

Elderly or unfit patients with relapsed acute myeloid leukemia (AML) are frequently unable to undergo intensive chemotherapy and allogeneic stem cell transplantation, the only curative treatment approach for this entity. They often rapidly exhaust the few approved and reimbursable (registered) treatment options for AML at relapse, thus facing a poor prognosis.1,2 The situation is aggravated by the rapidly progressive nature of the disease, severely restricting the time frame for therapy selection.3 Recent studies have demonstrated the effectiveness of pharmacoscopy - an image-based ex vivo functional drug testing platform - to provide guidance when selecting therapies for hematological malignancies lacking standard treatment protocols.4–7 However, no previous study has focused exclusively on AML patients that have exhausted all registered therapeutic options. Furthermore, the issue of obtaining financial coverage for such therapy plans remains unaddressed. We aimed to establish whether pharmacoscopy can be employed for therapy selection in AML patients that have exhausted the registered treatment options. We evaluated whether such therapies can be made available within a suitable time frame and adequate financial coverage and whether they provide a clinical benefit in heavily pretreated and frail patients. In our prospective, non-randomized, single-center observational study (DARTT-1; clinicaltrials gov. Identifier: NCT05732688; BASEC-ID: 2021-01294, Department of Medical Oncology, University Hospital Bern, Switzerland), we enrolled and screened 24 adult AML patients at relapse who had exhausted all registered treatment options. Of those, five patients were screened at least a second time after relapsing. In total, 30 screening events with subsequent treatment and follow-up from 24 patients were included in our intention-to-treat population. We successfully collected sufficient samples for subsequent drug screening from all intended patients, of which 14 were from bone marrow origin, 14 from peripheral blood, and two from skin tissue. Excluded were patients who had not undergone previous treatment or still had registered therapy options available. All participants signed informed consent, and the study was executed in accordance with good clinical practice and approved by the relevant review boards and regulatory agencies. The 24 patients were pretreated with a median of two previous treatment lines (interquartile range (IQR), 1-3). The median patient age was 68.5 years (IQR, 66-73). The sex distribution was 62.5% male versus 37.5% female. According to the European LeukemiaNet (ELN) risk category,1 12.5% of the patients were classified as favorable, 37.5% as intermediate, and 50.0% as adverse. Further demographics are listed in Table 1. For statistical analyses, each screening event was treated as a separate data point. The complete drug screening results used in this study, including more detailed patient information, prior lines of treatments, and other relevant clinical parameters, as well as more detailed descriptions of the methodologies and statistical approaches employed in this study, are available at https:// www.snijderlab.org/trials/DARTT-1/.
For each patient and screening event, we performed pharmacoscopy using real-time patient-derived leukemic samples to generate treatment recommendations (Figure 1), as previously described.4–6 The results of the drug screen were communicated in the form of a short list of drugs recommended for the treatment of the respective patient (pharmacoscopy report). If the compounds in these reports could not be made available within a reasonable time frame and adequate financial coverage, patients were provided with a therapy based on in-house guidelines. Mandatory health insurance in Switzerland reimburses pharmaceuticals if they are on the national list of reimbursable specialties. Other drugs may be reimbursed upon reasoned request if they are expected to have a substantial effect against a serious illness for which no other approved treatment is available.8 Patients were provided with best supportive care if they could not undergo further treatment attempts. Online Supplementary Table S1 lists a summary of ex vivo drug screening results, waiting times, and characteristics of treatment choice. The median waiting time for screening results was 5.0 days (IQR, 4.0-6.0). The pharmacoscopy reports listed a median of 5.5 drugs per patient (IQR, 4.3-8.8), ranked by their predicted efficacy. In 17 (56.7%) instances, the patient received one of the recommended therapy options, while no recommended drug was administered in 13 (43.3%) instances. Nine screening instances (30.0%) resulted in patients receiving an AML-specific therapy not listed in the pharmacoscopy reports. Four patients were switched to best supportive care due to their deteriorating condition or refusal of further therapy. The duration from receiving the drug recommendations to starting a new therapy was a median of 11 days (IQR, 6-24). The top six most frequently recommended drugs were navitoclax, venetoclax, omacetaxine, cladribine, carfilzomib, and panobinostat. Whereas omacetaxine and panobinostat were never administered to patients in the study due to the difficulty of obtaining financial coverage, venetoclax was the most frequently administered drug.
In order to monitor response and outcome, we used clinical assessments, as well as blood and bone marrow testing during routine follow-ups. Our primary endpoints were how frequently pharmacoscopy derived treatments could be started, the frequency of patients realizing a complete remission (CR) in the bone marrow, overall survival (OS), and event-free survival (EFS). We assessed these endpoints by comparing patients who received a therapy recommended by pharmacoscopy versus patients receiving a therapy based on in-house guidelines. In order to compare different treatment regimens (pharmacoscopy based vs. in-house guidelines) in terms of their performance during the drug screen, we calculated the integrated peritoneal cancer index (i-PCY) score of each regimen. The i-PCY score is a previously established score calculated during pharmacoscopy and indicates a treatment regimen’s capacity to selectively eliminate leukemic blasts from a patient-derived sample.4 We divided patients into two groups based on their therapy regimen’s i-PCY score (above or below the median of the study population) and separately assessed the frequency of CR, OS, and EFS. Neither of our stratification strategies differed significantly in patient characteristics or tissue origin of the sample (Online Supplementary Table S2). The response to the chosen therapy regimen in the bone marrow could be assessed for 25 screening instances (Online Supplementary Table S3). We found that a significantly higher percentage (45.5% vs. 21.4%) of patients receiving a drug combination with an i-PCY score above the median of the study population (i.e., a regimen that performed exceptionally well during the respective drug screen) achieved a CR than patients receiving a regimen with a lower i-PCY score (odds ratio [OR] =3.078; P=0.0005). Conversely, patients that achieved a complete remission tended to receive treatment regimens with a higher i-PCY score (mean 0.278) than patients that did not achieve a CR (mean 0.155). When comparing patients receiving a pharmacoscopy-recommended therapy with patients receiving a regimen-based on in-house guidelines, the difference in the relative number of complete responders was 35.3% versus 25.0% (OR=1.615; P=0.1646).
Table 1.
Summary of study group.
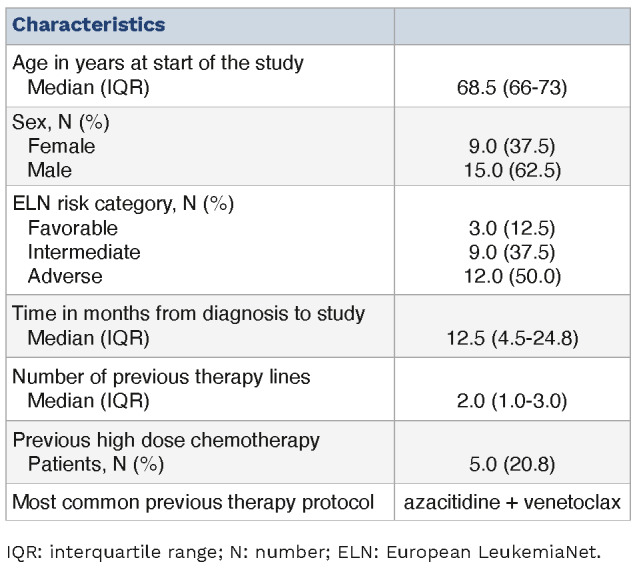
Figure 1.

Pharmacoscopy workflow for acute myeloid leukemia at relapse. Patient samples (bone marrow draws, peripheral blood, or subcutaneous/skin samples) were shipped by courier to the pharmacoscopy laboratory. There, the cells from the samples were processed by either density centrifugation (blood and bone marrow) or tissue dissociation (skin) and seeded into 384-well imaging plates, with each well containing a chemo- or immunotherapeutic compound from our test library. The plates were then incubated overnight. Immunofluorescence stainings against specific surface antigen characteristics of the patient’s leukemic cells were used to distinguish between healthy cells and malignant blasts. The cells were then subjected to automated confocal microscopy (Opera Phenix, Perkin Elmer) and image analysis using nuclear morphology to quantify the viability of malignant and healthy cells, respectively. Based on this readout, the ex vivo blast reduction capacity (peritoneal cancer index [PCY] score) was calculated for each compound. Pharmacoscopy reports were provided to the treating oncologists in the form of a short list of top-scoring drugs ranked by their predicted efficacy, as well as complete drug response profiles. The selection of treatment regimens was subsequently based on the pharmacoscopy report and the availability of compounds listed therein. If none of the listed compounds could be made available within a reasonable time frame, therapy regimens were chosen based on previously established in-house guidelines at our department.
Figure 2.

Patients outcome. (A) Kaplan-Meier estimates of overall survival (OS) in the intention-to-treat population stratified by whether patients received a pharmacoscopy-derived treatment regimen (17 screening instances) or a regimen based on in-house guidelines (13 screening instances). (B) Kaplan-Meier estimates of event-free survival (EFS) in the intention-to-treat population stratified by whether patients received a pharmacoscopy-derived treatment regimen or not (17 vs. 13 screening instances). (C) Kaplan-Meier estimates of OS in the intention-to-treat population stratified by the ex vivo blast reduction capacity of their respective treatment regimen (integrated peritoneal cancer index [i-PCY] score) (14 screening instances with above median i-PCY score and 16 below). (D) Kaplan-Meier estimates of EFS in the intention-to-treat population stratified by the i-PCY score of their respective treatment regimen (14 vs. 16 screening instances). (E) Kaplan-Meier estimates of OS in patients receiving an acute myeloid leukemia (AML)-specific therapy (excluding patients receiving best supportive care) stratified by the i-PCY score of their respective treatment regimen (12 screening instances with above median i-PCY score and 14 below). (F) Kaplan-Meier estimates of EFS in patients receiving an AML-specific therapy stratified by the i-PCY score of their respective treatment regimen (12 vs. 14 screening instances). All P values were calculated by Gehan-Breslow-Wilcoxon test. CI: confidence interval; NS: not significant.
We next evaluated EFS and OS using standard outcome definitions in AML.1 Patients receiving a pharmacoscopy recommended therapy had a median OS of 18.0 weeks versus 8.0 weeks in patients receiving a regimen based on in-house guidelines (OS ratio =2.250; 95% confidence interval [CI]: 1.021-4.958) (Figure 2A). Median EFS was 11.1 weeks in patients receiving a recommended therapy compared to 6.3 weeks in the rest of the cohort (EFS ratio =1.773; 95% CI: 0.805-3.906) (Figure 2B). When stratifying the intention-to-treat population by i-PCY score of their therapy regimen (i.e., its performance in the drug screen), we found that patients receiving a regimen with an i-PCY score above the median of the study population showed a median OS of 28.6 weeks as opposed to 8.4 weeks for the other half of the cohort (ratio 3.390; 95% CI: 1.506-7.632; P=0.006) (Figure 2C). Median EFS for patients receiving a regimen with an i-PCY score above the median was 12.4 in comparison to 6.4 weeks for the other half of the cohort (EFS ratio =1.933; 95% CI: 0.859-4.353; P= 0.0446) (Figure 2D). The significant effect of a treatment regimen’s i-PCY score on OS and a strong effect on EFS was also present when focusing only on patients receiving an AML-specific therapy (Figure 2E, F).
The inherently poor prognosis of AML patients at relapse is aggravated by the limited availability of registered therapy options at this stage and the rapid progression of the disease. Thus, improving the prognosis of AML patients that have exhausted all registered therapy options remains an unsolved issue.3 We evaluated a novel approach, basing treatment decisions on the recommendations of pharmacoscopy, an automated imaging-based ex vivo drug screening platform. We could demonstrate that integrating pharmacoscopy into the clinical decision-making AML treatment at relapse is technically feasible and appears beneficial to the patients.
The screening procedure is fast, taking a median of only 16 days from sample taking to the start of a new protocol. Thus, clinical decision-making is not significantly delayed, a key concern in AML at relapse.1,3 Financial coverage for pharmacoscopy-derived treatment plans could be obtained for most patients in our cohort (56.7%), and such therapy regimens led to promising trends in response and survival rates. Additionally, we found that the i-PCY score of a treatment regimen (i.e., its performance during the drug screen) is an excellent predictor of response and survival. Patients receiving a therapy regimen with an above-average i-PCY score showed significantly higher rates of CR and significantly longer OS than the rest of the cohort. Thus the i-PCY score can be a useful cue to prioritize between readily available standard therapy options even when the highest-scoring compounds in the screen prove unavailable. Previous studies have evaluated integrating ex vivo drug screening into therapy selection for AML patients.4,5,7 However, direct comparisons with these studies are inherently complex, given that previous research either adopted an observational approach,9 employed different inclusion criteria (e.g., including patients for whom standard treatment options were still viable4,5,7), or lacked control groups.7 To the best of our understanding, this is the first research effort concentrating solely on patients who have exhausted all registered treatment methodologies while including a control group consisting of patients for whom pharmacoscopy-guided treatment was not feasible. Additionally, our investigation is the inaugural one to address the crucial clinical issue of securing cost coverage for AML treatment protocols chosen via drug screening.
The major limitation of our study resides in the absence of patient randomization into distinct treatment groups. Nevertheless, significant stratification of the intention-to-treat population, based on the ex vivo blast reduction capacity, signals potential for future randomized trials. In such studies, patients could be divided into an intervention group, which would receive a treatment regimen optimized by a summed RBF, and a control group, which would adhere to either physician-chosen treatments or treatments grounded in established guidelines. We conclude that pharmacoscopy can rapidly provide valuable decision-making cues for therapy selection in late-stage AML patients, helping to choose between established therapies and to design novel treatment plans. We, therefore, suggest that it may standardly be employed to provide patients with optimized treatment plans.
Supplementary Material
References
- 1.Döhner H, Estey EH, Amadori S, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010;115(3):453-474. [DOI] [PubMed] [Google Scholar]
- 2.Laribi K, Sobh M, Ghez D, Baugier de Materre A. Impact of age, functional status, and comorbidities on quality of life and outcomes in elderly patients with AML: review. Ann Hematol. 2021;100(6):1359-1376. [DOI] [PubMed] [Google Scholar]
- 3.Webster JA, Luznik L, Gojo I. Treatment of AML relapse after allo-HCT. Front Oncol. 2021;11:812207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Snijder B, Vladimer GI, Krall N, et al. Image-based ex-vivo drug screening for patients with aggressive haematological malignancies: interim results from a single-arm, open-label, pilot study. Lancet Haematol. 2017;4(12):e595-e606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kornauth C, Pemovska T, Vladimer GI, et al. Functional precision medicine provides clinical benefit in advanced aggressive hematologic cancers and identifies exceptional responders. Cancer Discov. 2022;12(2):372-387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Heinemann T, Kornauth C, Severin Y, et al. Deep morphology learning enhances ex vivo drug profiling-based precision medicine. Blood Cancer Discov. 2022;3(6):502-515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Malani D, Kumar A, Brück O, et al. Implementing a functional precision medicine tumor board for acute myeloid leukemia. Cancer Discov. 2022;12(2):388-401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.De Pietro C, Camenzind P, Sturny I, et al. Switzerland: health system review. Health Syst Transit. 2015;17(4):1-288, xix. [PubMed] [Google Scholar]
- 9.Kuusanmäki H, Kytölä S, Vänttinen I, et al. Ex vivo venetoclax sensitivity testing predicts treatment response in acute myeloid leukemia. Haematologica. 2023;108(7):1768-1781. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.