.
Objectives
To examine the distribution of within-individual BP response to dietary sodium, the difference in BP between individuals allocated to consume a high- or low-sodium diet first, and whether these varied according to baseline BP and antihypertensive medication use.
Design, Setting, and Participants
Prospectively allocated diet order with crossover in community-based participants enrolled between April 2021 and February 2023 in 2 US cities. A total of 213 individuals aged 50 to 75 years, including those with normotension (25%), controlled hypertension (20%), uncontrolled hypertension (31%), and untreated hypertension (25%), attended a baseline visit while consuming their usual diet, then completed 1-week high- and low-sodium diets.
Intervention
High-sodium (approximately 2200 mg sodium added daily to usual diet) and low-sodium (approximately 500 mg daily total) diets.
Main Outcomes and Measures
Average 24-hour ambulatory systolic and diastolic BP, mean arterial pressure, and pulse pressure.
Results
Among the 213 participants who completed both high- and low-sodium diet visits, the median age was 61 years, 65% were female and 64% were Black. While consuming usual, high-sodium, and low-sodium diets, participants’ median systolic BP measures were 125, 126, and 119 mm Hg, respectively. The median within-individual change in mean arterial pressure between high- and low-sodium diets was 4 mm Hg (IQR, 0-8 mm Hg; P < .001), which did not significantly differ by hypertension status. Compared with the high-sodium diet, the low-sodium diet induced a decline in mean arterial pressure in 73.4% of individuals. The commonly used threshold of a 5 mm Hg or greater decline in mean arterial pressure between a high-sodium and a low-sodium diet classified 46% of individuals as “salt sensitive.” At the end of the first dietary intervention week, the mean systolic BP difference between individuals allocated to a high-sodium vs a low-sodium diet was 8 mm Hg (95% CI, 4-11 mm Hg; P < .001), which was mostly similar across subgroups of age, sex, race, hypertension, baseline BP, diabetes, and body mass index. Adverse events were mild, reported by 9.9% and 8.0% of individuals while consuming the high- and low-sodium diets, respectively.
Conclusions and Relevance
Dietary sodium reduction significantly lowered BP in the majority of middle-aged to elderly adults. The decline in BP from a high- to low-sodium diet was independent of hypertension status and antihypertensive medication use, was generally consistent across subgroups, and did not result in excess adverse events.
Trial Registration
ClinicalTrials.gov Identifier: NCT04258332
This crossover trial assesses whether high-sodium and low-sodium dietary interventions affect 24-hour ambulatory blood pressure measures among middle-aged to elderly adults with normotension, controlled hypertension, uncontrolled hypertension, or untreated hypertension.
Introduction
Sodium is a dietary component that substantially contributes to blood pressure (BP).1,2 Estimated daily average sodium intake in middle-aged to elderly US adults is 3.5 g, exceeding World Health Organization, US Department of Health and Human Services, and American Heart Association recommendations, and in the prior decade, deaths attributable to excess dietary sodium increased.3,4,5,6,7 Randomized trials inform recommendations to reduce sodium consumption to lower BP; however, individual variability in the BP response to dietary sodium can make determining personalized treatment responses from clinical trials challenging.7,8,9,10,11,12,13,14,15,16
The within-individual BP response to variation in sodium intake, known as salt sensitivity of BP (SSBP), has been used to define individuals who experience meaningful BP differences with sodium intake reduction.17,18 Estimates suggest that approximately 50% and 25% of individuals with and without hypertension exhibit SSBP, respectively; however, few contemporary data exist and thresholds for defining SSBP may underestimate the impact of dietary sodium reduction on BP.17,18,19 Most randomized trials testing dietary sodium reduction excluded individuals taking antihypertensive medications.9,10,11 Thus, among individuals with treated hypertension, uncertainty persists regarding the extent to which dietary sodium reduction lowers BP and whether antihypertensive pharmacotherapies are associated with lessening of SSBP.8,9,10,11,20
We conducted the Coronary Artery Risk Development in Young Adults (CARDIA)–SSBP study in a contemporary community dwelling population of middle-aged to elderly persons including the spectrum of individuals with normotension through treated and untreated hypertension. Using a prospectively allocated diet order crossover design of 1-week high-sodium and low-sodium diets, we examined (1) the distribution of within-individual BP response to dietary sodium, (2) the difference in BP between individuals allocated to high- or low-sodium diet first, and (3) whether these varied by baseline BP and antihypertensive medication use.
Methods
Trial Oversight
The CARDIA Executive Committee, Observational Study Monitoring Board, and University of Alabama at Birmingham (UAB) Institutional Review Board, serving as the single institutional review board, approved the study protocol (eAppendix 1 in Supplement 1). All participants provided written informed consent. Participants received stipends.
Participants
Briefly, CARDIA is a prospective, multicenter, observational cohort study that aims to identify the factors in young adulthood influencing development of cardiovascular disease.21 Participant enrollment occurred in 1985-1986 and was balanced by sex, self-identified race (Black or White), age (18-24 or 25-30 years), and education (high school or more than high school) subgroups from 4 study sites across the US: Birmingham, Alabama; Chicago, Illinois; Minneapolis, Minnesota; and Oakland, California. Longitudinal follow-up since enrollment is ongoing.
Between April 2021 and February 2023, enrollment into CARDIA-SSBP occurred through 2 sources, initially the CARDIA year 35 core examination, and then an amendment in 2022 allowing for non-CARDIA participants from Chicago and Birmingham. Detailed eligibility criteria are in eAppendix 1 in Supplement 1. Briefly, the inclusion criterion was age 50 to 75 years and key exclusion criteria were enrollment visit systolic or diastolic BP outside of 90 to 160 mm Hg or 50 to 100 mm Hg, respectively, resistant hypertension, or contraindications to high- or low-sodium diets.
Study Protocol
Sodium content and 1-week duration of diets, use of 24-hour ambulatory BP monitoring (ABPM), and 24-hour urine collections for assessment of dietary adherence were based on the American Heart Association’s SSBP recommendations.18 Participants attended 4 study visits: enrollment, baseline, end of the first diet week, and end of the second diet week, with the latter 3 occurring over consecutive 1-week intervals. Study visits occurred at the UAB and Northwestern University CARDIA field centers. Allocation to diet order alternated by weekday at each site. The high-sodium diet was achieved pragmatically by daily supplementation of each participant’s usual diet with 2 bullion packets, each containing 1100 mg of sodium. The low-sodium diet was standardized across sites and prepared in metabolic kitchens at the University of Illinois–Chicago and UAB. One week of low-sodium meals, snacks, and beverages were provided at no cost to participants with instructions not to consume anything outside that provided. The low-sodium diet was designed to provide daily averages of approximately 500 mg of sodium, approximately 4500 mg of potassium, and approximately 1000 mg of calcium, with an individual’s caloric need estimated using the Mifflin-St Jeor formula (eAppendix 2 in Supplement 1).22 The potassium and calcium content of the prepared meals aligns with US dietary guideline recommendations.4
Outcomes
Twenty-four-hour ABPM (OnTrak, Spacelabs Healthcare) and 24-hour urine collections were performed beginning the day before each of the baseline, end of first diet week, and end of second diet week visits. For study visits, participants were instructed to arrive fasting for 6 hours or longer. Participant-reported adverse events while consuming study diets were recorded. Twenty-four-hour ABPM results were transmitted to Vanderbilt University Medical Center (VUMC) for safety review and BP outcomes. For each individual, systolic BP, diastolic BP, mean arterial pressure, and pulse pressure at the end of each diet week were calculated as the averages from 24-hour ABPM. Urine collections were processed on study visit days, stored frozen at −80 °C, then batch shipped overnight on dry ice to VUMC. Urine sodium and creatinine were measured using flame photometry (Jenway PFP7/C, Cole-Parmer) and ELISA (Exocell, Ethos Biosciences), respectively. Assessors for 24-hour ABPM and urinalysis results were masked to diet order.
Statistical Analysis
Salt sensitivity of BP, calculated as 24-hour BP during a high-sodium diet minus 24-hour BP during a low-sodium diet, provides a continuous measure of within-individual BP response to variation in sodium loading. The precision of the estimate of SSBP for mean arterial pressure, the primary outcome, was estimated a priori, and a sample size of 200 individuals at an SD of 7 mm Hg yielded a margin of error of 1 mm Hg.
Prospective allocation to either diet order with a crossover design enabled not only within-individual analysis examining SSBP between high- and low-sodium diets, but also between parallel-group analysis examining contrast in BP between groups at the end of the first diet week. Analyses were performed using an intention-to-treat approach. Baseline characteristics were calculated as medians and IQRs or counts and percentages.
The distribution of SSBP for mean arterial pressure was summarized as medians and IQRs in the overall cohort and within prespecified subgroups by age, sex (self-report), race (self-report), hypertension status, antihypertensive medication use, baseline BP, body mass index, study site, diabetes, and enrollment source, and analyzed using the Wilcoxon signed rank test. The SSBP for mean arterial pressure was then compared between subgroups using the Wilcoxon rank sum test. Distributions of SSBP for systolic BP, diastolic BP, and pulse pressure in the overall cohort were also examined, summarized as medians and IQRs and analyzed using the Wilcoxon signed rank test. Whether SSBP differed by allocated diet order was tested using unadjusted ordinary least-squares regression. In prespecified exploratory analysis, whether SSBP differed between individuals with baseline normotension, controlled hypertension, untreated hypertension, and uncontrolled hypertension was analyzed by the Kruskal-Wallis test. In additional exploratory analysis, associations between classes of antihypertensive medications and SSBP were examined in ordinary least-squares models adjusted for demographic and clinical covariates. The proportion of individuals with any decline, no change, or any increase in BP between high- and low-sodium diets was quantified and then repeated using commonly used thresholds of a 5–mm Hg or greater decrease and a 7–mm Hg or greater increase in mean arterial pressure to define salt sensitivity and inverse salt sensitivity, respectively.18,19,23 The analysis for within-individual BP changes was also recalculated between the usual and low-sodium diets and between the usual and high-sodium diets.
Next, we performed parallel-group analysis to examine contrast in BP at the end of just the first diet week between the groups of individuals allocated to either high- or low-sodium diet first. Primary unadjusted then multivariable-adjusted ordinary least-squares regression was used to calculate mean between-group differences and 95% CIs. Adjustment covariates included age, sex, race, baseline BP, history of hypertension, number of antihypertensive medications, diabetes, body mass index, end of first diet week urine potassium, study site, and CARDIA vs non-CARDIA participants. The overall between-group parallel analysis was then repeated using just the BP from the end of the second diet week. Crossover analysis was performed to assess for interindividual sequence, intra-individual period, or carryover effects, which were all nonsignificant at P = .89, P = .78, and P = .98, respectively. Variation in the difference in systolic BP at the end of the first diet week between the high- and low-sodium diet groups was examined in the aforementioned subgroups by including interaction terms with first diet assignment.
The proportion of participants reporting adverse events while consuming high- and low-sodium diets was tabulated. Analyses were performed using Stata version 15.1 (StataCorp). Statistical significance threshold was set at a 2-sided α ≤ .05. Subgroup analyses were prespecified but considered exploratory, without a priori Bonferroni P value correction. Post hoc, for subgroup analyses we calculated a Bonferroni corrected significance threshold of P < .002.
Results
Of 281 individuals who consented, 232 met eligibility and 228 were randomized and attended the baseline visit (eFigure 1 in Supplement 1). Enrollment characteristics for the 213 individuals who completed both high- and low-sodium diet visits according to allocation are shown in the Table.
Table. Enrollment Characteristics According to Allocation to High-Sodium Diet First or Low-Sodium Diet First.
| Characteristics | High-sodium diet first (n = 118) | Low-sodium diet first (n = 95) |
|---|---|---|
| Age, median (IQR), y | 61 (56-64) | 61 (58-65) |
| Sex, No. (%) | ||
| Female | 76 (64) | 63 (66) |
| Male | 42 (36) | 32 (34) |
| Race, No. (%) | ||
| Black | 75 (64) | 61 (65) |
| White | 39 (33) | 31 (33) |
| Other or unknown | 4 (3) | 3 (3) |
| Enrollment source, No. (%) | ||
| CARDIA | 85 (72) | 70 (74) |
| Non-CARDIA | 33 (28) | 25 (26) |
| Location, No. (%) | ||
| Birmingham | 84 (71) | 47 (49) |
| Chicago | 34 (29) | 48 (51) |
| Hypertension, No. (%) | 59 (50) | 44 (47) |
| No. of antihypertensive medications, No. (%) | ||
| 0 | 59 (50) | 50 (53) |
| 1 | 34 (29) | 29 (31) |
| 2 | 21 (18) | 12 (13) |
| ≥3 | 4 (3) | 3 (3) |
| Use of antihypertensive medication, by drug class, No. (%) | ||
| ACE inhibitor or ARB | 31 (26) | 27 (28) |
| β-Blocker | 13 (11) | 5 (5) |
| Calcium channel blocker | 20 (17) | 19 (20) |
| Diuretic | 17 (14) | 12 (13) |
| Systolic blood pressure, median (IQR), mm Hga | 128 (117-139) | 127 (119-137) |
| Diastolic blood pressure, median (IQR), mm Hga | 80 (73-87) | 77 (73-86) |
| Mean arterial pressure, median (IQR), mm Hga | 96 (88-104) | 94 (88-103) |
| Pulse pressure, median (IQR), mm Hga | 47 (40-56) | 49 (45-56) |
| Heart rate, median (IQR), /mina | 69 (60-78) | 68 (59-75) |
| Diabetes, No. (%) | 22 (19) | 23 (24) |
| Body mass index, median (IQR)b | 31.2 (27.0-36.8) | 30.7 (26.6-34.6) |
| 24-h Urine volume, median (IQR), Lc | 1.47 (0.96-2.04) | 1.54 (1.08-2.36) |
| 24-h Urine sodium, median (IQR), gc | 4.57 (2.57-5.73) | 4.88 (3.16-6.62) |
| 24-h Urine creatinine, median (IQR), gc | 1.12 (0.76-1.46) | 1.15 (0.84-1.53) |
Abbreviations: ACEI, angiotensin-converting enzyme; ARB, angiotensin receptor blocker.
Baseline in-clinic measure.
Calculated as weight in kilograms divided by height in meters squared.
Urine measurements were available for 176 participants.
Assessed by 24-hour urine excretion, the high-sodium diet significantly increased sodium intake above the low-sodium and usual diets (eTable 1 in Supplement 1). The subset of individuals not taking antihypertensive medications at baseline provides population estimates of usual sodium consumption and the contrast between high- and low-sodium diets. Participants’ usual diets were already high in sodium (median, 4.45 g/d; IQR, 2.57-6.93 g/d), which was significantly raised and lowered to medians of 5.00 and 1.27 g/d while participants were consuming the high- and low-sodium diets, respectively.
Figure 1 shows 24-hour ABPM results according to allocated diet order and study visit. Figure 2 shows distributions of SSBP calculated as the within-individual difference in 24-hour ABP for the high-sodium diet minus the low-sodium diet. For the primary outcome of SSBP for mean arterial pressure, the median was 4 mm Hg (IQR, 0-8 mm Hg; P < .001). The SSBP for mean arterial pressure did not significantly differ between subgroups, except by diastolic BP, in whom individuals with baseline diastolic BP of 74 mm Hg or lower had a relatively smaller but still significant decline in mean arterial pressure while consuming a low-sodium diet vs a high-sodium diet, compared with individuals whose baseline diastolic BP was above 74 mm Hg (Figure 3). The SSBP did not differ according to diet order (eTable 2 in Supplement 1).
Figure 1. 24-Hour Ambulatory BP According to Allocated Diet Order and Study Visit.
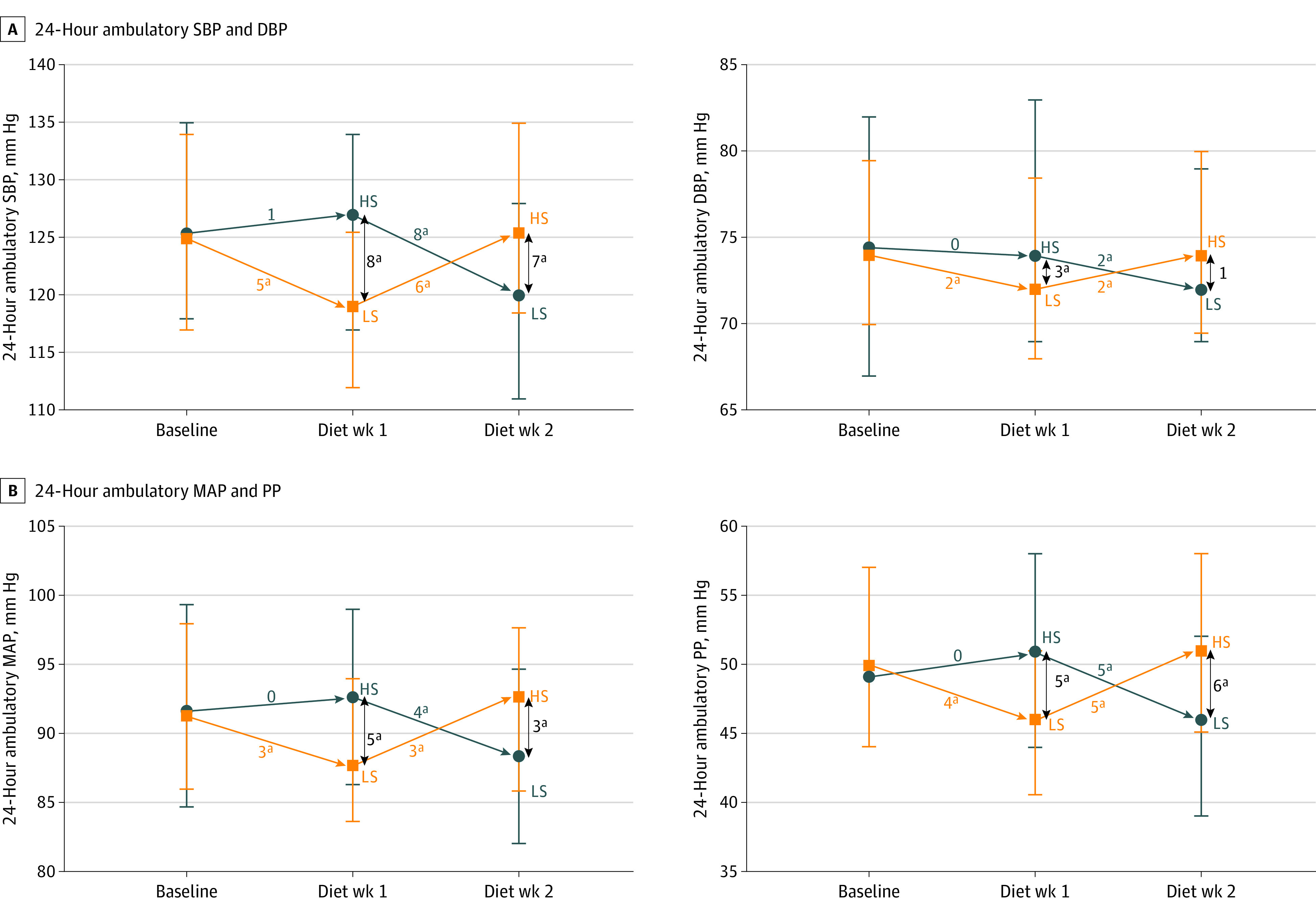
BP indicates blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; PP, pulse pressure; and SBP, systolic blood pressure. Delta values in blue or orange reflect median within-individual differences between diets, while delta values in black are mean differences between the high-sodium (HS) and low-sodium (LS) diet groups. Orange squares are median group values for each time point in those allocated to an LS diet first. Blue circles are median group values for each time point in those allocated to an HS diet first. Vertical bars indicate interquartile range. Between the groups randomized to an HS diet vs an LS diet first, at the end of the first diet week, mean differences in BP were as follows: SBP, 8 mm Hg (95% CI, 4-11 mm Hg; P < .001), DBP, 3 mm Hg (95% CI, 1-5 mm Hg; P = .01), MAP, 5 mm Hg (95% CI, 2-7 mm Hg; P = .001), and PP, 5 mm Hg (95% CI, 2-7 mm Hg; P = .001).
aStatistically significant change.
Figure 2. Distributions of Within-Individual 24-Hour Ambulatory BP Response to Dietary Sodium Intake, Calculated From High-Sodium Diet Minus Low-Sodium Diet.
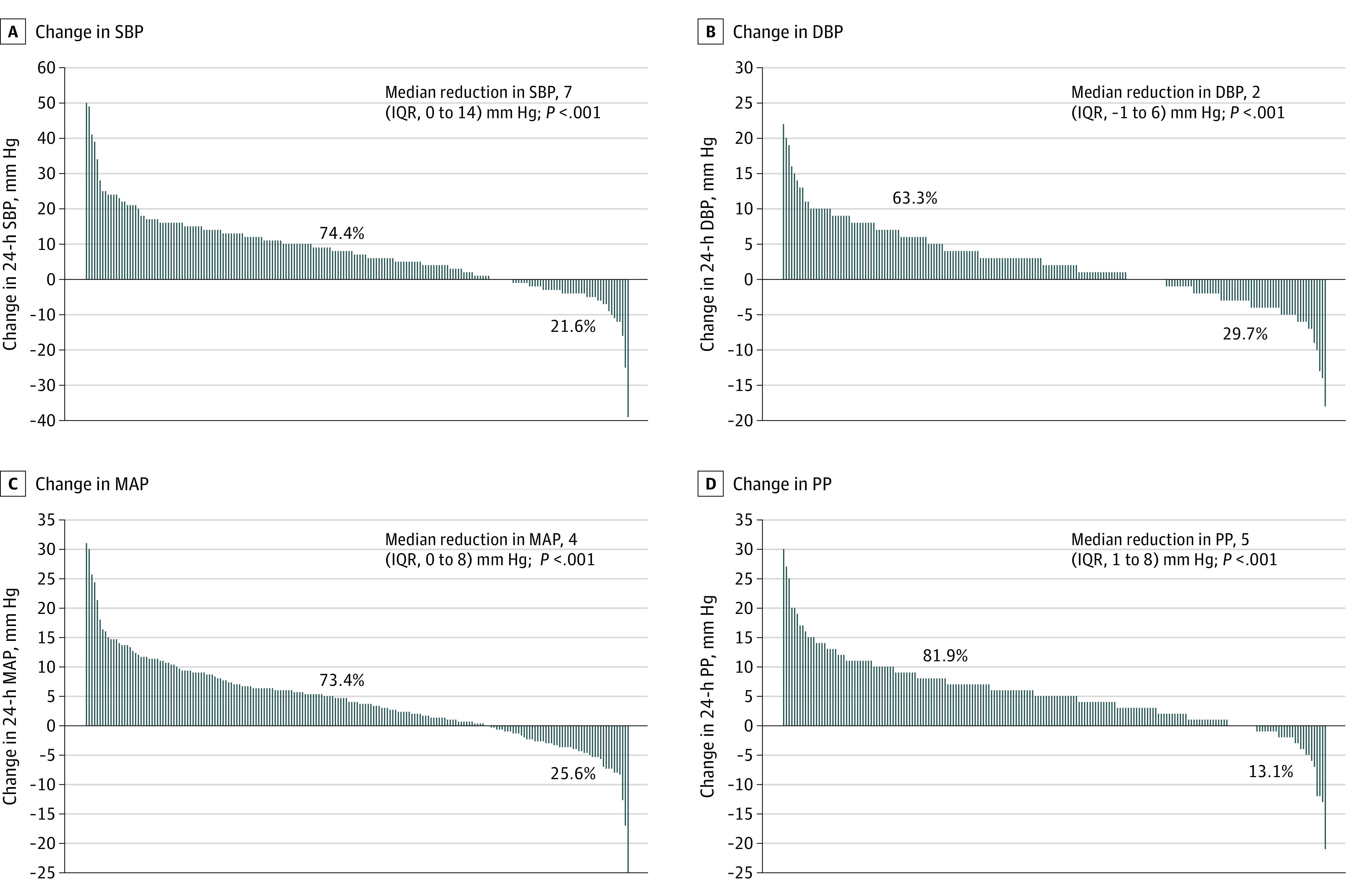
BP indicates blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; PP, pulse pressure; and SBP, systolic blood pressure. Bars above 0 reflect a reduction in BP during low-sodium diet vs high-sodium diet; bars below 0 reflect an increase in BP during low-sodium diet vs high-sodium diet. Percentages above 0 reflect proportion of individuals who experienced a reduction in BP during low-sodium diet vs high-sodium diet; percentages below 0 reflect proportion of individuals who experienced an increase in BP during low-sodium diet vs high-sodium diet. P values based on Wilcoxon signed rank test.
Figure 3. Variation in Salt Sensitivity of Blood Pressure for MAP Across Subgroups.

DBP indicates diastolic blood pressure; MAP, mean arterial pressure; and SBP, systolic blood pressure. Plot of within-individual salt sensitivity of blood pressure, calculated as the difference in MAP between high- and low-sodium diets. For each of the subgroups shown, the within-individual difference in MAP was significant at P < .001 for all except for non-CARDIA participants (P = .003) based on Wilcoxon signed rank tests with post hoc Bonferroni-corrected threshold for significance of P < .002. For each of the subgroup comparisons, eg, male vs female, the Wilcoxon rank sum tests were nonsignificant (P ≥ .10) for all except by DBP (P = .04).
aCalculated as weight in kilograms divided by height in meters squared.
The SSBP was also similar among individuals with normotension, controlled hypertension, untreated hypertension, and uncontrolled hypertension (Figure 4; eTables 3 and 4 in Supplement 1). In exploratory multivariable analysis, antihypertensive drug classes (ie, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, β-blockers, calcium channel blockers, and diuretics) were not consistently associated with SSBP (eTable 5 in Supplement 1).
Figure 4. Within-Individual 24-Hour Ambulatory BP Response to Low-Sodium vs High-Sodium Diets Stratified According to Baseline Hypertension Status.
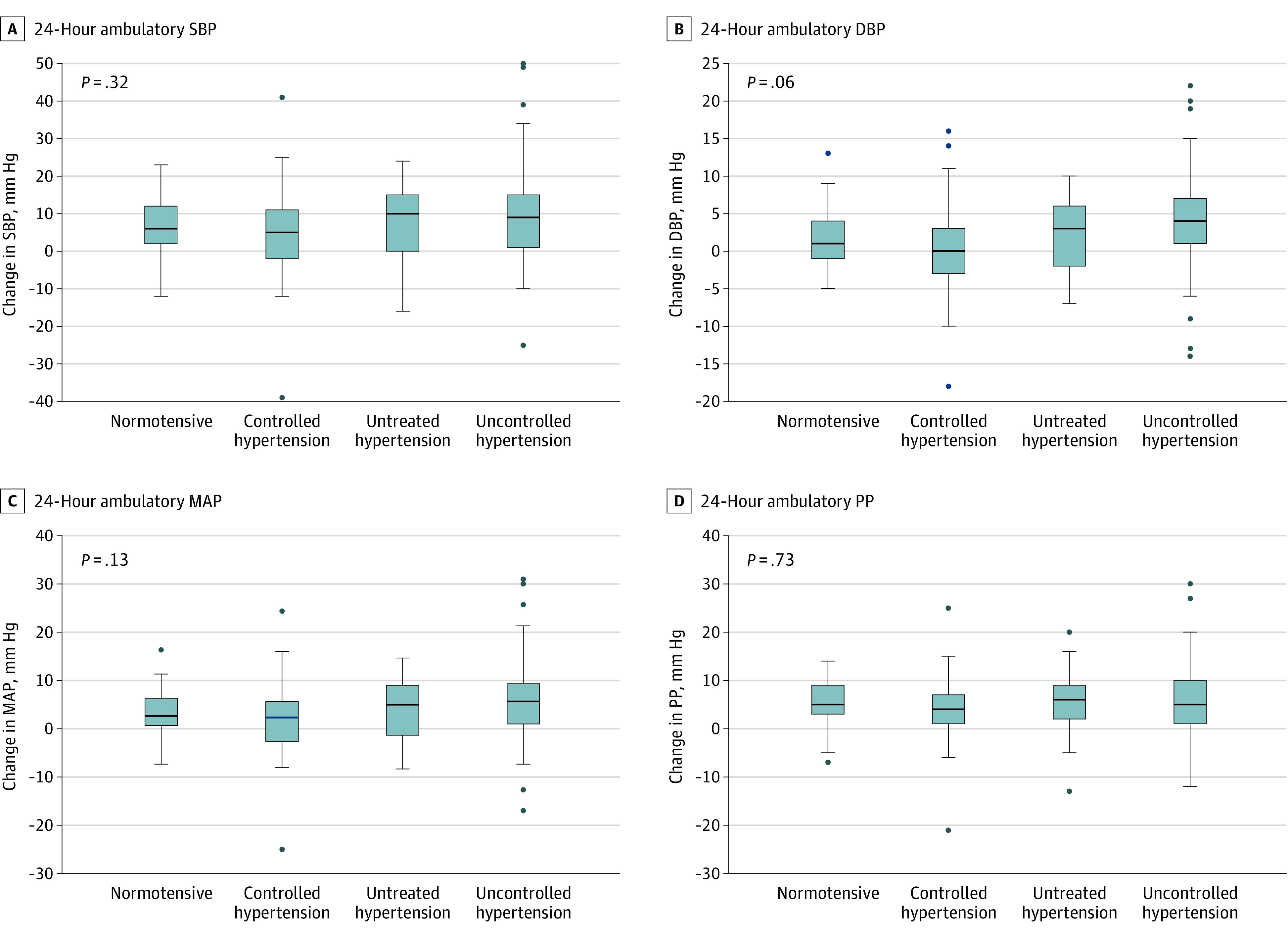
BP indicates blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; PP, pulse pressure; and SBP, systolic blood pressure. Change in BP was calculated as BP during high-sodium diet minus BP during low-sodium diet. Box center bars indicate medians; box tops and bottoms, IQRs; whiskers, the most extreme values within 75th percentile + 1.5 times IQR and 25th percentile − 1.5 times IQR; and circles, outliers. The within-individual salt sensitivity of BP response to high- minus low-sodium diets was similar between individuals with normotension (n = 49), controlled hypertension (n = 39), untreated hypertension (n = 50), and uncontrolled hypertension (n = 61).
In the overall cohort, while consuming the low-sodium diet compared with the high-sodium diet, mean arterial pressure declined, was unchanged, or increased in 73.4%, 1.0%, and 25.6% of individuals, respectively, with similar patterns for systolic BP, diastolic BP, and pulse pressure (eTable 6 in Supplement 1). The commonly used threshold of a 5–mm Hg or greater decline in mean arterial pressure from high- to low-sodium diets classified 46% of individuals as “salt sensitive.” This group had a median difference in 24-hour urine sodium in high-sodium minus low-sodium diet of 3.4 g (IQR, 1.4-4.9 g; P < .001). Using a threshold of a 7–mm Hg or greater increase in mean arterial pressure from a high- to a low-sodium diet, 5% of individuals exhibited inverse salt sensitivity. These individuals had a median difference in 24-hour urine sodium in high-sodium minus low-sodium diet of 0.3 g (IQR, −4.6 to 1.4 g; P = .92).
Compared with usual diet, the low-sodium diet reduced daily sodium intake by a median of 2.3 g (IQR, 0.4- g; P < .001), which was similar to the 7–mm Hg median difference between high- and low-sodium diets (eTable 7 in Supplement 1). Compared with usual diet, 71.7% of individuals demonstrated a decline in systolic BP with the low-sodium diet (eTable 6 in Supplement 1). In contrast, the high-sodium diet raised dietary sodium intake by a median of 1.1 g (IQR, −0.4 to 2.7 g; P < .001), but without significant changes in BP (eTable 6 in Supplement 1).
In the parallel-group analysis performed to examine the differences in BP at the end of the first diet week between the groups of individuals allocated to either high- or low-sodium diets first, systolic BP was 8 mm Hg lower (95% CI, 4-11 mm Hg; P < .001) in those allocated to a low-sodium diet first compared with a high-sodium diet first (Figure 1), which was similar following multivariable adjustment (8 mm Hg; 95% CI, 5-11 mm Hg; P < .001). This between-group effect was also consistent comparing low- and high-sodium diet groups using just the end of the second diet week BP (7 mm Hg; 95% CI, 3-11 mm Hg; P < .001), without evidence for interindividual sequence or carryover effects. Mean differences in diastolic BP, mean arterial pressure, and pulse pressure between individuals randomized to a high- vs low-sodium diet first were also significant (Figure 1). The reduction in systolic BP resulting from a low-sodium diet compared with a high-sodium diet was largely consistent across subgroups, including age, sex, and race, with relatively greater effects in individuals with higher baseline BP and diabetes (eFigure 2 in Supplement 1).
A total of 35 and 24 adverse events were reported in 21 (9.9%) and 17 (8.0%) individuals while consuming high- and low-sodium diets, respectively (eTable 8 in Supplement 1). These were generally mild and self-remitted. The most frequent symptoms while consuming the high-sodium diet were headache, gastrointestinal discomfort, and edema; while consuming the low-sodium diet, these were cramping and weakness.
Discussion
In this sample of community-dwelling middle-aged to elderly individuals, sodium reduction significantly lowered BP compared with a high-sodium diet after a 1-week diet study period. Furthermore, the within-individual and between-group declines in BP from a high-sodium to a low-sodium diet were independent of hypertension status and antihypertensive medication use, were generally consistent across subgroups, and did not result in excess adverse events.
Based on 24-hour urine sodium excretion, during the 1-week low-sodium dietary intervention, median sodium intake was approximately 1.3 g/d. Compared with usual diet, the low-sodium diet resulted in a median reduction of about 1 tsp of table salt (2.3 g of sodium) per day with a corresponding median 6–mm Hg reduction in systolic BP. The magnitude of this 24-hour ABP effect is similar to the mean 6.7–mm Hg reduction in clinic systolic BP via a low-sodium diet of 1.5 g/d observed in the DASH-Sodium trial, in which individuals consumed fully controlled sodium diets for 30 days each.10 The 6–mm Hg reduction in systolic BP achieved with dietary sodium reduction compared with usual diet in the overall cohort is also similar to the average effect observed with 12.5 mg of hydrochlorothiazide.24 The low-sodium diet was well tolerated, with 8% of individuals reporting any adverse event vs 9.9% consuming the high-sodium diet. Collectively, these data may inform recommendations to patients; namely, clinically meaningful lowering of BP through dietary sodium reduction can be achieved safely and rapidly within 1 week; an effect comparable with that of a common first-line antihypertensive medication.
In participants in this study, the estimated median daily sodium intake during usual diet was approximately 4.5 g. Although further increase in daily sodium intake achieved a significant increase of approximately 0.5 tsp of table salt (approximately 1.1 g of sodium), parallel increases in BP were not observed. This approach of supplementing dietary sodium above each individual’s usual diet was not only pragmatic but also designed to reflect real-life variability in sodium intake. It also contrasts with the DASH-Sodium and GenSalt studies, in which the “high-sodium” diets did not, on average, surpass the sodium intake of usual diets.10,13 This distinction in study design enabled us to address the impact of sodium supplementation beyond usual diet, providing complementary information to the existing literature. That further sodium supplementation did not increase BP in the participants of this study suggests that usual diets may already have been sodium saturated. We caution against the interpretation that added sodium beyond usual diet does not adversely contribute to health.25 Rather, our data demonstrate that the greatest impact on BP compared with usual diet is achieved through lowering sodium intake. Once a low-sodium diet is attained, returning to a higher-sodium diet afterward did raise BP, consistent with findings from others.11,13
Conventional thresholds for defining SSBP may underestimate the proportion of individuals who experience clinically meaningful lowering of BP with sodium reduction. Using a difference in mean arterial pressure threshold of 5 mm Hg or greater in high-sodium minus low-sodium diets to define SSBP, 46% of participants met this criterion.18 This contrasts with the 73.4% of individuals who experienced any reduction in mean arterial pressure with a low-sodium diet. Furthermore, we found that the reduction in mean arterial pressure between individuals allocated to a high- vs a low-sodium diet first was largely consistent across subgroups. We also appreciate the concept of inverse salt sensitivity, in which BP appears to increase with sodium reduction.23 An increase in BP with the low-sodium diet occurred in some individuals, with 5% meeting the inverse SSBP for mean arterial pressure threshold of 7 mm Hg or greater, in whom we found a smaller difference in 24-hour urine sodium between high- and low-sodium diets, raising consideration for dietary nonadherence. Fully observed dietary studies may be needed to confirm whether and to what extent BP rises in response to sodium reduction in some individuals, and its prevalence.
In contrast to most prior studies evaluating dietary sodium’s effect on BP, we included individuals across the spectrum of normotensive to hypertensive, treated and untreated, controlled and uncontrolled.11,13 The reduction in BP between high- and low-sodium diets was similar across these groups. Moreover, in exploratory analyses, we did not find different classes of antihypertensive medications consistently associated with the BP response to variation in dietary sodium. That none of the classes of antihypertensive medications was consistently associated with the BP response to dietary sodium emphasizes the importance of continued lifestyle modification even among individuals with treated hypertension.
Limitations
There are some limitations to this study. The 24-hour urine sodium levels on the low-sodium diet were higher than expected for the provided standardized low-sodium meals, suggesting that there was dietary nonadherence, that equilibrium had not yet been obtained, or both. This reflects what is likely to occur in an individual’s life even if attempts are made to adhere to a low-sodium diet because sodium content of food and day-to-day dietary patterns vary. It does not, however, negate the contrast achieved between usual or high-sodium diet and low-sodium diet and the BP effects attained, and may suggest underestimation of the magnitude of difference in BP. The usual, high-sodium, and low-sodium diets were not fully controlled; thus, we cannot exclude contributions of nonsodium dietary components, but reassuringly, the magnitude of effect observed from high- to low-sodium diets was independent of differences in 24-hour urine potassium between high- and low-sodium diets and on par with that of fully controlled sodium feeding trials, eg, DASH-Sodium.11,26 Intra-individual variability in BP over time may also contribute to overestimation or underestimation of the observed BP effects attributed to contrasts between diets. We also acknowledge that intra-individual variability in BP can make interpreting individual treatment responses from parallel-design trials challenging. Our study design enabled us to assess both the between-group and within-individual BP difference between high- and low-sodium diets, and we are reassured by the similar magnitudes of effect, ie, medians of 8 mm Hg and 7 mm Hg, respectively, and that we did not observe carryover effects. Our study design does not allow assessment of BP effects of longer time consuming high- or low-sodium diets, but this does not negate the effects observed at 1 week, which was when the majority of BP effect of dietary sodium reduction was observed in DASH-Sodium.27 Our study does not address sustainability of a low-sodium diet, but the magnitudes of BP effects were similar to longer feeding studies, ie, DASH-Sodium, and are consistent with a meta-analysis demonstrating similar effects of 1-week dietary interventions to those of 1 to 6 months’ duration.10,15 Null findings for differences in SSBP between subgroups by hypertension status or antihypertensive medication class might be related to insufficient power for subgroup analysis. Evaluating the effect of dietary sodium on daytime and nocturnal BP is a future direction. Our results may not be generalizable outside of the community-based population studied.
Conclusions
In conclusion, sodium reduction significantly lowered BP in the majority of middle-aged to elderly adults in this study. The decline in BP from a high-sodium diet to a low-sodium diet was independent of hypertension status and antihypertensive medication use, generally consistent across subgroups, and did not result in excess adverse events.
Educational Objective: To identify the key insights or developments described in this article.
-
Why was it necessary to undertake a contemporary trial of dietary sodium reduction and its impact on blood pressure?
Among individuals with treated hypertension, the extent to which dietary sodium reduction lowers blood pressure, that is, the salt sensitivity of blood pressure, remains uncertain.
Most prior randomized trials of dietary sodium reduction enrolled individuals taking multiple antihypertensive medications that are no longer in use today.
US adults have reduced sodium intake to below American Heart Association, US Department of Health and Human Services, and World Health Organization guidelines, and it is unclear whether further reduction confers additional blood pressure–related benefit.
-
How was the low-sodium diet achieved?
All sources of additional salt, including table salt, kitchen salt, and salted butter, were removed from areas where meals were prepared or consumed.
Low-sodium meals, snacks, and beverages were provided for 1 week and totaled approximately 500 mg of sodium daily.
No dietary changes were required for the low-sodium diet because all participants’ usual diets were already low in sodium.
-
What proportion of the total study cohort demonstrated a decline in blood pressure while consuming the low-sodium diet compared with the high-sodium diet?
Less than 25% of individuals exhibited salt-sensitive blood pressure, which was consistent with older studies.
More than 90% of participants experienced lower blood pressure while consuming the low-sodium diet, and those few with unchanged blood pressure also experienced greater rates of measurement error.
Overall, 73% of individuals experienced a decline in blood pressure while consuming the low-sodium diet, and 46% experienced a ≥5–mm Hg decline in mean arterial pressure.
eAppendix 1. CARDIA-SSBP Protocol
eAppendix 2. Sample menu for low-sodium diet
eFigure 1. Consort Diagram
eTable 1. Urine analytes from 24-hour collections on usual, high-sodium, and low-sodium diets
eTable 2. Mean difference in the within-individual BP response to high- vs. low-sodium diet between individuals randomized to a high- then low- compared to low- then high-sodium diet order
eTable 3. Within individual difference in blood pressure between high- minus- low-sodium diet according to baseline hypertensive status, along with proportions of individuals who displayed a decrease, no change, or increase in blood pressure
eTable 4. Baseline characteristics of individuals according to hypertensive status
eTable 5. Associations between baseline use of anti-hypertensive medications by class and the difference in 24-hour ambulatory BP between high- minus low-sodium diet in mm Hg
eTable 6. Proportion of individuals whose 24-hour ambulatory blood pressure declined, was unchanged, or increased from high to low sodium diet, usual to low-sodium diet, or usual to high-sodium diet
eTable 7. Within-individual differences in BP between high- and low-sodium compared with usual- and low-sodium diets
eFigure 2. Variation in mean difference in 24-hour ambulatory systolic BP at the end of the first diet week between groups randomized to high- or low-sodium diet first
eTable 8. Symptoms and adverse events reported by individuals while on high- and low-sodium diet
Data Sharing Statement
References
- 1.Suter PM, Sierro C, Vetter W. Nutritional factors in the control of blood pressure and hypertension. Nutr Clin Care. 2002;5(1):9-19. doi: 10.1046/j.1523-5408.2002.00513.x [DOI] [PubMed] [Google Scholar]
- 2.Zhao D, Qi Y, Zheng Z, et al. Dietary factors associated with hypertension. Nat Rev Cardiol. 2011;8(8):456-465. doi: 10.1038/nrcardio.2011.75 [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization . WHO Guideline: Sodium Intake for Adults and Children. World Health Organization; 2012. [PubMed] [Google Scholar]
- 4.Department of Agriculture and Department of Health and Human Services . Dietary Guidelines for Americans, 2020-2025. 9th ed. Dept of Agriculture and Dept of Health and Human Services; 2020. [Google Scholar]
- 5.Lichtenstein AH, Appel LJ, Vadiveloo M, et al. 2021 Dietary guidance to improve cardiovascular health: a scientific statement from the American Heart Association. Circulation. 2021;144(23):e472-e487. doi: 10.1161/CIR.0000000000001031 [DOI] [PubMed] [Google Scholar]
- 6.Cogswell ME, Loria CM, Terry AL, et al. Estimated 24-hour urinary sodium and potassium excretion in US adults. JAMA. 2018;319(12):1209-1220. doi: 10.1001/jama.2018.1156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Institute for Health Metrics and Evaluation . Diet high in sodium level 3 risk. Published 2019. Accessed November 2, 2023. https://www.healthdata.org/results/gbd_summaries/2019/diet-high-sodium-level-3-risk
- 8.Trials of Hypertension Prevention Collaborative Research Group . Effects of weight loss and sodium reduction intervention on blood pressure and hypertension incidence in overweight people with high-normal blood pressure: the Trials of Hypertension Prevention, phase II. Arch Intern Med. 1997;157(6):657-667. doi: 10.1001/archinte.1997.00440270105009 [DOI] [PubMed] [Google Scholar]
- 9.Whelton PK, Appel LJ, Espeland MA, et al. ; TONE Collaborative Research Group . Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of nonpharmacologic interventions in the elderly (TONE). JAMA. 1998;279(11):839-846. doi: 10.1001/jama.279.11.839 [DOI] [PubMed] [Google Scholar]
- 10.Sacks FM, Svetkey LP, Vollmer WM, et al. ; DASH-Sodium Collaborative Research Group . Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med. 2001;344(1):3-10. doi: 10.1056/NEJM200101043440101 [DOI] [PubMed] [Google Scholar]
- 11.Appel LJ, Champagne CM, Harsha DW, et al. ; Writing Group of the PREMIER Collaborative Research Group . Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial. JAMA. 2003;289(16):2083-2093. [DOI] [PubMed] [Google Scholar]
- 12.Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the Trials of Hypertension Prevention (TOHP). BMJ. 2007;334(7599):885-888. doi: 10.1136/bmj.39147.604896.55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chen J, Gu D, Huang J, et al. ; GenSalt Collaborative Research Group . Metabolic syndrome and salt sensitivity of blood pressure in non-diabetic people in China: a dietary intervention study. Lancet. 2009;373(9666):829-835. doi: 10.1016/S0140-6736(09)60144-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bibbins-Domingo K, Chertow GM, Coxson PG, et al. Projected effect of dietary salt reductions on future cardiovascular disease. N Engl J Med. 2010;362(7):590-599. doi: 10.1056/NEJMoa0907355 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Huang L, Trieu K, Yoshimura S, et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: systematic review and meta-analysis of randomised trials. BMJ. 2020;368:m315. doi: 10.1136/bmj.m315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Senn S. Individual response to treatment: is it a valid assumption? BMJ. 2004;329(7472):966-968. doi: 10.1136/bmj.329.7472.966 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Weinberger MH, Miller JZ, Luft FC, Grim CE, Fineberg NS. Definitions and characteristics of sodium sensitivity and blood pressure resistance. Hypertension. 1986;8(6 pt 2):II127-II134. doi: 10.1161/01.HYP.8.6_Pt_2.II127 [DOI] [PubMed] [Google Scholar]
- 18.Elijovich F, Weinberger MH, Anderson CA, et al. ; American Heart Association Professional and Public Education Committee of the Council on Hypertension, Council on Functional Genomics and Translational Biology, and Stroke Council . Salt sensitivity of blood pressure: a scientific statement from the American Heart Association. Hypertension. 2016;68(3):e7-e46. doi: 10.1161/HYP.0000000000000047 [DOI] [PubMed] [Google Scholar]
- 19.Kurtz TW, DiCarlo SE, Pravenec M, Morris RC Jr. An appraisal of methods recently recommended for testing salt sensitivity of blood pressure. J Am Heart Assoc. 2017;6(4):e005653. doi: 10.1161/JAHA.117.005653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pimenta E, Gaddam KK, Oparil S, et al. Effects of dietary sodium reduction on blood pressure in subjects with resistant hypertension: results from a randomized trial. Hypertension. 2009;54(3):475-481. doi: 10.1161/HYPERTENSIONAHA.109.131235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Friedman GD, Cutter GR, Donahue RP, et al. CARDIA: study design, recruitment, and some characteristics of the examined subjects. J Clin Epidemiol. 1988;41(11):1105-1116. doi: 10.1016/0895-4356(88)90080-7 [DOI] [PubMed] [Google Scholar]
- 22.Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO. A new predictive equation for resting energy expenditure in healthy individuals. Am J Clin Nutr. 1990;51(2):241-247. doi: 10.1093/ajcn/51.2.241 [DOI] [PubMed] [Google Scholar]
- 23.Felder RA, Gildea JJ, Xu P, et al. Inverse salt sensitivity of blood pressure: mechanisms and potential relevance for prevention of cardiovascular disease. Curr Hypertens Rep. 2022;24(9):361-374. doi: 10.1007/s11906-022-01201-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Musini VM, Nazer M, Bassett K, Wright JM. Blood pressure-lowering efficacy of monotherapy with thiazide diuretics for primary hypertension. Cochrane Database Syst Rev. 2014;2014(5):CD003824. doi: 10.1002/14651858.CD003824.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mente A, O’Donnell M, Rangarajan S, et al. Urinary sodium excretion, blood pressure, cardiovascular disease, and mortality: a community-level prospective epidemiological cohort study. Lancet. 2018;392(10146):496-506. doi: 10.1016/S0140-6736(18)31376-X [DOI] [PubMed] [Google Scholar]
- 26.Mente A, O’Donnell MJ, Rangarajan S, et al. ; PURE Investigators . Association of urinary sodium and potassium excretion with blood pressure. N Engl J Med. 2014;371(7):601-611. doi: 10.1056/NEJMoa1311989 [DOI] [PubMed] [Google Scholar]
- 27.Obarzanek E, Proschan MA, Vollmer WM, et al. Individual blood pressure responses to changes in salt intake: results from the DASH-Sodium trial. Hypertension. 2003;42(4):459-467. doi: 10.1161/01.HYP.0000091267.39066.72 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix 1. CARDIA-SSBP Protocol
eAppendix 2. Sample menu for low-sodium diet
eFigure 1. Consort Diagram
eTable 1. Urine analytes from 24-hour collections on usual, high-sodium, and low-sodium diets
eTable 2. Mean difference in the within-individual BP response to high- vs. low-sodium diet between individuals randomized to a high- then low- compared to low- then high-sodium diet order
eTable 3. Within individual difference in blood pressure between high- minus- low-sodium diet according to baseline hypertensive status, along with proportions of individuals who displayed a decrease, no change, or increase in blood pressure
eTable 4. Baseline characteristics of individuals according to hypertensive status
eTable 5. Associations between baseline use of anti-hypertensive medications by class and the difference in 24-hour ambulatory BP between high- minus low-sodium diet in mm Hg
eTable 6. Proportion of individuals whose 24-hour ambulatory blood pressure declined, was unchanged, or increased from high to low sodium diet, usual to low-sodium diet, or usual to high-sodium diet
eTable 7. Within-individual differences in BP between high- and low-sodium compared with usual- and low-sodium diets
eFigure 2. Variation in mean difference in 24-hour ambulatory systolic BP at the end of the first diet week between groups randomized to high- or low-sodium diet first
eTable 8. Symptoms and adverse events reported by individuals while on high- and low-sodium diet
Data Sharing Statement