

ABSTRACT
Following a request from the European Commission (EC), the EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA) was asked to deliver a scientific opinion on the revision of the tolerable upper intake level (UL) for folic acid/folate. Systematic reviews of the literature were conducted to assess evidence on priority adverse health effects of excess intake of folate (including folic acid and the other authorised forms, (6S)‐5‐methyltetrahydrofolic acid glucosamine and l‐5‐methyltetrahydrofolic acid calcium salts), namely risk of cobalamin‐dependent neuropathy, cognitive decline among people with low cobalamin status, and colorectal cancer and prostate cancer. The evidence is insufficient to conclude on a positive and causal relationship between the dietary intake of folate and impaired cognitive function, risk of colorectal and prostate cancer. The risk of progression of neurological symptoms in cobalamin‐deficient patients is considered as the critical effect to establish an UL for folic acid. No new evidence has been published that could improve the characterisation of the dose–response between folic acid intake and resolution of megaloblastic anaemia in cobalamin‐deficient individuals. The ULs for folic acid previously established by the Scientific Committee on Food are retained for all population groups, i.e. 1000 μg/day for adults, including pregnant and lactating women, 200 μg/day for children aged 1–3 years, 300 μg/day for 4–6 years, 400 μg/day for 7–10 years, 600 μg/day for 11–14 years and 800 μg/day for 15–17 years. A UL of 200 μg/day is established for infants aged 4–11 months. The ULs apply to the combined intake of folic acid, (6S)‐5‐methyltetrahydrofolic acid glucosamine and l‐5‐methyltetrahydrofolic acid calcium salts, under their authorised conditions of use. It is unlikely that the ULs for supplemental folate are exceeded in European populations, except for regular users of food supplements containing high doses of folic acid/5‐methyl‐tetrahydrofolic acid salts.
Keywords: folate, folic acid, 5‐methyltetrahydrofolic acid salt, tolerable upper intake level
1. INTRODUCTION
1.1. Background as provided by the European Commission
Article 6 of Regulation (EC) No 1925/2006 on the addition of vitamins and minerals and of certain other substances to foods and Article 5 of Directive 2002/46/EC on the approximation of the laws of the Member States relating to food supplements provide that maximum amount of vitamins and minerals added to foods and to food supplements respectively, shall be set.
The above‐mentioned provisions lay down the criteria to be taken into account when establishing these maximum amounts that include the upper safe levels of vitamins and minerals established by scientific risk assessment based on “generally accepted scientific data, taking into account, as appropriate, the varying degrees of sensitivity of different groups of consumers”.
To set maximum amounts of vitamins and minerals in fortified foods and food supplements, the Commission would like to ask the European Food Safety Authority (EFSA) to review the previous opinions of the Scientific Committee on Food (SCF) or the NDA Panel on the ULs for vitamin A, 1 folic acid/folate,1 vitamin D,1 vitamin E,1 vitamin B6,1 iron,1 manganese1 and β‐carotene1 to take into account recent scientific developments and evidence.
In this context, EFSA should first review the guidelines of the SCF1 for the development of tolerable upper intake levels for vitamins and minerals (adopted on 19 October 2000).
Tolerable Upper Intake Levels should be presented separately for the age group from 4/6 months onwards until 3 years of age and the general population group from 3 years onwards, taking into account, as appropriate, the varying degrees of sensitivity of different consumer groups. As foods intended for the general population are also consumed by young children, young children should be considered as a potentially sensitive consumer group.
1.2. Terms of Reference as provided by the European Commission
In accordance with Article 29(1)(a) of Regulation (EC) No 178/2002, the European Commission requests the European Food Safety Authority to:
Update the guidelines of the SCF for the development of Tolerable Upper Intake Levels for vitamins and minerals in the light of available recent scientific and methodological developments.
- Review existing scientific evidence and provide advice on Tolerable Upper Intake Levels for the following vitamins and minerals including their currently authorized forms for the addition to fortified foods and food supplements for the general population and, as appropriate, for vulnerable subgroups of the population:
- vitamin A
- folic acid/folate
- vitamin D
- vitamin E
- iron
- manganese
- β‐carotene
- vitamin B6
For nutrients for which there are no, or insufficient, data on which to base the establishment of an UL, an indication should be given on the highest level of intake where there is reasonable confidence in data on the absence of adverse effects.
1.3. Interpretation of the Terms of Reference
According to the mandate, EFSA has first reviewed the guidelines of the SCF for the development of tolerable upper intake levels (ULs) for vitamins and minerals (SCF, 2000). A draft guidance has been endorsed by the Nutrition, Novel Foods and Food Allergens (NDA) Panel and published for a 1‐year pilot phase (EFSA NDA Panel, 2022b), after which it will be revised and complemented as necessary, following a public consultation.
The Panel interprets that the UL for folic acid/folate should be revised according to the principles laid down in the above‐mentioned guidance, following a protocol developed for that purpose (Annex A) and covering all sources of folate authorised for addition to foods and food supplements in the EU (i.e. folic acid, l‐5‐methyltetrahydrofolic acid calcium salt and (6S)‐5‐methyltetrahydrofolic acid glucosamine salt).
1.4. Context of the assessment
Previous safety assessments by the SCF and EFSA
The SCF evaluated the UL for folate in 2000 (SCF, 2000). The committee considered that the modification of cobalamin 2 neurological sequelae in pernicious anaemia (PA) patients as a result of folic acid supplementation, such as masking of the haematological signs and the potential of progression of neurological symptoms, was the most serious adverse effect known in humans. The committee noted that correction of the haematological signs in PA patients had been reported to frequently and consistently occur with daily folic acid intakes of 5000 μg/day, whereas insufficient data were available for evaluation of dose levels between 1000 and 5000 μg/day. The committee considered that ‘although no systematic toxicological studies of folic acid or other folates are available, an upper safe level can be set for (synthetic) folic acid (pteroylglutamic acid) on the basis of findings in PA patients treated with high doses of folic acid. There is no evidence for risk associated with high intakes of natural, reduced folates, and thus no data to set an UL for natural folate’. A UL for folic acid of 1000 μg/day was established for adults (≥18 years), considering that dosages up to 1000 μg of folic acid were unlikely to cause masking of the haematological signs in PA patients. The same UL was applied to pregnant and lactating women. ULs for children and adolescents (1–17 years) were extrapolated from the UL for adults on the basis of body weight (bw) (isometric scaling) (Table 1). No UL was established for infants (less than 1 year).
TABLE 1.
Overview of existing Tolerable Upper Intake Levels (ULs) for folic acid, in μg/day.
| Population group | SCF (2000) | IOM (1998) | NHMRC (2006) |
|---|---|---|---|
| Infants | |||
| 0–6 mo | Nd | Nd | Nd |
| 7–12 mo | Nd | Nd | Nd |
| Children and adolescents | |||
| 1–3 y | 200 | 300 | 300 |
| 4–6 y | 300 | – | – |
| 4–8 y | – | 400 | 400 |
| 7–10 y | 400 | – | – |
| 9–13 y | – | 600 | 600 |
| 11–14 y | 600 | – | |
| 14–18 y | – | 800 a | 800 |
| 15–17 y | 800 | – | – |
| Adults | |||
| ≥18 y | 1000 a | – | – |
| ≥19 y | – | 1000 a | 1000 a |
Abbreviations: IOM, Institute of Medicine; mo, month; Nd, not defined; NHMRC, National Health and Medical Research Council; Australia and New Zealand; SCF, Scientific Committee on Food; y, year.
Including pregnant and lactating women.
The safety of l‐5‐methyltetrahydrofolic acid calcium salt (l‐5‐MTHF‐Ca) as a novel nutrient source for use in food supplements and addition to foods was previously assessed by EFSA (EFSA AFC Panel, 2004). The Panel on food additives, flavourings, processing aids and materials in contact with food (AFC) concluded that ‘the use of l‐5‐MTHF‐Ca as a source of folate in foods for particular nutritional uses, food supplements and foods intended for the general population, with a tolerable upper level of 1000 μg/adult person/day is not of concern from a safety point of view. This evaluation is based on the assumption that the previously established tolerable upper intake level for folic acid of 1000 μg/adult person/day would also be applied to the combined intake of folic acid and l‐5‐MTHF‐Ca (expressed as folic acid)’.
In 2008, the European Food Safety Authority (EFSA) established an EFSA Scientific Cooperation Working Group (ESCO WG) on the ‘Analysis of risks and benefits of fortification of food with folic acid’, with the aim of sharing experiences and concerns regarding folic acid food fortification among Member States. In this context, EFSA and the Swedish National Food Administration organised a scientific meeting on ‘Folic Acid: An Update on Scientific Developments’ in 2009, with the aim to consider the evidence regarding folic acid and risk of cancer. The discussions were reported in an EFSA meeting summary report (EFSA, 2009).
The safety and efficacy of folic acid as a feed additive has been evaluated by EFSA FEEDAP Panel (EFSA FEEDAP Panel, 2012). The FEEDAP Panel concluded that the use of folic acid in animal nutrition was not of concern for the safety of consumers under the proposed conditions of use.
The safety of (6S)‐5‐methyltetrahydrofolic acid glucosamine salt (5‐MTHF‐glucosamine) as a novel nutrient source for use in food supplements was previously assessed by EFSA (EFSA ANS Panel, 2013). The Panel on Food Additives and Nutrient Sources added to Food (ANS) noted that 5‐MTHF‐glucosamine dissociates to its respective individual ions in the digestive tract, and therefore carried out the toxicity assessment based on the individual components, i.e. 5‐MTHF and glucosamine. The requested condition of use was up to a dose of 1800 μg/day, corresponding to 1000 μg 5‐MTHF and 800 μg glucosamine. Regarding the 5‐MTHF moiety, the ANS Panel referred to the previous assessment of l‐5‐MTHF‐Ca by the AFC Panel. Regarding the glucosamine moiety, the ANS Panel referred to the NDA Panel opinion on the safety of glucosamine hydrochloride from Aspergillus niger published in 2009 (EFSA NDA Panel, 2009) and considered that the maximum exposure to glucosamine resulting from the proposed uses and use levels was negligible. The ANS Panel concluded that the proposed use and use levels of 5‐MTHF‐glucosamine was not of safety concern.
A request for the extension of use of l‐5‐MTHF‐Ca to infant and follow‐on formula, baby food and processed cereal‐based food was requested in 2018 and evaluated by the NDA Panel with a positive outcome (EFSA NDA Panel, 2020). The applicant proposed to use l‐5‐MTHF‐Ca to meet the compositional requirements for folate in infant formula and follow‐on formula and in processed cereal‐based food and baby food. According to Commission Delegated Regulation (EU) 2016/127 3 , infant formula and follow‐on formula must contain folate at concentrations between 15 and 47.6 μg dietary folate equivalents (DFE 4 )/100 kcal. As per Commission Directive 2006/125/EC 5 , processed cereal‐based food and baby food for infants and young children must contain a maximum of folic acid of 50 μg/100 kcal.
Average requirements and Population Reference Intakes for folate
Regarding folate dietary requirement, the NDA Panel established an average requirement (AR) for folate of 250 μg DFE/day and a population reference intake (PRI) of 330 μg DFE/day for adults (EFSA NDA Panel, 2014). For infants aged 7–11 months, an Adequate Intake (AI) of 80 μg DFE/day was derived by extrapolating upwards from the estimated folate intake in exclusively breast‐fed infants. For children, ARs were extrapolated from the AR for adults using allometric scaling 6 and growth factors 7 and considering differences in reference weights. PRIs ranging from 120 μg DFE/day for 1–3 year‐old children to 330 μg DFE/day for boys and girls aged 15–17 years were derived. For pregnant women, an AI of 600 μg DFE/day was derived based on a study on maintenance of serum and red blood cell folate concentrations in pregnancy. For lactating women, an additional intake of 130 μg DFE/day was considered to cover folate losses via breast milk; a PRI of 500 μg DFE/day was derived for this population group.
Conversion of l‐5‐MTHF‐Ca and 5‐MTHF‐glucosamine into dietary folate equivalents
The NDA Panel was asked to deliver a scientific opinion on the conversion of l‐5‐MTHF‐Ca and 5‐MTHF‐glucosamine into DFE (EFSA NDA Panel, 2022a). The Panel proposed to use the same factor as for folic acid for conversion of 5‐MTHF into DFE for intakes <400 μg/day. As such intake levels are unlikely to be exceeded through fortified food consumption, the Panel considered that the conversion factor of 1.7 relative to natural food folate (NF) could be applied to 5‐MTHF added to foods and to food supplements providing <400 μg/day. At 400 μg/day, 5‐MTHF was found to be more bioavailable than folic acid and a conversion factor of 2 was proposed for this intake level and for higher intakes. The derived DFE equations were DFE = NF + 1.7 × FA + 1.7 × 5‐MTHF for fortified foods and food supplements providing intakes <400 μg/day; and DFE = NF + 1.7 × FA + 2.0 × 5‐MTHF for food supplements providing intakes ≥400 μg/day.
1.5. Previous assessments by other bodies
Similar to the SCF (Section 1.4), previous safety assessments of folate intake by other bodies consistently considered the risk of ‘masking’ PA, due to the correction of the anaemia by ‘high’ folic acid, as the critical health concern regarding ‘high’ folic acid intake, because of the risk that neuropathy would progress undiagnosed to a point where it could become irreversible (EVM, 2003; FAO/WHO, 2004; IOM, 1998; NHMRC, 2006).
In its evaluation of UL for folate, the Institute of Medicine (IOM) concluded that ‘no adverse effects had been associated with the consumption of the amounts of folate normally found in fortified foods’ and restricted its review to evidence concerning intake of folate supplements (IOM, 1998). The expert committee concluded that ‘the weight of the limited but suggestive evidence that excessive folate intake may precipitate or exacerbate neuropathy in cobalamin‐deficient individuals justifies the selection of this endpoint as the critical endpoint for the development of a UL for folate’. Case reports of cobalamin‐deficient patients who had received oral doses of folate and experienced progression of neurological disorders were used to identify a reference point (RP). A lowest observed adverse effect level (LOAEL) of 5000 μg/day of ‘folate’ was derived, which was divided by an uncertainty factor (UF) of 5 considering the severity of neurological complications and the use of a LOAEL as a RP. As a result, a UL for adults of 1000 μg/day of ‘folate’ from food supplements or fortified food was established. The committee considered that this UL was also applicable to pregnant and lactating women. For infants the UL could not be determined because of a lack of data on adverse effects in this age group and concern about the infant's ability to handle excess amounts. The UL for children (≥1 year) and adolescents was derived from the UL for adults by applying isometric scaling 8 (Table 1).
In line with the approach followed by the IOM, the National Health and Medical Research Council (NHMRC) established a UL of 1000 μg/day of folic acid for adults, applicable also to pregnant and lactating women (NHMRC, 2006) (Table 1). The ULs for children and adolescents were derived by applying isometric scaling. No UL for infants was set. The ULs apply to folic acid intake from fortified foods or food supplements.
The UK Expert Group on Vitamins and Minerals concluded that data from animal or human studies were insufficient to establish a safe upper level for folic acid (EVM, 2003). A guidance level (GL) for supplemental folic acid of 1000 μg/day (equivalent to 17 μg/kg bw/day for a 60 kg adult) was established for adults. Assuming a maximum intake from food of approximately 490 μg/day (97.5th percentile estimate), the expert group concluded that a total dose of 1500 μg/day (equivalent to 25 μg/kg bw/day in a 60 kg adult) was not expected to have any adverse effects. GLs for children were not set as there were no data reporting adverse effects in children. The UK Scientific Advisory Committee on Nutrition (SACN) published recommendations regarding folic acid fortification, in which potential adverse effects associated with excess folic acid intake were evaluated (Scientific Advisory Committee on Nutrition (SACN), 2006, 2009, 2017). In its latest review, the SACN reviewed the evidence on masking/exacerbation of low cobalamin status, cognitive decline in older individuals, cancer (prostate, breast, colorectal and overall), and long‐term effects of unmetabolised folic acid (UFA) in the systemic circulation. The established GL was retained.
No UL for folate or folic acid has been established by the World Health Organization (WHO)/Food and Agriculture Organization (FAO) (FAO/WHO, 2004). Considering the IOM assessment, the WHO concluded that ‘400 μg/day of folic acid, in addition to dietary folate, would seem safe. There is probably no great risk of toxicity at a range of intakes between 400 and 1000 μg of folic acid per day, with the exception of some increased difficulty in diagnosing pernicious anaemia’.
2. DATA AND METHODOLOGIES
2.1. Problem formulation
In accordance with the draft NDA Panel guidance on establishing and applying ULs for vitamins and essential minerals (EFSA NDA Panel, 2022b), the assessment questions underlying the UL evaluation are formulated as follows:
What is the maximum level of total chronic daily intake of folate (from all sources) which is not expected to pose a risk of adverse health effects to humans? (Hazard identification and hazard characterisation)
What is the daily intake of folate from all dietary sources in EU populations? (Intake assessment)
What is the risk of adverse effects related to the intake of folate in EU populations, including attendant uncertainties? (Risk characterisation)
The hazard identification and hazard characterisation relate to the identification of adverse health effects of a given nutrient and the qualitative and quantitative evaluation of the adverse health effects associated with the nutrient, including dose–response assessment and derivation of an UL, if possible.
Adverse (health) effects are defined as ‘a change in the morphology, physiology, growth, development, reproduction or life span of an organism, system or (sub)population that results in an impairment of functional capacity to compensate for additional stress or an increase in susceptibility to other influences (EFSA Scientific Committee, 2017a; FAO/WHO, 2009). The observable effects of high nutrient intake within the causal pathway of an adverse health effect can range from biochemical changes without functional significance (e.g. certain changes in enzyme activity) to irreversible clinical outcomes. Notably, some changes that occur before clinical manifestations could be used as surrogate or predictive markers of subsequent adverse health effects, i.e. biomarkers of effect’ (EFSA NDA Panel, 2022b).
Priority adverse health effects, i.e. those that are expected to play a critical role for establishing a UL, were identified in consultation with a panel of qualified experts on folate 9 and after discussion by the ULs Working Group (WG) as follows: development of neuropathy in humans with low cobalamin status, impairment of cognitive function in humans with low cobalamin status, risk of colorectal cancer (CRC) and risk of prostate cancer. The rationale for the prioritisation is detailed in the protocol (Annex A).
As a result of the problem formulation, the overarching risk assessment questions were further specified into assessment sub‐questions (sQs) and the methods to address each sQ was selected, as outlined in Table 2. The assessment should cover folate from all dietary sources, including all forms of folate authorised for addition to foods and food supplements in the EU (i.e. folic acid, l‐5‐methyltetrahydrofolic acid calcium salt and (6S)‐5‐methyltetrahydrofolic acid glucosamine salt).
TABLE 2.
Assessment sub‐questions and methods to address them.
| Sub‐question | Method | |
|---|---|---|
| sQ1 | Absorption, distribution, metabolism and excretion (ADME) of the different forms of folate | |
| 1a. What is the ADME of the different forms of folate in humans? | Narrative review | |
| 1b. Are there differences related to age or other individual factors, e.g. genetic polymorphisms of folate or cobalamin metabolism? | Narrative review | |
| sQ2 | Biomarkers of exposure to folate | |
| 2a. What is the dose–response relationship between total folate intake and serum/plasma or red blood cell (RBC) folate concentrations in adults? | Systematic review | |
| 2b. How does serum unmetabolised folic acid reflect ‘high’ folic acid exposure? What is the relevance of this marker as biomarker of exposure? | Narrative review | |
| sQ3 | Neuropathy and impairment of cognitive function in humans with low cobalamin status | |
| 3a. What is the relationship between ‘high’ folate intake and the development of neuropathy in humans with low cobalamin status? Could a dose–response be characterised? | Systematic review | |
| 3b. What is the relationship between ‘high’ folate intake and the impairment of cognitive function in humans with low cobalamin status? Could a dose–response be characterised? | Systematic review | |
| 3c. What are the potential mechanisms/mode(s) of action underlying the relationships between folate intake and these endpoints? | Narrative review | |
| sQ4 | Risk of cancer | |
| 4a. Does ‘high folate’ intake increase the risk of cancer? | Narrative review | |
| 4b. Does ‘high folate’ intake increase the risk of colorectal cancer in human adults? If so, could a dose–response be characterised? | Systematic review | |
| 4c. Does ‘high folate’ intake increase the risk of prostate cancer in human adults? If so, could a dose–response be characterised? | Systematic review | |
| 4d. What are the potential mechanisms/mode(s) of action underlying the relationships between folate intake and these endpoints? | Narrative review | |
| sQ5 | Other adverse health effects | Narrative review |
| What other adverse health effects have been reported to be associated with ‘high’ intake of folate? | ||
| sQ6 | Folate intake | |
| 6a. What are the levels of folate in foods, beverages and food supplements in the EU? | Food composition and food consumption data in the EU | |
| 6b. What is the distribution of daily folate intake from all dietary sources in EU populations and subgroups thereof? |
2.2. Hazard identification and characterisation
Preparatory work regarding sub‐questions sQ1 to sQ5 was performed by a contractor. 10 The technical report of the contractor is published (Åkesson et al., 2023). The technical report served as the primary source of information for this assessment. The Panel made an independent evaluation of the evidence and adapted the outcome of the contractor's work where needed.
2.2.1. Data
A description of the processes applied for evidence retrieval, study selection and data extraction is provided below. These steps were conducted by a contractor and were undertaken by the Karolinska Institutet in collaboration with the University of Oslo. Detailed description of the steps is published in the final report of this outsourcing project (Åkesson et al., 2023).
2.2.1.1. Priority adverse health effects
To address sQ3a, sQ3b, sQ4b and sQ4c, relevant human studies on the selected adverse health effects were identified through systematic searches of the literature in MEDLINE (Ovid), Embase (Ovid) and Cochrane Central Register of Controlled Trials for articles published in English. The search strategies were created by information specialists of the Karolinska Institutet and peer‐reviewed by information specialists at University of Oslo and EFSA. The searches were performed on 7 March 2022 regarding sQ3a and SQ3b (combined search) and 18th of February 2022 regarding sQ4b and sQ4c (combined search). Grey literature was not searched.
Retrieved articles were screened in duplicate in Distiller SR® at title and abstract level, also with the use of the artificial intelligence tool of Distiller SR®, and at full text level for inclusion/exclusion according to the criteria defined in the protocol (Annex A). Relevant systematic reviews were hand‐searched for additional pertinent studies. Reviews, expert opinions, editorials, letters to the editors, abstracts, posters and theses were excluded.
Eligible designs: eligible study designs were limited to prospective designs, i.e. human controlled trials (HCTs; randomised [RCT] or non‐randomised), prospective cohort studies (PCs) and nested case–control studies (NCCs). Regarding sQ3a, relevant case reports/series have been gathered in several reviews (Berry, 2019; IOM, 1998; Savage & Lindenbaum, 1995; SCF, 2000; van Gool et al., 2020). The period of publication of these case reports/series spans from 1947 to 1990, with the large majority published in the 1940s–1950s. Thus, previous reviews were used to identify the relevant publications for sQ3a.
Eligible study populations: studies were eligible if they involved individuals of any age, either healthy individuals or diseased individuals, if the disease was considered not to be related to the exposure‐outcome relationship.
Eligible exposure measurements: human controlled trials were eligible if they investigated oral folate supplementation (in any form, including folic acid or 6S‐5‐MTHF salts) vs. placebo/no treatment/lower doses. Observational studies were eligible if they measured folate intake (i.e. total folate or any specific form thereof) by dietary assessment methods or used accepted biomarkers of folate intake, i.e. plasma/serum/RBC folate (see Section 3.3). Studies investigating the relationship between serum/plasma unmetabolised folic acid concentration or plasma/serum 5‐MTHF concentration and the priority adverse health effects were also included to inform sQ2b.
In relation to sQ3a and sQ3b, 5804 unique references were identified after removing duplicates (flow chart in Appendix A.2). The title and abstract screening left 82 relevant articles that underwent a full‐text review. No eligible study was retrieved in relation to sQ3a. Regarding sQ3b, one RCT and three observational studies were included.
In relation to sQ4b and SQ4c, 2644 unique references were identified after removing duplicates (flow chart in Appendix A.3). The title and abstract screening left 139 relevant articles that underwent a full‐text review. A total of 63 publications were included, i.e. eight reports from six RCTs and 41 reports from observational studies addressing risk of colorectal cancer and two reports from one RCT and 14 reports from observational studies addressing prostate cancer.
Data were extracted by three extractors of the Karolinska Institutet into Microsoft Excel®, for the purpose of data plotting and analysis, and in Microsoft Word® for the preparation of evidence tables.
2.2.1.2. Other background information
The evidence used to inform sQ1, sQ2, sQ3c, SQ4a, SQ4d and SQ5 was retrieved from textbooks, authoritative reviews and research papers through non‐systematic searches in bibliographic databases, and was synthesised as narrative reviews.
2.2.2. Methodologies
The methodology for this assessment follows the guidance for establishing ULs developed by the EFSA NDA Panel (2022b). Other guidance documents from EFSA were also considered, including those addressing the application of the systematic review methodology in food and feed safety assessments (EFSA, 2010), the principles and processes for dealing with data and evidence in scientific assessments (EFSA, 2015b), the statistical significance and biological relevance (EFSA Scientific Committee, 2011), the biological relevance of data (EFSA Scientific Committee, 2017a), the use of the weight of evidence approach (EFSA Scientific Committee, 2017b), the appraisal and integration of evidence from epidemiological studies (EFSA Scientific Committee, 2020) and the analysis of uncertainty in scientific assessments (EFSA Scientific Committee, 2018).
2.2.2.1. Evidence appraisal
A risk of bias (RoB) appraisal of individual studies, i.e. evaluation of their internal validity, was applied to eligible studies which addressed sQ3a, sQ3b, sQ4b and sQ4c. The appraisal was performed by two independent reviewers from the Karolinska Institutet using a customised version of the Office of Health Assessment and Translation (OHAT) RoB tool developed by the US National Toxicology Program (NTP) (OHAT‐NTP, 2015). Any discrepancies in the RoB assessment for each bias domain were discussed among the assessors. If there was disagreement, a third reviewer was consulted for resolution.
The RoB criteria and rating instructions provided therein were tailored to the specific research questions, for the questions addressing: (1) consideration of potential confounders, (2) confidence in the exposure characterisation and (3) confidence in the outcome assessment (Appendix B).The OHAT RoB tool proposes five response options for each RoB question: definitely low RoB (++), probably low RoB (+), not reported (NR), probably high RoB (−), definitely high RoB (−–).
Studies were categorised according to their overall RoB based on a three‐tier system (i.e. at low (tier 1), moderate (tier 2) or high (tier 3) RoB), according to the strategy proposed by OHAT (OHAT‐NTP, 2019) (Appendix B).
2.2.2.2. Evidence synthesis
Regarding sQ2, sQ3 and sQ5, results from eligible studies were plotted using descriptive forest plots, when three or more studies reported on the same outcome. For intervention studies with several folate/folic acid doses, the mean difference between the highest dose group and control group was selected for the plot, unless specified otherwise. For observational studies reporting both continuous and categorical analyses, the latter was selected for the plot. Further information is provided in the technical report from the contractor (Åkesson et al., 2023).
2.2.2.3. Evidence integration and uncertainty analysis
Hazard identification
The hazard identification step consisted of assessing the evidence for a causal positive relationship between folate intake and the health effects identified. The available body of evidence is organised in separate lines of evidence (LoE), which are classified in hierarchical order:
Standalone main LoE: Studies on disease endpoints (e.g. incidence of CRC). These studies could, on their own, answer the sQ directly.
Standalone surrogate LoE: Studies on endpoints which are surrogate measures of the disease risk (e.g. incidence of colorectal adenomas for risk of CRC). These studies also could, on their own, answer the sQ, on the assumption that a sustained increase in (or progression of) the surrogate measure over time would eventually lead to an increased risk of disease. However, the Panel is aware of the uncertainty inherent in this assumption, and this was considered in the uncertainty analysis (UA) for each sQ.
Conclusions on each health effect are reached by study design, through considering the uncertainties in the body of evidence (BoE) and in the methods.
A stepwise approach was applied as illustrated in Figure 1 and described below.
FIGURE 1.
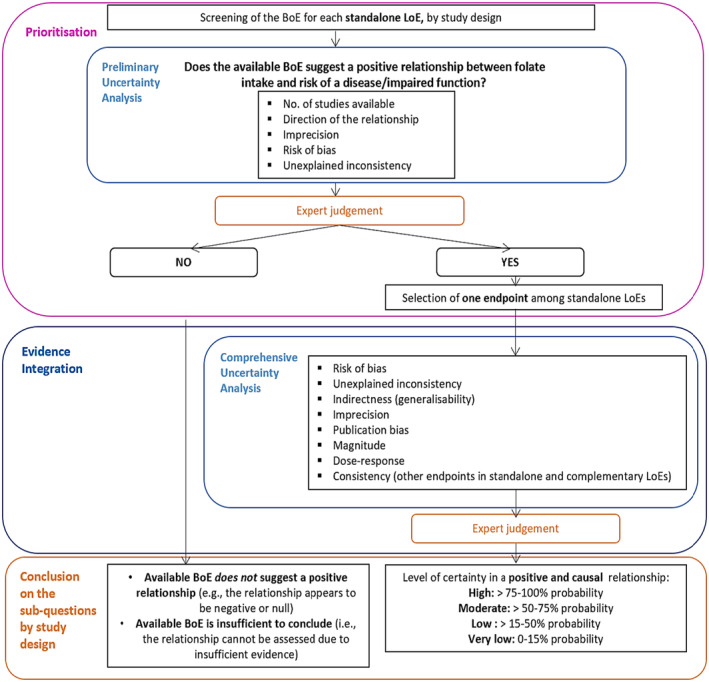
Stepwise approach for evidence integration and uncertainty analysis. BoE, body of evidence; LoE, line of evidence.
Prioritisation
A prioritisation step is applied to identify health effects for which the available BoE suggests a positive relationship between dietary intake of folate and risk of disease/impaired function based on a preliminary UA and expert judgement. The Panel considers that health effects for which the available BoE (i) does not suggest a positive relationship (i.e. the relationship appears to be negative or null) or (ii) is insufficient to conclude on a relationship, cannot be used to inform the setting of a UL for folate. Data gaps and research needs are identified, where appropriate.
When the available BoE suggests a positive association between folate intake and the risk of a disease/impaired function, a comprehensive UA is performed to inform the formulation of the hazard identification conclusions, i.e. judgement on the level of certainty for a causal relationship. For health effects with more than one standalone LoE, the comprehensive UA is undertaken for the endpoint with the highest level of evidence for a positive relationship with the exposure.
Evidence integration and conclusions on the prioritised sub‐questions, by study design
The OHAT‐NTP framework for the formulation of hazard identification conclusions is used and adapted (OHAT‐NTP, 2019). The BoE on a particular sQ is given an initial level of certainty based on study design, which is assigned by considering four features of the design (i.e. exposure is experimentally controlled, exposure occurs prior to the endpoint, endpoint is assessed at individual level and an appropriate comparison group is included in the study). As a result, OHAT assigns a ‘high’ confidence rating to human controlled trial (HCTs), a ‘moderate’ confidence rating to PCs and a ‘low’ confidence rating to case series/reports 11 (OHAT‐NTP, 2019). In accordance with EFSA's Scientific Committee recommendation probability has been used as the means for expressing uncertainty (EFSA Scientific Committee, 2018) and OHAT's ‘initial confidence ratings’ have been translated into ‘initial levels of certainty’ expressed as approximate probability ranges. Similarly, the final level of certainty for a positive and causal relationship between the exposure and risk of disease is expressed as probability ranges, corresponding to four levels of certainty, i.e. ‘high’ (>75%–100% probability), ‘moderate’ (>50%–75% probability), ‘low’ (>15%–50% probability) and ‘very low’ (0%–15% probability). This standard four‐level probability scale facilitates the formulation of experts' judgement and is used for the formulation of hazard identification conclusions in nutrient risk assessments.
A schematic representation of the approach for assessing the final level of certainty in the hazard identification conclusions by study design is provided in Figure 2. This initial rating is downgraded on the basis of factors that decrease certainty in the results (RoB, unexplained inconsistency, indirectness or lack of applicability, imprecision and publication bias) and upgraded for factors that increase certainty in the results (large magnitude of effect, dose response, consistency across study designs/populations/animal models or species and consideration of residual confounding or other factors that increase the certainty in the causal nature of the relationship).
FIGURE 2.
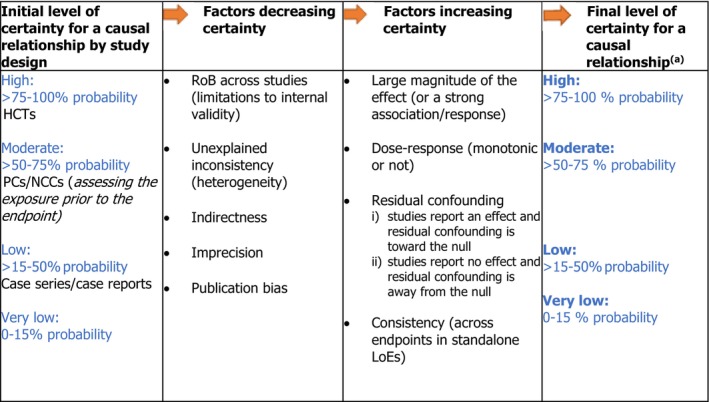
Approach applied to assign the final level of certainty in a causal relationship. Adapted from OHAT‐NTP (2019). HCT, human controlled trial; LoE, line of evidence; NCC, nested case–control; PC, prospective cohort study; RoB, risk of bias. aAs an example, a ‘high level of certainty’ means that, based on the available evidence, experts are 75%–100% certain that folate intake is positively and causally associated with the adverse health outcome of interest.
Reaching overall conclusions on the prioritised sub‐questions
Adapted from the OHAT‐NTP approach, the overall conclusion regarding the relationship is formulated as follows:
hazard identification conclusions are primarily based on the BoE providing the highest level of certainty on the relationship;
consistent results across study designs could result in higher level of certainty on the causality of a positive relationship;
mechanistic or mode‐of‐action data are considered as other relevant supporting types of evidence; they could provide strong support or opposition for biological plausibility and could thus result in higher or lower certainty on the causality of the positive relationship.
It is noted that the formulation of hazard identification conclusions necessarily requires expert judgement. The value of this type of approach is that it involves using a reproducible and transparent framework for expressing uncertainty in the evidence and in the methods.
Hazard characterisation
At this step, evidence is integrated to select the critical effect(s) and establish the UL (EFSA NDA Panel, 2022b). The rationale for the derivation of ULs for folate is documented in Section 3.5 of the Opinion.
2.3. Dietary intake assessment
The assessment follows the approach outlined in the protocol for the intake assessments performed in the context of the revision of ULs for selected nutrients (EFSA, 2022). The principles of the data cleaning and methodology used for the present intake assessment are described in Annex B.
2.3.1. Data
Food intake data from the EFSA Comprehensive European Food Consumption Database (hereinafter referred as Comprehensive Database) 12 and data on natural folate content in foods from the EFSA food composition database (FCDB)12 as available in 2022 were used.
Food consumption data
The Comprehensive Database provides a compilation of existing national information on food consumption at individual level collected through repeated non‐consecutive 24‐h dietary recalls or dietary records (EFSA, 2011; EFSA ANS Panel, 2013). The latest version of the Comprehensive Database, updated in 2022, contains results from a total of 83 different dietary surveys carried out in 29 different European countries (including EU Member States, pre‐accession countries and the United Kingdom) covering 154,388 individuals. In the present assessment, food consumption surveys from 22 EU member states covering at least 2 days per subject were used.
Food composition data
Composition data for folate in foods and beverages were derived from the EFSA Nutrient Composition Database, which was compiled as a deliverable of the procurement project ‘Updated food composition database for nutrient intake’ (Roe et al., 2013). When needed, publicly available national food composition databases and the Mintel Global New Products Database (GNPD) 13 were used to complement EFSA's food composition database.
Other data sources
Since folate is sensitive to heat treatment of foods, to be able to properly consider the cooking processes in the assessment, a database of retention factors was extracted from the publicly available 2008 document of EUROFIR, namely ‘Report on collection of rules on use of recipe calculation procedures including the use of yield and retention factors for imputing nutrient values for composite food’. 14
To complement EFSA's intake assessment, folate intake estimates from natural sources, from addition to foods and from food supplements based on nationally representative food consumption surveys without date limits were collected. These data have been also used to evaluate the accuracy of the results obtained, comparing EFSA's estimates with published intake estimates from the same surveys with the same (or similar) window of data collection and population groups, when available (EFSA, 2022). Data were collected between September and November 2021 by contacting 64 competent authorities in 37 European countries through EFSA Focal Points 15 and the EFSA Food Consumption Network. 16 An additional search in sources of bibliographic information (Google Scholar, PubMed) was performed to collect reports of national surveys included in the Comprehensive Database that had not been obtained through the competent authorities. Between August and October 2022, EFSA contacted all EU Member States and Norway through the European Commission Working Group on Food supplements and Fortified foods 17 and collected data on the intake of folate specifically from food supplements.
The Mintel GNPD was used as a data source to identify the type of folate containing food supplements and fortified foods available on the EU market. The search was limited to the past 5 years, from November 2017 to November 2022. The Panel notes that this search captures only those products that were newly introduced on the market and for which the packaging was changed during this period. Therefore, the information collected is indicative and does not necessarily represent a comprehensive overview of the products available on the market.
2.3.2. Methodologies
Intake assessment from natural sources
Composition data on folate was extracted from the EFSA FCDB and was subject to a cleaning procedure. As the scope of the intake assessment was to consider natural sources of folate only, a data cleaning strategy was applied to exclude fortified foods from the composition database (Annex B). This is with the exception of infant and follow‐on formula for which data from the Mintel's GNPD were used for the calculations. Indeed, the minimum content of folate in these food categories is subject to regulatory requirements to guarantee an adequate supply of the nutrient to the consumers (Regulation (EU) 2016/1273 and Regulation (EU) 2017/1522 18 ). As a result, a pooled database containing data from 12 countries was created. Folate intake estimates were calculated by matching the food intake data from the Comprehensive Database and the data on folate content in foods from the EFSA FCDB. The FoodEx2 classification and description system was used to facilitate the linkage between the databases (EFSA, 2015a). Since folate is sensitive to heat treatment of foods, retention factors were applied to adjust the folate content in foods for losses during cooking.
Dietary intakes of folate in μg/day from natural food sources were calculated at individual level. The resulting intakes per food item were summed up to obtain total daily intakes of folate for each individual. The mean, P5, Median and P95 of intakes were subsequently calculated for each survey by population group and sex, as well as total populations.
The data cleaning procedure and methodology followed for the assessment are described in details in Annex B.
Intake assessment from fortified foods and food supplements
Folate intake data from recent national food consumption surveys conducted in European countries, including specific estimates of intake from food supplements and/or fortified foods, were extracted (Annex D).
Information on food products fortified with folic acid and folic acid‐containing supplements available on the EU market, and their folic acid content as reported on the label, were extracted from the Mintel GNPD. These data were used qualitatively to describe the types of fortified foods and food supplements available and to gain insight into their potential contribution to total folate intake.
2.4. Public consultation
In line with EFSA's policy on openness and transparency, and for EFSA to receive comments from the scientific community and stakeholders, a draft of the Scientific Opinion was released for public consultation from 22 May 2023 to 30 June 2023. 19 The outcome of the public consultation is described in a technical report published as Annex E to this Scientific Opinion.
3. ASSESSMENT
The assessment addresses folate from all dietary sources, i.e. foods (including fortified foods), beverages (including water) and food supplements (EFSA NDA Panel, 2022b).
3.1. Folate chemistry
Folate is a generic term used for a group of compounds with a core structure consisting of a pterin moiety linked through a methylene bridge to p‐aminobenzoic acid, to which one or more glutamate residues are bound by peptide bonds. The pterin moiety exists in different oxidation states (reduced, partially reduced and oxidised) and can be substituted at the N‐5 or N‐10 position by different one‐carbon units.
Natural folates are reduced vitamers that usually exist in tissues as polyglutamates containing five to seven glutamate residues. They are unstable, and some losses occur in the presence of light and oxygen and at high temperatures (EFSA NDA Panel, 2014).
Tetrahydrofolate (THF) is the fully reduced form of the vitamin and is found in the cell together with 10‐formyl‐THF, 5‐formyl‐THF, 5,10‐methenyl‐THF, 5,10‐methylene‐THF and 5‐methyl‐THF (Figure 3). The folate forms are interconverted through enzyme‐mediated reactions and retained in the cell as polyglutamates (Section 3.2 and Figure 4 in Section 3.2.3).
FIGURE 3.
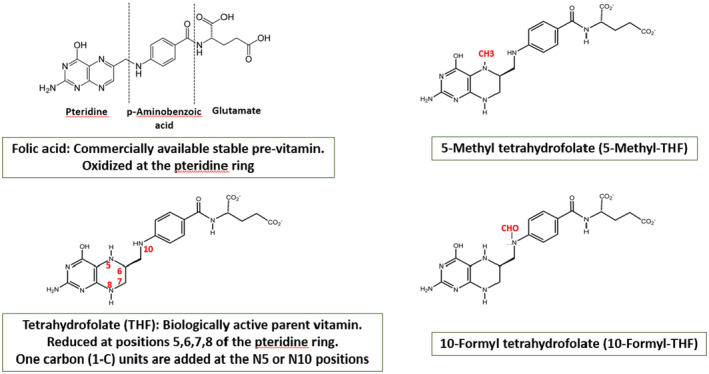
Structures of folic acid, 5 methyl‐tetrahydrofolate, tetrahydrofolate and 10‐formyl‐THF.
FIGURE 4.
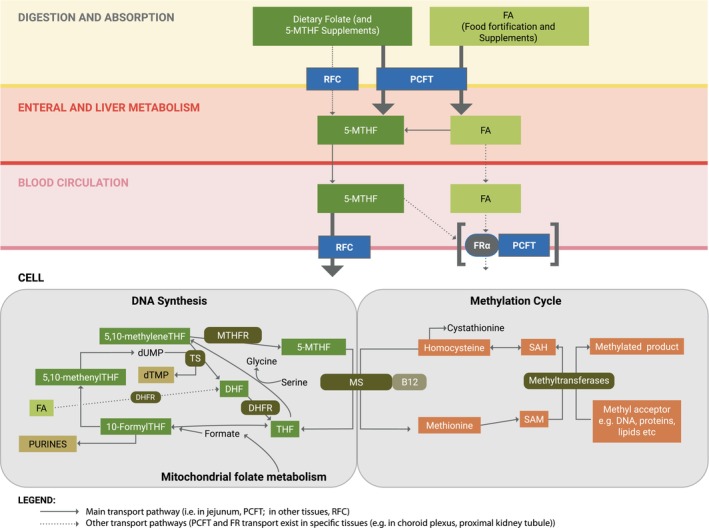
Overview of folate metabolism and transport. Folate metabolism is depicted, from its intestinal absorption to its intracellular function as a carrier of one‐carbon units (methyl, methylene, methenyl and formyl moieties) in the de‐novo synthesis of purines and thymidine and the transfer of methyl groups to methionine for use in methylation reactions. Dietary folates are converted from polyglutamate forms to monoglutamates in the duodenum and are absorbed in the intestine primarily via the PCFT, but also to some extent through the RFC, depending on local pH. Folates enter the enteral and hepatic system mainly as 5‐MTHF, and excess folates emerge into the blood circulation in this form. 5‐MTHF enters cells via the RFC and becomes incorporated in the cellular folate pool after passing through the cobalamin dependent enzyme, methionine synthase (MS), where the methyl group is removed and attached to homocysteine, producing methionine. THF, the other product of the MS reaction, is polyglutamated and picks up one‐carbon units as formyl groups from mitochondrial derived formate or as methylene groups from serine. 10‐Formyl groups are passed to intermediates in the de‐novo purine synthesis pathway, and 5,10‐methylene groups are used to produce thymidylate from dUMP. In specific tissues (e.g. choroid plexus, proximus kidney tubule), a family of receptors, named folate receptors (FRs), can transport 5‐MTHF or folic acid across cellular barriers by endocytosis, probably linked to the PCFT transporter. DHF, dihydrofolate; DHFR, dihydrofolate reductase; dUMP, deoxyuridine monophosphate; dTMP, deoxythymidine monophosphate; FA, folic acid; FR, folate receptor; MS, methionine synthase; MTHFR, 5,10‐methylenetetrahydrofolate reductase; PCFT, proton‐coupled folate transporter; RFC, reduced folate carrier; THF, tetrahydrofolate; TS, thymidylate synthetase; SAH, S‐adenosyl homocysteine; SAM, S‐adenosyl methionine.
Several synthetic forms of folates are authorised for addition to food or used in food supplements (Table 3). Folic acid is a fully oxidised monoglutamate. It is the most chemically stable form and is also the most widely used. It has vitamin activity after it has been fully reduced to THF. Other synthetic forms of folate include Ca‐salts or glucosamine salts of (6S)‐5‐methyl‐THF (denoted 5‐MTHF hereafter), e.g. 5‐MTHF‐glucosamine and CaLMF (EFSA NDA Panel, 2022a). 5‐MTHF has two chiral carbon atoms, i.e. the C‐atom in position 6 of the pteroyl moiety and the α‐C atom in the glutamic acid moiety.
TABLE 3.
Forms of folate authorised as nutrient sources in the EU.
| Addition to foods Regulation (EC) 1925/2006 a | Food supplements Directive 2002/46/EC b | |
|---|---|---|
| Pteroylmonoglutamic (folic) acid | x | x |
| Calcium‐l‐methylfolate | x | x |
| (6S)‐5‐methyltetrahydrofolic acid, glucosamine salt | x |
Regulation (EC) No 1925/2006 of the European Parliament and of the Council of 20 December 2006 on the addition of vitamins and minerals and of certain other substances to foods. OJ L 404, 30.12.2006, p. 26–38.
Directive 2002/46/EC of the European Parliament and of the Council of 10 June 2002 on the approximation of the laws of the Member States relating to food supplements (Text with EEA relevance). OJ L 183, 12.7.2002, p. 51–57.
3.2. Absorption, distribution, metabolism and excretion
3.2.1. Absorption and bioavailability
Native reduced monoglutamate food folates as well as synthetic folic acid or 5‐MTHF are absorbed by both an active, saturable and pH‐dependent carrier process, as well as by a passive, unsaturable mechanism (EFSA NDA Panel, 2014, 2022b). Polyglutamated forms of food folates are first hydrolysed by jejunal γ‐glutamyl hydrolase (EC 3.4.17.21) to their monoglutamate form.
Folate monoglutamates are transported by the reduced folate carrier (RFC; SLC19A1) and the proton‐coupled folate transporter (PCFT; SLC46A1) into the jejunal epithelial cell, however PCFT is considered the most important high‐affinity enteral folate transporter at the intestinal pH (EFSA NDA Panel, 2014, 2022a). Mechanistic studies have shown similar affinity of PCFT for folic acid and reduced folates at pH 5.5 (Zhao et al., 2010). Folate absorption by passive diffusion takes place primarily in the ileum. There is also folate absorption to a small extent in the large intestine (EFSA NDA Panel, 2014).
It is now considered that reduction and conversion of absorbed dietary folates and folic acid to 5‐MTHF takes place both in the intestinal cells and in the liver. Folate forms are exported through a carrier‐mediated process into the portal vein and systemic circulation. There is evidence from studies using stable isotopes that an undetermined fraction of folic acid may pass unchanged from the intestinal cells via the portal vein to the liver (Hu et al., 2016; Wright et al., 2005).
Folic acid undergoes a two‐stage reduction via dihydrofolate to THF by the enzyme dihydrofolate reductase (DHFR; EC 1.5.1.3). However, compared with rodents, the activity of DHFR in human liver is low and highly variable, which limits its ability to efficiently reduce folic acid (Bailey & Ayling, 2009). Under the conditions of high folic acid intake, DHFR is quickly saturated and UFA appears in the systemic circulation (EFSA NDA Panel, 2014, 2022a). Since folic acid is not a normal constituent of the body, concerns have been raised regarding potential adverse health effects of UFA.
Absorption and bioavailability of folate from foods may be affected by the food matrix as well as different food constituents. Natural food folates are bound by strong covalent bonds to macromolecules (proteins and carbohydrates) and thereby they become trapped in the food matrix and require enzymatic digestion in the gastrointestinal tract to be released for absorption (EFSA NDA Panel, 2022a). In contrast, folic acid and other synthetic folates added to food may interact with the food matrix (i.e. with folate binding protein) but their accessibility is less dependent on the food composition, which renders them more readily available for absorption (Ringling & Rychlik, 2017).
To account for differences in absorption efficiency and bioavailability of synthetic folic acid and natural folate forms, the concept of dietary folate equivalent (DFE) was proposed by IOM in 1998:
1 μg DFE = 1 μg food/natural folate
1 μg DFE = 0.6 μg folic acid from fortified food or as supplement consumed with food
1 μg DFE = 0.5 μg folic acid supplement taken on an empty stomach.
The values above correspond to a factor of 1.7 to convert folic acid consumed with food into DFE and a factor of 2 to convert folic acid taken on an empty stomach (EFSA NDA Panel, 2014, 2022a).
In a recent evaluation of the conversion of 5‐MTHF‐glucosamine and CaLMF to DFE (EFSA NDA Panel, 2022b), the Panel concluded that, at folate intakes below 400 μg/day, a conversion factor (CF) of 1.7, as for folic acid, can be applied for those two forms. At intakes above 400 μg/day, 5‐MTHF was found to be more bioavailable and a CF of 2 is recommended (Section 1.4).
3.2.2. Distribution and uptake into tissues
The most prevalent folate form in the circulation is 5‐MTHF (EFSA NDA Panel, 2014). In plasma, most folates are bound to albumin or soluble folate receptors (FRs, sometimes termed folate binding proteins) (Holm & Hansen, 2020). A smaller proportion exists as free folate. Average serum/plasma folate concentrations between 14 and 26 nmol/L have been reported in European populations (de Batlle et al., 2018; Hopkins et al., 2015; Mensink et al., 2016; Öhrvik et al., 2018). In countries with mandatory folic acid food fortification, such as the USA and Canada, the blood concentration of 5‐MTHF (both in plasma and in the red blood cell compartment) can be high, especially among those who are regular users of folic acid or multivitamin supplements. For example, the geometric mean total serum folate in US NHANES participants 2012–2016 was 40.6 (95% [confidence interval] CI 39.8, 41.4) nmol/L and 54.6 (53.1, 56.2) nmol/L in supplement users. People aged 60 years and over were found to have the highest concentrations among population age groups over 11 years old (Pfeiffer et al., 2019).
UFA is found in blood when intake of folic acid is high and the conversion capacity of DHFR is exceeded (EFSA NDA Panel, 2015). Early studies indicated that the appearance of UFA in the blood starts after ingestion of folic acid at doses around and above 200 μg (Kelly et al., 1997; Sweeney et al., 2003, 2006). More recent reports using advanced methodology show detectable UFA in nearly all serum samples after the implementation of mandatory folic acid fortification era in US and Canadian populations (Pfeiffer, Sternberg, Fazili, Yetley, et al., 2015), as well as in an older Irish population exposed to liberal voluntary fortification (Boilson et al., 2012). In the NHANES population‐based US study, the proportion of UFA corresponded to <3% of total serum folate (average 1.54 nmol/L among users of folic acid‐containing supplements vs. 0.79 nmol/L among nonusers), irrespective of the fasting state (Pfeiffer, Sternberg, Fazili, Yetley, et al., 2015). Recent data from the US NHANES shows that elevated UFA (>2 nmol/L) among fasting participants is most prevalent in supplement users (11%), persons over 70 years old (9%) and in those with kidney disease (Fazili et al., 2020). Fast clearance of folic acid from the circulation has been reported after a single oral dose (Lin et al., 2004) or intravenous injection of folic acid (Metz et al., 1961). However, folic acid has a very high affinity for soluble FRs present in serum (Holm & Hansen, 2020), which has been suggested to explain the detection of low plasma/serum UFA concentrations even in a fasting state (Bailey et al., 2015).
The internalisation of folate into cells and across specific barriers, such as the blood brain barrier, is a tissue specific process, which occurs against a concentration gradient and requires the involvement of three separate types of folate transporters (i.e. RFC, PCFT) and receptors (i.e. FRs) (Figure 4). The RFC is expressed in all tissues, including the brain, and is considered the main folate transporter from the blood circulation to tissues. It is optimally active at a pH of around 7.4 and has a high affinity for reduced folates (5‐MTHF and 5‐formylTHF) but the affinity for folic acid is about 100 times lower. RFC activity is reduced as pH drops, with minimal activity below pH 6.5 (Zhao et al., 2010). RFC does not contribute significantly to the intestinal absorption of folate. In contrast, PCFT, which has equivalent affinity for 5‐MTHF and folic acid, is optimally active at lower pH, and, as such, is the preferred folate carrier across the jejunal intestinal wall where the active transport of folate occurs. Outside the enteral system, PCFT is only active in some tissues, the most important being the kidney proximal tubule and the choroid plexus, where it may function in association with FRs to transport folates. PCFT has, however, minimal activity under physiological systemic pH conditions. Although much clarity on the role of PCFT has been achieved in the past decade, the various mechanisms of folate transport into the brain are still poorly understood (Zhao et al., 2017).
FRs are a family of glycoproteins, the most important being the FRα. Unlike RFC and PCFT, these receptors internalise folate by endocytosis and it is thought that PCFT functions within the acidic milieu of the endosome to export folate from the endosome into the cytosol (Zhao et al., 2017). While the FRα is capable of transporting folate into cells, it is not expressed in most normal cells and is mainly found on the apical surface of cells where it is not in contact with the circulation (Elnakat & Ratnam, 2004). Because folic acid has a high affinity for FRs, but has a lower affinity for RFC than reduced folates, it has been suggested that its uptake is mainly into tissues that express PCFT and FRs (Bailey et al., 2015).
5‐MTHF is transported into the cerebrospinal fluid (CSF) via the choroid plexus epithelial cells that form the blood–brain barrier. Both the RFC and FRα are important transporters for this process although evidence from studies of patients with hereditary deficiencies of FRα or PCFT suggest that receptor mediated transport linked to PCFT is essential to achieve adequate CSF 5‐MTHF. The concentration of 5‐MTHF in CSF is approximately three times higher than in plasma and low concentrations of CSF 5‐MTHF, or a low CSF to plasma ratio, has been associated with neurological conditions, including dementia (Surtees & Hyland, 1990). Folic acid has a somewhat higher affinity for the FRα than 5‐MTHF, although both are in the picomolar range, and it has been suggested that UFA might inhibit the binding of 5‐MTHF to FRs and thereby interfere with 5‐MTHF uptake into the brain (Bottiglieri & Reynolds, 2010). However, others have argued that the high affinity of 5‐MTHF for the FRα, coupled with its 20‐fold higher concentration, makes this an unlikely consideration (Kamen & Smith, 2004). Nevertheless, folic acid treatment is not recommended to patients with hereditary PCFT deficiency or cerebral folate deficiency, on the basis of its tight binding to FRs in the choroid plexus in the absence of functioning PCFT to release it from the endosome (Zhao et al., 2017).
Folates are retained in hepatic or other tissue cells after conversion to THF polyglutamates by folylpolyglutamate synthase (EC 6.3.2.17). Both 5‐MTHF monoglutamate and folic acid are poor substrates for folylpolyglutamate synthase and are unlikely to be retained by the tissues unless they are first converted to THF (Cichowicz & Shane, 1987; Osborne et al., 1993) (Section 3.2.3).
3.2.3. Metabolism
Reduced folate polyglutamates are the metabolically active forms, which serve as cofactors in folate‐dependent enzyme reactions in one‐carbon metabolism (Ducker & Rabinowitz, 2017). Folate is required for de novo purine and thymidine synthesis that is essential for DNA synthesis and repair, and consequently for cell division and tissue growth. 10‐formylTHF contributes formyl groups in the purine synthesis pathway and 5,10‐methyleneTHF contributes a methyl group to deoxyuridine monophosphate (dUMP) in the formation of deoxythymidine monophosphate (dTMP) (Figure 4). This latter reaction produces dihydrofolate (DHF) as co‐product, hence the cellular requirement for the enzyme DHFR, to replenish THF by reduction of DHF. Notably, folic acid is reduced to DHF, then to THF and enters the biologically active folate pool via this enzyme.
Folate cofactors are also fundamental for the normal functioning of the methylation cycle, which is responsible for the conversion of homocysteine to methionine and the production of the universal methyl donor S‐adenosylmethionine (SAM) (EFSA NDA Panel, 2014). SAM donates its methyl group to more than 100 methyltransferases for a wide range of substrates including DNA, hormones, proteins and neurotransmitters, which act as regulators of important physiological processes (EFSA NDA Panel, 2014). For example, DNA methylation is one of the epigenetic mechanisms regulating gene expression without altering the underlying DNA sequence (Armstrong, 2014). High maternal folic acid intake in pregnancy has been related to altered genome‐wide or site‐specific DNA methylation in cord blood (Caffrey et al., 2018; Irwin et al., 2019), newborn infants (Joubert et al., 2016) and in older offspring (Richmond et al., 2018). Similarly, an RCT of combined supplementation with folic acid (400 μg/day) and cobalamin (500 μg/day) for 2 years in older adults resulted in differential DNA methylation of several genes whereas no changes were detected in the placebo treated individuals (Kok et al., 2015). However, to date, alterations of DNA methylation by high folate intake have not been causally linked to adverse health effects. Further research is required to better understand the potential effects of epigenetic changes on health in responses to high dietary folate intake.
Folate interacts with cobalamin (vitamin B12) in one of the key reactions of the methylation cycle. Cobalamin, in the form of methylcobalamin, functions as a cofactor and 5‐MTHF acts as a co‐substrate for the enzyme methionine synthase (MS; EC 2.1.1,13) where homocysteine is methylated to methionine and 5‐MTHF is converted to THF (Figure 4). This reaction is a critical step for the retention of 5‐MTHF monoglutamates entering from the plasma circulation. 5‐MTHF monoglutamate is a poor substrate for the enzyme folylpolyglutamate synthetase (EC 6.3.2.17) and is lost from the cell if not metabolised through MS. In contrast THF produced in the reaction is a highly effective substrate for folylpolyglutamate synthetase and is polyglutamated by the addition of up to six to eight glutamate residues. Folate polyglutamates in the form of 10‐formyl‐THF and 5,10‐methylene‐THF are the preferred substrates for nucleotide synthesis (EFSA NDA Panel, 2014). 5‐MTHF polyglutamates are formed through the irreversible action of methylenetetrahydrofolate reductase (MTHFR; EC 1.5.1.20) on 5,10‐methylene‐THF polyglutamates and compete with 5‐MTHF monoglutamate for MS enzyme (Smulders et al., 2006). Therefore, cobalamin has a critical role for both retention of folates and for the provision of one‐carbon units for DNA synthesis and for methylation processes (Section 3.2.5.4). In contrast, folic acid does not require MS to be retained in the cell, since it is converted to THF via DHFR (Bailey & Ayling, 2009).
3.2.4. Catabolism and excretion
Cellular folate catabolism is poorly understood (Zheng & Cantley, 2019). Folate is catabolised by oxidative cleavage at the C9–N10 bond to p‐aminobenzoylglutamate, which is enzymatically (EC 2.3.1.5) acetylated in the liver before urinary excretion (Zheng & Cantley, 2019). In urine, most folate is excreted in form of (acetylated) breakdown products because of an effective glomerular reabsorption of intact folate. With increasing doses of folic acid, proportionally greater amounts of unaltered folic acid have been found to be excreted through the kidneys (Scott & Weir, 1986).
The majority of folate in faeces is derived from the gut microbiota, plus a small amount of endogenous folate from lysed enterocytes and non‐absorbed food folate (Ohrvik & Witthoft, 2011). Studies in rodents demonstrate rapid export of hepatic 5‐MTHF into the bile and show that bile drainage results in a 30%–40% depletion of serum folates, suggesting that the enterohepatic circulation is a major factor in folate homeostasis (Steinberg et al., 1979). There is a lack of human data regarding the extent of folate excretion into bile (EFSA NDA Panel, 2014); however biliary folate is expected to be reabsorbed to a large extent (EFSA NDA Panel, 2014; Lin et al., 2004).
During lactation, some folate is secreted into breast milk, mainly as 5‐MTHF, but also UFA has been detected in breast milk (EFSA NDA Panel, 2014; Su et al., 2022).
3.2.5. Factors affecting the ADME of folate
3.2.5.1. Life stages
There are conflicting data regarding the effect of age on folate absorption. One investigation found no difference in the luminal disappearance of labelled folic acid from synthetically prepared mono‐ and polyglutamate forms between younger and older adults (Bailey et al., 1984). In contrast, another study reported a 20% lower absorption (calculated by kinetic modelling based on plasma folate concentrations recorded for 6 h) after a single oral dose of around 200 μg labelled folic acid in subjects aged ≥50 years compared with younger adults (de Meer et al., 2005). Conditions such as atrophic gastritis with hypochlorhydria as well as the use of antiacid drugs have been associated with reduced folate absorption in studies with labelled folic acid (Russell et al., 1986, 1988). The change of the pH in the intestine due to these conditions may affect PCFT‐folate binding, with consequences on folate absorption. Reduced release of folate from food due to the insufficient secretion of hydrochloric acid from the gastric mucosa is also a contributing factor for the low amount of absorbed folate in these cases.
For women of reproductive age, a higher folate intake is recommended to prevent the occurrence of neural tube defects and to improve maternal folate status, both to account for the increased folate requirements during pregnancy and breast feeding and for pregnancy‐induced metabolic changes (EFSA NDA Panel, 2014; Nordic Council of Ministers, 2014). Pregnancy‐induced adaptations of one‐carbon metabolism (in which folate and other B‐vitamins are involved) are reported during healthy pregnancy to support the accelerated growth of maternal and fetal tissues (Cochrane et al., 2022), and a high amount of B‐vitamins is transported to placenta and fetus. Temporal alteration of one‐carbon pathways (the folate cycle and the methionine cycle and the transsulfuration pathway) and alterations of methyl nutrient flux and amino acid demand (methionine) at different pregnancy stages have been reported (Cai et al., 2021; Cochrane et al., 2022). Epigenetic adaptations by alterations of DNA methylation and histone methylation during early embryonic development have also been described (Cai et al., 2021).
In infants and children, data are lacking on absorption, metabolism, distribution and elimination of folate, including the maturation of these processes and how they might differ from those in adults. Some experimental data suggested that plasma clearance of folate in newborns may be more rapid than that in adults, associated with a more rapid tissue uptake, while folate absorption by newborns may be slower but the net absorption comparable to that of adults (Shojania & Hornady, 1970a, 1970b). Higher serum folate concentrations have been observed in early infancy compared to adults, while values were found to be comparable in late infancy (Smith et al., 1985). Poor tubular reabsorption of filtered folate in kidneys in the first days of life has been reported (Landon & Hey, 1974), however longer‐term studies are lacking. Folate‐binding proteins in breast milk have been shown to stimulate folate absorption (EFSA NDA Panel, 2014, 2022a). Observational data indicate higher average serum folate concentrations among children (aged 1–11 years), compared to older other age groups (Kerr et al., 2009; Pfeiffer, Sternberg, Fazili, Lacher, et al., 2015).
3.2.5.2. Sex
Winkels et al. (2008) analysed data from two folic acid intervention trials for sex‐related differences in response to treatment. In a three‐year intervention trial with subjects supplemented with 800 μg/day folic acid, the erythrocyte folate increased 10% (corresponding to 143 nmol/L) less in men than in women. Men and women in the trial had initially the same folate status, however, men were taller and heavier with larger lean body mass and body surface (Winkels et al., 2008). In the second study, a 12‐week trial, subjects in the folic acid groups ingested between 50 and 800 μg/day folic acid. Pooled dose–response in men was lower than for women, and male subjects receiving 800 μg folic acid had a 5% lower increase of erythrocyte folate than women. Authors attributed the sex differences to differences in body size (lean body mass) (Winkels et al., 2008).
3.2.5.3. Genetics
Various genotypes for enzymes in folate‐mediated one‐carbon metabolism are associated with changes in cellular metabolism, genome methylation and health outcomes (Amenyah et al., 2020; EFSA NDA Panel, 2014; Stover, 2011).
Homozygosity for the T‐allele of the 677C → T polymorphism of the gene encoding the MTHFR enzyme has been associated with decreased serum folate status, increased homocysteine levels and, after folate intervention, with lower plasma response (Crider et al., 2011). Consequently, higher folate requirements (up to 20%) in these individuals have been suggested due to reduced enzyme activity (EFSA NDA Panel, 2014).
In a genome‐wide association study in 2232 healthy Irish subjects of 18–28 years, Shane et al. (2018) found that the MTHFR 677C → T polymorphism was the only significant modifier of red cell and serum folate. It was also a genome‐wide modifier of plasma total homocysteine, confirming previous studies. The MTHFR 1298 A → C had no independent effect on status biomarkers.
Although MTHFR 677C → T polymorphism has been linked to an inverse association with CRC (RR = 0.62; 95% CI 0.44, 0.90) (Lee et al., 2012), several recent large mendelian randomisation studies have revealed no association between MTHFR polymorphism and breast cancer or CRC risk, emphasising the need for more research (Papadimitriou et al., 2021; Tsilidis et al., 2021; Yuan et al., 2021).
A 19‐base pair deletion polymorphism in DHFR (del/del genotype) has also been found to be associated with increased plasma UFA concentrations and decreased plasma/red blood cell folate compared with the wild type (WT)/del and WT/WT genotypes in some studies (Bortolus et al, 2020; Kalmbach et al., 2008), and a potential functional effect from this polymorphism on folate status/function has been proposed (Kalmbach et al., 2008). In contrast, other studies failed to detect any association between the del/del genotype and folate biomarkers (Gellekink et al., 2007; Ozaki et al., 2015; Stanisławska‐Sachadyn et al., 2008).
The Panel considers that, although there is emerging evidence that genetics may affect folate metabolism and disease risk, further research is required to characterise the impact of the different polymorphisms of enzymes and proteins involved in folate metabolism on health.
3.2.5.4. Cobalamin metabolism
In cobalamin deficiency, the activity of MS is reduced, which results in metabolic trapping of 5‐MTHF. Cellular 5‐MTHF polyglutamate cannot be metabolised by any other way because the MTHFR reaction is essentially irreversible under physiological conditions. Moreover, SAM is an important allosteric inhibitor of MTHFR and when MS activity is reduced, the concentration of SAM decreases and MTHFR becomes fully active, channelling other folate polyglutamate derivatives away from nucleotide synthesis and through MTHFR into the 5‐MTHF form. Incoming 5‐MTHF from plasma is not retained because it is a poor substrate for folylpolyglutamate synthetase. Consequently, a state of functional folate deficiency may develop in the cell (Savage & Lindenbaum, 1995; Smulders et al., 2006). Metabolically, this results in increased 5‐MTHF and homocysteine concentrations in plasma, simultaneously depleted folate concentrations in erythrocytes and other rapidly proliferating cells and – due to low SAM levels – a reduced availability of methyl groups for transmethylation reactions, i.e. the methylation of DNA (EFSA NDA Panel, 2015).
Clinically, cobalamin deficiency may be manifested by haematological and/or neurological and psychiatric components (EFSA NDA Panel, 2015). The haematological abnormality presents as a megaloblastic anaemia identical to that seen in folate deficiency. It is understood to be a consequence of the disruption of de‐novo DNA synthesis within developing erythrocytes and other haematopoietic cells. The neurological abnormalities of cobalamin deficiency are, in most severe form, manifested by a classical myeloneuropathy resulting from demyelination of peripheral and central neurons. Other features include mental symptoms, such as irritability, memory disturbances, depression and, in severe deficiency or advanced stages, a dementia‐like illness, frank psychosis with hallucinations and paranoia may occur. Neurological manifestations of cobalamin deficiency appear to be independent of haematological manifestations in that they can occur before, after or in complete absence of haematological manifestations. Moreover, classical neurological symptoms of cobalamin deficiency are almost never seen in folate deficiency. The underlying mechanism of the neurological manifestations of cobalamin deficiency is unknown, but evidence from patients with congenital defects of MTHFR and MS suggest that disruption of MS is the major cause, rather than disruption of the only other mammalian cobalamin‐dependent enzyme, methylmalonylCoA mutase (Green et al., 2017).
As folic acid is converted to THF via DHFR, folic acid supplements can initiate DNA synthesis in a cobalamin‐deficient person. However, folic acid cannot correct the disturbance of the methylation cycle created by loss of MS activity.
3.2.5.5. Folate antagonists
Several medicines (especially folate antagonists such as methotrexate) interfere with folate metabolism. Folic acid (folate) supplementation in patients under medical treatment with these drugs requires specific medical advice. These patients are outside the target population for this assessment.
3.2.6. Biomarkers of intake
Serum/plasma folate
Serum/plasma total folate concentration is a sensitive marker of recent dietary intake. However, if used for the assessment of folate status, multiple measurements of serum/plasma folate are needed over a period of several weeks. If a single measurement is available, it needs to be combined with other biomarkers of folate status (EFSA NDA Panel, 2014, 2022a).
A dose–response analysis between total intake of folate and serum/plasma folate concentration was performed as part of the preparatory work for this assessment (Åkesson et al., 2023). The purpose of this analysis was to support the interpretation and integration of findings from observational studies which used plasma/serum folate concentrations as biomarker of folate intake into the UL assessment. The relationship between total intake of folate (i.e. the sum of folate intake from natural sources, fortified foods and/or food supplements, expressed in μg DFE) and plasma/serum folate concentrations (in nmol/L) was modelled using data from controlled trials. Both linear (meta‐regression using a weighted mixed effects model) and non‐linear (restricted cubic splines) dose–response relationships were investigated. No departures from linearity could be identified over the range of total folate intakes investigated; the linear meta‐regression model was retained and specified as follows:
Red blood cell folate
RBC folate concentration is the most reliable biomarker of folate status and reflects long‐term dietary intake. As folate is incorporated into RBCs only during their maturation in the bone marrow and folate concentration remains stable throughout the 120‐day lifespan of the cells, this biomarker responds only slowly to changes in folate intake (EFSA NDA Panel, 2014, 2022b).
Unmetabolised folic acid (UFA)
Serum/plasma UFA concentration has been proposed as a biomarker of high folic acid intake. In a folic acid supplementation trial involving 50 pregnant women, higher serum concentrations of UFA were found in the group taking ‘high’ folic acid supplementation (5000 μg/day; median: 4.6 nmol/L, interquartile range (IQR): 2.5–33.8) compared to the group receiving a lower level of folic acid supplementation (1000 μg/day [1.9 nmol/L, IQR: 0.9–4.1]) (Murphy et al., 2021). However, in a cohort of pregnant women in Canada, no difference was found in mean plasma UFA concentration between users of folic acid supplements (2.44 nmol/L) and nonusers (2.37 nmol/L) when measured at 12–16 weeks of gestation (Plumptre et al., 2015). In populations exposed to mandatory folic acid fortification, weak to moderate correlations have been observed between estimated folic acid intake and serum UFA concentration (r 2 ꞊ 0.08 in the log–log plot in the UFA detected group (Bailey et al., 2010); r = 0.303, p < 0.001 (Palchetti et al., 2017).
Differences in the ADME of folic acid may contribute to UFA concentration variability across individuals. As mentioned above (Section 3.2.1), substantial interindividual variability in DHFR activity has been reported, which may be influenced by specific polymorphisms (Kalmbach et al., 2008) (Section 3.2.5.3). A recent analysis of NHANES data in the US indicated higher UFA concentrations with decreasing kidney function and lower UFA concentrations with increasing alcohol intake (Fazili et al., 2020). Differences in UFA concentrations were also observed across various ethnic groups, which appeared to be independent of supplement use.
At the present time, serum UFA concentration has not been validated as a biomarker of folic acid intake. Detection of UFA in fasted blood can only be used as a qualitative marker of exposure to folic acid fortification and supplementation.
3.3. Intake assessment
This section provides harmonised intake estimates of folate naturally present in foods (i.e. from the background diet) across EU countries calculated using the EFSA Comprehensive food consumption and the EFSA food composition databases, following extensive data cleaning to exclude fortified foods (Section 2.3.2). Data available to EFSA in these databases were insufficient to provide harmonised intake estimates of folate from fortified food and/or food supplements. Published data on folate from fortified food and/or food supplements from national food consumption surveys is presented instead.
3.3.1. Sources of dietary folate
Naturally occurring folates are found in a wide variety of foods; however, there are few foods which can be considered particularly rich folate sources (Annex C). Although most fruits and vegetables contain small amounts of folate, the richest sources are dark green vegetables (e.g. spinach, broccoli, lettuces), beans and legumes, and nuts. Meat generally contains low amounts of folate, with the exception of offal such as liver and kidney, which are particularly high in folate. Baker's yeast is also rich in folate. Food processing and cooking result in considerable losses of folate.
In its assessment of the safety and efficacy of folic acid as a feed additive for all animal species, the FEEDAP Panel concluded that feed supplementation at the level currently authorised in the EU can increase the folate content in eggs and meat, but not in liver or milk (EFSA FEEDAP Panel, 2012). As folic acid supplementation of animal feed is widespread and routine, intake estimates (Section 3.3.2) already contain the contribution from edible tissues and the products of animals fed folic acid‐supplemented diets.
Fortified foods
In the EU, authorised forms of folate for addition to foods 20 and foods for specific groups 21 are folic acid and CaLMF (Section 3.1). EU regulations set minimum and maximum content of folate in infants and follow‐on formulae, and maximum content of folate in processed cereal‐based foods and baby foods for infants and children. 22
In the Mintel GNPD a total of 4530 packaged food products available in 24 EU Member States and Norway were identified as containing added folate (mostly folic acid) in the ingredients list. Most of the products belong to the Mintel categories ‘breakfast cereals’ (25%), ‘baby food’ (22%), ‘nutritional drinks and other beverages’ (18%) and ‘snacks’ (10%).
Data on ‘folic acid’ 23 content per serving (as recommended by the manufacturer) were available for 33% of the products (n = 1499). Among those, this information was available for 61% of ‘breakfast cereals’ (n = 682, range 7.5–157 μg ‘folic acid’ per serving, median = 51 μg folate); 36% of ‘nutritional drinks and other beverages’ (n = 301, range 29–800 μg ‘folic acid’ per serving, median = 80 μg folate); and 30% of ‘snacks’ (n = 136, range 9–400 μg ‘folic acid’ per serving, median = 50 μg folate).
Food supplements
In the EU, authorised forms of folate for use in food supplements are folic acid, 5‐MTHF‐glucosamine and CaLMF 24 (Section 3.1). A search in Mintel GNDP ‘vitamins and dietary supplements’ category yielded a total of 1554 products available in 24 EU Member States and Norway. The median dose per serving 25 stated on labels was 200 μg ‘folic acid’, i.e. the nutrient reference value (NRV) for ‘folic acid’, with about 80% of food supplements reporting between 100 and 400 μg ‘folic acid’ per serving (50%–200% of the NRV) (Figure 5). About 2% of food supplements reported doses per serving of 800 μg (400% of the NRV). Three products contained higher doses, i.e. 880, 1000 and 1500 μg/serving, respectively.
FIGURE 5.
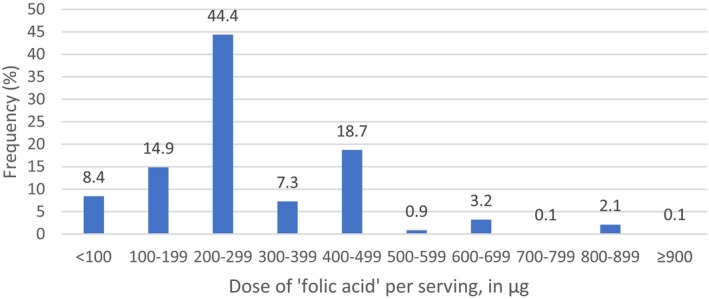
Distribution of doses per serving displayed on folate‐containing food supplement labels in EU Member States and Norway.Source: Mintel GNPD. Search for folate‐containing supplements available in the EU market in the last 5 years (from November 2017 to November 2022). A total of 1554 products available in 24 EU Member States and Norway were identified, of which 1528 contained complete data on μg/serving.
3.3.2. EFSA's intake assessment on background intake
Background folate intakes from natural food sources in European populations were calculated based on the data from the latest version of the EFSA Comprehensive Database and the EFSA FCDB.
3.3.2.1. Estimated intakes across countries and age groups
The intake estimates are presented below by age group, sex and country (Figures 6, 7, 8). A summary overview, providing the ranges of means and 95th percentiles (P95) across EU surveys is given in Table 4.
FIGURE 6.
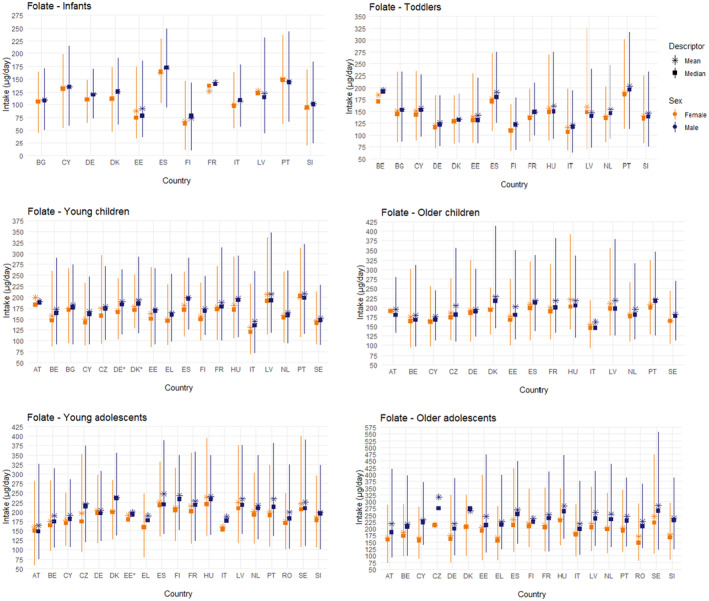
Mean, median, 5th and 95th percentiles of background folate intakes in infants (≥4 to <12 months), toddlers (≥1 year to <3 years old), young children (≥3 years to <7 years old), older children (≥7 years to <10 years old), intakes in young adolescents (≥10 to <14 years old) and older adolescents (≥14 to <18 years old), by sex and country. Estimates for females are shown in orange and for males in blue. Squares correspond to medians and stars to means. Lines represent the range between the 5th and 95th percentiles. Estimated intakes from 5th and 95th percentiles are not presented when sample size is below 60 participants. AT: Austria; BE: Belgium; BG: Bulgaria; CY: Cyprus; CZ: Czech Republic; DE: Germany; DK: Denmark; EE: Estonia; EL: Greece; ES: Spain; FI: Finland; FR: France; HU: Hungary; IT: Italy; LV: Latvia; NL: The Netherlands; PT: Portugal; SE: Sweden; SI: Slovenia. *Country for which more than one survey was available; estimates presented in the plot are those of the most recent survey; when surveys covered the same period those with the highest number of participants are displayed.
FIGURE 7.
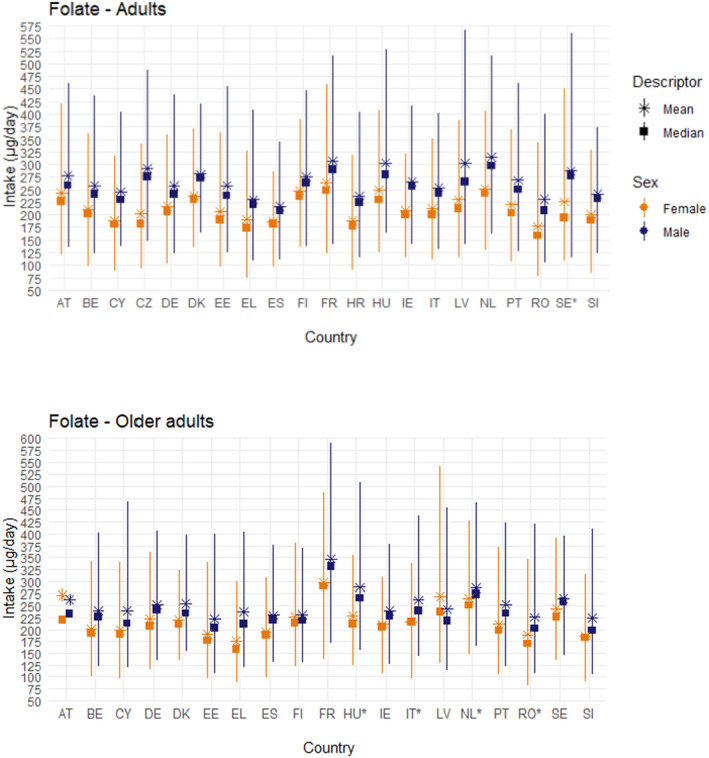
Mean, median, 5th and 95th percentiles of background folate intakes in adults (≥18 years to <65 years old) and older adults (≥65 years), by sex and country. Estimates for females are shown in orange and for males in blue. Squares correspond to medians and stars to means. Lines represent the range between the 5th and 95th percentiles. Estimated intakes from 5th and 95th percentiles are not presented when sample size is below 60 participants. AT: Austria; BE: Belgium; CY: Cyprus; CZ: Czech Republic; DE: Germany; DK: Denmark; EE: Estonia; EL: Greece; ES: Spain; FI: Finland; FR: France; HR: Croatia; HU: Hungary; IE: Ireland; IT: Italy; LV: Latvia; NL: The Netherlands; PT: Portugal; RO: Romania; SE: Sweden; SI: Slovenia. *Country for which more than one survey was available; estimates presented in the plot are those of the most recent survey; when surveys covered the same period those with the highest number of participants are displayed.
FIGURE 8.
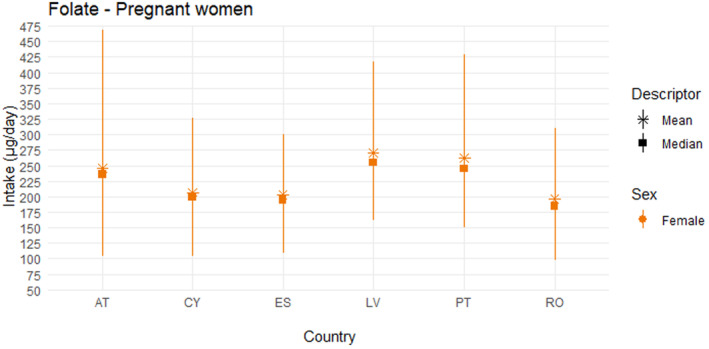
Mean, median, 5th and 95th percentiles of folate intakes in pregnant women, by country. Squares correspond to medians and stars to means. Lines represent the range between the 5th and 95th percentiles. Estimated intakes from 5th and 95th percentiles are not presented when sample size is below 60 participants. AT, Austria; CY, Cyprus; ES, Spain; LV, Latvia; PT, Portugal; RO, Romania.
TABLE 4.
Background folate intake from food sources (supplements and fortified foods excluded) across European dietary surveys, by population group (μg/day).
| Population group, age range | N of surveys | Males | Females | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | P95 a | Mean | P95 a | ||||||
| Min. b | Max. b | Min. b | Max. b | Min. b | Max. b | Min. b | Max. b | ||
| Infants, ≥4 to <12 mo | 12 | 73 | 172 | 143 | 248 | 67 | 162 | 146 | 237 |
| Toddlers, ≥1 to <3 y | 15 | 121 | 204 | 179 | 316 | 111 | 190 | 165 | 325 |
| Young children, ≥3 to <7 y | 20 | 131 | 208 | 186 | 347 | 130 | 206 | 198 | 336 |
| Older children, ≥7 to <10 y | 15 | 162 | 228 | 245 | 413 | 154 | 221 | 218 | 392 |
| Young adolescents, ≥10 to <14 y | 20 | 164 | 248 | 285 | 390 | 161 | 239 | 247 | 401 |
| Older adolescents, ≥14 to <18 y | 19 | 217 | 317 | 366 | 556 | 165 | 245 | 280 | 474 |
| Adults, ≥18 to <65 y | 22 | 217 | 314 | 345 | 567 | 177 | 264 | 285 | 459 |
| Older adults, ≥65 y | 23 | 222 | 347 | 369 | 590 | 176 | 298 | 300 | 541 |
| Pregnant women | 6 | – | – | – | – | 196 | 271 | 301 | 468 |
| Lactating women | 2 | – | – | – | – | 228 | 242 | 406 | 423 |
| Vegetarians c | 1 | 340 | 340 | 585 | 585 | 284 | 284 | 546 | 546 |
Abbreviations: mo: months, n: number, P, percentile; y: years.
The 95th percentile estimates obtained from dietary surveys and population groups with fewer than 60 subjects may not be statistically robust (EFSA, 2011) and are not considered in this table.
Minimum and maximum mean and 95th percentile estimates across European surveys, for each population group.
Age range (12–70 years).
3.3.2.2. Main food contributors
The main food groups contributing to background folate intake were grains and grain‐based products (mainly bread and similar products), milk and dairy products (mainly milk, whey and cream) and vegetables and vegetable products (leafy and fruiting vegetables) in all age groups, except infants, with minor differences between sexes. In infants, main contributors were infant and follow‐on formulae 26 and processed cereal‐based foods (Annex C).
3.3.2.3. Sources of uncertainty
Sources of uncertainty and their potential impact on the intake estimates, where possible, are identified and discussed in detail in Annex B.
Specific to the folate intake assessment, uncertainties arise from the reporting of ‘folate’ composition data. This is due to the lack of harmonisation across national food composition databases regarding the differentiation between naturally occurring folates and synthetic folic acid and the use of terms (‘folic acid’, ‘total folate’, ‘dietary folate’) and units (μg or μg DFE), as well as the diversity of analytical methods for quantifying folate and folic acid in food. Assumptions had to be made for building the EFSA pooled food composition database from individual national food composition databases (Section 2.3.1). The use of a pooled food composition database is, however, expected to have reduced the impact of these uncertainties.
Also, as the scope of intake assessment was to consider natural sources of folate only, a data cleaning strategy was applied to exclude fortified foods from the composition database. Since fortification was not always clearly reported, assumptions had to be made to exclude suspected fortified foods (e.g. by identifying high outlier folate content values). This could result in both an overestimation or underestimation of the background intake of folate; however, the impact of this uncertainty is expected to be small as the folate content values in the EFSA pooled food composition database used in this assessment were similar to those reported in the individual national food composition databases. EFSA's intake estimates are in line with national estimates which reported on the intake from the background diet only but are generally lower than those national estimates which included both natural sources of folate and fortified foods (Annex C).
3.3.3. Data on fortified foods and food supplements
Data on folate intake from fortified foods and food supplements were collected from nationally representative consumption surveys (Section 2.3.1). Survey characteristics, mean and P95 intake estimates are presented in Annex D. Key information is summarised in the following paragraphs.
3.3.3.1. Intake from fortified foods
There is no mandatory folate fortification policy among EU countries. Folate may be added to foods voluntarily.
Estimates of folate intake from food, including fortified foods, are available for 27 dietary surveys conducted in 18 European countries (Belgium, Bulgaria, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Latvia, Lithuania, the Netherlands, Norway, Slovenia, Spain and Sweden). The survey characteristics and intake estimates are provided in Annex D. The highest P95 values in males from foods including fortified foods were reported in France for infants (368 μg/day) and toddlers (355 μg/day), in Denmark for all children (452 μg/day) and in Germany for all adolescents (735 μg/day). For all adults, highest P95 values were reported in Germany (1382 μg/day). Estimated intakes for females were generally lower than for males in all studies and age groups. As noted in several reports, data on folic acid content of fortified foods are often missing from food composition tables and the contribution of fortified foods is likely underestimated (Mitsopoulou et al., 2020, 2021; Teppers & Ost, 2016; Valsta et al., 2018).
Only one publication reported estimates of folic acid intake from fortified foods only (Hopkins et al., 2015). Based on data from the National Adult Nutrition Survey (NANS) survey in Ireland including 1126 adult men and women, median (IQR) intakes of folic acid from fortified foods ranged from 58 (12, 125) to 64 (11, 180) μg/day in men and from 35 (6, 87) to 47 (0, 138) μg/day in women, with the highest values observed in the age group ≥65 years. In the whole survey population 79% of the individuals consumed folic acid–fortified foods (79%), with the highest percentage in the age group ≥65 years. The mean percent contribution of folic acid from fortified foods to total folate intake was 20%. The main contributors were breakfast cereals and fat spreads.
3.3.3.2. Intake from food supplements
Most European countries have policies in place advising periconceptional supplementation with 400 μg of folic acid taken daily prior to conception and for the first 3 months of pregnancy to prevent neural tube defects.
A total of 18 dietary surveys conducted in 11 countries (Belgium, Denmark, Estonia, Finland, Germany, Ireland, the Netherlands, Norway, Poland, Portugal and Sweden) reported information on folate supplementation. Some national reports refer to ‘folate’ intake from food supplements, while other refer to ‘folic acid’. The term ‘folate’ is used below for consistency. However, given that folic acid is the most used form, it can be assumed that most of the available estimates relates to folic acid intake, while the contribution from other forms (i.e. 5‐MTHF‐glucosamine and CaLMF) is low. The survey characteristics and intake estimates are presented in Annex D.
Eleven surveys from seven countries (Denmark, Finland, Germany, Ireland, the Netherlands, Norway and Poland) reported data on folate intake from food supplements among users.
Among children and adolescents, the mean percent contribution of food supplements to total folate intake was estimated in two countries and ranged from 18% to 27% in Denmark, and 26% to 38% in Ireland, across age groups. Absolute intakes of folate from food supplements in high consumers (P95) were estimated to range between 200 μg/day in children aged 1–4 years and 03215697 μg/day in children aged 13–18 years in Ireland and between 140/198 μg/day in children aged 1–3 years and 344/198 μg/day in male/female children aged 14–18 years in the Netherlands (Table 5).
TABLE 5.
Percent folate supplement users in EU surveys and folate intake from food supplements among users (toddlers, children and adolescents).
| Country Survey name (N subjects) Reference | Dietary method (N of days) | Sex | Age range | % folate supplement users in total survey sample/among supplements users | Folate a from supplements, P95 (μg/day) | % contribution of supplements to total folate intake, mean |
|---|---|---|---|---|---|---|
|
Denmark DANSDA 2011–2013 (n = 3936) (Hindborg, 2015, Unpublished) |
Face‐to‐face interview |
m f |
4–10 y 11–17 y 11–17 y |
60 b /NR 46 b /NR 42 b /NR |
NR |
18 26 27 |
|
Germany EsKiMo II 2015–2017 (n = 2644) (Perlitz et al., 2019) |
Short questionnaire + weighing logs | m + f |
6–11 y 12–17 y |
NR/NR 4.1/25.2 |
NR | NR |
|
Ireland NPNS 2011–2012 (n = 500) NCFS II 2017–2018 (n = 600) NTFS II 2019–2020 (n = 428) (Kehoe & Walton, 2022) |
Weighted food diary (4 days) | m + f |
1–4 y 5–12 y 13–18 y |
9.6/44.9 8.5/39.1 7.2/50.9 |
200 200 397 |
29.3 25.7 38.5 |
|
Netherlands DNFCS 2012–2016 (n = 4313) (Van Rossum et al., 2022) |
Questionnaire (online/paper) | m + f |
1–3 y 3–10 y 10–14 y 14–18 y |
m 15/17 f 16/19 m 22/40 f 23/38 m 14/35 f 20/41 m 10/29 f 9/23 |
m 140/f 198 m 188/f 199 m 195/f 272 m 344/f 198 |
NR |
|
Norway Småbarnskost 2015 (n = 1674) Ungkost 3 2016 (4 y, n = 399) Ungkost 3 2015 (9 y, n = 636) Ungkost 3 2015 (13 y, n = 687) (VKM et al., 2015) |
FFQ + food diary +24‐h dietary interviews | m + f |
2 y 4 y 9 y 13 y |
NR/NR NR/NR NR/NR NR/NR |
Mean 77 55 68 102 |
NA |
|
Slovenia SI.Menu 2017–2018 (n = 1248) (Pravst et al., 2021) |
FPQ | m + f | 10–17 y |
Multivitamins/folic acid only 27.5/0.2 |
NR | NR |
Abbreviations: d, day; DANSDA, The Danish National Survey of Diet and Physical Activity; DNFCS, Dutch National Food Consumption Survey; EsKiMo, Eating study as a KiGGS Module; f, females; FFQ, food frequency questionnaire; FPQ, food propensity questionnaire; m, males; N, number; NA, cannot be calculated; NCFS, National Children's Food Survey; NPNS, National Pre‐School Nutrition Survey; NR, not reported in the publication; NTFS, National Teen's Food Consumption Survey; SD, standard deviation; VKM, Vitenskapskomiteen format og miljø (Norwegian Scientific Committee for Food and Environment); y, year.
Folic acid is the most commonly used form in foods supplements.
% users of multivitamin/mineral supplements. By default, multivitamin/mineral supplements were considered to contain manganese based on Danish households purchases data.
Among adults, the mean percent contribution of food supplements to total folate intake was available for four countries and ranged between 25% (older adults in Ireland) and 67% (adult women in Germany). P95 absolute intakes of folate from food supplements were in the range 400–600 μg/day in Ireland, the Netherlands and Norway, and up to 893 μg/day in women and 1020 μg/day in men in Germany (Table 6).
TABLE 6.
Percent folate supplement users in EU surveys and folate intake from food supplements among users (adults and older adults).
| Country Survey name (N subjects) Reference | Dietary method (N of days) | Sex | Age range | % Folate supplement users in total survey sample/among supplements users | Folate a intake from supplements, P95 (μg/day) | % contribution of supplements to total folate intake, mean |
|---|---|---|---|---|---|---|
|
Denmark DANSDA 2011–2013 (n = 3936) (Hindborg, 2015, Unpublished) |
Face‐to‐face interview |
m f m f |
18–50 y 18–50 y 51–75 y 51–75 y |
42/NR 51/NR 43/NR 55/NR |
NR |
27 29 29 34 |
|
Finland FINDIET 2017 (n = 1655) (Valsta et al., 2018) |
FPQ |
m f |
18–74 y |
23/NR 32/NR |
Mean 237 235 |
47.8 49.9 |
|
Germany NVS II 2005–2007 (n = 13,753) (Heuer et al., 2012; Martiniak et al., 2015) |
24‐h recall (2 days) | m‐f |
14–18 y 19–24 y 25–34 y 35–50 y 51–64 y 65–80 y |
2.7–3.3/NR 5–8.2/NR 6.4–10.4/NR 7.6–8.6/NR 7.5–11.5/NR 9.1–11.9/NR |
m 893 (b) f 1020 (b) |
m 50.6 (b) f 67.3 (b) |
|
Ireland NANS 2008–2010 (n = 1500) (Kehoe & Walton, 2022) |
Weighted food diary (4 days) | m + f |
18–64 y 65–91 y |
14.4/48.3 11.9/31.8 |
400 400 |
39.5 25.8 |
|
Netherlands DNFCS 2012–2016 (n = 4313) (Van Rossum et al., 2022) |
Questionnaire (online/paper) | m + f |
18–65 y 65–80 y |
m 15/41 f 22/39 m 14/40 f 22/38 |
m 579/f 564 m 500/f 592 |
NR |
|
Norway Norkost 3 2015 (n = 1787) (Totland et al., 2012; VKM et al., 2015) |
FFQ + food diary +24‐h dietary interviews |
m f |
18–70 y |
NR/18 NR/26 |
500 400 |
NA |
|
Poland National Dietary Survey 2019–2020 (n = 1831) (Stos et al., 2021) |
FPQ |
m f |
18–65+ y |
NR/NR NR/NR |
Mean ± SD (range) 278 ± 123 (150–600) 304.9 ± 227.4 (60–800) |
NA |
|
Slovenia SI.Menu 2017–2018 (n = 1248) (Pravst et al., 2021) |
FPQ | m + f |
18–64 y 65–74 y |
Multivitamins/folic acid only 36.5/1.9 22.6/0.2 |
NR | NR |
Abbreviations: d, day; DANSDA, The Danish National Survey of Diet and Physical Activity; DNFCS, Dutch National Food Consumption Survey; f, females; FINDIET, The Finnish National Dietary Survey in Adults and Elderly; FFQ, food frequency questionnaire; FPQ, food propensity questionnaire; m, males; N, number; NA, cannot be calculated; NANS, National Adult Nutrition Survey; NR, not reported in the publication; NVS II, Nationale Verzehrsstudie II (National Consumption Study II); SD, standard deviation; VKM, Vitenskapskomiteen format og miljø (Norwegian Scientific Committee for Food and Environment); y, year.
Folic acid is the most commonly used form in foods supplements.
Age range: 14–80 years.
Absolute intakes of folate from all sources among supplement users were reported in five surveys in four countries (Denmark, Finland, Germany and Sweden) and are provided in Annex D.
3.3.4. Overall conclusions on intake data
The Panel notes that the P95 estimated background intake of folate from natural food sources (i.e. without fortified foods and food supplements) in males is up to 248 μg/day in infants (4 to <12 months), up to 325 μg/day in toddlers (1 to <3 years), up to 347 μg/day in young children (3 to <7 years), up to 413 μg/day in older children (7 to <10 years), up to 401 μg/day in young adolescents (10 to <14 years), up to 556 μg/day in older adolescents (14 to <18 years), up to 590 μg/day in adults (≥18 years), up to 468 μg/day in pregnant women and up to 423 μg/day in lactating women across surveys included in EFSA's intake assessment (Table 4) (Annex C). Intakes are slightly lower in females, mainly due to smaller quantities of food consumed per day.
There is no mandatory folate fortification policy in EU countries. On the EU market, folate may be added to foods voluntarily (mostly found in breakfast cereals, nutritional drinks and snacks), with large variability in folate content per serving (e.g. a search in the Mintel GNDP database indicates folate contents between 7.5 and 200 μg per serving among breakfast cereals).
Folate is also used in food supplements. A search in the Mintel GNDP database indicates substantial variability in the dose per serving across food supplements, with most values between 100 and 400 μg ‘folic acid’ (50%–200% of the NRV) and about 2% of products with values >800 μg (maximum 1500 μg) per serving. Most European countries have policies in place advising periconceptional supplementation with 400 μg of folic acid taken daily prior to conception and for the first 3 months of pregnancy to prevent neural tube defects.
The Panel notes that estimates of the contribution of fortified foods and food supplements to folate intake in EU populations are scarce. The NANS survey in Ireland is the only survey for which estimates of folic acid intake from fortified foods and food supplements are available. Significant contribution of food supplements and fortified foods to total folate intake were found in this country, i.e. mean contribution of 30%–40% for fortified foods and 20% for food supplements. Among users of food supplements, the mean contribution of food supplements to total folate intake ranged between about 25% and 70% in adults (data from three countries) and between about 20% and 40% in children and adolescents (data from two countries). The Panel notes that in regular consumers of folate‐containing fortified foods and food supplements, the contribution of these foods to total folate intake can be substantial.
3.4. Hazard identification
3.4.1. Risk of cobalamin‐dependent neuropathy
Concerns regarding a potential contribution of high folic acid intake to the progression and, possibly, the exacerbation of cobalamin‐dependent neurological abnormalities arose from case reports and case series of patients with PA, who were treated with folic acid as a sole medication.
A frequent clinical expression of cobalamin deficiency is megaloblastic anaemia, which affects all developing cells of the haematopoietic system, including red blood cells (EFSA NDA Panel, 2014) (Section 3.5.2). Neurological involvement associated with severe cobalamin deficiency in adults includes combined spinal sclerosis, peripheral neuropathy and dementia. Paraesthesia in the extremities, ataxia of gait or both symptoms, are the initial complaints in 90% of patients with cobalamin‐dependent neuropathy. Impaired vibratory sensation, proprioception and cutaneous touch and pain sensation are the most frequent neurological signs on examination. In advanced cobalamin‐dependent neuropathy, corticospinal tract involvement may develop, eventually progressing to spastic paraparesis. Global dementia or memory disturbances are the most common cerebral disorders. The speed of progression varies markedly between patients and is not necessarily constant. Notably, haematological and neurological manifestations are often dissociated (Savage & Lindenbaum, 1995). Whereas megaloblastic anaemia is a relatively specific sign of cobalamin (and/or folate) deficiency, early neurological signs/symptoms of cobalamin deficiency may be unspecific.
In its previous evaluation of the UL for folate, the SCF reviewed the evidence from case reports/case series and animal experimental data and concluded that:
The evidence for an exacerbation of the neurological sequelae in PA patients by folic acid supplementation was equivocal (causal relationship not established).
There was evidence that intake of folic acid can correct megaloblastic anaemia (at least transiently) in PA patients (causal relationship established). The risk of ‘masking’ of cobalamin deficiency through the resolution of megaloblastic anaemia, allowing neurological manifestations to concurrently progress, was considered the most serious adverse effect of folic acid supplementation in humans and was selected as a critical endpoint to set an UL for folic acid. As dosages up to 1000 μg of folic acid were considered unlikely to cause masking of the haematological signs in PA patients, the UL was set at 1000 μg of folic acid per day in adults.
The direct and indirect relationships between the supplemental intake of folic acid and the risk of cobalamin‐dependent neuropathy are illustrated in Figure 9.
FIGURE 9.
Relationships between the supplemental intake of folic acid and the risk of cobalamin‐dependent neuropathy.
This section reviews whether new evidence has arisen since the SCF evaluation regarding:
a positive and causal relationship between the supplemental intake of folic acid and an exacerbation of the neurological manifestations of cobalamin deficiency (Section 3.4.1.1);
the doses at which supplemental intake of folic acid may resolve the haematological signs of cobalamin deficiency (Section 3.4.1.2).
3.4.1.1. Exacerbation of the neurological manifestations of cobalamin deficiency
LoE1. Standalone main: incidence/recurrence of neuropathy in cobalamin deficient individuals treated with folic acid
Preliminary UA
Relevant case reports/series of cobalamin deficient individuals treated with folic acid were identified through previous reviews (Berry, 2019; IOM, 1998; Savage & Lindenbaum, 1995; SCF, 2000; van Gool et al., 2020) (Section 2.2.1.1).
The available publications may be grouped as follows: (i) reports of prospective examinations of patients treated with folic acid in the clinical setting; (ii) retrospective reports of patients admitted in the hospital after a period of folic acid supplementation outside of the clinical setting. The description below is limited to cases of oral treatments.
Prospective case series
Sixteen publications reported on prospective case series (Berk et al., 1948; Bethell & Sturgis, 1948; Chodos & Ross, 1951; Davidson & Girdwood, 1947; Hall & Watkins, 1947; Heinle et al., 1947; Israëls & Wilkinson, 1949; Meyer, 1947; Ross et al., 1948; Schwartz et al., 1950; Spies et al., 1948; Spies & Stone, 1947; Vilter et al., 1947; Wagley, 1947; Wilkinson, 1948; Will et al., 1959). The vast majority of cases were PA patients (Bethell & Sturgis, 1948; Chodos & Ross, 1951; Hall & Watkins, 1947; Heinle et al., 1947; Israëls & Wilkinson, 1949; Meyer, 1947; Ross et al., 1948; Spies et al., 1948; Wilkinson, 1948; Will et al., 1959), while a few cases were related to patients with gastric resection (Chodos & Ross, 1951; Heinle et al., 1947; Meyer, 1947; Ross et al., 1948; Wagley, 1947) or sprue (Chodos & Ross, 1951; Davidson & Girdwood, 1947; Spies et al., 1948; Wagley, 1947). Cases were patients treated with folic acid as an alternative to liver extract, which was the standard treatment for PA at that time (Berk et al., 1948; Bethell & Sturgis, 1948; Chodos & Ross, 1951; Davidson & Girdwood, 1947; Heinle et al., 1947; Ross et al., 1948; Will et al., 1959) or patients treated with folic acid as first therapy or after an interruption of the therapy with a liver extract (Berk et al., 1948; Bethell & Sturgis, 1948; Hall & Watkins, 1947; Heinle et al., 1947; Israëls & Wilkinson, 1949; Meyer, 1947; Spies & Stone, 1947; Wagley, 1947; Wilkinson, 1948; Will et al., 1959).
The number of cases described varied between 14 and 48 across publications, adding up to around 300 cases in total. The doses of folic acid were usually between 5000 and 20,000 μg/day, although higher doses were administered in a few cases (i.e. 40,000, 50,000 and 600,000 μg/day). The treatment duration varied from some weeks to several years. During folic acid treatment, the patients were visiting the clinics for regular examinations, where their haematological and neurological signs and symptoms were monitored.
In the period following the substitution of liver extract by folic acid, the haematological status of the majority of patients was found to be maintained (Berk et al., 1948; Bethell & Sturgis, 1948; Chodos & Ross, 1951; Heinle et al., 1947; Ross et al., 1948; Wilkinson, 1948; Will et al., 1959), although deterioration (Bethell & Sturgis, 1948; Heinle et al., 1947) or, in contrast, further improvement were also described in some cases (Berk et al., 1948; Bethell & Sturgis, 1948; Heinle et al., 1947). An improvement of the haematological signs of PA was also observed in most patients who had not been previously treated with liver extracts (Bethell & Sturgis, 1948; Hall & Watkins, 1947; Heinle et al., 1947; Israëls & Wilkinson, 1949; Meyer, 1947; Spies et al., 1948;Wagley, 1947 ; Will et al., 1959). The effectiveness and speed of the haematological responses were found to vary substantially among patients.
In the longer term, however, a relapse of the haematological symptoms was consistently observed (Chodos & Ross, 1951; Israëls & Wilkinson, 1949; Ross et al., 1948; Schwartz et al., 1950; Will et al., 1959). Among 70 PA patients treated with a daily dose of 5000 μg folic acid for 3.5 years, Schwartz et al. (1950) reported that a satisfactory health status was maintained in 12 patients, while 58 patients relapsed. Among those, haematological relapse was observed in 23 patients, neurological relapse in 23 patients, 9 patients experienced combined neurological and haematological relapses and sore tongue and/or weight loss were described in the three remaining cases. Neurological relapses were typically observed to occur sooner than haematological relapses (within 2 years vs. within 3 years, respectively). The authors also noted that the haematological relapses were remarkably delayed as compared to the time‐to‐relapse observed in untreated PA patients (typically within 1 year).
Several publications reported deterioration or onset of neurological manifestations during the period of folic acid treatment (Berk et al., 1948; Bethell & Sturgis, 1948; Chodos & Ross, 1951; Hall & Watkins, 1947; Heinle et al., 1947; Israëls & Wilkinson, 1949; Ross et al., 1948; Spies et al., 1948; Spies & Stone, 1947; Vilter et al., 1947; Wilkinson, 1948; Will et al., 1959). The neurological manifestations were characteristic of cobalamin‐dependent neuropathy (i.e. numbness/tingling in hands and feet, ataxic gait, loss of vibratory sense, diminished touch and pain sensation; difficulty in walking or even paralysis of the legs were also described in some cases). In several cases, neurological manifestations developed at a time where haematological signs were absent (Hall & Watkins, 1947; Heinle et al., 1947). The time to the onset of the neurological signs and symptoms varied across patients (ranging from a few months to years). The proportion of patients affected varied substantially across studies. Neurological signs and symptoms often resolved upon the reintroduction of liver extracts (or other cobalamin supply), but in several cases neurological manifestations had become irreversible.
Some clinicians noted a more rapid and or/frequent progression in PA patients receiving folic acid therapy as compared to untreated PA patients (Wagley, 1947; Will et al., 1959), which raised concerns about a potential exacerbation of neurological manifestations by folic acid.
Retrospective cases reports
Seven publications described a total of 20 isolated cases of patients who had been taking folic acid‐containing supplements, as a treatment for macrocytic anaemia (sometimes in substitution for previous liver therapy) or other conditions (Allen et al., 1990; Baldwin & Dalessio, 1961; Best, 1959; Conley & Krevans, 1951; Crosby, 1960; Ellison, 1960; Victor & Lear, 1956). In most cases admission to the hospital was triggered by the onset of neurological symptoms, with varying degree of severity. Upon questioning, patients reported having taken supplements containing folic acid, in most cases in combination with other nutrients. Doses of folic acid were estimated between 350 and 5000 μg/day (Allen et al., 1990; Baldwin & Dalessio, 1961; Conley & Krevans, 1951; Crosby, 1960; Ellison, 1960; Victor & Lear, 1956), with higher doses in a few cases (6300–10,000 μg/day) (Baldwin & Dalessio, 1961; Best, 1959; Conley & Krevans, 1951; Victor & Lear, 1956). Upon clinical examination at the time of hospital admission, PA was diagnosed in the majority of cases (Allen et al., 1990; Baldwin & Dalessio, 1961; Conley & Krevans, 1951; Crosby, 1960; Ellison, 1960; Victor & Lear, 1956). In a few cases cobalamin deficiency was due to ileal resection (Allen et al., 1990; Best, 1959) or jejunal diverticulosis (Allen et al., 1990). Haematological signs were not always detected (Baldwin & Dalessio, 1961; Crosby, 1960; Ellison, 1960; Victor & Lear, 1956). Neurological signs and symptoms were found to improve upon treatment with cobalamin.
The Panel notes that there is consistent evidence from human case reports/series that neurological complications may start or progress in cobalamin deficient individuals given supplemental folic acid as sole treatment (i.e. without cobalamin).
A comprehensive UA is performed regarding a positive and causal relationship between the intake of folic acid and the exacerbation of the neurological manifestations of cobalamin deficiency.
Comprehensive UA
Risk of bias
No RoB appraisal of the individual publications was performed. Instead, potential sources of bias regarding the exposure characterisation, outcome assessment and potential confounders applying to the whole body of evidence are discussed below.
As the dose and duration of folic acid treatment were prescribed and monitored in the clinical setting in most cases (prospective cases series), there is low concern regarding RoB for the exposure characterisation overall. Indirect evidence for patients' compliance to treatment arises from the resolution of haematological abnormalities during the intervention period.
As for the outcome assessment, the level of reporting regarding the method and criteria applied to evaluate neurological manifestations varies across publications. As treatment of PA was the primary objective of the folic acid supplementation in many studies and patients were regularly examined by clinicians for their condition, including neurological manifestations, there is low concern regarding RoB for the outcome assessment overall.
In relation to confounders, cobalamin body stores and subclinical neurological changes at the start of folic acid treatment are key potential confounders of the relationship between supplemental intake of folic acid and the risk of neuropathy in individuals with PA. It is expected that neurological effects of cobalamin deficiency will become more severe as they remain untreated. The nature of the evidence precludes controlling for these factors. Because of their uncontrolled design, case studies cannot reliably investigate any exacerbation of cobalamin‐related neurological manifestations due to folic acid treatment alone.
Unexplained inconsistency
There is consistent evidence that neurological complications may start or progress in individuals with PA (or other gastric conditions which affect the production or function of intrinsic factor) who received supplemental folic acid as sole treatment. On the other hand, there is substantial variability in the doses and durations of folic acid supplementation which have been associated with neurological manifestations and in the severity of the symptoms reported in these patients.
In addition to the variety of dose and duration of the folic acid treatments reported in the available case reports/series, sources of heterogeneity across studies include: the inclusion of patients with or without prior treatment with liver extracts or other sources of cobalamin (i.e. factors causing variability in cobalamin body stores at start of folic acid treatment); the inclusion of patients with or without pre‐existing neurological manifestations at the start of the folic acid intervention; the criteria applied for the diagnosis of neurological abnormalities. Also, due to the similarity of clinical haematological symptoms of folate and cobalamin deficiency and the lack of differential diagnostic methods at the time of these case reports/series, some of the cases reported above, classified as cobalamin deficient, may have been folate‐deficient patients, contributing to the heterogeneity of the individual responses to folic acid supplementation.
Indirectness
Evidence mostly arises from individuals with PA; a few cases were also reported in patients with other gastric conditions that affect the production or function of intrinsic factor. These are common causes of cobalamin deficiency and thus relevant population groups to investigate the risk assessment question.
Dose–response relationship
Available data from case reports/series do not provide consistent evidence for a dose–response relationship between dose and/or duration of folic acid treatment and the onset or progression of neurological manifestations. Most cases of neuropathy were reported at doses of 5000 μg folic acid/day or higher, which are most frequently used for the therapeutic treatment of PA. Onset or progression of neurological manifestations (with or without haematological abnormalities) were also reported with folic acid doses below 5000 μg/day. The Panel notes that evidence at these dose levels is scarce and limited to retrospective case reports with doses estimated based on patients reports. The period with folic acid treatment coincided with the period without cobalamin treatment (liver extracts), so that any effect of folic acid treatment cannot be assessed independently from the effect of the lack of cobalamin.
Consistency across lines of evidence (LoEs)
Animal experiments in monkeys (Agamanolis et al., 1976) and fruit bats (Van der Westhuyzen et al., 1982; van der Westhuyzen & Metz, 1983) fed a cobalamin deficient diet, reported that cobalamin‐deficient animals receiving supplemental folic acid developed signs of neuropathology earlier than controls.
Bats were fed a cobalamin deficient diet and exposed to the anaesthetic gas nitrous oxide, which oxidises methyl cobalamin thereby inhibiting the cobalamin‐dependent methionine synthase (Van der Westhuyzen et al., 1982). Diet was supplemented with folic acid (1540 μg/kg bw) in one group and 5‐formylTHF, a reduced folate form, was administered intramuscularly to another group (1150 μg/kg bw). The onset of neurological impairment was observed after an average (range) of 4.3 (4.1–5.4) weeks in the folic acid group (n = 6), 4.5 (2.7–5.4) weeks in the 5‐formylTHF group (n = 5) compared to 5.0 (2–6.9) weeks in the group without folic acid/5‐formylTHF treatment (n = 12); flight was reduced to hops after 4.8 (4.0–5.4) weeks, 4.8 (2.7–6.1) weeks and 6.2 (5.0–7.4) weeks, respectively. In a subsequent experiment with a similar design and the same folic acid dose, van der Westhuyzen and Metz (1983) observed ataxia after an average of 8.8 weeks in the folic acid‐treated group (n = 6), compared to 9.8 weeks in the control group (n = 6).
Agamanolis et al. (1976) fed nine rhesus monkeys a cobalamin deficient diet; three out of nine animals received supplemental folic acid (initially 5000 μg of folic acid intramuscularly weekly followed by 5000 μg folic acid in the drinking water 5 days a week). Degeneration of visual pathway was observed after 33 months in the three folic acid‐treated monkeys versus 37–53 months among those not receiving folic acid. Two of the three folic acid‐treated monkeys developed motor deficits after 37 months of treatment, while these deficits were observed in two of the six other monkeys after 48 and 52 months, respectively. Cell morphology and counts of peripheral blood and bone marrow were not affected by cobalamin deficiency, in any monkey.
Differences have, however, been observed between animals and humans regarding the effects of cobalamin deficiency. Although development of neurological symptoms was observed in experiments in which nitrous oxide was administered to monkeys, no haematological symptoms occurred in these animal models of cobalamin deficiency (Dinn et al., 1978, 1980; Scott et al., 1981) or pigs (Molloy, 2023, Personal communication). Nitrous oxide has been reported to cause haematological and neurological effects identical to those seen in cobalamin deficiency after inhalation in humans (Chanarin, 1980; Winstock & Ferris, 2020).
While the studies in monkeys and fruit bats are consistent with the hypothesis that folic acid might exacerbate neurological lesions, the low numbers of animals, the difference in effects over repeated studies, and the inherent differences between these animals and humans in relation to haematological aspects of cobalamin deficiency make these studies difficult to interpret.
Outcome of the comprehensive analysis of the uncertainties
Conclusions from case reports/cases series
The level of certainty in a positive and causal relationship between the intake of folic acid and the exacerbation of the neurological manifestations of cobalamin deficiency is low (15%–50% probability) (rationale in Table 7).
TABLE 7.
Comprehensive analysis of the uncertainties in the BoE.
| What is the level of certainty that the dietary intake of folic acid is positively and causally associated with the exacerbation of the neurological manifestations of cobalamin deficiency? | ||
|---|---|---|
| BoE | LoE1. Standalone main: incidence/recurrence of neuropathy in cobalamin deficient individuals >300 cases, reported in 23 publications (16 prospective case series and 7 retrospective case reports) | Initial certainty: Low (<15%–50% probability) |
| Domain | Rationale | Evaluation |
| RoB |
Exposure characterisation: low concern regarding risk of bias Outcome assessment: low concern regarding risk of bias Potential confounders: high concern regarding risk of bias due to potential confounding by cobalamin body stores and subclinical neurological changes at start of folic acid treatment |
Serious |
| Unexplained inconsistency | There is substantial variability in the doses and durations of folic acid supplementation which have been associated with neurological manifestations and in the severity of the symptoms reported in these patients. Sources of heterogeneity, which may have contributed to the inconsistency, include: the inclusion of patients with or without prior treatment with liver extracts (or other cobalamin supply) (i.e. variability in cobalamin body stores at start of folic acid treatment); the inclusion of patients with or without pre‐existing neurological manifestations at the start of folic acid intervention; the criteria applied for the diagnostic of neurological symptoms | Not serious |
| Indirectness | Evidence mostly arises from individuals with PA; few cases were also reported in patients with other gastric conditions which affect the production of intrinsic factor. These are common causes of cobalamin deficiency | Not serious |
| Imprecision | Not applicable | NA |
| Publication bias | No private funding involved. Publication bias could not be assessed through funnel plot and Egger test | Undetected |
| Upgrading factors |
Dose–response: No consistent evidence for a dose–response Consistency across LoEs: Limited support from animal experiments. Insufficient to upgrade the level of certainty. Magnitude: Not applicable |
None identified |
| Final certainty | Started ‘low’. No further downgrade was applied for the concerns related to confounding as it is considered to be inherent to the study design (i.e. already accounted for through the initial uncertainty rating assigned to this design) | Low (15%–50% probability) |
Abbreviations: BoE, body of evidence; LoEs, lines of evidence; NA, not applicable; PA, pernicious anaemia.
Modes of action
Savage and Lindenbaum (1995) summarised hypotheses by which folic acid/folate may causally contribute to the onset/progression of neurological manifestations in cobalamin deficient individuals: (i) 5‐MTHF toxicity; (ii) diversion of cobalamin from the nervous system; (iii) diversion of cobalamin from the mutase reaction; (iv) diversion of methionine from the nervous system.
Folic acid has also been suggested to oxidise cobalt in the cobalamin coenzyme of methionine synthase, thus interfering with cobalamin metabolism. However, in vitro studies failed to show any oxidation of the enzyme by folic acid (Paul & Selhub, 2017). It has been further hypothesised that high folate status may deplete active cobalamin in serum, holoTC, thereby limiting the availability of cobalamin for tissues (Selhub et al., 2022).
The Panel notes that, although several mechanisms have been proposed for a causal role of folic acid in the exacerbation of the neurological manifestations in cobalamin deficient individuals, experimental evidence in support of these hypotheses is limited.
Overall conclusions
The level of certainty in a positive and causal relationship between the dietary intake of folic acid and the exacerbation of the neurological manifestations of cobalamin deficiency is low (15%–50% probability) (rationale in Table 7). The available BoE regarding the mode of action cannot be used to modify the level of certainty in this conclusion.
3.4.1.2. Progression of the neurological manifestations of cobalamin deficiency
A causal relationship between the intake of folic acid and a (transient) resolution of megaloblastic anaemia in cobalamin deficient individuals is well established (IOM, 1998; Savage & Lindenbaum, 1995; SCF, 2000). Of note, a similar effect was reported with supplemental intake of natural reduced folate 5‐formyl‐THF (Savage & Lindenbaum, 1995).
As discussed above, there is concern that the resolution of megaloblastic anaemia by folic acid could delay the diagnosis of cobalamin deficiency, allowing neurological manifestations to concurrently progress. Based on its review of the evidence from the above‐mentioned case reports/series, the SCF previously concluded in relation to folic acid supplementation that ‘masking of the haematological signs in PA patients occurs with high frequencies and consistently with daily intakes of 5000 μg; however, insufficient data are available for evaluation of dose levels between 1000 and 5000 μg’. The SCF considered that dosages up to 1000 μg of folic acid ‘are unlikely to cause masking of the haematological signs in PA patients’.
The Panel found no new evidence that can be used to further characterise the dose–response between the intake of folic acid and the resolution of megaloblastic anaemia in cobalamin deficient individuals. The Panel also found no new evidence that the correction of haematological signs of cobalamin deficiency would delay diagnosis at doses of folic acid ≤1000 μg/day.
3.4.2. Cognitive impairment in individuals with low cobalamin status
It has been hypothesised that high folate intake/status may increase the risk of poor cognitive performance or exacerbate the decline in cognition in older individuals, with low or marginally low cobalamin status. Some cross‐sectional studies have investigated the association between combined measures of folate and cobalamin status and measures of cognitive function. Several found that the combination of high folate and low cobalamin status was associated with higher risk of cognitive impairment, increased grey matter atrophy and faster decline in cognition over time; however, other studies reported no such associations (Molloy, 2020). The study design and outcome measurements varied substantially, with a variety of biochemical markers and cut‐offs being used to define a deficient or insufficient cobalamin status, or a ‘high’ folate status, making comparisons between studies difficult.
For cognitive impairment, studies addressing changes in functional measures of cognitive function or incidence of dementia or Alzheimer disease are included in standalone main LoEs.
A systematic review of the literature was conducted. Eligible study designs were limited to prospective designs, i.e. RCTs, PCs and NCCs (see protocol in Annex A). The flow chart is provided in Appendix A.1 and an overview of the eligible studies retrieved is provided in Table 8.
TABLE 8.
Outcome of the systematic search on folate and cognitive impairment (sQ2b).
| LoE | Endpoints | RCTs | PCs/NCCs |
|---|---|---|---|
| LoE1. Standalone (main) | Changes in functional measures of cognitive function | 1 |
3 P/S folate: 2 RBC folate: 0 P/S UFA: 0 Dietary intake of FA/folate: 0 |
| LoE1. Standalone (main) | Incidence of dementia or Alzheimer disease | 0 | 1 |
Abbreviations: FA, folic acid; LoE, line of evidence; NCC, nested case–control; P/S, plasma/serum; PC, prospective cohort; RBC, red blood cell; RCT, randomised controlled trial; UFA, unmetabolised folic acid.
3.4.2.1. Intervention studies
LoE1. Standalone main: changes in functional measures of cognitive function
Preliminary UA
The effect of 3‐year folic acid supplementation (800 μg/day) on cognitive function was evaluated in adults aged 50–70 years with elevated homocysteine (≥13 μmol/L) in the Netherlands (Durga et al., 2007) (Appendix C.1.1). Subjects with serum cobalamin <200 pmol/L at baseline were excluded. Mean (IQR) serum folate at baseline was 12 (9–15) nmol/L in the intervention group (n = 405) and 10 (10–15) nmol/L in the control group (n = 413). At the end of trial, concentrations were 76 (50–103) nmol/L versus 13 (10–17) nmol/L in the respective groups. Cognitive function was assessed at baseline and end of trial with five tests used in the Maastricht Aging Study to construct five a‐priori‐defined cognitive domains: memory, sensorimotor speed, complex speed, information processing speed and word fluency. Better scores were obtained in relation to global cognitive function, memory, sensorimotor speed and information processing speed in the folic acid‐supplemented group vs. controls. In stratified analysis according to serum cobalamin, folic acid supplementation improved sensorimotor speed (difference in Z‐score 0.112; 95% CI 0.001, 0.223) and information processing speed (0.190; 95% CI 0.055, 0.325) compared to placebo among the 230 participants with ‘low’ cobalamin status at baseline (serum cobalamin <250 pmol/L). No effect was found on the other endpoints. No significant differences were observed among the 588 participants with baseline serum cobalamin ≥250 pmol/L. The study was judged at low risk of bias (tier 1) (Appendix B.1.1).
The Panel considers that the available BoE from RCTs does not suggest a positive relationship between dietary intake of folate and cognitive impairment in individuals with low cobalamin status at the intake level investigated. No comprehensive UA is performed.
3.4.2.2. Observational prospective studies
Four eligible prospective observational studies were retrieved. The study by Wang et al. (2001) regarding the incidence of Alzheimer's disease is not further discussed as it investigates the association in subjects with ‘low’ compared to ‘normal’ serum folate concentration (>10 nmol/L), thus providing no relevant information for this assessment. The results of the three other studies (Clarke et al., 2007; Doets et al., 2014; Morris et al., 2012) are discussed below.
LoE1. Standalone main: changes in functional measures of cognitive function
Preliminary UA
The evidence table is in Appendix C.1.2.
Morris et al. (2012) studied plasma folate and cobalamin concentrations in relation to cognitive decline among 549 participants from the US Framingham cohort (mean age 75 years). Cognitive function was assessed through biannual mini‐mental state examination (MMSE) over an 8‐year follow‐up. Participants were categorised in quintiles of plasma folate then stratified according to plasma cobalamin (< or ≥258 pmol/L). No association between plasma folate concentration and cognition was seen among participants with plasma cobalamin ≥258 pmol/L at baseline. Among participants with plasma cobalamin <258 pmol/L at baseline, plasma folate in the highest quintile (>21.75 nmol/L) was associated with greater decline in cognitive function compared to the other quintiles (MMSE score in Q1 [n = 60]: –0.32 [95% CI –0.44, −0.21]; Q2 [n = 64]: –0.32 [95% CI –0.42, −0.21]; Q3 [n = 44]: –0.22 [95% CI –0.35, −0.08]; Q4 [n = 39]: –0.28 [95% CI –0.42, −0.14]; Q5 [n = 24]: –0.92 [95% CI –1.09, −0.74]). The Panel notes that the rates of cognitive decline among participants of the 1st to 4th quintiles of plasma folate were comparable, with no apparent dose–response. Among individuals with plasma cobalamin <258 pmol/L at baseline, the use of supplements containing folic acid (mainly multivitamins) was associated with greater cognitive decline compared to no use of supplemental folic acid (MMSE score − 0.78 [95% CI –1.00, −0.57] vs. −0.34; [95% CI –0.39, −0.27]). No such association was found in those with plasma cobalamin ≥258 pmol/L at baseline. The study was judged at low risk of bias (tier 1) (Appendix B.1.2). The Panel notes that the number of individuals with plasma cobalamin <258 pmol/L in the highest quintile of plasma folate is relatively small (n = 24), that the range of folate concentrations covered by the highest quintile is large (between 21.75 and 149 nmol/L), and that the proportion of individuals with folate concentrations above the normal range is unknown.
Clarke et al. (2007) investigated interactions between serum cobalamin and folate concentrations for associations with cognitive decline over 10 years, assessed through at least three MMSE among 574 participants of the UK Oxford Healthy Aging Project (mean age 72 years). The authors reported that the ‘interaction terms were not statistically significant’ (data not shown). The study was judged at low risk of bias (tier 1) (Appendix B.1.2).
Using data from the Hordaland Health Study in Norway, Doets et al. (2014) investigated the interaction between serum cobalamin and folate in relation to cognitive decline, assessed through several cognitive tests performed after 6 years of follow‐up. The population (2203 participants; mean age at follow‐up 72.5 years) was not exposed to mandatory or voluntary folate food fortification; 9.5% of the participants were users of supplements containing B‐vitamins. The median (P5th–P95th) plasma folate concentration was 12.5 (8.7, 20.9) nmol/L. No interaction was found between plasma folate and cobalamin concentrations at baseline in relation to overall cognitive performance (β = 0.024, SE = 0.028, p = 0.394). The study was judged at low risk of bias (tier 1) (Appendix B.1.2).
The Panel notes the paucity of data from prospective observational studies that would allow the evaluation of an association between ‘high’ folate intake and impaired cognitive function in individuals with low cobalamin status. No comprehensive UA is performed.
3.4.2.3. Overall conclusions on cognitive impairment
The Panel considers that the available BoE is insufficient to conclude on a relationship between high dietary intake of folate and impaired cognitive function in individuals with low cobalamin status.
3.4.3. Risk of colorectal cancer
For the risk of CRC, studies addressing the incidence of CRC are included in the standalone main LoE and studies addressing the incidence of colorectal adenomas are included in the standalone surrogate LoE.
A systematic review of the literature was conducted (see protocol in Annex A). The flow chart is provided in Appendix A.2.
An overview of the eligible studies retrieved is provided in Table 9.
TABLE 9.
Outcome of the systematic search on folate and risk of colorectal cancer (sQ3b).
| LoE | Endpoints | RCTs | PCs/NCCs |
|---|---|---|---|
| LoE1. Standalone (main) | Incidence/recurrence of CRC | 1 |
34 P/S folate: 14 RBC folate: 2 a P/S UFA: 2 b Dietary intake of FA/folate: 23 c |
| LoE2. Standalone (surrogate) | Incidence/recurrence of colorectal adenomas | 7 d |
7 P/S folate: 2 RBC folate: 0 P/S UFA: 0 Dietary intake of FA/folate: 5 |
Abbreviations: CRC, colorectal cancer; FA, folic acid; LoE, line of evidence; NCC, nested case–control; P/S, plasma/serum; PC, prospective cohort; RBC, red blood cell; RCT, randomised controlled trial; UFA, Unmetabolised folic acid
The two studies assessing RBC also assessed P/S folate.
One study assessing UFA also assessed P/S folate.
Three studies assessing dietary intake of folate also assessed P/S folate.
3.4.3.1. Intervention studies
A total of eight publications reporting on six RCTs met the inclusion criteria.
LoE1. Standalone main: incidence/recurrence of colorectal cancer
Preliminary UA
One eligible RCT was retrieved (Appendix C.2.1.a). The China Stroke Primary Prevention Trial (CSPPT) (Qin et al., 2017), which involved 20,702 hypertensive men and women, was designed to test whether enalapril–folic acid treatment is more effective in reducing the risk of stroke than enalapril alone (Huo et al., 2015). The intervention was 800 μg folic acid and 10 mg enalapril per day compared to 10 mg/day enalapril alone for a median duration of 4.5 years. The median (IQR) baseline serum folate was ~18 nmol/L (12–23 nmol/L). Cancer events, including CRC, were reported by participants among the safety endpoints of the trial during follow‐up visits; cases were reviewed and adjudicated by an independent committee. In intention‐to‐treat (ITT) analysis for CRC, the hazard ratio (HR) was 2.17 (95% CI 0.82, 5.70), p = 0.117 (13 cases [0.13%] in the group on enalapril–folic acid treatment vs. six cases [0.06%] in the group on enalapril alone). The HR for all cancer subtypes was 1.00 (95% CI 0.77, 1.29). The study was considered to be at low risk of bias (tier 1) (Appendix B.2.1).
The Panel notes the limited BoE from intervention studies on the effect of folic acid supplementation on the incidence of CRC.
The Panel considers that the available BoE from intervention studies is insufficient to conclude on a relationship between dietary intake of folate and risk of CRC. The Panel notes that all available evidence is on folic acid. No comprehensive UA is performed.
LoE2. Standalone surrogate: incidence/recurrence of colorectal adenomas
Preliminary UA
A total of seven publications reporting on five eligible RCTs explored the effect of folic acid supplementation on the risk of colorectal adenomas (Jaszewski et al., 2008; Logan et al., 2008) (the United Kingdom Colorectal Adenoma Prevention [ukCAP] trial); (Wu et al., 2009) (Nurses' Health Study [NHS]/Health Professionals Follow‐Up Study [HPFS]); (Cole et al., 2007; Passarelli et al., 2019) (Aspirin/Folate Polyp Prevention Study [AFPPS]); (Gao et al., 2013). In the trial by Gao et al. (2013), about 30% of the trial participants had an inadequate folate status at baseline (<10 nmol/L). Given the potential relationship between ‘low’ folate status and a higher risk of colorectal cancer (National Toxicology Program, 2015), the study is not further discussed.
Among the four remaining trials, the supplemental intake of folic acid ranged from 500 to 5000 μg per day and the mean intervention period ranged from 3 to 8 years.
The study size ranged between 49 (Jaszewski et al., 2008) and 501 participants (Cole et al., 2007) in the intervention groups. Trials involved men and women, with mean age at baseline ranging between 57 years (Cole et al., 2007; Passarelli et al., 2019) and 65 years (Wu et al., 2009). All trials recruited patients with a previous history of colorectal adenoma. Three studies were conducted in the US (AFPPS, NHS/HPFS and the trial by Jaszewski et al.) and one in the UK and Denmark (UkCAP). In the three US studies, mean/median plasma/serum folate concentration at baseline were 21 and 23 nmol/L (no mandatory food fortification at trial start [Cole et al., 2007; Wu et al., 2009]); and 38 nmol/L (mandatory fortification in place [Jaszewski et al., 2008]).
In the AFPPS, ukCAP and the trial by Jaszewski et al. (2008), all participants had a colonoscopy planned at the end of the intervention phase (i.e. after ≥3 years of supplementation), while in the NHS/HPFS trial the ascertainment of colorectal adenomas was based on participants who self‐reported having at least one endoscopy ≤4 years after initiation of trial.
The AFPPS, ukCAP, NHS/HPFS trials reported risk ratios (RRs) and their corresponding 95% CIs for the recurrence of at least one colorectal adenoma (primary outcome) and the risk of ‘advanced adenomas’ 27 (secondary outcome) (Cole et al., 2007;Logan et al., 2008 ; Wu et al., 2009). The AFPPS and NHS/HPFS trials also analysed the risk of developing multiple lesions (secondary outcome) (Cole et al., 2007; Wu et al., 2009). In a subsequent analysis of the AFPPS trial, risk ratios for specific types of adenomas (i.e. conventional vs. sessile serrated adenomas/polyps [SSA/P]) were estimated (Passarelli et al., 2019). Jaszewski et al. (2008) provided a comparison of the mean number of adenomas per patient in the treatment versus placebo groups (primary outcome).
The evidence table is provided in Appendix C.2.1.b and the outcome of the risk of bias appraisal in Appendix B.2.1. For three out of the four studies (Logan et al., 2008; Wu et al., 2009), key study characteristics, together with the effect estimates and related CIs for ‘any recurrent adenoma’ and ‘advanced adenomas’ are plotted in Figure 10. For the AFPPS, results reported by Cole et al. (2007) are displayed, upon consideration of the comparability of definitions of ‘advanced adenomas’ between trials. The results from Jaszewski et al. (2008) are not included in the plot as they are not directly comparable to those reported in the other studies, i.e. outcome analysed as mean number of adenomas per patient. No meta‐analysis was conducted in view of the limited number of studies and their heterogeneity (folic acid dose and duration; mandatory fortification in place or not).
FIGURE 10.

RCTs on the effect of folic acid supplementation on recurrent colorectal adenomas. Mandatory fort, yes/no: reflects mandatory fortification policy status at study start. For Cole et al., 2007 and Wu et al., 2009, fortification became mandatory during the trials. For Logan et al., 2008 and Cole et al., 2007 unadjusted risk ratios (RRs); for Wu et al., 2009, RRs from the multivariable‐adjusted models.
In the AFPPS (Cole et al., 2007; Passarelli et al., 2019), participants were randomised to a placebo (with or without aspirin; n = 505) or 1000 μg folic acid/day (with or without aspirin; n = 516) for 3 years (first follow‐up). Then, 71.4% of participants voluntarily continued the folic acid/placebo intervention for an additional 3–5 years (second follow‐up; n = 359 in the placebo group vs. n = 370 in the folic acid group). The aspirin investigation was not continued in the second follow‐up. Colonoscopies were performed toward the end of each follow‐up. A proportion (20%) of the participants stopped taking folic acid/placebo during the second follow‐up period but completed the second follow‐up colonoscopy.
Cole et al. (2007) evaluated outcome incidence during the first and second follow‐up intervals until study treatment was terminated in the entire study population (including participants who discontinued supplementation during the second follow‐up). The number of participants with follow‐up colonoscopies were 486 in the placebo group and 501 in the folic acid group at the end for the first follow‐up (i.e. 97% of initial study population), and 304 in the placebo group and 303 in the folic acid group at the end of the second follow‐up (i.e. 59% of the initial study population). The number of events was higher in the folic acid vs. placebo groups for any adenoma, advanced lesion and ≥3 adenomas in both periods. At the end of the second follow‐up, the unadjusted RRs were 1.13 (95% CI 0.93, 1.37) for any adenoma (113/304 [37%] in placebo vs. 127/303 [42%] in folic acid group), 1.67 (95% CI 1.00, 2.80) for advanced lesions (21/304 [7%] vs. 35/303 [12%]) and 2.32 (95% CI 1.23, 4.35) for ≥three lesions (13/304 [4%] vs. 30/303 [10%]). Investigators reported similar results after adjustment for age, sex, clinical centre, number of lifetime adenomas and duration of follow‐up (data not shown), and when the analysis was restricted to the participants who had agreed to extended treatment with folic acid or placebo in the second follow‐up interval. In the first period, no significant interaction between folic acid and aspirin treatment was found; however, the suggestion of an increased risk with folic acid was confined to participants not allocated to aspirin. The study was judged at low risk of bias (tier 1). In a subsequent analysis, no evidence was found that baseline folate intake or plasma/RBC concentrations modified the association between folic acid treatment and risk of adenomas (Figueiredo et al., 2008).
Passarelli et al. (2019) performed a secondary analysis of the second follow‐up period restricted to participants who had agreed to extend treatment. In this re‐analysis, all colonoscopies performed until the intended end of the second follow‐up (i.e. including those who were completed after study treatment was terminated) were included and the incidence of SSA/P was re‐ascertained in view of the latest definition by an expert panel (i.e. with and without cytological dysplasia). 28 The number of participants included were 338 for the folic acid group and 325 for the placebo group (i.e. 91% of the participants with prolonged treatment, in both groups). Different from the Cole analysis, SSA/Ps were not counted among advanced or multiple lesions; advanced conventional adenomas and SSA/Ps were analysed separately 29 (Passarelli, 2023. Personal communication). RRs were 1.21 (95% CI 0.99, 1.47; 118/325 [36%] in placebo vs. 146/338 [43%] in folic acid group) for any adenoma, 1.20 (95% CI 0.73, 1.97; 27/325 [8%] in placebo vs. 32/338 [9%] in folic acid group) for advanced conventional adenomas, 1.58 (95% CI 0.87, 2.86; 16/325 [5%] in placebo vs. 30/338 [9%] in folic acid group) for ≥three conventional adenomas and 1.94 (95% CI 1.02, 3.68; 16/325 [5%] in placebo vs. 28/338 [8%] in folic acid group) for SSA/P. RRs were adjusted for randomisation strata and baseline characteristics associated with agreement to extend treatment and the availability of post‐treatment follow‐up. The study was judged at low risk of bias (tier 1).
In an analysis of lesions found during the surveillance interval, which lasted 7.5 years after the termination of study treatment, RRs were attenuated and null for all outcomes (Passarelli et al., 2019).
In a post hoc analyses of the AFPPS data, Rees et al. (2017) investigated the associations between plasma concentrations of 5‐MTHF or UFA, measured at the end of the 1st follow‐up period, and adenoma recurrence. The mean ± SD concentrations of 5‐MTHF and UFA were 46.3 ± 21.7 nmol/L and 3.4 ± 8.5 nmol/L in the placebo group (UFA detected in 23% samples) and 84.8 ± 29.5 nmol/L and 21.7 ± 24.9 nmol/L in the folic acid group (UFA detected in 73% samples). No association was found between plasma 5‐MTHF and overall adenoma risk during either follow‐up intervals: RRs for upper (>85.5 nmol/L) versus lowest quartiles of 5‐MTHF (<37.3 nmol/L) were 1.02 (95% CI 0.74, 1.42) and 1.01 (0.68, 1.59) in the respective periods. During the second follow‐up, the RRs for the upper vs. lowest quartiles of 5‐MTHF were 1.25 (95 CI% 0.61, 2.55) for advanced adenomas (13/166 [7.8%] in Q1 vs. 15/158 [9.5%] in Q4), 1.58 (95 CI% 0.80, 3.09) for the composite endpoint of advanced and ≥3 adenomas (15/170 [8.8%] in Q1 vs. 21/162 [12.9%] in Q4), and 0.61 (95% CI 0.36, 1.23) for serrated lesions (i.e. hyperplastic polyps, sessile serrated adenomas/polyps and traditional serrated adenomas; 52/167 [31%] in Q1 vs. 28/158 [17.7%] in Q4). No indication of higher risk of adenomas with elevated UFA was found.
In the ukCAP trial (Logan et al., 2008), participants were randomised to 500 μg/day folic acid versus placebo (with or without 300 mg aspirin/day) for 3 years. Of the 939 initially randomised, 853 (91%) completed a colonoscopy at the end of the intervention and were included in the analysis. RRs were 1.07 (95% CI 0.85, 1.34) for the risk of any adenoma recurrence (105/421 (25%) in placebo vs. 115/432 (27%) in folic acid group) and 0.98 (95% CI 0.68, 1.40) for the risk of advanced adenoma recurrence (52/421 in placebo vs. 52/432 in folic acid group). No evidence was found for an interaction between aspirin and folic acid. The study was judged at low risk of bias (tier 1).
In the NHS/HPFS trial (Wu et al., 2009), participants were randomised to 1000 μg folic acid/day or placebo for an initial period of 3 years. About half of the participants consented to extend the treatment for a total of 5–6.5 years. Participants were requested to report recent endoscopies on a yearly basis during follow‐up; endoscopies performed ≥3 months after initiation of trial and <12 months after completion of the trial were included. Of the 672 initially randomised, 475 (71%) reported follow‐up endoscopies and were included in the analysis. RRs were 0.87 (95% CI 0.65, 1.16) for colorectal adenoma (72/238 [30%] in placebo vs. 62/237 [26%] in folic acid group) and 1.03 (95% CI 0.53, 1.98) for advanced adenoma (17/225 [8%] in placebo vs. 16/221 [7%] in folic acid group). In stratified analyses, RRs for colorectal adenomas were 0.61 (95% CI 0.42, 0.90) among participants with baseline plasma folate ≤7.5 ng/mL (17 nmol/L) and 1.28 (95% CI 0.82, 1.99) in those with plasma folate >7.5 ng/mL. In a sensitivity analysis stratifying according to the time between start of trial and first endoscopy (≤24 months vs. >24 months), associations were reported to be similar (data not shown). The study was judged at low risk of bias (tier 1).
In the trial by Jaszewski et al. (2008), 137 participants were randomised to 5000 μg folic acid per day or a placebo for 3 years, after which a follow‐up colonoscopy was performed. A total of 70% (n = 94) of the participants completed the 3 years follow‐up examination (n = 49 in the intervention group; n = 45 in the control group). The mean (±SD) number of adenomas per patient was 0.36 ± 0.69 in the intervention group vs. 0.82 ± 1.17 in the control group (p = 0.03). The study was judged at moderate risk of bias (tier 2).
The Panel notes that evidence from RCTs on the relationship between folic acid supplementation and risk of recurrence of colorectal adenomas is inconsistent. Among the three studies judged to be at low risk of bias (tier 1), two trials reported no association at doses of 500 μg/day for 3 years (UkCAP) and 1000 μg/day for up to 6.5 years (NHS/HPFS), whereas the AFPPS trial suggested a higher risk of adenoma recurrence, specifically SSA/P, with 1000 μg folic acid/day for up to 8 years. The size and precision of the trials were comparable, and the 95% CIs of the three trials overlap (Figure 10). Potential sources of heterogeneity are difficult to identify in view of the low number of studies available.
The Panel notes that the diagnostic criteria for the classification of colorectal adenomas have evolved as research progressed, especially as insight was gained about the clinical relevance of sessile serrated lesions 30 (WHO, 2000, 2010, 2019). Before 2010, neoplastic serrated lesions were not well detected during endoscopy and were often interpreted as hyperplastic polyps (Crockett & Nagtegaal, 2019). Specific risks for conventional adenomas vs. sessile serrated lesions (SSA/Ps) were only evaluated in the secondary analysis of the AFPPS trial (WHO, 2000, 2010, 2019). An increased risk with folic acid supplementation was found for SSA/Ps (RR 1.94 (95% CI 1.02, 3.68)), indicating that the increased risk of advanced adenomas observed by Cole was mainly driven by this type of lesions.
The Panel considers that the available BoE from intervention studies is insufficient to conclude on a positive and causal relationship between dietary intake of folate and risk of CRC. The Panel notes that all available evidence is on folic acid. No comprehensive UA is performed.
3.4.3.2. Observational prospective studies
LoE1. Standalone main: incidence/recurrence of colorectal cancer
Preliminary UA
Plasma/Serum (P/S) and RBC folate
Among the 14 studies which assessed P/S folate, 2 were PCs (Geijsen et al., 2020; Rossi et al., 2006) and 12 were NCCs (Eussen et al., 2010; Glynn et al., 1996; Gylling et al., 2014; Kato et al., 1999; Le Marchand et al., 2005; Lee et al., 2012; Neuhouser et al., 2015; Otani et al., 2008; Shrubsole et al., 2009; Takata et al., 2014; Van Guelpen et al., 2006; Weinstein et al., 2008). All investigated incident CRC, except one which investigated recurrent CRC (Geijsen et al., 2020). The size of the PCs ranged between 1988 and 2024 participants and of the NCCs between 474 and 3566 participants. The length of follow‐up ranged from 3.7 years (Geijsen et al., 2020) to 23 years (Rossi et al., 2006). The cohorts were based in Europe (n = 6), USA (n = 4), China (n = 2), Australia (n = 1) and Japan (n = 1). Three studies involved females only, three studies males only and eight studies both males and females.
Four studies were at low risk of bias (tier 1) and nine studies at moderate risk of bias (tier 2) (Appendix B.2.2).
The evidence table is in Appendix C.2.2.a. Key study characteristics, together with the risk estimates and related 95% CIs, are plotted in Figure 11.
FIGURE 11.
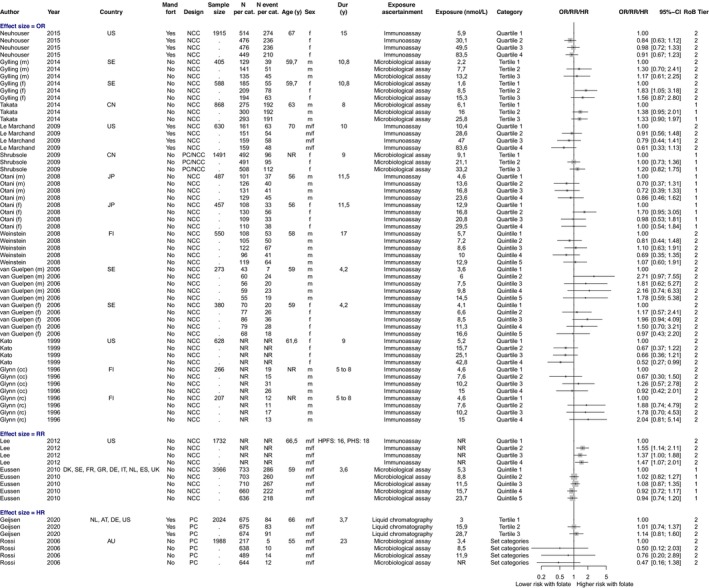
Observational studies on plasma/serum folate and incident/recurrent colorectal cancer, most adjusted RRs from PCs and NCCs. Exposure values, age and duration correspond to the mean/median of each category; mandatory fort, yes/no: reflects policy status at baseline; (cc): incident colon cancer; (rc): incident rectal cancer; (m): men; (f): women; Rossi et al. and Kato et al. the cases denote CRC morbidity; Rossi et al. presented values with the highest category as reference, which was converted; For Glynn et al., 1996, the risk estimates adjusted for matching factors only is displayed; For Neuhouser et al. (2015), the plasma sampling period was between 1993 and 1998, thus before and after the introduction of folate fortification; For Lee et al., 2012 the median levels of plasma folate across quartiles ranged between 9 and 40 nmol/L in the NHS, 7 and 25 nmol/L in the HPFS and 5 and 25 nmol/L in the PHS. AT, Austria; AU, Australia; CN, China; DE, Germany; DK, Denmark; ES, Spain; FI, Finland; FR, France; GR, Greece; IT, Italy; JP, Japan; NL, The Netherlands; SE, Sweden; UK, United Kingdom; US, United States; pc, prospective cohort; ncc, nested case–control study; Dur, duration; Mand fort, mandatory fortification; n per cat, number of participants per category; n event per cat, number of events per category.
The findings across studies are inconsistent, with studies suggesting positive (five studies), null (six studies) or inverse associations (three studies) between P/S folate and risk of incident/recurrent CRC (Figure 11). In the five studies suggesting a positive association, a similar higher risk of CRC was found for all categories of P/S folate compared to the lowest category and no indication of a dose–response was evident (Glynn et al., 1996; Gylling et al., 2014; Lee et al., 2012; Takata et al., 2014; Van Guelpen et al., 2006).
Two US cohorts considered folate exposure after the introduction of mandatory fortification in 1998, thus including participants with the highest folate exposure (P/S folate ≥60 nmol/L in the top quartiles) (Le Marchand et al., 2009; Neuhouser et al., 2015). No evidence for a positive association was found after a follow‐up duration of 10 and 15 years, respectively.
In the two studies which assessed RBC folate in addition to P/S folate, no positive association with the risk of CRC was found (findings between the two biomarkers were consistent) (Neuhouser et al., 2015; Rossi et al., 2006) (Appendix C.2.2.a).
The Panel considers that the BoE from observational studies does not suggest a positive relationship between P/S folate or RBC folate and risk of CRC over the range of exposures investigated in these studies.
P/S UFA
In a subgroup analysis, Geijsen et al. (2020) also investigated the association between UFA concentration and recurrent CRC (median follow‐up duration: 3.7 years) among participants from European and US cohort studies with detectable folic acid (15% of all participants; median [IQR] 1.0 [0.7–1.9] nmol/L). A higher risk of CRC recurrence was observed for each two‐fold increase in UFA (HR = 1.31; 95% CI 1.02, 1.58). The HR was 1.86 (95% CI 0.76,4.56) in the 2nd tertile (UFA 0.75–1.46 nmol/L) and 3.12 (95% CI 1.22, 8.00) in the 3rd tertile (UFA >1.46 nmol/L) as compared to the 1st tertile (UFA <0.75 nmol/L). The study was judged at moderate risk of bias (tier 2).
In the NCC study within the NHS and HPFS cohorts, Cho et al. (2015) investigated the association between UFA concentration, measured before the introduction of the mandatory fortification, and incident CRC (follow‐up duration: 16 years for HPFS and 20 years for NHS). UFA was detected in 21.4% of the control and 22.0% of the CRC case patients. Among those, the median UFA level was 0.61 nmol/L in both control and case patients. Compared to individuals with undetectable folic acid levels (254 cases/437 controls), the odds ratios (ORs) were 1.03 (95% CI 0.73, 1.46) for participants with UFA concentration <0.5 nmol/L (233 cases/507 controls) and 1.12 (95% CI 0.81, 1.55) for participants with UFA concentration ≥0.5 nmol/L (131 cases/263 controls). The study was judged at moderate risk of bias (tier 2).
The Panel notes the low UFA concentrations in both studies. The Panel considers that the BoE available on a relationship between UFA concentrations and risk of CRC is limited and insufficient to draw conclusions.
Dietary intake of folate/folic acid
A total of 23 studies investigated the relationship between dietary folate and risk of CRC. The exposure was assessed as total folate intake (n = 13), folate intake from natural sources and fortified foods (i.e. excluding intake from food supplements; n = 4), natural folate intake (n = 16), folic acid intake (n = 2) and supplemental folic acid intake (n = 3), respectively. Some studies reported findings on more than one of the aforementioned exposures.
Studies addressing natural folate intake provide no relevant information for the present evaluation (Åkesson et al., 2023), and are thus not further discussed below.
Total folate intake
Among the 11 studies which investigated the relationship between total folate intake and incident CRC, 8 were PCs (Flood et al., 2002; Gibson et al., 2011; Kim et al., 2010; Lee et al., 2011; Razzak et al., 2012; Roswall et al., 2010; Stevens et al., 2011; Wang, Wu, et al., 2021; Zhang et al., 2006; Zschäbitz et al., 2013) and 3 were NCCs (Glynn et al., 1996; Kato et al., 1999; Le Marchand et al., 2005). Two additional articles included datasets which overlapped with the above‐mentioned studies, i.e. Kim et al. (2010), which is a pooled analysis of individual PCs, 31 and Wang, Wu, et al. (2021), which included a longer follow‐up of the NHS cohort compared to Lee et al. (2011), but did not include the HPFS cohort.
The size of the PCs ranged between 35,216 and 322,206 participants, and of the NCCs between 140 and 2781 participants. The length of follow‐up ranged from 5 to 8 years (Glynn et al., 1996) to 28 years (Wang, Wu, et al., 2021). The cohorts were based in Europe (n = 2), USA (n = 9) or both (n = 2). Six studies involved females only, one study males only and six studies both males and females.
Food frequency questionnaires (FFQs) were used to assess total folate intake in all studies. Two studies included repeated measurements of dietary folate intake over the duration of follow‐up (Lee et al., 2011; Wang, Wu, et al., 2021). The median/mean total folate intake in the lowest categories of intake was between 36 and 268 μg/day and in the highest categories of intake between 388 and 1417 μg/day.
Three studies were considered to be at low risk of bias (tier 1) and 10 studies at moderate risk of bias (tier 2) (Appendix B.2.2).
The evidence tables are in Appendix C.2.2.b and C.2.2.c. Key study characteristics, together with the risk estimates and related 95% CIs, are plotted in Figure 12 (all studies except Kim et al. (2010) and Wang, Wu, et al. (2021)).
FIGURE 12.
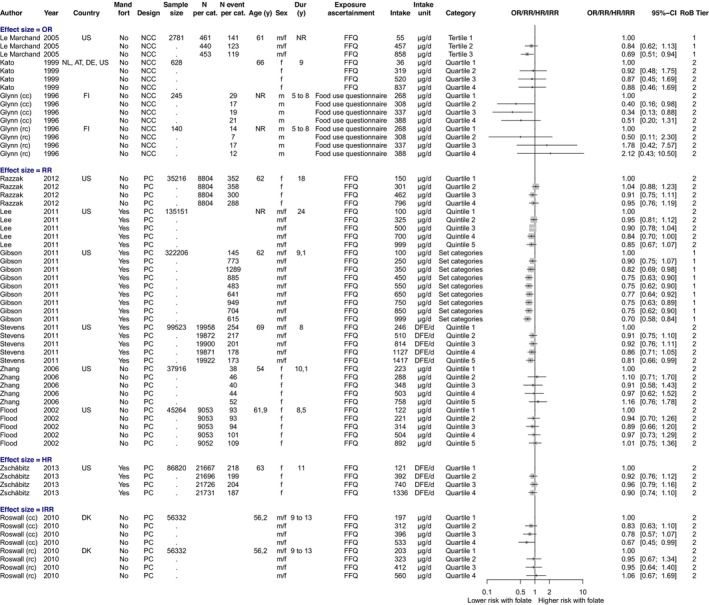
Total folate intake and incident colorectal cancer, most adjusted RRs from PCs and NCCs. Intake values, age and duration correspond to the mean/median of each category; mandatory fort, yes/no: reflects policy status at baseline; (cc): incident colon cancer; (rc): incident rectal cancer; In Kato et al. the cases denote CRC morbidity; In Le Marchand et al., the values are for the CC genotype; For Lee et al. (2011), Zschäbitz et al. (2013) and Gibson et al. (2011), mandatory fortification was considered as of 1998. Set categories refers to: Lee et al. (2011), Q1 (ref): <250; Q2: 250– < 400; Q3: 400– < 600; Q4: 600– < 800; Q5: ≥800 μg total folate/day, Gibson et al. (2011), Q1 (ref): ≤199; Q2: 200– ≤ 299; Q3: 300– ≤ 399; Q4: 400– ≤ 499; Q5: 500– ≤ 599; Q6: 600– ≤ 699; Q7: 700– ≤ 799; Q8: 800– ≤ 899; Q9: ≥900 μg total folate/day. AT, Austria; DE, Germany; DK, Denmark; FI, Finland; NL, The Netherlands; US, United States; pc, prospective cohort; ncc, nested case–control study; Dur, duration; Mand fort, mandatory fortification, n per cat, number of participants per category; n event per cat, number of events per category; DFE, dietary folate equivalent.
Four studies suggested an inverse association (Gibson et al., 2011; Le Marchand et al., 2005;Lee et al., 2011 ; Stevens et al., 2011) and five studies found no association with incident colorectal cancer (Flood et al., 2002; Kato et al., 1999; Razzak et al., 2012; Zhang et al., 2006; Zschäbitz et al., 2013). Glynn et al. (1996) and Roswall et al. (2010) reported a site‐specific association for the colon, but not the rectum (Figure 12).
No evidence for a positive relationship between total folate intake and risk of CRC was found in the additional analyses by Kim et al. (2010) and Wang, Wu, et al. (2021) (see evidence table Appendix C.2.2.c).
Five US studies considered total folate intake after the introduction of mandatory fortification, thus including participants with the highest total folate intake (≥800 μg/day in the top categories) (Gibson et al., 2011; Lee et al., 2011; Stevens et al., 2011; Wang, Wu, et al., 2021; Zschäbitz et al., 2013). No evidence for a positive association with the risk of CRC was found after of 8–28 years follow‐up, depending on the study.
The Panel considers that the BoE from observational studies does not suggest a positive relationship between total folate intake and risk of CRC over the range of intakes investigated in these studies.
Folate intake from natural sources and fortified foods
Four PCs investigated the relationship between folate intake from natural sources and fortified foods and incident CRC (Gibson et al., 2011; Lee et al., 2011; Stevens et al., 2011; Zschäbitz et al., 2013). The size of the cohorts ranged between 86,820 to 322,206 participants. The length of follow‐up ranged from 8 (Stevens et al., 2011) to 24 years (Lee et al., 2011). All cohorts were located in the USA and three involved both males and females, while one involved females only.
FFQs were used to assess dietary folate intake in all studies. The median/mean folate intake from natural sources and fortified foods were between 126 and 258 μg/day in the lowest categories of intake and between 434 and 599 μg/day in the highest categories of intake.
One study was considered to be at low risk of bias (tier 1) and three studies at moderate risk of bias (tier 2) (Appendix B.2.2).
The evidence table is in Appendix C.2.2.c. Key study characteristics, together with the risk estimates and related 95% CIs, are plotted in Figure 13.
FIGURE 13.
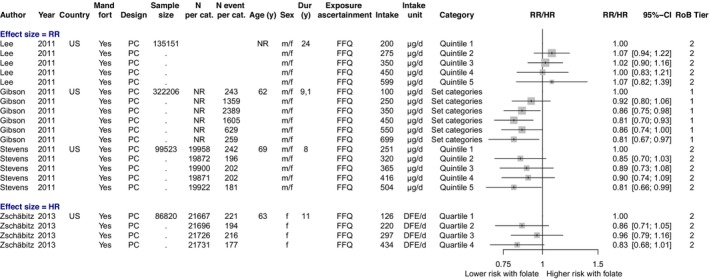
Folate intake from natural sources and fortified foods and incident colorectal cancer, most adjusted RRs from PCs. Intake values, age and duration correspond to the mean/median of each category; mandatory fort, yes/no: reflects policy status at baseline; Set categories refers to: Lee et al. (2011), Q1 (ref): <250; Q2: 250– < 400; Q3: 400– < 600; Q4: 600– < 800; Q5: ≥800 μg total folate/day; For Lee et al. (2011), Zschäbitz et al. (2013) and Gibson et al. (2011), mandatory fortification was considered as of 1998. US, United States; pc, prospective cohort; Dur, duration; Mand fort, mandatory fortification; n per cat, number of participants per category; n event per cat, number of events per category.
There was no indication for an increased risk of CRC associated with higher folate intake from natural sources and fortified foods in any of these studies (Figure 13).
The Panel considers that the BoE from observational studies does not suggest a positive relationship between folate intake from natural sources and fortified foods and risk of CRC over the range of intakes investigated in these studies.
Folic acid intake
Among the PCs reported above, five also analysed the association between intake of folic acid, either total (Lee et al., 2011; Stevens et al., 2011) or from supplementation alone (Gibson et al., 2011; Roswall et al., 2010; Zschäbitz et al., 2013), and risk of CRC. In this subset, the size of the PCs ranged between 56,332 and 322,206 participants. The length of follow‐up ranged from 8 (Stevens et al., 2011) to 24 years (Lee et al., 2011). Four cohorts were based in the USA and one in Denmark. One study involved females only, while the rest included both males and females.
One study was at low risk of bias (tier 1) and four studies at moderate risk of bias (tier 2) (Appendix B.2.2).
None of these studies support a positive relationship between folic acid intake (either total or from supplementation only) and risk of CRC (evidence table in Appendix C.2.2.c; data not plotted).
LoE1. Conclusion on observational prospective studies
The Panel considers that the available BoE from observational studies does not suggest a positive relationship between dietary folate intake and risk of CRC over the range of exposures investigated in these studies. No comprehensive UA is performed.
LoE2. Standalone surrogate: incidence/recurrence of colorectal adenoma
Preliminary UA
P/S folate
Two prospective studies investigated the association between P/S folate and occurrence or recurrence of colorectal adenomas (Appendix C.2.2.d). The study by Ding et al. (2016) is not further discussed as it compared the risk of colorectal adenomas between subjects with P/S folate above or below 10 nmol/L, thus providing no relevant information for this assessment.
Martínez et al. (2006) used data collected in 2125 US participants from two trials (Wheat bran fibre [WBF] trial and Ursodeoxycholic Acid [UDCA] trial), who were followed‐up for 2–3 years. An inverse association between plasma folate at baseline and adenoma recurrence was observed across quartiles (OR 0.74 [95% CI 0.56, 0.98] for the highest quartile >15.4 nmol/L vs. lowest <7.2 nmol/L; p‐trend <0.01). The study was judged at moderate risk of bias (tier 2).
Dietary intake of folate/folic acid
A total of five studies investigated the relationship between dietary folate/folic acid and the risk of colorectal adenomas. The exposure was assessed as total folate intake (n = 5), folate intake from natural sources and fortified foods (i.e. excluding intake from food supplements; n = 1) and natural folate intake (n = 3).
Evidence from studies addressing natural folate intake provides no relevant information for the present evaluation (Åkesson et al., 2023), and is thus not further discussed below.
Total folate intake
Four studies investigated the association between total folate intake and adenoma recurrence (polyp prevention trial [PPT] [Murphy et al., 2008]; polyp prevention study [PPS] [Baron et al., 1998]; WBF trial [Martínez et al., 2004]) or incidence [NHS/HPFS [Lee et al., 2011]). Three were PCs and one NCC. In addition, He et al. (2018) reported further analyses of the NHS and HPFS cohorts, adding data from the NHS II cohort and investigating the risk of conventional adenomas and serrated polyps separately.
The size of the cohorts ranged between 706 and 141,143 participants. The length of follow‐up ranged from 3 to 24 years. The studies were conducted in the USA and included both males and females.
FFQs were used to assess total folate intake in all studies. Two studies included repeated measurements of dietary folate intake over the duration of follow‐up (He et al., 2018; Lee et al., 2011). The median/mean total folate intake in the lowest categories of intake were between 100 and 243 μg/day and in the highest categories of intake between 391 and 999 μg/day.
The five studies were considered to be at moderate risk of bias (tier 2) (Appendix B.2.2).
The evidence tables are in Appendix C.2.2.e and Appendix C.2.2.f. Key study characteristics, together with the risk estimates and related 95% CIs, are plotted in Figure 14 (all studies except [He et al., 2018]).
FIGURE 14.
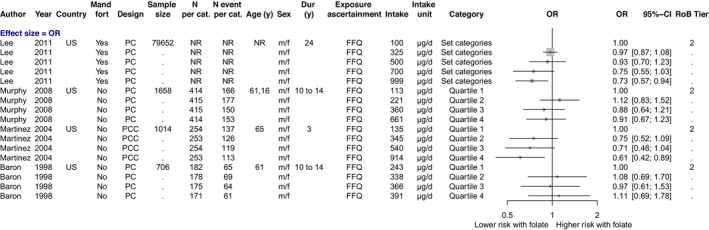
Total folate intake and incident/recurrent colorectal adenomas, most adjusted RRs from PCs and PCCs. Intake values, age and duration correspond to the mean/median of each category; mandatory fort, yes/no: reflects policy status at baseline; Set categories refers to Q1 (ref): <250; Q2: 250– < 300; Q3: 300– < 400; Q4: 400– < 500; Q5: ≥500 μg dietary folate/day. For Murphy et al. (2008), total folate intake estimate was calculated as energy density‐adjusted dietary folate + intake of folate from supplements as presented by the authors. For Lee et al. (2011), mandatory fortification was considered as of 1998. pc, prospective cohort; pcc, case cohort study; Dur, duration; Mand fort, mandatory fortification; n per cat, number of participants per category; n event per cat, number of events per category.
The available studies reported null (two studies; [Baron et al., 1998; Murphy et al., 2008]) or negative associations (two studies; [Lee et al., 2011; Martínez et al., 2004] between total folate intake and the risk of colorectal adenomas (Figure 14).
In the additional analysis of the NHS, NHS II, HPFS cohorts, He et al. (2018) investigated the association between total folate intake and the risk of conventional adenomas and serrated polyps (SPs) separately, over a follow‐up of 18–20 years. Any diagnosis of polyps was reported by the participants every 2 years and records of endoscopy and pathology were reviewed by study investigators. SPs included hyperplastic polyps and mix/serrated adenomas, while conventional adenomas included tubular, tubulovillous and villous adenomas, and adenomas with high‐grade dysplasia. Mean ± SD total folate intake was 527 ± 212 μg/day. A higher risk of SPs was observed in all quartiles of total folate intake compared to the lowest quartile, with no indication of a dose–response (OR for Q2 = 1.14 [95% CI 1.07, 1.21]; Q3 = 1.08 [95% CI 1.01, 1.15]; Q4 = 1.04 [95% CI 0.97, 1.11]). An inverse association was reported with conventional adenomas (OR for Q4 vs. Q1 = 0.93 [95% CI 0.87, 0.99]) (Appendix C.3.2). The study was considered to be at moderate risk of bias (tier 2).
The Panel considers that the BoE from observational studies does not suggest a positive relationship between total folate intake and risk of colorectal adenomas over the range of intakes investigated in these studies.
Folate intake from natural sources and fortified foods
Lee et al. (2011) also analysed the association between folate intake from natural sources and fortified foods and risk of colorectal adenoma. An inverse association comparing highest (≥500 μg/day) versus lowest (<250 μg/day) categories (OR 0.71; 95% CI 0.59,0.85) was found. The study was judged at moderate risk of bias (tier 2).
LoE2. Conclusion on observational prospective studies
The Panel considers that the available BoE from observational studies does not suggest a positive relationship between dietary folate intake and risk of colorectal adenomas over the range of exposure investigated in these studies. No comprehensive UA is performed.
3.4.3.3. Animal data
Several experiments in rodents have investigated the effect of dietary intake of folate on the risk of CRC. Supplemental intake of folate was given in the form of folic acid.
In male Fischer 344 rats exposed to AOM as carcinogenic agent (Wargovich et al., 1996), the number of colonic aberrant crypt foci (ACF) was found to be increased in the group receiving a diet containing 2.5 g folic acid/kg diet compared to control, when supplemental intake of folic acid was initiated before the induction of neoplastic lesion. The opposite was observed when supplemental intake of folic acid started after the induction of neoplastic lesion. There was no difference between the group receiving a diet containing 5 g folic acid/kg diet and the control group under either of the conditions. Notably, the doses of folic acid used in these experiments were >1000–2500 times rat basal dietary requirement (BDR) for folate.
In male Sprague–Dawley rats, Kim et al. (1996) found a protective effect of supplemental intake of folic acid of 8000 μg/kg diet compared to a folate‐adequate (2000 μg/kg diet, i.e. rat BDR for folate) or a folate‐deficient (0 μg/kg diet) diet for 30 weeks on the development of colorectal macroscopic tumours induced by DMH (injected weekly from week 5 to 15) as carcinogenic agent. At the highest dose tested of 40,000 μg/kg diet, no difference was found with the group receiving the folate‐adequate diet. In a later experiment in which folic acid dietary intervention was initiated for 28 weeks after the induction of neoplastic lesion by AOM, the mean numbers of colorectal tumours, adenocarcinomas and ACF per animal were not statistically significantly different in animals treated with folic acid at 2000, 5000 or 8000 μg/kg in the diet. Rectal epithelial proliferation increased significantly with FA doses (Lindzon et al., 2009).
In another experiment in Apc Min mice, a genetic murine model characterised by the spontaneous development of small intestinal and colonic tumours, which were randomised to a folate‐deficient (0 μg folic acid /kg diet), a folate‐adequate (2000 μg folic acid/kg diet) or diets containing either 8000 μg folic acid/kg diet or 20,000 μg folic acid/kg diet, Song et al. (2000) found no effect of the ‘high’ folic acid diets compared to the folate‐adequate on the risk of developing colonic ACF, colorectal adenomas or small intestinal adenomas.
The Panel considers that evidence from animal experiments on an adverse effect of ‘high’ folate intake on the risk of CRC is limited and inconclusive.
3.4.3.4. Mode of action
In the light of folate's role in nucleotide biosynthesis and DNA methylation processes (Section 3.2.3), hypotheses have been formulated by which excess folate intake may have a dual effect in CRC risk, depending on the stage of cell transformation at the time of the intervention. In normal colorectal epithelial cells, folate supplementation might prevent global DNA hypomethylation and reduce the risk of neoplastic transformation by ensuring genomic stability and integrity. An opposite effect might be induced in transformed colorectal epithelial cells, by providing nucleotide precursors for proliferation and growth of neoplastic cells, and/or by inducing de novo methylation of the promoter CpG island of cancer‐related genes, thereby altering gene expression and promoting tumour progression (Kim, 2016; Pieroth et al., 2018). Notably, FRs, which can transport folate into cells via endocytosis (Section 3.2.2), are often overexpressed in cancer cells. FRs are now being used as target molecules in the development of anti‐cancer drugs and in the delivery of drugs to cancer tissues (Scaranti et al., 2020). FRα has been found to be more frequently expressed in colon carcinoma compared to normal colonic tissue or adenomas (Shia et al., 2008).
The Panel notes that the fundamental role of folate in one‐carbon metabolism provides several potential pathways by which folate might affect cancer development. These are intricate pathways, subject to complex modulatory mechanisms and potentially affected by numerous factors (e.g. nutrition, environment, genetics). Further research is required to better understand the biological processes involved in CRC development and how they might be affected by the folate body pool.
3.4.3.5. Overall conclusions on colorectal cancer
The Panel considers that the available BoE is insufficient to conclude on a positive and causal relationship between high dietary intake of folate and risk of CRC.
3.4.4. Risk of prostate cancer
For the risk of prostate cancer, studies addressing the incidence of prostate cancer are included in the standalone main LoE.
A systematic review of the literature was conducted (see protocol in Annex A). The flow chart is provided in Appendix A.2. An overview of the eligible studies retrieved is provided in Table 10.
TABLE 10.
Outcome of the systematic search on folate and prostate cancer (sQ3c).
| LoE | Endpoints | RCTs | PCs/NCCs |
|---|---|---|---|
| LoE1. Standalone (main) | Incidence of prostate cancer | 2 a |
14 P/S folate: 7 RBC folate: 1 b Dietary intake of FA/folate: 7 |
Abbreviations: FA, folic acid; LoE, line of evidence; NCC, nested case–control; P/S, plasma/serum; PC, prospective cohort; RBC, red blood cell; RCT, randomised controlled trial.
One study assessing P/S folate also assessed RBC.
3.4.4.1. Intervention studies
LoE1. Standalone main: incidence of prostate cancer
Preliminary UA
One eligible RCT, i.e. the AFPPS, was identified (Figueiredo et al., 2009) (Appendix C.3.1). The design of the trial has been described above (Section 3.4.3.1). Participants were randomised to 1000 μg folic acid/day (with or without aspirin) or a placebo (with or without aspirin) for 3 years (first follow‐up). Then, 71.4% of participants voluntarily continued the folic acid/placebo intervention for an additional 3–5 years. While on treatment, medical events, including illnesses and hospitalisations, were reported by participants through a questionnaire sent every 4 months. Cancer cases were centrally adjudicated based on medical records and diagnosis was confirmed by histopathology. A total of 643 males were included in the analysis (N = 316 in control group and N = 327 in folic acid group). The mean Gleason score (available for all subjects) was 6.4 (SD = 1.1) and did not differ between treatment groups. Information on the clinical stage was not available for all cases. A total of 25 cases (9.7%) of prostate cancer were reported in the folic acid group versus 9 (3.3%) in the control group during follow‐up (median [IQR] follow‐up duration: 7 [6–7.8] years). The HRs were 2.63 (95% CI 1.23, 5.65) after adjustment for age, and 2.58 (1.14, 5.86) after further adjustment for aspirin treatment group, alcohol use, baseline multivitamin use and baseline plasma levels of vitamins B2, B6 and cobalamin. The study was judged at low risk of bias (tier 1) (Appendix B.3.1). When including the additional cases identified during the post‐trial surveillance period which followed the termination of the study, a total of 35 men (11%) in the folic acid group developed prostate cancer compared with 22 men (7%) in the control group (Passarelli et al., 2019).
The Panel notes that the BoE is limited to one intervention study in which prostate cancer was recorded among potential adverse events.
The Panel considers that the available BoE from intervention studies is insufficient to conclude on a positive and causal relationship between dietary intake of folate and risk of prostate cancer. The Panel notes that the available evidence is on folic acid. No comprehensive UA is performed.
3.4.4.2. Observational prospective studies
LoE1. Standalone main: incidence of prostate cancer
Preliminary UA
P/S and RBC folate
Among the seven studies which assessed P/S folate, two were PCs (Essén et al., 2019; Rossi et al., 2006) and five were NCCs (Beilby et al., 2010; de Vogel et al., 2013; Hultdin et al., 2005; Johansson et al., 2008; Weinstein et al., 2003). All investigated incident prostate cancer. The size of the PCs ranged between 964 and 8783 participants and of the NCCs between 306 and 6000 participants. The length of follow‐up ranged from 4.9 years (Hultdin et al., 2005) to 23 years (Rossi et al., 2006). In two studies the duration was not reported (de Vogel et al., 2013; Weinstein et al., 2003). The studies were based in Europe (n = 5) and Australia (n = 2).
Three studies were at low risk of bias (tier 1) and four studies at moderate risk of bias (tier 2) (Appendix B.3.2).
The evidence table is in Appendix C.3.2.a. Key study characteristics, together with the risk estimates and related 95% CIs, are plotted in Figure 15.
FIGURE 15.
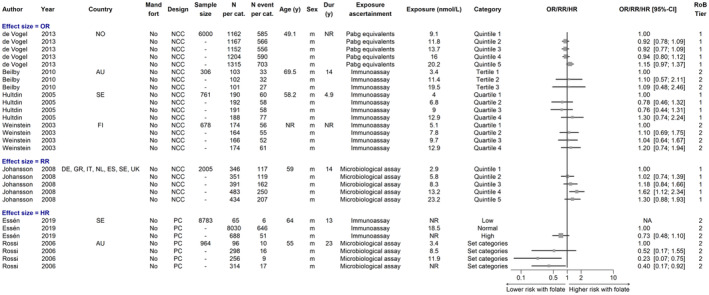
Observational studies on plasma/serum folate and incident prostate cancer, most adjusted RRs from PCs and NCCs. Exposure values, age and duration correspond to the mean/median of each category; mandatory fort, yes/no: reflects policy status at baseline; Hultdin et al. assessed plasma; Johansson et al. assessed both plasma and serum; Rossi et al. presented values with the highest category as reference, which was converted. AU, Australia; DE, Germany; ES, Spain; FI, Finland; GR, Greece; IT, Italy; NL, The Netherlands; NO, Norway; SE, Sweden; UK, United Kingdom; pc, prospective cohort; ncc, nested case–control study; pcc, case cohort study; Dur, duration; Mand fort, mandatory fortification; n per cat, number of participants per category; n event per cat, number of events per category; NA, not applicable.
Five studies found no association between P/S folate and risk of prostate cancer (Beilby et al., 2010; de Vogel et al., 2013; Essén et al., 2019; Hultdin et al., 2005; Weinstein et al., 2003), while one study found an inverse association (Rossi et al., 2006) and one suggested a positive association in the highest quartiles of plasma folate (Johansson et al., 2008) (Figure 15). None of the studies included participants in settings with mandatory folate fortification. The mean/median P/S folate in the top categories were between 13 and 23 nmol/L.
In the only study which assessed RBC folate in addition to P/S folate, no association was found (Rossi et al., 2006) (Appendix C.3.2.a).
The Panel considers that the BoE does not suggest a positive relationship between P/S folate or RBC folate and risk of prostate cancer.
Dietary intake of folate/folic acid
A total of seven studies investigated the relationship between dietary folate/folic acid and prostate cancer risk. The study by (Tomaszewski et al., 2014) is not further discussed as it compared the risk of recurrent prostate cancer in subjects in the lowest decile of folate intake compared to the combined 2nd to 10th deciles (taken as reference category), thus providing no relevant data for this assessment.
The exposure was assessed as total folate intake (n = 3), folate intake from natural sources and fortified foods (i.e. excluding intake from food supplements; n = 1), natural folate intake (n = 4) and supplemental folic acid intake (n = 1). Some studies reported on several exposure variables.
Studies addressing natural folate intake provide no relevant information for the present evaluation (Åkesson et al., 2023), and are thus not further discussed below.
Total folate intake
Three PCs studies investigated the relationship between total folate intake and incidence of prostate cancer (Roswall et al., 2013; Stevens et al., 2006; Weinstein et al., 2006). The studies included between 26,856 and 65,836 participants. The length of follow‐up ranged from 5 years (Weinstein et al., 2006) to 14.3 years (median value; [Roswall et al., 2013]). The cohorts were based in Europe (n = 2) and the USA (n = 1).
FFQs were used to assess total folate intake in all studies. The median/mean total folate intake in the lowest categories of intake were between 179 μg/day and 254 μg/day and in the highest categories of intake between 415 μg/day and 910 μg/day.
One study was at low risk of bias (tier 1) and two studies at moderate risk of bias (tier 2) (Appendix B.3.2).
The evidence table is in Appendix C.3.2.b. Key study characteristics, together with the risk estimates and related CIs, are plotted in Figure 16.
FIGURE 16.
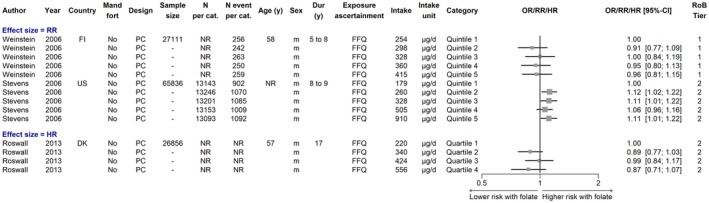
Total folate intake and incident prostate cancer, most adjusted RRs from PCs. Intake values, age and duration correspond to the mean/median of each category; mandatory fort, yes/no: reflects policy status at baseline. DK, Denmark; FI, Finland; US, United States; pc, prospective cohort; Dur, duration; Mand fort, mandatory fortification; n per cat, number of participants per category; n event per cat, number of events per category.
Of the three studies which investigated the relationship between total folate intake and incident prostate cancer, two reported null associations and one reported a higher risk of prostate cancer in all quartiles of intake compared to the lowest quartile, with no indication of a dose–response (Stevens et al., 2006) (Figure 16).
The Panel considers that the BoE does not suggest a positive relationship between total folate intake and risk of prostate cancer.
Folate intake from natural sources and fortified foods
Stevens et al. (2006) also analysed the association between folate intake from natural sources and fortified foods and risk of prostate cancer. Taking the lowest quintile of intake as referent category (<204 μg/day), the RR in the 5th quintile (≥ 347 μg/day) was 1.03 (95% CI 0.94, 1.13), with similar RRs in the other quintiles (Appendix C.3.2.b). The study was judged at moderate risk of bias (tier 2) (Appendix B.3.2).
Folic acid intake
Roswall et al. (2013) also investigated the relationship between supplemental intake of folic acid and prostate cancer risk (Appendix C.3.2.b). This PC study included 26,856 participants, had a median follow‐up of 14.3 years, and was conducted in Denmark. Supplement use was assessed through open‐ended questions on brands, doses and consumption frequency. The median (5‐95th percentiles) supplemental folic acid intakes, among users, were 100 (11.9–250) μg/day. The HRs for the 4th quartile (>133.2 μg/day supplemental folic acid intake) versus 1st quartile (no supplemental folic acid intake) was 0.93 (95% CI 0.73, 1.17). The study was judged at moderate risk of bias (tier 2).
Conclusion
The Panel considers that the available BoE from observational studies does not suggest a positive relationship between dietary folate intake and the risk of prostate cancer over the range of exposures investigated in these studies. No comprehensive UA is performed.
3.4.4.3. Animal data
Male mice of the transgenic adenoma of the mouse prostate (TRAMP) model, which spontaneously develops prostate tumours following the onset of puberty, were randomised to a folate adequate diet (2000 μg/kg diet), a folate‐deficient diet (300 μg/kg diet) and a folic acid‐supplemented diet (20,000 μg/kg diet) between 3 and 22 weeks of age (Bistulfi et al., 2011). No effect of the ‘high’ folic acid diet compared to the folate‐adequate diet was found on the development of prostate cancer.
In a further experiment in male mice, the CWR22 human xenograft model was used to investigate the effect of dietary folate on prostate cancer recurrence (Affronti et al., 2017). Engrafted mice were fed a folate‐adequate diet (2000 μg/kg diet), a folate deficient diet (200 μg/kg diet) and a folic acid‐supplemented diet (20,000 μg/kg diet), beginning at androgen withdrawal or prior to xenograft injection. Under both conditions, the percent of animals with prostate cancer recurrence was lower in the group fed the folic acid‐supplemented diet compared to the group receiving folate adequate diet.
The Panel considers that evidence from animal experiments is limited and does not support an adverse effect of ‘high’ folate intake on the risk of prostate cancer.
3.4.4.4. Mode of action
As discussed in relation to CRC (Section 3.4.3.4), the Panel notes that the fundamental role of folate in one‐carbon metabolism provides several potential pathways by which folate might affect cancer development. These are intricate pathways, subject to complex modulatory mechanisms and potentially affected by numerous factors (e.g. nutrition, environment, genetics). Further research is required to better understand the biological processes involved in prostate cancer development and how they might be affected by the folate body pool.
3.4.4.5. Overall conclusions on prostate cancer
The Panel considers that the available BoE is insufficient to conclude on a positive and causal relationship between high dietary intake of folate and risk of prostate cancer.
3.4.5. Risk of cancer at other sites
At the time of protocol development for the assessment, colorectal cancer and prostate cancer were identified to provide the strongest available evidence for a relationship between folate and risk of cancer (Annex A) (Maruvada et al., 2020; National Toxicology Program, 2015). Thus, these two sites were prioritised and no systematic reviews have been conducted on the risk of cancer occurring at other sites. Instead, a narrative overview of the evidence, based on recent systematic reviews and meta‐analyses, is provided below.
3.4.5.1. Randomised controlled trials
Several systematic reviews have assessed the evidence from RCTs on the effect of folate supplementation on overall and site‐specific cancer incidence or mortality (Qin et al., 2013; Vollset et al., 2013; Wien et al., 2012).
A total of 15 individual RCTs, published between 2004 and 2014, were identified across these reviews, of which 12 were designed for the prevention of cardiovascular disease (CVD) and three for the prevention of colorectal adenomas. Fourteen trials used folic acid with daily doses ranging between 500 and 50,000 μg and one trial used MTHF at a dose of 560 μg per day. Trial durations ranged between 2 and 8 years. All of the CVD trials used supplemental folate in combination with other nutrients (i.e. cobalamin [n = 2]; cobalamin and vitamin B6 [n = 9]; cobalamin and vitamin B6 and fatty acids [n = 1]).
The meta‐analyses by Qin et al. (2013), Vollset et al. (2013) and Wien et al. (2012) combined largely overlapping bodies of evidence (Appendix E). However, Qin et al. (2013) and Wien et al. (2012) conducted meta‐analyses of summary estimates of individual trials, while Vollset et al. (2013) used individual data collected through the B‐Vitamin Treatment Trialists' Collaboration. Pooled RRs for overall cancer risk were similar: the pooled RRs were 1.06 (95% CI 0.99, 1.13) based on 13 studies, 1.05 (95% CI 0.99, 1.11) based on 13 studies and 1.07 (95% CI 1.00, 1.14) based on 10 studies in the respective analyses of Vollset et al. (2013), Qin et al. (2013) and Wien et al. (2012). With respect to total cancer mortality, pooled RRs of 1.02 (95% CI 0.90, 1.15) based on six trials and 1.09 (95% CI 0.92, 1.30) based on five studies (561/15,408 vs. 573/16,919) were estimated by Wien et al. and Qin et al., respectively.
The most recent review by O'Connor et al. (2021) had a narrower scope, i.e. was restricted to trials using folic acid alone or in combination with cobalamin; also, it excluded trials using doses above the current UL or which involved % individuals with active/current CVD, diabetes mellitus or cancer. As compared to the previous reviews, one additional trial, the B‐Vitamins for the Prevention Of Osteoporotic Fractures (B‐PROOF), published in 2014, was identified. Three trials (AFPPS, NHS/HPPS and B‐PROOF) were eligible for the meta‐analysis on total cancer incidence, with a pooled RR of 1.42 (95% CI 1.10, 1.84).
Regarding site‐specific cancers (other than prostate and CRC which were discussed above), no evidence was found for an increased risk of cancer at any site in the folic acid groups compared to the control groups, in any of the reviews (O'Connor et al., 2021; Qin et al., 2013; Vollset et al., 2013; Wien et al., 2012). The number of cases for each cancer type were limited.
The Panel notes that the majority of the trials used supplemental folate in combination with other nutrients (i.e. B‐vitamins) and concomitant effects cannot be excluded. Only three trials used folic acid alone, i.e. the AFPPS, NHS/HPPS and UkCAP trials. These trials, which are discussed above with respect to prostate cancer and colorectal cancer (Section 3.4.3), did not report increased cancer risk at other sites (Cole et al., 2007; Logan et al., 2008; Passarelli et al., 2019; Wu et al., 2009).
3.4.5.2. Evidence from observational prospective studies
A number of systematic reviews and meta‐analyses have also reviewed observational studies which investigated the association between dietary folate intake (using P/S folate as biomarker of intake or estimated through dietary assessment methods) and incidence of cancer at specific sites, i.e. pancreatic cancer, oesophageal cancer, gastric cancer, breast cancer, lung cancer, ovarian cancer, endometrial cancer, urothelial cancer and skin cancers. The most recent systematic reviews and meta‐analyses of observational studies of prospective design (i.e. PCs or NCCs), as well as pooled analyses, are tabulated in Appendix F.
Most of the individual studies included in these reviews reported null or negative associations, while the direction of the association with folate/folic acid intake or folate status was positive in some studies addressing pancreatic cancer (2 out of 10 studies [Keszei et al., 2009; Schernhammer et al., 2007]), breast cancer (1 out of 21 studies, (Kim et al., 2016), lung cancer (1 out of 9 studies, Kabat et al., 2008), endometrial cancer (1 out of 5 studies, Uccella et al., 2011), urothelial carcinoma (2 out of 10 studies, Bassett et al., 2019; Michaud et al., 2002), basal cell carcinoma (2 out of 2 studies, van Dam et al., 2000; Fung et al, 2002) and overall skin cancer risk (1 out of 1 study, Donnenfeld et al., 2015) (Appendix F). The Panel notes the imprecision of the risk estimates in these studies (low number of cases). The Panel also notes that, in all studies, individuals included in the referent categories had folate intake or plasma/serum concentrations indicative of an inadequate intake/status.
The Panel notes that evidence for a positive relationship between ‘high’ folate/folic acid intake or folate status and risk of cancer at these sites is scarce. Further investigation of the relationship between high folate intake and the risk of cancer is needed.
3.4.6. Other adverse health effects
3.4.6.1. Risk of insulin resistance
In a systematic review of human studies and animal experiments which investigated the effect of maternal folate/folic acid intake during pregnancy on the risk of insulin resistance in offspring, Xie et al. (2016) retrieved one RCT, two PCs and four studies in rodents. The RCT involved Nepalese women who received supplementation with folic acid (400 μg/day, alone or in combination with other nutrients) during pregnancy (Stewart et al., 2009). No effect of folic acid supplementation or maternal folate status during pregnancy were found on homeostasis model assessment‐estimated insulin resistance (HOMA‐IR) measured in their children at ages 6–8 years. In a sub‐group analysis, an increased HOMA‐IR was found in children born to mothers with cobalamin concentration below 148 pmol/L during pregnancy as compared with those children born to mothers with cobalamin concentration above this threshold, while no association between maternal folate status and HOMA‐IR was observed (Stewart et al., 2011). In two PCs in India, higher RBC folate concentration at 28 weeks of gestation was positively associated with HOMA‐IR in the offspring at age of 6 years (Yajnik et al., 2008), while no association was found between maternal plasma folate and this outcome when measured in their children at 5 years of age and a positive association was reported when assessed at 9 years of age (Krishnaveni et al., 2014). Data from animal experiments were inconsistent (Cho et al., 2013; Hoile et al., 2012; Huang et al., 2014; Sinclair et al., 2007).
In a RCT among children with overweight or obesity, supplemental folic acid in doses up to 5000 μg/day for 8 weeks was reported to decrease insulin resistance, measured using HOMA‐IR (Dehkordi et al., 2016).
The Panel notes that evidence on the association between folate/folic acid intake and risk of insulin resistance is limited and inconsistent.
The Panel considers that the available evidence on the relationship between dietary intake of folate intake and risk of insulin resistance cannot be used for establishing a UL for folate.
3.4.6.2. Impaired immune function
In a cross‐sectional analysis among US women, reduced nature killer (NK) cytotoxicity was observed among those who consumed folic acid supplements >400 μg/day in addition to a diet supplying >233 μg/day, compared to those who did not consume supplements or lower supplemental doses (Troen et al., 2006). Lower NK cytotoxicity was found among women in the top tertile of UFA concentration (>3 nmol/L) vs. bottom tertile (<1.7 nmol/L). Paniz et al. (2017) reported a reduction in absolute NK cell count and their cytotoxicity capacity in Brazilian adults supplemented with 5000 μg folic acid per day for 90 days. The Panel notes that this trial was uncontrolled.
In mice experiments, reduced survival to infection, decreased numbers of splenocytes, total T cells and specific T and NK cells, and lower NK cell cytotoxicity have been found in animals fed high folic acid diet (10–20 times the basal folate requirement) compared to the those on control diet (Meadows et al., 2015; Sawaengsri et al., 2016).
The Panel notes that evidence on an effect of folate/folic acid intake on immune function is limited.
The Panel considers that the available evidence on the relationship between folate intake and impairment of immune function cannot be used for establishing a UL for folate.
3.4.6.3. Risk of allergies
Crider et al. (2013) conducted a systematic review of the association of folate and folic acid intake during pregnancy and risk of asthma and other allergic outcomes in children. A total of 12 prospective observational studies were identified (published until 2012) (Dunstan et al., 2012; Granell et al., 2008; Haberg et al., 2009, 2011; Kiefte‐de Jong et al., 2012; Litonjua et al., 2006; Magdelijns et al., 2011; Martinussen et al., 2012; Miyake et al., 2011; Nwaru et al., 2011; Triche et al., 2011; Whitrow et al., 2009). In a more recent systematic review, Chen, Xing, et al. (2021) identified seven additional prospective observational studies (published between 2013 and 2019) (den Dekker et al., 2018; Molloy et al., 2020; Parr et al., 2017; Roy et al., 2018; Trivedi et al., 2018; Veeranki et al., 2015; Zetstra‐van der Woude et al., 2014). There is substantial heterogeneity across studies in the folate exposure measures (i.e. folic acid supplements, dietary folate, total folate from diet and supplements, blood folate concentrations [maternal red blood cell, maternal plasma and cord blood]), the timing of exposure assessment (e.g. pre‐pregnancy, different stages of pregnancy, at delivery), the allergic outcomes assessed and the age of children at the time of assessment.
Among seven studies which examined the effect of maternal folic acid supplement use compared with no use in the periconceptional period or first trimester on risk of asthma or wheezing in childhood, one reported an increased risk of wheezing associated with folic acid supplementation taken in late pregnancy (median dose 300 μg/day), but not when taken in early pregnancy, among Australian women (Veeranki et al., 2015; Whitrow et al., 2009) and another reported an increased risk of asthma associated with folic acid supplementation in both early and late pregnancy (dose of 1000 μg/day in most cases) among US women (Veeranki et al., 2015); the other five studies found no association (Haberg et al., 2009; Kiefte‐de Jong et al., 2012; Magdelijns et al., 2011; Martinussen et al., 2012; Trivedi et al., 2018). No increased risk of asthma or wheezing was reported among the six studies which examined the association with other folate exposure variable (i.e. dietary folate or blood folate measurements) measured in the first trimester (den Dekker et al., 2018; Kiefte‐de Jong et al., 2012; Litonjua et al., 2006; Martinussen et al., 2012; Triche et al., 2011; Whitrow et al., 2009). No increased risk of asthma or wheezing in childhood was found in the three studies which examined the effect of maternal folic acid supplement use compared with no use (Kiefte‐de Jong et al., 2012; Veeranki et al., 2015; Whitrow et al., 2009), and the seven studies which used other folate exposure variables, in the second and third trimester (Haberg et al., 2009, 2011; Magdelijns et al., 2011; Miyake et al., 2011; Nwaru et al., 2011; Roy et al., 2018; Trivedi et al., 2018). Finally, among five studies which investigated the association between folic acid supplement use, total folate intake or plasma folate throughout pregnancy, one reported an increase in the risk of wheezing with the use of folic acid supplement (Whitrow et al., 2009), one reported an increased risk of asthma with total folate intake (Parr et al., 2017), while no association with asthma and/or wheezing was found in the other three studies (Granell et al., 2008; Haberg et al., 2009; Zetstra‐van der Woude et al., 2014).
Among five studies, which investigated folic acid supplement use compared with no use or other folate exposure variables in the periconceptional period or first trimester and risk of other allergic outcomes (i.e. atopy, eczema and atopic dermatitis), no association was found (Dunstan et al., 2012; Haberg et al., 2009; Litonjua et al., 2006; Martinussen et al., 2012; Molloy et al., 2020), except for a higher risk of atopic dermatitis in children of mothers belonging to the top quartile of plasma folate versus bottom quartile (Martinussen et al., 2012). Among five studies, which investigated folic acid supplement use compared with no use or other folate exposure variables in the second and third trimester, and three studies, which investigated folic acid supplement use compared with no use or other folate exposure variables throughout pregnancy, no association was found with the risk of other allergic outcomes (Dunstan et al., 2012; Granell et al., 2008; Haberg et al., 2009, 2011; Kiefte‐de Jong et al., 2012; Nwaru et al., 2011; Roy et al., 2018).
In a cohort of infants at hereditary risk of allergic disease in Australia, no association was found between maternal serum folate or UFA concentrations (detectable at 93% of samples, median 1.6 nmol/L, IQR 0.6–4.7 nmol/L, min‐max 0.03–244.7 nmol/L) assessed in late pregnancy and allergic disease outcomes at 1 year of age (Best et al., 2021).
The Panel notes that most of the studies investigated the risk of asthma or wheezing, while studies on other allergic outcomes are limited. Evidence for a positive relationship between maternal folate/folic acid intake or folate status pre‐ and during pregnancy and risk of allergies is scarce; most studies reported no association between maternal intake of folate/folic acid pre‐ or during pregnancy and risk of allergies in offspring.
The Panel considers that the available evidence on the relationship between folate intake and risk of allergies cannot be used for establishing a UL for folate.
3.4.6.4. Risk of autism/autism spectrum disorder
A systematic review and meta‐analysis which included six prospective observational studies reported that folic acid intake supplements before and during pregnancy (at different time periods) was associated with a lower risk of autism spectrum disorder in the offspring (OR 0.51, 95% CI 0.37, 0.69; I 2 = 78.9%) (Liu et al., 2022). Similar results were also reported in another systematic review and meta‐analysis (Chen, Qin, et al., 2021), which investigated the association between maternal folic acid supplementation and the risk of autistic traits in the offspring. An inverse association was found when pooling results of eight eligible prospective observational studies (OR fixed effects model 0.81; 95% CI 0.78, 0.95, OR random effects model 0.69; 95% CI 0.51, 0.93; I 2 = 92%). Out of the 10 individual prospective observational studies identified by these reviews (Chen et al., 2014; DeVilbiss et al., 2017; Jiang et al., 2016; Levine et al., 2018; Nilsen et al., 2013; Schmidt et al., 2019; Strøm et al., 2018; Sun et al., 2016; Surén et al., 2013; Virk et al., 2016), all reported a protective effect of folic acid supplementation during pregnancy, except one which reported an increased risk of autism spectrum disorder among children of mothers who used folic acid supplementation in early pregnancy compared with no use (dose not reported) (DeVilbiss et al., 2017). All studies compared the risk among women who took folic acid supplements vs. not, without categorising the doses, except in the study by (Schmidt et al., 2019), which categorised individuals into tertiles of folic acid doses (T1: 0–57 μg/day, T2: 80–800 μg/day, T3: 805–4800 μg/day) and reported RRT2 vs. T1 of 0.63 (95% CI 0.40–0.98) and RRT3 vs. T1 of 0.42 (95% CI 0.17–0.99).
A few studies used cord/maternal plasma folate concentrations as a measure of folate exposure. (Raghavan et al., 2018) investigated the relationship between the use of multivitamin supplements and the risk of ASD among mother–child pairs attending the Boston Medical Center in the US. Moderate use of multivitamin supplements (three to five times/week) during pregnancy was associated with a decreased risk of ASD, while high maternal plasma folate (≥60.3 nmol/L; measured in samples collected 24–72 h after delivery) was associated with higher risk of ASD in their infants (HR 2.5; 95% CI 1.3, 4.6; n = 125), compared to lower maternal post‐delivery concentrations (>14.7 to <60.3 nmol/L; n = 1007). In a subsequent publication on a subsample of the same cohort (n = 567), Raghavan et al. (2020) found no association between cord blood total folate or 5‐MTHF concentrations and risk of ASD; a positive association between cord UFA concentration and risk of ASD, restricted to Black children, was reported. In a retrospective case–control study (100 women with an offspring diagnosed with ASD and 100 matched control women from Sweden), Egorova et al. (2020) assessed the association between 62 serum biomarkers and risk of ASD. Early pregnancy folate concentrations (collected during the first or second trimester) were associated with an increased risk of having an offspring with ASD (ORper 1 SD 1.70; 95% CI 1.22, 2.37) (Egorova et al., 2020). Taking multiple testing into account, weak evidence remained (FDR adjusted p = 0.07).
The Panel notes that evidence for a positive relationship between maternal folate/folic acid intake or folate status pre‐ and during pregnancy and risk of autism/autism spectrum disorder is scarce; most prospective observational studies reported a protective association between maternal folic acid intake pre‐ and during pregnancy and risk of autism/autism spectrum disorder in offspring.
The Panel considers that the available evidence on the relationship between folate intake and autism/autism spectrum disorder cannot be used for establishing a UL for folate.
3.4.6.5. Risk of anaemia
In a cross‐sectional analysis among older adults with a low cobalamin status (defined as serum cobalamin concentration < 148 pmol/L) from the 1999 to 2002 US National Health and Nutrition Examination Survey, Morris et al. (2007) reported that serum total folate >59 nmol/L vs. ≤59 nmol/L, was associated with a higher risk of anaemia (defined as a haemoglobin concentration <120 g/L in women or <130 g/L in men) (OR: 3.1; 95% CI: 1.5, 6.6). In a further cross‐sectional analysis using data from the same survey, Morris et al. (2010) reported that higher serum 5‐MTHF was associated with an increased risk of anaemia (defined as above) (OR 1.01, 95% CI 1.0, 1.02). Presence of detectable UFA in serum was associated with increased risk of anaemia among alcohol users (OR: 3.37, 95% CI 1.42, 8.01), but not among nonusers (OR: 0.77, 95% CI 0.41, 1.45). No association was found between 5‐MTHF or UFA and risk of macrocytosis (defined as mean cell volume ≥99 fL).
In a cross‐sectional study among older people with low cobalamin status (defined as holotranscobalamin <45 pmol/L) in the UK, no evidence for a modification by ‘high’ folate status (defined either as serum folate >30 nmol/L or >60 nmol/L) of the associations of low cobalamin with anaemia (defined as Hb level <110 g/L in women and <120 g/L in men) was found (Clarke et al., 2008).
The Panel notes that severe cobalamin deficiency leads to increased risk of anaemia and is also associated with high plasma/serum folate concentrations because of the metabolic interactions between these vitamins (Section 3.2.5.4). The Panel notes that the available evidence is limited to a few cross‐sectional studies, with inconsistent results.
The Panel considers that the available evidence on the relationship between folate intake and risk of anaemia cannot be used for establishing a UL for folate.
3.5. Hazard characterisation
3.5.1. Selection of a critical effect
The Panel systematically reviewed the available evidence on a relationship between high dietary intake of folate and risk of cognitive decline, prostate cancer and CRC:
The Panel considers that the available BoE is insufficient to conclude on a positive and causal relationship between dietary intake of folate and impaired cognitive function in individuals with low cobalamin status.
The Panel considers that the available BoE is insufficient to conclude on a positive and causal relationship between dietary intake of folate and CRC risk.
The Panel considers that the available BoE is insufficient to conclude on a positive and causal relationship between dietary intake of folate and risk of prostate cancer.
Since the previous assessment by the SCF, no new evidence has emerged to support a causal role of folic acid in the exacerbation of the neurological manifestations of cobalamin deficiency. Because of their uncontrolled design, case studies cannot reliably investigate any exacerbation of neurological manifestations due to folic acid intake. The Panel considers that, based on the available BoE, there is low level of certainty for a positive and causal relationship between dietary intake of folic acid and exacerbation of the neurological manifestations of cobalamin deficiency (15%–50% probability).
On the other hand, there is a well‐established relationship between the dietary intake of folic acid and a (transient) correction of megaloblastic anaemia in cobalamin deficient individuals, which could lead to masking of cobalamin deficiency. Early diagnosis and treatment of cobalamin deficiency is critical, as patients with severe/prolonged neurological symptoms tend to have persistent symptoms despite treatment. Cobalamin deficiency (due to PA or other more common causes e.g. hypochlorhydria, low cobalamin diets) is frequent in EU populations, and the prevalence of these conditions is likely to be underdiagnosed due to the limitations in available diagnostic tests (Bizzaro & Antico, 2014; Green et al., 2017; Harrington, 2017).
In line with the SCF, the Panel considers that the risk of progression of cobalamin‐dependent neurological symptoms in cobalamin‐deficient patients should be considered the most serious adverse effect of ‘high’ folic acid intake and used as the critical effect to establish an UL for folic acid. No new evidence has been published that could improve the characterisation of the dose–response between the intake of folic acid and resolution of megaloblastic anaemia in cobalamin deficient individuals.
3.5.2. Derivation of a tolerable upper intake level
The SCF did not set an UL for natural folate because no adverse effect was found from background intakes of folates (SCF, 2000). At that time, synthetic forms of reduced folates were not available for addition to food or use in food supplements.
The SCF considered that ‘an upper safe level can be set for (synthetic) folic acid on the basis of findings in PA patients treated with high doses of folic acid’. The committee concluded that dosages up to 1000 μg of folic acid ‘are unlikely to cause masking of the haematological signs in PA patients’. The UL was set at 1000 μg of folic acid for adults (SCF, 2000).
Considering the totality of the available evidence and related uncertainties (Section 3.4), the Panel found no basis to change this conclusion. The Panel retains the UL previously established by the SCF of 1000 μg folic acid/day for adults.
On the consideration that the data available did not suggest that other life‐stage groups have increased susceptibility to adverse effects of high folic acid intake compared to adults, the SCF considered the UL for adults to be also applicable to pregnant or lactating women and adjusted the ULs for children and adolescents aged 1–17 years on the basis of bodyweight (isometric scaling). In the absence of new data on these other life stages, the previously established ULs for folic acid are also maintained for all population groups (Table 12).
TABLE 12.
ULs for supplemental folate a from fortified foods and food supplements, for all population groups.
| Age group | UL males and females (μg/day) |
|---|---|
| 4–6 months | 200 |
| 7–11 months | 200 |
| 1–3 years | 200 |
| 4–6 years | 300 |
| 7–10 years | 400 |
| 11–14 years | 600 |
| 15–17 years | 800 |
| Adults | 1000 |
| Pregnant women | 1000 |
| Lactating women | 1000 |
Abbreviation: UL: tolerable upper intake level.
Folic acid, 5‐MTHF‐glucosamine and l‐5‐MTHF‐Ca.
There are no data to support a derivation of an UL for infants. On the other hand, there is no indication from the literature that infants may be more susceptible than adults to folate toxicity. In selecting the scaling approach for the extrapolation of UL of adults to infants aged 4–6 months (EFSA NDA Panel, 2022b), the Panel considered that:
mean/median folate concentration of mature breast milk is reported to be in the range of 45–99 μg/L, with an approximate average of 80 μg/L (EFSA NDA Panel, 2014)
applying isometric scaling 32 for the derivation of the UL for infants aged 4–6 months based on the UL for adults would result in a value of ca. 100 μg/day for the combined intake of folic acid and other forms of folates, which is in the order of estimated folate intake from breast milk.
infant formula is the sole source of nutrition for exclusively formula fed infants and most folate in infant formulae is in the form of added folate (i.e. typically folic acid) (Campos‐Giménez et al., 2018).
Thus, the Panel considered isometric scaling to be an overconservative approach for this age group. Instead, allometric scaling was considered to be sufficiently conservative, in view of the physiological requirement for folate at that age. The following equation was applied:
This results in an UL of 200 μg/day for this age group. The value is rounded to the closest 0.1 mg.
For infants aged 7–11 months, a UL of 200 μg/day is established by interpolation of the ULs for infants aged 4–6 months and for young children aged 1–3 years.
TABLE 11 UL for infants aged 4–11 months.
| Age range | Reference bw males and females (kg) a | UL males and females (μg/day) |
|---|---|---|
| 4–6 months | 7.2 | 200 |
| 7–11 months | 8.6 | 200 |
Abbreviations: bw: body weight; UL: tolerable upper intake level.
The averages of the median weights‐for‐age for boys and girls at 5 and 9 months, respectively, were used as reference weights (WHO Multicentre Growth Reference Study Group, 2006)
The safety of 5‐MTHF‐glucosamine for use in food supplements, and of l‐5‐MTHF‐Ca for addition to food and use in food supplements, was previously evaluated by the EFSA AFC and ANS Panels (EFSA AFC Panel, 2004; EFSA ANS Panel, 2013) (Section 1.4). The safety of these folate forms was established under the consideration that the UL of 1000 μg/day for folic acid would apply to the combined intake of folic acid and 5‐MTHF salts. The Panel notes that most of the data available for this risk assessment concern folic acid. The Panel acknowledges that there are differences in ADME of these forms compared to folic acid and that there is no indication that 5‐MTHF salts would correct the haematological manifestations of cobalamin deficiency, thereby increasing the risk of progression of the neurological manifestations of cobalamin deficiency. On the other hand, no new data have been identified regarding 5‐MTHF‐glucosamine or l‐5‐MTHF‐Ca and the Panel considers that no statement can be made about the safety of 5‐MTHF‐glucosamine or l‐5‐MTHF‐Ca above the UL for folic acid. The Panel retains that the proposed UL applies to the combined intake of folic acid and 5‐MTHF salts under their authorised conditions of use.
3.6. Risk characterisation
The ULs are established for the general European population and apply to the combined intake of supplemental folate from currently authorised forms for addition to food and use in food supplements.
Harmonised data on folate intake from all sources, including fortified foods and food supplements, for the European population are currently not available. Data on the intake of folate from fortified foods and food supplements available from national surveys are scarce (Section 3.3.3).
The Panel considers that it is unlikely that the ULs for supplemental folate are exceeded in European populations, except for regular users of food supplements containing high doses of folic acid/5‐MTHF salts (Sections 3.3.1 and 3.3.3).
4. CONCLUSIONS
The following ULs are established for the intake of supplemental folate (i.e. folic acid, 5‐MTHF‐glucosamine and L‐5‐MTHF‐Ca; Table 12) from fortified foods and food supplements:
5. RECOMMENDATIONS FOR RESEARCH
Further research is required regarding all groups of the population to characterise potential critical effects of excess folate intake. This should address potential differences in the toxicity profile of the various forms of folate added to foods and used in food supplements. Also, investigations of the potential vulnerability of specific subgroups of the population, such as infants and children, pregnant women and older adults, is needed, taking into account specific issues in terms of absorption, metabolism, distribution and excretion of various folate forms in these groups.
Further investigation of the relationship between high folate intake and the risk of cancer is needed, including colorectal and prostate cancer. Additional research is needed on the relationship between high folate intake and the risk of SSA/Ps.
Further research is required to clarify the impact of high doses of folic acid and 5‐MTHF on brain structures and functions.
Research is needed to investigate whether the epigenetic changes found in interventions with high doses of folic acid in some populations are causally related to alterations in any phenotypic characteristics. Research is also needed in that respect on the other forms of folate.
Additional research on UFA is required, in particular whether UFA can specifically affect biological pathways leading to adverse health effects.
Data on the consumption of fortified foods and food supplements containing folic acid and/or 5‐MTHF salts in EU populations are scarce. For the risk characterisation, there is a need to generate more and harmonised data on folate intake in its different forms from food supplements and fortified foods among users of those products.
Abbreviations
- 5‐MTHF
(6S)‐5‐methyl‐tetrahydrofolate
- 5‐MTHF‐glucosamine
(6S)‐5‐methyltetrahydrofolic acid glucosamine salt
- ACF
aberrant crypt foci
- ADME
absorption, distribution, metabolism and excretion
- AFC
Panel on food additives, flavourings, processing aids and materials in contact with food
- AFPPS
aspirin/folate polyp prevention study
- AI
adequate intake
- AR
average requirement
- BDR
basal dietary requirement
- BoE
body of evidence
- B‐PROOF
B‐Vitamins for the PRevention Of Osteoporotic Fractures
- bw
body weight
- CF
conversion factor
- CI
confidence interval
- CRC
colorectal cancer
- CSF
cerebrospinal fluid
- CSPPT
China Stroke Primary Prevention Trial
- CVD
cardiovascular disease
- DFE
dietary folate equivalents
- DHF
dihydrofolate
- DHFR
dihydrofolate reductase
- dTMP
deoxythymidine monophosphate
- dUMP
deoxyuridine monophosphate
- FAF
Panel on Food Additives and Flavourings
- FAO
Food and Agriculture Organization
- FCDB
Food composition database
- FDR
false discovery rate
- FFQ
food frequency questionnaire
- FR
folate receptor
- GL
guidance level
- GNPD
Global New Products Database
- HCT
human controlled trial
- HOMA‐IR
homeostasis model assessment‐estimated insulin resistance
- HPFS
health professionals follow‐up study
- HR
hazard ratio
- IOM
Institute of Medicine
- IQR
interquartile range
- ITT
intention‐to‐treat
- l‐5‐MTHF‐Ca
l‐5‐methyltetrahydrofolic acid calcium salt
- LOAEL
lowest observed adverse effect level
- LoE
line of evidence
- MMSE
mini‐mental state examination
- MS
methionine synthase
- MTHFR
methylenetetrahydrofolate reductase
- NANS
National Adult Nutrition Survey
- NCC
nested case–control study
- NDA
Nutrition, Novel Foods and Food Allergens Panel
- NF
natural food folate
- NHMRC
National Health and Medical Research Council
- NHS
Nurses' Health Study
- NOAEL
no‐observed‐adverse effect level
- NR
not reported
- NRV
Nutrient Reference Value
- NTP
US National Toxicology Program
- OHAT
Office of Health Assessment and Translation
- OR
odds ratio
- P/S
plasma/serum
- PA
pernicious anaemia
- PC
prospective cohort study
- PCFT
proton‐coupled folate transporter
- PPS
polyp prevention study
- PPT
polyp prevention trial
- PRI
population reference intake
- RBC
red blood cell
- RCT
randomised controlled trial
- RFC
reduced folate carrier
- RoB
risk of bias
- RP
reference point
- RR
risk ratio
- SACN
UK Scientific Advisory Committee on Nutrition
- SAM
S‐adenosylmethionine
- SCF
Scientific Committee on Food
- SP
serrated polyps
- sQ
sub‐question
- SSA/P
sessile serrated adenomas/polyps
- THF
tetrahydrofolate
- TRAMP
transgenic adenoma of the mouse prostate
- UA
uncertainty analysis
- UF
uncertainty factor
- UFA
unmetabolised folic acid
- UkCAP
United Kingdom Colorectal Adenoma Prevention
- UL
tolerable upper intake levels
- WBF
Wheat bran fibre
- WG
Working Group
- WHO
World Health Organization
CONFLICT OF INTEREST
If you wish to access the declaration of interests of any expert contributing to an EFSA scientific assessment, please contact interestmanagement@efsa.europa.eu.
REQUESTOR
European Commission
QUESTION NUMBER
EFSA‐Q‐2021‐00366
PANEL MEMBERS
Dominique Turck, Torsten Bohn, Jacqueline Castenmiller, Stefaan De Henauw, Karen Ildico Hirsch‐Ernst, Helle Katrine Knutsen, Alexandre Maciuk, Inge Mangelsdorf, Harry J McArdle, Androniki Naska, Kristina Pentieva, Alfonso Siani, Frank Thies, Sophia Tsabouri and Marco Vinceti.
COPYRIGHT FOR NON‐EFSA CONTENT
EFSA may include images or other content for which it does not hold copyright. In such cases, EFSA indicates the copyright holder and users should seek permission to reproduce the content from the original source.
LIST OF ANNEXES
1.
Annex A – Protocol for the Scientific Opinion on the revision of the EFSA's tolerable upper intake level of folate
Annex B – Methodological considerations in the calculation of intake estimates for total folate in European countries
Annex C – EFSA's intake assessment of folate
Annex D – Folate intake data from Competent Authorities in European countries
Annex E – Public consultation on the draft scientific opinion on the tolerable upper intake level for folate
Annexes A–E can be found in the online version of this output (in the ‘Supporting information’ section).
Supporting information
Protocol for the Scientific Opinion on the revision of the EFSA's tolerable upper intake level of folate
Methodological considerations in the calculation of intake estimates for total folate in European countries
EFSA's intake assessment of folate
Folate intake data from Competent Authorities in European countries
Public consultation on the draft scientific opinion on the tolerable upper intake level for folate
ACKNOWLEDGEMENTS
The Panel wishes to thank for their contribution to this output the WG on Upper Levels: Peter Aggett, Brandy Beverly, Torsten Bohn, Julia Bornhorst, Marta Crous‐Bou, Francesco Cubadda, Aymeric Dopter, Susan Fairweather‐Tait, Reginald Fitzgerald, Susan Lanham New, Georg Lietz, Harry J. McArdle, Anne Molloy, Androniki Naska, Giovanni Passeri, Kristina Pentieva, Marco Vinceti and Misha Vrolijk; and EFSA staff members: Irene Muñoz Guajardo, Franco Neri, Roanne Marie Saad and Angeliki Sofroniou. The Panel also wishes to thank Carmen Peláez for her contribution as member of the NDA Panel until June 2023. The Panel acknowledges Agneta Åkesson, Linnea Bärebring, Jacob Juel Christensen, Thomas Olsen, Fredrik Söderlund and Cornelia Witthöft for the preparatory work as part of a procurement procedure. The Panel also wishes to acknowledge the contribution of all national institutions in European countries that provided consumption data for this scientific output and the authors of published papers on folate who provided additional information upon request.
APPENDIX A. LITERATURE SCREENING AND SELECTION – FLOW CHARTS
A.1. Flow chart for the selection of studies on dose–response for serum/plasma‐intake (sQ2)
Figure A.1
FIGURE A.1.
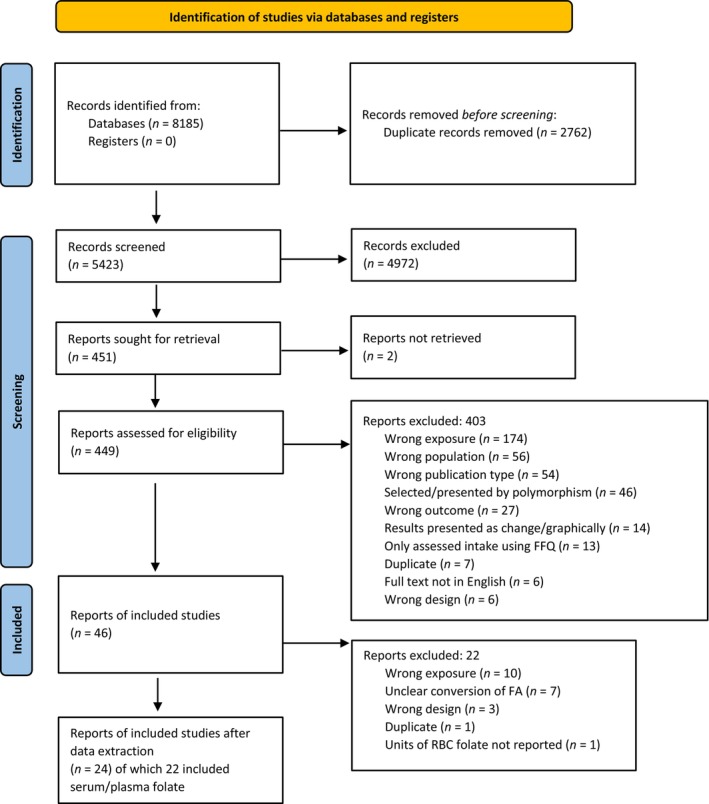
Flow chart for the selection of studies on dose–response for serum/plasma‐intake.
A.2. Flow chart for the selection of studies on cognitive function (sQ3)
Figure A.2
FIGURE A.2.
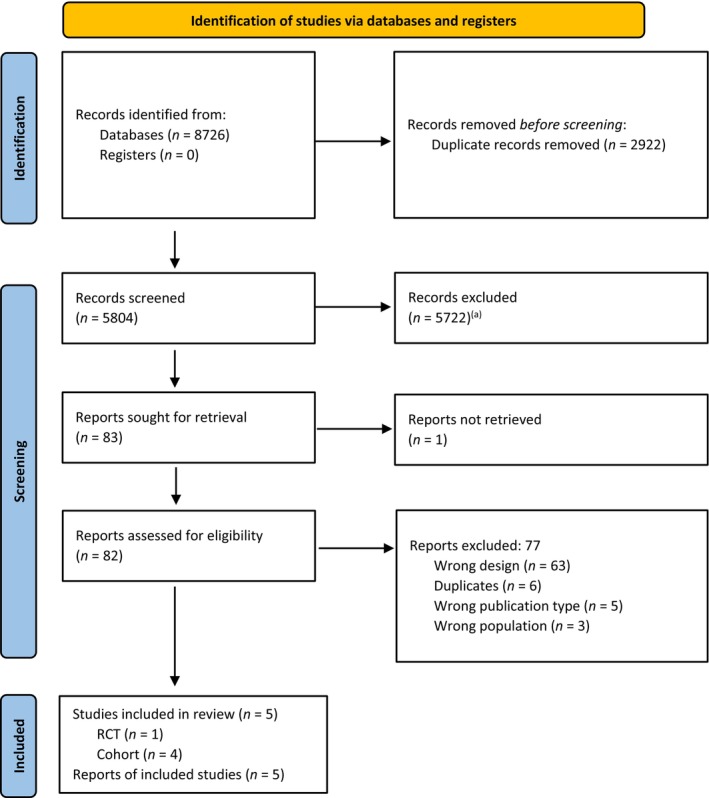
Flow chart for the selection of studies on cognitive function. aThe figures differ from the original flow chart (Åkesson et al., 2023) because, as a result of public consultation on this scientific opinion, the study by Doets et al. (2014), which had been erroneously excluded at the time of title/abstract screening was re‐incorporated in the eligible body of evidence.
A.3. Flow chart for the selection of studies on colorectal and prostate cancer (sQ4b & sQ4c)
Figure A.3
FIGURE A.3.
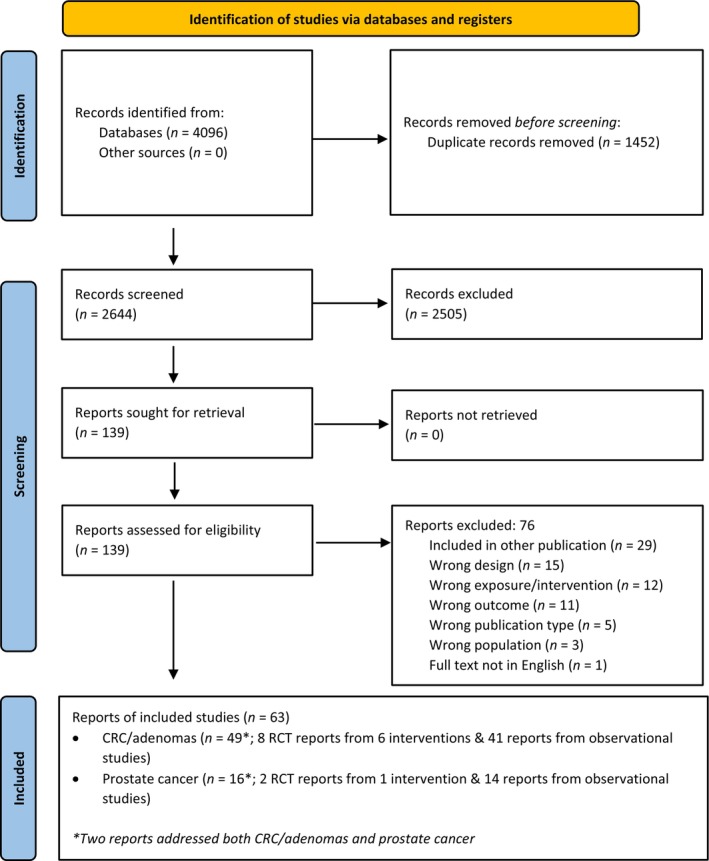
Flow chart for the selection of studies on colorectal cancer and prostate cancer.
APPENDIX B. RISK OF BIAS APPRAISAL
B.1. Cognitive function (sQ3b)
B.1.1. Intervention study
| References | Risk of bias (RoB) domains a | Tier b | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Exposure KEY | Outcome KEY | Randomization KEY | Allocation concealment | Blinding | Attrition | Reporting | Other threats to internal validity | ||
| Durga et al. ( 2007 ) | + | ++ | ++ | ++ | ++ | ++ | + | + | 1 |
Expert judgement was translated into a rating scale for each question to be answered as follows: (++): definitely low RoB; (+): probably low RoB; (NR): not reported; (−): probably high RoB; (− −): definitively high RoB.
The individual rating for each question was combined by an algorithm and translated to an overall tier of reliability for each individual study (RoB tier 1: low RoB; RoB tier 2: moderate RoB; RoB tier 3: high RoB).
B.1.2. Observational studies
| References | Risk of bias (RoB) domains a | Tier b | |||||
|---|---|---|---|---|---|---|---|
| Exposure KEY | Outcome KEY | Confounding KEY | Inappropriate selection | Attrition | Other sources of bias/statistics | ||
| Clarke et al. ( 2007 ) | ++ | ++ | ++ | + | – | + | 1 |
| Morris et al. ( 2012) | + | ++ | ++ | ++ | NR | + | 1 |
| Doets et al. (2014) | + | + | ++ | + | NR | + | 1 |
Expert judgement was translated into a rating scale for each question to be answered as follows: (++): definitely low RoB; (+): probably low RoB; (NR): not reported; (−): probably high RoB; (− −): definitively high RoB.
The individual rating for each question was combined by an algorithm and translated to an overall tier of reliability for each individual study (RoB tier 1: low RoB; RoB tier 2: moderate RoB; RoB tier 3: high RoB).
B.2. Colorectal cancer (sQ4b)
B.2.1. Intervention studies
| References | Risk of bias domains a | Tier b | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Exposure KEY | Outcome KEY | Randomization KEY | Allocation concealment | Blinding | Attrition | Reporting | Other threats to internal validity | ||
| Colorectal cancer | |||||||||
| Qin et al. ( 2017 ) | + | + | + | + | + | + | + | + | 1 |
| Colorectal adenomas | |||||||||
| Cole et al. ( 2007 ) | + | + | ++ | ++ | + | – e | + | NR | 1 |
| Passarelli et al. ( 2019 ) c | + | + | + | ++ | + c | − | + | NR | 1 |
| Logan et al. ( 2008 ) | + | + | ++ | ++ | ++ | + f | + | NR | 1 |
| Wu et al. ( 2009 ) | + | + | ++ | + | ++ | − | + | + | 1 |
| Jaszewski et al. ( 2008 ) | + | + | ++ | ++ | + | NR d | − d | − | 2 |
Abbreviations: ITT, intention‐to‐treat; AFPPS, Aspirin/Folate Polyp Prevention Study (AFPPS); HPFS, Health Professionals Follow‐Up Study; NHS, Nurses' Health Study; NR, Not reported; RoB, risk of bias; ukCAP, the United Kingdom Colorectal Adenoma Prevention.
Expert judgement was translated into a rating scale for each question to be answered as follows: (++): definitely low RoB; (+): probably low RoB; (−): probably high RoB; (− −): definitively high RoB.
The individual rating for each question was combined by an algorithm and translated to an overall tier of reliability for each individual study (RoB tier 1: low RoB; RoB tier 2: moderate RoB; RoB tier 3: high RoB).
The rating differs from the initial appraisal (Åkesson et al., 2023); the Panel noted that the number of participants having a 2nd colonoscopy in the treated vs. control groups was balanced (91% of the participants who accepted to prolong treatment) and that care was taken by the investigators to adjust for factors associated with missing data.
The rating differs from the initial appraisal (Åkesson et al., 2023); the Panel noted that discrepant figures were reported in different places of the publication (e.g. the number of subjects randomised and analysed in the respective arms) and the reporting of the study results was unclear. Due to unclear reporting, attrition in the intervention vs. control groups is unknown, thus a NR is assigned to this domain.
Results for the 2nd follow‐up are appraised.
The rating differs from the initial appraisal (Åkesson et al., 2023); the Panel noted that 91% of the participants initially randomised completed a colonoscopy and the distribution of drop out between groups was even.
B.2.2. Observational studies
| References | Risk of bias (RoB) domains a | Tier b | |||||
|---|---|---|---|---|---|---|---|
| Exposure KEY | Outcome KEY | Confounding KEY | Inappropriate selection | Attrition | Other sources of bias/statistics | ||
| Colorectal cancer | |||||||
| Roswall et al. (2010) | + | ++ | – | + | + | + | 2 |
| Wang, Wu, et al. (2021) | + | + | ++ | + | – | + | 1 |
| Otani et al. (2008) | + | + | + | + | + | + | 1 |
| Stevens et al. (2011) | + | + | – | + | + | + | 2 |
| Zhang et al. (2006) | – (c) | + | – | + | + | + | 2 |
| Rossi et al. (2006) | + | NR | – | + | – | + | 2 |
| Zschäbitz et al. ( 2013) | NR | + | ++ | ++ | NR | + | 2 |
| Glynn et al. ( 1996 ) | + | ++ | – | + | + | + | 2 |
| Lee et al. ( 2012 ) | + | + | – | + | + | + | 2 |
| Flood et al. ( 2002 ) | + | – | – | – | + | + | 2 |
| Lee et al. ( 2011 ) | + | + | – | + | – | + | 2 |
| Razzak et al. ( 2012 ) | – (c) | + | – | + | + | + | 2 |
| Neuhouser et al. ( 2015 ) | + | + | – | – | + | + | 2 |
| Shrubsole et al. ( 2009 ) | + | + | + | + | + | NR | 1 |
| Gibson et al. ( 2011 ) | + | + | ++ | + | + | – | 1 |
| Le Marchand et al. ( 2005 ) | – (c) | + | + | + | + | + | 1 |
| Eussen et al. ( 2010 ) | + | + | ++ | + | ++ | + | 1 |
| Van Guelpen et al. ( 2006 ) | + | ++ | – | + | + | + | 2 |
| Kato et al. ( 1999 ) | + | + | – | + | + | + | 2 |
| Kim et al. ( 2010 ) | – | + | + | + | NR | + | 2 |
| Gylling et al. ( 2014 ) | + | ++ | – | + | + | + | 2 |
| Takata et al. ( 2014 ) | + | + | + | + | + | + | 1 |
| Le Marchand et al. ( 2009 ) | + | + | – | + | + | + | 2 |
| Weinstein et al. ( 2008 ) | + | ++ | – | + | + | + | 2 |
| Cho et al. ( 2015 ) | – c | + | – | + | + | NR | 2 |
| Geijsen et al. ( 2020 ) | + | + | – | + | NR | + | 2 |
| Colorectal Adenomas | |||||||
| Baron et al. ( 1998 ) | + | ++ | – | + | + | + | 2 |
| He et al. ( 2018 ) | + | + | – | + | + | NR | 2 |
| Martínez et al. ( 2004 ) | + | + | – | + | + | NR | 2 |
| Murphy et al. ( 2008 ) | + | + | – | + | NR | NR | 2 |
| Lee et al. ( 2011 ) | + | + | – | + | – | + | 2 |
| Martínez et al. ( 2006 ) | + | + | – | + | + | – | 2 |
Expert judgement was translated into a rating scale for each question to be answered as follows: (++): definitely low RoB; (+): probably low RoB; (NR): not reported; (−): probably high RoB; (− −): definitively high RoB.
The individual rating for each question was combined by an algorithm and translated to an overall tier of reliability for each individual study (RoB tier 1: low RoB; RoB tier 2: moderate RoB; RoB tier 3: high RoB).
The rating differs from the initial appraisal (Åkesson et al., 2023); the Panel noted that, in these studies, exposure was assessed before the introduction of mandatory fortification in the US and a large proportion of the follow‐up period occurred after the introduction of mandatory fortification but change in exposure due to the fortification policy was not addressed in the analysis.
B.3. Prostate cancer (sQ4c)
B.3.1. Intervention studies
| References | Risk of bias (RoB) domains a | Tier b | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Exposaure KEY | Outcome KEY | Randomization KEY | Allocation concealment | Blinding | Attrition | Reporting | Other threats to internal validity | ||
| Figueiredo et al. (2009) | + | + | ++ | ++ | NR | + | + | NR | 1 |
Expert judgement was translated into a rating scale for each question to be answered as follows: (++): definitely low RoB; (+): probably low RoB; (NR): not reported; (−): probably high RoB; (− −): definitively high RoB.
The individual rating for each question was combined by an algorithm and translated to an overall tier of reliability for each individual study (RoB tier 1: low RoB; RoB tier 2: moderate RoB; RoB tier 3: high RoB).
B.3.2. Observational studies
| References | Risk of bias (RoB) domains a | Tier b | |||||
|---|---|---|---|---|---|---|---|
| Exposure KEY | Outcome KEY | Confounding KEY | Inappropriate selection | Attrition | Other sources of bias/statistics | ||
| de Vogel et al. (2013) | + | + | + | + | + | + | 1 |
| Rossi et al. (2006) | + | NR | + | + | – | + | 2 |
| Johansson et al. (2008) | + | + | + | + | + | + | 1 |
| Essén et al. (2019) | + | ++ | ‐ | + | + | + | 2 |
| Hultdin et al. (2005) | + | + | + | + | + | + | 1 |
| Weinstein et al. (2006) | + | ++ | + | + | + | + | 1 |
| Stevens et al. (2006) | + | + | – | + | – | + | 2 |
| Roswall et al. (2013) | – | ++ | + | NR | ++ | + | 2 |
| Beilby et al. (2010) | + | + | – | NR | + | + | 2 |
| Weinstein et al. (2003) | + | ++ | – | NR | NR | + | 2 |
Expert judgement was translated into a rating scale for each question to be answered as follows: (++): definitely low RoB; (+): probably low RoB; (NR): not reported; (−): probably high RoB; (− −): definitively high RoB.
The individual rating for each question was combined by an algorithm and translated to an overall tier of reliability for each individual study (RoB tier 1: low RoB; RoB tier 2: moderate RoB; RoB tier 3: high RoB).
APPENDIX C. EVIDENCE TABLES
C.1. Cognitive function and dementia among individuals with low vitamin cobalamin status (sQ3b)
C.1.1. Intervention study on folic acid supplementation and changes in functional measures of cognitive function
| Reference Study Country Duration Funding | Design | Subject characteristics at baseline | Intervention | Endpoint assessed | Results |
|---|---|---|---|---|---|
|
Durga et al. (2007) FACIT trial The Netherlands 3 years Mixed |
RCT (parallel), double blind Inclusion/exclusion criteria : age 50–70 yrs, men and post‐menopausal women Exclusion: Hcy <13 or >26 μmol/L, cobalamin <200 pmol/L, renal or thyroid disease, medications that influence folate metabolism or atherosclerotic progression, intestinal disease, B‐vitamin users, <80% compliance during first 6 weeks N participants randomised/completed/analysed G1: 406/389/405 G2: 413/405/413 |
Sex (% women) G1: 28% G2: 30% Age (mean ± SD) G1: 60 ± 5 G2: 60 ± 6 Nutrient status marker, cobalamin (pmol/L), median (IQR): G1: 290 (239–366) G2: 286 (247–363) BMI (kg/m2): G1: 26.6 (3.6) G2: 26.5 (3.6) Current smokers: G1: 21% G2: 20% Dyslipidemia: G1: 39% G2: 33% |
Folic acid Doses: G1: 800 μg/day G2: placebo Background nutrient intake, baseline, median (IQR): G1: 192 (159–238) G2: 195 (158–242) Compliance: 99% of capsules consumed |
Cognition: Global cognitive function, Memory, Sensorimotor speed, Comple × speed, Information processing speed, Word fluency Word learning test, Concept shifting test, Stroop colour‐word test, Verbal fluency test, Letter digit substitution test |
Effects among those with baseline cobalamin <250 pmol/L (n = 230), all as change versus placebo: Sensorimotor speed, mean (95% CI) Z‐score: 0.112 (0.001–0.223) Information processing speed, mean (95% CI) Z‐score: 0.190 (0.055–0.325) Effects among those with baseline cobalamin ≥250 pmol/L (n = 588), all as change versus placebo: Sensorimotor speed, mean (95% CI) Z‐score: 0.046 (−0.033–0.126) Information processing speed, mean (95% CI) Z‐score: 0.048 (−0.036–0.131) Overall effects (all participants), all as change versus placebo: Global cognitive function, mean (95% CI) Z‐score: 0.050 (0.004–0.096), p = 0.033 Memory, mean (95% CI) Z‐score: 0.132 (0.032–0.233), p = 0.010 Sensorimotor speed, mean (95% CI) Z‐score: 0.064 (−0.001–0.129), p = 0.055 Complex speed, mean (95% CI) Z‐score: 0.037 (−0.049–0.122), p = 0.40 Information processing speed, mean (95% CI) Z‐score: 0.087 (0.016–0.158), p = 0.016 Word fluency, mean (95% CI) Z‐score: −0.07 (−0.188–0.048), p = 0.245 |
Abbreviations: BMI, body mass index; CI, confidence interval; CT, controlled trial; FACIT, Folic Acid and Carotid Intimamedia Thickness; G, group; Hcy, homocysteine; IQR, Interquartile range; RoB, risk of bias; RCT, randomised controlled trial; yrs, years.
C.1.2. Observational studies
| Reference Study name Country Study design Follow‐up Funding | Original cohort (N total) Exclusion criteria Study population (n) | Ascertainment of outcome | Exposure groups n/person‐years Exposure assessment method | Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Clarke et al. (2007) The Oxford Healthy Aging Project UK PC 10 yrs Public |
N = 2741 Population sampled: ≥65 yrs, residents in Oxford UK % lost to follow‐up: 79% n = 574 Sex (as % women): 60% Age (mean ± SD): 71.9 ± 5.2 MMSE (mean ± SD): 27.3 ± 2.7 |
Cognitive function assessed with the use of the MMSE on 3 occasions during 10 y |
S‐holoTC, mean ± SD (pmol/L;): 73 ± 43 S‐cobalamin, mean ± SD (pmol/L): 280 ± 106 S‐Folate, mean ± SD (nmol/L): 15.8 ± 14.6 S‐holoTC by enzyme‐linked immunoabsorbent assay method modified for use on an automated analyser S‐cobalamin by automated chemiluminescence system S‐Folate by microbiological method |
Outcome: change in MMSE score |
Model 1: Sex, education, smoking, history of vascular disease, systolic blood pressure, APOE, genotypes Model 2: Model 1+ all markers of vitamin status (holoTC, tHcy, MMA, cobalamin, folate) |
Change in cognitive decline (MMSE) per 100% increase in folate concentration ( β (SE) ): Model 1: 0.015 (0.012), p = NR Model 2: 0.004 (0.013), p = NR |
|
Morris et al. (2012) Framingham Heart Study US PC 8 yrs Public |
N = 5209 (examination 20, n = 1401) Population sampled: 2/3 of the adult population in Framingham, MA, US % lost to follow‐up: NR n = 549 Age (mean ± SD): 74.8 ± 4.6 MMSE (mean ± SD): 28.2 ± 2.1 MMSE <18 at examination 20 (1986–1990), non‐diabetic, normal kidney function, valid FFQ, baseline p‐cobalamin, p‐folate. Those with p‐cobalamin concentrations >701 pmol/L were excluded |
MMSE every 2 years |
p‐Folate (nmol/L): Q1 (ref): <5 Q2: 5–7.69 Q3: 7.7–12 Q4: 12.01–21.7 Q5: ≥21.75 Folate intake (μg/day) per quintile of p‐Folate (geometric mean (95% CI): Q1: 210 (190–232) Q2: 269 (248–291) Q3: 322 (296–350) Q4: 381 (348–416) Q5: 488 (445–536) Folic acid supplement users (%): Q1: 4.9 Q2: 5.5 Q3: 10 Q4: 23 Q5: 50 N (among those with p‐cobalamin <258 pmol/L) Q1 (ref): 60 Q2: 64 Q3: 44 Q4: 39 Q5: 24 126‐item, semiquantitative FFQ P‐cobalamin: non‐fasting, radioassay kit P‐folate: non‐fasting, microbial (L. casei) assay |
Outcome: change in MMSE score |
Analysis 1: adjusted for age, sex, educational achievement, baseline BMI, alcohol use versus nonuse Analysis 2: age, sex, educational achievement, baseline serum creatinine status, body mass index, smoking status |
Change in MMSE score per quintile of plasma folate among those with low (<258 pmol) p‐cobalamin (β (95% CI): Analysis 1: β (95% CI) Q1 (ref): −0.32 (−0.44 to −0.21) Q2: −0.32 (−0.42 to −0.21), p = 0.94 Q3: −0.22 (−0.35 to −0.08), p = 0.25 Q4: −0.28 (−0.42 to −0.14), p = 0.67 Q5: −0.92 (−1.09 to −0.74), p < 0.001 P for trend <0.001 Change in MMSE score per quintile of plasma folate among those without low (≥258 pmol) p‐cobalamin (β (95% CI): Analysis 1: β (95% CI) Q1 (ref): −0,18 (−0.30 to −0.06) Q2: −0.14 (−0.27 to −0.01), p = 0.62 Q3: −0.17 (−0.27 to −0.06), p = 0.85 Q4: −0.14 (−0.24 to −0.03), p = 0.57 Q5: −0.14 (−0.23 to −0.05), p = 0.59 p for trend 0.48 Analysis 2: β (95% CI) Change in MMSE score per use of folate supplements among those with low (<258 pmol) p‐cobalamin (β (95% CI)*: Non‐supplement users: −0.15 (−0.11 to −0.22) Supplement users: −0.1 (−0.04 to −0.24) Change in MMSE score per use of folate supplements among those without low (≥258 pmol) p‐cobalamin (β (95% CI)*: Non‐supplement users: −0.34 (−0.27 to −0‐37) Supplement users: −0.78 (−0.57 to −1.0) (p for interaction between cobalamin status and folate supplementation = 0.002) *numbers extracted from figure using graphreader.com |
|
Doets et al., 2014 Hordaland Homocysteine Study/Hordaland Health Study Norway PC 6 yrs Public |
N = 2841 Population sampled: apparently healthy residents of Bergen (Norway), who participated both in the Hordaland Homocysteine Study in 1992–3 and in the Hordaland Health Study in 1997–9% lost to follow‐up: NR n = 2203 Sex (as % women): 55% Age (mean, 95% CI): 72.5 (71.5, 73.6) Modified MMSE (median, P5th–P95th): 12 (10–12) |
Six cognitive tests were performed at the end of follow‐up: modified versions of the MMSE and of the Digit Symbol Test; a short form of the Block Design; the Kendrick Object Learning; an abridged version of the Controlled Oral Word Association Test; the Trail Making Test Part A. Principal component analysis was used to create a summary score for cognitive performance |
At baseline p‐folate, median (P5th‐P95th) (nmol/L): 12.5 (8.7, 20.9) p‐cobalamin, median (P5th‐P95th) (pmol/L): 338 (196, 595) At end of follow‐up p‐folate, median (P5th‐P95th) (nmol/L): 15.8 (12.0, 34.0) p‐cobalamin, median (P5th‐P95th) (pmol/L): 339 (192, 651) 9.5% participants used B‐vitamin supplements P‐folate, p‐cobalamin: non‐fasting, microbiological assays |
Outcome: cognitive score | Sex, education level, history of CVD /hypertension, apoE‐14 genotype and creatinine. |
Multivariate quantile regression and ordinary least‐squares regression of the cognitive score: No associations of plasma folate (β = 0.019, SE = 0.031, p = 0.540) or plasma cobalamin (β = 0.020, SE = 0.033, p = 0.541), measured at baseline, with cognitive performance and no indication of an interaction between plasma folate and cobalamin (β = 0.024, SE = 0.028, p = 0.394) |
Abbreviations: AD, Alzheimer disease; APOE, apolipoprotein E; CI, Confidence Interval; FFQ, food frequency questionnaire; FU, follow‐up; G, group; holoTC, holotranscobalamin; MMA, methylmalonic acid; MMSE, mini‐mental state examination; NA, Not assessed; NR, not reported; p, plasma; PC, prospective cohort; RoB, risk of bias; RR, Relative risk; S, serum; SE, standard error; SWE, Sweden; tHcy, total homocysteine; yrs, years.
C.2. Colorectal cancer (sQ4b)
C.2.1a. Intervention study on folic acid supplementation and incidence of colorectal cancer
| Reference Study Country Duration Funding | Design | Subject characteristics at baseline a | Intervention a | Endpoint assessed | Results |
|---|---|---|---|---|---|
|
Qin et al. (2017) CSPPT China 4.5 yrs 2008–2013 Mixed |
RCT, multi‐community Inclusion criteria: cancer free 45–75 yrs with hypertension Exclusion: overt CVD, pregnant/breast feeding etc long‐term use of folic acid, cobalamin, B6 Eligible participants were stratified by MTHFR C677T genotype (CC, CT, TT) (CC = 27%, CT = 49%, TT = 23%) Number participants randomised/completed/analysed G1: 10348/10276/10348 G2: 10354/10354/10354 |
Sex (% women) G1: 59% G2: 58.9% Age G1: 60 ± 7.5 G2: 60 ± 7.6 Nutrient status marker: S‐folate; median (interquartile range) baseline S‐folate was 8.1 (5.6–10.4) ng/mL (~18; 12–23 nmol/L). Extracted from Huo et al. (2015) |
Folic acid Doses: G1: 800 μg folic acid+10 mg Enalapril G2: 10 mg Enalapril Background nutrient intake: NR Compliance: Assessed every third months Around 70% took at least 70% of the study medication throughout the trial |
CRC (physician or oncologist diagnosed) |
Number of CRC cases (%) G1: 13 (0.13%) G2: 6 (0.06%) HR 2.17 (95% CI 0.82–5.70) p = 0.117 |
Abbreviations: CI, confidence Interval; CRC, colorectal cancer; CSPPT, China Stroke Primary Prevention Trial; CVD, cardiovascular disease; HR, hazard Ratio; G, group; MTHFR, methylenetetrahydrofolate reductase; NR, not reported; RCT, randomised controlled trial; S, serum; SD, standard deviation; yrs, years.
Values reported as mean ± standard deviation or median (inter quartile range) unless otherwise indicated.
C.2.1b. Intervention studies on folic acid supplementation and incidence of colorectal adenomas
|
Reference Study Country Duration Funding |
Design |
Subject characteristics at baselinea |
Interventiona | Endpoint assessed | Results |
|---|---|---|---|---|---|
|
Cole et al. (2007) AFPPS USA 3 yrs + 3–5 yrs (trial follow‐up with continued folic acid treatment) Enrolment 1994–98 Fortification started 1996, and was mandatory 1998 Public, Supplements by private company |
RCT 3 × 2 factorial design, with folic acid and aspirin Inclusion criteria: 21–80 yrs and histologically confirmed adenoma removed. Each participant had a complete colonoscopy, with removal of all known polyps, within 3 mo of enrolment. Exclusion criteria: familial polyposis syndromes, intestine cancer, malabsorption syndromes, condition worsened by supplemental aspirin or folic acid, conditions treated with aspirin, non‐steroidal anti‐inflammatory drugs or folate. Cobalamin deficient individuals were excluded. N participants randomised/completed 1st follow‐up/completed 2nd follow‐up/Consented continue folic acid or placebo/analysed 2nd follow‐up G1: 516/501/475/370/303 G1a: 175/NR/NR/NR/NR G1b: 171/NR/NR/NR/NR G1c: 170/NR/NR/NR/NR G2: 505/486/451/359/304 G2a: 169/NR/NR/NR/NR G2b: 167/NR/NR/NR/NR G2c: 169/NR/NR/NR/NR |
Sex (% women) G1: 36% G2: 36.4% Age G1: 57 ± 9.6 G2: 57 ± 9.5 Nutrient status marker (ng/mL) G1: P‐folate 10.5 ± 7.9 G2: P‐folate 10.4 ± 7.5 No other relevant sources of heterogeneity |
Folic Acid Doses 1st follow‐up (3 years) G1: 1000 μg /day G1a: 1000 μg/day + 81 mg/day aspirin G1b: 1000 μg/day + 325 mg/day aspirin G1c: 1000 μg/day + aspirin placebo 2nd follow‐up (+ 3–5 years) G2: Placebo G2a: Placebo +81 mg/day aspirin G2b: Placebo +325 mg/day aspirin G2c: Placebo + aspirin placebo Background nutrient intake: dietary folate G1: 320 ± 147 G2: 325 ± 163 Compliance: Reported adherence ‘excellent’ 87% ≥6 d/week during 1st interval 71% ≥6 day/week during 2nd interval Similar across treatments |
Colonoscopy at the end of the initial 3‐year intervention (1st follow‐up) and at the end of the 2nd follow‐up (completed by 1 October 2004). Primary outcome: at least 1 colorectal adenoma. Secondary outcomes: advanced lesions (tubulovillous adenomas [25%–75% villous features], villous adenomas ≥75% villous features], large adenomas [≥1 cm in diameter], adenomas with high‐grade dysplasia or invasive cancer), adenoma multiplicity (0, 1–2 or ≥3 adenomas). |
Primary outcome: at least 1 colorectal adenoma 1st follow‐up G1: 44.1%, 221/501 G2: 42.4%, 206/486 uRR 1.04 (95% CI 0.90–1.20) 2nd follow‐up G1: 41.9%, 127/303 G2: 37.2%, 113/304 uRR 1.13 (95% CI 0.93–1.37) Both follow‐ups (n = 607) G1: 71.3% G2: 65.5% uRR 1.09 (95% CI 0.98–1.21) Multivariable‐adjusted RR were similar (NR). No significant effect modification by sex, age, alcohol, smoking, plasma folate, BMI, presence/absence of advanced lesions); no significant interaction Folic acid/aspirin. However, the suggested increased risk for folic acid was confined to participants not allocated to aspirin. Secondary outcomes: advanced lesions 1st follow‐up G1: 11.4% 57/501 G2: 8.6% 42/486 uRR 1.32 (95% CI 0.90–1.92) 2nd follow‐up G1: 11.6% 35/303 G2: 9.6% 21/304 uRR 1.67 (95% CI 1.00–2.80) Both follow‐ups G1: 23.1% G2: 17.1% uRR 1.35 (95% CI 0.98–1.86) Secondary outcome: ≥3 lesions 1st follow‐up G1: 9.4% 47/501 G2: 7.8% 38/486 uRR 1.20 (95% CI 0.80–1.81) 2nd follow‐up G1: 9.9% 30/303 G2: 4.3% 13/304 uRR 2.32 (95% CI 1.23–4.35) Results were similar when the analysis was restricted to the 501 participants who agreed to extended treatment with folic acid or placebo in the second follow‐up interval |
|
Passarelli et al. (2019) AFPPS As of above but with additional post‐treatment follow‐up from Oct 1st, 2004 to May 31st 2012 |
As of above As compared to the 2007 publication, and because the study was terminated Oct 2004 due to funding, some colonoscopies were scheduled after that date and thus not included. In the 2019 paper, a total 218 additional colonoscopies were performed (after Oct 2004) of which 161 had agreed to continue treatment (G1 or G2). This was still the 2nd follow‐up. Aspirin treatment ended after the first endoscopy follow‐up (i.e. 3 yrs) |
As of above | As of above |
Colonoscopy at the end of the initial 3‐year intervention (1st follow‐up) and at the end of the 2nd follow‐up (until the intended end of the second interval). Primary outcome: at least 1 colorectal neoplastic lesion (i.e. conventional adenomas, sessile serrated adenomas/polyps (SSA/Ps) and invasive CRC). Secondary outcomes: advanced conventional adenomas (tubulovillous or villous adenomas, or ≥1 cm in diameter, or with high‐grade dysplasia or CRC), ≥3 conventional adenomas, and SSA/Ps. |
Relative risk adjusted for age, sex, centre, race, BMI, smoking, family history of CRC, number of advanced adenomas on examination qualifying, for study entry (all at baseline). 1st follow‐up Any conventional adenoma, SSA/P, CRC G1: 44% (221/501) G2: 42% (206/486) Relative Risk 1.04 (95% CI 0.90–1.21) Advanced conventional adenomas, CRC G1: 10% (48/501) G2: 9% (43/486) Relative Risk 1.00 (95% CI 0.66–1.52) ≥3 conventional adenomas, CRC G1:6% (30/501) G2: 6% (27/486) Relative Risk 1.12 (95% CI 0.65–1.94) SSA/P G1: 12% (60/501) G2: 9% (44/486) Relative Risk 1.41 (95% CI 0.96–2.08) 2nd follow‐up Any conventional adenoma, SSA/P, CRC G1: 43% (146/338) G2: 36% (118/325) Relative Risk 1.21 (95% CI 0.99–1.47) Advanced conventional adenomas, CRC G1: 9% (32/338) G2: 8% (27/325) Relative Risk 1.20 (95% CI 0.73–1.97) ≥3 conventional adenomas, CRC G1:9% (30/338) G2: 5% (16/325) Relative Risk 1.58 (95% CI 0.87–2.86) SSA/P G1: 8% (28/338) G2: 5% (16/325) Relative Risk 1.94 (95% CI 1.02–3.68) |
|
Logan et al. (2008) UkCAP 9 UK, 1 DK centers Recruitment 1997–2001 3 yrs Public |
RCT 2 × 2 factorial design with Folic acid, aspirin Inclusion criteria: <75 yrs of age, CR adenoma > = 0.5 cm removed 6 mo before randomisation. Exclusion: medical conditions hindering participation N participants randomised/completed 2nd colonoscopy/completed both meds: G1: 234/215/161 G2: 236/217/149 G3: 236/217/159 G4: 233/204/158 |
Sex (% women) G1: 48.7% G2: 45.8% G3: 39% G4: 39.1% Age: mean 57.8 yr (range 27.6–74.6 yr) Nutrient status marker: NR |
Folic acid Doses: G1: 500 μg folic acid per day G2: 300 mg aspirin per day G3: 500 μg folic acid +300 mg aspirin per day G4: Placebo Background folate intake: (μg/day) G1: 309 ± 126 G2: 311 ± 108 G3: 312 ± 107 G4: 298 ± 105 Those with ≥95% Folate Compliance in those with 2nd coloscopy were: G1 & G3: 80% G2 & G4: 81% |
Colonoscopy Any adenomas (%)/ advanced adenomas (%), no of outcome adenomas/participant (mean) Advanced adenomas: adenomas ≥1 cm in diameter |
Those who completed 2nd colonoscopy per single treatment group % with any adenomas/% with advanced adenomas/No. of adenomas per patient (mean) G1: 30.2/15.4/0.48 G2: 22.6/10.1/0.33 G3: 23/8.8/0.29 G4: 27.5/14.7/0.42 Main effect folic acid treatment according to: Any adenomas n (%)/Advanced adenomas n (%) G1 & G3 (folate): 115 (26.6)/52 (12) vs. G2 & G4 (no folate): 105 (24.9)/52 (12.4) Relative Risk (RR) (95% CI): RR = 1.07 (0.85–1.34) for any adenomas RR = 0.98 (0.68–1.40) for advanced adenomas |
|
Wu et al. (2009) HPFS & NHS Folic acid prevention trial USA 3–6.5 yrs; 1996–2004 Fortification started 1996, i.e. post‐ fortification era Public, supplements from private |
RCT Inclusion/exclusion criteria: NHS & HPFS participants who had a history of CR adenoma confirmed by medical record, planned another endoscopy 4 y after initiation of trial, agreed not to take multivitamins, cancer free at randomisation except for early‐stage prostate or breast cancer or non‐melanoma skin cancer. Only included non‐cobalamin deficient (defined as, 200 pg/mL or as 200–299 pg/mL with methylmalonic acid concentrations >32 lg/L). Ineligible if presently taking multivitamin, folic acid or vitamin B‐12 supplements for a diagnosed vitamin deficiency or had homocysteinemia or pernicious anaemia, gastrectomy or gastrointestinal disorder or other illnesses N participants randomised/completed colonoscopy/analysed G1: 338/NR/237 G2: 334/NR/238 49% agreed to extend treatment from 3 yrs to 5–6.5 yrs |
Sex (% women) G1: 62% G2: 63% Age G1: 64.5 ± 6.9 G2: 65.5 ± 6.3 Baseline P‐folate (ng/mL): G1: 9.2 ± NR G2: 9.1 ± NR No major baseline differences between treatments and between randomised and those having a colonoscopy (i.e. 475 out of 672 participants) Baseline P‐folate (ng/mL) for those who donated blood samples twice (see next column: G1: 9.7 ± 6.8 G2: 9.3 ± 6.2 |
Folic acid Doses: G1: 1000 μg/day G2: Placebo Background folate intake (μg/day) G1: 323 G2: 324 Compliance: 77% performed adherence P‐folate at midtrial: G1: 39.2 ± 24.8 ng/mL G2: 17.0 ± 7.9 ng/mL, reasonable pill compliance for those who donated two blood samples |
Colonoscopy performed by their physician ≥3 mo after initiation and ≤12 after trial completion. Primary outcome: any new (recurrent) adenoma Secondary outcome: adenoma by site and stage and number |
At least 1 adenoma/total G1: n = 62/237 G2: n = 72/238 Risk Ratio (RR): 0.87 (95% CI 0.65–1.16) Advanced adenoma/total (please note not all adenomas were classified according to advanced or early) G1: n = 16/221 G2: n = 14/225 Risk Ratio (RR): 1.03 (95% CI 0.53–1.98) Stratified analyses: By baseline P‐folate ≤7.5 ng/mL RR 0.61 (95% CI 0.42–0.90) >7.5 ng/mL RR 1.28 (95% CI 0.82–1.99) By combination alcohol intake (g/d)/P‐folate ≤5.6 g/day and >7.5 ng/mL RR 1.23 (95% CI 0.64, 2.37) >5.6 g/day and ≤7.5 ng/mL RR 0.49 (95% CI 0.28, 0.84) p = 0.009 |
|
Jaszewski et al. (2008) USA 3 yrs Dec 1998‐ June 2005 NR |
RCT Inclusion criteria: 18–80 yrs and had a colonoscopy and had at least one adenoma Exclusion: severe co‐morbid conditions, heart disease, cancer or other organ dysfunction or contraindications for colonoscopy/polypectomy. Gastrointestinal disorders affecting absorption/metabolism of folic acid, cobalamin deficiency and hereditary CRC. Pregnant or lactating women. Patients who drank more than 2 alcoholic drinks daily or who were regularly using vitamin, minerals, steroids and non‐steroidal anti‐inflammatory drugs (excluding aspirin for CVD prevention), antineoplastic agents or folate. N participants invited/ eligible of polyp histology and run‐in compliance/completed colonoscopy 3 yrs later G1: 80/NR/46 G2: 97/NR/48 |
Sex (% women) G1: 7% G2: 8% Age G1: 60 ± 10 G2: 63 ± 10 S‐folate ng/mL G1: 14.53 ± 19.51 G2: 11.35 ± 6.65 RBC‐folate ng/mL G1: 447 ± 165 G2: 478 ± 149 |
Folic acid Doses: G1: 5000 μg/day G2: Placebo Folate intake μg/day G1: 184 ± 232 G2: 162 ± 140 Compliance: Pill count and telephone contact every 90 days (NR). Participants were required to take 90% of their pills. |
Colonoscopy at 3‐y follow‐up (all identified polyps) |
Number of adenomas/patient G1: 0.36 +/− 0.69 G2: 0.82 +/− 1.17 p = 0.02514 Number of hyperplastic polyps/patient G1: 0.44 +/− 0.89 G2: 0.51 +/− 0.94 NS Advanced adenomas or Left‐sided p < 0.02 for both outcomes in favour of folic acid, and folic acid was more protective in those <70 yr |
Abbreviations: AFPPS, Aspirin/Folate Polyp Prevention Study; BMI, body mass index; CI, confidence Interval; CR, colorectal; CRC, colorectal cancer; CVD, cardiovascular disease; d, day(s); DK, Denmark; G, group; HPFS, Health Professionals Follow‐Up Study; mo, months; NHS, Nurses' Health Study; NR, not reported; p, plasma; RBC, red blood cells; RCT, randomised controlled trial; S, serum; SD, standard deviation; SSA/P, sessile serrated adenomas/polyps; U, unadjusted; UK, United Kingdom; ukCAP, United Kingdom Colorectal Adenoma Prevention; yr, year.
C.2.2. Observational studies
C.2.2a. Observational studies on folate biomarkers and incidence of colorectal cancer
|
Reference Study name Country Study design Follow‐up Funding |
Original cohort (N total) Exclusion criteria Study population |
Ascertainment of outcome |
Exposure groups n/person‐years Exposure assessment method |
Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Eussen et al. (2010) EPIC DK, SE, FR, GR, DE, IT, NL, ES, GB NCC 3.6 yrs (median) Mixed |
N = 521,000 (EPIC, all countries) Population sampled: Middle‐aged male and female population Exclusion criteria: Controls: existing cancer diagnosis % lost to follow‐up: 1.57% n = 1367 (cases), 2325 (controls) Sex (% women): Cases: 51% Controls: 53% Age at blood donation, mean (min‐max): Cases: 59.1 (36.8–77.0) Controls: 58.9 (36.6–76.6) |
Cancer cases based on population cancer registries or combination of methods incl. health insurance records, cancer/pathology registries, active contact with study subjects or next of kin. Histologic confirmation of CRC was available for 93%; 6% clinical observation, cytology or autopsy, 1% missing. |
Unit of measurement: Min‐max (nmol/L), plasma folate: Q1: <7.6 (ref) Q2: 7.6–9.9 Q3: 9.9–13.0 Q4: 13.0–18.3 Q5: >18.3 Lactobacillus casei microbiological assay |
Not reported by quintile |
Model 1: Controls matched on age, sex, study centre Model 2: Matching factors and smoking status, education level, physical activity, fibre intake, intake of red and processed meat, alcohol consumption, BMI |
Plasma folate versus CRC: RR (95% CI) Model 1: Q1: 1.0 (ref) Q2: 0.97 (0.78–1.2) Q3: 1.06 (0.86–1.31) Q4: 0.87 (0.69–1.09) Q5: 0.91 (0.73–1.14) P‐trend: 0.29 Model 2: Q1: 1.0 (ref) Q2: 1.02 (0.82–1.27) Q3: 1.08 (0.87–1.35) Q4: 0.92 (0.72–1.16) Q5: 0.94 (0.74–1.20) P‐trend: 0.44 |
|
Neuhouser et al. (2015) WHI‐OS US NCC ~15 yrs Public |
N = 93,676 Population sampled: Post‐menopausal women, 50–79 yrs Exclusion criteria: Pre‐existing intestinal disease, including history of CRC, carcinoma in situ, ulcerative colitis, Crohn's disease, BMI ≤15 or ≥50. % lost to follow‐up: NR n = 988 (cases), 988 (controls) Sex (as % women): 100% Age yrs (mean ± SD): Cases: 67 ± 7 Controls: 67 ± 7 |
Via annual medical status update questionnaires. Cancer diagnoses were confirmed by trained physician adjudicators using medical records |
Unit of measurement: RBC folate in ng/mL (min‐max): Q1: <427 (ref) Q2: 427–577 Q3: 577–742 Q4: >742 Plasma folate in ng/mL (min‐max): Q1: ≤9.72 (ref) Q2: 9.72–16.85 Q3: 16.85–26.85 Q4: >26.85 Plasma and RBC folate concentrations were determined by radio assay |
(Cases/controls) RBC folate Q1: 281/248 (ref) Q2: 227/247 Q3: 222/247 Q4: 235/246 Plasma folate Q1: 274/240 (ref) Q2: 236/240 Q3: 236/240 Q4: 210/239 |
Model 1: Age Model 2: Age, BMI, post‐menopausal hormone use, family history of CRC and history of colonoscopy Analyses also conducted to test effect modification by folic acid fortification (stratified by pre‐ or post‐fortification) |
RBC folate versus CRC OR (95% CI) Model 1: Q1: 1.0 (ref) Q2: 0.86 (0.67–1.11) Q3: 0.81 (0.63–1.06) Q4: 0.85 (0.65–1.12) P‐trend: 0.26 Model 2: Q1: 1.0 (ref) Q2: 0.84 (0.63–1.13) Q3: 0.85 (0.63–1.13) Q4: 0.91 (0.67–1.24) P‐trend: 0.63 Plasma folate versus CRC OR (95% CI) Model 1: Q1: 1.0 (ref) Q2: 0.87 (0.68–1.12) Q3: 0.86 (0.66–1.12) Q4: 0.78 (0.60–1.02) P‐trend: 0.09 Model 2: Q1: 1.0 (ref) Q2: 0.84 (0.63–1.12) Q3: 0.98 (0.72–1.32) Q4: 0.91 (0.67–1.23) P‐trend: 0.80 |
|
Rossi et al. (2006) 1969 Busselton Health survey Australia PC 23 yrs Public |
Population sampled: General population 40–90 yrs with information on nonfatal cancer‐related events Exclusion criteria: History of cancer % lost to follow‐up: NR n = 1035 Sex (% women): 55.0% Age: 55 yrs (average) |
Cancer morbidity was obtained by linkage to the death register, cancer register and hospital admissions. The event of interest was the first of cancer registration, hospital admission for cancer or cancer death (individuals censored at the time of the first event) |
Serum folate (μg/L, min‐max): Q1: <3.00 Q2: 3.00–4.49 Q3: 4.50–5.99 Q4: ≥6.00 (ref) RBC folate (μg/L, min‐max): Q1: 0.0–199.9 Q2: 200.0–274.9 Q3: 275–349.9 Q4: ≥350.0 (ref) In‐house automated microbiological assay system |
Incident cases Serum folate: Q1: 5 Q2:10 Q3:14 Q4: 12 (ref) RBC folate: Q1: 11 Q2: 9 Q3: 11 Q4: 10 (ref) |
Age and sex and baseline cancer‐risk factors based on established risk factors for each cancer outcome: smoking, alcohol and body mass index for all cancers, including CRC |
HR (95% CI): 2 μg/L decrease in serum folate. Serum folate versus CRC morbidity: 1.20 (0.91, 1.61), p = 0.20 100 μg/L decrease in RBC folate. RBC folate vs. CRC morbidity: 1.19 (0.93, 1.54), p = 0.18 Serum folate versus CRC morbidity: Q1: 2.15 (0.73, 6.31) Q2: 1.07 (0.45, 2.54) Q3: 1.64 (0.75, 3.59) Q4: 1.0 (ref) RBC folate versus CRC morbidity: Q1: 2.00 (0.82, 4.83) Q2: 1.31 (0.53, 3.28) Q3: 2.03 (0.86, 4.80) Q4: 1.0 (ref) |
|
Otani et al. (2008) JPHC Japan NCC 11.5 yrs Public |
N = 38,373 with baseline data (from 133,232) Population sampled: General population, 40–69 yrs old Exclusion criteria: Cancer diagnosis at baseline % lost to follow‐up: 10.1% n = 375 cases, 750 controls Sex (% women): 47.7% Age (Mean): Men: 56.9 yrs Women: 56.5 yrs Controls matched on sex, age, date of blood drawn, time since last meal and study location |
Incidence CRC data were collected for the JPHC cancer registry through two data sources: local major hospitals, and population‐based cancer registries |
Plasma folate (ng/mL, range) Men Q1 (ref): <5.6 Q2: 5.6–6.7 Q3: 6.8–8.5 Q4: >8.5 Women Q1 (ref): <6.6 Q2: 6.6–8.3 Q3: 8.4–10.5 Q4: >10.6 Plasma folate concentrations were measured by chemiluminescence immunoassay |
CRC cases/controls Men Q1 (ref): 37/64 Q2: 40/86 Q3: 41/90 Q4: 45/84 Women Q1 (ref): 33/75 Q2: 56/74 Q3: 33/76 Q4: 38/72 |
Matching factors: sex, age, date of blood drawn, time since last meal and study location. Pack‐years of smoking (continuous), alcohol consumption (g/week ethanol, continuous), body mass index (continuous), physical exercise (less than once a week or once a week or more), vitamin supplement use, and family history of CRC. Results also stratified by tumour site (colon or rectum) |
Plasma folate versus CRC OR (95% CI) Men Q1 (ref): 1.0 Q2: 0.70 (0.37–1.3) Q3: 0.72 (0.38–1.3) Q4: 0.86 (0.45–1.6) p‐trend: 0.88 Women Q1 (ref): 1.0 Q2: 1.7 (0.93–3.0) Q3: 0.98 (0.53–1.8) Q4: 1.0 (0.56–1.9) p‐trend: 0.63 |
|
Lee et al. (2012) NHS US NCC 24 yrs HPFS US NCC 16 yrs PHS NCC 18 yrs Public |
NHS N = 121,700 Population sampled: Female nurses Exclusion criteria: NR % lost to follow‐up: NR n = 189 cases/377 controls Sex (% women): 100 Age at blood draw (yrs, mean) Q1: 59 Q2: 59 Q3: 60 Q4: 62 Matching criteria: Controls matched on age, month and year of blood draw, fasting status at blood collection HPFS N = 51,529 Population sampled: Male health professionals Exclusion criteria: NR % lost to follow‐up: NR n = 173 cases/345 controls Sex (% women): 0 Age at blood draw (yrs, mean) Q1: 64 Q2: 66 Q3: 68 Q4: 69 Controls matched on age, month and year of blood draw PHS N = 22,071 Population sampled: Male physicians Exclusion criteria: NR % lost to follow‐up: NR n = 240 cases/408 controls Sex (% women): 0 Age at randomisation (yrs, mean) Q1:54 Q2: 58 Q3: 58 Q4: 57 Controls matched on age, smoking Total: N = 602 incident CRC cases N = 1130 controls All blood samples were collected prior to FDA‐mandated fortification of grain products with folate, which began in 1998 |
Cases were identified by annual (PHS) or biennial (NHS and HPFS) follow‐up questionnaires and then confirmed by review of medical records by the study investigators (NHS, HPFS) or an end‐point committee (PHS) |
Plasma folate (ng/mL (median) NHS Cases: 7.9 ng/mL Controls: 7.5 ng/mL Batch 1 Q1: 3.8 ng/mL Q2: 6.4 ng/mL Q3: 10.0 ng/mL Q4: 17.6 ng/mL Batch 2 Q1: 3.6 ng/mL Q2: 5.9 ng/mL Q3: 9.0 ng/mL Q4: 15.7 ng/mL HPFS Cases: 5.7 ng/mL Controls: 6.0 ng/mL Q1: 2.9 ng/mL Q2: 4.8 ng/mL Q3: 7.3 ng/mL Q4: 11.3 ng/mL PHS Cases: 5.4 ng/mL Controls: 5.1 ng/mL Batch 1 Q1: 3.2 ng/mL Q2: 5.1 ng/mL Q3: 7.1 ng/mL Q4: 11.0 ng/mL Batch 2 Q1: 1.7 ng/mL Q2: 2.6 ng/mL Q3: 3.9 ng/mL Q4: 6.6 ng/mL Plasma folate was measured using a radioassay kit (Bio‐Rad, Richmond, CA) in the NHS and HPFS or a microbiological method in the PHS |
Incident cases of CRC: 602 |
Model 1: matching factors, BMI, family history of CRC, physical activity, pack years of smoking, post‐menopausal hormone use and fasting status (only HPFS), aspirin use, height and history of endoscopy in the NHS and HPFS; models were adjusted for BMI, physical activity, fasting status and aspirin assignment in the PHS Model 2: Model 1 and alcohol intake, red meat intake, vitamin D from food and calcium from food in the NHS and HPFS; red meat intake, dairy calcium, alcohol intake in the PHS Results stratified by fortification status at diagnosis |
All three cohorts: Plasma folate versus CRC RR (95% CI) Model 1 Q1 (ref): 1.0 Q2: 1.47 (1.09–1.99) Q3: 1.31 (0.97–1.79) Q4: 1.39 (1.02–1.89) p‐trend: 0.17 Model 2 Q1 (ref): 1.0 Q2: 1.55 (1.14–2.11) Q3: 1.37 (1.00–1.88) Q4: 1.47 (1.07–2.01) p‐trend: 0.10 Stratified analyses Models reported by cohort NS Results stratified by fortification status at diagnosis NS (only reported as Q1 versus Q2–Q4), except post‐fortification in the pooled data set: Q1: 1.0 (ref) Q2–4: 2.56 (1.09–6.02) |
|
Van Guelpen et al. (2006) Northern Sweden Health and Disease Cohort (MONICA, VIP, MSP) Sweden NCC 4.2 yrs (median) Public |
N = NR Population sampled MONICA: General population, 25–74 yrs old. VIP: General population, 40–60 yrs old. MSP: Women, 50–70 yrs old Exclusion criteria: Previous CRC diagnosis, prioritisation to other studies, insufficient plasma sample, and lack of at least one matching referent % lost to follow‐up: NR n = 226 cases, 437 controls Sex (% women): 58% Age (Median, IQR): Cases: 59.8 (50.3–60.2) Controls: 59.7 (50.2–60.2) Matching criteria: Control matched for (2:1): sex, age, subcohort, date of health survey, fasting status at sample donation |
CRC cases identified by linking the Northern Sweden Health and Disease Cohort with the National Cancer Registry, using Swedish personal numbers as the matching variable. Verification of diagnosis by histopathology was an inclusion criterion for the study, and questionable diagnoses were reviewed by a pathologist |
Plasma folate (nmol/L, min‐max). Quintile cut‐offs. Men Q1 (ref): <5.1 Q2: 5.1–6.7 Q3: 6.7–8.1 Q4: 8.1–11.3 Q5: ≥11.3 Women Q1 (ref): <5.7 Q2: 5.7–7.4 Q3: 7.4–9.4 Q4: 9.4–13.0 Q5: ≥13.0 Plasma folate was analysed by Quantaphase II radioassay |
Incident CRC cases/controls for model 2 Men: Q1 (ref): 7/36 Q2: 24/36 Q3: 20/36 Q4: 23/36 Q5: 19/36 Women: Q1 (ref): 20/50 Q2: 26/51 Q3: 36/50 Q4: 28/51 Q5: 18/50 |
Model 1: Unadjusted Model 2: BMI, current smoking, recreational and occupational physical activity, alcohol intake Results stratified by sex, age at baseline, follow‐up duration, tumour site (right, left, rectum) and stage (Dukes) Matching factors (sex, age, subcohort, date of health survey, fasting status at sample donation) |
Plasma folate versus CRC OR (95% CI) Model 1 (both sexes) Q1 (ref): 1.00 Q2: 1.85 (1.07–3.19) Q3: 2.26 (1.29–3.95) Q4: 1.97 (1.12–3.47) Q5: 1.55 (0.85–2.85) p‐trend: 0.173 Model 2 (both sexes) Q1 (ref): 1.00 Q2: 1.72 (0.99–3.03) Q3: 2.00 (1.13–3.56) Q4: 1.87 (1.04–3.36) Q5: 1.34 (0.72–2.50) p‐trend: 0.325 Men (model 2) Q1 (ref): 1.00 Q2: 2.71 (0.97–7.53) Q3: 1.81 (0.62–5.26) Q4: 2.16 (0.74–6.35) Q5: 1.78 (0.59–5.39) p‐trend: 0.726 Women (model 2) Q1 (ref): 1.00 Q2: 1.17 (0.57–2.42) Q3: 1.96 (0.94–4.09) Q4: 1.50 (0.70–3.21) Q5: 0.97 (0.42–2.17) p‐trend: 0.698 |
|
Le Marchand et al. (2009) Multiethnic Cohort study US NCC ~10 yrs Public |
N = 67,594 Population sampled: Age 45–75 yrs, from five racial/ethnic groups: African Americans, Native Hawaiians, Japanese Americans, Latinos and Whites. Exclusion criteria: NR % lost of follow‐up: NR n = 224 cases, 411 controls Sex (% women): 37.5% Age (median, IQR) Cases: 70.5 (63–76) Controls: 70.0 (63–76) Matching criteria: age, sex, race/ethnicity, study site, date/time of blood draw and hours of fasting |
Incident colorectal cancer cases were identified through the Hawaii and California tumour registries of the SEER Program of the National Cancer Institute |
Plasma folate (ng/mL, min‐max) Q1 (ref): ≤9.94 Q2: 9.95–15.3 Q3: 15.4–26.1 Q4: >26.1 Plasma folate and cobalamin concentrations were determined by a radioimmunoassay method |
Incident cases Cases/controls Q1 (ref): 63/98 Q2: 54/97 Q3: 58/101 Q4: 48/111 |
Model 1: Age, hours of fasting at blood draw Model 2: model 1 and physical activity, processed meat, pack‐years, BMI, ethanol, family history of CRC and history of CRC screening |
Plasma folate versus CRC OR (95% CI) Model 1 Q1 (ref): 1.00 Q2: 0.87 (0.54–1.41) Q3: 0.74 (0.42–1.30) Q4: 0.56 (0.31–1.03) p‐trend: 0.055 Model 2 Q1 (ref): 1.00 Q2: 0.91 (0.56–1.49) Q3: 0.79 (0.44–1.41) Q4: 0.61 (0.33–1.13) p‐trend: 0.097 |
|
Gylling et al. (2014) Northern Sweden Health and Disease study Sweden NCC VIP: 13–24 yrs MSP: 11 yrs Public |
N= VIP: 85,877 MSP: 28,802 Population sampled: VIP: general population MSP: women residing in the Västerbotten County 50–70 yrs Exclusion criteria: Previous cancer diagnosis, other than non‐melanoma skin cancer, insufficient plasma sample volume available, prioritised to other studies or with no matching control, falsely low plasma folate % lost to follow‐up: NR N = Cases: 331 Controls: 662 Sex (% women): 59.2% Age [median (25th–75th percentile)]: 59.7 (50.1–60.1) Median time from blood draw to diagnosis of cases was 10.8 yrs, range 0.3–19.8 yrs Matching criteria: Controls (2:1) were matched by age, sex, cohort and year of blood sampling and data collection |
CRC cases diagnosed between 14/2/2003 and 31/3/2009 were identified by linkage with the essentially complete Cancer Registry of Northern Sweden |
Plasma Folate (nmol/L) Men: T1: <5.8 T2: 5.8–9.5 T3: >9.5 Women: T1: <6.1 T2: 6.1–10.7 T3: >10.7 Folate concentrations determined by microbiologic method, using Lactobacillus casei |
Incident cases: case/controls for model 2 Men: T1: 39/90 T2: 51/90 T3: 45/90 Women: T1: 55/130 T2: 78/131 T3: 63/131 |
Model 1: Unadjusted Model 2: Adjusted for BMI, current smoking, recreational and occupational physical activity, alcohol intake |
Plasma folate versus CRC OR (95% CI) Model 1: T1: 1.00 (ref) T2: 1.55 (1.05–2.28) T3: 1.31 (0.87–1.98) p for trend: 0.503 Model 2: T1: 1.00 (ref) T2: 1.62 (1.08–2.42) T3: 1.42 (0.94–2.21) p for trend: 0.322 Men: T1: 1.00 (ref) T2: 1.30 (0.70–2.41) T3: 1.17 (0.61–2.25) p for trend: 0.621 Women: T1: 1.00 (ref) T2: 1.83 (1.05–3.17) T3: 1.56 (0.87–2.80) p for trend: 0.411 |
|
Geijsen et al. (2020) COLON study, EnCoRe, CORSA, ColoCare The Netherlands, Austria, Germany, US PC 3, 7 yrs (median) Public |
N = 8853 Population sampled: NR Exclusion criteria: NR % lost to follow‐up: NR n = 2,024 COLON: 1094 EnCoRe: 297 CORSA: 209 ColoCare HD: 260 ColoCare HCI: 46 ColoCare FHCRC: 118 Sex (% women): 35.6% Age (median, IQR) 66.0 (60.0–72.7) |
Clinical data, including CRC stage, tumour site, resection status and treatment regimen were obtained from medical records. Clinical outcome data were abstracted from medical records and through linkage with national cancer registries |
Plasma or serum folate (nmol/L, median, IQR) T1 (ref): 8.5 (6.3 to 9.8) T2: 15.0 (13.2 to 17.4) T3: 30.9 (24.5 to 45.3) Plasma or serum unmetabolised folic acid (nmol/L, median, IQR) T1 (ref): 0.6 (0.6 to 0.7) T2: 1.0 (0.9 to 1.2) T3: 2.7 (1.9 to 5.5) Plasma/serum folate, unmetabolized folic acid by liquid chromatography–tandem mass spectrometry |
CRC recurrence/number at risk CRC recurrence Plasma or serum folate; T1 (ref): 84/672 T2: 83/659 T3: 91/642 Unmetabolised folic acid: T1 (ref): 8/98 T2: 14/99 T3: 20/99 |
Model 1: Crude Model 2: Age, sex, chemotherapy status, cohort |
Folate (plasma or serum) vs. CRC recurrence: HR (95% CI) Model 1 T1 (ref): 1.00 T2: 1.02 (0.75 to 1.38) T3: 1.14 (0.85 to 1.54) p‐trend: 0.35 Model 2 T1 (ref): 1.00 T2: 1.01 (0.74 to 1.37) T3: 1.14 (0.81 to 1.60) p‐trend: 0.40 Continuous model 1 (HR and 95% CI for doubling concentration): 1.06 (0.94 to 1.20) Continuous model 2 (HR and 95% CI for doubling concentration): 1.05 (0.91 to 1.21) UFA vs. CRC recurrence: Model 1 T1 (ref): 1.00 T2: 1.78 (0.75 to 4.24) T3: 2.59 (1.14 to 5.89) p‐trend: 0.03 Model 2 T1 (ref): 1.00 T2: 1.86 (0.76 to 4.56) T3: 3.12 (1.22 to 8.00) p‐trend: 0.03 Continuous model 1 (HR and 95% CI for doubling concentration): 1.23 (1.05 to 1.44) Continuous model 2 (HR and 95% CI for doubling concentration): 1.31 (1.02 to 1.58) |
|
Weinstein et al. (2008) The Wei Study Finland NCC 17 yrs Public |
N = 29,133 Population sampled: Men 50–69 yrs who smoked ≥5 cigarettes/day Exclusion criteria: Men with prior cancer or serious illness, or current use of vitamin E, vitamin A or beta‐carotene in excess of defined amounts % lost to follow‐up: NR n = 278 cases, 278 controls Sex (% women): 0 Age (median, IQR) Cases, colon: 59 (54–62) Controls, colon: 58 (55–61) Cases, rectum: 58 (54–61) Controls, rectum: 57 (54–60) Matching criteria: Controls matched on age and date of blood draw |
Cancer cases were identified through the Finnish Cancer Registry. For cases diagnosed through April 1999 medical records were reviewed centrally by two study oncologists for diagnostic confirmation and staging, and cases with histolopathologic or cytologic specimens available were also reviewed and confirmed by one or two pathologists Information on CRC cases diagnosed since May 1999 was derived only from the Finnish Cancer Registry |
Serum folate (nmol/L, median) Q1 (ref): 5.7 Q2: 7.2 Q3: 8.6 Q4: 10.0 Q5: 12.9 Serum folate and cobalamin were determined by radioassay |
Incident cases/controls Q1 (ref): 53/55 Q2: 50/55 Q3: 67/55 Q4: 41/55 Q5: 64/55 |
Age, BMI, occupational and leisure physical activity, intakes of vitamin D and iron |
Serum folate versus CRC risk. OR (95% CI) Q1 (ref): 1.00 Q2: 0.81 (0.44–1.47) Q3: 1.10 (0.63–1.90) Q4: 0.69 (0.35–1.33) Q5: 1.07 (0.60–1.91) p‐trend: 0.68 |
|
Cho et al. (2015) NHS, HPFS US NCC NHS: ⁓ 20 yrs HPFS: ⁓ 16 yrs Public |
N = NHS: 32,826 HPFS: 18,225 Population sampled NHS: female registered nurses aged 30–55 yrs HPFS: US male health professionals, aged 40–75 yrs Exclusion criteria: NR % lost to follow‐up: NR n = 617 cases, 1,207 controls Sex (% women) Cases: 55.7% Controls: 56.0% Age (mean) Cases: 62.0 Controls: 61.9 Matching criteria: Controls matched on age, year and month of blood donation, fasting status |
On each biennial questionnaire we inquired whether CRC had been diagnosed and, if so, the date of the diagnosis. Medical records were obtained from the cases and were reviewed by physicians who were blinded to questionnaire data |
UFA, (nmol/L, category cut‐offs) G1 (ref): Undetectable G2: <0.5 G3: ≥0.5 Plasma UFA level was measured using a liquid chromatography tandem mass spectrometry method (LC/MS/MS) |
Incident cases/controls: G1 (ref): 254/437 G2: 233/507 G3: 131/263 |
Model 1: Crude Model 2: Age, date of blood draw, sex, race, height, fasting status, smoking, BMI, physical activity, family history of CRC, history of colonoscopy or sigmoidoscopy, alcohol intake, intake of red and processed meat, vitamin D intake, calcium intake, aspirin use Stratified analysis by tumour site (colon, rectum, proximal, distal) |
UFA versus CRC risk OR (95% CI) Model 1 1 (ref): 1.00 2: 0.94 (0.67–1.31) 3: 1.01 (0.74–1.38) p‐trend: 0.71 Model 2 1 (ref): 1.00 2: 1.03 (0.73 to 1.46) 3: 1.12 (0.81 to 1.55) p‐trend: 0.32 |
|
Shrubsole et al. (2009) Shanghai Women's Health Study China NCC ⁓ 9 yrs Public |
N = 74,942 Population sampled: General female population Exclusion criteria: Previous history of cancer, unreasonably high or low energy intake or emigration from Shanghai shortly after baseline recruitment % lost to follow‐up: NR n = 72,861 Sex (% women): 100 Age: ranged from 40 to 70 yrs |
Cancer case data collected by the Shanghai Cancer Registry and death certificates collected by the Shanghai Municipal Center for Disease Control and Prevention |
Plasma folate (μg/mL) T1 (ref): 2.04–7.54 T2: 7.55–11.09 T3: 11.10–304.00 Baseline plasma folate levels were analysed using the microbiological assay |
N: Cases/controls T1 (ref): 96/396 T2: 95/396 T3: 112/396 |
Age, educational attainment, baseline household income, smoking status, drinking status, physical activity, hormone replacement therapy, menopausal status, family history of CRC, BMI, NSAID use, use of a B‐vitamin supplement, history of CR polyps, diabetes history, daily intakes of energy, vegetables, fruits, red meats and calcium |
T1: 1.0 (ref) T2: 1.0 (0.7–1.3) T3: 1.2 (0.8–1.7) p per tend = 0.30 |
|
Takata et al. (2014) Shanghai Men's Health Study China NCC 8 yrs Public |
N = 61,480 Population sampled: Men 40–74 yrs living in urban Shanghai, no prior history of cancer Exclusion criteria: Lacking blood and urine samples % lost to follow‐up: NR n = 288 cases, 575 controls Sex (% women): 0% Age (mean ± SD): Cases: 63.1 ± 8.7 Controls: 63.4 ± 8.6 Matching criteria: Controls matched on age, time of blood sample (morning/afternoon), use of vitamin supplement, time interval between last meal and time of blood collection, date of blood collection |
Participants' data files were linked to the Shanghai Vital Statistics Registry and Shanghai Cancer Registry databases annually. Cancer diagnoses were verified by review of medical charts |
Plasma folate (ng/mL): T1 (ref): <5.59 T2: 5.59–8.50 T3: ≥8.50 Folate concentrations in plasma samples were measured microbiologically using Lactobacillus casei |
Incident cases/controls Plasma folate T1 (ref): 83/192 T2: 108/192 T3: 97/191 |
Plasma folate: smoking status, income and CRP category Stratified analyses by tumour site, state, years from blood collection to diagnosis |
OR (95% CI) T1 (ref): 1.00 T2: 1.38 (0.95–2.02) T3: 1.33 (0.90–1.98) p‐trend: 0.15 |
Abbreviations: BMI, body mass index; CI, confidence Interval; CR, colorectal; CRC, colorectal Cancer; DE, Germany; DK, Denmark; EPIC, European Prospective Investigation into Cancer and Nutrition; ES, Spain; FR, France; GB, Great Britain; GR, Greece; HPFS, Health Professionals Follow‐up Study; HR, Hazard ratio; IQR, Interquartile range; IT, Italy; JPHC, Japan Public Health Center; MONICA, Northern Sweden WHO Monitoring of Trends and Cardiovascular Disease; MSP, Mammography Screening Project; NCC, Nested case–control; NHS, Nurses' Health Study; NL, The Netherlands; NR, not reported; OR, odds ratio; PC, prospective cohort; PHS, Physicians' Health Study; RBC, red blood cell; SD, standard deviation; SE, Sweden; SEER, surveillance, epidemiology and end results; UFA, Unmetabolised folic acid; VIP, Västerbotten Intervention Project; WHI‐OS, Women's Health Initiative Observational Study.
C.2.2b. Observational studies on mixed folate exposures (plasma, serum and/or diet) and incidence of colorectal cancer
|
Reference Study name Country Study design Follow‐up Funding |
Original cohort (N total) Exclusion criteria Study population |
Ascertainment of outcome |
Exposure groups n/person‐years Exposure assessment method |
Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Glynn et al. (1996) ATBC Cancer Prevention Study Finland NCC 5–8 yrs Mixed |
N = 29,133 Population sample: Middle‐aged men smoking ≥5 cigarettes/day Exclusion criteria: malignancies (except non‐melanoma skin cancer and in situ carcinoma), severe angina with exertion, chronic renal insufficiency, alcoholism, cirrhosis, anticoagulants or supplementation with B‐carotene or vitamin A or vitamin E in excess of defined amounts % lost to follow‐up: NR N = 144 cases, 276 controls (dietary intake, N = 136 cases, 249 controls) Sex (% women): 0 Age: 50–69 yrs Matching criteria: Controls (2:1) matched by age, study centre, month of blood collection |
Finnish Cancer Registry colon (ICD‐153) and rectal (ICD‐154) |
Serum folate (ng/mL), range: Q1 (ref): ≤2.9 Q2: 2.91–3.8 Q3: 3.81–5.2 Q4: >5.2 Total folate intake for incident colon cancer (median) (μg/day) Q1 (ref): 268 Q2: 308 Q3: 337 Q4: 388 N and person‐years: NR Serum folate was measured by Folate radioassay kit Dietary folate was measured using a food use questionnaire Energy‐adjusted: nutrient residual method |
Incident cases (N controls NR) Colon Q1 (ref): 19 Q2: 15 Q3: 31 Q4: 26 Rectum Q1 (ref): 12 Q2: 11 Q3: 17 Q4: 13 |
Serum Colon/Rectum Model 1 Contains serum folate alone. ORs adjusted for matching factors: age, clinic and time of blood collection Model 2 Includes serum folate, total energy intake and energy‐adjusted intakes of vitamin A and starch (residuals) Total folate intake Colon/Rectum Model 1 Includes total energy intake and energy‐adjusted intakes of total folate (residuals) Model 2 Includes physical activity during leisure, total energy intake and energy‐adjusted intakes of total folate, vitamin A and starch (residuals) Interactions by alcohol‐protein‐folate status reported |
Serum folate versus Colon cancer OR (95% CI) Model 1 Q1: 1.0 (ref) Q2: 0.67 (0.30–1.50) Q3: 1.26 (0.57–2.78) Q4: 0.92 (0.42–2.00) p per tend = 0.87 Model 2 Q1: 1.0 (ref) Q2: 0.61 (0.25–1.45) Q3:1.25 (0.50–3.17) Q4: 0.96 (0.40–2.30) p per tend = 0.83 Serum folate versus rectum cancer OR (95% CI) Model 1 Q1: 1.0 (ref) Q2: 1.88 (0.74–4.81) Q3: 1.78 (0.70–4.54) Q4: 2.04 (0.81–5.15) p per tend = 0.15 Model 2 Q1: 1.0 (ref) Q2: 2.21 (0.65–7.48) Q3: 2.43 (0.72–8.19) Q4: 2.94 (0.84–10.33) p per tend = 0.10 Total folate intake versus Colon cancer OR (95% CI) Model 1 Q1: 1.0 (ref) Q2: 0.47 (0.21–1.03) Q3: 0.47 (0.22–1.01) Q4: 0.52 (0.24–1.12) p per tend = 0.07 Model 2 Q1: 1.0 (ref) Q2: 0.40 (0.16–0.96) Q3: 0.34 (0.13–0.88) Q4: 0.51 (0.20–1.31) p per tend = 0.15 |
|
Total folate intake versus rectum cancer OR (95% CI) Model 1 Q1: 1.0 (ref) Q2: 0.53 (0.16–1‐76) Q3: 1.17 (0.46–2.95) Q4: 1.13 (0.43–10.54) p per tend = 0.66 Model 2 Q1: 1.0 (ref) Q2: 0.50 (0.11–2.32) Q3: 1.78 (0.42–7.59) Q4: 2.12 (0.43–10.54) p per tend = 0.26 |
||||||
|
Kato et al. (1999) New York University Women's Health Study US NCC 9 yrs Public |
N = 15,785 Population sampled: Women, 34–65 yrs, who in the preceding 6 months had neither used hormonal medications nor been pregnant Exclusion criteria: NR % lost to follow‐up: NR N = 150 cases, 523 controls Sex (% women): 100% Age at baseline mean ± SD: Cases: 61.6 ± 7.5 Controls: 61.6 ± 7.4 |
Mailed questionnaires in order to identify incident cases of cancer diagnosed prior to 1995. If subject did not respond they were phoned. Medical records were obtained from hospitals and reviewed to confirm pathological diagnoses for self‐reported cancer. Record linkage with state cancer registries in New York, New Jersey and Connecticut and with the National Death Index supplemented the active follow‐up |
Serum folate (nmol/L) Q1: ≤12.23 Q2: 12.24–19.25 Q3: 19.26–31.03 Q4: >31.04 Total folate intake (μg/day) Q1: ≤224 Q2: 225–413 Q3: 414–625 Q4: >626 Serum folate was measured using an automated clinical immunoassay analyser Dietary folate intake by self‐administered, semi‐quantitative diet questionnaire Energy‐adjusted: no |
Incident cases NR by quartile |
Model 1: Unadjusted Model 2: Adjusted for family history of CRC, beer intake, prior occult blood testing and number of hours spent in sport activities in their early 30s. Energy intake was tested, but not considered a confounder |
Serum folate versus CRC OR (95% CI) Model 1: Q1 (ref): 1.00 Q2: 0.66 (0.38–1.17) Q3: 0.60 (0.34–1.06) Q4: 0.45 (0.25–0.85) p‐trend: 0.01 Model 2: Q1 (ref): 1.00 Q2: 0.67 (0.37–1.23) Q3: 0.66 (0.36–1.21) Q4: 0.52 (0.27–0.97) p‐trend: 0.04 Total folate intake versus CRC Model 1: Q1 (ref): 1.00 Q2: 0.78 (0.42–1.44) Q3: 0.70 (0.38–1.29) Q4: 0.67 (0.36–1.23) p‐trend: 0.17 Model 2: Q1 (ref): 1.00 Q2: 0.92 (0.48–1.74) Q3: 0.87 (0.45–1.70) Q4: 0.88 (0.46–1.69) p‐trend: 0.067 |
Abbreviations: CI, Confidence Interval; CRC, Colorectal Cancer; NCC, Nested case–control; NR, Not reported; OR, Odds ratio; SD, Standard deviation; yrs, years.
C.2.2c. Observational studies on dietary folate and incidence of colorectal cancer
|
Reference Study name Country Study design Follow‐up Funding |
Original cohort (N total) Exclusion criteria Study population |
Ascertainment of outcome |
Exposure groups n/person‐years Exposure assessment method |
Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Zschäbitz et al. (2013) WHI‐OS US PC 11 yrs (median) Public |
N = 93,676 Population sampled: Post‐menopausal women, 50–79 yrs, unlikely to die of a pre‐existing medical condition within 3 yrs Exclusion criteria: History of CRC at enrolment, no follow‐up, diagnosed in situ CRC during follow‐up, death certificate only report of CRC, extreme reported dietary intake, extreme BMI % lost to follow‐up: 4% n = 88,045 Sex (% women): 100% Age (mean ± SD) Q1: 62.9 ± 7.5 Q2: 63.4 ± 7.4 Q3: 63.6 ± 7.4 Q4: 64.2 ± 7.1 |
Clinical outcomes were reported annually by self‐administered medical history update questionnaires and a clinic follow‐up visit in year 3. Medical records were centrally reviewed, and major diagnoses were confirmed by physician adjudicators |
Dietary folate (DFE, min‐max) Q1 (ref): <189 Q2: 189–252 Q3: 252–343 Q4: ≥343 Supplemental folic acid (μg, min‐max) G1 (ref): 0 G2: 0–400 G3: >400 Total folate intake (DFE, min‐max) Q1 (ref): <242 Q2: 242–542 Q3: 542–939 Q4: >939 Self‐administered FFQ developed specifically for WHI. Energy‐adjusted: no |
Incident cases for model 2: Dietary folate Q1 (ref): 221 Q2: 194 Q3: 216 Q4: 177 Supplemental folic acid G1 (ref): 425 G2: 341 G3: 42 Total folate intake Q1 (ref): 218 Q2: 199 Q3: 204 Q4: 187 |
Model 1: Age Model 2: Age, BMI, race‐ethnicity, past medical history of colonoscopy, smoking status, physical activity, post‐menopausal hormone use Additional models segmenting by tumour stage, time since exposure to folic acid fortification and alcohol use have not been extracted. Energy intake was tested, but not considered a confounder |
HR (95% CI) Dietary folate versus CRC Model 1 Q1 (ref): 1.00 Q2: 0.87 (0.72, 1.04) Q3: 0.92 (0.76, 1.10) Q4: 0.79 (0.65, 0.96) P‐trend: 0.03 Model 2 Q1 (ref): 1.00 Q2: 0.86 (0.71, 1.05) Q3: 0.96 (0.80, 1.17) Q4: 0.83 (0.68, 1.01) p‐trend: 0.14 Supplemental folic acid versus CRC Model 1 G1 (ref): 1.00 G2: 0.88 (0.76, 1.01) G3: 0.90 (0.66, 1.23) p‐trend: 0.10 Model 2 G1 (ref): 1.00 G2: 0.94 (0.81, 1.09) G3: 1.01 (0.74, 1.39) p‐trend: 0.59 Total folate intake versus CRC Model 1 Q1 (ref): 1.00 Q2: 0.88 (0.73, 1.06) Q3: 0.88 (0.73, 1.06) Q4: 0.81 (0.66, 0.97) p‐trend: 0.06 Model 2 Q1 (ref): 1.00 Q2: 0.92 (0.76, 1.12) Q3: 0.96 (0.79, 1.16) Q4: 0.90 (0.74, 1.10) p‐trend: 0.51 |
|
Flood et al. (2002) Breast Cancer Detection Demonstration Project (BCDDP) Follow‐up cohort US PC 8.5 yrs Public |
N = 64,182 Population sampled: Women diagnosed with breast cancer or with biopsies showing benign breast disease or recommended for biopsy or breast surgery, plus controls matched on age, time of enrolment, ethnicity, screening centre and length of participation in the BCDDP. Exclusion criteria: Incomplete FFQ (30 skipped items), extreme reported energy intakes, unusually high intakes of folate and alcohol % lost to follow‐up: NR n = 45,264 Sex (% women): 100% Age (mean, range): 61.9 yrs, 40–93 |
Case ascertainment through self‐reports, pathology reports, National Death Index and state cancer registries. Women with pathology reports contradicting self‐reported CRC were not included as cases |
Total folate, energy‐adjusted dietary folate intake (the residual of dietary folate regressed on energy plus mean value for dietary folate in the analytic cohort) + intake of folate from supplements. (μg, range) Q1 (ref): <188 Q2: 188–253 Q3: 254–374 Q4: 375–633 Q5: >633 62‐item Block/NCI FFQ to assess usual intake over the previous year Energy‐adjusted: multivariate nutrient density method |
Incident cases/participants Q1 (ref): 93/9053 Q2: 93/9053 Q3: 94/9053 Q4: 101/9053 Q5:109/9052 |
Model 1: Energy Model 2 Energy, methionine, alcohol and total fat Interaction terms tested: Alcohol and methionine intakes |
RR (95% CI) Model 1 Q1 (ref): 1.0 Q2: 0.94 (0.70–1.25) Q3: 0.90 (0.67–1.19) Q4: 0.98 (0.74–1.30) Q5: 1.02 (0.77–1.35) P‐trend: 0.63 Model 2 Q1 (ref): 1.0 Q2: 0.94 (0.70–1.25) Q3: 0.89 (0.66–1.20) Q4: 0.97 (0.73–1.30) Q5: 1.01 (0.75–1.35) p‐trend: 0.67 |
|
Lee et al. (2011) NHS, HPFS US PC ⁓ 24 yrs Public |
N = NHS: 121,700 HPFS: 51,529 Population sampled: NHS: Registered nurses, 30–55 yrs old. HPFS: Male health professionals aged 40–75 yrs Exclusion criteria: No FFQ, previous cancer diagnosis, extreme caloric intake, extensive number of FFQ questions unanswered, had ulcerative colitis. % lost to follow‐up: NR n = NHS: 87,861 HPFS: 47,290 Sex (% women): 65% Age: NR |
Self‐reported diagnoses confirmed by medical records. The National Death Index was also used to identify fatalities |
Total folate (μg/day, min‐max) Q1 (ref): <250 Q2: 250–400 Q3: 400–600 Q4: 600–800 Q5: 800+ Dietary folate (natural + fortified) intake Q1 (ref): <250 Q2: 250–300 Q3: 300–400 Q4: 400–500 Q5: ≥500 Synthetic folic acid intake (supplements + fortified) (μg/day) Q1 (ref): <50 Q2: 50–100 Q3: 100–200 Q4: 200–400 Q5: ≥400 FFQ Energy‐adjusted: nutrient residual method |
Incident cases: NHS: 1312 HPFS: 987 Not reported by quintile. |
Age, calendar year, smoking, physical activity, aspirin dose, height, BMI, family history of CRC, menopausal status, hormone therapy use, history of endoscopy, red meat intake, alcohol intake, calcium intake from foods, total energy intake. Analysis also stratified by lag‐time between FFQ and diagnoses. Results not extracted |
RR (95% CI) Data extracted for the model on cumulative average exposure. Total folate intake versus CRC: Q1 (ref): 1.00 Q2: 0.95 (0.81, 1.12) Q3: 0.90 (0.78, 1.04) Q4: 0.84 (0.70, 1.00) Q5: 0.85 (0.68, 1.08) p‐trend: 0.07 p for heterogeneity: 0.50 Dietary folate intake versus CRC: Q1 (ref): 1.00 Q2: 1.07 (0.94, 1.22) Q3: 1.02 (0.89, 1.15) Q4: 1.00 (0.83, 1.21) Q5: 1.07 (0.82, 1.38) p‐trend: 0.92 p for heterogeneity: 0.99 Synthetic folic acid versus CRC: Q1 (ref): 1.00 Q2: 0.89 (0.77, 1.02) Q3: 0.97 (0.86, 1.10) Q4: 0.89 (0.78, 1.00) Q5: 0.93 (0.81, 1.06) p‐trend: 0.26 p for heterogeneity: 0.75 |
|
Razzak et al. (2012) Iowa Women's Health Study US PC ⁓18 yrs Public |
N = 41,836 Population sampled: General population, female, 55–69 yrs, living in Iowa, with a valid driver's license Exclusion criteria: follow‐up <1 day, history of malignancy other than non‐melanoma skin cancer, incomplete/implausible dietary intake n = 35,216% lost to follow‐up: ⁓1% per year Sex (% women): 100% Age (mean, SD): Q1: 61.8 (4.2) Q2: 62.0 (4.2) Q3: 62.1 (4.2) Q4: 62.1 (4.2) |
Incident CRC cases were identified through annual linkage with the Iowa Cancer Registry |
Total folate intake (μg/day, min‐max) Q1 (ref): ≤251.0 Q2: 251.1–350.7 Q3: 350.8–573.4 Q4: ≥573.5 Person‐years: Q1 (ref): 142,477 Q2: 143,152 Q3: 142,999 Q4: 141,705 Dietary habits were assessed using a semiquantitative FFQ adapted from a 126‐item instrument developed by Willett and colleagues. Energy‐adjusted: no |
Incident cases Q1 (ref): 352 Q2: 358 Q3: 300 Q4: 288 |
Age, BMI, waist‐to‐hip ratio, smoking status, exogenous estrogen use, physical activity level, history of diabetes mellitus and daily intakes of total energy, total fat, sucrose, red meat, calcium, vitamin E, alcohol. Analysis also stratified by tumour site (proximal, distal) and moleculary defined subtypes (microsatellite instability, BRAF, KRAS). Results not extracted |
RR (95% CI) Total folate intake versus CRC: Q1 (ref): 1.00 Q2: 1.04 (0.88–1.24) Q3: 0.91 (0.74–1.10) Q4: 0.95 (0.76–1.20) p for trend: 0.46 |
|
Gibson et al. (2011) NIH‐AARP Diet and Health Study US PC 9.1 yrs Public |
N = 525,488 Population sampled: AARP members in selected states, male and female, 50–71 yrs Exclusion criteria: Proxy respondents, colon cancer, end‐stage renal disease, any cancer diagnosis except non‐melanoma skin cancer, cancer as cause of death but no cancer registry record, extreme total energy intake, extreme folate intakes. n = NR % lost to follow‐up: NR Sex (% women): Q1: 35.5% Q3: 42.8% Q5: 46.0% Age (mean ± SD): Q1: 61.6 ± 0.02 Q3: 61.9 ± 0.02 Q5: 62.5 ± 0.02 |
Incident CRC cases were identified by using probabilistic linkage with state and metropolitan area cancer registries. Information on anatomic site and histology was obtained via the cancer registries, and the vital status of all participants was updated annually by linkage to the Social Security Administration Death Master File and the cancer registries |
Total folate intake (μg/d, min‐max) (diet+supplemental intake): 1 (ref): <200 (ref) 2: 200–300 3: 300–400 4: 400–500 5: 500–600 6: 600–700 7: 700–800 8: 800–900 9: ≥900 Total folate intake (μg/d, min‐max) (diet+supplemental intake): 1 (ref): <200 (ref) 2: 200–300 3: 300–400 4: 400–500 5: 500–600 6: ≥600 Supplemental folic acid intake (μg/day, min‐max): 1 (ref): 0 (ref) 2:<400 3: 400 4:>400 Self‐administered, grid‐based version of the National Cancer Institute's DHQ Energy‐adjusted: nutrient residual method |
Incident cases: Total folate intake: Pre‐fortification period (baseline to 30 June 1997) 1: 77 2: 141 3: 109 4: 57 5: 64 6: 133 7: 85 8: 27 9: 35 Post‐fortification period (beginning on 1 July 1997) 1: 145 2: 773 3: 1289 4: 885 5: 483 6: 641 7: 949 8: 704 9: 615 Dietary folate intake: Post‐fortification period (beginning on 1 July 1997) 1: 243 2: 1359 3: 2389 4: 1605 5: 629 6: 259 |
Model 1: Unadjusted Model 2: sex, smoking, physical activity, use of aspirin/NSAIDs, BMI, dietary calcium and red meat intakes Dietary intake energy‐adjusted, residual method. Analysis also stratified by dietary (natural + fortified) and supplemental folic acid. Results not extracted |
RR (95% CI): Pre‐fortification period Model 1 1 (ref): 1.00 2: 0.79 (0.60, 1.04) 3: 0.80 (0.60, 1.07) 4: 0.87 (0.62, 1.23) 5: 0.78 (0.56, 1.09) 6: 0.86 (0.65, 1.14) 7: 0.70 (0.51, 0.95) 8: 0.58 (0.37, 0.90) 9: 0.58 (0.39, 0.87) p‐trend: 0.01 Model 2 1 (ref): 1.00 2: 0.85 (0.64, 1.13) 3: 0.94 (0.70, 1.28) 4: 1.06 (0.75, 1.51) 5: 0.90 (0.64, 1.26) 6: 1.03 (0.77, 1.38) 7: 0.90 (0.65, 1.24) 8: 0.78 (0.49, 1.23) 9: 0.74 (0.49, 1.11) p‐trend: 0.47 Post‐fortification period Total folate Model 1 1 (ref): 1.00 2: 0.89 (0.74, 1.06) 3: 0.75 (0.63, 0.89) 4: 0.64 (0.53, 0.76) 5: 0.62 (0.52, 0.75) 6: 0.67 (0.56, 0.80) 7: 0.63 (0.52, 0.74) 8: 0.59 (0.49, 0.70) 9: 0.54 (0.45, 0.64) p‐trend: <0.001 Model 2 1 (ref): 1.00 2: 0.90 (0.76, 1.08) 3: 0.82 (0.69, 0.98) 4: 0.75 (0.63, 0.90) 5: 0.75 (0.62, 0.90) 6: 0.77 (0.64, 0.92) 7: 0.75 (0.63, 0.89) 8: 0.75 (0.62, 0.90) 9: 0.70 (0.58, 0.84) p‐trend: <0.001 |
|
Dietary folate folate Model 2 1 (ref): 1.00 2: 0.92 (0.80, 1.06) 3: 0.86 (0.75, 0.98) 4: 0.81 (0.70, 0.93) 5: 0.86 (0.74, 1.00) 6: 0.81 (0.67, 0.97) p‐trend: 0.003 Supplemental folic acid intake Model 2 1 (ref): 1.00 2: 0.93 (0.86, 1.01) 3: 0.91 (0.86, 0.96) 4: 0.82 (0.72, 0.92) |
||||||
|
Le Marchand et al. (2005) Multiethnic Cohort Study US NCC Follow‐up duration: NR Public |
N = 96,810 men, 118,441 women Population sampled: 45–75 yrs, Japanese American (26%) White (23%), Latino (22%), African American (16%), Native Hawaiian (7%) and other ethnic/racial origin (6%) Exclusion criteria: NR n = 822 cases, 2,021 controls % lost to follow‐up: NR Sex (% women) Cases: 44.3% Controls: 43.9% Age (mean, SD) Cases: 63.5, 7.7 Controls: 59.4, 8.7 A sample of cohort participants was randomly selected to serve as controls at the onset of the nested case–control study. The selection was stratified by sex, race/ethnicity |
CRC cases were identified through the Rapid Reporting System of the Hawaii Tumour Registry, the Los Angeles County Cancer Surveillance Program and two cancer registries that are members of the SEER program of the National Cancer Institute. Complemented by annual linkages to the State of California's cancer registry |
Total folate intake (μg/day, min‐max) T1 (ref): <322 T2: 322–590 T3: >590 The FFQ asked about the frequency and amount of consumption for >140 food items during the last year Energy‐adjusted: no |
Incident cases by MTHFR genotype and folate source Folate from foods CC T1 (ref): 0 T2: 119 T3: 124 CT T1: 112 T2: 107 T3: 111 TT T1: 25 T2: 32 T3: 26 Folate from foods and supplements CC T1 (ref): 141 T2: 123 T3: 119 CT T1: 123 T2: 98 T3: 109 TT T1: 26 T2: 35 T3: 22 |
Age at blood draw, sex, race/ethnicity |
OR (95% CI) folate intake and MTHFR genotype vs. CRC risk Total folate intake CC T1 (ref): 1.00 T2: 0.84 (0.62–1.13) T3: 0.69 (0.51–0.94) CT T1: 0.95 (0.70–1.30) T2: 0.79 (0.57–1.09) T3: 0.79 (0.57–1.08) TT T1: 0.74 (0.44–1.23) T2: 0.90 (0.57–1.44) T3: 0.39 (0.23–0.65) p‐interaction: 0.22 |
|
Roswall et al. (2010) Diet, Cancer and Health study Denmark PC 9–13 yrs Public |
N = 57,053 Population sampled: 50–64 yrs, residence in the greater Copenhagen or Aarhus area and no previous cancer diagnosis in the Danish Cancer Registry Exclusion criteria: Cancer diagnosis before baseline and missing information on one or more confounders or exposure n = 56,332% lost to follow‐up: NR Sex (% women): 52.3% Age (median): 56.2 |
CRC cases during follow‐up were identified by linkage to the Danish Cancer Registry |
Total folate intake (μg/d, min‐max) Colon cancer Q1 (ref): ≤273.71 Q2: >273.71–≤350.73 Q3: >350.73–≤441.66 Q4: >441.66 Rectal cancer Q1 (ref): ≤282.80 Q2: 282.80–362.55 Q3: 62.55–461.22 Q4: >461.22 Supplemental folic acid intake (μg/d, min‐max) Colon cancer Q1 (ref): 0 Q2: >0–≤83.2 Q3: >83.2–≤142.8 Q4: >142.8 Rectal cancer Q1 (ref): 0 Q2: >0– ≤83.2 Q3: >83.2–≤133.2 Q4: >133.2 192‐item FFQ mailed to each participant, which considered food intake during the past 12 months. Energy‐adjusted: no |
Incident cases Colon: 465 Rectal: 283 |
Intakes of vitamin C, E, beta‐carotene. BMI, education, alcohol, red meat intake, processed meat intake, smoking status, leisure time physical activity, calcium consumption, HRT use (among women only). Stratified analysis by natural, dietary (natural + fortified), synthetic FA (supplement + fortified), alcohol intake not extracted |
IRR (95% CI) Total folate intake vs. colon cancer: Q1 (ref): 1.00 Q2: 0.83 (0.63–1.10) Q3: 0.78 (0.57–1.07) Q4: 0.67 (0.46–1.00) p‐trend: 0.23 Continuous folate vs. colon cancer, Crude: 0.91 (0.85–0.97) Adjusted: 0.94 (0.85–1.04) Total folate intake vs. rectal cancer: Q1 (ref): 1.00 Q2: 0.95 (0.67–1.34) Q3: 0.95 (0.64–1.39) Q4: 1.06 (0.67–1.70) p‐trend: 0.46 Continuous folate vs. rectal cancer, Crude: 0.93 (0.85–1.01) Adjusted: 0.95 (0.83–1.09) Supplemental folic acid intake vs. colon cancer: (adjusted for dietary folate intake) Q1 (ref): 1.00 Q2: 0.79 (0.55–1.13) Q3: 0.90 (0.61–1.30) Q4: 0.83 (0.58–1.20) p‐trend: 0.76 Supplemental folic acid intake vs. rectal cancer: (adjusted for dietary folate intake) Q1 (ref): 1.00 Q2: 0.56 (0.34–0.91) Q3: 0.82 (0.51–1.33) Q4: 0.60 (0.36–0.99) p‐trend: 0.83 |
|
Wang, Wu, et al. (2021) NHS US PC 36 yrs Public |
N = 121,700 Population sampled: Female registered nurses 30–55 yrs Exclusion criteria: Incomplete FFQ, missing info on folate intake, implausible energy intake levels, missing info on height, birthday. Previous diagnosis of cancer (except non‐melanoma skin cancer) or ulcerative colitis. n = 86,320% lost to follow‐up: ∼10% Sex (% women): 100% Age (mean) Pre‐fortification Q1: 45 Q3 47 Q5: 47 Post‐fortification Q1: 63 Q3: 63 Q5: 64 |
Self‐reported information on the diagnosis of CRC was collected with biennial questionnaires. Participants who reported a diagnosis of CRC or next‐of‐kin who reported for participants who died were contacted for permission to review their medical records. We identified deaths using information from next‐of‐kin, death certificates and the National Death Index. |
Total folate (DFE/d, mean) Pre‐fortification Q1 (ref): 189 Q3: 377 Q5: 1126 Post‐fortification Q1 (ref): 432 Q3: 1073 Q5: 1745 Person‐years Pre‐fortification Q1 (ref): 301,168 Q3: 299,454 Q5: 299,524 Post‐fortification Q1 (ref): 216,011 Q3: 214,542 Q5: 214,346 Dietary information was collected via validated semiquantitative FFQs in 1980,1984, 1986 and every 4 yrs thereafter. Participants were asked how frequently, on average, they had consumed 1 standard serving of a specific food item during the past yr Energy‐adjusted: nutrient residual method |
Incident cases Baseline (Folate intake from baseline FFQ) 1,988 Cumulative (average folate intake across follow‐up period) 1,988 Simple update (folate intake from most recent FFQ) 1,687 |
Age, calendar year of the current questionnaire cycle, family history of CRC, endoscopy, height, BMI, pack‐y of smoking before age 30 yrs, physical activity, duration of regular aspirin or other NSAIDs use, menopausal status, menopausal hormone use, alcohol intake, total energy, dietary fibre, total vitamin D, total calcium, red meat and processed meat Additional analyses stratified by dietary folate, synthetic folic acid; by FFQ reporting lag; and by pre‐/post‐ fortification periods not extracted |
HR (95% CI) Data extracted for the model on cumulative average exposure. Total folate intake vs. CRC risk Q1 (ref): 1.00 Q2: 1.06 (0.91, 1.24) Q3: 1.11 (0.94, 1.30) Q4: 1.02 (0.85, 1.23) Q5: 0.92 (0.73, 1.15) p‐trend: 0.50 Per 400 μg DFE/d: 0.97 (0.88, 1.07) |
|
Stevens et al. (2011) Cancer Prevention Study II (CPS‐II) Nutrition Cohort US PC ⁓8 yrs Public |
N = 151,348 Population sampled: 21 states, 50–74 yrs Exclusion criteria: Lost to follow‐up, prevalent cancer other than non‐melanoma skin cancer, self‐reported and not verified CRC, non‐adenocarcinoma CRCs, missing dietary or supplement data, extreme BMI n = 99,523% lost to follow‐up: 3.8% Sex (% women): 56% Age (years): Women: 68.2–68.9 Men: 70–70.5 |
Cases identified through self‐report on the follow‐up questionnaires and verified through medical records or linkage with state cancer registries and fatal cases identified through linkage with the National Death Index |
Total folate intake (DFE/d) Q1 (ref): <422 Q2: 422–598 Q3: 598–1030 Q4: 1030–1224 Q5: ≥1224 Person‐years Q1 (ref): 88,778 Q2: 93,508 Q3: 97,990 Q4: 102,115 Q5: 102,918 Dietary folate (natural + fortified) (μg/d): Q1: <297 Q2: 297–343 Q3: 343–387 Q4: 387–446 Q5: ≥446 Person‐years: Q1: 90,989 Q2: 94,162 Q3: 97,929 Q4: 99,817 Q5: 102,411 Folic acid intake (μg/d): Q1: <101 Q2: 101– <182 Q3: 182– <452 Q4: 452– <560 Q5: ≥560 Person‐years: Q1: 88,466 Q2: 94,366 Q3: 98,209 Q4: 102,183 Q5: 102,084 152‐item, semi‐quantitative, modified Willett FFQ /previous year Energy‐adjusted: nutrient residual method |
Incident cases Total folate: Q1 (ref): 254 Q2: 217 Q3: 201 Q4: 178 Q5: 173 Dietary folate: Q1 (ref): 242 Q2: 196 Q3: 202 Q4: 202 Q5: 181 |
Age, sex, alcohol use, race, smoking status, education, NDAIDs use, BMI, family history of CRC, history of colorectal endoscopy, diabetes, post‐menopausal hormone use, low fat dairy intake, red meat consumption, total energy intake, sex Results also stratified by gender (men, women) and for natural folate and synthetic folic acid (supplement + fortified). Results not extracted. |
RR (95% CI) Total folate intake vs. CRC risk Q1 (ref): 1.00 Q2: 0.91 (0.75–1.09) Q3: 0.92 (0.76–1.11) Q4: 0.86 (0.70–1.04) Q5: 0.81 (0.66–0.99) p‐trend: 0.047 Dietary folate intake vs. CRC risk Q1 (ref): 1.0 Q2: 0.85 (0.70–1.02) Q3: 0.89 (0.73–1.08) Q4: 0.90 (0.74–1.09) Q5: 0.81 (0.66–0.99) p for trend: 0.10 Folic acid intake vs. CRC risk Q1 (ref): 1.0 Q2: 1.03 (0.86–1.24) Q3: 0.95 (0.78–1.16) Q4: 0.96 (0.79–1.18) Q5: 0.84 (0.68–1.03) p for trend: 0.12 |
|
Zhang et al. (2006) Women's Health Study US PC 10.1 yrs Public |
N = 39,345 Population sampled: Female US health professionals aged ≥45 yrs, free of cancer and CVD and enrolled in an RCT: low‐dose aspirin and vitamin E for cancer/CVD prevention. Exclusion criteria: No dietary information, implausible total energy intakes, no info on multivitamin supplements, newly diagnosed non‐adenocarcinoma CRC n = 37,916% lost to follow‐up: NR Sex (% women): 100% Age (mean) Q1: 52.9 Q3: 54.2 Q5: 54.5 |
Every 6 months during the first yr of follow‐up and then annually thereafter, questionnaires were sent about newly diagnosed diseases, including colon or rectal cancer, and other clinical endpoints. Deaths of participants were identified through reports from family members, postal authorities and a search of the National Death Index For participants who reported a CRC diagnosis and for those deceased, medical records and other relevant information were sought |
Total folate intake (μg/day) Q1 (ref):<259 Q2: 259–317 Q3: 317–392 Q4: 392–614 Q5: ≥614 131‐item FFQ, a format that has been used in the NHS. The questionnaire assessed average consumption over the past year of a specific amount of each food. Energy‐adjusted: nutrient residual method |
Incident cases: Total folate: Q1 (ref): 38 Q2: 46 Q3: 40 Q4: 44 Q5: 52 |
Model 1: Age, randomised treatment assignment Model 2: model 1 + BMI, family history of CRC in a first‐degree relative, history of colon polyps, physical activity, smoking status, red meat intake, alcohol consumption, total energy intake, menopausal status, baseline post‐menopausal hormone use, baseline aspirin use. Stratified analysis by supplement use not extracted |
RR (95% CI) Total folate intake vs. CRC risk Model 1 Q1 (ref): 1.00 Q2: 1.13 (0.74, 1.74) Q3: 0.93 (0.60, 1.45) Q4: 1.01 (0.65, 1.56) Q5: 1.17 (0.77, 1.78) p‐trend: 0.46 Model 2 Q1 (ref): 1.00 Q2: 1.10 (0.71, 1.70) Q3: 0.91(0.58, 1.44) Q4: 0.97(0.62, 1.52) Q5: 1.16(0.76, 1.79) p‐trend: 0.46 |
|
Kim et al. (2010) Pooled analysis: BCDDP, CPS2_f, CPS2_m, HPFS, IWHS, NYS_f NYS_m, NYUWHS, NHSa, NHSb, WHS US PC BCDDP: 11 yrs CPS2_f: 7 yrs CPS2_m: 6 yrs HPFS: 14 yrs IWHS: 15 yrs NLCS_f: 7 yrs NLCS_m: 7 yrs NYS_f: 7 yrs NYS_m: 7 yrs NYUWHS: 13 yrs NHSa: 6 years NHSb: 14 yrs WHS: 10 yrs Public |
Populations sampled: NR Exclusion criteria: Loge‐transformed energy intakes beyond 3SD from loge‐transformed mean of the baseline population of each study or who had a history of cancer (except non‐melanoma skin cancer) at baseline. n = 725,134 BCDDP: 41,987 CPS2_f: 74,046 CPS2_m: 66,071 HPFS: 47,766 IWHS: 34,588 NNYS_f: 22,550 NYS_m: 30,363 NYUWHS: 13,258 NHSa: 88,651 NHSb: 68,502 WHS: 38,384% lost to follow‐up: NR Sex (% women): 68% Age: NR |
Each study ascertained incident CRC using follow‐up questionnaires and subsequent medical record review, linkage with a cancer registry or both. In addition, some studies used linkage with a death registry. |
Total folate intake Q1, Q5 (μg/day, median) BCDDP: 200, 835 CPS2_f: 181, 779 CPS2_m: 212, 777 HPFS: 255, 827 IWHS: 178, 679 NYS_f: 289, 861 NYS_m: 307, 874 NYUWHS: 183, 770 NHSa: 159, 667 NHSb: 202, 709 WHS: 211, 706 Diet was assessed at baseline in each study with a study‐specific food frequency questionnaire. Energy‐adjusted: nutrient residual method |
Incident cases, colon cancer (pooled) Q1 (ref): 801 Q2: 808 Q3: 757 Q4: 752 Q5: 710 |
Model 1: Age Model 2: Age, education, BMI, height, smoking, energy intake, alcohol intake, red meat intake, multi‐vitamin use, family history of CRC, NSAID use, physical activity and among women: oral contraceptive use and use of post‐menopausal hormone therapy. Multivariate analyses with dietary folate (natural in some studies and natural + fortified in others), alcohol, smoking, methionine intake and by tumour site not extracted. |
RR (95% CI) Total folate intake vs. CRC risk Model 1 Q1 (ref): 1.00 Q2: 0.94 (0.85–1.04) Q3: 0.85 (0.77–0.94) Q4: 0.85 (0.77–0.94) Q5: 0.78 (0.70–0.86) p‐trend: < 0.001 Model 2 Q1 (ref): 1.00 Q2: 0.98 (0.88–1.08) Q3: 0.90 (0.81–1.00) Q4: 0.92 (0.83–1.01) Q5: 0.85 (0.77–0.95) p‐trend: 0.02 Women, Model 2 Q1 (ref): 1.00 Q2: 0.97 (0.86–1.09) Q3: 0.92 (0.81–1.04) Q4: 0.92 (0.81–1.04) Q5: 0.89 (0.78–1.01) p‐trend: 0.75 Men, Model 2 Q1 (ref): 1.00 Q2: 0.99 (0.81–1.21) Q3: 0.87 (0.72–1.03) Q4: 0.90 (0.75–1.08) Q5: 0.77 (0.57–1.03) p‐trend: 0.06 |
Abbreviations: BMI, body mass index; CI, confidence Interval; CRC, colorectal Cancer; DFE, dietary folate equivalent; FFQ, Food frequency questionnaire; HPFS, Health Professionals Follow‐up Study; HR, hazard ratio; IQR, interquartile range; MTHFR, methylenetetrahydrofolate reductase; NCC, nested case–control; NHS, Nurses' Health Study; NR, not reported; OR, odds ratio; PC, prospective cohort; SD, standard deviation; WHI‐OS, Women's Health Initiative Observational Study; yrs, years.
C.2.2d. Observational study on folate biomarkers and incidence of recurrent colorectal adenomas
| Reference Study name Country Study design Follow‐up Funding | Original cohort (N total) Exclusion criteria Study population | Ascertainment of outcome | Exposure groups n/person‐years Exposure assessment method | Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Martínez et al. (2006) WBF and UDCA US 2 RCTs used as a cohort study WBF: 3.06 yrs UDCA: 2.6 yrs Public |
N = WBF: 1429 UDCA: 1285 Population sampled: 40–80 yrs who had had ≥1 colorectal adenoma measuring ≥3 mm removed at colonoscopy within 3 months before study entry Exclusion criteria: History of previous polyps prior to qualifying colonoscopy, history of CRC in sibling or parent, presence of any adenoma ≥1 cm in size, presence of any tubuvillous or villous adenoma, presence of any proximal adenoma % lost to follow‐up: WBF: 8.8% UDCA: 13% N = WBF: 1014 UDCA: 1111 Sex (% women): WBF: 30% UDCA: 32.6% Age at baseline mean (SD): WBF: 65.3 ± 9 UDCA: 66.2 ± 8.5 |
Data on adenoma characteristics were obtained from medical record review and the pathology reports. Dietary intake was assessed by FFQ that contained a vitamin/mineral section which ascertains current regular use of multiple vitamin preparations and supplements. WBF: Plasma folate was assessed by Radioassay method UDCA: Plasma folate was assessed by the IMMULITE folic acid analysis kit/ immunoassay method |
Unit of measurement Plasma folate (nmol/L) Total population (n = 2125) Q1: <7.20 Q2: 7.20–11.21 Q3: 11.22–15.38 Q4: >15.38 Nonmultivitamin users (n = 1140): Q1: <5.40 Q2: 5.40–8.29 Q3: 8.30–11.90 Q4: >11.90 Multivitamin users (n = 985) Q1: <11.06 Q2: 11.06–14.60 Q3: 14.68–18.10 Q4: >18.10 |
Incident recurrence/total Total population (n = 2125) Q1: 261/530 Q2: 242/532 Q3: 244/532 Q4: 218/531 Nonmultivitamin users (n = 1140) Q1: 147/286 Q2: 141/284 Q3: 127/287 Q4: 118/283 Multivitamin users (n = 985) Q1: 107/247 Q2: 123/251 Q3: 99/244 Q4: 103/243 |
Adjusted for age, gender, number of colonoscopies and year of randomisation |
OR (95% CI) Plasma folate vs. adenoma recurrence Total population Q1 (ref): 1.00 Q2: 0.83 (0.64–1.09) Q3: 0.85 (0.65–1.12) Q4: 0.74 (0.56–0.98) p for trend: <0.01 Nonmultivitamin users Q1 (ref): 1.00 Q2: 0.78 (0.55–1.12) Q3: 0.73 (0.50–1.07) Q4: 0.63 (0.43–0.94) p for trend: <0.01 Multivitamin users Q1 (ref): 1.00 Q2: 1.19 (0.81–1.73) Q3: 0.84 (0.57–1.23) Q4: 1.00 (0.67–1.48) p for trend: 0.56 |
Abbreviations: CI, confidence Interval; CRC, colorectal Cancer; OR, odds ratio; RCT, randomised controlled trial; UDCA, The Ursodeoxycholic acid trial; WBF, wheat bran fibre trial; yrs, years.
C.2.2e. Observational study on mixed folate exposures (plasma, serum and/or diet) and incidence of recurrent colorectal adenomas
| Reference Study name Country Study design Follow‐up Funding | Original cohort (N total) Exclusion criteria Study population | Ascertainment of outcome | Exposure groups n/person‐years Exposure assessment method | Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Martínez et al. (2004) WBF US RCT analysed as PC 3 yrs Mixed |
N = 1429 Population sampled: 40–80 yrs who had had ≥1 colorectal adenoma measuring ≥3 mm removed at colonoscopy within 3 months before study entry were recruited Exclusion criteria: subjects with a personal history of inflammatory bowel disease or hereditary colon cancer syndromes as well as those with more than one first‐degree family member with CRC % lost to follow‐up: 8.8% N = 1014 Sex (% women): 30% Age (mean ± SD): 65,275 ± 8.95 |
Data on adenoma characteristics (i.e. number, size, location, histology) were obtained from medical records and pathology reports as previously reported FFQ was used for the dietary intake and plasma folate was analysed by using the Bio‐Rad Quantaphase II Radioassay |
Unit of measurement Plasma folate (nmol/L) Q1: <5.02 Q2: 5.02–8.19 Q3: 8.20–12.75 Q4: >12.75 Total folate intake (μg/d), mean: Q1: <275 Q2: 275–414 Q3: 415–664 Q4: >664 Energy‐adjusted: no |
Incident recurrence/ without recurrence Q1: 133/254 Q2: 115/254 Q3: 128/253 Q4: 119/253 Dietary folate: Q1: 121/254 Q2: 129/253 Q3: 124/254 Q4: 121/253 Total folate intake: Q1: 137/254 Q2: 126/253 Q3: 119/254 Q4: 113/253 |
Adjusted for age, sex, number of colonoscopies, history of polyps before baseline examination. |
OR (95% CI) Plasma folate vs. adenoma recurrence Q1 (ref): 1.00 Q2: 0.61 (0.42, 0.89) Q3: 0.79 (0.54, 1.15) Q4: 0.66 (0.46, 0.97) p for trend: 0.04 Total folate intake vs. adenoma recurrence Q1 (ref): 1.00 Q2: 0.75 (0.52, 1.09) Q3: 0.71 (0.48, 1.03) Q4: 0.61 (0.42, 0.89) p for trend: 0.01 |
Abbreviations: CI, Confidence Interval; CRC, Colorectal Cancer; OR, Odds ratio; PC, Prospective cohort; RCT, Randomised controlled trial; SD, Standard deviation; WBF, Wheat Bran Fibre Trial; yrs, Years.
C.2.2f. Observational studies on dietary folate and incidence of recurrent colorectal adenomas
| Reference Study name Country Study design Follow‐up Funding | Original cohort (N total) Exclusion criteria Study population | Ascertainment of outcome | Exposure groups n/person‐years Exposure assessment method | Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Baron et al. (1998) The Polyp Prevention Study US PC 10–14 yrs Public |
N = 864 Population sampled: Patients with an adenoma diagnosed within the previous 3 months, who have undergone colonoscopy with the entire large bowel seen and judged to be free of further polyps, who were in good health, ≤ 80 yrs Exclusion criteria: Patients with familial polyposis, a history of invasive CRC or malabsorption syndromes, those with conditions that might be worsened by vitamin C or E, such as renal calculi or thrombophlebitis, those unwilling to forego supplements containing study agents % lost to follow‐up: 13% N = 751 Sex (% women): 20.95% Age mean (SD): 61.3 ± 8.3 |
Colonoscopic follow‐up was scheduled at 1 yr and at 4 yrs after the qualifying colonoscopic examination. Adenomas detected after the 1‐yr examination up to and including the 4‐yr examination were the principal end points of the study. At study entry and at the end of the trial, subjects completed a semiquantitative FFQ requesting information regarding dietary intake during the prior year. Use of vitamin (including folate) and mineral supplements and over‐the‐counter drugs was assessed from responses to the baseline and interval questionnaires |
Unit of measurement: Total folate intake (μg/day) Q1: 243 Q2: 338 Q3: 366 Q4: 391 Energy‐adjusted: nutrient residual method |
Incident recurrence/ without recurrence Dietary folate: Q1: 69/103 Q2: 75/113 Q3: 57/115 Q4: 59/118 Total folate: Q1: 65/117 Q2: 69/109 Q3: 64/111 Q4: 61/110 |
Model 1: Adjusted for calories Model 2: Adjusted for age, sex, clinical centre, fat residuals, total dietary fibre residuals, energy intake, colonoscopy interval |
OR (95% CI) Total folate vs. adenoma recurrence Model 1: Q1 (ref): 1.00 Q2: 1.07 (0.68–1.67) Q3: 0.90 (0.57–1.41) Q4: 0.90 (0.57–1.41) p for trend: 0.73 Model 2: Q1 (ref): 1.00 Q2: 1.08 (0.69–1.70) Q3: 0.97 (0.61–1.52) Q4: 1.11 (0.69–1.78) p for trend: 0.57 |
|
Murphy et al. (2008) The Polyp Prevention Trial US PC, based on an RCT 10–14 yrs Public |
N = 2079 Population sampled: ≥35 yrs, with ≥1 histologically confirmed colorectal adenoma removed in the prior 6 months Exclusion criteria: No prior surgically resected adenomatous polyps, or CRC, IBD, or polyposis syndrome, weight no more than 150% of the recommended level. No lipid‐ lowering drugs and no medical conditions or dietary restrictions that would limit compliance with the protocol. % lost to follow‐up: 8.4% N = 1603 Sex (% women): NR Age mean (SD): 61.16 ± 9.9 |
Recurrence outcomes defined at year 4 colonoscopy as: any, advanced or multiple (C2) adenoma recurrence, relative to no adenoma recurrence |
Unit of measurement: Total folate intake μg Q1: 53.4–185 Q2: 185.1–256.7 Q3: 259.9–460.5 Q4: 460.6–2640 FFQ was used for dietary folate Total folate = energy‐adjusted dietary folate + supplemental intake. Energy‐adjusted: nutrient density method |
No. of incident recurrence in the two groups: Total folate intake μg: Q1: 166 Q2: 177 Q3: 150 Q4: 153 Dietary folate intake μg/1000 kcal: Q1: 152 Q2: 169 Q3: 172 Q4: 153 |
Age, gender, race, total fibre intake |
OR (95% CI) Total folate intake vs. any adenoma recurrence Q1 (ref): 1.00 Q2: 1.12 (0.83, 1.52) Q2: 0.88 (0.64, 1.21) Q4: 0.91 (0.67, 1.23) P value: NR |
|
He et al. (2018) NHS 1–2, HPFS US PC 18–20 yrs Mixed |
N= NHS: 121,700 NHS2: 116,430 HPFS: 51,529 Population sampled: NHS/NHS 2: US female nurses aged 25–55 yrs at enrolment HPFS: Male health professionals aged 40–75 yrs Exclusion criteria: NR % lost to follow‐up: NR N = 141,143 Sex (% women): 80% Age mean ± SD: 60.2 ± 10.6 |
On biannual questionnaires, participants were asked if they had undergone a colonoscopy or sigmoidoscopy and if any colorectal polyp had been diagnosed in the past 2 years. For those who reported yes, permission was asked to acquire their endoscopic and pathologic records SPs included hyperplastic polyps and mix/serrated adenomas. Conventional adenomas included tubular, tubulovillous and villous adenomas and adenomas with high‐grade dysplasia. Mixed/serrated adenoma included both mixed polyps (those with both adenomatous and hyperplastic changes in histology) and polyps with any serrated diagnosis (e.g. serrated adenoma, serrated polyp and SSA/P). If a participant had both SPs and conventional adenomas on an endoscopy, we recorded each type of polyps separately and considered the patient as being a synchronous SPs and conventional adenomas case in the current study |
Total folate intake (μg/day) mean ± SD: Overall population: 527 ± 212 Non‐Polyps: 528 ± 213 SPs only: 513 ± 202 Conventional adenomas: 511 ± 202 Synchronous SPs and conventional adenomas: 499 ± 196 FFQ was used for the dietary intake of total folate Energy adjusted: no |
Incident cases SP only: Q1: 2091 Q2: 2121 Q3: 1916 Q4: 1817 Conventional adenomas only: Q1: 2388 Q2: 2460 Q3: 2249 Q4: 2115 Synchronous SPs and conventional: Q1: 649 Q2: 640 Q3: 559 Q4: 534 |
Adjustment for cohort, time period of endoscopy (2‐yr intervals), n of prior endoscopies, years since most recent endoscopy, reason for endoscopy (routine screening or symptom), race (Caucasian or non‐Caucasian), age, family history of CRC, pack‐years of smoking, BMI, physical activity, alcohol intake, height, regular aspirin use |
OR (95% CI) Total folate intake vs. SPs: Q1 (ref): 1 Q2: 1.14 (1.07–1.21) Q3: 1.08 (1.01–1.15) Q4: 1.04 (0.97–1.11) p for trend: 0.79 Total folate intake vs. Conventional adenomas: Q1 (ref): 1 Q2: 1.07 (1.01–1.14) Q3: 1.01 (0.95–1.07) Q4: 0.93 (0.87–0.99) p for trend: 0.002 Synchronous SPs and conventional Q1 (ref): 1.0 Q2: 1.03 (0.92–1.16) Q3: 0.94 (0.84–1.06) Q4: 0.90 (0.80–1.02) p for trend: 0.03 |
|
Lee et al. (2011) NHS, HPFS US PC ⁓ 24 yrs Public |
N = NHS: 121,700 HPFS: 51,529 Population sampled: NHS: Registered nurses, 30–55 yrs HPFS: Male Health professionals 40–75 yrs Exclusion criteria: No FFQ, previous cancer diagnosis, extreme caloric intake, extensive number of FFQ questions unanswered, had ulcerative colitis. % lost to follow‐up: NR n = NHS: 87,861 HPFS: 47,290 Sex (% women): 65% Age: NR |
Self‐reported diagnoses confirmed by medical records. The National Death Index was also used to identify fatalities. |
Total folate (μg/d, min‐max) Q1 (ref): <250 Q2: 250‐ < 400 Q3: 400‐ < 600 Q4: 600‐ < 800 Q5: ≥800 Dietary folate intake (natural + fortified) Q1 (ref): <250 Q2: 250‐ < 300 Q3: 300‐ < 400 Q4: 400‐ < 500 Q5: ≥500 Folic acid intake (supplements + fortified) (μg/d) Q1 (ref): <50 Q2: 50‐ < 100 Q3: 100‐ < 200 Q4: 200‐ < 400 Q5: ≥400FFQ Energy adjusted: least‐square mean |
Incident cases: NHS: 3,101 HPFS: 2,554 Not reported by quintile. |
Age, calendar year, smoking, physical activity, aspirin dose, height, BMI, family history of CRC, menopausal status, hormone therapy use, history of endoscopy, red meat intake, alcohol intake, calcium intake from foods, total energy intake |
OR (95% CI) Data extracted for the model on cumulative average exposure. Total folate intake vs. any adenoma: Q1 (ref): 1.00 Q2: 0.97 (0.87, 1.08) Q3: 0.93 (0.70, 1.22) Q4: 0.75 (0.55, 1.03) Q5: 0.73 (0.57, 0.94) p‐trend: 0.005 p for heterogeneity: 0.15 Dietary folate intake vs. any adenoma: Q1 (ref): 1.00 Q2: 1.03 (0.85, 1.25) Q3: 0.94 (0.73, 1.21) Q4: 0.92 (0.74, 1.14) Q5: 0.71 (0.59, 0.85) p‐trend: 0.008 p for heterogeneity: 0.49 Folic acid vs. any adenoma: Q1 (ref): 1.00 Q2: 1.02 (0.93, 1.12) Q3: 0.97 (0.89, 1.06) Q4: 0.85 (0.77, 0.94) Q5: 0.75 (0.65, 0.87) p‐trend: <0.001 p for heterogeneity: 0.13 |
Abbreviations: BMI, Body mass index; CI, Confidence Interval; CRC, Colorectal Cancer; FFQ, Food frequency questionnaire; HPFS, Health Professionals Follow‐up Study; IBD, Inflammatory bowel disease; NHS, Nurses' Health Study; NR, Not reported; OR, Odds ratio; PC, Prospective cohort; RCT, Randomised controlled trial; SD, Standard deviation; SP, Serrated polyps; yr, year; yrs, years.
C.3. Prostate cancer
C.3.1. Intervention study on folic acid supplementation and incidence of prostate cancer
|
Reference Study Country Duration Funding |
Design | Subject characteristics at baseline a | Intervention a | Endpoint assessed | Results |
|---|---|---|---|---|---|
|
Figueiredo et al. (2009) AFPPS USA 3 yr (trial) + 3–5 yr (trial follow‐up with continued folic acid treatment) Enrolment 1994–98 Fortification started 1996, and was mandatory 1998 Public, Supplements by private company |
Report of secondary findings based on additional analysis of the colorectal adenoma trial (Cole et al., 2007) RCT 3 × 2 factorial design Inclusion criteria: 21–80 yrs with histologically confirmed adenoma removed. Participants had a complete colonoscopy, with removal of all known polyps, within 3 months of enrolment Exclusion criteria: familial polyposis syndromes, intestine cancer, malabsorption syndromes, conditions worsened by supplemental aspirin or folic acid, conditions treated with aspirin, NSAIDs or folate. Cobalamin deficient individuals were excluded. Prostate cancer: only men in AFPPS. 651 randomised of which 643 were included below Randomised and started (ITT)/completed first trial phase/consented continued follow‐up/consented continued treatment G1: 327/318/303/235 G1a: 112/NR/NR/NR/NR G1b: 108/NR/NR/NR/NR G1c: 107/NR/NR/NR/NR G2: 316/306/292/237 G2a: 109/NR/NR/NR/NR G2b: 105/NR/NR/NR/NR G2c: 102/NR/NR/NR/NR |
Age 57.4 +/−9.2 P‐folate (nmol/L) G1: 23.2 G2: 22.7 RBC‐folate (nmol/L) G1: 388.6 G2: 404 Other relevant sources of heterogeneity None in general, but herein lower baseline plasma cobalamin in G1 (G2 = 348.1 pmol/L; G1 = 317.0 pmol/L, difference = 31.1 pmol/L, 95% CI = 1.8 to 60.4 pmol/L, p = 0.04) |
Folic Acid Doses: G1: 1000 μg/day G1a: 1000 μg/day + 81 mg/day Aspirin G1b: 1000 μg/day + 325 mg/day Aspirin G1c: 1000 μg/day + Aspirin placebo G2: Placebo G2a: Placebo + 81 mg/day Aspirin G2b: Placebo + 325 mg/day Aspirin G2c: Placebo + Aspirin placebo Background dietary folate (μg/day) G1: 337 G2: 350 Compliance: NR |
Prostate cancer self‐reported; medical records obtained and diagnosis confirmed by histopathology |
Type of analysis extracted: ITT Prostate cancer cases G1: 25 G2: 9 Estimated probability of being diagnosed with prostate cancer over 10 yrs: G1: 9.7% (95% CI 6.5–14.5) G2: 3.3% (95% CI 1.7–6.4) Age‐adjusted HR: 2.63 (95% CI 1.23–5.65) Multivariable‐adjusted HR: 2.58 (95% CI 1.14–5.86) |
Abbreviations: AFPPS, Aspirin/Folate Polyp Prevention Study; CI, Confidence Interval; G, Group; HR, Hazard ratio; ITT, Intention‐to‐treat; NR, Not reported; P, Plasma; RBC, Red blood cell; RCT, Randomised controlled trial; yr, year; yrs, years.
Values reported as mean ± standard deviation or median (inter quartile range) unless otherwise indicated.
C.3.2a. Observational studies on folate biomarkers and incidence of prostate cancer
|
Reference Study name Country Study design Follow‐up Funding |
Original cohort (N total) Exclusion criteria Study population | Ascertainment of outcome | Exposure groups n/person‐years Exposure assessment method | Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Weinstein et al. (2003) ATBC Study NCC Finland Follow up: NR Public |
N = 29,133 Population sampled: Male smokers, 50–69 yrs Exclusion criteria: NR % lost to follow‐up: 8 cases and 10 controls n = 224 cases and 454 controls Age: NR Matching criteria: Controls matched on age, clinic, intervention group, date of baseline blood draw |
Cases were defined as incident prostate cancers diagnosed through 1994 with available serum |
Unit of measurement Serum Folate (nmol/L) (min‐max): Q1 (ref): ≤6.87 Q2: 6.88–8.69 Q3: 8.70–10.79 Q4: >10.79 Person‐years: NA Radioassay method Prostate cancer cases reported greater use of vitamin/mineral supplements than did controls |
N cases/controls Q1 (ref): 56/118 Q2: 55/109 Q3: 52/114 Q4: 61/113 |
Adjusted for: Benign prostatic hyperplasia |
OR (95% CI) Serum folate versus Prostate cancer: Q1 (ref): 1.00 Q2: 1.10 (0.69–1.75) Q3: 1.04 (0.64–1.67) Q4: 1.20 (0.74–1.94) p for trend = 0.52 |
|
Johansson et al. (2008) EPIC Germany, Greece, Italy, the Netherlands, Spain, Sweden, UK NCC 14 yrs Public |
N = 519,978 Population sampled: Individuals across Europe Exclusion criteria: Cases with no available blood sample and those who had missing information on the date of blood donation or who had a history of another cancer (except non‐melanoma skin cancer) at the time of blood donation 238 cases from Sweden had been used in previous study and were excluded. % lost to follow‐up: NR N = Cases: 869 Controls: 1174 Age at blood collection (mean ± SD): Cases: 59.1 ± 6.7 Controls: 58.3 ± 6.8 Matching criteria: Study centre, age at enrolment, time of day of blood collection, time between blood draw and last consumption of food or drink |
In Italy, the Netherlands, Spain, Sweden and the UK incident cancer cases identified through record linkage with regional or national cancer registries. In Germany and Greece a combination of methods, including health insurance records, cancer and pathology registries, and active follow‐up through study subjects and next‐of‐kin |
Unit of measurement Circulating Folate concentration (nmol/L) (min‐max): Q1 (ref): <4.82 Q2: 4.83–6.77 Q3: 6.78–9.87 Q4: 9.89–16.52 Q5: ≥16.55 Person yrs: NR Folate concentrations were determined by a Lactobacillus casei microbiological assay |
N cases/controls Q1 (ref): 117/229 Q2: 119/232 Q3: 162/229 Q4: 250/233 Q5: 207/227 |
Model 1: crude Model 2: Adjusted for BMI, smoking status, alcohol intake, physical Activity, marital status, educational level |
RR (95% CI) Circulating folate versus prostate cancer: Model 1 Q1 (ref): 1.00 Q2: 0.99 (0.73–1.36) Q3: 1.15 (0.83–1.61) Q4: 1.52 (1.06–2.18) Q5: 1.23 (0.84–1.81) p for trend: 0.62 Model 2 Q1 (ref): 1.00 Q2: 1.02 (0.74–1.39) Q3: 1.18 (0.84–1.66) Q4: 1.62 (1.12–2.34) Q5: 1.30 (0.88–1.93) p for trend 0.46 |
|
Essén et al. (2019) Swedish Apolopoprotein Mortality Risk Sweden PC 13 yrs (mean) Mixed |
N = 812,073 Population sampled: Individuals mainly from Stockholm area, men aged 30 yrs and older Exclusion criteria: NR % lost to follow‐up: NR N = 8783 Age mean ± SD: 64 ± 15.2 |
Swedish National Cancer Register, to which reporting is mandated, the National Prostate Cancer Register |
Unit of measurement Serum Folate (nmol/L) (min‐max): Categories defined based on specific cut‐off values G1: <5 G2: 5–32 G3: >32 |
Incident cases/controls: G1: 6/65 G2: 646/8030 G3: 51/688 |
Model 1: Crude Model 2: Adjusted for age Model 3: model 2 and education level, SES, CCI, serum glucose, triglycerides, cholesterol, fasting status |
HR (95% CI) Serum Folate vs. prostate cancer: Model 1 G1: 1.77 (0.79–3.95) G2 (ref): 1.00 G3: 1.01 (0.76–1.34) p for trend: 0.40 Model 2 G1: 1.42 (0.63–3.16) G2 (ref): 1.00 G3: 0.82 (0.62–1.09) p for trend: 0.13 Model 3 G1: NA G2 (ref): 1.00 G3: 0.73 (0.48–1.10) p for trend: 0.07 |
|
Hultdin et al. (2005) Northern Sweden Heatlh and Disease Cohort Sweden NCC 4.9 yrs Mixed |
N = 37,776 Population sampled: In one sub cohort general population upon turning 40, 50 and 60 yrs invited to complete a survey and participate in future research, in the other random selection Exclusion criteria: NR % lost to follow‐up: NR N = 768 Age at recruitment (mean ± SD) Cases: 58.2 ± 4.9 Controls: 58.2 ± 3.9 Matching criteria: Controls (2:1) matched for age, recruitment date and subcohort |
Incident cases of prostate cancer were identified through linkage with the regional cancer registry |
Unit of measurement Plasma Folate (nmol/L) (min‐max): Q1 (ref): <5.85 Q2: 5.85–7.70 Q3: 7.70–10.30 Q4: >10.30 Radioassay method |
Incident cases/ controls: Q1 (ref): 60/130 Q2: 58/134 Q3: 58/133 Q4: 77/111 |
Model 1: Crude Model 2: Adjusted for p‐cobalamin, homocysteine, BMI, smoking |
OR (95% CI) Plasma Folate vs. prostate cancer: Model 1 Q1 (ref): 1.00 Q2: 0.94 (0.60–1.47) Q3: 0.95 (0.61–1.48) Q4: 1.60 (1.03–2.49) p for trend: 0.02 Model 2 Q1 (ref): 1.00 Q2: 0.78 (0.46–1.32) Q3: 0.76 (0.44–1.31) Q4: 1.30 (0.74–2.24) p for trend: 0.17 |
|
Rossi et al. (2006) 1969 Busselton Health survey Australia PC 23 yrs Public |
N = NR Population sampled: General population, 40–90 yrs Exclusion criteria: History of cancer % lost to follow‐up: NR n = 1035 Age (mean): 55 years |
Cancer morbidity was obtained by linkage to the death register, cancer register and hospital admissions. The event of interest was the first of cancer registration, hospital admission for cancer or cancer death (individuals censored at the time of the first event) |
Serum folate (μg/L, min‐max): Q1: < 3.00 Q2: 3.00–4.49 Q3: 4.50–5.99 Q4: ≥ 6.00 (ref) RBC folate (μg/L, min‐max): Q1: 0.0–199.9 Q2: 200.0–274.9 Q3: 275–349.9 Q4: ≥ 350.0 (ref) In‐house automated microbiological assay system n/person years: Men: 20,254 |
Incident cases Prostate cancer morbidity Serum folate: Q1: 10 Q2: 16 Q3: 9 Q4: 17 (ref) RBC folate: Q1: 14 Q2: 13 Q3: 8 Q4: 17 (ref) |
Age and sex and baseline cancer‐risk factors based on established risk factors for each cancer outcome: smoking, alcohol and BMI for all cancers, including prostate cancer |
HR (95% CI) Serum folate vs. prostate cancer morbidity (2 μg/L decrease in serum folate): 1.18 (0.90, 1.51), p = 0.24 RBC folate vs. prostate Cancer morbidity (100 μg/L decrease in RBC folate): 1.20 (0.96, 1.52), p = 0.10 Serum folate vs. prostate Cancer morbidity: Q1: 2.50 (1.09, 5.75) Q2: 1.30 (0.64, 2.64 Q3: 0.58 (0.25, 1.32) Q4: 1.0 (ref) RBC folate vs. prostate cancer morbidity: Q1: 1.51 (0.72, 3.17) Q2: 1.02 (0.49, 2.13) Q3: 0.97 (0.41, 2.25) Q4: 1.0 (ref) |
|
Beilby et al. (2010) Australia NCC 14 yrs Public |
N = 6903 Population sampled: former Wittenoom crocidolite mine and mill workers Exclusion criteria: NR % lost to follow‐up: NR N = Cases: 96 Controls: 225 Age at diagnosis (mean ± SD): Cases: 69.8 ± 7.2 Controls: 69.3 ± 6.7 |
Prostate cancer cases were histologically confirmed cases identified through record linkage with the Western Australian Cancer Registry and the Australian National Cancer Statistics Clearing House. |
Unit of measurement: Serum folate (μg/L, min‐max): T1: 1.50–3.80 T2: 3.90–6.20 T3: 6.30–45.1 Automated immunoassay |
Incident cases/controls: T1: 33/70 T2: 32/70 T3: 27/74 |
Adjusted for age, administered vitamin A supplement |
OR (95% CI) Serum folate versus prostate Cancer T1 (ref): 1.00 T2: 1.10 (0.57–2.11) T3: 1.09 (0.48–2.46) p for trend: 0.83 Continuous OR (95% CI): 0.99 (0.56–1.77) |
|
de Vogel et al. (2013) JANUS cohort Norway NCC 15.6 years (mean) Public |
N = 317,000 Population sampled: Individuals who participated in health screening surveys or were Red Cross blood donors in Norway between 1973 and 2004 Exclusion criteria: Residency outside Norway, diagnosed cancer other than non‐melanoma skin cancer % lost to follow‐up: NR N= Cases 3000 Controls: 3000 Age at serum sampling (mean ± SD) Cases: 49.1 ± 8.7 Controls: 49.1 ± 8.7 Matching criteria: Controls were matched by age at serum sampling, date of serum sampling and country of residence |
Cancer incidence data were obtained from the Cancer Registry of Norway |
Unit of measurement: Serum folate (nmol/L) (min‐max): Q1: <10.9 Q2: 10.9–12.8 Q3: 12.8–14.7 Q4: 14.7–17.5 Q5: ≥17.5 p‐Aminobenzoylglutamate Equivalents |
Incident cases/control Q1: 585/577 Q2: 566/601 Q3: 556/596 Q4: 590/614 Q5: 703/612 |
Model 1: Crude Model 2: Adjusted for education, smoking, physical activity, BMI, serum creatinine |
OR (95% CI) Serum folate concentration vs. prostate Cancer Model 1 Q1 (ref): 1.00 Q2: 0.93 (0.79–1.10) Q3: 0.93 (0.79–1.10) Q4: 0.96 (0.81–1.14) Q5: 1.17 (0.99–1.39) p trend: 0.02 Model 2 Q1 (ref): 1.00 Q2: 0.92 (0.78–1.09) Q3: 0.92 (0.77–1.09) Q4: 0.94 (0.80–1.12) Q5: 1.15 (0.97–1.37) p trend: 0.04 |
Abbreviations: BMI, body mass index; CCI, Charlson comorbidity index; CI, Confidence Interval; EPIC, European Prospective Investigation into Cancer and Nutrition; G, Group; HR, Hazard ratio; NA, Not available; NCC, Nested case–control; NR, Not reported; OR, Odds ratio; PC, Prospective cohort; RBC, Red blood cell; SD, Standard deviation; SES, Socioeconomic status; yrs, years.
C.3.2b. Observational studies on dietary folate and incidence of prostate cancer
| Reference Study name Country Study design Follow‐up Funding | Original cohort (N total) Exclusion criteria Study population | Ascertainment of outcome | Exposure groups n/person‐years Exposure assessment method | Incident cases | Model covariates | Results |
|---|---|---|---|---|---|---|
|
Weinstein et al. (2006) ATBC Study Finland PC in an RCT 5–8 years Public |
N = 29,133 Population sampled: men, 50–69 years, who smoked ≥5 cigarettes/day Exclusion criteria: incomplete dietary information % lost to follow‐up: NR N = 27,111 Age, years (mean ± SD) Cases: 59 ± 5 Controls: 57 ± 5 |
These cancers were identified through the Finnish Cancer Registry and the Register of Causes of Death |
Unit of measurement: Total folate intake (μg/d) (mix‐max): Q1: ≤283 Q2: 283–≤313 Q3: 313–≤341 Q4: 341–≤378 Q5: >378 Persons years: Q1: 64,743 Q2: 67,514 Q3: 67,891 Q4: 68,146 Q5: 68,199 FFQ Energy‐adjusted: nutrient residual method |
Incident cases: Q1: 256 Q2: 242 Q3: 263 Q4: 250 Q5: 259 |
Adjusted for age at randomisation, vitamin supplement use. Energy intake was tested, but not considered a confounder |
RR (95% CI) Total folate intake versus prostate cancer: Q1 (ref): 1 Q2: 0.91 (0.77–1.09) Q3: 1.00 (0.84–1.19) Q4: 0.95 (0.80–1.13) Q5: 0.96 (0.81–1.15) p for trend: 0.84 |
|
Roswall et al. (2013) Diet, Cancer and Health Cohort study Denmark PC 14.3 years (median) Public |
N: 27,178 Population sampled: Men 50–64 years, born in Denmark, residency in Copenhagen or Aarhus, no previous cancer diagnosis in the Danish Cancer Registry Exclusion criteria: Previous cancer, information of confounders/exposure variables lacking % lost to follow‐up: NR N = 26,856 Age at baseline median (p5‐p95) Cases: 58 (51.0–64.7) Controls: 56 (50.7–64.2) |
Information on cancer was obtained from the Danish Cancer Registry, containing accurate and virtually complete data on cancer incidence in Denmark |
Unit of measurement: Median (p5–p95): Total folate intake (μg/day) Controls: 376.1 (215.8–642.27) Cases: 379.8 (218.2–636.9) Supplemental folate intake among supplement users: Controls: 100.0 (11.9–250.0) Cases: 100.0 (9.6–229.0) N/person yrs: NR FFQ was used for food intake. Open ended question for supplements Energy‐adjusted: no |
Incident cases: 1571 Incident cases are not presented by quartiles. |
Categorical analyses: Adjusted for intake of vitamin C, vitamin E, B‐carotene and dietary intake for the supplemental intake and supplemental intake for the dietary intake and further for height, weight, education, intake of red meat, alcohol consumption, selenium intake. Continuous analysis: Crude: Vitamin C, vitamin E, beta‐carotene. Adjusted: model 1 + dietary intake for the supplemental intake and supplemental intake for the dietary intake, height, weight, education, intake of red meat, alcohol consumption, selenium intake |
HR (95% CI) Total folate intake vs. prostate cancer Q1 (ref): 1.00 Q2: 0.89 (0.77–1.03) Q3: 0.99 (0.84–1.17) Q4: 0.87 (0.71–1.07) p for trend: 0.23 Supplemental Folate intake vs. prostate cancer Q1 (ref): 1.00 Q2: 1.17 (0.95–1.45) Q3: 0.97 (0.78–1.22) Q4: 0.93 (0.73–1.17) p for trend: 0.0213 Continuous analyses (HR 95% CI): Total folate intake vs. prostate cancer Crude: 0.98 (0.95–1.02) Adjusted: 0.96 (0.91–1.02) Dietary folate intake vs. prostate cancer: Crude: 0.99 (0.95–1.04) Adjusted: 1.00 (0.93–1.08) Supplemental Folate intake vs. prostate cancer Crude: 0.96 (0.90–1.02) Adjusted: 0.88 (0.79–0.98) Test for different effect of source: 0.05 |
|
Stevens et al. (2006) Cancer Prevention II Nutrition Cohort USA PC 8–9 yrs Funding NR |
N = 86,404 men Population sampled: CPS‐II members who resided in 21 US states, 50–74 yrs Exclusion criteria: Lost to follow‐up, prior cancer, self‐reported prostate cancer not verified, reported diagnosis more than 6 months after the interview date, men with stage 1 prostate cancer, missing dietary data, primary cause of death was not prostate cancer % lost to follow‐up: 0.04% N = 65,836 Age: NR |
Cancer cases identified through self‐report on the follow‐up questionnaires and subsequently verified the prostate cancer diagnosis through either medical records or linkage with state cancer registries during the process of verifying another Cancer and cases for whom prostate cancer was the underlying cause of death were identified through linkage with the National Death Index |
Unit of measurement: Folate intake (μg/day) Total Folate intake: Q1: <223 Q2: 223–<286 Q3: 286– <370 Q4: 370– <640 Q5: ≥640 Dietary Folate intake (natural + fortified): Q1: <204 Q2: 204– <250 Q3: 250– <293 Q4: 293– <347 Q5: ≥347 FFQ method was used for dietary and supplemental folate intake. Energy‐adjusted: no |
Incident cases: 5,158 Total Folate: Q1: 902 Q2: 1070 Q3: 1085 Q4: 1009 Q5: 1092 Dietary Folate: Q1: 913 Q2: 997 Q3: 1052 Q4: 1136 Q5: 1060 |
Adjusted for age, race, education, total calories, total calcium, ethanol, family history of prostate cancer, cobalamin, prostate‐specific antigen screening, history of diabetes. |
RR (95% CI) Total folate intake vs. prostate cancer Q1 (ref): 1.00 Q2: 1.12 (1.02–1.22) Q3: 1.11 (1.01–1.22) Q4: 1.06 (0.96–1.16) Q5: 1.11 (1.01–1.22) p for trend: 0.35 Dietary folate intake versus prostate cancer Q1 (ref): 1.00 Q2: 1.02 (0.93–1.11) Q3: 1.05 (0.96–1.15) Q4: 1.11 (1.01–1.21) Q5: 1.03 (0.94–1.13) p for trend: 0.29 |
Abbreviations: FFQ, Food frequency questionnaire; NR, Not reported; PC, Prospective cohort; RCT, Randomised controlled trial; yrs, years.
APPENDIX D. DOSE RESPONSE MODELLING OF THE RELATIONSHIP BETWEEN TOTAL FOLATE INTAKE, EXPRESSED AS μG DFE AND P/S FOLATE CONCENTRATION
D.1.
A dose–response meta‐analysis was conducted to characterise the relationship between mean total folate intake, expressed in μg dietary folate equivalents (DFE) and mean plasma/serum folate concentrations. The purpose of this analysis was to support the interpretation and integration of findings from observational studies which used plasma/serum folate concentrations as biomarker of folate intake into the UL assessment. The dose–response between folic acid intake and plasma/serum folate concentrations has been investigated by other authors and was outside of the scope of the present evaluation.
The method and results are summarised below. The reader is referred to the contractor's report for further details (Åkesson et al., 2023).
Eligible studies were feeding trials or supplement interventions in adults with a minimum duration of 2 weeks, reporting on end‐of‐trial plasma or serum (P/S) folate concentrations and total folate intake (i.e. from natural sources, fortified foods and/or food supplements). The analysis excluded studies (i) which used FFQ, diet history questionnaire or 24 h‐recalls to estimate background folate intake; and/or (ii) for which the method for nutrient intake analysis was not reported; and/or (iii) for which the consideration of voluntary fortified foods or the conversion of folic acid into DFE were unclear.
A total of 22 randomised controlled trials (n = 19 parallel and n = 3 cross‐over) were included in the analysis (Brämswig et al., 2009; Castenmiller et al., 2000; Caudill et al., 1997; de Jong et al., 2005; Duthie et al., 2018; Fenech et al., 2005; Green et al., 2005; Hiraoka et al., 2004; Hursthouse et al., 2011; Kauwell et al., 2000; Kawashima et al., 2007; Krondl et al., 1999; McClung et al., 2020; Norsworthy et al., 2004; O'Keefe et al., 1995; Riddell et al., 2000; Silaste et al., 2003; Smidt et al., 1990; Venn, Mann, Williams, Riddell, Chisholm, Harper, & Aitken, 2002; Venn, Mann, Williams, Riddell, Chisholm, Harper, Aitken, & Rossaak, 2002; Winkels et al., 2007; Wolters et al., 2005). They were conducted in New Zealand (n = 6), USA (n = 4), the Netherlands (n = 3), Germany (n = 2), Japan (n = 2), Australia (n = 1), Canada (n = 1), Finland (n = 1), Ireland (n = 1) and Scotland (n = 1) and consisted of women alone (n = 11) or both sexes (n = 11). The P/S analyses were assessed using immunoassay (n = 13), microbiological assay (n = 8) or HPLC (n = 1).
Total intake of folate was expressed in μg DFE/day representing the sum of folate intake from natural sources, fortified foods and/or food supplements. For studies in which the level of folic acid intake (from fortified food and/or food supplements) was not reported as DFE, the value was converted applying the following formula: μg DFE = μg folic acid/0.6, under the assumption that most folic acid was consumed in conjunction with food. The P/S folate biomarker data were harmonised into nmol/L by applying a conversion factor of 2.266 when the original unit was in ng/mL.
Both linear (meta‐regression using a weighted mixed effects model) and non‐linear (restricted cubic splines) dose–response relationships were investigated. Random‐effects models were fitted on mean values applying the maximum likelihood approach. Potential modifying factors were characterised in stratified analyses. Contextual sources of heterogeneity tested were sex and type of dietary folate administered to the participants. Methodological sources of heterogeneity included: type of media sampled (P or S), and the analytical method used to assess P/S folate. Sensitivity analyses were run to address uncertainties regarding the reliability of specific studies' features, i.e. (i) exclusion of the studies considered to have less reliable data from dietary assessment; (ii) exclusion of the studies using non‐fasting blood samples; and (iii) exclusion of data points that corresponded to ‘uncontrolled’ folate dietary intake (i.e. data from control groups left on their habitual diet).
Potential non‐linear dose–response relationships were examined using restricted cubic splines with three knots at 10%, 50% and 90% percentiles of the intake distribution. The location of the knots was chosen based on Harrell's recommended percentiles (Harrell, 2001). The non‐linear model did not provide a better fit to the data than the linear model.
The linear meta‐regression model describing the dose–response relation between total folate intake, expressed as μg DFE and P/S folate concentrations (in nmol/L) is presented in Figure D.1 and is as follows: S/P folate (nmol/L) = 6.0 + 0.034 * μg DFE/day [95% Confidence Interval (CI); 0.027–0.040], R 2 = 0.68.
FIGURE D.1.
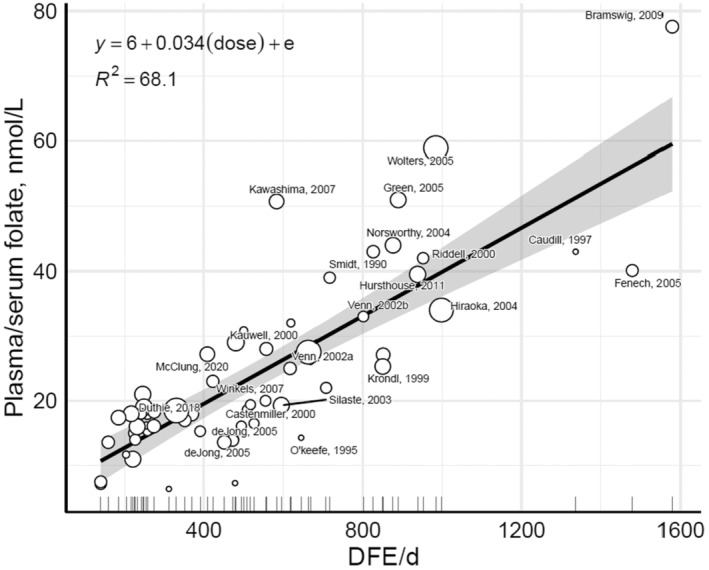
The linear meta‐regression line (black) and 95% confidence interval (grey) between μg DFE and plasma/serum folate (in nmol/L) for the 22 studies and 60 data points included from the weighted mixed effects model. The size of the circle represents the size of the study. Unnamed circles correspond to ‘control groups’/other arms. d, day; DFE, dietary folate equivalents.
The outcome of the stratified and sensitivity analyses conducted on this model are presented in the contractor's report (Åkesson et al., 2023). While some sources of heterogeneity were observed (in particular participants' gender and analytical method used to measure P/S folate), the number of studies included in the subgroups was small and results must be interpreted with caution. The inclusion of data from non‐fasting blood samples, ‘uncontrolled’ folate dietary intake and total folate intake estimates based on less reliable intake assessment methods was found to have a limited impact on the model.
Table D.1 presents predictions of P/S folate mean value and related 95% CI, in nmol/L (column 2), at relevant μg DFE daily intakes (column 1) based on the weighted meta‐regression model. Table D.2 presents the estimated μg DFE daily intakes (column 2) by applying the inverse solution of the prediction equation to relevant P/S folate values, in nmol/L (column 1).
TABLE D.1.
Predicted P/S folate concentration from predefined DFE intake based on the equation.
| DFE (μg/day) | P/S folate (nmol/L) Mean (95% CI) |
|---|---|
| 200 | 13 (11, 14) |
| 400 | 20 (17, 22) |
| 600 | 26 (22, 30) |
| 800 | 33 (28, 38) |
| 1000 | 40 (33, 46) |
| 1200 | 47 (38, 54) |
| 1400 | 54 (44, 62) |
| 1600 | 60 (49, 70) |
Abbreviations: CI, confidence interval; DFE, dietary folate equivalents; P/S, plasma/serum.
TABLE D.2.
Estimated DFE from predefined P/S folate based on the prediction equation.
| P/S folate (nmol/L) | DFE (μg/day) |
|---|---|
| 10 | 118 |
| 20 | 412 |
| 30 | 706 |
| 40 | 1000 |
| 50 | 1294 |
| 60 | 1588 |
Abbreviations: DFE, dietary folate equivalents; P/S, plasma/serum.
APPENDIX E. SYSTEMATIC REVIEWS AND META‐ANALYSES OF RCTS ON OVERALL CANCER RISK
E.1.
TABLE E.1 Overview of the identified systematic reviews and meta‐analyses of RCTS on the association between folic acid and cancer risk.
| Study Name Ref | Comparison | Vollset et al. (2013) a | Qin et al. (2013) | Wien et al. (2012) | AHRQ, 2021 b | ||||
|---|---|---|---|---|---|---|---|---|---|
| FA | FA + B12 | FA + B12 + B6 | FA + A | P | |||||
|
SEARCH Armitage 2010 |
x | x | x | – | |||||
|
NORVIT Bønaa 2006 |
x | x | x | – | |||||
|
AFPPS Cole 2007 |
x | x | x | x | |||||
|
VITRO e den Heijer 2007 |
x | – | – | – | |||||
|
NORVIT, WENBIT Ebbing 2008 |
x | x | x | – | |||||
|
SU‐FOL‐OM3 f Galan 2010/Andreeva 2012 |
x | x | – (c) | – | |||||
|
VITATOPS Hankey 2012 |
x | x | – | – | |||||
|
BVAIT Hodis 2009 |
‐ | x | – | – | |||||
|
HOST e Jamison 2007 |
x | x | x | – | |||||
|
UkCAP Logan 2008 |
x | x | x | – | |||||
|
HOPE−2 Lonn 2006 |
x | x | x | – | |||||
|
Toole 2004 |
x | x | x | – | |||||
|
B‐PROOF van Wijngaarden, 2014 |
– | – | – | x | |||||
|
NHS/HPFS Wu 2009 |
x | x | x | x | |||||
|
WAFACS Zhang 2008 |
x | x | x | – | |||||
| N studies included | 13 | 13 | 10 | 3 | |||||
| FA arms: Cases/total (%) | 1904/24,799 (7.7%) | 1914/24,692 (7.8%) | 1639/19,107 (8.6%) | 144/2315 (6.2%) | |||||
| P arms: Cases/total (%) | 1809/24,822 (7.3%) | 1827/24,714 (7.4%) | 1545/19,128 (8.1%) | 102/2297 (4.4%) | |||||
| Pooled RR (95% CI) | 1.06, 95% CI 0.99–1.13, p = 0.10, I 2 15.26% | 1.05, 95% CI 0.99–1.11, p = 0.13 | 1.07, 95% CI 1.00 to 1.14, I 2 0% | 1.42, 95% CI 1.10 to 1.84, I2 0% | |||||
Abbreviations: A, aspirin; B6, vitamin B6; B12, vitamin B12/cobalamin CI, confidence interval; FA, folic acid (except in SU‐FOL‐OM3, in which 5‐MTHF was used); I2, heterogeneity index; MI, Myocardial infraction; N, count; P, placebo; RCT, randomised controlled trial; RR, relative risk.
Pooled analysis of individual data by the B‐Vitamin Treatment Trialists' Collaboration.
Included studies with FA alone or in combination with cobalamin (combinations with other nutrients excluded); excluded studies with dose >UL or in which >10% individuals had active/current cardiovascular disease, diabetes mellitus or cancer
Included in a sensitivity analysis: RR 1.08, 95% CI 1.01–1.1.
Compared combination of FA + vitamin B6 + cobalamin at high versus low doses.
Data unpublished.
Also included concomitant supplementation with Docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA).
APPENDIX F. SYSTEMATIC REVIEWS, META‐ANALYSES AND POOLED ANALYSES OF PCS AND NCCS ON INCIDENCE OF CANCER AT SPECIFIC SITES
F.1.
TABLE F.1 Data from the most recent and complete systematic reviews and meta‐analyses on each type of cancer.
| Reference | Cancer type | Exposure variable | Eligible designs | Search | N eligible studies | Pooled estimate a | Results of individual studies (highest vs. lowest) a |
|---|---|---|---|---|---|---|---|
| Fu et al. (2021) | Incident pancreatic cancer | Folate intake and P/S folate | PCs, NCCs and CCs |
Pubmed and eMBASe databases Until November 2019 |
7 PCs + 3 NCCs [8 assessed dietary folate intake and 2 P/S folate] | RR (highest vs. lowest) = 0.85, 95% CI: 0.66–1.09, p = 0.244; I 2 61.8% | Positive associations in two studies (Schernhammer et al., 2007) (RRQ4 vs. Q1 1.34 (0.79, 2.26), Q4 > 17.4 nmol/L vs. Q1 < 14.9 nmol/L) and (Keszei et al., 2009) (RRQ5 vs. Q1 1.37 (0.97, 1.94), Q5 > 259.1 μg/day vs. Q1 < 176.3 μg/day total folate); null or negative associations in other studies |
| Liu et al. (2017) | Incident oesophageal cancer | Folate intake and P/S folate | Cohort studies and CCs |
Pubmed, MEDLINE and EMBASE Until May 2017 |
2 PCs [1 assessed dietary folate intake and 1 S folate] | OR (highest vs. lowest) = 0.82, 95% CI: 0.57–1.07; I 2 51.4% | Null or negative associations in all studies |
| Liu et al. (2017) | Incident gastric cancer | Folate intake and P/S folate | Cohort studies and CCs |
Pubmed, MEDLINE and EMBASE Until May 2017 |
5 PCs [4 assessed dietary folate intake and 1 S folate] | OR (highest vs. lowest) = 0.97, 95%CI:0.80–1.13; I 2 0.0% | Null or negative associations in all studies |
| Ren et al. (2020) | Incident breast cancer | Folate intake and P/S folate | PCs and CCs |
Pubmed and eMBASe databases Until April 2019 |
19 PCs on folate intake 2 PCs on P/S folate |
Folate intake OR (highest vs. lowest) = 0.97, 95% CI: 0.91–1.03; p = 0.003; I 2 53.3% S folate OR (highest vs. lowest) = 1.63, 95% CI: 0.61–4.37; p = 0.078; I 2 67.% |
Positive association in one study (OR Q5 vs. Q1 4.11 (0.84, 20.18), Q5 > 63 nmol/L vs. Q1 ≤14 nmol/L) (Kim et al., 2016); null or negative associations in other studies |
| Zhang et al. (2014) | Incident lung cancer | Folate intake | PCs and NCCs |
PubMed, Embase and the Cochrane Library Until September 2013 |
9 PCs | RR (highest vs. lowest) = 0.92; 95% CI: 0.84–1.01; p = 0.076; I 2 0.0% |
Positive association in one study (HRQ5 vs. Q1 1.12 (0.83, 1.52) for Q5 > 374 vs. Q1 ≤237 μg/day natural folate) (Kabat et al., 2008); null or negative associations in other studies |
| Wang, Zhang, and Yang (2021) | Incident ovarian cancer | Folate intake | CCs, cross‐sectional or cohort studies |
PubMed, Web of Science, Embase, Cochrane and Wanfang databases Until May 2020 |
4 PCs on dietary folate intake 4 PCs on total folate intake |
Total folate intake (including FS) RR (highest vs. lowest) = 1.21, 95% CI: 0.89–1.65; I2 40.8% |
Null or negative associations in all studies |
| Du et al. (2016) | Incident endometrial cancer | Folate intake | PCs, NCCs, CCs |
PubMed, Embase and Web of Science Search date NR |
5 PCs | OR (highest vs. lowest) = 1.05, 95% CI: 0.90–1.20; I 2 = 19.8% | Positive association for type II but not type I endometrial cancer in one study (ORQ4 vs. Q1 1.71 (0.87, 3.36), Q4 > 560 vs. Q1 < 250 μg/day total folate) (Uccella et al., 2011); null or negative associations in other studies |
| Gu et al. (2022) | Urothelial carcinoma | Folate intake and P/S folate | PCs, NCCs, CCs |
Pubmed and eMBASe databases Until October 2019 |
8 PCs +2 NCCs [9 assessed dietary folate intake and 1 plasma folate] | RR (highest vs. lowest) = 0.97, 95% CI: 0.87–1.09, p = 0.638; I 2 0% | Positive associations in two studies (Bassett et al., 2019) (RRQ5 vs. Q1 1.27, 95% CI 0.81, 2.00; <9.3 vs. >17.0 nmol/L) and (Michaud et al., 2002) (RRQ5 vs. Q1 1.16, 95% CI 0.82, 1.64; median Q1 257.3 vs. Q5 400.2 μg/day natural folate); null or negative associations in other studies |
| Hezaveh et al. (2021) | Incidence of non‐melanoma skin cancer (BCC, SCC or both) or overall skin cancer | Folate intake | Cohort studies and CCs |
Scopus, ISI Web of Science and PubMed From 2000 to July 2021 |
4 PCs | Not pooled (few studies and heterogeneous) | Positive association in two studies with BCC risk (RR positive in all quintiles vs. Q1 < 284 μg/day total folate, RRQ5 vs. Q1 1.19, 95% CI 1.01, 1.40 (van Dam et al., 2000); positive in all quintiles versus Q1, median Q1 208 μg/day total folate, RRQ5 vs. Q1: 1.2 95% CI:1.1–1.3 (Fung et al. 2002). Positive association with overall skin cancer (HR positive for T2 and T3 vs. T1, T1 mean 222 μg DFE/day total folate, HRT3 vs. T1: 1.79; 95% CI: 1.07, 2.99 (Donnenfeld et al., 2015). No association with SCC in one study (Fung et al., 2003) |
Abbreviations: BCC, basal cell carcinoma; CCs, case–control studies; CI, confidence interval; FS, food supplements; NCCs, nested case–control studies; OR, odd ratio; PCs, prospective cohort studies; P/S, plasma/serum; RR, relative risk; SCC, squamous cell carcinoma.
Results for case–control and cross‐sectional designs not extracted.
TABLE F.2 Data from pooled analyses of individual studies on each type of cancer.
| Reference | Cancer type | Exposure variable | Eligible designs | Search | N included studies a | Pooled estimate |
|---|---|---|---|---|---|---|
| Cho et al. (2006) | Incident lung cancer | Folate intake | PCs and NCCs | Members of the Pooling Project of Prospective Studies of Diet and Cancer | 8 PCs |
Total folate intake Study specific quintiles Multivariable RR (highest vs. lowest) = 1.02; 95% CI 0.83–1.26; Pheterogeneity in quintiles 5 = 0.07 Uniform absolute intake cutpoints Multivariable RR (top category (>600 μg/day) vs. the referent category (200–250 μg/day)) = 1.12; 95% CI 0.85–1.46 |
| Bao et al. (2011) | Incident pancreatic cancer | Folate intake | PCs and NCCs | Members of the Pooling Project of Prospective Studies of Diet and Cancer | 14 PCs |
Total folate intake Study specific quintiles Multivariable RR (highest vs. lowest) = 0.96 (95% CI 0.80–1.16) (Pheterogeneity in quintiles 5 = 0.22) |
| Koushik et al. (2015) | Incident ovarian cancer | Folate intake | PCs and NCCs | Members of the Pooling Project of Prospective Studies of Diet and Cancer | 9 PCs |
Total folate intake Study specific quintiles Multivariable RR (highest vs. lowest) = 1.07; 95% CI 0.89–1.28; Pheterogeneity in quintiles 5 = 0.52 Uniform absolute intake cutpoints Multivariable RR (top category (>800 μg/day) vs. the referent category (250–300 μg/day)) = 0.84; 95% CI 0.65–1.10 |
Abbreviations: CI, confidence interval; NCCs, nested case–control studies; PCs, prospective cohort studies; RR, relative risk.
Members of the Pooling Project of Prospective Studies of Diet and Cancer
EFSA NDA Panel (EFSA Panel on Nutrition, Novel Foods and Food Allergens) , Turck, D. , Bohn, T. , Castenmiller, J. , de Henauw, S. , Hirsch‐Ernst, K.‐I. , Knutsen, H. K. , Maciuk, A. , Mangelsdorf, I. , McArdle, H. J. , Pentieva, K. , Siani, A. , Thies, F. , Tsabouri, S. , Vinceti, M. , Crous‐Bou, M. , Molloy, A. , Ciccolallo, L. , de Sesmaisons Lecarré, A. , Fabiani, L. … Naska, A. (2023). Scientific opinion on the tolerable upper intake level for folate. EFSA Journal, 21(11), 1–119. 10.2903/j.efsa.2023.8353
Adopted: 27 September 2023
Annexes A–E can be found in the online version of this output (in the ‘Supporting information’ section)
NOTES
SCF, 2000. Scientific Committee on Food. Guidelines of the Scientific Committee on Food for the Development of Tolerable Upper Intake Levels for Vitamins and Minerals. in: Scientific Committee on Food, Scientific Panel on Dietetic Products, Nutrition and Allergies (2006). Tolerable Upper Intake Levels for Vitamins and Minerals. European Food Safety Authority. SCF (2001). Scientific Committee on Food. Opinion of the Scientific Committee on Food on the Tolerable Upper Intake Level of Magnesium. in: Scientific Committee on Food, Scientific Panel on Dietetic Products, Nutrition and Allergies (2006). Tolerable Upper Intake Levels for Vitamins and Minerals. European Food Safety Authority.
Vitamin B12 is the generic descriptor for corrinoid compounds exhibiting qualitatively the biological activity of cobalamin. The term cobalamin will be used throughout this opinion.
Commission Delegated Regulation (EU) 2016/127 of 25 September 2015 supplementing Regulation (EU) No 609/2013 of the European Parliament and of the Council as regards the specific compositional and information requirements for infant formula and follow‐on formula and as regards requirements on information relating to infant and young child feeding (Text with EEA relevance). OJ L 25, 2.2.2016, p. 1–29.
Defined as dietary folate equivalent: 1 μg DFE = 1 μg food folate = 0.6 μg folic acid from formula.
Commission Directive 2006/125/EC of 5 December 2006 on processed cereal‐based foods and baby foods for infants and young children (Codified version) (Text with EEA relevance) OJ L 339, 6.12.2006, p. 16–35.
i.e. AR for the population group under consideration was derived by multiplication of the AR of adults with the ratio between the typical weight of each population group and the weight of adults, to the power of 0.75.
i.e. corrections for growth requirements were applied to account for the nutrient amount required to be incorporated into newly formed tissue during growth.
i.e. the UL for the population group under consideration was derived by multiplication of the UL of adults with the ratio between the typical weight of each population group and the weight of group adults.
The expert panel was composed of Anne Molloy (School of Medicine, Trinity College Dublin, Ireland), Amanda MacFarlane (Nutrition Research Division, Health Canada, Canada), Joshua Miller (School of Environmental and Biological Sciences, State University of New Jersey, USA), Barry Shane (Department of Nutritional Sciences and Toxicology, University of California, USA). A hearing of the expert panel was held on 9 December 2021.
Call for tender OC/EFSA/NUTRI/2021/01.
See Table 8 of OHAT's Handbook for Conducting Systematic Reviews for Health Effects Evaluations (OHAT‐NTP, 2019).
Available online: https://www.efsa.europa.eu/it/data‐report/food‐consumption‐data
The Mintel GNPD contains information on over 3 million food and beverage products, of which more than 1 million are or have been available on the European food market. Twenty‐five out of the twenty‐seven EU Member States and Norway are present in the database. The database provides the compulsory ingredient information reported on product labels and the nutrition declaration when available. http://www.mintel.com/globalnew‐products‐database
Working Group consisting of representatives of 27 EU Member States and Norway.
Commission Delegated Regulation (EU) 2017/1522 of 2 June 2017 supplementing Regulation (EU) No 609/2013 of the European Parliament and of the Council as regards the specific compositional and information requirements for total diet replacement for weight control. C/2017/3664. OJ L 230, 6.9.2017, p. 1–9.
Regulation (EC) No 1925/2006 of the European Parliament and of the Council of 20 December 2006 on the addition of vitamins and minerals and of certain other substances to foods, OJ L 404, 30.12.2006, p. 26.
Regulation (EU) No 609/2013 of the European Parliament and of the Council of 12 June 2013 on food intended for infants and young children, food for special medical purposes and total diet replacement for weight control and repealing Council Directive 92/52/EEC, Commission Directives 96/8/EC, 1999/21/EC, 2006/125/EC and 2006/141/EC, Directive 2009/39/EC of the European Parliament and of the Council and Commission Regulations (EC) No 41/2009 and (EC) No 953/2009. OJ L 181, 29.6.2013, pp. 35–56.
Commission Directive 2006/125/EC of 5 December 2006 on processed cereal‐based foods and baby foods for infants and young children, OJ L 339, 6.12.2006, p. 16.
According to Annex XIII of Regulation (EU) No 1169/2011, the generic term ‘folic acid’ is used to designate the vitamin on nutrition declarations. The actual forms used in fortified foods may be folic acid or calcium‐l‐methylfolate. Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the provision of food information to consumers, amending Regulations (EC) No 1924/2006 and (EC) No 1925/2006 of the European Parliament and of the Council, and repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004 Text with EEA relevance. OJ L 304, 22.11.2011, p. 18–63.
Directive 2002/46/EC of the European Parliament and of the Council of 10 June 2002 on the approximation of the laws of the Member States relating to food supplements, OJ L 183, 12.7.2002, p. 51.
The Mintel GNPD provides data on the content of supplements per serving which may not always reflect the daily dose recommended by the manufacturer.
Considering that the minimum and maximum contents of folate in infant formulae and follow‐on formulae are regulated, these are the only foods categories for which ‘added folate’ was not excluded from the estimates (see Annex D).
Defined in the trials as large or tubular–villous or villous or high‐grade dysplasia or colorectal cancer.
Rex, D. K., Ahnen, D. J., Baron, J. A., Batts, K. P., Burke, C. A., Burt, R. W., Goldblum, J. R., Guillem, J. G., Kahi, C. J., Kalady, M. F., et al. Serrated lesions of the colorectum: review and recommendations from an expert panel. Am J Gastroenterology, 107(9), 1315–1329.
When the trial was planned, SSA/Ps were not distinguished from conventional adenoma. Accordingly, SSA/Ps (with and without dysplasia) were included among ‘advanced adenomas’ in the analysis by Cole et al. In the subsequent analysis, ‘advanced conventional adenomas’ and SSA/Ps were analysed separately.
Since 2019, the WHO recommends use of the term sessile serrated lesion rather than sessile serrated adenoma, sessile serrated polyp or sessile serrated adenoma/polyp.
Out of the seven cohorts included in the pooled analysis, five cohorts are included in the forest plot [(i.e. Breast Cancer Detection Demonstration Project (BCDDP) Follow‐up cohort (Flood et al., 2002); NHS and HPFS (Lee et al., 2011); Cancer Prevention Study II (CPS‐II) Nutrition Cohort (Stevens et al., 2011); WHI‐OS (Zschäbitz et al., 2013) and two are not (unpublished data; Prospective Study on Hormones, Diet and Breast Cancer (ORDET); New York State cohort]).
ULadult × (weightinfant 4–6mo/weightadult) = 1000 X (7.2/70) = 102.
REFERENCES
- Affronti, H. C. , Long, M. D. , Rosario, S. R. , Gillard, B. M. , Karasik, E. , Boerlin, C. S. , Pellerite, A. J. , Foster, B. A. , Attwood, K. , Pili, R. , Wilton, J. H. , Campbell, M. J. , & Smiraglia, D. J. (2017). Dietary folate levels alter the kinetics and molecular mechanism of prostate cancer recurrence in the CWR22 model. Oncotarget, 8, 103758–103774. 10.18632/oncotarget.21911 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agamanolis, D. P. , Chester, E. M. , Victor, M. , Kark, J. A. , Hines, J. D. , & Harris, J. W. (1976). Neuropathology of experimental vitamin‐B12 deficiency in monkeys. Neurology, 26, 905–914. 10.1212/wnl.26.10.905 [DOI] [PubMed] [Google Scholar]
- Åkesson, A. , Söderlund, F. , Bärebring, L. , Christensen, J. J. , Olsen, T. , & Witthöft, C. (2023). Preparatory work for the update of the tolerable upper intake levels for folic acid/folate. EFSA supporting publication, 210. 10.2903/sp.efsa.20YY.EN-NNNN [DOI] [Google Scholar]
- Allen, R. H. , Stabler, S. P. , Savage, D. G. , & Lindenbaum, J. (1990). Diagnosis of cobalamin deficiency I: Usefulness of serum methylmalonic acid and total homocysteine concentrations. American Journal of Hematology, 34, 90–98. 10.1002/ajh.2830340204 [DOI] [PubMed] [Google Scholar]
- Amenyah, S. D. , Ward, M. , Strain, J. J. , McNulty, H. , Hughes, C. F. , Dollin, C. , Walsh, C. P. , & Lees‐Murdock, D. J. (2020). Nutritional epigenomics and age‐related disease. Current Developments in Nutrition, 4, nzaa097. 10.1093/cdn/nzaa097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armstrong, L. (2014). Epigenetics (1st ed.). Garland Science. [Google Scholar]
- Bailey, L. B. , Cerda, J. J. , Bloch, B. S. , Busby, M. J. , Vargas, L. , Chandler, C. J. , & Halsted, C. H. (1984). Effect of age on poly‐ and monoglutamyl folacin absorption in human subjects. The Journal of Nutrition, 114, 1770–1776. 10.1093/jn/114.10.1770 [DOI] [PubMed] [Google Scholar]
- Bailey, L. B. , Stover, P. J. , McNulty, H. , Fenech, M. F. , Gregory, J. F., III , Mills, J. L. , Pfeiffer, C. M. , Fazili, Z. , Zhang, M. , Ueland, P. M. , Molloy, A. M. , Caudill, M. A. , Shane, B. , Berry, R. J. , Bailey, R. L. , Hausman, D. B. , Raghavan, R. , & Raiten, D. J. (2015). Biomarkers of nutrition for development‐folate review. Journal of Nutrition, 145, 1636–1680. 10.3945/jn.114.206599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bailey, R. L. , Mills, J. L. , Yetley, E. A. , Gahche, J. J. , Pfeiffer, C. M. , Dwyer, J. T. , Dodd, K. W. , Sempos, C. T. , Betz, J. M. , & Picciano, M. F. (2010). Unmetabolized serum folic acid and its relation to folic acid intake from diet and supplements in a nationally representative sample of adults aged ≥ 60 y in the United States. American Journal of Clinical Nutrition, 92, 383–389. 10.3945/ajcn.2010.29499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bailey, S. W. , & Ayling, J. E. (2009). The extremely slow and variable activity of dihydrofolate reductase in human liver and its implications for high folic acid intake. Proceedings of the National Academy of Sciences of the United States of America, 106, 15424–15429. 10.1073/pnas.0902072106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baldwin, J. N. , & Dalessio, D. J. (1961). Folic acid therapy and spinalcord degeneration in pernicious anemia. The New England Journal of Medicine, 264, 1339–1342. 10.1056/nejm196106292642604 [DOI] [PubMed] [Google Scholar]
- Bao, Y. , Michaud, D. S. , Spiegelman, D. , Albanes, D. , Anderson, K. E. , Bernstein, L. , van den Brandt, P. A. , English, D. R. , Freudenheim, J. L. , Fuchs, C. S. , Giles, G. G. , Giovannucci, E. , Goldbohm, R. A. , Håkansson, N. , Horn‐Ross, P. L. , Jacobs, E. J. , Kitahara, C. M. , Marshall, J. R. , Miller, A. B. , … Smith‐Warner, S. A. (2011). Folate intake and risk of pancreatic cancer: Pooled analysis of prospective cohort studies. Journal of the National Cancer Institute, 103, 1840–1850. 10.1093/jnci/djr431 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron, J. A. , Sandler, R. S. , Haile, R. W. , Mandel, J. S. , Mott, L. A. , & Greenberg, E. R. (1998). Folate intake, alcohol consumption, cigarette smoking, and risk of colorectal adenomas. Journal of the National Cancer Institute, 90, 57–62. 10.1093/jnci/90.1.57 [DOI] [PubMed] [Google Scholar]
- Bassett, J. K. , Brinkman, M. T. , Dugué, P. A. , Ueland, P. M. , Midttun, Ø. , Ulvik, A. , Bolton, D. , Southey, M. C. , English, D. R. , Milne, R. L. , Hodge, A. M. , & Giles, G. G. (2019). Circulating concentrations of B group vitamins and urothelial cell carcinoma. International Journal of Cancer, 144, 1909–1917. 10.1002/ijc.31927 [DOI] [PubMed] [Google Scholar]
- Beilby, J. , Ambrosini, G. L. , Rossi, E. , de Klerk, N. H. , & Musk, A. W. (2010). Serum levels of folate, lycopene, β‐carotene, retinol and vitamin E and prostate cancer risk. European Journal of Clinical Nutrition, 64, 1235–1238. 10.1038/ejcn.2010.124 [DOI] [PubMed] [Google Scholar]
- Berk, W. B. , Bauer, L. , & Castle, J. L. (1948). Folic acid: A report of 12 patients treated with synthetic pteroylglutamic acid: With comments on the pertinent literature. South African Medical Journal, 22, 604–611. 10.10520/AJA20785135_23311 [DOI] [Google Scholar]
- Berry, R. J. (2019). Lack of historical evidence to support folic acid exacerbation of the neuropathy caused by vitamin B12 deficiency. American Journal of Clinical Nutrition, 110, 554–561. 10.1093/ajcn/nqz089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Best, C. N. (1959). Subacute combined degeneration of spinal cord after extensive resection of ileum in Crohn's disease: Report of a case. British Medical Journal, 2, 862–864. 10.1136/bmj.2.5156.862 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Best, K. P. , Green, T. J. , Sulistyoningrum, D. C. , Sullivan, T. R. , Aufreiter, S. , Prescott, S. L. , Makrides, M. , Skubisz, M. , O'Connor, D. L. , & Palmer, D. J. (2021). Maternal late‐pregnancy serum unmetabolized folic acid concentrations are not associated with infant allergic disease: A prospective cohort study. Journal of Nutrition, 151, 1553–1560. 10.1093/jn/nxab040 [DOI] [PubMed] [Google Scholar]
- Bethell, F. H. , & Sturgis, C. C. (1948). The relation of therapy in pernicious anemia to changes in the nervous system; early and late results in a series of cases observed for periods of not less than ten years, and early results of treatment with folic acid. Blood, 3, 57–67. [PubMed] [Google Scholar]
- Bistulfi, G. , Foster, B. A. , Karasik, E. , Gillard, B. , Miecznikowski, J. , Dhiman, V. K. , & Smiraglia, D. J. (2011). Dietary folate deficiency blocks prostate cancer progression in the TRAMP model. Cancer Prevention Research (Philadelphia, Pa), 4, 1825–1834. 10.1158/1940-6207.Capr-11-0140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bizzaro, N. , & Antico, A. (2014). Diagnosis and classification of pernicious anemia. Autoimmunity Reviews, 13, 565–568. 10.1016/j.autrev.2014.01.042 [DOI] [PubMed] [Google Scholar]
- Boilson, A. , Staines, A. , Kelleher, C. C. , Daly, L. , Shirley, I. , Shrivastava, A. , Bailey, S. W. , Alverson, P. B. , Ayling, J. E. , McDermott, A. P. , MacCooey, A. , Scott, J. M. , & Sweeney, M. R. (2012). Unmetabolized folic acid prevalence is widespread in the older Irish population despite the lack of a mandatory fortification program. American Journal of Clinical Nutrition, 96, 613–621. 10.3945/ajcn.111.026633 [DOI] [PubMed] [Google Scholar]
- Bortolus, R. , Filippini, F. , Udali, S. , Rinaldi, M. , Genesini, S. , Gandini, G. , Montagnana, M. , Chiaffarino, F. , Lippi, G. , Pattini, P. , de Grandi, G. , Olivieri, O. , Parazzini, F. , & Friso, S. (2021). B vitamin blood concentrations and one‐carbon metabolism polymorphisms in a sample of Italian women and men attending a unit of transfusion medicine: A cross‐sectional study. European Journal of Nutrition, 60, 2643–2654. 10.1007/s00394-020-02448-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bottiglieri, T. , & Reynolds, E. (2010). Folate and neurological disease: Basic mechanisms. Folate in Health and Disease (Second ed.). CRC Press. [Google Scholar]
- Brämswig, S. , Prinz‐Langenohl, R. , Lamers, Y. , Tobolski, O. , Wintergerst, E. , Berthold, H. K. , & Pietrzik, K. (2009). Supplementation with a multivitamin containing 800 microg of folic acid shortens the time to reach the preventive red blood cell folate concentration in healthy women. International Journal for Vitamin and Nutrition Research, 79, 61–70. 10.1024/0300-9831.79.2.61 [DOI] [PubMed] [Google Scholar]
- Caffrey, A. , Irwin, R. E. , McNulty, H. , Strain, J. J. , Lees‐Murdock, D. J. , McNulty, B. A. , Ward, M. , Walsh, C. P. , & Pentieva, K. (2018). Gene‐specific DNA methylation in newborns in response to folic acid supplementation during the second and third trimesters of pregnancy: Epigenetic analysis from a randomized controlled trial. American Journal of Clinical Nutrition, 107, 566–575. 10.1093/ajcn/nqx069 [DOI] [PubMed] [Google Scholar]
- Cai, S. , Quan, S. , Yang, G. , Ye, Q. , Chen, M. , Yu, H. , Wang, G. , Wang, Y. , Zeng, X. , & Qiao, S. (2021). One carbon metabolism and mammalian pregnancy outcomes. Molecular Nutrition & Food Research, 65, 2000734. 10.1002/mnfr.202000734 [DOI] [PubMed] [Google Scholar]
- Campos‐Giménez, E. , Bénet, S. , Oguey, Y. , Martin, F. , & Redeuil, K. (2018). The contribution of minor folates to the total vitamin B9 content of Infant formula and clinical nutrition products. Food Chemistry, 249, 91–97. 10.1016/j.foodchem.2017.12.061 [DOI] [PubMed] [Google Scholar]
- Castenmiller, J. J. , van de Poll, C. J. , West, C. E. , Brouwer, I. A. , Thomas, C. M. , & van Dusseldorp, M. (2000). Bioavailability of folate from processed spinach in humans. Effect of food matrix and interaction with carotenoids. Annals of Nutrition & Metabolism, 44, 163–169. 10.1159/000012840 [DOI] [PubMed] [Google Scholar]
- Caudill, M. A. , Cruz, A. C. , Gregory, J. F., 3rd , Hutson, A. D. , & Bailey, L. B. (1997). Folate status response to controlled folate intake in pregnant women. Journal of Nutrition, 127, 2363–2370. 10.1093/jn/127.12.2363 [DOI] [PubMed] [Google Scholar]
- Chanarin, I. (1980). Cobalamins and nitrous oxide: A review. Journal of Clinical Pathology, 33, 909–916. 10.1136/jcp.33.10.909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen, H. , Qin, L. , Gao, R. , Jin, X. L. , Cheng, K. , Zhang, S. , Hu, X. , Xu, W. , & Wang, H. (2021). Neurodevelopmental effects of maternal folic acid supplementation: A systematic review and meta‐analysis. Critical Reviews in Food Science and Nutrition, 63, 3771–3787. 10.1080/10408398.2021.1993781 [DOI] [PubMed] [Google Scholar]
- Chen, Q. , Huang, L. X. , Xu, W. J. , Chen, H. , Zhong, J. Q. , & Zeng, C. X. (2014). Research on the prevalence and the risk factors of autism spectrum disorder from 1.5 to 3 years old in Zhuhai city. Chinese Journal of Child Health Care, 22, 649–651. 10.11852/zgetbjzz2014-22-06-28 [DOI] [Google Scholar]
- Chen, Z. , Xing, Y. , Yu, X. , Dou, Y. , & Ma, D. (2021). Effect of folic acid intake on infant and child allergic diseases: Systematic review and meta‐analysis. Frontiers in Pediatrics, 8, 615406. 10.3389/fped.2020.615406 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cho, C. E. , Sánchez‐Hernández, D. , Reza‐López, S. A. , Huot, P. S. , Kim, Y. I. , & Anderson, G. H. (2013). High folate gestational and post‐weaning diets alter hypothalamic feeding pathways by DNA methylation in Wistar rat offspring. Epigenetics, 8, 710–719. 10.4161/epi.24948 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cho, E. , Hunter, D. J. , Spiegelman, D. , Albanes, D. , Beeson, W. L. , van den Brandt, P. A. , Colditz, G. A. , Feskanich, D. , Folsom, A. R. , Fraser, G. E. , Freudenheim, J. L. , Giovannucci, E. , Goldbohm, R. A. , Graham, S. , Miller, A. B. , Rohan, T. E. , Sellers, T. A. , Virtamo, J. , Willett, W. C. , & Smith‐Warner, S. A. (2006). Intakes of vitamins A, C and E and folate and multivitamins and lung cancer: A pooled analysis of 8 prospective studies. International Journal of Cancer, 118, 970–978. 10.1002/ijc.21441 [DOI] [PubMed] [Google Scholar]
- Cho, E. , Zhang, X. , Townsend, M. K. , Selhub, J. , Paul, L. , Rosner, B. A. , Fuchs, C. S. , Willett, W. C. , & Giovannucci, E. L. (2015). Unmetabolized folic acid in prediagnostic plasma and the risk for colorectal cancer. JNCI: Journal of the National Cancer Institute, 107, djv260. 10.1093/jnci/djv260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chodos, R. B. , & Ross, J. F. (1951). The effects of combined folic acid and liver extract therapy. Blood, 6, 1213–1233. [PubMed] [Google Scholar]
- Cichowicz, D. J. , & Shane, B. (1987). Mammalian folylpoly‐gamma‐glutamate synthetase. 2 Substrate specificity and kinetic properties. Biochemistry, 26, 513–521. 10.1021/bi00376a025 [DOI] [PubMed] [Google Scholar]
- Clarke, R. , Birks, J. , Nexo, E. , Ueland, P. M. , Schneede, J. , Scott, J. , Molloy, A. , & Evans, J. G. (2007). Low vitamin B‐12 status and risk of cognitive decline in older adults. The American Journal of Clinical Nutrition, 86, 1384–1391. 10.1093/ajcn/86.5.1384 [DOI] [PubMed] [Google Scholar]
- Clarke, R. , Sherliker, P. , Hin, H. , Molloy, A. M. , Nexo, E. , Ueland, P. M. , Emmens, K. , Scott, J. M. , & Evans, J. G. (2008). Folate and vitamin B‐12 status in relation to cognitive impairment and anaemia in the setting of voluntary fortification in the UK. British Journal of Nutrition, 100, 1054–1059. 10.1017/s0007114508958001 [DOI] [PubMed] [Google Scholar]
- Cochrane, K. M. , Williams, B. A. , Elango, R. , Barr, S. I. , & Karakochuk, C. D. (2022). Pregnancy‐induced alterations of 1‐carbon metabolism and significance for maternal nutrition requirements. Nutrition Reviews, 80, 1985–2001. 10.1093/nutrit/nuac015 [DOI] [PubMed] [Google Scholar]
- Cole, B. F. , Baron, J. A. , Sandler, R. S. , Haile, R. W. , Ahnen, D. J. , Bresalier, R. S. , McKeown‐Eyssen, G. , Summers, R. W. , Rothstein, R. I. , & Burke, C. A. (2007). Folic acid for the prevention of colorectal adenomas: A randomized clinical trial. JAMA, 297, 2351–2359. 10.1001/jama.297.21.2351 [DOI] [PubMed] [Google Scholar]
- Conley, C. L. , & Krevans, J. R. (1951). Development of neurologic manifestations of pernicious anemia during multivitamin therapy. New England Journal of Medicine, 245, 529–531. 10.1056/nejm195110042451404 [DOI] [PubMed] [Google Scholar]
- Crider, K. S. , Cordero, A. M. , Qi, Y. P. , Mulinare, J. , Dowling, N. F. , & Berry, R. J. (2013). Prenatal folic acid and risk of asthma in children: A systematic review and meta‐analysis. American Journal of Clinical Nutrition, 98, 1272–1281. 10.3945/ajcn.113.065623 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crider, K. S. , Zhu, J. H. , Hao, L. , Yang, Q. H. , Yang, T. P. , Gindler, J. , Maneval, D. R. , Quinlivan, E. P. , Li, Z. , Bailey, L. B. , & Berry, R. J. (2011). MTHFR 677C‐>T genotype is associated with folate and homocysteine concentrations in a large, population‐based, double‐blind trial of folic acid supplementation. The American Journal of Clinical Nutrition, 93, 1365–1372. 10.3945/ajcn.110.004671 [DOI] [PubMed] [Google Scholar]
- Crockett, S. D. , & Nagtegaal, I. D. (2019). Terminology, molecular features, epidemiology, and management of serrated colorectal neoplasia. Gastroenterology, 157, 949–966.e4. 10.1053/j.gastro.2019.06.041 [DOI] [PubMed] [Google Scholar]
- Crosby, W. H. (1960). The danger of folic acid in multivitamin preparations. Military Medicine, 125, 233–235. [PubMed] [Google Scholar]
- Davidson, L. S. , & Girdwood, R. H. (1947). Folic acid as a therapeutic agent. British Medicine Journal, 1, 587–591. 10.1136/bmj.1.4504.587 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Batlle, J. , Matejcic, M. , Chajes, V. , Moreno‐Macias, H. , Amadou, A. , Slimani, N. , Cox, D. G. , Clavel‐Chapelon, F. , Fagherazzi, G. , & Romieu, I. (2018). Determinants of folate and vitamin B12 plasma levels in the French E3N‐EPIC cohort. European Journal of Nutrition, 57, 751–760. 10.1007/s00394-016-1365-z [DOI] [PubMed] [Google Scholar]
- de Jong, R. J. , Verwei, M. , West, C. E. , van Vliet, T. , Siebelink, E. , van den Berg, H. , & Castenmiller, J. J. (2005). Bioavailability of folic acid from fortified pasteurised and UHT‐treated milk in humans. European Journal of Clinical Nutrition, 59, 906–913. 10.1038/sj.ejcn.1602159 [DOI] [PubMed] [Google Scholar]
- de Meer, K. , Smulders, Y. M. , Dainty, J. R. , Smith, D. E. , Kok, R. M. , Stehouwer, C. D. , Finglas, P. M. , & Jakobs, C. (2005). [6S]5‐methyltetrahydrofolate or folic acid supplementation and absorption and initial elimination of folate in young and middle‐aged adults. European Journal of Clinical Nutrition, 59, 1409–1416. 10.1038/sj.ejcn.1602254 [DOI] [PubMed] [Google Scholar]
- de Vogel, S. , Meyer, K. , Fredriksen, Å. , Ulvik, A. , Ueland, P. M. , Nygård, O. , Vollset, S. E. , Tell, G. S. , Tretli, S. , & Bjørge, T. (2013). Serum folate and vitamin B12 concentrations in relation to prostate cancer risk–a Norwegian population‐based nested case‐control study of 3000 cases and 3000 controls within the JANUS cohort. International Journal of Epidemiology, 42, 201–210. 10.1093/ije/dys199 [DOI] [PubMed] [Google Scholar]
- Dehkordi, E. H. , Sedehi, M. , Shahraki, Z. G. , & Najafi, R. (2016). Effect of folic acid on homocysteine and insulin resistance of overweight and obese children and adolescents. Advanced Biomedical Research, 5, 88. 10.4103/2277-9175.182219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- den Dekker, H. T. , Jaddoe, V. W. V. , Reiss, I. K. , de Jongste, J. C. , & Duijts, L. (2018). Maternal folic acid use during pregnancy, methylenetetrahydrofolate reductase gene polymorphism, and child's lung function and asthma. Clinical and Experimental Allergy: Journal of the British Society for Allergy and Clinical Immunology, 48, 175–185. 10.1111/cea.13056 [DOI] [PubMed] [Google Scholar]
- DeVilbiss, E. A. , Magnusson, C. , Gardner, R. M. , Rai, D. , Newschaffer, C. J. , Lyall, K. , Dalman, C. , & Lee, B. K. (2017). Antenatal nutritional supplementation and autism spectrum disorders in the Stockholm youth cohort: Population based cohort study. BMJ, 359, j4273. 10.1136/bmj.j4273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ding, H. , Gao, Q. Y. , Chen, H. M. , & Fang, J. Y. (2016). People with low serum folate levels have higher risk of colorectal adenoma/advanced colorectal adenoma occurrence and recurrence in China. The Journal of international medical research, 44, 767–778. 10.1177/0300060516650075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dinn, J. J. , McCann, S. , Wilson, P. , Reed, B. , Weir, D. , & Scott, J. (1978). Animal model for subacute combined degeneration. The Lancet, 312, 1154. 10.1016/S0140-6736(78)92314-0 [DOI] [PubMed] [Google Scholar]
- Dinn, J. J. , Weir, D. G. , McCann, S. , Reed, B. , Wilson, P. , & Scott, J. M. (1980). Methyl group deficiency in nerve tissue: A hypothesis to explain the lesion of subacute combined degeneration. Irish Journal of Medical Science, 149, 1–4. 10.1007/BF02939099 [DOI] [PubMed] [Google Scholar]
- Doets, E. L. , Ueland, P. M. , Tell, G. S. , Vollset, S. E. , Nygard, O. K. , Van't Veer, P. , De Groot, L. , Nurk, E. , Refsum, H. , Smith, A. D. , & Eussen, S. (2014). Interactions between plasma concentrations of folate and markers of vitamin B‐12 status with cognitive performance in elderly people not exposed to folic acid fortification: The Hordaland Health Study. British Journal of Nutrition, 111, 1085–1095. 10.1017/s000711451300336x [DOI] [PubMed] [Google Scholar]
- Donnenfeld, M. , Deschasaux, M. , Latino‐Martel, P. , Diallo, A. , Galan, P. , Hercberg, S. , Ezzedine, K. , & Touvier, M. (2015). Prospective association between dietary folate intake and skin cancer risk: Results from the Supplémentation en Vitamines et Minéraux Antioxydants cohort. The American Journal of Clinical Nutrition, 102, 471–478. 10.3945/ajcn.115.109041 [DOI] [PubMed] [Google Scholar]
- Du, L. , Wang, Y. , Zhang, H. , Zhang, H. , & Gao, Y. (2016). Folate intake and the risk of endometrial cancer: A meta‐analysis. Oncotarget, 7, 85176–85184. 10.18632/oncotarget.13211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ducker, G. S. , & Rabinowitz, J. D. (2017). One‐carbon metabolism in health and disease. Cell Metabolism, 25, 27–42. 10.1016/j.cmet.2016.08.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunstan, J. A. , West, C. , McCarthy, S. , Metcalfe, J. , Meldrum, S. , Oddy, W. H. , Tulic, M. K. , D'Vaz, N. , & Prescott, S. L. (2012). The relationship between maternal folate status in pregnancy, cord blood folate levels, and allergic outcomes in early childhood. Allergy, 67, 50–57. 10.1111/j.1398-9995.2011.02714.x [DOI] [PubMed] [Google Scholar]
- Durga, J. , van Boxtel, M. P. , Schouten, E. G. , Kok, F. J. , Jolles, J. , Katan, M. B. , & Verhoef, P. (2007). Effect of 3‐year folic acid supplementation on cognitive function in older adults in the FACIT trial: A randomised, double blind, controlled trial. Lancet, 369, 208–216. 10.1016/s0140-6736(07)60109-3 [DOI] [PubMed] [Google Scholar]
- Duthie, S. J. , Duthie, G. G. , Russell, W. R. , Kyle, J. A. M. , Macdiarmid, J. I. , Rungapamestry, V. , Stephen, S. , Megias‐Baeza, C. , Kaniewska, J. J. , Shaw, L. , Milne, L. , Bremner, D. , Ross, K. , Morrice, P. , Pirie, L. P. , Horgan, G. , & Bestwick, C. S. (2018). Effect of increasing fruit and vegetable intake by dietary intervention on nutritional biomarkers and attitudes to dietary change: A randomised trial. European Journal of Nutrition, 57, 1855–1872. 10.1007/s00394-017-1469-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA (European Food Safety Authority) . (2009). EFSA meeting summary report. Folic acid: An update on scientific developments. EFSA Journal, 6(8), EN‐2. 10.2903/sp.efsa.2009.EN-2 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2010). Application of systematic review methodology to food and feed safety assessments to support decision making. EFSA Journal, 8(6), 90. 10.2903/j.efsa.2010.1637 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2011). Use of the EFSA Comprehensive European Food Consumption Database in Exposure Assessment. EFSA Journal, 9(3), 34. 10.2903/j.efsa.2011.2097 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2015b). Scientific report on principles and process for dealing with data and evidence in scientific assessments. EFSA Journal, 13(5), 35. 10.2903/j.efsa.2015.4121 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2015a). The food classification and description system FoodEx 2 (revision 2). EFSA Supporting Publication, 12(5), 90. 10.2903/sp.efsa.2015.EN-804 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2022). Protocol for the intake assessments performed in the context of the revision of Tolerable Upper Intake Levels for selected nutrients. EFSA Supporting publication, 2022, e200801. 10.2903/sp.efsa.2022.e200801 [DOI] [Google Scholar]
- EFSA AFC Panel (EFSA Panel on food additives, flavourings, processing aids and materials in contact with food) . (2004). Opinion of the Scientific Panel on food additives, flavourings, processing aids and materials in contact with food (AFC) related to Calcium L‐Methylfolate. EFSA Journal, 2(11), 20. 10.2903/j.efsa.2004.135 [DOI] [Google Scholar]
- EFSA ANS Panel (EFSA Panel on Food Additives and Nutrient Sources added to Food) . (2013). Scientific Opinion on (6S)‐5‐methyltetrahydrofolic acid, glucosamine salt as a source of folate added for nutritional purposes to food supplements. EFSA Journal, 11(10), 20. 10.2903/j.efsa.2013.3358 [DOI] [Google Scholar]
- EFSA FEEDAP Panel (Panel on Additives and Products or Substances used in Animal Feed) , 2012. Scientific Opinion on the safety and efficacy of folic acid as a feed additive for all animal species. EFSA Journal, 10(5), 18. [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies) . (2009). Scientific Opinion of the Panel on Dietetic Products Nutrition and Allergies on a request from the European Commission on the safety of glucosamine hydrochloride from Aspergillus niger as food ingredient. EFSA Journal, 8(7), 19. 10.2903/j.efsa.2010.1687 [DOI] [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition, Allergies) . (2014). Scientific Opinion on Dietary Reference Values for folate. EFSA Journal, 12(11), 59. 10.2903/j.efsa.2014.3893 [DOI] [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies) . (2015). Scientific Opinion on Dietary Reference Values for cobalamin (vitamin B12). EFSA Journal, 13(7), 64. 10.2903/j.efsa.2015.4150 [DOI] [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Nutrition, Novel Foods, Food Allergens) . (2022a). Guidance for establishing and applying tolerable upper intake levels for vitamins and essential minerals. EFSA Journal, 20(1), 27. 10.2903/j.efsa.2022.e200102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Nutrition, Novel Foods, Food Allergens) . (2020). Calcium l‐methylfolate as a source of folate added for nutritional purposes to infant and follow‐on formula, baby food and processed cereal‐based food. EFSA Journal, 18(1), 17. 10.2903/j.efsa.2020.5947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Nutrition, Novel Foods, Food Allergens) . (2022b). Conversion of calcium‐l‐methylfolate and (6S)‐5‐methyltetrahydrofolic acid glucosamine salt into dietary folate equivalents. EFSA Journal, 20(8), 56. 10.2903/j.efsa.2022.7452 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA Scientific Committee . (2011). Statistical significance and biological relevance. EFSA Journal, 9(9), 17. 10.2903/j.efsa.2011.2372 [DOI] [Google Scholar]
- EFSA Scientific Committee . (2017a). Guidance on the assessment of the biological relevance of data in scientific assessments. EFSA Journal, 15(8), 73. 10.2903/j.efsa.2017.4970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA Scientific Committee . (2017b). Guidance on the use of the weight of evidence approach in scientific assessments. EFSA Journal, 15(8), 69. 10.2903/j.efsa.2017.4971 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA Scientific Committee . (2018). Guidance on Uncertainty Analysis in Scientific Assessments. EFSA Journal, 16(1), 39. 10.2903/j.efsa.2018.5123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA Scientific Committee . (2020). Draft for internal testing Scientific Committee guidance on appraising and integrating evidence from epidemiological studies for use in EFSA's scientific assessments. EFSA Journal, 18(8), 83. 10.2903/j.efsa.2020.6221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Egorova, O. , Myte, R. , Schneede, J. , Hägglöf, B. , Bölte, S. , Domellöf, E. , Ivars A'roch, B. , Elgh, F. , Ueland, P. M. , & Silfverdal, S. A. (2020). Maternal blood folate status during early pregnancy and occurrence of autism spectrum disorder in offspring: A study of 62 serum biomarkers. Molecular Autism, 11, 7. 10.1186/s13229-020-0315-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellison, A. B. (1960). Pernicious anemia masked by multivitamins containing folic acid. Journal of the American Medical Association, 173, 240–243. 10.1001/jama.1960.03020210020006 [DOI] [PubMed] [Google Scholar]
- Elnakat, H. , & Ratnam, M. (2004). Distribution, functionality and gene regulation of folate receptor isoforms: Implications in targeted therapy. Advanced Drug Delivery Reviewa, 56, 1067–1084. 10.1016/j.addr.2004.01.001 [DOI] [PubMed] [Google Scholar]
- Essén, A. , Santaolalla, A. , Garmo, H. , Hammar, N. , Walldius, G. , Jungner, I. , Malmstrom, H. , Holmberg, L. , & Van Hemelrijck, M. (2019). Baseline serum folate, vitamin B12 and the risk of prostate and breast cancer using data from the Swedish AMORIS cohort. Cancer Causes and Control, 30, 603–615. 10.1007/s10552-019-01170-6 [DOI] [PubMed] [Google Scholar]
- Eussen, S. J. , Vollset, S. E. , Igland, J. , Meyer, K. , Fredriksen, A. , Ueland, P. M. , Jenab, M. , Slimani, N. , Boffetta, P. , Overvad, K. , Tjonneland, A. , Olsen, A. , Clavel‐Chapelon, F. , Boutron‐Ruault, M. C. , Morois, S. , Weikert, C. , Pischon, T. , Linseisen, J. , Kaaks, R. , … Riboli, E. (2010). Plasma folate, related genetic variants, and colorectal cancer risk in EPIC. Cancer Epidemiology, Biomarkers and Prevention, 19, 1328–1340. 10.1158/1055-9965.EPI-09-0841 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EVM (Food Standards Agency) , 2003. Safe upper levels for vitamins and minerals (pp. 81–92).
- FAO/WHO (Food and Agriculture Organization of the United Nations/World Health Organization) , 2004. Vitamin and Mineral Requirements in Human Nutrition.WHO and FAO (Eds.), (2nd ed). [Google Scholar]
- FAO/WHO (Food and Agriculture Organization of the United Nations/World Health Organization) . (2009). Principles and methods for the risk assessment of chemicals in food. Environmental Health Criteria, 240. [Google Scholar]
- Fazili, Z. , Sternberg, M. R. , Potischman, N. , Wang, C. Y. , Storandt, R. J. , Yeung, L. , Yamini, S. , Gahche, J. J. , Juan, W. , Qi, Y. P. , Paladugula, N. , Gabey, G. , & Pfeiffer, C. M. (2020). Demographic, physiologic, and lifestyle characteristics observed with serum total folate differ among folate forms: Cross‐sectional data from fasting samples in the NHANES 2011–2016. Journal of Nutrition, 150, 851–860. 10.1093/jn/nxz278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fenech, M. , Noakes, M. , Clifton, P. , & Topping, D. (2005). Aleurone flour increases red‐cell folate and lowers plasma homocyst(e)ine substantially in man. British Journal of Nutrition, 93, 353–360. 10.1079/bjn20051377 [DOI] [PubMed] [Google Scholar]
- Figueiredo, J. C. , Grau, M. V. , Haile, R. W. , Sandler, R. S. , Summers, R. W. , Bresalier, R. S. , Burke, C. A. , McKeown‐Eyssen, G. E. , & Baron, J. A. (2009). Folic acid and risk of prostate cancer: Results from a randomized clinical trial. JNCI‐Journal of the National Cancer Institute, 101, 432–435. 10.1093/jnci/djp019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Figueiredo, J. C. , Levine, A. J. , Grau, M. V. , Barry, E. L. , Ueland, P. M. , Ahnen, D. J. , Byers, T. , Bresalier, R. S. , Summers, R. W. , Bond, J. , McKeown‐Eyssen, G. E. , Sandler, R. S. , Haile, R. W. , & Baron, J. A. (2008). Colorectal adenomas in a randomized folate trial: The role of baseline dietary and circulating folate levels. Cancer Epidemiol Biomarkers Prev, 17, 2625–2631. 10.1158/1055-9965.Epi-08-0382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flood, A. , Caprario, L. , Chaterjee, N. , Lacey, J. V., Jr. , Schairer, C. , & Schatzkin, A. (2002). Folate, methionine, alcohol, and colorectal cancer in a prospective study of women in the United States. Cancer Causes & Control, 13, 551–561. 10.1023/a:1016330609603 [DOI] [PubMed] [Google Scholar]
- Fu, H. J. , Zeng, J. , Liu, C. , Gu, Y. , Zou, Y. X. , & Chang, H. (2021). Folate intake and risk of pancreatic cancer: A systematic review and updated meta‐analysis of epidemiological studies. Digestive Diseases and Sciences, 66, 2368–2379. 10.1007/s10620-020-06525-7 [DOI] [PubMed] [Google Scholar]
- Fung, T. T. , Spiegelman, D. , Egan, K. M. , Giovannucci, E. , Hunter, D. J. , & Willett, W. C. (2003). Vitamin and carotenoid intake and risk of squamous cell carcinoma of the skin. International Journal of Cancer, 103, 110–115. 10.1002/ijc.10798 [DOI] [PubMed] [Google Scholar]
- Gao, Q. Y. , Chen, H. M. , Chen, Y. X. , Wang, Y. C. , Wang, Z. H. , Tang, J. T. , Ge, Z. Z. , Chen, X. Y. , Sheng, J. Q. , & Fang, D. C. (2013). Folic acid prevents the initial occurrence of sporadic colorectal adenoma in Chinese older than 50 years of age: A randomized clinical trial. Cancer Prevention Research (Philadelphia, Pa), 6, 744–752. 10.1158/1940-6207.Capr-13-0013 [DOI] [PubMed] [Google Scholar]
- Geijsen, A. , Ulvik, A. , Gigic, B. , Kok, D. E. , van Duijnhoven, F. J. B. , Holowatyj, A. N. , Brezina, S. , van Roekel, E. H. , Baierl, A. , Bergmann, M. M. , Böhm, J. , Bours, M. J. L. , Brenner, H. , Breukink, S. O. , Bronner, M. P. , Chang‐Claude, J. , de Wilt, J. H. W. , Grady, W. M. , Grünberger, T. , … Kampman, E. (2020). Circulating folate and folic acid concentrations: Associations with colorectal cancer recurrence and survival. JNCI Cancer Spectrum, 4. 10.1093/jncics/pkaa051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gellekink, H. , Blom, H. J. , van der Linden, I. J. M. , & den Heijer, M. (2007). Molecular genetic analysis of the human dihydrofolate reductase gene: Relation with plasma total homocysteine, serum and red blood cell folate levels. European Journal of Human Genetics, 15, 103–109. 10.1038/sj.ejhg.5201713 [DOI] [PubMed] [Google Scholar]
- Gibson, T. M. , Weinstein, S. J. , Pfeiffer, R. M. , Hollenbeck, A. R. , Subar, A. F. , Schatzkin, A. , Mayne, S. T. , & Stolzenberg‐Solomon, R. (2011). Pre‐ and postfortification intake of folate and risk of colorectal cancer in a large prospective cohort study in the United States. American Journal of Clinical Nutrition, 94, 1053–1062. 10.3945/ajcn.110.002659 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glynn, S. A. , Albanes, D. , Pietinen, P. , Brown, C. C. , Rautalahti, M. , Tangrea, J. A. , Gunter, E. W. , Barrett, M. J. , Virtamo, J. , & Taylor, P. R. (1996). Colorectal cancer and folate status: A nested case‐control study among male smokers. Cancer epidemiology, biomarkers & prevention, 5, 487–494. [PubMed] [Google Scholar]
- Granell, R. , Heron, J. , Lewis, S. , Davey Smith, G. , Sterne, J. A. , & Henderson, J. (2008). The association between mother and child MTHFR C677T polymorphisms, dietary folate intake and childhood atopy in a population‐based, longitudinal birth cohort. Clinical and Experimental Allergy: Journal of the British Society for Allergy and Clinical Immunology, 38, 320–328. 10.1111/j.1365-2222.2007.02902.x [DOI] [PubMed] [Google Scholar]
- Green, R. , Allen, L. H. , Bjørke‐Monsen, A. L. , Brito, A. , Guéant, J. L. , Miller, J. W. , Molloy, A. M. , Nexo, E. , Stabler, S. , Toh, B. H. , Ueland, P. M. , & Yajnik, C. (2017). Vitamin B(12) deficiency. Nature reviews. Disease Primers, 3, 17040. 10.1038/nrdp.2017.40 [DOI] [PubMed] [Google Scholar]
- Green, T. J. , Skeaff, C. M. , Rockell, J. E. , & Venn, B. J. (2005). Folic acid fortified milk increases blood folate and lowers homocysteine concentration in women of childbearing age. Asia Pacific Journal of Clinical Nutrition, 14, 173–178. [PubMed] [Google Scholar]
- Gu, Y. , Zeng, J. , Zou, Y. , Liu, C. , Fu, H. , & Chang, H. (2022). Folate intake and risk of urothelial carcinoma: a systematic review and meta‐analysis of epidemiological studies. Nutrition and Cancer, 74, 1593–1605. 10.1080/01635581.2021.1973518 [DOI] [PubMed] [Google Scholar]
- Gylling, B. , Van Guelpen, B. , Schneede, J. , Hultdin, J. , Ueland, P. M. , Hallmans, G. , Johansson, I. , & Palmqvist, R. (2014). Low folate levels are associated with reduced risk of colorectal cancer in a population with low folate status. Cancer Epidemiology, Biomarkers and Prevention, 23, 2136–2144. 10.1158/1055-9965.EPI-13-1352 [DOI] [PubMed] [Google Scholar]
- Haberg, S. E. , London, S. J. , Nafstad, P. , Nilsen, R. M. , Ueland, P. M. , Vollset, S. E. , & Nystad, W. (2011). Maternal folate levels in pregnancy and asthma in children at age 3 years. Journal of Allergy and Clinical Immunology, 127, 262–264. 10.1016/j.jaci.2010.10.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haberg, S. E. , London, S. J. , Stigum, H. , Nafstad, P. , & Nystad, W. (2009). Folic acid supplements in pregnancy and early childhood respiratory health. Archives of Disease in Childhood, 94, 180–184. 10.1136/adc.2008.142448 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall, B. E. , & Watkins, C. H. (1947). Experience with pterolyglutamic (synthetic folic) acid in the treatment of pernicious anemia. The Journal of Laboratory and Clinical Medicine, 32, 622–634. [PubMed] [Google Scholar]
- Harrell, F. (2001). Regression modeling strategies with applications to linear models, logistic regression, and survival analysis. Springer. [Google Scholar]
- Harrington, D. J. (2017). Laboratory assessment of vitamin B12 status. Journal of Clinical Pathology, 70, 168–173. 10.1136/jclinpath-2015-203502 [DOI] [PubMed] [Google Scholar]
- He, X. , Wu, K. , Ogino, S. , Giovannucci, E. L. , Chan, A. T. , & Song, M. (2018). Association between risk factors for colorectal cancer and risk of serrated polyps and conventional adenomas. Gastroenterology, 155, 355–373.e318. 10.1053/j.gastro.2018.04.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heinle, R. W. , Dingle, J. T. , & Weisberger, A. S. (1947). Folic acid in the maintenance of pernicious anemia. The Journal of Laboratory and Clinical Medicine, 32, 970–981. [PubMed] [Google Scholar]
- Heuer T, Walter C, Krems C and Hoffmann I (Max Rubner‐Institut), 2012. Nährstoffzufuhr über Supplemente – Ergebnisse der Nationalen Verzehrsstudie II (pp. 86–97).
- Hezaveh, E. , Jafari, S. , Jalilpiran, Y. , Zargarzadeh, N. , Mahdavi, R. , & Gargari, B. P. (2021). Dietary components and the risk of non‐melanoma skin cancer: A systematic review of epidemiological studies. Critical Reviews in Food Science and Nutrition:1–16., 63, 5290–5305. 10.1080/10408398.2021.2016600 [DOI] [PubMed] [Google Scholar]
- Hindborg H (DTU Food National Institute) . (2015. Unpublished). Dietary supplements may contribute to an adequate micronutrient intake in Danish adults but increase the risk of overdose in children.
- Hiraoka, M. , Kato, K. , Saito, Y. , Yasuda, K. , & Kagawa, Y. (2004). Gene‐nutrient and gene‐gene interactions of controlled folate intake by Japanese women. Biochemical and Biophysical Research Communications, 316, 1210–1216. 10.1016/j.bbrc.2004.02.174 [DOI] [PubMed] [Google Scholar]
- Hoile, S. P. , Lillycrop, K. A. , Grenfell, L. R. , Hanson, M. A. , & Burdge, G. C. (2012). Increasing the folic acid content of maternal or post‐weaning diets induces differential changes in phosphoenolpyruvate carboxykinase mRNA expression and promoter methylation in rats. British Journal of Nutrition, 108, 852–857. 10.1017/s0007114511006155 [DOI] [PubMed] [Google Scholar]
- Holm, J. , & Hansen, S. I. (2020). Characterization of soluble folate receptors (folate binding proteins) in humans. Biological roles and clinical potentials in infection and malignancy. Biochimica et Biophysica Acta. Proteins and proteomics, 1868, 140466. 10.1016/j.bbapap.2020.140466 [DOI] [PubMed] [Google Scholar]
- Hopkins, S. M. , Gibney, M. J. , Nugent, A. P. , McNulty, H. , Molloy, A. M. , Scott, J. M. , Flynn, A. , Strain, J. J. , Ward, M. , Walton, J. , & McNulty, B. A. (2015). Impact of voluntary fortification and supplement use on dietary intakes and biomarker status of folate and vitamin B‐12 in Irish adults. American Journal of Clinical Nutrition, 101, 1163–1172. 10.3945/ajcn.115.107151 [DOI] [PubMed] [Google Scholar]
- Hu, J. , Wang, B. , & Sahyoun, N. R. (2016). Application of the key events dose‐response framework to folate metabolism. Critical Reviews in Food Science and Nutrition, 56, 1325–1333. 10.1080/10408398.2013.807221 [DOI] [PubMed] [Google Scholar]
- Huang, Y. , He, Y. , Sun, X. , He, Y. , Li, Y. , & Sun, C. (2014). Maternal high folic acid supplement promotes glucose intolerance and insulin resistance in male mouse offspring fed a high‐fat diet. International Journal of Molecular Sciences, 15, 6298–6313. 10.3390/ijms15046298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hultdin, J. , Van Guelpen, B. , Bergh, A. , Hallmans, G. , & Stattin, P. (2005). Plasma folate, vitamin B12, and homocysteine and prostate cancer risk: A prospective study. International Journal of Cancer, 113, 819–824. 10.1002/ijc.20646 [DOI] [PubMed] [Google Scholar]
- Huo, Y. , Li, J. , Qin, X. , Huang, Y. , Wang, X. , Gottesman, R. F. , Tang, G. , Wang, B. , Chen, D. , He, M. , Fu, J. , Cai, Y. , Shi, X. , Zhang, Y. , Cui, Y. , Sun, N. , Li, X. , Cheng, X. , Wang, J. , … Hou, F. F. (2015). Efficacy of folic acid therapy in primary prevention of stroke among adults with hypertension in China: The CSPPT randomized clinical trial. JAMA, 313, 1325–1335. 10.1001/jama.2015.2274 [DOI] [PubMed] [Google Scholar]
- Hursthouse, N. A. , Gray, A. R. , Miller, J. C. , Rose, M. C. , & Houghton, L. A. (2011). Folate status of reproductive age women and neural tube defect risk: The effect of long‐term folic acid supplementation at doses of 140 μg and 400 μg per day. Nutrients, 3, 49–62. 10.3390/nu3010049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- IOM . (1998). Dietary reference intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline (pp. 150–195). The National Academies Press. [PubMed] [Google Scholar]
- Irwin, R. E. , Thursby, S. J. , Ondičová, M. , Pentieva, K. , McNulty, H. , Richmond, R. C. , Caffrey, A. , Lees‐Murdock, D. J. , McLaughlin, M. , Cassidy, T. , Suderman, M. , Relton, C. L. , & Walsh, C. P. (2019). A randomized controlled trial of folic acid intervention in pregnancy highlights a putative methylation‐regulated control element at ZFP57. Clinical Epigenetics, 11, 31. 10.1186/s13148-019-0618-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Israëls, M. C. G. , & Wilkinson, J. F. (1949). Risk of neurological complications in pernicious anaemia treated with folic acid. The British Medical Journal, 2, 1072–1075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaszewski, R. , Misra, S. , Tobi, M. , Ullah, N. , Naumoff, J. A. , Kucuk, O. , Levi, E. , Axelrod, B. N. , Patel, B. B. , & Majumdar, A. P. (2008). Folic acid supplementation inhibits recurrence of colorectal adenomas: A randomized chemoprevention trial. World journal of gastroenterology, 14, 4492–4498. 10.3748/wjg.14.4492 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jiang, H. , Liu, L. , Sun, D. L. , Yin, X. N. , Chen, Z. D. , Wu, C. A. , & Chen, W. Q. (2016). Interaction between passive smoking and folic acid supplement during pregnancy on autism spectrum disorder behaviors in children aged 3 years. Zhonghua Liu Xing Bing Xue Za Zhi, 37, 940–944. 10.3760/cma.j.issn.0254-6450.2016.07.007 [DOI] [PubMed] [Google Scholar]
- Johansson, M. , Appleby, P. N. , Allen, N. E. , Travis, R. C. , Roddam, A. W. , Egevad, L. , Jenab, M. , Rinaldi, S. , Kiemeney, L. A. , Bueno‐de‐Mesquita, H. B. , Vollset, S. E. , Ueland, P. M. , Sánchez, M.‐J. , Quirós, J. R. , González, C. A. , Larrañaga, N. , Chirlaque, M. D. , Ardanaz, E. , Sieri, S. , … Key, T. J. (2008). Circulating concentrations of folate and vitamin B12 in relation to prostate cancer risk: Results from the European Prospective Investigation into Cancer and Nutrition study. Cancer epidemiology, biomarkers & prevention, 17, 279–285. 10.1158/1055-9965.Epi-07-0657 [DOI] [PubMed] [Google Scholar]
- Joubert, B. R. , den Dekker, H. T. , Felix, J. F. , Bohlin, J. , Ligthart, S. , Beckett, E. , Tiemeier, H. , van Meurs, J. B. , Uitterlinden, A. G. , Hofman, A. , Håberg, S. E. , Reese, S. E. , Peters, M. J. , Andreassen, B. K. , Steegers, E. A. , Nilsen, R. M. , Vollset, S. E. , Midttun, Ø. , Ueland, P. M. , … London, S. J. (2016). Maternal plasma folate impacts differential DNA methylation in an epigenome‐wide meta‐analysis of newborns. Nature Communications, 7, 10577. 10.1038/ncomms10577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kabat, G. C. , Miller, A. B. , Jain, M. , & Rohan, T. E. (2008). Dietary intake of selected B vitamins in relation to risk of major cancers in women. British Journal of Cancer, 99, 816–821. 10.1038/sj.bjc.6604540 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalmbach, R. D. , Choumenkovitch, S. F. , Troen, A. P. , Jacques, P. F. , D'Agostino, R. , & Selhub, J. (2008). A 19‐base pair deletion polymorphism in dihydrofolate reductase is associated with increased unmetabolized folic acid in plasma and decreased red blood cell folate. The Journal of Nutrition, 138, 2323–2327. 10.3945/jn.108.096404 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kamen, B. A. , & Smith, A. K. (2004). A review of folate receptor alpha cycling and 5‐methyltetrahydrofolate accumulation with an emphasis on cell models in vitro. Advanced drug delivery reviews, 56, 1085–1097. 10.1016/j.addr.2004.01.002 [DOI] [PubMed] [Google Scholar]
- Kato, I. , Dnistrian, A. M. , Schwartz, M. , Toniolo, P. , Koenig, K. , Shore, R. E. , Akhmedkhanov, A. , Zeleniuch‐Jacquotte, A. , & Riboli, E. (1999). Serum folate, homocysteine and colorectal cancer risk in women: A nested case‐control study. British Journal of Cancer, 79, 1917–1922. 10.1038/sj.bjc.6690305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kauwell, G. P. , Lippert, B. L. , Wilsky, C. E. , Herrlinger‐Garcia, K. , Hutson, A. D. , Theriaque, D. W. , Rampersaud, G. C. , Cerda, J. J. , & Bailey, L. B. (2000). Folate status of elderly women following moderate folate depletion responds only to a higher folate intake. Journal of Nutrition, 130, 1584–1590. 10.1093/jn/130.6.1584 [DOI] [PubMed] [Google Scholar]
- Kawashima, A. , Madarame, T. , Koike, H. , Komatsu, Y. , & Wise, J. A. (2007). Four week supplementation with mixed fruit and vegetable juice concentrates increased protective serum antioxidants and folate and decreased plasma homocysteine in Japanese subjects. Asia Pacific Journal of Clinical Nutrition, 16, 411–421. [PubMed] [Google Scholar]
- Kehoe L and Walton J, 2022. Report on the intake of micronutrients (Vitamin A, β‐carotene, retinol, vitamin D, vitamin E, vitamin B6, folic acid, iron and manganese) from food supplements in the Irish population . Department of Biological Sciences, Munster Technological University, Report commissioned by the Food Safety Authority of Ireland, 7 pp. [Google Scholar]
- Kelly, P. , McPartlin, J. , Goggins, M. , Weir, D. G. , & Scott, J. M. (1997). Unmetabolized folic acid in serum: Acute studies in subjects consuming fortified food and supplements. American Journal of Clinical Nutrition, 65, 1790–1795. 10.1093/ajcn/65.6.1790 [DOI] [PubMed] [Google Scholar]
- Kerr, M. A. , Livingstone, B. , Bates, C. J. , Bradbury, I. , Scott, J. M. , Ward, M. , Pentieva, K. , Mansoor, M. A. , & McNulty, H. (2009). Folate, related B vitamins, and homocysteine in childhood and adolescence: Potential implications for disease risk in later life. Pediatrics, 123, 627–635. 10.1542/peds.2008-1049 [DOI] [PubMed] [Google Scholar]
- Keszei, A. P. , Verhage, B. A. , Heinen, M. M. , Goldbohm, R. A. , & van den Brandt, P. A. (2009). Dietary folate and folate vitamers and the risk of pancreatic cancer in The Netherlands cohort study. Cancer epidemiology, biomarkers & prevention, 18, 1785–1791. 10.1158/1055-9965.Epi-08-1220 [DOI] [PubMed] [Google Scholar]
- Kiefte‐de Jong, J. C. , Timmermans, S. , Jaddoe, V. W. , Hofman, A. , Tiemeier, H. , Steegers, E. A. , de Jongste, J. C. , & Moll, H. A. (2012). High circulating folate and vitamin B‐12 concentrations in women during pregnancy are associated with increased prevalence of atopic dermatitis in their offspring. The Journal of Nutrition, 142, 731–738. 10.3945/jn.111.154948 [DOI] [PubMed] [Google Scholar]
- Kim, D. H. , Smith‐Warner, S. A. , Spiegelman, D. , Yaun, S. S. , Colditz, G. A. , Freudenheim, J. L. , Giovannucci, E. , Goldbohm, R. A. , Graham, S. , Harnack, L. , Jacobs, E. J. , Leitzmann, M. , Mannisto, S. , Miller, A. B. , Potter, J. D. , Rohan, T. E. , Schatzkin, A. , Speizer, F. E. , Stevens, V. L. , … Hunter, D. J. (2010). Pooled analyses of 13 prospective cohort studies on folate intake and colon cancer. Cancer Causes & Control, 21, 1919–1930. 10.1007/s10552-010-9620-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, S. J. , Zuchniak, A. , Sohn, K. J. , Lubinski, J. , Demsky, R. , Eisen, A. , Akbari, M. R. , Kim, Y. I. , Narod, S. A. , & Kotsopoulos, J. (2016). Plasma folate, vitamin B‐6, and vitamin B‐12 and breast cancer risk in BRCA1‐ and BRCA2‐mutation carriers: A prospective study. American Journal of Clinical Nutrition, 104, 671–677. 10.3945/ajcn.116.133470 [DOI] [PubMed] [Google Scholar]
- Kim, Y. I. (2016). Current Status of Folic Acid Supplementation on Colorectal Cancer Prevention. Current Pharmacology Reports, 2, 21–33. 10.1007/s40495-016-0046-1 [DOI] [Google Scholar]
- Kim, Y. I. , Salomon, R. N. , Graeme‐Cook, F. , Choi, S. W. , Smith, D. E. , Dallal, G. E. , & Mason, J. B. (1996). Dietary folate protects against the development of macroscopic colonic neoplasia in a dose responsive manner in rats. Gut, 39, 732–740. 10.1136/gut.39.5.732 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kok, D. E. , Dhonukshe‐Rutten, R. A. , Lute, C. , Heil, S. G. , Uitterlinden, A. G. , van der Velde, N. , van Meurs, J. B. , van Schoor, N. M. , Hooiveld, G. J. , de Groot, L. C. , Kampman, E. , & Steegenga, W. T. (2015). The effects of long‐term daily folic acid and vitamin B12 supplementation on genome‐wide DNA methylation in elderly subjects. Clinical Epigenetics, 7, 121. 10.1186/s13148-015-0154-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koushik, A. , Wang, M. , Anderson, K. E. , van den Brandt, P. , Clendenen, T. V. , Eliassen, A. H. , Freudenheim, J. L. , Genkinger, J. M. , Håkansson, N. , Marshall, J. R. , McCullough, M. L. , Miller, A. B. , Robien, K. , Rohan, T. E. , Schairer, C. , Schouten, L. J. , Tworoger, S. S. , Wang, Y. , Wolk, A. , … Smith‐Warner, S. A. (2015). Intake of vitamins A, C, and E and folate and the risk of ovarian cancer in a pooled analysis of 10 cohort studies. Cancer Causes Control, 26, 1315–1327. 10.1007/s10552-015-0626-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krishnaveni, G. V. , Veena, S. R. , Karat, S. C. , Yajnik, C. S. , & Fall, C. H. D. (2014). Association between maternal folate concentrations during pregnancy and insulin resistance in Indian children. Diabetologia, 57, 110–121. 10.1007/s00125-013-3086-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krondl, M. , Coleman, P. H. , Bradley, C. L. , Lau, D. , & Ryan, N. (1999). Subjectively healthy elderly consuming a liquid nutrition supplement maintained body mass index and improved some nutritional parameters and perceived well‐being. Journal of the American Dietetic Association, 99, 1542–1548. 10.1016/s0002-8223(99)00378-8 [DOI] [PubMed] [Google Scholar]
- Landon, M. J. , & Hey, E. N. (1974). Renal loss of folate in the newborn infant. Archives of Disease in Childhood, 49, 292–296. 10.1136/adc.49.4.292 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Le Marchand, L. , White, K. K. , Nomura, A. M. , Wilkens, L. R. , Selhub, J. S. , Tiirikainen, M. , Goodman, M. T. , Murphy, S. P. , Henderson, B. E. , & Kolonel, L. N. (2009). Plasma levels of B vitamins and colorectal cancer risk: The multiethnic cohort study. Cancer epidemiology, biomarkers & prevention, 18, 2195–2201. 10.1158/1055-9965.EPI-09-0141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Le Marchand, L. , Wilkens, L. R. , Kolonel, L. N. , & Henderson, B. E. (2005). The MTHFR C677T polymorphism and colorectal cancer: The multiethnic cohort study. Cancer epidemiology, biomarkers & prevention, 14, 1198–1203. 10.1158/1055-9965.Epi-04-0840 [DOI] [PubMed] [Google Scholar]
- Lee, J. E. , Wei, E. K. , Fuchs, C. S. , Hunter, D. J. , Lee, I. M. , Selhub, J. , Stampfer, M. J. , Willett, W. C. , Ma, J. , & Giovannucci, E. (2012). Plasma folate, methylenetetrahydrofolate reductase (MTHFR), and colorectal cancer risk in three large nested case‐control studies. Cancer Causes & Control, 23, 537–545. 10.1007/s10552-012-9911-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, J. E. , Willett, W. C. , Fuchs, C. S. , Smith‐Warner, S. A. , Wu, K. , Ma, J. , & Giovannucci, E. (2011). Folate intake and risk of colorectal cancer and adenoma: Modification by time. American Journal of Clinical Nutrition, 93, 817–825. 10.3945/ajcn.110.007781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levine, S. Z. , Kodesh, A. , Viktorin, A. , Smith, L. , Uher, R. , Reichenberg, A. , & Sandin, S. (2018). Association of maternal use of folic acid and multivitamin supplements in the periods before and during pregnancy with the risk of autism spectrum disorder in offspring. JAMA Psychiatry, 75, 176–184. 10.1001/jamapsychiatry.2017.4050 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin, Y. , Dueker, S. R. , Follett, J. R. , Fadel, J. G. , Arjomand, A. , Schneider, P. D. , Miller, J. W. , Green, R. , Buchholz, B. A. , Vogel, J. S. , Phair, R. D. , & Clifford, A. J. (2004). Quantitation of in vivo human folate metabolism. American Journal of Clinical Nutrition, 80, 680–691. 10.1093/ajcn/80.3.680 [DOI] [PubMed] [Google Scholar]
- Lindzon, G. M. , Medline, A. , Sohn, K. J. , Depeint, F. , Croxford, R. , & Kim, Y. I. (2009). Effect of folic acid supplementation on the progression of colorectal aberrant crypt foci. Carcinogenesis, 30, 1536–1543. 10.1093/carcin/bgp152 [DOI] [PubMed] [Google Scholar]
- Litonjua, A. A. , Rifas‐Shiman, S. L. , Ly, N. P. , Tantisira, K. G. , Rich‐Edwards, J. W. , Camargo, C. A., Jr. , Weiss, S. T. , Gillman, M. W. , & Gold, D. R. (2006). Maternal antioxidant intake in pregnancy and wheezing illnesses in children at 2 y of age. American Journal of Clinical Nutrition, 84, 903–911. 10.1093/ajcn/84.4.903 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, W. , Zhou, H. , Zhu, Y. , & Tie, C. (2017). Associations between dietary folate intake and risks of esophageal, gastric and pancreatic cancers: An overall and dose‐response meta‐analysis. Oncotarget, 8, 86828–86842. 10.18632/oncotarget.18775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, X. D. , Zou, M. , Sun, C. , Wu, L. , & Chen, W. X. (2022). Prenatal folic acid supplements and offspring's autism spectrum disorder: A meta‐analysis and meta‐regression. Journal of Autism and Developmental Disorders, 52, 522–539. 10.1007/s10803-021-04951-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Logan, R. F. , Grainge, M. J. , Shepherd, V. C. , Armitage, N. C. , & Muir, K. R. (2008). Aspirin and folic acid for the prevention of recurrent colorectal adenomas. Gastroenterology, 134, 29–38. 10.1053/j.gastro.2007.10.014 [DOI] [PubMed] [Google Scholar]
- Magdelijns, F. J. , Mommers, M. , Penders, J. , Smits, L. , & Thijs, C. (2011). Folic acid use in pregnancy and the development of atopy, asthma, and lung function in childhood. Pediatrics, 128, e135–e144. 10.1542/peds.2010-1690 [DOI] [PubMed] [Google Scholar]
- Martínez, M. E. , Giovannucci, E. , Jiang, R. , Henning, S. M. , Jacobs, E. T. , Thompson, P. , Smith‐Warner, S. A. , & Alberts, D. S. (2006). Folate fortification, plasma folate, homocysteine and colorectal adenoma recurrence. International Journal of Cancer, 119, 1440–1446. [DOI] [PubMed] [Google Scholar]
- Martínez, M. E. , Henning, S. M. , & Alberts, D. S. (2004). Folate and colorectal neoplasia: Relation between plasma and dietary markers of folate and adenoma recurrence. The American Journal of Clinical Nutrition, 79, 691–697. 10.1093/ajcn/79.4.691 [DOI] [PubMed] [Google Scholar]
- Martiniak, Y. , Heuer, T. , & Hoffmann, I. (2015). Intake of dietary folate and folic acid in Germany based on different scenarios for food fortification with folic acid. European Journal of Nutrition, 54, 1045–1054. 10.1007/s00394-014-0781-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martinussen, M. P. , Risnes, K. R. , Jacobsen, G. W. , & Bracken, M. B. (2012). Folic acid supplementation in early pregnancy and asthma in children aged 6 years. American Journal of Obstetrics and Gynecology, 206, 72.e71–72.e77. 10.1016/j.ajog.2011.07.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maruvada, P. , Stover, P. J. , Mason, J. B. , Bailey, R. L. , Davis, C. D. , Field, M. S. , Finnell, R. H. , Garza, C. , Green, R. , Gueant, J. L. , Jacques, P. F. , Klurfeld, D. M. , Lamers, Y. , MacFarlane, A. J. , Miller, J. W. , Molloy, A. M. , O'Connor, D. L. , Pfeiffer, C. M. , Potischman, N. A. , … Zappal, G. (2020). Knowledge gaps in understanding the metabolic and clinical effects of excess folates/folic acid: A summary, and perspectives, from an NIH workshop. American Journal of Clinical Nutrition, 112, 1390–1403. 10.1093/ajcn/nqaa259 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McClung, H. L. , Armstrong, N. J. , Hennigar, S. R. , Staab, J. S. , Montain, S. J. , & Karl, J. P. (2020). Randomized trial comparing consumption of military rations to usual intake for 21 consecutive days: Nutrient adequacy and indicators of health status. Journal of the Academy of Nutrition and Dietetics, 120, 1791–1804. 10.1016/j.jand.2020.06.018 [DOI] [PubMed] [Google Scholar]
- Meadows, D. N. , Bahous, R. H. , Best, A. F. , & Rozen, R. (2015). High dietary folate in mice alters immune response and reduces survival after malarial infection. Plos One, 10, e0143738. 10.1371/journal.pone.0143738 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mensink, G. B. M. , Weißenborn, A. , & Richter, A. (2016). Folate status in Germany. Journal of Health Monitoring, 1, 24–28. 10.17886/rki-gbe-2016-040.2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Metz, J. , Stevens, K. , Krawitz, S. , & Brandt, V. (1961). The plasma clearance of injected doses of folic acid as an index of folic acid deficiency. Journal of Clinical Pathology, 14, 622–625. 10.1136/jcp.14.6.622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer, L. M. (1947). Folic acid in the treatment of pernicious anemia. Blood, 2, 50–62. [PubMed] [Google Scholar]
- Michaud, D. S. , Pietinen, P. , Taylor, P. R. , Virtanen, M. , Virtamo, J. , & Albanes, D. (2002). Intakes of fruits and vegetables, carotenoids and vitamins A, E, C in relation to the risk of bladder cancer in the ATBC cohort study. British Journal of Cancer, 87, 960–965. 10.1038/sj.bjc.6600604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitsopoulou, A. V. , Magriplis, E. , Dimakopoulos, I. , Karageorgou, D. , Bakogianni, I. , Micha, R. , Michas, G. , Chourdakis, M. , Ntouroupi, T. , Tsaniklidou, S. M. , Argyri, K. , Panagiotakos, D. B. , & Zampelas, A. (2020). Micronutrient intakes and their food sources among Greek children and adolescents. Public Health Nutrition, 23, 2314–2326. 10.1017/s136898001900449x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitsopoulou, A. V. , Magriplis, E. , Michas, G. , Micha, R. , Chourdakis, M. , Chrousos, G. P. , Roma, E. , Panagiotakos, D. B. , Zampelas, A. , Karageorgou, D. , Bakogianni, I. , Dimakopoulos, I. , Ntouroupi, T. , Tsaniklidou, S. M. , Argyri, K. , Fappa, E. , Theodoraki, E. M. , Trichia, E. , Sialvera, T. E. , … Manios, I. (2021). Micronutrient dietary intakes and their food sources in adults: the Hellenic National Nutrition and Health Survey (HNNHS). Journal of Human Nutrition and Dietetics, 34, 616–628. 10.1111/jhn.12840 [DOI] [PubMed] [Google Scholar]
- Miyake, Y. , Sasaki, S. , Tanaka, K. , & Hirota, Y. (2011). Maternal B vitamin intake during pregnancy and wheeze and eczema in Japanese infants aged 16‐24 months: The Osaka Maternal and Child Health Study. Pediatric Allergy and Immunology, 22, 69–74. 10.1111/j.1399-3038.2010.01081.x [DOI] [PubMed] [Google Scholar]
- Molloy A (Trinity College), 2023. Personal communication. Oral communication at the expert meeting of the EFSA task force on folate/folic acid. . [Google Scholar]
- Molloy, A. M. (2020). Adverse effects on cognition caused by combined low vitamin B‐12 and high folate status‐we must do better than a definite maybe! Am J Clin Nutr, 112, 1422–1423. 10.1093/ajcn/nqaa286 [DOI] [PubMed] [Google Scholar]
- Molloy, J. , Collier, F. , Saffery, R. , Allen, K. J. , Koplin, J. J. , Louise Ponsonby, A. , Tang, M. L. K. , Ward, A. C. , Martino, D. , Burgner, D. , Carlin, J. B. , Ranganathan, S. , Symeonedies, C. , Dwyer, T. , & Vuillermin, P. (2020). Folate levels in pregnancy and offspring food allergy and eczema. Pediatric Allergy and Immunology, 31, 38–46. 10.1111/pai.13128 [DOI] [PubMed] [Google Scholar]
- Morris, M. S. , Jacques, P. F. , Rosenberg, I. H. , & Selhub, J. (2007). Folate and vitamin B‐12 status in relation to anemia, macrocytosis, and cognitive impairment in older Americans in the age of folic acid fortification. American Journal of Clinical Nutrition, 85, 193–200. 10.1093/ajcn/85.1.193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris, M. S. , Jacques, P. F. , Rosenberg, I. H. , & Selhub, J. (2010). Circulating unmetabolized folic acid and 5‐methyltetrahydrofolate in relation to anemia, macrocytosis, and cognitive test performance in American seniors. American Journal of Clinical Nutrition, 91, 1733–1744. 10.3945/ajcn.2009.28671 [DOI] [PubMed] [Google Scholar]
- Morris, M. S. , Selhub, J. , & Jacques, P. F. (2012). Vitamin B‐12 and Folate Status in Relation to Decline in Scores on the Mini‐Mental State Examination in the Framingham Heart Study. Journal of the American Geriatrics Society, 60, 1457–1464. 10.1111/j.1532-5415.2012.04076.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy, G. , Sansbury, L. B. , Cross, A. J. , Stolzenberg‐Solomon, R. , Laiyemo, A. , Albert, P. S. , Wang, Z. , Schatzkin, A. , Lehman, T. , Kalidindi, A. , Modali, R. , & Lanza, E. (2008). Folate and MTHFR: Risk of adenoma recurrence in the Polyp Prevention Trial. Cancer Causes & Control, 19, 751–758. 10.1007/s10552-008-9137-6 [DOI] [PubMed] [Google Scholar]
- Murphy, M. S. Q. , Muldoon, K. A. , Sheyholislami, H. , Behan, N. , Lamers, Y. , Rybak, N. , White, R. R. , Harvey, A. L. J. , Gaudet, L. M. , Smith, G. N. , Walker, M. C. , Wen, S. W. , & MacFarlane, A. J. (2021). Impact of high‐dose folic acid supplementation in pregnancy on biomarkers of folate status and 1‐carbon metabolism: An ancillary study of the Folic Acid Clinical Trial (FACT). The American Journal of Clinical Nutrition, 113, 1361–1371. 10.1093/ajcn/nqaa407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Toxicology Program (US National Toxicology Program) . (2015). NTP monograph: identifying research needs for assessing safe use of high intakes of folic acid (p. 60). US Department of Health and Human Services. https://ntp.niehs.nih.gov/ntp/ohat/folicacid/final_monograph_508.pdf [Google Scholar]
- Neuhouser, M. L. , Cheng, T. Y. , Beresford, S. A. , Brown, E. , Song, X. , Miller, J. W. , Zheng, Y. , Thomson, C. A. , Shikany, J. M. , Vitolins, M. Z. , Rohan, T. , Green, R. , & Ulrich, C. M. (2015). Red blood cell folate and plasma folate are not associated with risk of incident colorectal cancer in the Women's Health Initiative observational study. International Journal of Cancer, 137, 930–939. 10.1002/ijc.29453 [DOI] [PMC free article] [PubMed] [Google Scholar]
- NHMRC (New Zealand Ministry of Health) , 2006. Nutrient reference values for Australia and New Zealand including recommended dietary intakes. . [Google Scholar]
- Nilsen, R. M. , Surén, P. , Gunnes, N. , Alsaker, E. R. , Bresnahan, M. , Hirtz, D. , Hornig, M. , Lie, K. K. , Lipkin, W. I. , Reichborn‐Kjennerud, T. , Roth, C. , Schjølberg, S. , Smith, G. D. , Susser, E. , Vollset, S. E. , Øyen, A. S. , Magnus, P. , & Stoltenberg, C. (2013). Analysis of self‐selection bias in a population‐based cohort study of autism spectrum disorders. Paediatric and Perinatal Epidemiology, 27, 553–563. 10.1111/ppe.12077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nordic Council of Ministers . (2014). Nordic Nutrition Recommendations 2012. Integrating nutrition and physical activity., 629. [Google Scholar]
- Norsworthy, B. , Skeaff, C. M. , Adank, C. , & Green, T. J. (2004). Effects of once‐a‐week or daily folic acid supplementation on red blood cell folate concentrations in women. European Journal of Clinical Nutrition, 58, 548–554. 10.1038/sj.ejcn.1601843 [DOI] [PubMed] [Google Scholar]
- Nwaru, B. I. , Erkkola, M. , Ahonen, S. , Kaila, M. , Kronberg‐Kippilä, C. , Ilonen, J. , Simell, O. , Knip, M. , Veijola, R. , & Virtanen, S. M. (2011). Intake of antioxidants during pregnancy and the risk of allergies and asthma in the offspring. European Journal of Clinical Nutrition, 65, 937–943. 10.1038/ejcn.2011.67 [DOI] [PubMed] [Google Scholar]
- O'Connor, E. A. , Evans, C. V. , Ivlev, I. , Rushkin, M. C. , Thomas, R. G. , Martin, A. , Lin, J. S. , & (Agency for Healthcare Research and Quality (US)) . (2021). Vitamin, mineral, and multivitamin supplementation for the primary prevention of cardiovascular disease and cancer: A systematic evidence review for the U.S. Preventive Services Task Force. (Evidence Synthesis No. 209). 21‐05278‐EF‐1, Rockville, MD. [PubMed]
- OHAT‐NTP (Office of Health Assessment and Translation‐Division of the National Toxicology Program) . (2015). OHAT risk of bias rating tool for human and animal studies, 37. https://ntp.niehs.nih.gov/ntp/ohat/pubs/riskofbiastool_508.pdf [Google Scholar]
- OHAT‐NTP (Office of Health Assessment and Translation‐Division of the National Toxicology Program) , 2019. Handbook for conducting a literature‐based health assessment using OHAT approach for systematic review and evidence integration. https://ntp.niehs.nih.gov/ntp/ohat/pubs/handbookjan2015_508.pdf [Google Scholar]
- Öhrvik, V. , Lemming, E. W. , Nälsén, C. , Becker, W. , Ridefelt, P. , & Lindroos, A. K. (2018). Dietary intake and biomarker status of folate in Swedish adults. European Journal of Nutrition, 57, 451–462. 10.1007/s00394-016-1328-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ohrvik, V. E. , & Witthoft, C. M. (2011). Human folate bioavailability. Nutrients, 3, 475–490. 10.3390/nu3040475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Keefe, C. A. , Bailey, L. B. , Thomas, E. A. , Hofler, S. A. , Davis, B. A. , Cerda, J. J. , & Gregory, J. F., 3rd . (1995). Controlled dietary folate affects folate status in nonpregnant women. Journal of Nutrition, 125, 2717–2725. 10.1093/jn/125.10.2717 [DOI] [PubMed] [Google Scholar]
- Osborne, C. B. , Lowe, K. E. , & Shane, B. (1993). Regulation of folate and one‐carbon metabolism in mammalian cells. I. Folate metabolism in Chinese hamster ovary cells expressing Escherichia coli or human folylpoly‐gamma‐glutamate synthetase activity. J Biol Chem, 268, 21657–21664. [PubMed] [Google Scholar]
- Otani, T. , Iwasaki, M. , Sasazuki, S. , Inoue, M. , Tsugane, S. , & Japan Public Health Center‐based Prospective Study G . (2008). Plasma folate and risk of colorectal cancer in a nested case‐control study: The Japan Public Health Center‐based prospective study. Cancer Causes & Control, 19, 67–74. [DOI] [PubMed] [Google Scholar]
- Ozaki, M. , Molloy, A. M. , Mills, J. L. , Fan, R. , Wang, Y. , Gibney, E. R. , Shane, B. , Brody, L. C. , & Parle‐McDermott, A. (2015). The dihydrofolate reductase 19 bp polymorphism is not associated with biomarkers of folate status in healthy young adults, irrespective of folic acid intake. The Journal of Nutrition, 145, 2207–2211. 10.3945/jn.115.216101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palchetti, C. Z. , Paniz, C. , de Carli, E. , Marchioni, D. M. , Colli, C. , Steluti, J. , Pfeiffer, C. M. , Fazili, Z. , & Guerra‐Shinohara, E. M. (2017). Association between Serum Unmetabolized Folic Acid Concentrations and Folic Acid from Fortified Foods. Journal of the American College of Nutrition, 36, 572–578. 10.1080/07315724.2017.1333929 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paniz, C. , Bertinato, J. F. , Lucena, M. R. , De Carli, E. , Amorim, P. , Gomes, G. W. , Palchetti, C. Z. , Figueiredo, M. S. , Pfeiffer, C. M. , Fazili, Z. , Green, R. , & Guerra‐Shinohara, E. M. (2017). A daily dose of 5 mg folic acid for 90 days is associated with increased serum unmetabolized folic acid and reduced natural killer cell cytotoxicity in healthy brazilian adults. The Journal of Nutrition, 147, 1677–1685. 10.3945/jn.117.247445 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Papadimitriou, N. , Dimou, N. , Gill, D. , Tzoulaki, I. , Murphy, N. , Riboli, E. , Lewis, S. J. , Martin, R. M. , Gunter, M. J. , & Tsilidis, K. K. (2021). Genetically predicted circulating concentrations of micronutrients and risk of breast cancer: A Mendelian randomization study. International Journal of Cancer, 148, 646–653. 10.1002/ijc.33246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parr, C. L. , Magnus, M. C. , Karlstad, Ø. , Haugen, M. , Refsum, H. , Ueland, P. M. , McCann, A. , Nafstad, P. , Håberg, S. E. , Nystad, W. , & London, S. J. (2017). Maternal folate intake during pregnancy and childhood asthma in a population‐based cohort. American Journal of Respiratory and Critical Care Medicine, 195, 221–228. 10.1164/rccm.201604-0788OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- Passarelli, M. (2023). Personal communication. Re: Question from EFSA on Am J Clin Nutr 2019;110:903–911. Message to Agnès de Sesmaisons Lecarré. 6 April 2023. Email.
- Passarelli, M. N. , Barry, E. L. , Rees, J. R. , Mott, L. A. , Zhang, D. , Ahnen, D. J. , Bresalier, R. S. , Haile, R. W. , McKeown‐Eyssen, G. , Snover, D. C. , Cole, B. F. , & Baron, J. A. (2019). Folic acid supplementation and risk of colorectal neoplasia during long‐term follow‐up of a randomized clinical trial. The American Journal of Clinical Nutrition, 110, 903–911. 10.1093/ajcn/nqz160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paul, L. , & Selhub, J. (2017). Interaction between excess folate and low vitamin B12 status. Molecular aspects of medicine, 53, 43–47. 10.1016/j.mam.2016.11.004 [DOI] [PubMed] [Google Scholar]
- Perlitz, H. , Mensink, G. B. M. , Lage Barbosa, C. , Richter, A. , Brettschneider, A. K. , Lehmann, F. , Patelakis, E. , Frank, M. , Heide, K. , & Haftenberger, M. (2019). Use of vitamin and mineral supplements among adolescents living in Germany‐Results from EsKiMo II. Nutrients, 11. 10.3390/nu11061208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pfeiffer, C. M. , Sternberg, M. R. , Fazili, Z. , Lacher, D. A. , Zhang, M. , Johnson, C. L. , Hamner, H. C. , Bailey, R. L. , Rader, J. I. , Yamini, S. , Berry, R. J. , & Yetley, E. A. (2015). Folate status and concentrations of serum folate forms in the US population: National Health and Nutrition Examination Survey 2011‐2. British Journal of Nutrition, 113, 1965–1977. 10.1017/s0007114515001142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pfeiffer, C. M. , Sternberg, M. R. , Fazili, Z. , Yetley, E. A. , Lacher, D. A. , Bailey, R. L. , & Johnson, C. L. (2015). Unmetabolized folic acid is detected in nearly all serum samples from US children, adolescents, and adults. Journal of Nutrition, 145, 520–531. 10.3945/jn.114.201210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pfeiffer, C. M. , Sternberg, M. R. , Zhang, M. , Fazili, Z. , Storandt, R. J. , Crider, K. S. , Yamini, S. , Gahche, J. J. , Juan, W. , Wang, C. Y. , Potischman, N. , Williams, J. , & LaVoie, D. J. (2019). Folate status in the US population 20 y after the introduction of folic acid fortification. The American Journal of Clinical Nutrition, 110, 1088–1097. 10.1093/ajcn/nqz184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pieroth, R. , Paver, S. , Day, S. , & Lammersfeld, C. (2018). Folate and Its Impact on Cancer Risk. Current nutrition reports, 7, 70–84. 10.1007/s13668-018-0237-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plumptre, L. , Masih, S. P. , Ly, A. , Aufreiter, S. , Sohn, K. J. , Croxford, R. , Lausman, A. Y. , Berger, H. , O'Connor, D. L. , & Kim, Y. I. (2015). High concentrations of folate and unmetabolized folic acid in a cohort of pregnant Canadian women and umbilical cord blood. American Journal of Clinical Nutrition, 102, 848–857. 10.3945/ajcn.115.110783 [DOI] [PubMed] [Google Scholar]
- Pravst, I. , Lavriša, Ž. , Hribar, M. , Hristov, H. , Kvarantan, N. , Seljak, B. K. , Gregorič, M. , Blaznik, U. , Gregorič, N. , Zaletel, K. , Oblak, A. , Osredkar, J. , Žmitek, K. , & Kušar, A. (2021). Dietary intake of folate and assessment of the folate deficiency prevalence in Slovenia using serum biomarkers. Nutrients, 13. 10.3390/nu13113860 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qin, X. , Cui, Y. , Shen, L. , Sun, N. , Zhang, Y. , Li, J. , Xu, X. , Wang, B. , Xu, X. , Huo, Y. , & Wang, X. (2013). Folic acid supplementation and cancer risk: A meta‐analysis of randomized controlled trials. International Journal of Cancer, 133, 1033–1041. 10.1002/ijc.28038 [DOI] [PubMed] [Google Scholar]
- Qin, X. , Shen, L. , Zhang, R. , Li, Y. , Wang, X. , Wang, B. , Jiang, X. , Jiang, H. , Lei, Y. , & Hou, F. F. (2017). Effect of folic acid supplementation on cancer risk among adults with hypertension in China: A randomized clinical trial. International Journal of Cancer, 141, 837–847. 10.1002/ijc.30094 [DOI] [PubMed] [Google Scholar]
- Raghavan, R. , Riley, A. W. , Volk, H. , Caruso, D. , Hironaka, L. , Sices, L. , Hong, X. M. , Wang, G. Y. , Ji, Y. L. , Brucato, M. , Wahl, A. , Stivers, T. , Pearson, C. , Zuckerman, B. , Stuart, E. A. , Landa, R. , Fallin, M. D. , & Wang, X. B. (2018). Maternal multivitamin intake, plasma folate and vitamin B‐12 levels and autism spectrum disorder risk in offspring. Paediatric and Perinatal Epidemiology, 32, 100–111. 10.1111/ppe.12414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raghavan, R. , Selhub, J. , Paul, L. , Ji, Y. L. , Wang, G. Y. , Hong, X. M. , Zuckerman, B. , Fallin, M. D. , & Wang, X. B. (2020). A prospective birth cohort study on cord blood folate subtypes and risk of autism spectrum disorder. American Journal of Clinical Nutrition, 112, 1304–1317. 10.1093/ajcn/nqaa208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Razzak, A. A. , Oxentenko, A. S. , Vierkant, R. A. , Tillmans, L. S. , Wang, A. H. , Weisenberger, D. J. , Laird, P. W. , Lynch, C. F. , Anderson, K. E. , French, A. J. , Haile, R. W. , Harnack, L. J. , Potter, J. D. , Slager, S. L. , Smyrk, T. C. , Thibodeau, S. N. , Cerhan, J. R. , & Limburg, P. J. (2012). Associations between intake of folate and related micronutrients with molecularly defined colorectal cancer risks in the Iowa Women's Health Study. Nutrition and Cancer, 64, 899–910. 10.1080/01635581.2012.714833 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rees, J. R. , Morris, C. B. , Peacock, J. L. , Ueland, P. M. , Barry, E. L. , McKeown‐Eyssen, G. E. , Figueiredo, J. C. , Snover, D. C. , & Baron, J. A. (2017). Unmetabolized folic acid, tetrahydrofolate, and colorectal adenoma risk. Cancer Prevention Research, 10, 451–458. 10.1158/1940-6207.CAPR-16-0278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ren, X. , Xu, P. , Zhang, D. , Liu, K. , Song, D. , Zheng, Y. , Yang, S. , Li, N. , Hao, Q. , Wu, Y. , Zhai, Z. , Kang, H. , & Dai, Z. (2020). Association of folate intake and plasma folate level with the risk of breast cancer: A dose‐response meta‐analysis of observational studies. Aging (Albany NY), 12, 21355–21375. 10.18632/aging.103881 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richmond, R. C. , Sharp, G. C. , Herbert, G. , Atkinson, C. , Taylor, C. , Bhattacharya, S. , Campbell, D. , Hall, M. , Kazmi, N. , Gaunt, T. , McArdle, W. , Ring, S. , Davey Smith, G. , Ness, A. , & Relton, C. L. (2018). The long‐term impact of folic acid in pregnancy on offspring DNA methylation: Follow‐up of the Aberdeen Folic Acid Supplementation Trial (AFAST). International Journal of Epidemiology, 47, 928–937. 10.1093/ije/dyy032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riddell, L. J. , Chisholm, A. , Williams, S. , & Mann, J. I. (2000). Dietary strategies for lowering homocysteine concentrations. The American Journal of Clinical Nutrition, 71, 1448–1454. 10.1093/ajcn/71.6.1448 [DOI] [PubMed] [Google Scholar]
- Ringling, C. , & Rychlik, M. (2017). Simulation of food folate digestion and bioavailability of an oxidation product of 5‐methyltetrahydrofolate. Nutrients, 9. 10.3390/nu9090969 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roe, M. A. , Bell, S. , Oseredczuk, M. , Christensen, T. , Westenbrink, S. , Pakkala, H. , Presser, K. , & Finglas, P. M. (2013). Updated food composition database for nutrient intake. Project developed on the procurement project CFT/EFSA/DCM/2011/03. EFSA Supporting Publication 2013, 10(6), 21. 10.2903/sp.efsa.2013.EN-355 [DOI] [Google Scholar]
- Ross, J. F. , Belding, H. , & Paegel, B. L. (1948). The development and progression of subacute combined degeneration of the spinal cord in patients with pernicious anemia treated with synthetic pteroylglutamic (folic) acid. Blood, 3, 68–90. [PubMed] [Google Scholar]
- Rossi, E. , Hung, J. , Beilby, J. P. , Knuiman, M. W. , Divitini, M. L. , & Bartholomew, H. (2006). Folate levels and cancer morbidity and mortality: Prospective cohort study from Busselton, Western Australia. Annals of epidemiology, 16, 206–212. 10.1016/j.annepidem.2005.03.010 [DOI] [PubMed] [Google Scholar]
- Roswall, N. , Larsen, S. B. , Friis, S. , Outzen, M. , Olsen, A. , Christensen, J. , Dragsted, L. O. , & Tjonneland, A. (2013). Micronutrient intake and risk of prostate cancer in a cohort of middle‐aged, Danish men. Cancer Causes & Control, 24, 1129–1135. 10.1007/s10552-013-0190-4 [DOI] [PubMed] [Google Scholar]
- Roswall, N. , Olsen, A. , Christensen, J. , Dragsted, L. O. , Overvad, K. , & Tjonneland, A. (2010). Micronutrient intake and risk of colon and rectal cancer in a Danish cohort. Cancer Epidemiology, 34, 40–46. 10.1016/j.canep.2009.12.012 [DOI] [PubMed] [Google Scholar]
- Roy, A. , Kocak, M. , Hartman, T. J. , Vereen, S. , Adgent, M. , Piyathilake, C. , Tylavsky, F. A. , & Carroll, K. N. (2018). Association of prenatal folate status with early childhood wheeze and atopic dermatitis. Pediatric Allergy and Immunology, 29, 144–150. 10.1111/pai.12834 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell, R. M. , Golner, B. B. , Krasinski, S. D. , Sadowski, J. A. , Suter, P. M. , & Braun, C. L. (1988). Effect of antacid and H2 receptor antagonists on the intestinal absorption of folic acid. Journal of Laboratory and Clinical Medicine, 112, 458–463. [PubMed] [Google Scholar]
- Russell, R. M. , Krasinski, S. D. , Samloff, I. M. , Jacob, R. A. , Hartz, S. C. , & Brovender, S. R. (1986). Folic acid malabsorption in atrophic gastritis. Possible compensation by bacterial folate synthesis. Gastroenterology, 91, 1476–1482. 10.1016/0016-5085(86)90204-0 [DOI] [PubMed] [Google Scholar]
- SACN (Scientific Advisory Committee on Nutrition) . (2006). Folate and Disease Prevention. TSO. [Google Scholar]
- SACN (Scientific Advisory Committee on Nutrition) . (2009). Folic acid and colorectal cancer risk: Review of recommendation for mandatory folic acid fortification.
- SACN (Scientific Advisory Committee on Nutrition) . (2017). Update on folic acid.
- Savage, D. G. , & Lindenbaum, J. (1995). Folate‐cobalamin interactions. In Bailey L. (Ed.), Folate in health and disease (pp. 237–285). M. Dekker. [Google Scholar]
- Sawaengsri, H. , Wang, J. P. , Reginaldo, C. , Steluti, J. , Wu, D. Y. , Meydani, S. N. , Seihub, J. , & Paul, L. (2016). High folic acid intake reduces natural killer cell cytotoxicity in aged mice. Journal of Nutritional Biochemistry, 30, 102–107. 10.1016/j.jnutbio.2015.12.006 [DOI] [PubMed] [Google Scholar]
- Scaranti, M. , Cojocaru, E. , Banerjee, S. , & Banerji, U. (2020). Exploiting the folate receptor α in oncology. Nature Reviews. Clinical Oncology, 17, 349–359. 10.1038/s41571-020-0339-5 [DOI] [PubMed] [Google Scholar]
- SCF (Scientific Committee on Food) . (2000). Opinion of the Scientific Committee on Food on the Tolerable Upper Intake Level of vitamin B6, 15. [Google Scholar]
- Schernhammer, E. , Wolpin, B. , Rifai, N. , Cochrane, B. , Manson, J. A. , Ma, J. , Giovannucci, E. , Thomson, C. , Stampfer, M. J. , & Fuchs, C. (2007). Plasma folate, vitamin B6, vitamin B12, and homocysteine and pancreatic cancer risk in four large cohorts. Cancer Research, 67, 5553–5560. 10.1158/0008-5472.Can-06-4463 [DOI] [PubMed] [Google Scholar]
- Schmidt, R. J. , Iosif, A. M. , Guerrero Angel, E. , & Ozonoff, S. (2019). Association of maternal prenatal vitamin use with risk for autism spectrum disorder recurrence in young siblings. JAMA Psychiatry, 76, 391–398. 10.1001/jamapsychiatry.2018.3901 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz, S. O. , Kaplan, S. R. , & Amstrong, B. E. (1950). The long‐term evaluation of folic acid in the treatment of pernicious anemia. The Journal of Laboratory and Clinical Medecine, 35, 894–898. [PubMed] [Google Scholar]
- Scott, J. M. , & Weir, D. G. (1986). Nutritional, Pharmacological and Physiological Aspects. In Blakley R. L. & Whitehead V. M. (Eds.), Folates and Pterins: Volume 3. New York. [Google Scholar]
- Scott, J. M. , Wilson, P. , Dinn, J. J. , & Weir, D. G. (1981). Pathogenesis of subacute combined degeneration: A result of methyl group deficiency. The Lancet, 318, 334–337. 10.1016/S0140-6736(81)90649-8 [DOI] [PubMed] [Google Scholar]
- Selhub, J. , Miller, J. W. , Troen, A. M. , Mason, J. B. , & Jacques, P. F. (2022). Perspective: the high‐folate‐low‐vitamin B‐12 interaction is a novel cause of vitamin B‐12 depletion with a specific etiology‐A hypothesis. Advances in Nutrition, 13, 16–33. 10.1093/advances/nmab106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shane, B. , Pangilinan, F. , Mills, J. L. , Fan, R. , Gong, T. , Cropp, C. D. , Kim, Y. , Ueland, P. M. , Bailey‐Wilson, J. E. , Wilson, A. F. , Brody, L. C. , & Molloy, A. M. (2018). The 677C→T variant of MTHFR is the major genetic modifier of biomarkers of folate status in a young, healthy Irish population. The American Journal of Clinical Nutrition, 108, 1334–1341. 10.1093/ajcn/nqy209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shia, J. , Klimstra, D. S. , Nitzkorski, J. R. , Low, P. S. , Gonen, M. , Landmann, R. , Weiser, M. R. , Franklin, W. A. , Prendergast, F. G. , Murphy, L. , Tang, L. H. , Temple, L. , Guillem, J. G. , Wong, W. D. , & Paty, P. B. (2008). Immunohistochemical expression of folate receptor alpha in colorectal carcinoma: Patterns and biological significance. Human Pathology, 39, 498–505. 10.1016/j.humpath.2007.09.013 [DOI] [PubMed] [Google Scholar]
- Shojania, A. , & Hornady, G. (1970a). Folate metabolism in newborns and during early infancy: I. Absorption of pteroylglutamic (folic) acid in newborns. Pediatric Research, 4, 412–421. 10.1203/00006450-197009000-00004 [DOI] [PubMed] [Google Scholar]
- Shojania, A. , & Hornady, G. (1970b). Folate metabolism in newborns and during early infancy: II. Clearance of folic acid in plasma and excretion of folic acid in urine by newborns. Pediatric Research, 4, 422–426. 10.1203/00006450-197009000-00005 [DOI] [PubMed] [Google Scholar]
- Shrubsole, M. J. , Yang, G. , Gao, Y. T. , Chow, W. H. , Shu, X. O. , Cai, Q. , Rothman, N. , Gao, J. , Wagner, C. , & Zheng, W. (2009). Dietary B vitamin and methionine intakes and plasma folate are not associated with colorectal cancer risk in Chinese women. Cancer epidemiology, biomarkers & prevention, 18, 1003–1006. 10.1158/1055-9965.EPI-08-1200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silaste, M. L. , Rantala, M. , Alfthan, G. , Aro, A. , & Kesäniemi, Y. A. (2003). Plasma homocysteine concentration is decreased by dietary intervention. The British Journal of Nutrition, 89, 295–301. 10.1079/bjn2002776 [DOI] [PubMed] [Google Scholar]
- Sinclair, K. D. , Allegrucci, C. , Singh, R. , Gardner, D. S. , Sebastian, S. , Bispham, J. , Thurston, A. , Huntley, J. F. , Rees, W. D. , Maloney, C. A. , Lea, R. G. , Craigon, J. , McEvoy, T. G. , & Young, L. E. (2007). DNA methylation, insulin resistance, and blood pressure in offspring determined by maternal periconceptional B vitamin and methionine status. Proceedings of the National Academy of Sciences of the United States of America, 104, 19351–19356. 10.1073/pnas.0707258104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smidt, L. J. , Cremin, F. M. , Grivetti, L. E. , & Clifford, A. J. (1990). Influence of folate status and polyphenol intake on thiamin status of Irish women. The American Journal of Clinical Nutrition, 52, 1077–1082. 10.1093/ajcn/52.6.1077 [DOI] [PubMed] [Google Scholar]
- Smith, A. M. , Picciano, M. F. , & Deering, R. H. (1985). Folate intake and blood concentrations of term infants. American Journal of Clinical Nutrition, 41, 590–598. 10.1093/ajcn/41.3.590 [DOI] [PubMed] [Google Scholar]
- Smulders, Y. M. , Smith, D. E. , Kok, R. M. , Teerlink, T. , Swinkels, D. W. , Stehouwer, C. D. , & Jakobs, C. (2006). Cellular folate vitamer distribution during and after correction of vitamin B12 deficiency: A case for the methylfolate trap. British Journal of Haematology, 132, 623–629. 10.1111/j.1365-2141.2005.05913.x [DOI] [PubMed] [Google Scholar]
- Song, J. , Medline, A. , Mason, J. B. , Gallinger, S. , & Kim, Y. I. (2000). Effects of dietary folate on intestinal tumorigenesis in the apcMin mouse. Cancer Research, 60, 5434–5440. [PubMed] [Google Scholar]
- Spies, T. D. , & Stone, R. E. (1947). Liver extract, folic acid, and thymine in pernicious anaemia and subacute combined degeneration. Lancet, 1, 174–176. 10.1016/s0140-6736(47)91137-9 [DOI] [PubMed] [Google Scholar]
- Spies, T. D. , Stone, R. E. , Lopez, G. G. , Milanes, F. , Aramburu, T. , & Toca, R. L. (1948). The association between gastric achlorhydria and subacute combined degeneration of the spinal cord. Postgraduate Medicine, 4, 89–95. 10.1080/00325481.1948.11693668 [DOI] [PubMed] [Google Scholar]
- Stanisławska‐Sachadyn, A. , Brown, K. S. , Mitchell, L. E. , Woodside, J. V. , Young, I. S. , Scott, J. M. , Murray, L. , Boreham, C. A. , McNulty, H. , Strain, J. J. , & Whitehead, A. S. (2008). An insertion/deletion polymorphism of the dihydrofolate reductase (DHFR) gene is associated with serum and red blood cell folate concentrations in women. Hum Genet, 123, 289–295. 10.1007/s00439-008-0475-y [DOI] [PubMed] [Google Scholar]
- Steinberg, S. E. , Campbell, C. L. , & Hillman, R. S. (1979). Kinetics of the normal folate enterohepatic cycle. The Journal of clinical investigation, 64, 83–88. 10.1172/jci109467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevens, V. L. , McCullough, M. L. , Sun, J. , Jacobs, E. J. , Campbell, P. T. , & Gapstur, S. M. (2011). High levels of folate from supplements and fortification are not associated with increased risk of colorectal cancer. Gastroenterology, 141, 98–105. 10.1053/j.gastro.2011.04.004 [DOI] [PubMed] [Google Scholar]
- Stevens, V. L. , Rodriguez, C. , Pavluck, A. L. , McCullough, M. L. , Thun, M. J. , & Calle, E. E. (2006). Folate nutrition and prostate cancer incidence in a large cohort of US men. American Journal of Epidemiology, 163, 989–996. 10.1093/aje/kwj126 [DOI] [PubMed] [Google Scholar]
- Stewart, C. P. , Christian, P. , Schulze, K. J. , Arguello, M. , LeClerq, S. C. , Khatry, S. K. , & West, K. P., Jr. (2011). Low maternal vitamin B‐12 status is associated with offspring insulin resistance regardless of antenatal micronutrient supplementation in rural Nepal. Journal of Nutrition, 141, 1912–1917. 10.3945/jn.111.144717 [DOI] [PubMed] [Google Scholar]
- Stewart, C. P. , Christian, P. , Schulze, K. J. , Leclerq, S. C. , West, K. P., Jr. , & Khatry, S. K. (2009). Antenatal micronutrient supplementation reduces metabolic syndrome in 6‐ to 8‐year‐old children in rural Nepal. Journal of Nutrition, 139, 1575–1581. 10.3945/jn.109.106666 [DOI] [PubMed] [Google Scholar]
- Stos, K. , Wozniak, A. , Rychlik, E. , Ziolkowska, I. , Glowala, A. , & Oltarzewski, M. (2021). Assessment of food supplement consumption in Polish population of adults. Frontiers in Nutrition, 8. 10.3389/fnut.2021.733951 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stover, P. J. (2011). Polymorphisms in 1‐carbon metabolism, epigenetics and folate‐related pathologies. Journal of Nutrigenetics and Nutrigenomics, 4, 293–305. 10.1159/000334586 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strøm, M. , Granström, C. , Lyall, K. , Ascherio, A. , & Olsen, S. F. (2018). Research Letter: Folic acid supplementation and intake of folate in pregnancy in relation to offspring risk of autism spectrum disorder. Psychological Medicine, 48, 1048–1054. 10.1017/s0033291717002410 [DOI] [PubMed] [Google Scholar]
- Su, Y. , Mao, Y. , Tian, F. , Cai, X. , Chen, R. , Li, N. , Qian, C. , Li, X. , Zhao, Y. , & Wang, Y. (2022). Profile of folate in breast milk from chinese women over 1‐400 days postpartum. Nutrients, 14. 10.3390/nu14142962 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun, Y. , Shao, T. , Yao, Y. , Tao, H. , Ni, L. , Yan, S. , Gu, C. , Cao, H. , Huang, K. , & Tao, F. (2016). Pregnancy‐related anxiety and subthreshold autism trait in preschool children based a birth cohort study. Zhonghua Yu Fang Yi Xue Za Zhi, 50, 118–122. 10.3760/cma.j.issn.0253-9624.2016.02.004 [DOI] [PubMed] [Google Scholar]
- Surén, P. , Roth, C. , Bresnahan, M. , Haugen, M. , Hornig, M. , Hirtz, D. , Lie, K. K. , Lipkin, W. I. , Magnus, P. , Reichborn‐Kjennerud, T. , Schjølberg, S. , Davey Smith, G. , Øyen, A. S. , Susser, E. , & Stoltenberg, C. (2013). Association between maternal use of folic acid supplements and risk of autism spectrum disorders in children. JAMA, 309, 570–577. 10.1001/jama.2012.155925 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Surtees, R. , & Hyland, K. (1990). Cerebrospinal fluid concentrations of S‐adenosylmethionine, methionine, and 5‐methyltetrahydrofolate in a reference population: Cerebrospinal fluid S‐adenosylmethionine declines with age in humans. Biochem Med Metab Biol, 44, 192–199. 10.1016/0885-4505(90)90060-e [DOI] [PubMed] [Google Scholar]
- Sweeney, M. R. , McPartlin, J. , Weir, D. G. , Daly, L. , & Scott, J. M. (2006). Postprandial serum folic acid response to multiple doses of folic acid in fortified bread. British Journal of Nutrition, 95, 145–151. 10.1079/bjn20051618 [DOI] [PubMed] [Google Scholar]
- Sweeney, M. R. , McPartlin, J. , Weir, D. G. , & Scott, J. M. (2003). Measurements of sub‐nanomolar concentrations of unmetabolised folic acid in serum. Journal of Chromatography B, Analytical Technologies in the Biomedical and Life Sciences, 788, 187–191. 10.1016/s1570-0232(02)01010-3 [DOI] [PubMed] [Google Scholar]
- Takata, Y. , Shrubsole, M. J. , Li, H. , Cai, Q. , Gao, J. , Wagner, C. , Wu, J. , Zheng, W. , Xiang, Y. B. , & Shu, X. O. (2014). Plasma folate concentrations and colorectal cancer risk: A case‐control study nested within the Shanghai Men's Health Study. International Journal of Cancer, 135, 2191–2198. 10.1002/ijc.28871 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teppers, E. , & Ost, C. (WIV‐ISP). (2016). Acide folique. Enquête de Consommation Alimentaire, 2014–2015, 4. [Google Scholar]
- Tomaszewski, J. J. , Richman, E. L. , Sadetsky, N. , O'Keefe, D. S. , Carroll, P. R. , Davies, B. J. , & Chan, J. M. (2014). Impact of folate intake on prostate cancer recurrence following definitive therapy: Data from CaPSURE™. The Journal of urology, 191, 971–976. 10.1016/j.juro.2013.09.065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Totland, T. H. , Melnæs, B. K. , Lundberg‐Hallén, N. , Helland‐Kigen, K. M. , Lund‐Blix, N. A. , Myhre, J. B. , Wetting Johansen, A. M. , Løken, E. B. , & Andersen, L. F. (Universitetet i Oslo, Mattilsynet og Helsedirektoratet). (2012). Norkost 3 En landsomfattende kostholdsundersøkelse blant menn og kvinner i Norge i alderen 18–70 år, 2010–11. Oslo, Norway .
- Triche, E. W. , Lundsberg, L. S. , Wickner, P. G. , Belanger, K. , Leaderer, B. P. , & Bracken, M. B. (2011). Association of maternal anemia with increased wheeze and asthma in children. Annals of Allergy, Asthma & Immunology, 106, 131–139.e131. 10.1016/j.anai.2010.11.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trivedi, M. K. , Sharma, S. , Rifas‐Shiman, S. L. , Camargo, C. A., Jr. , Weiss, S. T. , Oken, E. , Gillman, M. W. , Gold, D. R. , DeMeo, D. L. , & Litonjua, A. A. (2018). Folic acid in pregnancy and childhood asthma: A US Cohort. Clinical Pediatrics, 57, 421–427. 10.1177/0009922817729482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Troen, A. M. , Mitchell, B. , Sorensen, B. , Wener, M. H. , Johnston, A. , Wood, B. , Selhub, J. , McTiernan, A. , Yasui, Y. , Oral, E. , Potter, J. D. , & Ulrich, C. M. (2006). Unmetabolized folic acid in plasma is associated with reduced natural killer cell cytotoxicity among postmenopausal women. Journal of Nutrition, 136, 189–194. 10.1093/jn/136.1.189 [DOI] [PubMed] [Google Scholar]
- Tsilidis, K. K. , Papadimitriou, N. , Dimou, N. , Gill, D. , Lewis, S. J. , Martin, R. M. , Murphy, N. , Markozannes, G. , Zuber, V. , Cross, A. J. , Burrows, K. , Lopez, D. S. , Key, T. J. , Travis, R. C. , Perez‐Cornago, A. , Hunter, D. J. , van Duijnhoven, F. J. B. , Albanes, D. , Arndt, V. , … Gunter, M. J. (2021). Genetically predicted circulating concentrations of micronutrients and risk of colorectal cancer among individuals of European descent: A Mendelian randomization study. The American Journal of Clinical Nutrition, 113, 1490–1502. 10.1093/ajcn/nqab003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uccella, S. , Mariani, A. , Wang, A. H. , Vierkant, R. A. , Robien, K. , Anderson, K. E. , & Cerhan, J. R. (2011). Dietary and supplemental intake of one‐carbon nutrients and the risk of type I and type II endometrial cancer: A prospective cohort study. Annals of Oncology, 22, 2129–2136. 10.1093/annonc/mdq724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- VKM (Norwegian Scientific Committee for Food Safety , Haugen, M. , Frølich, W. , Strand, T. A. , & Tell, G. S. (2015). Risk assessment of folic acid in food supplements. Scientific opinion of the Panel on Nutrition, Dietetic Products, Novel Food and Allergy.
- Valsta, L. , Kaartinen, N. , Tapanainen, H. , Männistö, S. , Sääksjärvi, K. , & National Institute for Health and Welfare . (2018). Nutrition in Finland: The National FinDiet 2017 Survey.
- van Dam, R. M. , Huang, Z. , Giovannucci, E. , Rimm, E. B. , Hunter, D. J. , Colditz, G. A. , Stampfer, M. J. , & Willett, W. C. (2000). Diet and basal cell carcinoma of the skin in a prospective cohort of men. he American journal of clinical nutrition, 71, 135–141. 10.1093/ajcn/71.1.135 [DOI] [PubMed] [Google Scholar]
- Van der Westhuyzen, J. , Fernandes‐Costa, F. , & Metz, J. (1982). Cobalamin inactivation by nitrous‐oxide produces severe neurological impairment in fruit bats ‐ protection by methionine and aggravation by folates. Life Sciences, 31, 2001–2010. 10.1016/0024-3205(82)90039-x [DOI] [PubMed] [Google Scholar]
- van der Westhuyzen, J. , & Metz, J. (1983). Tissue S‐adenosylmethionine levels in fruit bats (Rousettus aegyptiacus) with nitrous oxide‐induced neuropathy. British Journal of Nutrition, 50, 325–330. 10.1079/BJN19830100 [DOI] [PubMed] [Google Scholar]
- van Gool, J. D. , Hirche, H. , Lax, H. , & Schaepdrijver, L. (2020). Fallacies of clinical studies on folic acid hazards in subjects with a low vitamin B(12) status. Critical reviews in toxicology, 50, 177–187. 10.1080/10408444.2020.1727842 [DOI] [PubMed] [Google Scholar]
- Van Guelpen, B. , Hultdin, J. , Johansson, I. , Hallmans, G. , Stenling, R. , Riboli, E. , Winkvist, A. , & Palmqvist, R. (2006). Low folate levels may protect against colorectal cancer. Gut, 55, 1461–1466. 10.1136/gut.2005.085480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Rossum, C. T. M. , Buurma‐Rethans, E. J. M. , Dinnissen, C. S. , Beukers, M. H. , Brants, H. A. M. , Dekkers, A. L. M. , & Ocké MC (National Institute for Public Health and the Environment) . (2022). Intake and frequency of use of dietary supplements in the Netherlands. The diet of the Dutch. Results of the Dutch National Food Consumption Survey 2012–2016. Bilthoven, RIVM.
- Veeranki, S. P. , Gebretsadik, T. , Mitchel, E. F. , Tylavsky, F. A. , Hartert, T. V. , Cooper, W. O. , Dupont, W. D. , Dorris, S. L. , Hartman, T. J. , & Carroll, K. N. (2015). Maternal folic acid supplementation during pregnancy and early childhood asthma. Epidemiology, 26, 934–941. 10.1097/ede.0000000000000380 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Venn, B. J. , Mann, J. I. , Williams, S. M. , Riddell, L. J. , Chisholm, A. , Harper, M. J. , & Aitken, W. (2002). Dietary counseling to increase natural folate intake: A randomized, placebo‐controlled trial in free‐living subjects to assess effects on serum folate and plasma total homocysteine. The American Journal of Clinical Nutrition, 76, 758–765. 10.1093/ajcn/76.4.758 [DOI] [PubMed] [Google Scholar]
- Venn, B. J. , Mann, J. I. , Williams, S. M. , Riddell, L. J. , Chisholm, A. , Harper, M. J. , Aitken, W. , & Rossaak, J. I. (2002). Assessment of three levels of folic acid on serum folate and plasma homocysteine: A randomised placebo‐controlled double‐blind dietary intervention trial. European Journal of Clinical Nutrition, 56, 748–754. 10.1038/sj.ejcn.1601388 [DOI] [PubMed] [Google Scholar]
- Victor, M. , & Lear, A. A. (1956). Subacute combined degeneration of the spinal cord; current concepts of the disease process; value of serum vitamin B12; determinations in clarifying some of the common clinical problems. Am J Med, 20, 896–911. 10.1016/0002-9343(56)90210-8 [DOI] [PubMed] [Google Scholar]
- Vilter, C. F. , Vilter, R. W. , & Spies, T. D. (1947). The treatment of pernicious and related anemias with synthetic folic acid; observations on the maintenance of a normal hematologic status and on the occurrence of combined system disease at the end of one year. The Journal of Laboratory and Clinical Medicine, 32, 262–273. [PubMed] [Google Scholar]
- Virk, J. , Liew, Z. , Olsen, J. , Nohr, E. A. , Catov, J. M. , & Ritz, B. (2016). Preconceptional and prenatal supplementary folic acid and multivitamin intake and autism spectrum disorders. Autism: The International Journal of Research and Practice, 20, 710–718. 10.1177/1362361315604076 [DOI] [PubMed] [Google Scholar]
- Vollset, S. E. , Clarke, R. , Lewington, S. , Ebbing, M. , Halsey, J. , Lonn, E. , Armitage, J. , Manson, J. E. , Hankey, G. J. , Spence, J. D. , Galan, P. , Bonaa, K. H. , Jamison, R. , Gaziano, J. M. , Guarino, P. , Baron, J. A. , Logan, R. F. A. , Giovannucci, E. L. , den Heijer, M. , … Co, B. V. T. T. (2013). Effects of folic acid supplementation on overall and site‐specific cancer incidence during the randomised trials: Meta‐analyses of data on 50 000 individuals. Lancet, 381, 1029–1036. 10.1016/s0140-6736(12)62001-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wagley, P. F. (1947). Neurologic disturbances with folic acid therapy. N Engl J Med, 238, 11–15. 10.1056/nejm194801012380103 [DOI] [PubMed] [Google Scholar]
- Wang, F. L. , Wu, K. N. , Li, Y. P. , Song, R. , Wu, Y. , Zhang, X. H. , Song, M. Y. , Liang, L. M. , Smith‐Warner, S. A. , Giovannucci, E. L. , & Willett, W. C. (2021). Association of folate intake and colorectal cancer risk in the postfortification era in US women. American Journal of Clinical Nutrition, 114, 49–58. 10.1093/ajcn/nqab035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, H. X. , Wahlin, A. , Basun, H. , Fastbom, J. , Winblad, B. , & Fratiglioni, L. (2001). Vitamin B(12) and folate in relation to the development of Alzheimer's disease. Neurology, 56, 1188–1194. 10.1212/wnl.56.9.1188 [DOI] [PubMed] [Google Scholar]
- Wang, K. N. , Zhang, Q. W. , & Yang, J. H. (2021). The effect of folate intake on ovarian cancer risk A meta‐analysis of observational studies. Medicine, 100, e22605. 10.1097/md.0000000000022605 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wargovich, M. J. , Chen, C. D. , Jimenez, A. , Steele, V. E. , Velasco, M. , Stephens, L. C. , Price, R. , Gray, K. , & Kelloff, G. J. (1996). Aberrant crypts as a biomarker for colon cancer: Evaluation of potential chemopreventive agents in the rat. Cancer epidemiology, biomarkers & prevention, 5, 355–360. [PubMed] [Google Scholar]
- Weinstein, S. J. , Albanes, D. , Selhub, J. , Graubard, B. , Lim, U. , Taylor, P. R. , Virtamo, J. , & Stolzenberg‐Solomon, R. (2008). One‐carbon metabolism biomarkers and risk of colon and rectal cancers. Cancer epidemiology, biomarkers & prevention, 17, 3233–3240. 10.1158/1055-9965.EPI-08-0459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weinstein, S. J. , Hartman, T. J. , Stolzenberg‐Solomon, R. , Pietinen, P. , Barrett, M. J. , Taylor, P. R. , Virtamo, J. , & Albanes, D. (2003). Null association between prostate cancer and serum folate, vitamin B(6), vitamin B(12), and homocysteine. Cancer epidemiology, biomarkers & prevention, 12, 1271–1272. [PubMed] [Google Scholar]
- Weinstein, S. J. , Stolzenberg‐Solomon, R. , Pietinen, P. , Taylor, P. R. , Virtamo, J. , & Albanes, D. (2006). Dietary factors of one‐carbon metabolism and prostate cancer risk. The American Journal of Clinical Nutrition, 84, 929–935. 10.1093/ajcn/84.4.929 [DOI] [PubMed] [Google Scholar]
- Whitrow, M. J. , Moore, V. M. , Rumbold, A. R. , & Davies, M. J. (2009). Effect of supplemental folic acid in pregnancy on childhood asthma: a prospective birth cohort study. American Journal of Epidemiology, 170, 1486–1493. 10.1093/aje/kwp315 [DOI] [PubMed] [Google Scholar]
- WHO (World Health Organization) . (2000). In Hamilton S. & Aaltonen L. (Eds.), Pathology and genetics of tumours of the digestive system (3rd ed.). IARC. [Google Scholar]
- WHO Multicentre Growth Reference Study Group . (2006). WHO Child Growth Standards based on length/height, weight and age. Acta Paediatrica, 450(Suppl), 76–85. 10.1111/j.1651-2227.2006.tb02378.x [DOI] [PubMed] [Google Scholar]
- WHO (World Health Organization) . (2010). In Bosman F., Carneiro F., Hruban R., & Theise N. (Eds.), Classification of tumours of the digestive system (4th ed.). IARC. [Google Scholar]
- WHO (World Health Organization) . (2019). Digestive system tumours. In WHO classification of tumours editorial board (5th ed.). IARC. [Google Scholar]
- Wien, T. N. , Pike, E. , Wisloff, T. , Staff A , Smeland, S. , & Klemp, M. (2012). Cancer risk with folic acid supplements: A systematic review and meta‐analysis. Bmj Open, 2, e000653. 10.1136/bmjopen-2011-000653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilkinson, J. F. (1948). Folic acid. British Medical Journal, 1, 822–827. 10.1136/bmj.1.4556.822 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Will, J. J. , Mueller, J. F. , Brodine, C. , Kiely, C. E. , Friedman, B. , Hawkins, V. R. , Dutra, J. , & Vilter, R. W. (1959). Folic acid and vitamin B12 in pernicious anemia; studies on patients treated with these substances over a ten year period. Journal of Laboratory and Clinical Medicine, 53, 22–38. [PubMed] [Google Scholar]
- Winkels, R. M. , Brouwer, I. A. , Siebelink, E. , Katan, M. B. , & Verhoef, P. (2007). Bioavailability of food folates is 80% of that of folic acid. American Journal of Clinical Nutrition, 85, 465–473. 10.1093/ajcn/85.2.465 [DOI] [PubMed] [Google Scholar]
- Winkels, R. M. , Brouwer, I. A. , Verhoef, P. , van Oort, F. V. , Durga, J. , & Katan, M. B. (2008). Gender and body size affect the response of erythrocyte folate to folic acid treatment. Journal of Nutrition, 138, 1456–1461. 10.1093/jn/138.8.1456 [DOI] [PubMed] [Google Scholar]
- Winstock, A. R. , & Ferris, J. A. (2020). Nitrous oxide causes peripheral neuropathy in a dose dependent manner among recreational users. Journal of Psychopharmacology, 34, 229–236. 10.1177/0269881119882532 [DOI] [PubMed] [Google Scholar]
- Wolters, M. , Hermann, S. , & Hahn, A. (2005). Effect of multivitamin supplementation on the homocysteine and methylmalonic acid blood concentrations in women over the age of 60 years. European Journal of Nutrition, 44, 183–192. 10.1007/s00394-004-0510-2 [DOI] [PubMed] [Google Scholar]
- Wright, A. J. , Finglas, P. M. , Dainty, J. R. , Wolfe, C. A. , Hart, D. J. , Wright, D. M. , & Gregory, J. F. (2005). Differential kinetic behavior and distribution for pteroylglutamic acid and reduced folates: A revised hypothesis of the primary site of PteGlu metabolism in humans. Journal of Nutrition, 135, 619–623. [DOI] [PubMed] [Google Scholar]
- Wu, K. , Platz, E. A. , Willett, W. C. , Fuchs, C. S. , Selhub, J. , Rosner, B. A. , Hunter, D. J. , & Giovannucci, E. (2009). A randomized trial on folic acid supplementation and risk of recurrent colorectal adenoma. The American Journal of Clinical Nutrition, 90, 1623–1631. 10.3945/ajcn.2009.28319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xie, R. H. , Liu, Y. J. , Retnakaran, R. , MacFarlane, A. J. , Hamilton, J. , Smith, G. , Walker, M. C. , & Wen, S. W. (2016). Maternal folate status and obesity/insulin resistance in the offspring: A systematic review. International Journal of Obesity, 40, 1–9. 10.1038/ijo.2015.189 [DOI] [PubMed] [Google Scholar]
- Yajnik, C. S. , Deshpande, S. S. , Jackson, A. A. , Refsum, H. , Rao, S. , Fisher, D. J. , Bhat, D. S. , Naik, S. S. , Coyaji, K. J. , Joglekar, C. V. , Joshi, N. , Lubree, H. G. , Deshpande, V. U. , Rege, S. S. , & Fall, C. H. (2008). Vitamin B12 and folate concentrations during pregnancy and insulin resistance in the offspring: The Pune Maternal Nutrition Study. Diabetologia, 51, 29–38. 10.1007/s00125-007-0793-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yuan, S. , Carter, P. , Vithayathil, M. , Kar, S. , Mason, A. M. , Burgess, S. , & Larsson, S. C. (2021). Genetically predicted circulating B vitamins in relation to digestive system cancers. British Journal of Cancer, 124, 1997–2003. 10.1038/s41416-021-01383-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zetstra‐van der Woude, P. A. , De Walle, H. E. , Hoek, A. , Bos, H. J. , Boezen, H. M. , Koppelman, G. H. , De Jong‐Van Den Berg, L. T. , & Scholtens, S. (2014). Maternal high‐dose folic acid during pregnancy and asthma medication in the offspring. Pharmacoepidemiology and Drug Safety, 23, 1059–1065. 10.1002/pds.3652 [DOI] [PubMed] [Google Scholar]
- Zhang, S. M. , Moore, S. C. , Lin, J. , Cook, N. R. , Manson, J. E. , Lee, I. M. , & Buring, J. E. (2006). Folate, vitamin B6, multivitamin supplements, and colorectal cancer risk in women. American Journal of Epidemiology, 163, 108–115. 10.1093/aje/kwj016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, Y. F. , Zhou, L. , Zhang, H. W. , Hou, A. J. , Gao, H. F. , & Zhou, Y. H. (2014). Association between folate intake and the risk of lung cancer: A dose‐response meta‐analysis of prospective studies. Plos One, 9, e93465. 10.1371/journal.pone.0093465 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao, R. , Diop‐Bove, N. , Visentin, M. , & Goldman, I. D. (2010). Mechanisms of membrane transport of folates into cells and across epithelia. Annual Review of Nutrition, 31, 177–201. 10.1146/annurev-nutr-072610-145133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao, Y. , Guo, C. , Hu, H. , Zheng, L. , Ma, J. , Jiang, L. , Zhao, E. , & Li, H. (2017). Folate intake, serum folate levels and esophageal cancer risk: An overall and dose‐response meta‐analysis. Oncotarget, 8, 10458–10469. 10.18632/oncotarget.14432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zheng, Y. , & Cantley, L. C. (2019). Toward a better understanding of folate metabolism in health and disease. Journal of Experimental Medicine, 216, 253–266. 10.1084/jem.20181965 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zschäbitz, S. , Cheng, T. Y. , Neuhouser, M. L. , Zheng, Y. , Ray, R. M. , Miller, J. W. , Song, X. , Maneval, D. R. , Beresford, S. A. , Lane, D. , Shikany, J. M. , & Ulrich, C. M. (2013). B vitamin intakes and incidence of colorectal cancer: Results from the Women's Health Initiative Observational Study cohort. American Journal of Clinical Nutrition, 97, 332–343. 10.3945/ajcn.112.034736 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Protocol for the Scientific Opinion on the revision of the EFSA's tolerable upper intake level of folate
Methodological considerations in the calculation of intake estimates for total folate in European countries
EFSA's intake assessment of folate
Folate intake data from Competent Authorities in European countries
Public consultation on the draft scientific opinion on the tolerable upper intake level for folate