

Abstract
INTRODUCTION
The aim of this study was to establish the quality of patient-facing websites advertising low-intensity shockwave therapy (LISWT) for erectile dysfunction (ED) and Peyronie’s disease (PD) patients in Canada.
METHODS
Canadian websites offering LIWST for ED or PD were identified using online web searches. The characteristics of these websites were reviewed, along with examining the presence of HONCode certification, assigning a brief DISCERN score (a tool designed to evaluate health information online) and readability scores. We also examined the LIWST technology advertised, as well as benefits of LIWST cited by the websites.
RESULTS
Twenty-five unique websites linked to 46 clinics were identified and reviewed. Twenty-four percent of websites were run by a urologist. Other specialties offering LISWT included general practitioners, anesthesiologists, naturopaths, nurse practitioners, physiotherapists, and registered massage therapists. Twenty-four percent of the websites advertised the use of a focused shockwave generator. Forty percent of the websites had peer-reviewed references. The average brief DISCERN score was 14 (standard deviation 3.4). There was no association between the physician-or non-physician-led websites and the use of peer-reviewed references, readability scores, the number of clinic locations, or higher brief discern scores.
CONCLUSIONS
LISWT is readily advertised online for ED and PD patients in Canada; however, only a minority use a focused shockwave generator. There is a wide diversity of practitioners offering LISWT. Websites offering LISWT are generally of poor quality and do not provide adequate information for patients to make educated treatment decisions.
INTRODUCTION
Low-intensity shockwave therapy (LISWT) was first used in the treatment of musculoskeletal diseases and chronic wounds.1,2 Tissue that was treated with LISWT showed evidence of neovascularization and enhancement of local blood flow.3 Conceptually, LISWT has been an attractive idea in the treatment of erectile dysfunction (ED), and to a lesser degree Peyronie’s disease (PD), as these conditions are related to vascular insufficiency in many patients.
LISWT is now being widely used to treat ED and PD. There is hope that LISWT may reduce costs of ongoing ED treatments and reduce the need for invasive therapy for ED and PD, which include injection therapy and surgery. While the use of LISWT is conceptually attractive, there is still controversy regarding the clinical efficacy of this treatment in sexual function disorders.
Clinical trials examining the use of LISWT for ED and PD are controversial and affected by the high heterogeneity between studies in terms of patient populations, outcome measurements, and treatment protocols.4–7 The Canadian Urological Association (CUA) guidelines conditionally recommend against the use of LIWST for ED.8 In terms of PD, current data does not support the use of LISWT to reduce curvature or reduce plaque size; however, it may be an option to reduce pain.4 Most of the research to date has been done with focused shockwave generators; these were used in all of the randomized controlled studies examined in the CUA guidelines.8 There are no guideline recommendations at present to support the use of alternative generator types for LIWST, such as radial wave generators.
Despite the lack of strong evidence supporting LISWT in urologic applications, LISWT is readily available to patients in Canada from a variety of sources. The goal of this study was to review the quality of Canadian websites offering LISWT for ED and/or PD, the type of LIWST therapy offered, and to establish to what extent this technology is available to patients in Canada.
METHODS
Website identification
Websites were identified using English-language search engines using a combination of key words: “shockwave,” “ultrasound,” “erectile dysfunction,” “Peyronie’s disease,” and “Canada,” in addition to the names of provinces, territories, and urban centers in Canada. This search was performed by two independent Canadian urologists. Both searches yielded identical resulting websites for evaluation. The search engines used for this study were Google and Bing. The web search was performed in July 2020. Website results were limited to English-language sites. A total of 27 relevant websites were identified, two of which were excluded, as they advertised the same clinic.
Website quality
The brief DISCERN instrument — a shorter version of the DISCERN instrument developed in 1999 to help consumers and healthcare providers assess websites for quality of health information —was used to assess the quality of the information presented on each website regarding treatment choices.9 The instrument uses a five-point Likert scale in a total of six categories (1=criteria have not been met; 2–4=criteria have partially been met; 5=criteria have been met). Achieving a score of >16 on brief DISCERN demonstrates good quality of content.
The presence or absence of the HON code was identified on the websites. HON code was developed by the Health on the Net Foundation to evaluate the quality of health information available online.10 It is based on eight principles that a healthcare website has to fulfill, including authority, complementarity, confidentiality, attribution, justifiability, transparency, financial disclosure, and advertising.
Website readability
Readability of the websites was evaluated using the Flesch-Kincaid grade level index and the Coleman-Liau readability index. These indices assess the level of readability of a website by the general public using an assigned grade. The Flesch-Kincaid grade level index relies on the word length, total number of syllables, and sentence length.11 The Coleman-Liau readability index relies on the number of characters per word instead of syllables.12 A free, online calculator (www.readabilityformulas.com) was used to calculate the readability level of the identified websites using these two methods.
Technology use
The generator type used for LISWT therapy — focused and radial — was identified where possible using information available on the websites.
Statistical analysis
Analysis was carried out using SPSS software (SPSS Statistics version 27 for Windows, IBM corporation). Data collected from websites was analyzed using descriptive and Chi-squared statistics. A p-value of <0.05 was considered significant.
RESULTS
A total of 25 English-language websites were identified and reviewed. These websites were linked to a total of 46 clinics providing shockwave therapy treatment for ED and/or PD throughout Canada (Figure 1). Forty percent of the websites had multiple clinic locations (Table 1). Most of the clinic locations were in Ontario, followed by Quebec and British Columbia. Doctors were explicitly identified as performing the LISWT procedures on 68% of the websites identified. Urologists, specifically, were involved in 24% of the websites. Specialities involved in running the clinics and performing procedures included urologists, general practitioners, anesthesiologists, naturopaths, nurse practitioners, physiotherapists, and registered massage therapists (Figure 1).
Figure 1.
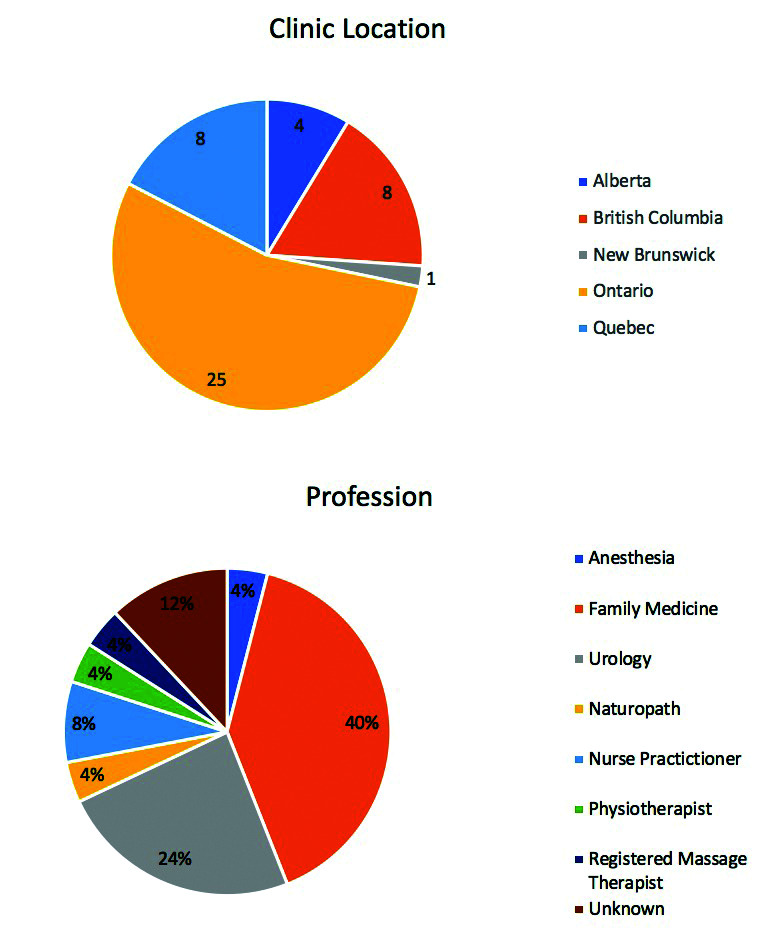
Breakdown of (A) the location of clinics/websites; and (B) the profession running them.
Table 1.
Basic characteristic of websites examined
| Website characteristics | All websites n=25 (%) |
|---|---|
| Multiple clinics | 10/25 (40%) |
| Literature references | 10/25 (40%) |
| HONcode certification | 0/25 (0%) |
| Cite a benefit of LISWT for ED | 24/25 (96%) |
| Cite a benefit of LISWT for PD | 6/25 (24%) |
| Year last updated present | 12/25 (48%) |
| Average year | Range: 2017–2020, mean: 2019 (SD 0.888) |
| Price per treatment session listed | 8/25 (32%) |
| Average price per session (CAD) | Range: 99–433, mean: 279.13 (SD 112) |
ED: erectile dysfunction; LISWT: low-intensity shockwave therapy; PD: Peyronie’s disease; SD: standard deviation.
Of the websites, 96% indicated a benefit of shockwave therapy in treating ED and 24% indicated a benefit for PD (Table 1). Only 40% of the websites had scientific literature references available. No websites had HON code certification. Eight websites had prices listed for the shockwave therapy. The average price per treatment was $279 CAD, with prices ranging from $99–433 per treatment. Additionally, only 24% of the websites were using focused shockwave generators for the treatments administered (Figure 2). The remaining websites either used radial generators (44%) or the generator type was unknown (32%).
Figure 2.
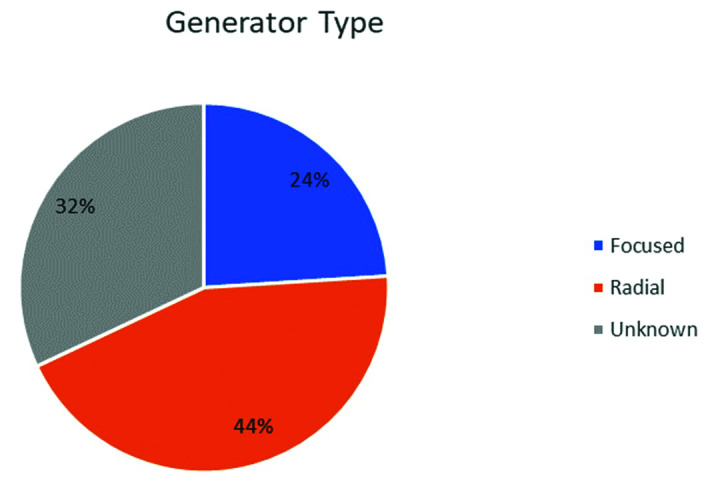
Breakdown of the shockwave generator type used by the clinics.
The average Flesch-Kincaid grade level index score was 12.04 (standard deviation [SD ] 1.7) and the average Coleman-Liau readability index score was 12.68 (SD 1.282) (Table 2). These both indicate the reading level appropriate for someone with 12th-grade education. The lowest readability level identified was a grade 9 level (Flesch-Kincaid grade level 9.2). The brief DISCERN score ranged from 7–22 for the websites, with an average value of 14 (SD 3.367) (Table 2). Only 28% of websites had a score above 16 — the level suggested by the tool to be reflective of good-quality content.
Table 2.
Brief discern, Flesch-Kincaid grade level index, and Coleman-Liau readability index scores for websites examined
| Index | Range, mean, and SD |
|---|---|
| Brief DISCERN | Range: 7–22, mean 14 (SD 3.367) |
| Flesch-Kincaid grade level index | Range: 9.2–15.7, mean 12.04 (SD 1.7) |
| Coleman-Liau readability index | Range: 10–15, mean 12.68 (SD 1.282) |
SD: standard deviation.
On Chi-squared analysis, there was no association between the presence of a physician administering the treatment and the quality of the websites as measured by any of the above metrics (Table 3). This same remained accurate when the analysis was focused on only urologists.
Table 3.
Univariate analysis for variables related to the presence of a doctor or urologist running the website
| Variable | Doctor | Urologist |
|---|---|---|
| Flesch-Kincaid grade level index >12 | 0.559 | 0.618 |
| Coleman-Liau readability index >12 | 0.906 | 0.887 |
| Brief DISCERN >16 | 0.816 | 0.789 |
| Presence of literature references on website | 0.432 | 0.629 |
| Price above average per treatment ($279 CAD) | 0.809 | 0.088 |
| Multiple clinics linked to website | 0.705 | 0.249 |
| Use of a focused shockwave generator | 0.82 | 0.655 |
DISCUSSION
LISWT has been at the forefront of research for ED and PD treatment, as it is an attractive disease-modifying therapy with the potential of avoiding costs and side effects of other modalities. The evidence behind it, however, remains controversial due to the heterogeneity of studies.4 Multiple randomized controlled trials (RCT), as well as five meta-analyses have been performed looking at the effect of LISWT from focused generators on ED outcomes.5–7,13,14 Only two of these meta-analyses exclusively included RCTs.7,13 Only one of these meta-analyses showed an overall mean difference of 2.54 in the International Index of Erectile Function (IIEF) erectile function score after treatment compared to the sham treatment group (95% confidence interval [CI] 0.83–4.25, p=0.004).7 In the Clavijo et al data, there was a trend towards a higher mean difference in IIEF erectile function scores of 4.17 (85% CI −0.5–8.3) in men treated with LISWT;13 however, this meta-analysis contains a study based on pooled data of five previously published RCTs, resulting in double inclusion of positive trials. RCTs exploring LISWT in the context of ED generally have small sample sizes.4 Furthermore, the actual net benefit in terms of IIEF erectile function scores is low (e.g., 2.54 points on a 30-point scale) and may not be clinically significant.7
When looking at LISWT treatment from focused generators in patients with PD, it has been associated with relief of pain and complete remission of pain compared to control groups in a meta-analysis of RCTs, cohort studies, and case-control studies.15 There have been no significant benefits in terms of penile curvature. There is evidence of side effects in the treatment of PD with LISWT, including cutaneous petechiae and urethral bleeding.16–18 The latest clinical guidelines from the European Society of Sexual Medicine suggest the data only support the use of LISWT for pain reduction in acute or stable PD patients, with no expectation of effect on curvature or plaque size.4 The most recent CUA guidelines regarding ED and PD do not recommend the routine use of LISWT.8,19
Given the current state of the evidence for LISWT in ED and PD patients, it is interesting to see how widely available it is as therapy for these indications. It is offered in most provinces in Canada, with a total of 46 Canadian clinics identified. LISWT comes at a cost to patients, with an average price of $279 CAD per session identified on the websites. The highest price recorded per treatment was $433. Websites offer a variety of treatment courses, with the usual courses lasting 6–12 sessions. This often translates into thousands of dollars being spent out-of-pocket for LISWT therapy. While LIST offers potential cost savings for both patients and the system, modest benefits in IIEF scores may still require the use of adjunctive therapies for adequate treatment of ED and PD.
It is also important to note that only 24% of the websites advertising shockwave therapy made use of a focused shockwave generator, compared to 44% of websites using a radial wave generator. Radial waves differ from those from a focused generator by having a lower-pressure wave with a lower peak energy and lower tissue penetrance.20 Focused shockwave devices are able to create a unique pressure wave that is directed at a focal point. Radial wave devices, however, have the maximum point of energy at the tip of the device. The waves disperse radially away from this point with rapid attenuation of the energy.21 Radial waves can penetrate up to a tissue depth of 3.5 cm, while a focused shockwave generator can target focal points up to 10–12 cm in tissue.21,22
The RCTs examined in the CUA guideline for the treatment of ED only used focused shockwave generators. 8 There is limited data at this time to support the use of radial wave generators in the treatment of ED. A retrospective comparison of focused shockwave therapy and radial wave therapy found the two modalities to be equivalent.23 Recently, however, a RCT found no difference between radial wave therapy and placebo.24 Another study showed that radial wave therapy did not improve the early recovery of ED after radical prostatectomy. 25 At the time of this publication, we identified no data to support the use of radial wave generators for the treatment of PD. Given the paucity of data to support the use of radial wave generators for LISWT treatment of ED and PD, it is concerning that 44% of the websites identified in this study advertise its use.
Only 40% of websites identified had visible scientific literature references available. When literature references are present on websites, they only include studies that support the use of LISWT. Some significant claims are present on a small number of websites that have no support in the literature, including that LISWT for ED results in an “increase in penile thickness (girth) and length.” No websites were identified to have HON code certification, and only 28% of the websites had a brief DISCERN score >16, which is felt to be a marker of good-quality content on a health website. Additionally, the average readability grade for these websites was at a grade 12 reading level, which may make it difficult for an element of the population to have a suitable understanding of the therapy offered. The recommended reading level for health information is grade 6.26
Our study demonstrated that LISWT is being offered by a variety of healthcare providers. While it is reasonable for many healthcare providers to offer treatments for ED, it becomes more problematic when providers are only offering a single treatment option for a disease with many known evidence-based treatments. This is compounded by the fact that the treatment being offered (LIWST) is experimental and more expensive than traditional treatment approaches, and that only a minority of providers are using focused generator for LIWST, which has more evidence-based data supporting its use than radial wave generators.
CONCLUSIONS
LISWT is an emerging treatment for sexual dysfunction that is widely available in Canada, with many Canadian websites promoting its use for the treatment of ED and PD at significant cost to the patient. These websites are generally of poor quality and lack the nuanced information patients would generally require to proceed with therapy. Many of the clinics providing LISWT do not advertise or provide alternative treatments for ED or PD. Additionally, a significant proportion of websites make use of radial wave generators, which have a paucity of data to support their use compared to focused shockwave generators. While the emergence of novel treatments for sexual dysfunction appears promising, the current landscape of patient-facing websites in Canada may mislead patients seeking treatment for sexual dysfunction.
KEY MESSAGES
■ Low-intensity shockwave therapy (LISWT) is an emerging treatment for sexual dysfunction that is widely available in Canada.
■ There are many websites in Canada promoting use of LISWT for the treatment of sexual dysfunction at significant cost. These websites are generally of poor quality and lack critical information.
■ While the emergence of novel treatments for sexual dysfunction appears promising, the current landscape of patient-facing websites in Canada may mislead patients
Supplementary Information
Footnotes
Appendix available at cuaj.ca
COMPETING INTERESTS: Dr. Krakowsky has been an advisory board member for Acerus, Felix Pharma, and Viatris. All other authors do not report any competing personal or financial interests related to this work.
This paper has been peer-reviewed.
REFERENCES
- 1.Becker M, Goetzenich A, Roehl AB, et al. Myocardial effects of local shockwave therapy in a Langendorff model. Ultrasonics. 2014;54:131–6. doi: 10.1016/j.ultras.2013.07.005. [DOI] [PubMed] [Google Scholar]
- 2.Hayashi D, Kawakami K, Ito K, et al. Low-energy extracorporeal shockwave therapy enhances skin wound healing in diabetic mice: A critical role of endothelial nitric oxide synthase. Wound Repair Regen. 2012;20:887–95. doi: 10.1111/j.1524-475X.2012.00851.x. [DOI] [PubMed] [Google Scholar]
- 3.Gruenwald I, Kitrey ND, Appel B, et al. Low-intensity extracorporeal shockwave therapy in vascular disease and erectile dysfunction: Theory and outcomes. Sex Med Rev. 2013;1:83–90. doi: 10.1002/smrj.9. [DOI] [PubMed] [Google Scholar]
- 4.Capogrosso P, Frey A, Jensen CFS, et al. Low-intensity shock wave therapy in sexual medicine-clinical recommendations from the European Society of Sexual Medicine (ESSM) J Sex Med. 2019;16:1490–1505. doi: 10.1016/j.jsxm.2019.07.016. [DOI] [PubMed] [Google Scholar]
- 5.Angulo JC, Arance I, de las Heras MM, et al. [Eficacia de la terapia de ondas de choque de baja intensidad para la disfunción eréctil: revisión sistemática y metaanálisis]. Actas Urol Esp. 2017;41:479–90. doi: 10.1016/j.acuro.2016.07.005. [DOI] [PubMed] [Google Scholar]
- 6.Lu Z, Lin G, Reed-Maldonado A, et al. Low-intensity extracorporeal shockwave treatment improves erectile function: A systematic review and meta-analysis. Eur Urol. 2017;71:223–33. doi: 10.1016/j.eururo.2016.05.050. [DOI] [PubMed] [Google Scholar]
- 7.Man L, Li G. Low-intensity extracorporeal shock wave therapy for erectile dysfunction: A systematic review and meta-analysis. Urology. 2018;119:97–103. doi: 10.1016/j.urology.2017.09.011. [DOI] [PubMed] [Google Scholar]
- 8.Domes T, Najafabadi BT, Roberts M, et al. Canadian Urological Association guideline: Erectile dysfunction. Can Urol Assoc J. 2021;15:310–22. doi: 10.5489/cuaj.7572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Khazaal Y, Chatton A, Cochand S, et al. Brief DISCERN, six questions for the evaluation of evidence-based content of health-related websites. Patient Educ Couns. 2009;77:33–7. doi: 10.1016/j.pec.2009.02.016. [DOI] [PubMed] [Google Scholar]
- 10.Our commitment to reliable health and medical information. [Accessed December 10, 2023]. Available at: https://myhon.ch/en/
- 11.Friedman DB, Hoffman-Goetz L. A systematic review of readability and comprehension instruments used for print and web-based cancer information. Heal Educ Behav. 2006;33:352–73. doi: 10.1177/1090198105277329. [DOI] [PubMed] [Google Scholar]
- 12.Tian C, Champlin S, Mackert M, et al. Readability, suitability, and health content assessment of web-based patient education materials on colorectal cancer screening. Gastrointest Endosc. 2014;80:284–90. doi: 10.1016/j.gie.2014.01.034. [DOI] [PubMed] [Google Scholar]
- 13.Clavijo RI, Kohn TP, Kohn JR, et al. Effects of low intensity extracorporeal shockwave therapy on erectile dysfunction: A systematic review and meta-analysis. J Sex Med. 2017;14:27–35. doi: 10.1016/j.jsxm.2016.11.001. [DOI] [PubMed] [Google Scholar]
- 14.Zou ZJ, Tang LY, Liu ZH, et al. Short-term efficacy and safety of low-intensity extracorporeal shockwave therapy in erectile dysfunction: a systematic review and meta-analysis. Int Braz J Urol. 2017;43:805–21. doi: 10.1590/s1677-5538.ibju.2016.0245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gao L, Qian S, Tang Z, et al. A meta-analysis of extracorporeal shock wave therapy for Peyronie’s disease. Int J Impot Res. 2016;28:161–6. doi: 10.1038/ijir.2016.24. [DOI] [PubMed] [Google Scholar]
- 16.Hatzichristodoulou G, Meisner C, Gschwend JE. Extracorporeal shockwave therapy in Peyronie’s disease: Results of a placebo-controlled, prospective, randomized, single-blind study. J Sex Med. 2013;10:2815–21. doi: 10.1111/jsm.12275. [DOI] [PubMed] [Google Scholar]
- 17.Mirone V, Imbimbo C, Palmieri A, et al. Our experience on the association of a new physical and medical therapy in patients suffering from induratio penis plastica. Eur Urol. 1999;36:327–30. doi: 10.1159/000020013. [DOI] [PubMed] [Google Scholar]
- 18.Hauck EW, Altinkilic BM, Ludwig M, et al. Extracorporal shockwave therapy in the treatment of Peyronie’s disease: First results of a case-controlled approach. Eur Urol. 2000;38:663–70. doi: 10.1159/000020359. [DOI] [PubMed] [Google Scholar]
- 19.Bella AJ, Lee JC, Grober ED, et al. 2018 Canadian Urological Association guideline for Peyronie’s disease and congenital penile curvature. Can Urol Assoc J. 2018;12:E197–209. doi: 10.5489/cuaj.5255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Katz JE, Clavijo RI, Rizk P, et al. The basic physics of waves, soundwaves, and shockwaves for erectile dysfunction. Sex Med Rev. 2020;8:100–5. doi: 10.1016/j.sxmr.2019.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Romeo P, Lavanga V, Pagani D, et al. Extracorporeal shockwave therapy in musculoskeletal disorders: A review. Med Princ Pract. 2014;23:7–13. doi: 10.1159/000355472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Elmansy HE, Lingeman JE. Recent advances in lithotripsy technology and treatment strategies: a systematic review update. Int J Surg. 2016;36:676–80. doi: 10.1016/j.ijsu.2016.11.097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wu SS, Ericson KJ, Shoskes DA. Retrospective comparison of focused shockwave therapy and radial wave therapy for men with erectile dysfunction. Transl Androl Urol. 2020;9:2122–8. doi: 10.21037/tau-20-911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sandoval-Salinas C, Saffon JP, Martínez JM, et al. Are radial pressure waves effective for the treatment of moderate or mild to moderate erectile dysfunction? A randomized sham therapy-controlled clinical trial. J Sex Med. 2022;19:738–44. doi: 10.1016/j.jsxm.2022.02.010. [DOI] [PubMed] [Google Scholar]
- 25.Bryk D, Murthy PB, Ericson JK, et al. Radial wave therapy does not improve early recovery of erectile function after nerve-sparing radical prostatectomy: A prospective trial. Transl Androl Urol. 2023;12:209–16. doi: 10.21037/tau-22-310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cotugna N, Vickery CE, Carpenter-Haefele KM. Evaluation of literacy level of patient education pages in health-related journals. J Community Health. 2005;30:213–9. doi: 10.1007/s10900-004-1959-x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.