

Abstract
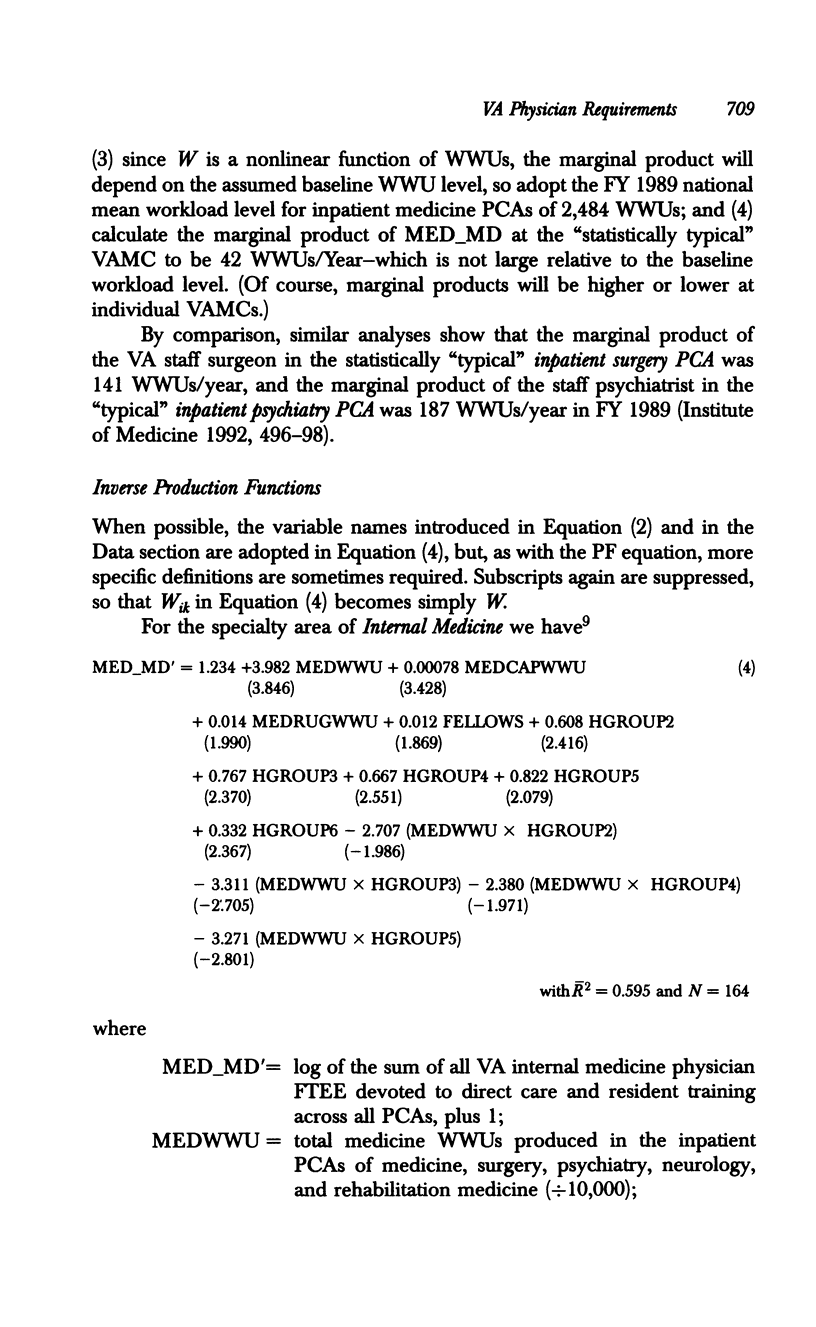
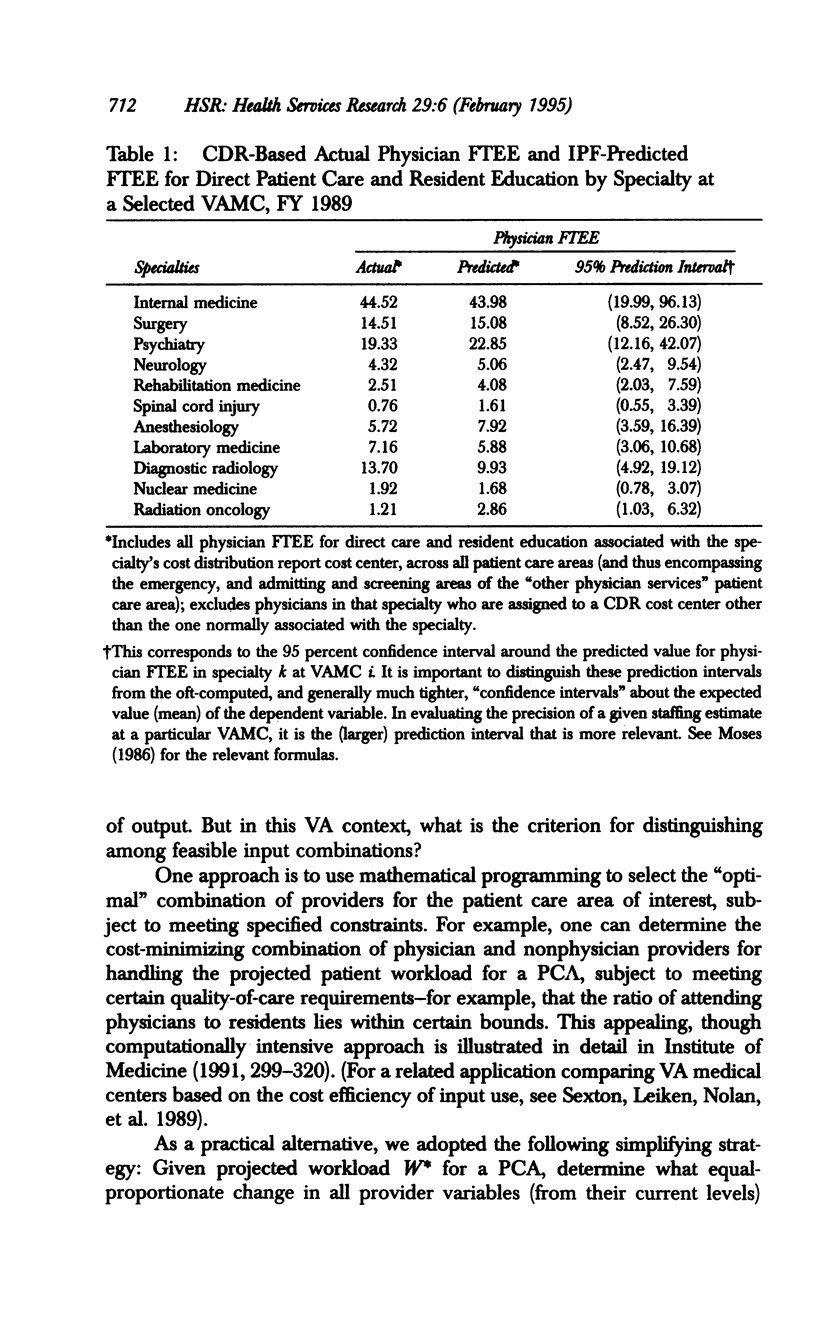
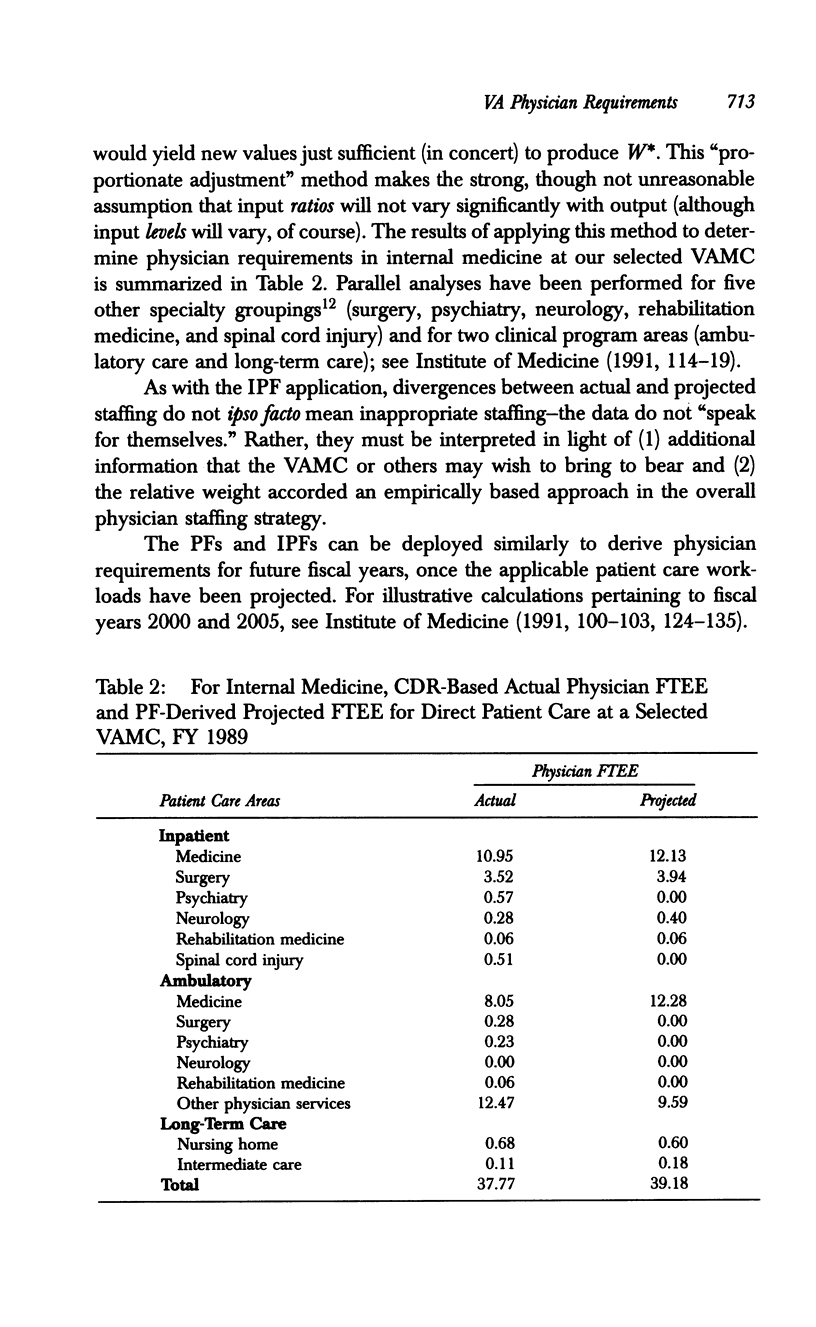
OBJECTIVE: As part of a project to estimate physician requirements for the Department of Veterans Affairs, the Institute of Medicine (IOM) developed and tested empirically based models of physician staffing, by specialty, that could be applied to each VA facility. DATA SOURCE/STUDY SETTING. These analyses used selected data on all patient encounters and all facilities in VA's management information systems for FY 1989. STUDY DESIGN. Production functions (PFs), with patient workload dependent on physicians, other providers, and nonpersonnel factors, were estimated for each of 14 patient care areas in a VA medical center. Inverse production functions (IPFs), with physician staffing levels dependent on workload and other factors, were estimated for each of 11 specialty groupings. These models provide complementary approaches to deriving VA physician requirements for patient care and medical education. DATA COLLECTION/EXTRACTION METHODS. All data were assembled by VA and put in analyzable SAS data sets containing FY 1989 workload and staffing variables used in the PFs and IPFs. All statistical analyses reported here were conducted by the IOM. PRINCIPAL FINDINGS. Existing VA data can be used to develop statistically strong, clinically plausible, empirically based models for calculating physician requirements, by specialty. These models can (1) compare current physician staffing in a given setting with systemwide norms and (2) yield estimates of future staffing requirements conditional on future workload. CONCLUSIONS. Empirically based models can play an important role in determining VA physician staffing requirements. VA should test, evaluate, and revise these models on an ongoing basis.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Feil E. C., Welch H. G., Fisher E. S. Why estimates of physician supply and requirements disagree. JAMA. 1993 May 26;269(20):2659–2663. [PubMed] [Google Scholar]
- Jensen G. A., Morrisey M. A. Medical staff specialty mix and hospital production. J Health Econ. 1986 Sep;5(3):253–276. doi: 10.1016/0167-6296(86)90017-2. [DOI] [PubMed] [Google Scholar]
- Sexton T. R., Leiken A. M., Nolan A. H., Liss S., Hogan A., Silkman R. H. Evaluating managerial efficiency of Veterans Administration medical centers using Data Envelopment Analysis. Med Care. 1989 Dec;27(12):1175–1188. doi: 10.1097/00005650-198912000-00009. [DOI] [PubMed] [Google Scholar]
- Stefos T., LaVallee N., Holden F. Fairness in prospective payment: a clustering approach. Health Serv Res. 1992 Jun;27(2):239–261. [PMC free article] [PubMed] [Google Scholar]