

Key Points
Question
Is anticoagulation superior to antiplatelet therapy for prevention of recurrent stroke in patients with cryptogenic stroke and evidence of atrial cardiopathy?
Findings
In this randomized clinical trial that included 1015 patients, the rate of recurrent stroke did not significantly differ between the apixaban group (annualized rate, 4.4%) and the aspirin group (annualized rate, 4.4%).
Meaning
In patients with cryptogenic stroke and evidence of atrial cardiopathy without atrial fibrillation, apixaban did not significantly reduce recurrent stroke risk compared with aspirin.
Abstract
Importance
Atrial cardiopathy is associated with stroke in the absence of clinically apparent atrial fibrillation. It is unknown whether anticoagulation, which has proven benefit in atrial fibrillation, prevents stroke in patients with atrial cardiopathy and no atrial fibrillation.
Objective
To compare anticoagulation vs antiplatelet therapy for secondary stroke prevention in patients with cryptogenic stroke and evidence of atrial cardiopathy.
Design, Setting, and Participants
Multicenter, double-blind, phase 3 randomized clinical trial of 1015 participants with cryptogenic stroke and evidence of atrial cardiopathy, defined as P-wave terminal force greater than 5000 μV × ms in electrocardiogram lead V1, serum N-terminal pro-B-type natriuretic peptide level greater than 250 pg/mL, or left atrial diameter index of 3 cm/m2 or greater on echocardiogram. Participants had no evidence of atrial fibrillation at the time of randomization. Enrollment and follow-up occurred from February 1, 2018, through February 28, 2023, at 185 sites in the National Institutes of Health StrokeNet and the Canadian Stroke Consortium.
Interventions
Apixaban, 5 mg or 2.5 mg, twice daily (n = 507) vs aspirin, 81 mg, once daily (n = 508).
Main Outcomes and Measures
The primary efficacy outcome in a time-to-event analysis was recurrent stroke. All participants, including those diagnosed with atrial fibrillation after randomization, were analyzed according to the groups to which they were randomized. The primary safety outcomes were symptomatic intracranial hemorrhage and other major hemorrhage.
Results
With 1015 of the target 1100 participants enrolled and mean follow-up of 1.8 years, the trial was stopped for futility after a planned interim analysis. The mean (SD) age of participants was 68.0 (11.0) years, 54.3% were female, and 87.5% completed the full duration of follow-up. Recurrent stroke occurred in 40 patients in the apixaban group (annualized rate, 4.4%) and 40 patients in the aspirin group (annualized rate, 4.4%) (hazard ratio, 1.00 [95% CI, 0.64-1.55]). Symptomatic intracranial hemorrhage occurred in 0 patients taking apixaban and 7 patients taking aspirin (annualized rate, 1.1%). Other major hemorrhages occurred in 5 patients taking apixaban (annualized rate, 0.7%) and 5 patients taking aspirin (annualized rate, 0.8%) (hazard ratio, 1.02 [95% CI, 0.29-3.52]).
Conclusions and Relevance
In patients with cryptogenic stroke and evidence of atrial cardiopathy without atrial fibrillation, apixaban did not significantly reduce recurrent stroke risk compared with aspirin.
Trial Registration
ClinicalTrials.gov Identifier: NCT03192215
This clinical trial compares the effectiveness of anticoagulation vs antiplatelet therapy for secondary stroke prevention in patients with cryptogenic stroke and evidence of atrial cardiopathy.
Introduction
Atrial cardiopathy is defined as any complex of structural, architectural, contractile, or electrophysiologic changes affecting the atria with the potential to produce clinically relevant manifestations.1 Atrial cardiopathy is strongly associated with incident atrial fibrillation and plays a role in thromboembolism related to atrial fibrillation.2 Various markers of atrial cardiopathy are associated with the risk of ischemic stroke even in the absence of clinically apparent atrial fibrillation.3 Unrecognized atrial cardiopathy may explain some of the many ischemic strokes that are classified as cryptogenic (ie, strokes that lack an identifiable etiology after standard diagnostic evaluation).4 Given the proven role of anticoagulation in atrial fibrillation and the interrelationship between atrial fibrillation and atrial cardiopathy, anticoagulation may also reduce the risk of stroke in patients with atrial cardiopathy and no clinically apparent atrial fibrillation. The Atrial Cardiopathy and Antithrombotic Drugs in Prevention After Cryptogenic Stroke (ARCADIA) trial was designed to test the hypothesis that anticoagulation is superior to antiplatelet therapy for preventing recurrent stroke in patients with a recent cryptogenic stroke and evidence of atrial cardiopathy.
Methods
Design
ARCADIA was a multicenter, randomized, double-blind trial of apixaban vs aspirin in patients with a recent cryptogenic stroke and evidence of atrial cardiopathy. The rationale and methods of the trial have been previously published (the trial protocol and statistical analysis plan are in Supplement 1).5 The trial was initiated by the investigators and conducted jointly with the National Institutes of Health (NIH) StrokeNet National Coordinating Center at the University of Cincinnati, the StrokeNet National Data Management Center at the Medical University of South Carolina, and a Canadian coordinating center at the Population Health Research Institute. Patients were recruited at 185 sites in StrokeNet and the Canadian Stroke Consortium. The US Food and Drug Administration granted the trial an Investigational New Drug application exemption. Health Canada, the StrokeNet Central Institutional Review Board, and institutional review boards or research ethics boards at participating sites approved the study protocol. All participants provided written, informed consent for trial participation. An NIH-appointed data and safety monitoring board (DSMB) monitored the conduct of the trial.
Patient Population
Major inclusion criteria were age 45 years or older, a clinical diagnosis of cryptogenic ischemic stroke, brain imaging to rule out hemorrhagic stroke, a modified Rankin Scale score of 4 or less, and the ability to be randomized no later than 180 days after stroke onset (Table 1). Because the term cryptogenic stroke can also be applied to cases with multiple potential etiologies and cases with an incomplete diagnostic evaluation, we used consensus criteria for an embolic stroke of undetermined source6 to establish a rigorous diagnosis of cryptogenic stroke that included only cases without any apparent etiology after standard investigation. Thus, our criteria for cryptogenic stroke required computed tomography or magnetic resonance imaging of the brain to exclude lacunar infarcts, vascular imaging of the cervical and intracranial arteries to exclude large-artery atherosclerosis causing 50% or more stenosis of a relevant arterial lumen, and transthoracic or transesophageal echocardiography, a 12-lead electrocardiogram (ECG), and 24 hours or more of continuous heart rhythm monitoring to exclude major-risk cardioembolic sources. Additional heart rhythm monitoring to detect atrial fibrillation was allowed at the discretion of treating physicians and local investigators, both before and after randomization. Key exclusion criteria were a major-risk cardioembolic source including any history of atrial fibrillation or a left ventricular ejection fraction less than 30%, a definite indication or contraindication to antiplatelet or anticoagulant therapy, a history of spontaneous intracranial hemorrhage, chronic kidney disease with serum creatinine level of 2.5 mg/dL or greater, or a clinically significant bleeding diathesis. The complete list of inclusion and exclusion criteria are provided in the trial protocol (Supplement 1). To ensure the representativeness of the trial population, site investigators and coordinators were instructed to directly ask participants to report their self-identified race and ethnicity, which were then categorized per NIH guidelines. The Other race category was defined as American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, or more than 1 race.
Table 1. Characteristics of Patients at Baseline in the ARCADIA Triala.
| Characteristic | Group, No. (%) | |
|---|---|---|
| Apixaban (n = 507) | Aspirin (n = 508) | |
| Age, mean (SD), y | 67.8 (10.8) | 68.2 (11.0) |
| Sex | ||
| Female | 272 (53.7) | 279 (54.9) |
| Male | 235 (46.3) | 229 (45.1) |
| Raceb | n = 501 | n = 500 |
| Asian | 7 (1.4) | 10 (2.0) |
| Black or African American | 107 (21.4) | 107 (21.4) |
| White | 381 (76.0) | 379 (75.8) |
| Other | 6 (1.2) | 4 (0.8) |
| Ethnicityb | n = 505 | n = 505 |
| Hispanic or Latino | 43 (8.5) | 39 (7.7) |
| Not Hispanic or Latino | 462 (91.5) | 466 (92.3) |
| Weight, mean (SD), kg | 85.1 (20.1) | 84.5 (20.2) [n = 506] |
| Documented medical comorbiditiesc | ||
| Hypertension | 396 (78.1) | 388 (76.4) |
| Prior or current tobacco use | 230 (45.4) | 200 (39.4) |
| Diabetes | 156 (30.8) | 159 (31.3) |
| Prior stroke or TIA | 97 (19.1) | 100 (19.7) |
| Ischemic heart disease | 58 (11.4) | 46 (9.1) |
| Heart failure | 36 (7.1) | 35 (6.9) |
| Peripheral arterial disease | 12 (2.4) | 7 (1.4) |
| CHA2DS2-VASc score, mean (SD)d | 4.7 (1.3) | 4.7 (1.3) |
| NIH Stroke Scale score, median (IQR)e | 1 (0-3) [n = 504] | 1 (0-3) [n = 506] |
| Atrial cardiopathy biomarkers | ||
| NT-proBNP, median (IQR), pg/mL | 288 (87-535) [n = 502] | 318 (130-551) [n = 496] |
| PTFV1, mean (SD), μV × ms | 4716 (2515) [n = 501] | 4766 (2920) [n = 503] |
| LA diameter index, mean (SD), cm/m2 | 1.9 (0.5) [n = 406] | 1.9 (0.5) [n = 412] |
| Days from index stroke to randomization, median (IQR) | 48 (21-96) | 53 (23-100) |
Abbreviations: ARCADIA, Atrial Cardiopathy and Antithrombotic Drugs in Prevention After Cryptogenic Stroke; CHA2DS2-VASc, congestive heart failure, hypertension, age ≥75 years (doubled), diabetes, stroke/transient ischemic attack/thromboembolism (doubled), vascular disease (prior myocardial infarction, peripheral artery disease, or aortic plaque), age 65-75 years, sex category (female); LA, left atrial; NIH, National Institutes of Health; NT-proBNP, N-terminal pro-B-type natriuretic peptide; PTFV1, P-wave terminal force in lead V1; TIA, transient ischemic attack.
Percentages may not total 100 because of rounding.
Other race was defined as Alaska Native or American Indian, Native Hawaiian or Other Pacific Islander, or more than 1. Site investigators and coordinators were instructed to ask participants to report self-identified race and ethnicity, which were then categorized per NIH guidelines.
Determined by site investigators and coordinators based on the medical record and patient self-report.
This score assigns 2 points each for age 75 years or older, prior stroke, or transient ischemic attack and 1 point each for hypertension, diabetes, peripheral vascular disease, age 65 to 74 years, or female sex. This score has been shown to have moderate predictive value for thromboembolism in atrial fibrillation. The score ranges from 0-9 and higher scores indicate a higher risk of thromboembolism.
The NIH Stroke Scale, a standardized neurologic examination used to quantify the degree of functional deficit resulting from a stroke, ranges from 0-42, with higher scores indicating a greater degree of neurologic impairment.
Screening and Randomization
Patients who met the eligibility criteria and provided consent underwent screening for atrial cardiopathy (Figure 1), defined as at least 1 of the following biomarkers: P-wave terminal force in ECG lead V1 greater than 5000 μV × ms, serum N-terminal pro-B-type natriuretic peptide (NT-proBNP) level greater than 250 pg/mL, or left atrial diameter index of 3 cm/m2 or greater on echocardiogram. These biomarkers and thresholds were chosen based on their associations with a 2-fold higher risk of stroke in observational studies.3 The left atrial diameter index was determined by the local echocardiography laboratory at each site. P-wave terminal force was centrally determined at the study ECG core using previously validated methods.7 Serum NT-proBNP was centrally measured in a Clinical Laboratory Improvement Amendments–certified core laboratory using the Elecsys assay (Roche Diagnostics).
Figure 1. Enrollment, Treatment Allocation, and Analysis in the ARCADIA Trial.

ARCADIA indicates Atrial Cardiopathy and Antithrombotic Drugs in Prevention After Cryptogenic Stroke.
aAtrial cardiopathy was defined as at least 1 of the following biomarkers: P-wave terminal force in electrocardiogram lead V1 >5000 μV × ms, serum N-terminal pro-B-type natriuretic peptide level >250 pg/mL, or left atrial diameter index ≥3 cm/m2 on echocardiogram.
bEligible participants were randomly assigned in a 1:1 ratio to apixaban or aspirin using a central randomization system and a method that controlled the treatment imbalance within each StrokeNet Regional Coordinating Center. One patient was incorrectly randomized despite not meeting the atrial cardiopathy biomarker criteria.
Patients who fulfilled any of the atrial cardiopathy criteria and continued to meet the other eligibility criteria were randomly assigned in a 1:1 ratio to apixaban or aspirin using a central randomization system and a method that controlled the treatment imbalance within each StrokeNet Regional Coordinating Center. The big stick design8 was applied to control the treatment imbalance within each regional coordinating center first. If the imbalance within a regional coordinating center did not reach the maximum tolerated imbalance, a block urn design9 was applied to control the overall imbalance. The maximum tolerated imbalances within each regional coordinating center and overall were set to 3. Randomization was generally allowed as early as poststroke day 3 but delayed until at least poststroke day 14 for patients with an initial NIH Stroke Scale score of 11 or greater, hemorrhagic transformation of the index stroke, or uncontrolled hypertension.
Intervention
Participants assigned to apixaban received a standard oral dose of apixaban, 5 mg, twice daily, unless standard criteria were met for dose reduction to 2.5 mg twice daily, and an aspirin placebo once daily. Those assigned to aspirin received an oral dose of 81 mg once daily and an apixaban placebo twice daily. Placebos were identical in appearance to the active drug. Participants diagnosed with atrial fibrillation after randomization crossed over to open-label anticoagulant therapy at the discretion of their treating physicians but were followed up until the end of the trial and were analyzed according to the groups to which they were randomized.
Outcomes
The primary efficacy end point was recurrent stroke of any type (ischemic, hemorrhagic, or undetermined type). The 2 secondary efficacy end points were the composite of recurrent ischemic stroke or systemic embolism and the composite of recurrent stroke of any type or death from any cause.
The 2 primary safety outcomes were symptomatic intracranial hemorrhage, which included symptomatic hemorrhagic transformation of an ischemic stroke, and major hemorrhage other than intracranial hemorrhage. The secondary safety outcome was all-cause mortality.
All primary and secondary end points, except for major hemorrhage, were adjudicated by 2 neurologists blinded to treatment assignment. Major hemorrhage was determined by sites using a standard definition of clinically overt bleeding accompanied by a 2-g/dL or greater decrease in the hemoglobin level during a 24-hour period, transfusion of 2 units or more of whole blood or red blood cells, involvement of a critical nonintracranial site (intraspinal, intraocular, pericardial, intra-articular, intramuscular with compartment syndrome, or retroperitoneal), or death.10
Sample Size Calculation
Key assumptions for sample size estimation included a 3.5% annual risk of recurrent stroke after a cryptogenic stroke, a doubling of that risk to 7% in patients with atrial cardiopathy treated with aspirin, a hazard ratio (HR) of 0.6 for recurrent stroke in patients with atrial cardiopathy treated with apixaban compared with aspirin, a 3% annual rate of crossover to open-label anticoagulation because of detection of atrial fibrillation, and a 3% annual rate of crossover to open-label antiplatelet therapy because of bleeding or other adverse events. The assumed HR of 0.6 was chosen as the minimal clinically important difference given the perceived and real risks of bleeding with anticoagulation over antiplatelet therapy. This HR was also supported by the effect of apixaban over aspirin for stroke prevention in patients with atrial fibrillation11 and pilot data on the potential benefit of anticoagulation in patients with noncardioembolic stroke and evidence of atrial cardiopathy.12 Given these parameters, the trial was estimated to require 1100 participants with 150 primary outcome events to have 80% power at a 2-sided α level of .05. This sample size also incorporated a plan for 1 interim analysis for efficacy and futility after 75 primary outcome events using an O’Brien-Fleming–type Lan-DeMets error spending function with nonbinding futility boundaries of an HR greater than 0.914 and less than 1.095.
Statistical Analysis
Efficacy outcomes among all randomized participants, including those who terminated trial participation early or who crossed over to open-label anticoagulant therapy because of detection of atrial fibrillation after randomization, were analyzed according to the groups to which they were randomized. Safety analyses included only participants who received at least 1 dose of study drug and included only trial outcomes within 30 days after permanent discontinuation of study drug. The log-rank statistic was used for efficacy and safety analyses, with results also presented as unadjusted HRs and their 95% CIs. In a prespecified secondary analysis, we included the regional coordinating center as a random effect. Tests of interaction with Bonferroni-corrected significance thresholds were used to examine the consistency of treatment effect on the primary efficacy outcome across 7 prespecified subgroup categories: age younger than 75 years vs 75 years or older; female vs male; Asian, Black, or other race or Hispanic ethnicity vs non-Hispanic White race; weight less than 70 kg vs 70 kg or greater; NT-proBNP level above vs below the median; P-wave terminal force in lead V1 above vs below the median; and left atrial diameter index above vs below the median. We also examined interactions between treatment and each atrial cardiopathy biomarker modeled as a continuous variable. Missing data were not imputed. The threshold of statistical significance was set at 2-sided α = .05. Secondary analyses should be interpreted as exploratory or hypothesis-generating. All analyses were performed with Stata/MP version 18 (StataCorp).
We performed several sensitivity analyses. First, in a prespecified analysis, we repeated our primary analysis using competing risk regression accounting for the competing risk of death. Second, in a prespecified analysis, we compared the risk of recurrent stroke between treatment groups with censoring of follow-up at the time of atrial fibrillation diagnosis. Third, in a post hoc analysis, we performed our primary analysis in only the 149 patients documented to have atrial fibrillation after randomization. Fourth, in a post hoc analysis, we performed our primary analysis within subgroups defined by each of the 3 atrial cardiopathy biomarker criteria.
Results
Early Trial Termination
On December 14, 2022, the DSMB met to review the findings of the prespecified interim analysis performed after 75 primary outcome events. There were no indications of safety concerns. The HR for apixaban vs aspirin (1.03 [95% CI, 0.65-1.61]) lay within the prespecified interim boundaries for futility (HR >0.914 and <1.095), indicating that the nonbinding stopping rule for futility had been met. Conditional power under the original design assumptions was 19%. The DSMB recommended stopping further recruitment, transitioning participants to open-label antithrombotic therapy, closing out trial participation, and collecting final outcome data. After completion of these steps, the DSMB met again on April 24, 2023, to review all available data, which now included 80 primary outcome events. The HR for apixaban vs aspirin (1.00 [95% CI, 0.64-1.55]) again lay within futility boundaries (HR >0.923 and <1.084), which had been updated to account for 80 rather than 75 events. It was estimated that conditional power under the original design assumptions would be 17% once 150 primary outcome events occurred. The DSMB confirmed the recommendation to terminate the trial and the NIH accepted the recommendation.
Participants and Follow-Up
From February 1, 2018, through December 14, 2022, 3745 patients with a qualifying cryptogenic stroke consented to screening for atrial cardiopathy, of whom 1548 (41.3%) met at least 1 of the atrial cardiopathy biomarker criteria. Compared with patients without evidence of atrial cardiopathy, those who met criteria for atrial cardiopathy were older; were more often female; were more often Black or African American and less often Hispanic; and more often had ischemic heart disease, heart failure, hypertension, and left atrial enlargement (eTable 1 in Supplement 2). Ultimately, 1015 patients with evidence of atrial cardiopathy were randomly assigned to apixaban or aspirin, with the remaining excluded mostly because of the interim development of exclusion criteria such as detection of atrial fibrillation prior to randomization (Figure 1; eTable 2 in Supplement 2). After randomization, 97 patients (9.6%) withdrew consent for participation, 5 (0.5%) had participation terminated for other reasons, and 25 (2.5%) were lost to follow-up (Figure 1; eTable 3 in Supplement 2). Permanent study drug discontinuation for nonprotocol reasons occurred in 24.5% of patients per year in the apixaban group and 25.1% of patients per year in the aspirin group.
The final analysis included data through February 28, 2023, from the 1015 randomized trial participants, with a mean (SD) follow-up period of 1.8 (1.3) years. The mean age of trial participants was 68 years, 54.3% were female, 21.1% were Black or African American, and 8.1% were Hispanic or Latino (Table 1). The median time of randomization was 50 days after stroke onset and the median NIH Stroke Scale score at the time of enrollment was 1, indicating mild stroke or significant recovery. Most patients qualified for randomization by the serum NT-proBNP level (61.1%) or ECG criteria (53.4%) for atrial cardiopathy (eFigure in Supplement 2).
Efficacy Outcomes
The primary efficacy outcome of recurrent stroke occurred in 40 patients in the apixaban group (annualized rate, 4.4%) and 40 patients in the aspirin group (annualized rate, 4.4%) (HR, 1.00 [95% CI, 0.64-1.55]; P value for log-rank test = .99) (Table 2 and Figure 2). This finding was unchanged in a secondary analysis adjusting for the regional coordinating center as a random effect (HR, 1.00 [95% CI, 0.64-1.55]) and in a prespecified sensitivity analysis accounting for the competing risk of death (HR, 0.99 [95% CI, 0.64-1.54]). The secondary efficacy outcome of recurrent ischemic stroke or systemic embolism occurred in 37 patients in the apixaban group (annualized rate, 4.1%) and 40 patients in the aspirin group (annualized rate, 4.4%) (HR, 0.92 [95% CI, 0.59-1.44]). The secondary efficacy outcome of recurrent stroke or death occurred in 67 patients in the apixaban group (annualized rate, 7.3%) and 62 patients in the aspirin group (annualized rate, 6.8%) (HR, 1.08 [95% CI, 0.76-1.52]) (Table 2).
Table 2. Efficacy and Safety Outcomes.
| Outcome | Apixaban (n = 507) | Aspirin (n = 508) | Difference, % (95% CI) | Hazard ratio (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|
| Total events | Person-years of observation | Annualized rate, % (95% CI) | Total events | Person-years of observation | Annualized rate, % (95% CI) | |||
| Primary efficacy outcome | ||||||||
| Recurrent stroke of any type | 40 | 913 | 4.4 (3.2 to 6.0) | 40 | 910 | 4.4 (3.2 to 6.0) | 0 (−1.9 to 1.9) | 1.00 (0.64 to 1.55) |
| Secondary efficacy outcomes | ||||||||
| Recurrent ischemic stroke or systemic embolism | 37 | 913 | 4.1 (2.9 to 5.6) | 40 | 909 | 4.4 (3.2 to 6.0) | −0.4 (−2.2 to 1.5) | 0.92 (0.59 to 1.44) |
| Recurrent stroke of any type or death from any cause | 67 | 913 | 7.3 (5.8 to 9.3) | 62 | 910 | 6.8 (5.3 to 8.7) | 0.5 (−1.9 to 3.0) | 1.08 (0.76 to 1.52) |
| Primary safety outcomes (on-treatment population) | ||||||||
| Symptomatic intracranial hemorrhagea | 0 | 668 | 0 | 7 | 660 | 1.1 (0.5 to 2.2) | −1.1 (−1.8 to −0.3) | |
| Major hemorrhageb | 5 | 668 | 0.7 (0.3 to 1.8) | 5 | 664 | 0.8 (0.3 to 1.8) | −0.0 (−0.9 to 0.9) | 1.02 (0.29 to 3.52) |
| Secondary safety outcome (on-treatment population) | ||||||||
| All-cause mortality | 12 | 668 | 1.8 (1.0 to 3.2) | 8 | 666 | 1.2 (0.6 to 2.4) | 0.6 (−0.7 to 1.9) | 1.53 (0.63 to 3.75) |
Includes symptomatic hemorrhagic transformation of ischemic stroke, which required new symptoms or signs adjudicated as being due to the hemorrhagic transformation or a patient whose initial imaging was judged to include hemorrhagic transformation of an ischemic stroke.
Excludes intracranial hemorrhage.
Figure 2. Cumulative Rates of the Primary Efficacy Outcome of Recurrent Stroke, Stratified by Treatment Group.

Recurrent stroke included stroke of ischemic, hemorrhagic, or unknown type. The mean (SD) follow-up period in both groups was 1.8 (1.3) years.
Atrial fibrillation was diagnosed in 149 patients (14.7%) at a median 30 weeks (IQR, 8-59) after randomization. In a prespecified sensitivity analysis, apixaban did not significantly reduce the rate of recurrent stroke when censoring follow-up at the time of atrial fibrillation diagnosis (HR, 1.05 [95% CI, 0.66-1.65]). A post hoc analysis was performed to assess whether any benefit of apixaban over aspirin may have been limited to patients with atrial cardiopathy that ultimately manifested in atrial fibrillation. When the primary analysis was repeated in only the 149 patients documented to have atrial fibrillation after randomization, no significant difference was found in the rate of recurrent stroke between the apixaban group (annualized rate, 1.8%) and the aspirin group (annualized rate, 2.2%) (HR, 0.84 [95% CI, 0.19-3.74]).
No significant evidence of heterogeneity of treatment effect on the primary efficacy outcome was found across prespecified subgroups; apixaban did not appear to be of greater benefit than aspirin at higher levels of atrial cardiopathy biomarkers (Figure 3). In a post hoc analysis of patients who met criteria for atrial cardiopathy by having P-wave terminal force in ECG lead V1 greater than 5000 μV × ms, no significant difference was found in the rate of recurrent stroke between the apixaban group (annualized rate, 2.6%) and the aspirin group (annualized rate, 4.2%) (HR, 0.61 [95% CI, 0.30-1.22]). Similarly, among those with serum NT-proBNP level greater than 250 pg/mL, no significant difference was found in the rate of recurrent stroke between the apixaban group (annualized rate, 5.9%) and the aspirin group (annualized rate, 4.6%) (HR, 1.29 [95% CI, 0.77-2.18]). Too few patients met the criterion of left atrial diameter index of 3 cm/m2 or greater on echocardiogram to allow a comparison of treatments in this subgroup.
Figure 3. Analysis of Treatment Effect on the Primary Efficacy Outcome Across Subgroups.
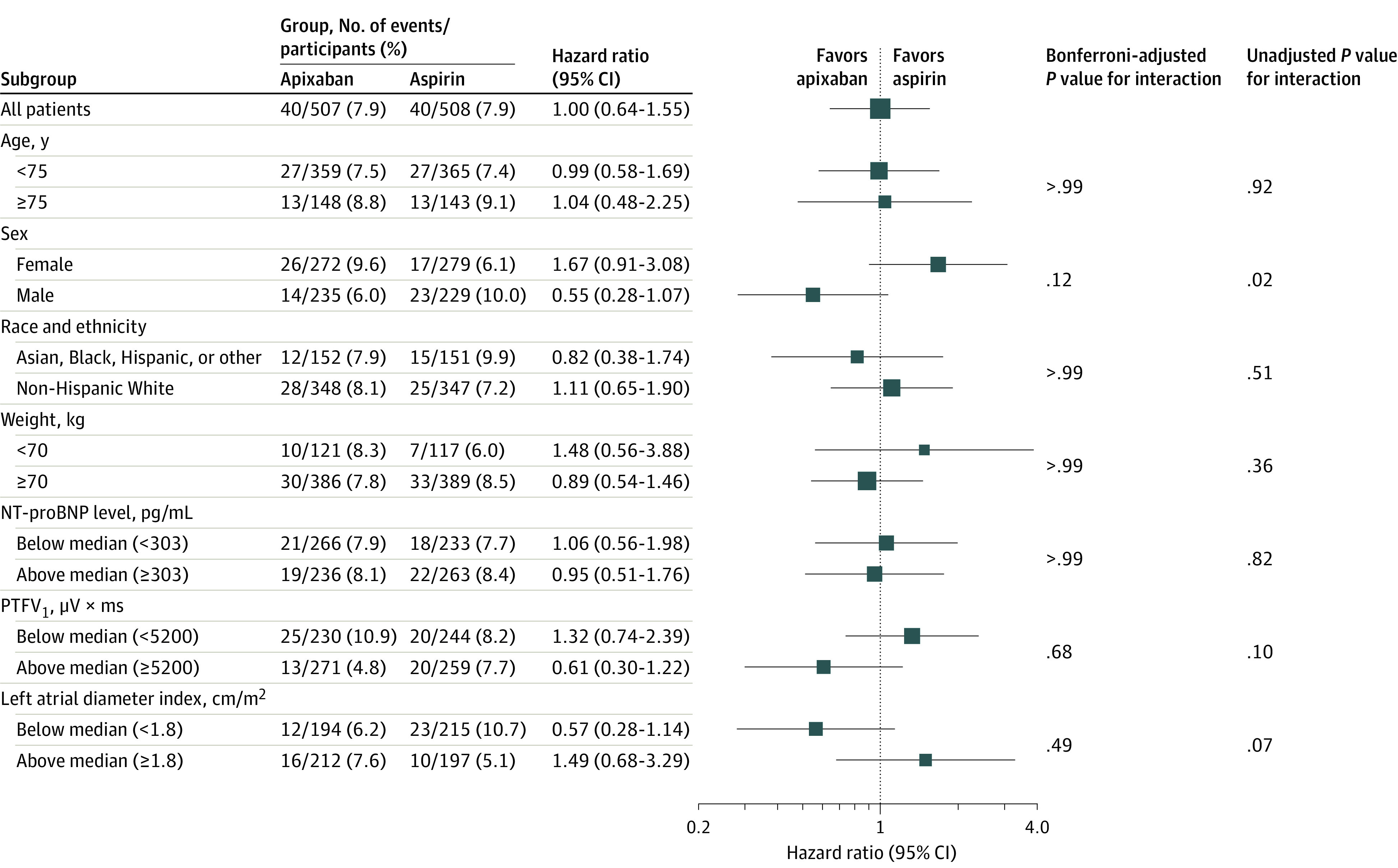
The primary efficacy outcome was recurrent stroke, which included stroke of ischemic, hemorrhagic, or unknown type. All subgroup analyses were prespecified. NT-proBNP indicates N-terminal pro-B-type natriuretic peptide and PTFV1, P-wave terminal force in lead V1. No statistically significant interactions were found at a Bonferroni-corrected P value threshold of .007, including when modeling the atrial cardiopathy biomarkers as continuous variables (P values for interaction: .68 [NT-proBNP], .35 [PTFV1], and .11 [left atrial diameter index] for treatment).
Safety Outcomes
In the safety sample, symptomatic intracranial hemorrhage occurred in no patients receiving apixaban (annualized rate, 0%) and 7 patients receiving aspirin (annualized rate, 1.1%) (Table 2). Major hemorrhage other than intracranial hemorrhage occurred in 5 patients receiving apixaban (annualized rate, 0.7%) and 5 patients receiving aspirin (annualized rate, 0.8%) (HR, 1.02 [95% CI, 0.29-3.52]). The secondary safety outcome of all-cause mortality occurred in 12 patients receiving apixaban (annualized rate, 1.8%) and 8 patients receiving aspirin (annualized rate, 1.2%) (HR, 1.53 [95% CI, 0.63-3.75]).
Discussion
In patients with a recent cryptogenic stroke and evidence of atrial cardiopathy based on 3 readily available biomarkers, oral anticoagulant therapy with apixaban did not significantly reduce the risk of recurrent stroke compared with aspirin. Apixaban did not appear to significantly increase the risk of symptomatic intracranial hemorrhage, other major bleeding, or death compared with aspirin.
Prospective observational studies found that several markers of atrial cardiopathy, including P-wave terminal force in ECG lead V1,13 serum NT-proBNP,14 and left atrial diameter,15 were associated with the risk of ischemic stroke. These markers were also associated with atrial fibrillation, but their associations with ischemic stroke were unchanged after adjustment for atrial fibrillation and were found in patients without clinically apparent atrial fibrillation. Given the results of the current trial, these previously demonstrated links between atrial cardiopathy and stroke may have reflected unmeasured confounding by subclinical atrial fibrillation, which was probably more thoroughly ruled out by continuous heart rhythm monitoring in potential trial participants than in earlier cohort studies. Other biomarkers of atrial cardiopathy, such as midregional proatrial natriuretic peptide, premature atrial contractions, left atrial fibrosis, left atrial volume, or functional measures including left atrial strain, were not used for patient selection in this trial.16,17 Nevertheless, nearly one-sixth of patients in the current trial were ultimately documented to have atrial fibrillation, the most widely accepted hallmark of atrial cardiopathy, and although this analysis was limited by a small sample size, the absolute risk of recurrent stroke in these patients was low and initiation of apixaban before atrial fibrillation diagnosis did not appear to be of benefit compared with aspirin.
Previously demonstrated associations between atrial cardiopathy and stroke may also have been confounded by atherosclerosis, which is more common in patients with atrial fibrillation than in the general population.18 Detailed data on the burden of atherosclerosis in trial participants were lacking, but recent observational studies have found that atherosclerotic plaques, in the absence of significant stenosis of the arterial lumen, are associated with ipsilateral stroke.19 Among patients with cryptogenic stroke, most recurrent strokes occur in the same cerebral arterial territory as the index stroke,20 a finding that appears more consistent with an upstream atherosclerotic source than a central cardioembolic source. The lack of benefit of anticoagulation over aspirin in trial participants despite selection for underlying cardiac abnormalities suggests that a substantial proportion of cryptogenic strokes may arise from nonstenosing atherosclerosis.
A significantly lower risk of symptomatic intracranial hemorrhage was found in trial participants taking apixaban compared with those taking aspirin. Previous randomized trials found that aspirin significantly increased the risk of intracranial hemorrhage compared with no aspirin therapy21 and apixaban did not increase the risk of intracranial hemorrhage compared with aspirin.22,23 In this context, the current findings further support the relative safety of apixaban compared with aspirin in regard to intracranial hemorrhage. Given the small overall number of such events in this trial, the reduction in intracranial hemorrhage with apixaban vs aspirin may reflect a chance finding.
Limitations
This study has several limitations. First, amid the COVID-19 pandemic, participants withdrew from the trial at a higher-than-expected rate. Withdrawal may have been nonrandomly different between treatment groups, but such a phenomenon typically favors the treatment with more adverse effects,24 which generally would be anticoagulation rather than antiplatelet therapy. In this trial, the dosing regimens and rates of adverse events were comparable between treatment groups. Thus, nonrandom withdrawal seems unlikely to explain the lack of benefit with apixaban vs aspirin. Random withdrawal from both treatment groups would have reduced the statistical power but is unlikely to explain the completely null results and low event rate in the aspirin group despite enrichment for atrial cardiopathy. Rates of atrial fibrillation diagnosis after randomization were also higher than projected, perhaps because of increasingly widespread use of continuous heart rhythm monitoring. However, the mean follow-up period was also longer than projected because of slower recruitment during the COVID-19 pandemic and, in a blinded analysis presented to the DSMB prior to the interim analysis, the pooled event rate was found to be in line with the original assumption, alleviating any concerns that the study may have been underpowered based on incorrect assumptions about the event rate.
Second, few patients met the atrial cardiopathy criterion of severe left atrial enlargement, but the other criteria led to the inclusion of most patients with mild or moderate left atrial enlargement, so a lower left atrial size threshold would not have substantially affected the profile of randomized participants. Overall, few patients with cryptogenic stroke had any degree of left atrial enlargement, so the exclusive use of left atrial size as the criterion for atrial cardiopathy would have rendered such a trial infeasible. Given the small number of patients with severe left atrial enlargement in this trial, the benefit of anticoagulation in such patients remains unknown. However, no interactions were found between the severity of atrial cardiopathy biomarkers and the effect of apixaban over aspirin, suggesting that different choices of biomarker thresholds would not have changed the current findings.
Conclusions
In patients with cryptogenic stroke and evidence of atrial cardiopathy without atrial fibrillation, apixaban did not significantly reduce recurrent stroke risk compared with aspirin.
Educational Objective: To identify the key insights or developments described in this article.
-
Markers of atrial cardiopathy, even without clinically apparent atrial fibrillation, are associated with risk of ischemic stroke. What was the purpose of this trial?
To test whether anticoagulation was superior to antiplatelet therapy for preventing recurrent stroke in patients with atrial cardiopathy and recent cryptogenic stroke.
To test whether aspirin alone, vs no antiplatelet therapy, provided primary protection from stroke in patients with atrial cardiopathy.
To test whether combined therapy of anticoagulation plus antiplatelet therapy was superior to monotherapy in preventing recurrent stroke in patients with atrial cardiopathy.
-
Criteria for atrial cardiopathy were chosen for their association with an increased risk of stroke in prior observational studies. Which of the following formed the eligibility criteria for atrial cardiopathy?
Any indication of atrial enlargement seen on ECG, echocardiogram, or cardiac computed tomography angiography.
Atrial dysfunction of any sort seen on echocardiogram in the absence of evidence of arrhythmia.
P-wave terminal force in electrocardiogram lead V1 greater than 5000 μV × ms, serum N-terminal pro-B-type natriuretic peptide level greater than 250 pg/mL, or left atrial diameter index of 3 cm/m2 or greater on echocardiogram.
-
This trial was terminated early at an interim analysis. Why?
Multiple cases of major bleeding, including intracranial hemorrhage, occurred in the anticoagulation group, and the trial was stopped for exceeding safety standards.
The anticoagulation group had fewer events of stroke, demonstrating early superiority and meeting stopping criteria.
The hazard ratio for apixaban vs aspirin met the predefined definition of futility leading to the conclusion that there was no difference between groups.
Trial Protocol and Statistical Analysis Plan
eFigure. Diagram of Atrial Cardiopathy Biomarker Criteria Leading to Trial Inclusion
eTable 1. Baseline Characteristics of Consented Patients, Stratified by Evidence of Atrial Cardiopathy
eTable 2. Baseline Characteristics of Consented Patients, Stratified by Whether Treatment Assignment Occurred
eTable 3. Characteristics of Randomized Patients at Baseline, Stratified by Completion of Full Duration of Follow-Up
Nonauthor Collaborators. ARCADIA Investigators
Data Sharing Statement
References
- 1.Goette A, Kalman JM, Aguinaga L, et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: definition, characterization, and clinical implication. Heart Rhythm. 2017;14(1):e3-e40. doi: 10.1016/j.hrthm.2016.05.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hirsh BJ, Copeland-Halperin RS, Halperin JL. Fibrotic atrial cardiomyopathy, atrial fibrillation, and thromboembolism: mechanistic links and clinical inferences. J Am Coll Cardiol. 2015;65(20):2239-2251. doi: 10.1016/j.jacc.2015.03.557 [DOI] [PubMed] [Google Scholar]
- 3.Kamel H, Okin PM, Elkind MS, Iadecola C. Atrial fibrillation and mechanisms of stroke: time for a new model. Stroke. 2016;47(3):895-900. doi: 10.1161/STROKEAHA.115.012004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ntaios G. Embolic stroke of undetermined source: JACC review topic of the week. J Am Coll Cardiol. 2020;75(3):333-340. doi: 10.1016/j.jacc.2019.11.024 [DOI] [PubMed] [Google Scholar]
- 5.Kamel H, Longstreth WT Jr, Tirschwell DL, et al. The Atrial Cardiopathy and Antithrombotic Drugs in Prevention After Cryptogenic Stroke randomized trial: rationale and methods. Int J Stroke. 2019;14(2):207-214. doi: 10.1177/1747493018799981 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hart RG, Diener HC, Coutts SB, et al. ; Cryptogenic Stroke/ESUS International Working Group . Embolic strokes of undetermined source: the case for a new clinical construct. Lancet Neurol. 2014;13(4):429-438. doi: 10.1016/S1474-4422(13)70310-7 [DOI] [PubMed] [Google Scholar]
- 7.Kamel H, O’Neal WT, Okin PM, Loehr LR, Alonso A, Soliman EZ. Electrocardiographic left atrial abnormality and stroke subtype in the atherosclerosis risk in communities study. Ann Neurol. 2015;78(5):670-678. doi: 10.1002/ana.24482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Soares JF, Jeff Wu CF. Some Restricted randomization rules in sequential designs. Commun Stat Theory Methods. 1983;12(17):2017-2034. doi: 10.1080/03610928308828586 [DOI] [Google Scholar]
- 9.Zhao W, Weng Y. Block urn design: a new randomization algorithm for sequential trials with two or more treatments and balanced or unbalanced allocation. Contemp Clin Trials. 2011;32(6):953-961. doi: 10.1016/j.cct.2011.08.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Schulman S, Angerås U, Bergqvist D, Eriksson B, Lassen MR, Fisher W; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis . Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. J Thromb Haemost. 2010;8(1):202-204. doi: 10.1111/j.1538-7836.2009.03678.x [DOI] [PubMed] [Google Scholar]
- 11.Diener HC, Eikelboom J, Connolly SJ, et al. ; AVERROES Steering Committee and Investigators . Apixaban versus aspirin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a predefined subgroup analysis from AVERROES, a randomised trial. Lancet Neurol. 2012;11(3):225-231. doi: 10.1016/S1474-4422(12)70017-0 [DOI] [PubMed] [Google Scholar]
- 12.Longstreth WT Jr, Kronmal RA, Thompson JL, et al. Amino terminal pro-B-type natriuretic peptide, secondary stroke prevention, and choice of antithrombotic therapy. Stroke. 2013;44(3):714-719. doi: 10.1161/STROKEAHA.112.675942 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kamel H, Soliman EZ, Heckbert SR, et al. P-wave morphology and the risk of incident ischemic stroke in the Multi-Ethnic Study of Atherosclerosis. Stroke. 2014;45(9):2786-2788. doi: 10.1161/STROKEAHA.114.006364 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Folsom AR, Nambi V, Bell EJ, et al. Troponin T, N-terminal pro-B-type natriuretic peptide, and incidence of stroke: the atherosclerosis risk in communities study. Stroke. 2013;44(4):961-967. doi: 10.1161/STROKEAHA.111.000173 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Benjamin EJ, D’Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death: the Framingham Heart Study. Circulation. 1995;92(4):835-841. doi: 10.1161/01.CIR.92.4.835 [DOI] [PubMed] [Google Scholar]
- 16.Maheshwari A, Norby FL, Inciardi RM, et al. Left atrial mechanical dysfunction and the risk for ischemic stroke in people without prevalent atrial fibrillation or stroke: a prospective cohort study. Ann Intern Med. 2023;176(1):39-48. doi: 10.7326/M22-1638 [DOI] [PubMed] [Google Scholar]
- 17.Schweizer J, Arnold M, König IR, et al. Measurement of midregional pro-atrial natriuretic peptide to discover atrial fibrillation in patients with ischemic stroke. J Am Coll Cardiol. 2022;79(14):1369-1381. doi: 10.1016/j.jacc.2022.01.042 [DOI] [PubMed] [Google Scholar]
- 18.Heeringa J, van der Kuip DA, Hofman A, et al. Subclinical atherosclerosis and risk of atrial fibrillation: the Rotterdam study. Arch Intern Med. 2007;167(4):382-387. doi: 10.1001/archinte.167.4.382 [DOI] [PubMed] [Google Scholar]
- 19.Kopczak A, Schindler A, Bayer-Karpinska A, et al. Complicated carotid artery plaques as a cause of cryptogenic stroke. J Am Coll Cardiol. 2020;76(19):2212-2222. doi: 10.1016/j.jacc.2020.09.532 [DOI] [PubMed] [Google Scholar]
- 20.Veltkamp R, Pearce LA, Korompoki E, et al. Characteristics of recurrent ischemic stroke after embolic stroke of undetermined source: secondary analysis of a randomized clinical trial. JAMA Neurol. 2020;77(10):1233-1240. doi: 10.1001/jamaneurol.2020.1995 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Huang WY, Saver JL, Wu YL, Lin CJ, Lee M, Ovbiagele B. Frequency of intracranial hemorrhage with low-dose aspirin in individuals without symptomatic cardiovascular disease: a systematic review and meta-analysis. JAMA Neurol. 2019;76(8):906-914. doi: 10.1001/jamaneurol.2019.1120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Connolly SJ, Eikelboom J, Joyner C, et al. ; AVERROES Steering Committee and Investigators . Apixaban in patients with atrial fibrillation. N Engl J Med. 2011;364(9):806-817. doi: 10.1056/NEJMoa1007432 [DOI] [PubMed] [Google Scholar]
- 23.Healey JS, Lopes RD, Granger CB, et al. ; ARTESIA Investigators . Apixaban for stroke prevention in subclinical atrial fibrillation. N Engl J Med. 2023. doi: 10.1056/NEJMoa2310234 [DOI] [PubMed] [Google Scholar]
- 24.US Food and Drug Administration . Data retention when subjects withdraw from FDA-regulated clinical trials: guidance for sponsors, clinical investigators, and IRBs. Accessed May 31, 2023. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/data-retention-when-subjects-withdraw-fda-regulated-clinical-trials
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol and Statistical Analysis Plan
eFigure. Diagram of Atrial Cardiopathy Biomarker Criteria Leading to Trial Inclusion
eTable 1. Baseline Characteristics of Consented Patients, Stratified by Evidence of Atrial Cardiopathy
eTable 2. Baseline Characteristics of Consented Patients, Stratified by Whether Treatment Assignment Occurred
eTable 3. Characteristics of Randomized Patients at Baseline, Stratified by Completion of Full Duration of Follow-Up
Nonauthor Collaborators. ARCADIA Investigators
Data Sharing Statement