

Abstract
Background:
This work aims to review the current literature and our experience on vascular Eagle syndrome (ES) that can present misleading clinical presentations and better understand the possible therapeutic strategies.
Methods:
We reviewed the existing literature on PubMed from January 1, 2017, to December 31, 2022, including the sequential keywords “vascular AND Eagle syndrome,” “vascular AND styloid syndrome,” “vascular AND elongated styloid process,” “vascular AND stylocarotid syndrome,” and “Eagle syndrome AND carotid artery dissection.”
Results:
38 vascular ES cases, including our experience, were analyzed. The most frequent clinical onset was hemiparesis (n 21, 57%), but other regular clinical presentations were aphasia, loss of consciousness, amaurosis, headache, or a combination of the latter. Massive oral bleeding was reported only once in the literature before our case. Twelve patients were treated with only antiplatelet therapy, either single or double. Nine patients were treated with anticoagulation therapy only. In 14 patients, a carotid artery stent was used, associated with anticoagulation or antiplatelet therapy. In 17 cases, a styloid process (SP) resection was performed.
Conclusion:
ES has many clinical presentations, and carotid artery dissection resulting in oral bleeding seems rare. Literature results and our experience make us believe that when dealing with vascular ES, the best treatment strategy is endovascular internal carotid artery stenting with antiplatelet therapy, followed by surgical removal of the elongated SP to prevent stent fracture.
Keywords: Eagle syndrome, Elongated styloid process, Internal carotid artery dissection, Stylocarotid syndrome, Vascular Eagle syndrome

INTRODUCTION
Eagle syndrome (ES) is a rare condition with different clinical presentations. First described by Eagle in 1937, it refers to various symptoms caused by the conflict of an elongated styloid process (ESP) – unilateral or bilateral – and/or calcified styloid ligament (CSL) with the surrounding anatomical structures. Originally, Eagle described this condition as a unilateral throat pain associated with the sensation of a foreign body in the throat.[11] Subsequently, the symptoms were classified into two main types depending on the involvement of either neural or vascular structures.[12] Odynophagia, facial and cervical pain, migraine, and dysphagia are usually caused by the impingement of the lower nerves in the neck by the styloid process (SP). On the other hand, when talking about “vascular Eagle syndrome,” authors refer to an ESP causing vascular compression, and often resulting in carotid artery dissection (CAD) and/or ischemia in the internal carotid artery (ICA) or middle cerebral artery (MCA) territories.[39,48] Many authors have described this syndrome, and the average length of the SP varies significantly in the literature. Conventionally, the SP is defined as elongated when it reaches 30 mm long.[4,26,32,34,40] The prevalence of ESP in the general population is around 4%, while symptoms are seen in only 4–10% of this group;[22] therefore, length itself is not always associated with symptoms. Other causes can contribute to the pathogenesis of this condition, such as soft-tissue disease, trauma, surgical insult (tonsillectomy), endocrine causes, or abuse of substances that can cause vasculitis-like damage facilitating compression and CAD.[44,50]
This review focused on the vascular form, a rare condition caused by the contact between ESP and/or CSL and the extracranial carotid artery. This conflict can lead to neurological symptoms (ischemia of downstream cerebral territories) due to compression, especially during rotational movement, or due to dissection and/or dissecting aneurysms of the carotid artery itself. We also present a case of a 48-year-old man without vascular risk factors contributing to mass oral bleeding and a later episode of transient dysarthria diagnosed with ES and treated with dual antiplatelet therapy (DAPT) therapy, endovascular flow-diverter (FD), and surgical SP removal. Since there is significant variability in clinical presentations and there is not a clear consensus on the management of this condition, we aim to summarize the current literature and to make a systematic review of cases of ES and CAD, considering articles from January 1, 2017, to December 31, 2022, expanding a previous study published in 2020 by Baldino et al.[5]
MATERIALS AND METHODS
We reviewed the existing literature on PubMed from January 1, 2017, to December 31, 2022, without restrictions about the paper publication status, according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement.[33]
We researched PubMed for the literature regarding patients with an ESP and/or ligament calcification causing either cervical ICA dissection or cervical ICA dissecting aneurysms. The following sequential keywords were used: “vascular AND Eagle syndrome,” “vascular AND styloid syndrome,” “vascular AND elongated styloid process,” “vascular AND stylocarotid syndrome,” and “Eagle syndrome AND carotid artery dissection.”
Inclusion criteria included articles in English published between January 1, 2017, and December 31, 2022, and considering ES only associated with ICA dissection or dissecting aneurysms. Exclusion criteria were articles focused on ES presenting with clinical features other than ICA dissection, articles in different languages or only abstracts available, pure reviews (without new cases), or editorials.
We analyzed different features:
Population characteristics such as sex and age
Symptoms of onset
Laterality and length of ESPs
Initial and eventual additional treatment
Time of follow-up.
RESULTS
Through literature research on PubMed, between January 1, 2017, and December 31, 2022, 51 articles were found using the words “vascular AND Eagle syndrome, 48 articles using the words “vascular AND styloid syndrome,” 53 articles using the words “vascular AND elongated styloid process,” ten articles using the words “vascular AND stylocarotid syndrome,” and 31 articles using the words “Eagle syndrome AND carotid artery dissection.” Excluding repetitions, 67 original articles were screened through analysis of title and abstract. Thirty-two articles were then, excluded based on inclusion criteria cited before. A total of 35 articles were analyzed through full-text reading, and four more articles were excluded due to non-interesting data. In summary, 31 articles were used for this review [PRISMA graph in Figure 1].
Figure 1:

Preferred reporting items for systematic reviews and meta-analyses graph shows paper selection method.
This paper reports an additional case of CAD associated with an ESP, treated at Belcolle Hospital in Viterbo in September 2018.
Our review of the literature shows that between 2017 and 2022, 37 cases of internal CAD have been caused by the vascular variant of ES. The demographic, clinical characteristics, treatment strategies, and follow-up of the patients are summarized in Table 1.[1,2,5,6,10,14-16,18-21,23,24,27,30,31,37,38,42-47,50-52,54,55,57]
Table 1:
A comprehensive literature analysis of vascular Eagle’s syndrome cases.

The mean age of the patients was 48.2 years (range 30–72). In an article, one patient was described as a “teenager” but was not used for statistical evaluation. The prevalence was higher in men (n = 24, 69%) than in women (n = 11, 31%). In two cases, sex was not specified. In only one case, internal CAD was found occasionally, while an acute onset was described in all other cases. The most frequent clinical onset was hemiparesis (n = 21, 57%), but other frequent clinical presentations were aphasia, loss of consciousness, amaurosis, headache, or a combination of the latter. Bleeding from the oral cavity with hemoptysis was reported in only one case, resulting in a rare clinical presentation.
In the literature, there is a significant variability of treatment strategies. There is not a strong consensus on whether to prefer anticoagulation or antiplatelet therapy. In these cases, 12 patients were treated with only antiplatelet therapy, either single or double. Nine patients were treated with anticoagulation therapy only, with previous thrombus aspiration in two of these cases. In 14 patients, a carotid artery stent was used, associated with anticoagulation or antiplatelet therapy. In two cases, thrombectomy of MCA occlusion was necessary before stenting. In three cases, angioplasty was used before stenting. In 17 cases, a SP resection was performed. Only in one case, SP resection was used as the only treatment, while, in all other cases, it was used as a secondary procedure after the resolution of the CAD to eliminate the mechanical cause and prevent recurrence.
Clinical case
In September 2018, a 48-year-old man without any history of vascular and neurovascular risk factors was admitted to our Emergency Room due to a sudden massive oral bleeding and a slight spatial and temporal disorientation. Contrast enhancement computed tomography (CT) scan showed a large portion of hypodense tissue with poor enhancement in the left retropharyngeal space, with an axial diameter of about 5 × 3 cm [Figure 2]. Such tissue medially dislocated the tonsils, imprinting the oropharyngeal aerial column, and involved the vascular space laterally, compressing the left internal jugular vein, but with regular size internal and external carotid arteries. Such hypodense tissue with mass effect is oriented toward different diagnoses, including head and neck neoplasm, infectious-inflammatory disorders, or bleeding carotid artery aneurysms. Video laryngoscopy examination highlighted an ab extrinsic imprint of the oropharynx on the left. A week after admission, the patient experienced an episode of transient dysarthria, and magnetic resonance imaging of the head and neck region was performed. The examination better defined the tissue limits near the medium-distal extracranial tract of the left carotid artery, showing a possible aneurismatic dilatation of about 4.5 mm of the anterior wall of the artery. The patient underwent a CT angiography that confirmed the presence of a small bleb of about 3 mm in size, located at the top third of the left carotid artery at the apex of the left SP. The bone examination confirmed the presence of a longer SP bilaterally (about 50 mm on the left and 55 mm on the right) and a conflict on the left side, causing the compression of the homolateral ICA [Figure 3]. After multidisciplinary discussion, percutaneous endovascular treatment of the ICA dissection was performed, and an FD device (Streamline 5 mm × 25 mm) was placed [Figure 4]. DAPT was continued for six months. After 12 months, surgical removal of the left SP was obtained. The surgical procedure was performed in mono antiplatelet therapy. The patient fully recovered and remained asymptomatic, and at 48 months, the radiological examinations confirmed the presence of the previously implanted stent on the extracranial ICA, which appears normally positioned and patent [Figure 5].
Figure 2:
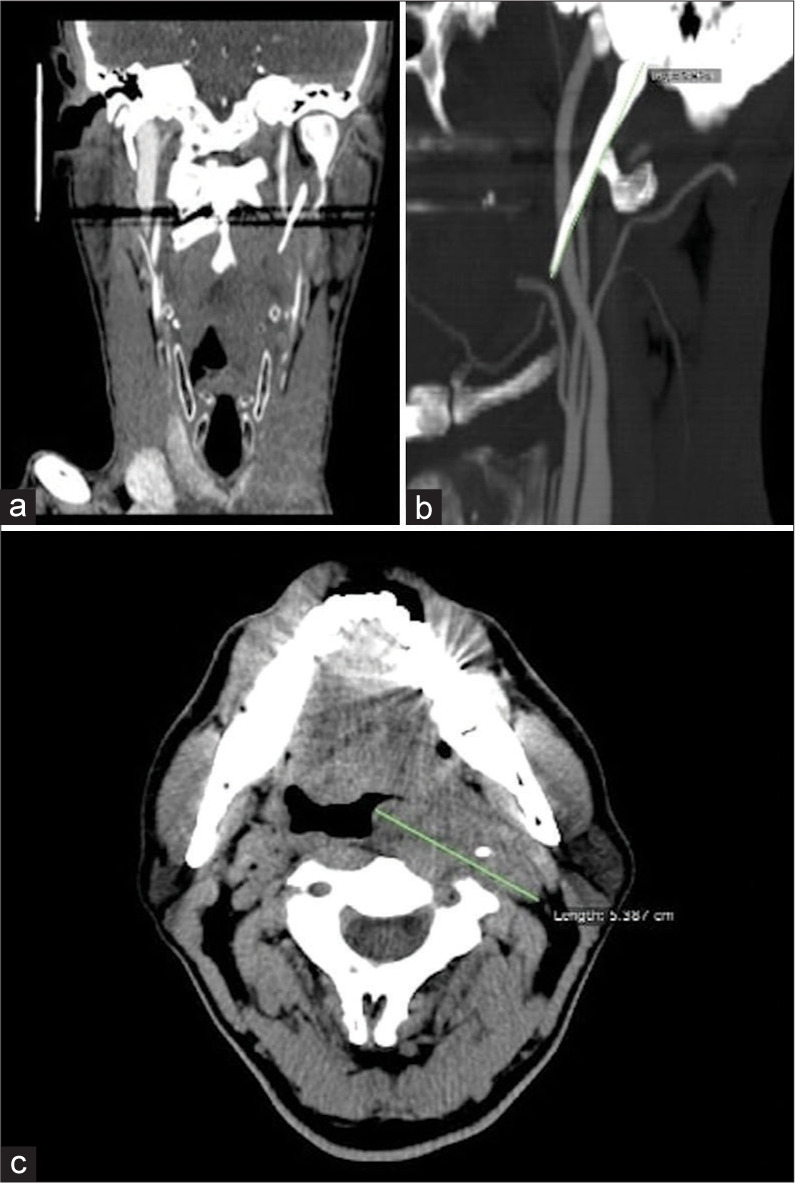
(a and b) Coronal and sagittal computed tomography (CT) scans show the elongated left styloid process causing internal carotid artery compression. (c) The axial CT scan showed hypodense tissue in the left retropharyngeal space with poor enhancement and diameters of about 5 × 3 cm.
Figure 3:
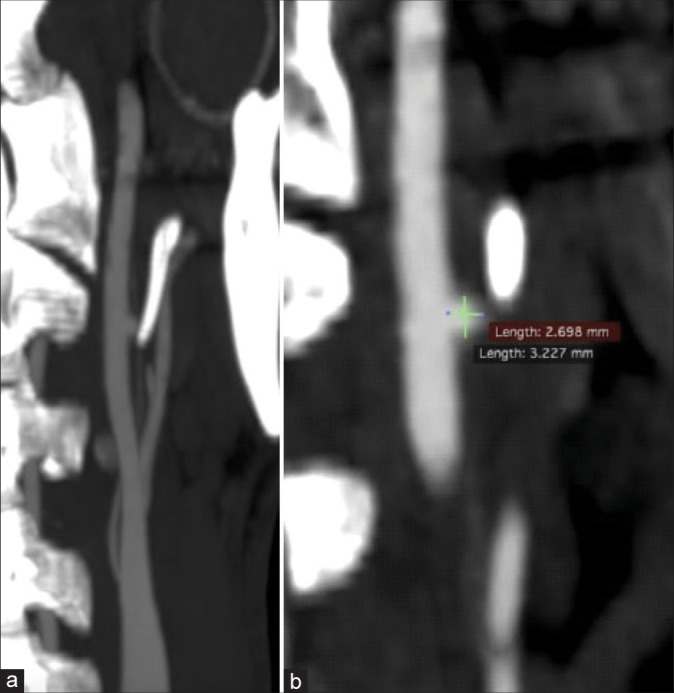
(a and b) A small bleb about 3 mm in size is shown, located at the top III left internal carotid artery at the height of the apex of the temporal style process.
Figure 4:
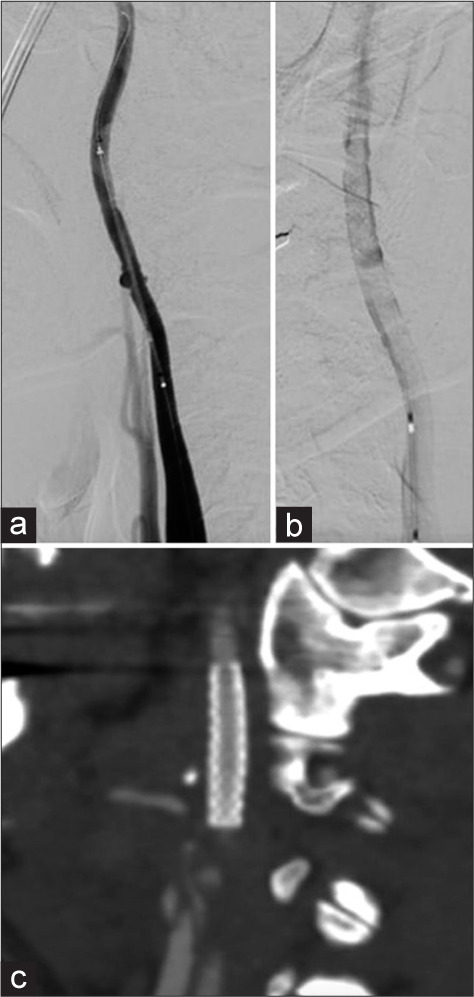
(a and b) Lateral angiography of the left carotid artery shows the placement of the flow-diverter device (Streamline 5 mm × 25 mm). (c) One month computed tomography scan shows stent placement with no complications.
Figure 5:
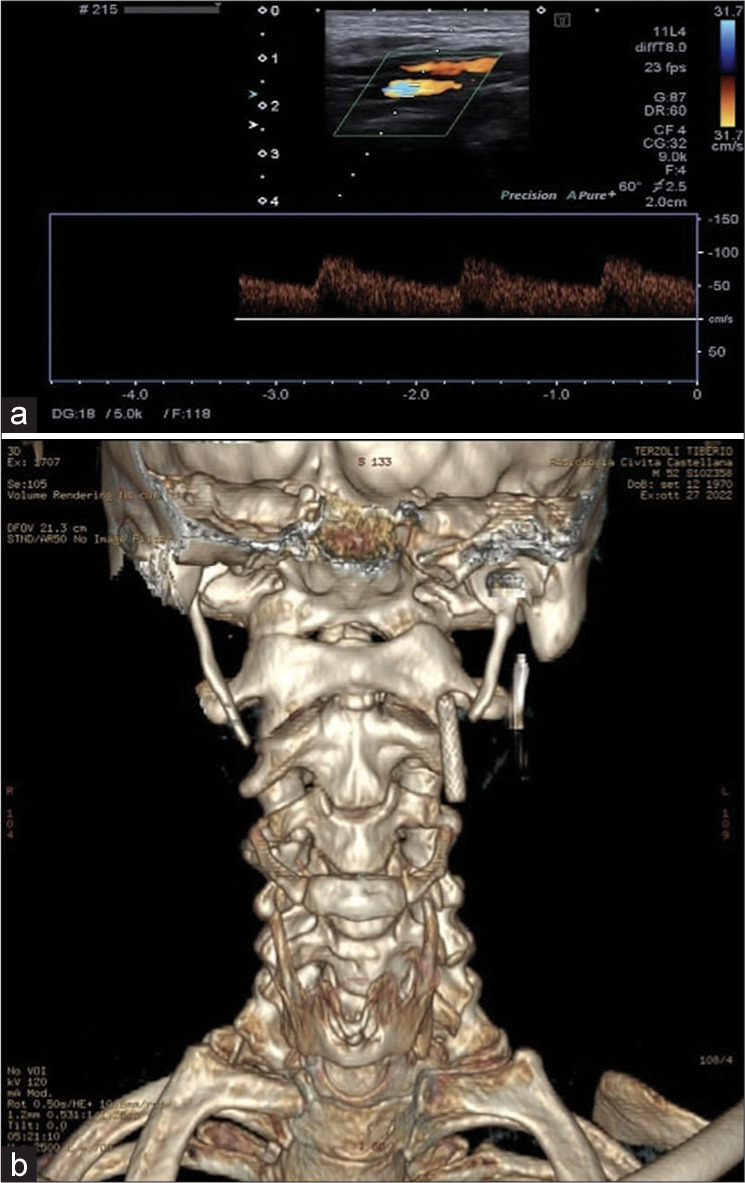
(a) The echo-color-Doppler examination of the left internal carotid artery documents the presence of the flow-diverter stent, which appears in the correct position and patent with an intra-stent sampled velocity index in range. (b) Postoperative 3D reconstruction computed tomography scan; reducing the styloid process length avoids impingement with the stent.
DISCUSSION
Massive oral bleeding is a rare and nonspecific clinical presentation related to traumatic events, upper gastrointestinal tract tumors or inflammatory processes, ulceration, rupture of esophageal varices, use of anticoagulation therapy, and many other underlying issues. When bleeding occurs in healthy young patients without comorbidities nor apparent triggers, it arouses concerns and attention. One rarely reported cause of oral cavity bleeding can be CAD associated with vascular ES.[25,31]
First described by Eagle in 1937, ES is a rare condition characterized by an abnormal length and/or slope of SP or a CSL.[11,12] The origin of an ESP or ossified styloid ligament may be identified in retained embryologic cartilage tissue from Reichert’s cartilage, calcification of the stylomandibular ligament or expansion of osseous tissue at the origin of the stylomandibular ligament,[35] inflammation due to aging,[7] and reactive hyperplasia or metaplasia from trauma or simply as an anatomical variant without evidence or history of trauma,[49] but the exact cause and etiopathogenesis remain unclear.
SP physiological length is around 20–25 mm, and 3 cm is usually the upper limit. A length of 4 cm is highly associated with symptoms, varying from pain in the lateral cervical area alone to severe vascular or nervous complications. In the presented case, SP length was 5 cm on the left side and 5.5 cm on the right. The incidence of elongated SP in the general population is 4–10%, but only approximately 4% of these cases are symptomatic; therefore, ES is <2% in the general population. As we can also notice in our case, even if the SP on the right side was longer, it did not conflict with neurovascular structures, highlighting that the length itself is insufficient to provoke the symptoms. In this small percentage of cases, the anatomical abnormality determines symptoms that define two pictures commonly recognized as “neurological variant” and “vascular variant” due to conflict with the adjacent anatomical structures. Indeed, in its course from the temporal bone posteriorly to the mastoid apex toward the maxillo-vertebro-pharyngeal recess, SP has a relationship with many important vascular (carotid arteries, and internal jugular vein) and nervous structures (facial, vagus, glossopharyngeal, and hypoglossal nerves). Based on clinical presentation, Eagle classified the syndrome into two subgroups: classic and vascular type. The classic type includes odynophagia, dysphagia, and/or cervical or facial pain elicited by head rotational movements. The vascular form, also known as stylocarotid syndrome, is a quite rare condition in which an elongated SP compresses the extracranial carotid artery and results in parietal or periorbital pain, and neurological symptoms such as headache, dizziness, transient visual loss, syncope, and stroke, often caused by compression or by the dissection of the carotid artery itself. In our case, oral bleeding was the first clinical presentation. This uncommon presentation has been described only once in the literature [31], and the exact mechanism remains unclear. Hemoptysis can probably be explained by blood leaks in the retropharyngeal recess and toward the surrounding cervical soft tissues.
Despite its benign nature, ES can lead to potentially severe complications. In the literature, many reports of transient ischemic attacks (TIAs) and strokes of the downstream territories of ICA are described, as an elongated SP has been recognized as a risk factor for CAD.[16,36,39,41,53]
The collection of medical, clinical, and radiological data can guide the diagnosis of vascular ES. Imaging, particularly a CT scan, is helpful in identifying the anatomical abnormalities and the presence of a neurovascular conflict. CT angiography is the gold standard and can provide further information regarding carotid flow, especially if stroke or dissection is suspected, and can be aided by 3D reconstructed images.[35]
Regarding treatment strategies, if patients with the classic form can be managed conservatively with analgesics, steroids, or local anesthetic, a surgical approach is preferred in cases of major vascular and neurological complications. A styloidectomy can be performed, and a transoral or transcervical method can be chosen.[3,9] Usually, the choice is dictated by the preference or experience of the surgeon. Since the association between CAD and elongated SP is uncommon, there are no exact guidelines regarding the best treatment.
Patients with symptomatic CAD presenting with ischemic stroke, TIA, retinal ischemia, or local symptoms only and without subarachnoid hemorrhage should be treated according to the ESO guidelines for managing extracranial and intracranial artery dissection.[8] When the patient presents with acute ischemic stroke and extracranial artery dissection, treatment with intravenous thrombolysis within 4.5 h from the symptom’s onset should be performed. Mechanic thrombolysis is also recommended when a large vessel occlusion of the anterior circulation is encountered. Two multicentric randomized controlled studies[13,28] were analyzed regarding the use of anticoagulant versus antiplatelet therapy. The two groups had no statistical difference in the composite outcome of ischemic stroke, major bleeding, and death. The functional result was available in only one randomized controlled trial[13] and did not differ between the two groups. Subgroups of single versus double antiplatelet therapy did not show differences between the previous outcomes.
There is no firm recommendation on whether to use emergency stenting of the dissected carotid artery. One study[29] showed better successful reperfusion results with stenting than the non-stenting control group, but functional results did not differ.
We suggest that stenting of the ICA is advisable to achieve CAD correction in case of persistent ischemic symptoms, as in our case (dysarthria). Stenting can lower the risk of persisting vessel damage caused by the ESP while guaranteeing successful reperfusion of the downstream territories. As a result of recent literature, endovascular management of ICA dissection can provide good results, with a low rate of periprocedural complication and good long-term follow-up. [56] moreover, an association of surgical styloidectomy is recommended to eliminate the initial cause of neurovascular conflict and to prevent further damage to the implanted stent.[17]
CONCLUSION
ES has many clinical presentations, as evidenced by the multitude of nonspecific symptoms reported in the literature. The pathophysiologic mechanism of ES is related to the compression of the surrounding neurovascular structures.
The classic form of ES is described when nerve compression leads to craniofacial and cervical pain, and the sympathetic plexus’s irritation around the ICA’s cervical segment can cause vertigo and syncope. On the other hand, the vascular form is caused by direct compression of the extracranial ICA by the elongated SP, resulting in TIA or stroke and sometimes in CAD. CAD resulting in oral bleeding seems to be a rare clinical presentation, and the exact mechanism remains unclear. Literature results and our experience make us believe that when dealing with vascular ES, the best treatment strategy is endovascular stenting of ICA with antiplatelet therapy, followed by surgical removal of the elongated SP to prevent stent fracture.
We want to highlight that our experience may contribute to identifying a rare possible complication of vascular ES. Furthermore, the vascular form of ES should always be considered in the differential diagnosis in the presence of spontaneous nontraumatic CAD.
Footnotes
How to cite this article: Pagano S, Ricciuti V, Mancini F, Barbieri FR, Chegai F, Marini A, et al. Eagle syndrome: An updated review. Surg Neurol Int 2023;14:389.
Contributor Information
Serena Pagano, Email: serena.pagano@asl.vt.it.
Vittorio Ricciuti, Email: vittorio.ricciuti@gmail.com.
Fabrizio Mancini, Email: fabrizio.geremia.mancini@gmail.com.
Francesca Romana Barbieri, Email: francesca.barbieri@asl.vt.it.
Fabrizio Chegai, Email: fabrizio.chegai@asl.vt.it.
Alessandra Marini, Email: marini.alessandra.am@gmail.com.
Daniele Marruzzo, Email: daniele.marruzzo@asl.vt.it.
Riccardo Paracino, Email: r.paracino@gmail.com.
Riccardo Antonio Ricciuti, Email: riccardo.ricciuti@gmail.com.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
REFERENCES
- 1.Amorim JM, Lopes M, Ferreira C, Pinho J. Carotid artery dissection associated with long styloid process. Vasc Med. 2017;22:245. doi: 10.1177/1358863X16681487. [DOI] [PubMed] [Google Scholar]
- 2.Aydin E, Quliyev H, Cinar C, Bozkaya H, Oran I. Eagle syndrome presenting with neurological symptoms. Turk Neurosurg. 2016;28:219–25. doi: 10.5137/1019-5149.JTN.17905-16.6. [DOI] [PubMed] [Google Scholar]
- 3.Badhey A, Jategaonkar A, Anglin Kovacs AJ, Kadakia S, De Deyn PP, Ducic Y, et al. Eagle syndrome: A comprehensive review. Clin Neurol Neurosurg. 2017;159:34–8. doi: 10.1016/j.clineuro.2017.04.021. [DOI] [PubMed] [Google Scholar]
- 4.Balcioglu HA, Kilic C, Akyol M, Ozan H, Kokten G. Length of the styloid process and anatomical implications for Eagle’s syndrome. Folia Morphol (Warsz) 2009;68:265–70. [PubMed] [Google Scholar]
- 5.Baldino G, Di Girolamo C, De Blasis G, Gori A. Eagle syndrome and internal carotid artery dissection: Description of five cases treated in two Italian institutions and review of the literature. Ann Vasc Surg. 2020;67:565.e17–24. doi: 10.1016/j.avsg.2020.02.033. [DOI] [PubMed] [Google Scholar]
- 6.Brassart N, Deforche M, Goutte A, Wery D. A rare vascular complication of Eagle syndrome highlight by CTA with neck flexion. Radiol Case Rep. 2020;15:1408–12. doi: 10.1016/j.radcr.2020.05.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Camarda AJ, Deschamps C, Forest D. I. Stylohyoid chain ossification: A discussion of etiology. Oral Surg Oral Med Oral Pathol. 1989;67:508–14. doi: 10.1016/0030-4220(89)90264-8. [DOI] [PubMed] [Google Scholar]
- 8.Debette S, Mazighi M, Bijlenga P, Pezzini A, Koga M, Bersano A, et al. ESO guideline for the management of extracranial and intracranial artery dissection. Eur Stroke J. 2021;6:XXXIX–LXXXVIII. doi: 10.1177/23969873211046475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Demirtaş H, Kayan M, Koyuncuoğlu HR, Çelik AO, Kara M, Şengeze N. Eagle syndrome causing vascular compression with cervical rotation: Case report. Pol J Radiol. 2016;81:277–80. doi: 10.12659/PJR.896741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Duarte-Celada WR, Jin D, Neves G, Windisch T. Bilateral carotid dissection due to Eagle syndrome in a young female. eNeurologicalSci. 2021;24:100353. doi: 10.1016/j.ensci.2021.100353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Eagle WW. Elongated styloid process; further observations and a new syndrome. Arch Otolaryngol (1925) 1948;47:630–40. doi: 10.1001/archotol.1948.00690030654006. [DOI] [PubMed] [Google Scholar]
- 12.Eagle WW. Elongated styloid process; symptoms and treatment. AMA Arch Otolaryngol. 1958;67:172–6. doi: 10.1001/archotol.1958.00730010178007. [DOI] [PubMed] [Google Scholar]
- 13.Engelter ST, Traenka C, Gensicke H, Schaedelin SA, Luft AR, Simonetti BG, et al. Aspirin versus anticoagulation in cervical artery dissection (TREAT-CAD): An open-label, randomised, non-inferiority trial. Lancet Neurol. 2021;20:341–50. doi: 10.1016/S1474-4422(21)00044-2. [DOI] [PubMed] [Google Scholar]
- 14.Entezami P, Entezami P, Field NC, Nourollah-Zadeh E, Pinheiro-Neto CD, Dalfino JC. Neurosurgical management of vascular compression presenting as visual symptoms secondary to elongated styloid processes (Eagle syndrome) Br J Neurosurg. 2021;35:1–4. doi: 10.1080/02688697.2021.1921108. [DOI] [PubMed] [Google Scholar]
- 15.Galletta K, Granata F, Longo M, Alafaci C, De Ponte FS, Squillaci D, et al. An unusual internal carotid artery compression as a possible cause of Eagle syndrome-a novel hypothesis and an innovative surgical technique. Surg Neurol Int. 2019;10:174. doi: 10.25259/SNI_317_2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hebant B, Guegan-Massardier E, Macaigne V, TriquenotBagan A. Ischemic stroke due to internal carotid artery dissection associated with an elongated styloid process (Eagle syndrome) J Neurol Sci. 2017;372:466–7. doi: 10.1016/j.jns.2016.10.055. [DOI] [PubMed] [Google Scholar]
- 17.Hooker JD, Joyner DA, Farley EP, Khan M. Carotid stent fracture from stylocarotid syndrome. J Radiol Case Rep. 2016;10:1–8. doi: 10.3941/jrcr.v10i6.1618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Horio Y, Fukuda K, Miki K, Hirao N, Iwaasa M, Abe H, et al. Dynamic assessment of internal carotid artery and elongated styloid process in a case of bilateral carotid artery dissection. Surg Neurol Int. 2020;11:163. doi: 10.25259/SNI_42_2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ikenouchi H, Takagi M, Nishimura A, Yamaguchi E, Koge J, Saito K, et al. Bilateral carotid artery dissection due to Eagle syndrome in a patient with vascular Ehlers-Danlos syndrome: A case report. BMC Neurol. 2020;20:285. doi: 10.1186/s12883-020-01866-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jelodar S, Ghadirian H, Ketabchi M, Ahmadi Karvigh S, Alimohamadi M. Bilateral ischemic stroke due to carotid artery compression by abnormally elongated styloid process at both sides: A case report. J Stroke Cerebrovasc Dis. 2018;27:e89–91. doi: 10.1016/j.jstrokecerebrovasdis.2017.12.018. [DOI] [PubMed] [Google Scholar]
- 21.Jo H, Choi EH, Song J, Chung JW, Bang OY. Carotid artery dissection caused by Eagle syndrome. Precis Future Med. 2017;1:173–6. [Google Scholar]
- 22.Kazmierski R, Wierzbicka M, Kotecka-Sowinska E, Banaszewski J, Pawlak MA. Expansion of the classification system for Eagle syndrome. Ann Intern Med. 2018;168:746–7. doi: 10.7326/L17-0507. [DOI] [PubMed] [Google Scholar]
- 23.Kesav P, Hussain SI, Dogar MA, John S. Stylo-carotid syndrome causing bilateral cervical carotid artery dissection requiring endovascular intervention. Clin Neurol Neurosurg. 2020;195:105943. doi: 10.1016/j.clineuro.2020.105943. [DOI] [PubMed] [Google Scholar]
- 24.Lakner K, Savšek L. Carotid artery type of Eagle syndrome: An uncommon cause of ischemic stroke. Wien Klin Wochenschr. 2022;135:158–61. doi: 10.1007/s00508-022-02072-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Landeen KC, Morse J, Mannion K. Spontaneous rupture of the internal carotid artery owing to an aberrant styloid process in an identical twin. JAMA Otolaryngol Head Neck Surg. 2020;146:385–6. doi: 10.1001/jamaoto.2019.4790. [DOI] [PubMed] [Google Scholar]
- 26.Langlais RP, Miles DA, Van Dis ML. Elongated and mineralized stylohyoid ligament complex: A proposed classification and report of a case of Eagle’s syndrome. Oral Surg Oral Med Oral Pathol. 1986;61:527–32. doi: 10.1016/0030-4220(86)90400-7. [DOI] [PubMed] [Google Scholar]
- 27.Mann A, Kujath S, Friedell ML, Hardouin S, Wood C, Carter R, et al. Eagle syndrome presenting after blunt trauma. Ann Vasc Surg. 2017;40:295.e5–8. doi: 10.1016/j.avsg.2016.07.077. [DOI] [PubMed] [Google Scholar]
- 28.Markus HS, Levi C, King A, Madigan J, Norris J, Cervical Artery Dissection in Stroke Study (CADISS) Investigators Antiplatelet therapy vs anticoagulation therapy in cervical artery dissection: The cervical artery dissection in stroke study (CADISS) randomized clinical trial final results. JAMA Neurol. 2019;76:657–64. doi: 10.1001/jamaneurol.2019.0072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Marnat G, Lapergue B, Sibon I, Gariel F, Bourcier R, Kyheng M, et al. Safety and outcome of carotid dissection stenting during the treatment of tandem occlusions: A pooled analysis of TITAN and ETIS. Stroke. 2020;51:3713–8. doi: 10.1161/STROKEAHA.120.030038. [DOI] [PubMed] [Google Scholar]
- 30.Matsukawa S, Ishibashi R, Kitamura K, Sugiyama J, Yoshizaki W, Motoie R, et al. Carotid micromesh stent for the cervical carotid artery dissecting aneurysm in a patient with vascular Eagle syndrome. J Stroke Cerebrovasc Dis. 2022;31:106487. doi: 10.1016/j.jstrokecerebrovasdis.2022.106487. [DOI] [PubMed] [Google Scholar]
- 31.Michiels TD, Marsman MS, van Veen A, Vriens PW, Lauret GJ, Heyligers JM. Eagle syndrome: A unique cause of carotid bleeding. JACC Case Rep. 2020;2:449–53. doi: 10.1016/j.jaccas.2019.12.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Moffat DA, Ramsden RT, Shaw HJ. The styloid process syndrome: Aetiological factors and surgical management. J Laryngol Otol. 1977;91:279–94. doi: 10.1017/s0022215100083699. [DOI] [PubMed] [Google Scholar]
- 33.Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Monsour PA, Young WG. Variability of the styloid process and stylohyoid ligament in panoramic radiographs. Oral Surg Oral Med Oral Pathol. 1986;61:522–6. doi: 10.1016/0030-4220(86)90399-3. [DOI] [PubMed] [Google Scholar]
- 35.Murtagh RD, Caracciolo JT, Fernandez G. CT findings associated with Eagle syndrome. AJNR Am J Neuroradiol. 2001;22:1401–2. [PMC free article] [PubMed] [Google Scholar]
- 36.Ohara N, Sakaguchi M, Okazaki S, Nagano K, Kitagawa K. Internal carotid artery dissection caused by an elongated styloid process: Usefulness of transoral ultrasonography. J Stroke Cerebrovasc Dis. 2012;21:918.e7–8. doi: 10.1016/j.jstrokecerebrovasdis.2012.05.014. [DOI] [PubMed] [Google Scholar]
- 37.Okada Y, Mitsui N, Ozaki H, Sanada T, Yamamoto S, Saito M, et al. Carotid artery dissection due to elongated styloid process treated by acute phase carotid artery stenting: A case report. Surg Neurol Int. 2022;13:183. doi: 10.25259/SNI_47_2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Qureshi S, Farooq MU, Gorelick PB. Ischemic stroke secondary to stylocarotid variant of Eagle syndrome. Neurohospitalist. 2019;9:105–8. doi: 10.1177/1941874418797763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Raser JM, Mullen MT, Kasner SE, Cucchiara BL, Messé SR. Cervical carotid artery dissection is associated with styloid process length. Neurology. 2011;77:2061–6. doi: 10.1212/WNL.0b013e31823b4729. [DOI] [PubMed] [Google Scholar]
- 40.Razak A, Short JL, Hussain SI. Carotid artery dissection due to elongated styloid process: A self-stabbing phenomenon. J Neuroimaging. 2014;24:298–301. doi: 10.1111/j.1552-6569.2012.00759.x. [DOI] [PubMed] [Google Scholar]
- 41.Renard D, Azakri S, Arquizan C, Swinnen B, Labauge P, Thijs V. Styloid and hyoid bone proximity is a risk factor for cervical carotid artery dissection. Stroke. 2013;44:2475–9. doi: 10.1161/STROKEAHA.113.001444. [DOI] [PubMed] [Google Scholar]
- 42.Sasaki K, Komatsu F, Kato Y, Hirose Y. Carotid artery dissection and aneurysm with styloid process fracture. Neurol India. 2022;70:366–8. doi: 10.4103/0028-3886.338648. [DOI] [PubMed] [Google Scholar]
- 43.Selvadurai S, Williamson A, Virk JS, Clarke P. Eagle syndrome and carotid artery dissection: A rare skull base cause of stroke. BMJ Case Rep. 2022;15:e247954. doi: 10.1136/bcr-2021-247954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Shi D, Liu C, Wang L, Cao Y, Shi J. Bilateral carotid artery dissection associated with Eagle syndrome in a drug-addicted young adult with stroke: A case report. Neurol Sci. 2022;43:6105–9. doi: 10.1007/s10072-022-06152-2. [DOI] [PubMed] [Google Scholar]
- 45.Shimozato R, Hayashi M, Niimura M, Kugasawa K, Uemura H, Hidaka Y, et al. Two patients with cerebral infarction who underwent endovascular treatment for internal carotid artery dissection related to an elongated styloid process. J Neuroendovasc Ther. 2018;12:355–61. [Google Scholar]
- 46.Shindo T, Ito M, Matsumoto J, Miki K, Fujihara F, Terasaka S, et al. A case of juvenile stroke due to carotid artery dissection from an elongated styloid process-revisiting conservative management. J Stroke Cerebrovasc Dis. 2019;28:104307. doi: 10.1016/j.jstrokecerebrovasdis.2019.104307. [DOI] [PubMed] [Google Scholar]
- 47.Smoot TW, Taha A, Tarlov N, Riebe B. Eagle syndrome: A case report of stylocarotid syndrome with internal carotid artery dissection. Interv Neuroradiol. 2017;23:433–6. doi: 10.1177/1591019917706050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Song JH, Ahn SK, Cho CB. Elongated styloid process as a cause of transient ischemic attacks. JAMA Neurol. 2013;70:1072–3. doi: 10.1001/jamaneurol.2013.1950. [DOI] [PubMed] [Google Scholar]
- 49.Steinmann EP. Styloid syndrome in absence of an elongated process. Acta Otolaryngol. 1968;66:347–56. doi: 10.3109/00016486809126301. [DOI] [PubMed] [Google Scholar]
- 50.Subedi R, Dean R, Baronos S, Dhamoon A. Carotid artery dissection: A rare complication of Eagle syndrome. BMJ Case Rep. 2017;2017:bcr2016218184. doi: 10.1136/bcr-2016-218184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Tan D, Crockett MT, Chiu AH. Delayed tine displacement of a CASPER carotid artery stent due to styloid process compression. Clin Neuroradiol. 2019;29:567–9. doi: 10.1007/s00062-019-00761-9. [DOI] [PubMed] [Google Scholar]
- 52.Tanti M, Smith A, Warren DJ, Idrovo L. Internal carotid artery dissection due to elongated styloid process. BMJ Case Rep. 2021;14:e245908. doi: 10.1136/bcr-2021-245908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Todo T, Alexander M, Stokol C, Lyden P, Braunstein G, Gewertz B. Eagle syndrome revisited: Cerebrovascular complications. Ann Vasc Surg. 2012;26:729.e1–5. doi: 10.1016/j.avsg.2011.12.005. [DOI] [PubMed] [Google Scholar]
- 54.Torikoshi S, Yamao Y, Ogino E, Taki W, Sunohara T, Nishimura M. A staged therapy for internal carotid artery dissection caused by vascular Eagle syndrome. World Neurosurg. 2019;129:133–9. doi: 10.1016/j.wneu.2019.05.208. [DOI] [PubMed] [Google Scholar]
- 55.Xhaxho S, Vyshka G, Kruja J. Eagle syndrome presenting as a neurological emergency: A case report. Surg Neurol Int. 2021;12:257. doi: 10.25259/SNI_362_2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Xianjun H, Zhiming Z. A systematic review of endovascular management of internal carotid artery dissections. Interv Neurol. 2012;1:164–70. doi: 10.1159/000353124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Zammit M, Chircop C, Attard V, D’Anastasi M. Eagle’s syndrome: A piercing matter. BMJ Case Rep. 2018;11:e226611. doi: 10.1136/bcr-2018-226611. [DOI] [PMC free article] [PubMed] [Google Scholar]