

Abstract
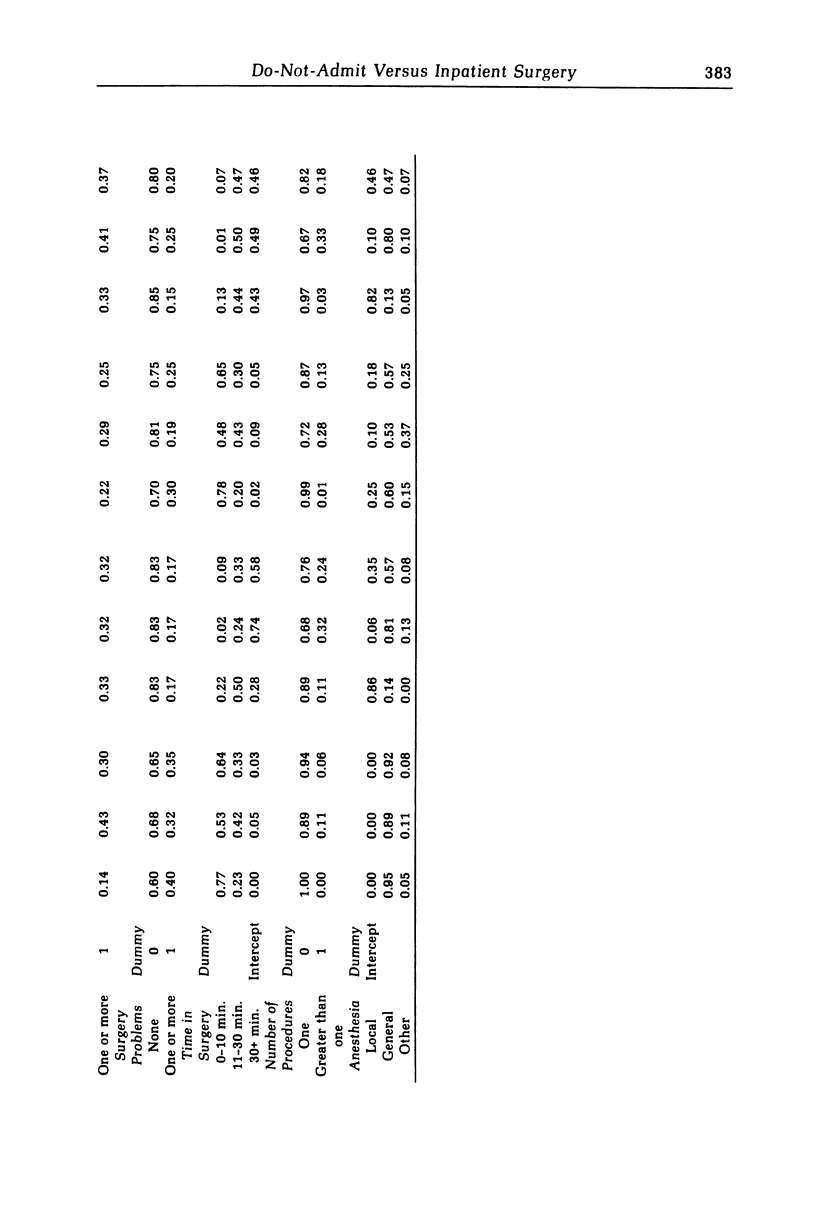
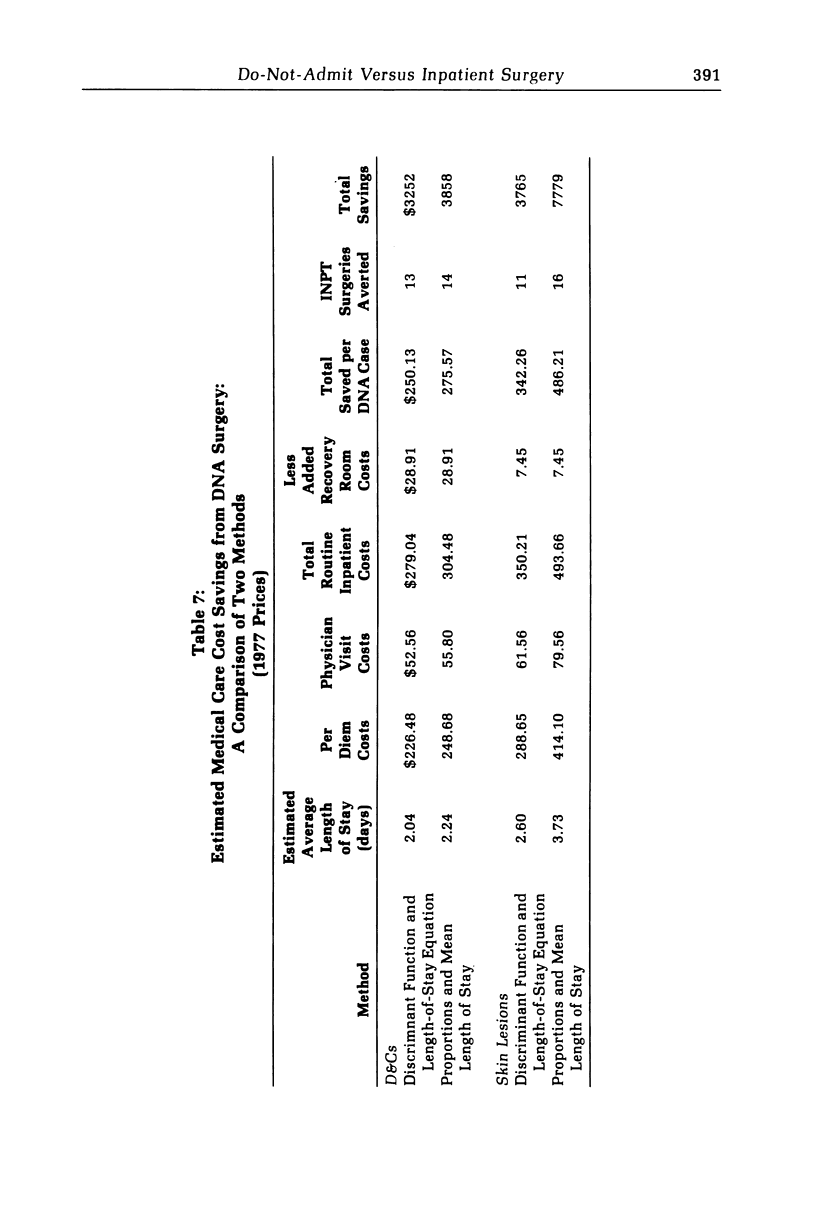
We develop a model for investigating the implications of policies that have encouraged a shift from inpatient to do-not-admit (DNA) surgery. We use discriminant function analysis on date for two surgical procedures from the Kaiser Permanente Medical Care Program of Portland, Oregon. Case attributes found to be significantly associated with the choice of surgery mode are surgeons' rate of inpatient surgery, number of chronic conditions per patient, time in surgery, number of procedures performed, and type of anesthesia used. Our estimates of cost savings provide support on economic grounds for the use of DNA surgery, for the types of surgery investigated. Our results also suggest that simple evaluation methods, based on the mean length of stay and on extrapolation of proportion of DNA cases from the base year to the current year, may overestimate the cost savings derived from the shift to DNA surgery.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Beyers C. K. Surgicenter tells plans for 5th, 6th freestanding surgery clinics. Mod Healthc (Short Term Care) 1976 Sep;6(3):49–49. [PubMed] [Google Scholar]
- Greenlick M. R., Hurtado A. V., Pope C. R., Saward E. W., Yoshioka S. S. Determinants of medical care utilization. Health Serv Res. 1968 Winter;3(4):296–315. [PMC free article] [PubMed] [Google Scholar]
- Marks S. D., Greenlick M. R., Hurtado A. V., Johnson J. D., Henderson J. Ambulatory surgery in an HMO. A study of costs, quality of care and satisfaction. Med Care. 1980 Feb;18(2):127–146. doi: 10.1097/00005650-198002000-00001. [DOI] [PubMed] [Google Scholar]
- Reed W. A., Ford J. L. Development of an independent outpatient surgical center. Int Anesthesiol Clin. 1976 Summer;14(2):113–130. doi: 10.1097/00004311-197614020-00007. [DOI] [PubMed] [Google Scholar]