

Abstract
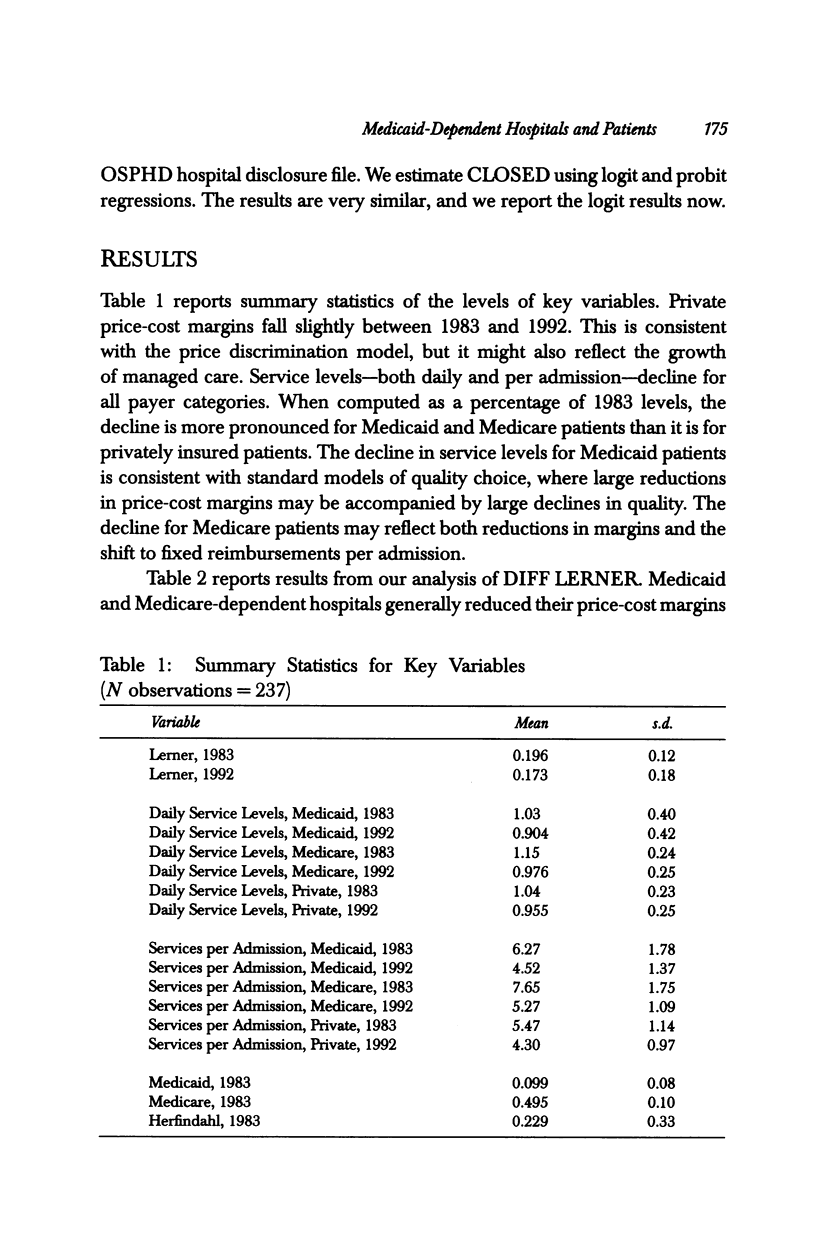
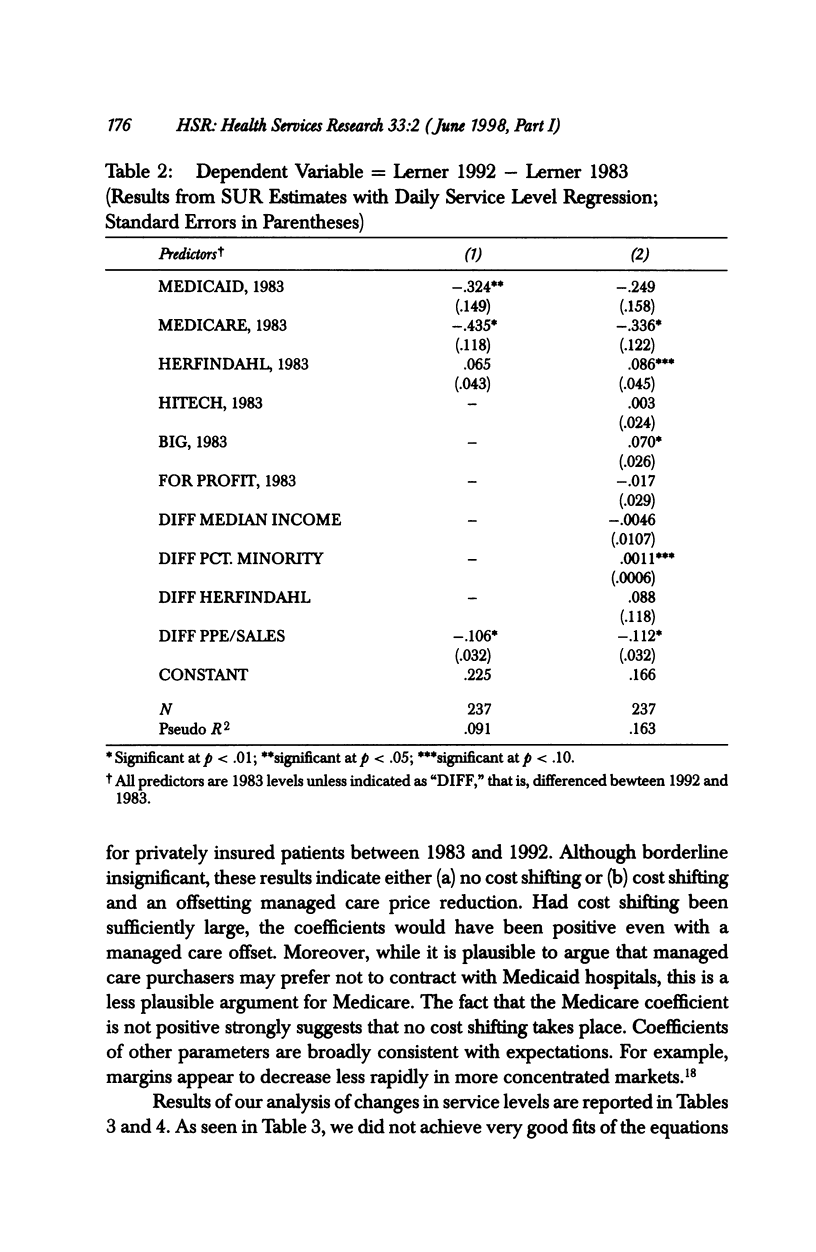
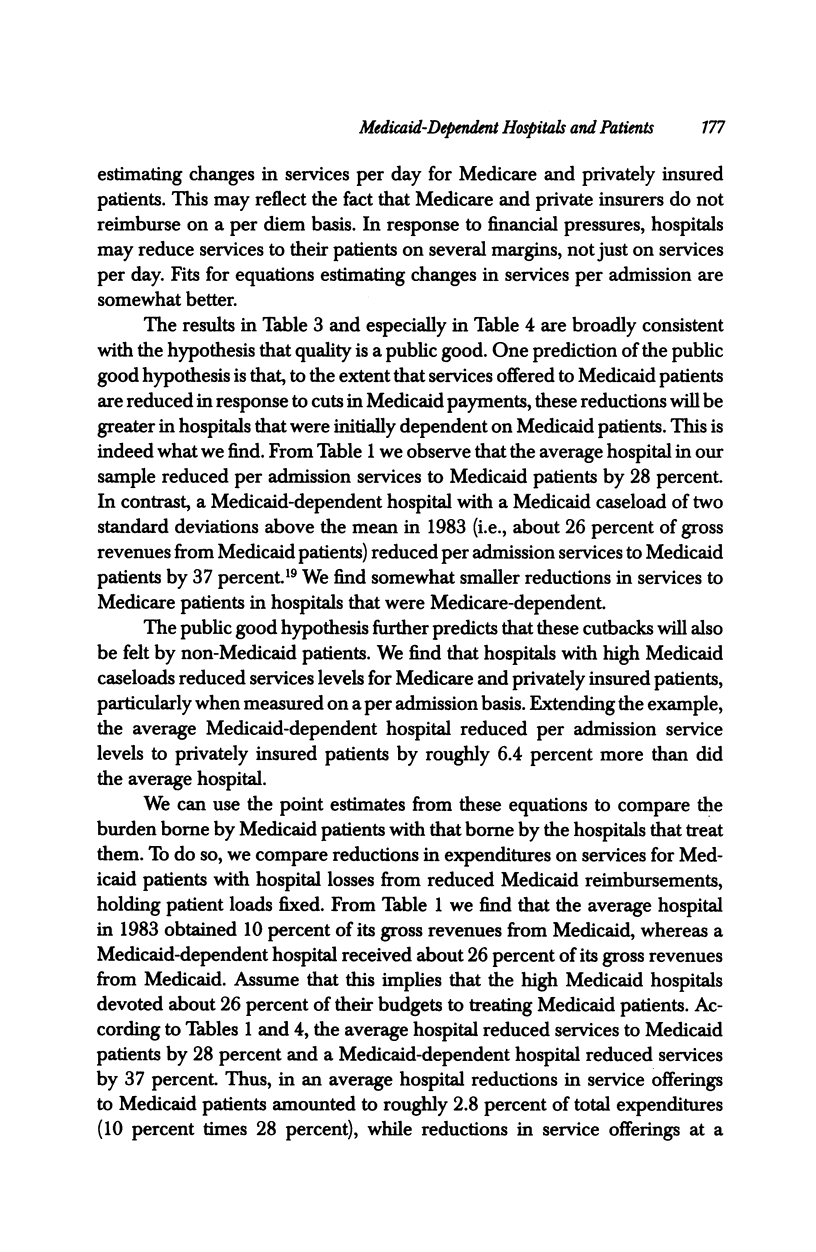
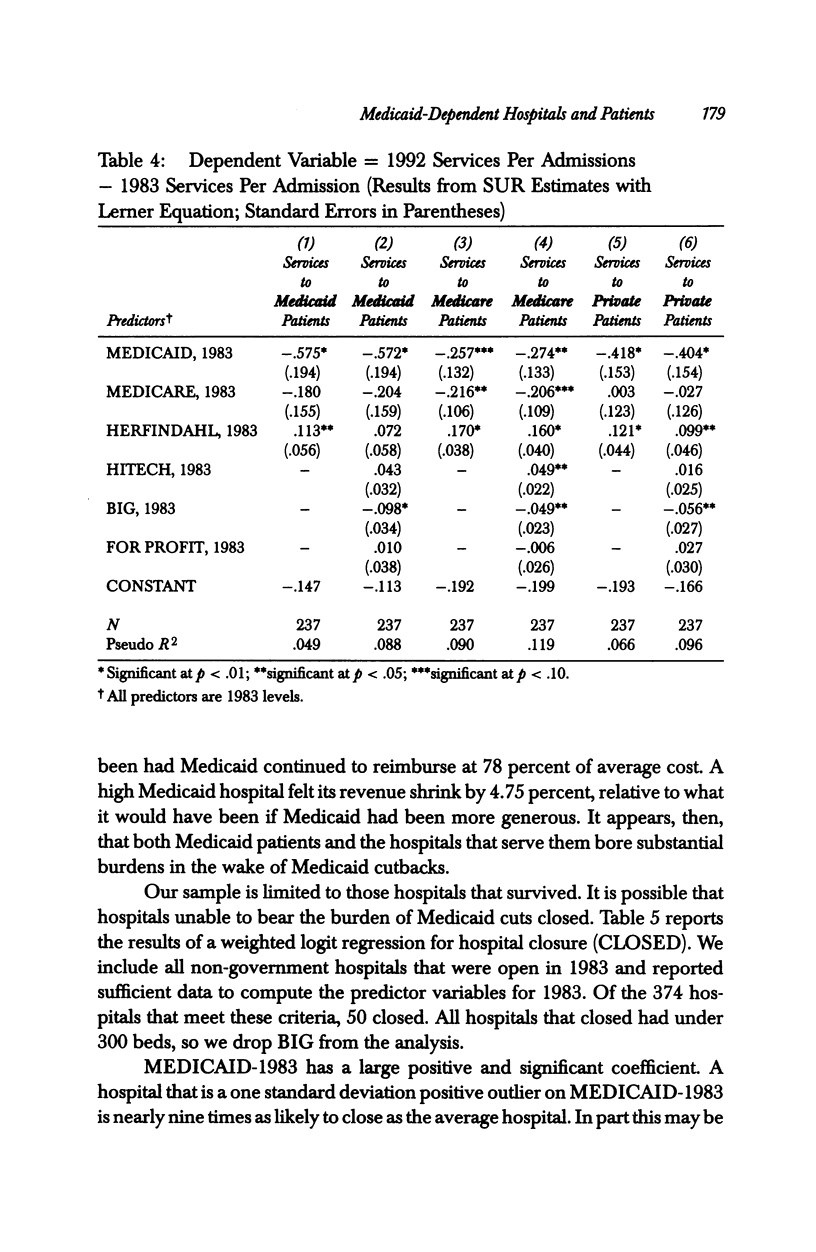
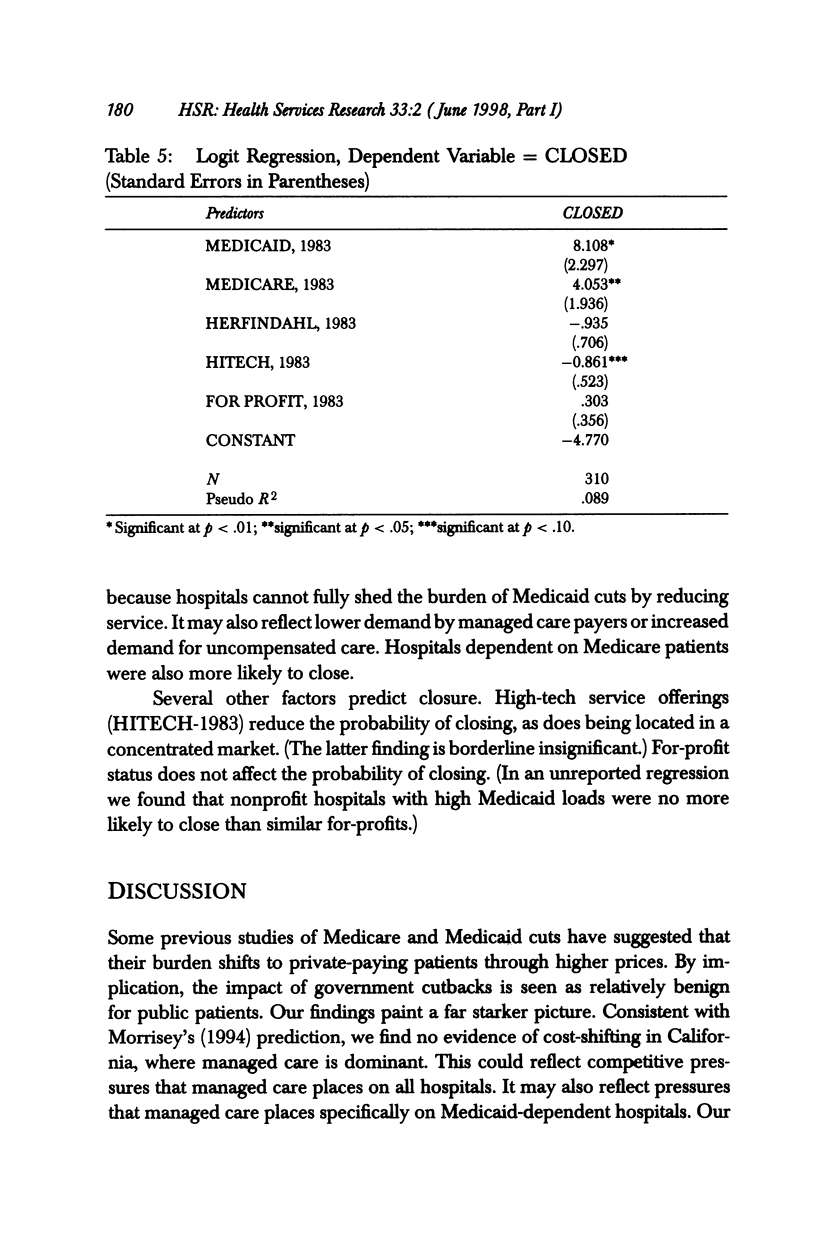
OBJECTIVE: To examine how private hospitals dependent on Medicaid for a large proportion of their revenues have fared in the face of substantial Medicaid (and more modest Medicare) reimbursement cutbacks and growing managed care. We specifically test three hypotheses regarding Medicaid-dependent hospitals: (1) that they are more likely to "cost-shift" cutbacks to private patients; (2) that they are more likely to cut services for Medicaid (and other) patients; and (3) that they are more likely to close. DATA/STUDY SETTING: Private short-term hospitals in California a state that has experienced a rapid growth in managed care since the early 1980s. Data are drawn from the California Office of Statewide Health Planning and Development (OSHPD) Hospital Disclosure Files for fiscal years 1983 and 1992. STUDY DESIGN: We compare changes in net prices and the provision of services, proxied by list price-adjusted charges, at hospitals for Medicaid, Medicare, and privately insured patients between fiscal years 1983 and 1992 controlling for hospital and market characteristics, case mix, and the proportion of revenues from Medicaid patients. We also examine the probability that a hospital closed during the study period as a function of hospital and market characteristics and payer mix. Although the growth of managed care is hypothesized to reduce opportunities for "cost shifting," it may also confound our analysis of price changes if Medicaid-dependent hospitals are unattractive to managed care patients and respond by offering lower prices to plans. PRINCIPAL FINDINGS: We find no evidence that Medicaid-dependent hospitals raised prices to private patients in response to Medicaid (or Medicare) cutbacks; if anything, they lowered them. However, we find that service levels fell for Medicaid (and Medicare) patients relative to those for privately insured patients and that reductions were greater at Medicaid-dependent hospitals. In addition, our findings suggest that service levels also fell for private patients at Medicaid-dependent hospitals, although reductions were smaller for these patients, suggesting that quality, may be a public good at hospitals. Finally, Medicaid-dependent hospitals were more likely to close. CONCLUSIONS: It been suggested that private hospitals may respond to public reimbursement cutbacks by simply "shifting" costs to privately insured patients, limiting overall cost savings but insulating public patients and hospitals from the effects of cutbacks. We find no evidence of cost shifting. Rather, our results suggest that patients and hospitals bore the brunt of cutbacks; service levels fell at Medicaid-dependent hospitals and such hospitals were more likely to go out of business. This suggests that the consequences of proposed Medicare and Medicaid cutbacks could be severe for public patients and the hospitals that care for them.
Full text
PDF





Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Dranove D. Pricing by non-profit institutions. The case of hospital cost-shifting. J Health Econ. 1988 Mar;7(1):47–57. doi: 10.1016/0167-6296(88)90004-5. [DOI] [PubMed] [Google Scholar]
- Dranove D., White W. D., Wu L. Segmentation in local hospital markets. Med Care. 1993 Jan;31(1):52–64. doi: 10.1097/00005650-199301000-00004. [DOI] [PubMed] [Google Scholar]
- Holahan J. The impact of alternative hospital payment systems on Medicaid costs. Inquiry. 1988 Winter;25(4):517–532. [PubMed] [Google Scholar]
- Langa K. M., Sussman E. J. The effect of cost-containment policies on rates of coronary revascularization in California. N Engl J Med. 1993 Dec 9;329(24):1784–1789. doi: 10.1056/NEJM199312093292407. [DOI] [PubMed] [Google Scholar]
- Pauly M. V. Nonprofit firms in medical markets. Am Econ Rev. 1987 May;77(2):257–262. [PubMed] [Google Scholar]
- Zwanziger J., Melnick G. A. The effects of hospital competition and the Medicare PPS program on hospital cost behavior in California. J Health Econ. 1988 Dec;7(4):301–320. doi: 10.1016/0167-6296(88)90018-5. [DOI] [PubMed] [Google Scholar]