

Abstract
Objective
To explore the potential associations between pregnancy cravings and various sociodemographic, lifestyle and health factors.
Design
Cross-sectional study.
Setting
Population-based study in Jordan.
Participants
A total of 500 women who had children and experienced pregnancy cravings were included.
Primary and secondary outcome measures
Pregnancy cravings are prevalent among Jordanian women and associated with some sociodemographic, lifestyle and health factors.
Results
The results showed that 75.40% (377/500) of women experienced food cravings, with 40.6% and 29.1% of them having iron deficiency and vitamin D deficiency, respectively. The most commonly craved food items were sweets (17.2%, 86/500) and salts (22.2%, 115/500), while less than 1.0% of women craved non-food items. No significant correlation (p>0.05) was found between food cravings and the gender of the babies. Significant associations were found between food cravings and the mother’s educational level (p=0.023), weight loss (p<0.001) and diseases such as anaemia (p=0.01).
Conclusion
Pregnancy cravings, particularly for food items, with sweets and salts being the most commonly craved, are prevalent among Jordanian women and are associated with the mother’s educational level, changes in weight and the presence of anaemia. Additionally, the study found that iron and vitamin D deficiencies are prevalent health issues among women experiencing these cravings in Jordan. This research has important implications, emphasising the pressing need for targeted nutritional interventions and healthcare strategies to address identified deficiencies and improve maternal health outcomes in the region.
Keywords: Maternal medicine, Eating disorders, PSYCHIATRY
Strengths and limitations of this study.
Being a population-based study, the findings are likely to reflect the prevalence and associations of pregnancy cravings with sociodemographic and lifestyle factors among a broader group of Jordanian women.
The study examines various sociodemographic, lifestyle and health factors in relation to pregnancy cravings, providing a comprehensive analysis of potential associations.
The study includes a good sample size of 500 women, which enhances the statistical power and generalisability of the findings to the population of Jordanian women experiencing pregnancy cravings.
Since the study relies on self-reported data, there may be potential recall bias as participants might not accurately recall past cravings, lifestyle factors or health conditions.
Despite statistical analyses, there might be unaccounted confounding factors that could influence the associations between pregnancy cravings and the studied variables.
Introduction
Craving is defined as ‘an intense desire or yearning’.1 Over time, craving has become closely linked to excessive patterns of food consumption in specific psychological and physiological contexts. Cravings are highly prevalent, with 97% of women and 68% of men reporting episodes of food cravings.2 Craving for unusual items is often considered a sign of pregnancy across various cultures. Pregnant women frequently experience changes in their appetites, including both aversions and strong cravings for specific foods and non-food items.
Women from diverse populations worldwide often report uncomfortable somatic changes during pregnancy, particularly in the early stages. These changes can include food aversions and cravings, and also pregnancy-specific stress, which is a consistent predictor of delivery prematurely.3 4 Early pregnancy is a critical period that can significantly impact placental growth and function, fetal physiology, and the subsequent development of obesity and chronic conditions like diabetes, hypertension, asthma and atopy.3
There are four primary hypotheses regarding the origin of pregnancy cravings, involving hormones, nutritional deficiencies, rewarding substances in desired foods, and complex cultural and psychosocial influences.5 One previous study proposed that pregnant women consume more food to meet the energetic demands of the growing fetus or compensate for nutrient losses due to nausea, vomiting and aversions in the first trimester.6 7 However, other studies have shown that pregnant women experience various clinical symptoms throughout pregnancy, including nausea, vomiting, fatigue and abdominal cramps, with greater intensity in the early and middle stages.8
Additionally, research indicates that less than one-third of pregnant women experiencing nausea and vomiting have symptoms confined to the morning, while the majority experience symptoms throughout the day.9 The specific foods craved during pregnancy can vary significantly. Studies conducted in Saudi Arabia and the UK found that pregnant women craved a wide range of foods, including milk, sweets, dates, salty foods, fruit and fruit juices.10 11 A study conducted in Fiji discovered that cravings predominantly centre around foods rich in calories and micronutrients, posing minimal risks to both mothers and fetuses.12 Moreover, the research indicated a correlation between aversions to certain foods and an increased likelihood of craving alternatives that fulfil nutritional requirements similar to the avoided foods. A study by Blau et al13 showed that preconception tobacco use demonstrated a link with increased frequency of food cravings during pregnancy, particularly for high-fat and fast-food options, in contrast to non-smoking women. Also, factors related to both emotional and physiological aspects of cravings contributed to 35% of the variation observed in excessive gestational weight gain. A recently published study in Brazil, which involved the recruitment of 233 pregnant women, demonstrated no correlation between the caloric midpoint and food cravings.14
Maintaining a healthy diet is crucial during pregnancy to ensure positive outcomes for both the mother and the baby.15 Craving sugary or salty processed foods can be detrimental to a healthy pregnancy diet. High simple sugar consumption during pregnancy may contribute to a marked increase in gestational weight as well as the development of various complications of pregnancy such as gestational diabetes, pre-eclampsia and preterm birth. High salt consumption, on the other hand, can have a number of negative health effects. This is regarded as a primary cause and contributory risk factor for many cardiovascular illnesses.16 17
Therefore, healthcare practitioners should provide adequate counselling and follow-up to pregnant women, emphasising the importance of consuming a balanced diet and avoiding cravings for unhealthy junk foods, which can contribute to better pregnancy outcomes.
Despite some existing literature on pregnancy cravings, research investigating the associations between this physiological and psychological phenomenon and its sociodemographic, lifestyle and health factors in pregnant women is still limited. Therefore, our hypothesis is that there are distinct associations between pregnancy cravings and at least one of the related sociodemographic, lifestyle or health factors. Considering genetic as well as environmental variations among different populations, we expect these associations to differ among Jordanian women. Therefore, this study aims to assess the prevalence and types of food cravings, identify factors influencing food cravings and examine the impact of food cravings on the nutritional status of pregnant women.
Materials and methods
Design and sampling
This cross-sectional survey was meticulously conducted between January and June 2023 using an online questionnaire to ensure accessibility and convenience for participants. The study exclusively focused on the experiences of pregnant women and those who had children with a history of pregnancy cravings, and the survey provided a nuanced understanding of this unique population. Notably, the majority of participants fell within the age range of 18–40, contributing diverse perspectives and insights representative of this critical reproductive stage.
The questionnaire used in this study was developed based on an extensive review of similar literature and was validated. Initially, a group of experts provided feedback on the survey items, which was then incorporated into the study survey. Subsequently, pilot testing was conducted using a modified version of the questionnaire, and feedback on the clarity and comprehensibility of the survey items was obtained from several participants. The responses from the pilot study were not included in the final data analysis.
Survey eligibility was extended to women proficient in reading Arabic, possessing internet access, and either currently pregnant or mothers of children. Exclusion criteria encompassed non-Jordanian women, individuals with a high abortion rate, women expecting twins or who had recently delivered twins, those with more than four children, individuals aged over 60 or below 18 and those unable to recall episodes of pregnancy cravings.
In pursuit of a representative sample size, a comprehensive strategy was employed to target potential participants for the online survey. Initial outreach efforts involved using prominent social media platforms, specifically Facebook and Instagram. Additionally, direct communication via WhatsApp served as a supplementary channel for participant recruitment. Employing a snowball sampling technique, participants were encouraged to extend the study invitation to acquaintances, family members and friends. It is crucial to emphasise that survey participation was entirely voluntary and that responses were collected anonymously. Consent was inferred based on the completion and submission of the online survey.
All forms were gathered by the end of June, and we initiated the process of sorting and collecting completed forms to complete the remaining steps of the study. Incomplete surveys were promptly excluded because the questions on the questionnaire are sequential and interrelated.
Study survey
The survey questionnaire used in this study consisted of 20 questions. Participants were asked about their age, occupation, smoking habits, presence of diseases, monthly income, place of residence, types of foods, drugs and diets during pregnancy, as well as the gender of their children (online supplemental file 1). To facilitate the survey, an online version was developed using Google Form (Google, Mountain View, California) and made accessible through a QR (quick response) code.
bmjopen-2023-078082supp001.pdf (2.9MB, pdf)
Sample size
The sample size for the study was estimated using G-Power V.3.1 from Universität Kiel, Germany, following the convenience sampling method, assuming a medium effect size, a power of 0.90 and an alpha level of 0.05.
Patient and public involvement
Public were involved in the design of this research.
Data analysis
Data were collected and compiled using Microsoft Excel V.2010 (Office 360, Microsoft, USA). Categorical data were expressed in terms of frequency and percentages. The χ2 test of independence was used to explore the association between food cravings and participants’ characteristics, as well as to examine the relationship between vitamins, minerals and newborn gender. An alpha level of 0.05 was considered statistically significant, and data analysis was performed using SPSS V.28 software.
Results
Participants’ sociodemographic characteristics (N=500)
The questionnaire produced a total of 776 responses. However, on examination, 140 were considered incomplete due to lack of fundamental information required for the investigation, while 136 were excluded for not meeting our inclusion criteria. Consequently, the number of valid and complete responses amounted to 500.
The majority of recruited women were aged between 18 and 40 years old, accounting for 428 participants (85.6%). Regarding education, 238 (47.6%) had a bachelor’s degree. In terms of monthly income, 351 (70.2%) reported earning less than 550 Jordanian dinar. Additionally, a significant portion of the participants (322, 64.4%) were unemployed and resided in the city.
In terms of the health characteristics of the mothers, the findings of the study indicated that the vast majority of them were non-smokers (410, 82.0%). There was a significant proportion of mothers with chronic diseases, with endocrine disorders being the most prevalent (34, 6.8%). Moreover, more than three-quarters of the sample reported experiencing rapid weight gain during their pregnancy journey. In terms of the babies delivered, the percentage was evenly split between male and female babies, with an average birth weight of 3062.95±621.63 g (table 1).
Table 1.
Sociodemographic characteristics of the participants
| Variables | Category | Frequency | Percentage |
| Mother’s age (years) | 18–40 | 428 | 85.6 |
| 41–60 | 72 | 14.4 | |
| Mother’s educational level | Secondary and less | 131 | 26.2 |
| Diploma | 78 | 15.6 | |
| Bachelor’s degree | 238 | 47.6 | |
| Higher education | 53 | 10.6 | |
| Family income (Jordanian dinar) | Less than 550 | 351 | 70.2 |
| 550 and above | 149 | 29.8 | |
| Occupation status | No job/ housewife | 322 | 64.4 |
| Private | 22 | 4.4 | |
| Non-government sector | 56 | 11.2 | |
| Government sector | 100 | 20.0 | |
| Place of living | City | 322 | 64.4 |
| Village | 178 | 35.6 | |
| Smoking status | Non-smoking | 410 | 82.0 |
| Smoking | 90 | 18.0 | |
| Chronic diseases | Endocrine | 34 | 6.8 |
| Hypertension | 29 | 5.8 | |
| Diabetes mellitus | 17 | 3.4 | |
| Obesity | 26 | 5.2 | |
| Anaemia | 27 | 5.4 | |
| Mother’s weight change | Rapid increment | 402 | 80.4 |
| Rapid decrement | 98 | 19.6 | |
| Newborn sex | Male | 249 | 49.8 |
| Female | 251 | 50.2 | |
| Number of pregnancies, mean±SD | 2.0±1.2 | ||
| Birth weight, mean±SD | 3062.95±621.63 |
Prevalence of maternal food cravings and the most frequently craved items
Approximately three-quarters of the sample (75.40%) experienced food cravings, while approximately a quarter (25.60%) did not (online supplemental file 2). Among the mothers who reported food cravings, the analysis revealed that the most commonly craved food items were sweets (17.2%) and salts (22.2%), as shown in figure 1. On the other hand, a minority (less than 1.0%) reported cravings for non-food items and carbohydrates.
Figure 1.

Percentage of food items craved by mothers.
bmjopen-2023-078082supp002.pdf (303.5KB, pdf)
Association between food cravings and participants’ sociodemographic characteristics
The study aimed to investigate the association between food cravings and the mothers’ characteristics using χ2 analysis. The results presented in table 2 indicate a significant association between the mother’s education and food cravings (p=0.023). Furthermore, 78.9% of mothers who experienced rapid weight gain reported food cravings, compared with 61.2% of mothers who had rapid weight loss (p<0.001). Additionally, 96.3% of mothers with endocrine disorders experienced food cravings (p=0.010). On the other hand, neither the mother’s age, place of residence, smoking status nor family income showed a significant association with food cravings (p>0.05 for all variables; table 2).
Table 2.
Association between food cravings and participants’ sociodemographic characteristics
| Variables | Category | Food craving | χ2 | P value | |
| No | Yes | ||||
| Mother’s educational level | Secondary and less | 45 (34.4)* | 86 (65.6)† | 9.567 | 0.023 |
| Diploma | 17 (21.8)* | 61 (78.2)* | |||
| Bachelor’s degree | 48 (20.2)* | 190 (79.8)† | |||
| Higher education | 13 (24.5)* | 40 (75.5)* | |||
| Mother’s weight change | Rapid increment | 85 (21.1) | 317 (78.9) | 13.205 | <0.001 |
| Rapid decrement | 38 (38.8) | 60 (61.2) | |||
| Chronic diseases (positive) | Anaemia | 1 (3.7) | 26 (96.3) | 6.719 | 0.010 |
| Endocrine | 9 (26.5) | 25 (73.5) | 0.069 | 0.793 | |
| Hypertension | 11 (37.9) | 18 (62.1) | 2.950 | 0.086 | |
| Diabetes mellitus | 6 (35.3) | 11 (64.7) | 1.085 | 0.298 | |
| Obesity | 5 (19.2) | 21 (80.8) | 0.426 | 0.514 | |
| Mother’s age (years), n (%) | 18–40 | 102 (23.8) | 326 (76.2) | 0.946 | 0.331 |
| 41–60 | 21 (29.2) | 51 (70.8) | |||
| Place of living | City | 85 (26.4) | 237 (73.6) | 1.576 | 0.209 |
| Village | 38 (21.3) | 140 (78.7) | |||
| Smoking status | Non-smoking | 100 (24.4) | 310 (75.6) | 0.054 | 0.816 |
| Smoking | 23 (25.6) | 67 (74.4) | |||
| Family income (Jordanian dinar) | Less than 550 | 87 (24.8) | 264 (75.2) | 0.022 | 0.882 |
| 550 and above | 36 (24.2) | 113 (75.8) | |||
p<0.05 considered statistically significant are in bold.
*Groups within each variable where column proportions do not significantly differ at p<0.05.
Association between food craving and the baby’s gender
A subset of craving mothers (n=377) were categorised based on the specific food items craved and correlated with the gender of their babies using χ2 test. The results indicated no significant association between food cravings and the gender of the babies (p=0.061). However, it is worth noting that 66.7% of mothers who craved caffeine and spicy foods gave birth to female babies. Refer to table 3 for detailed information.
Table 3.
Association between food craving and the baby’s gender
| Craved food items | Newborn sex | |
| Male, n (%) | Female, n (%) | |
| Sweets | 31 (36.0) | 55 (64.0) |
| Salts | 64 (57.7) | 47 (42.3) |
| Fruits, vegetables without citrus | 18 (39.1) | 28 (60.9) |
| Citrus | 29 (47.5) | 32 (52.5) |
| Carbohydrates | 2 (50.0) | 2 (50.0) |
| Proteins | 16 (64.0) | 9 (36.0) |
| Lipids and junk food | 8 (42.1) | 11 (57.9) |
| Caffeine | 4 (33.3) | 8 (66.7) |
| Non-food items (pica) | 3 (75.0) | 1 (25.0) |
| Spicy | 3 (33.3) | 6 (66.7) |
| Test values | χ2=16.270, p=0.061 | |
Pattern of vitamin and mineral deficiencies during the pregnancy period
Mothers were asked if they experienced any deficiencies of vitamins or minerals during the pregnancy period. Figure 2 shows the results, indicating that 29.1% of mothers experienced a deficiency in vitamin D. Additionally, 21.7% and 8.4% experienced deficiencies in vitamin B12 (cobalamin) and B9 (folate), respectively. In terms of mineral deficiencies, the majority experienced a deficiency in iron or ferritin (40.6%). Calcium deficiency accounted for 21.5% of the sample, while a minority (7.9%) had a deficiency in zinc.
Figure 2.
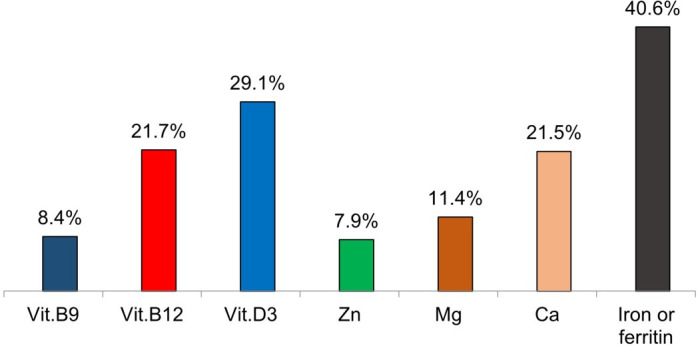
Vitamins and mineral deficiency patterns during pregnancy. Ca, calcium; Mg, magnesium; Zn, zinc.
Association between vitamins, minerals and the baby’s gender
The analysis of the χ2 test, as presented in table 1 and online supplemental file 2, examines the potential association between vitamins, minerals and the gender of the baby. The obtained p value of 0.639 suggests that no statistically significant relationship was found between the variables in this study.
Discussion
The objective of this exploratory study was to explore the potential associations between pregnancy cravings and various sociodemographic, lifestyle and health factors in a sample of pregnant women in Jordan. To the best of the authors’ knowledge, this is the first study of its kind to investigate the relationship between pregnancy cravings (alwaham) and these characteristics among Jordanian women.
The prevalence of maternal food cravings during pregnancy can vary across studies and populations. It has been reported that the majority of pregnant women experience food cravings at some point during their pregnancy.18–21 Subsequent research has demonstrated that the worldwide occurrence of food cravings ranges between 38% and 79%, exhibiting lower frequencies among European populations while displaying greater prevalence within the African continent.22 23 In our study on Jordanian women, the prevalence of food cravings during pregnancy was approximately 75%, which falls within the range reported in previous studies.
In Western cultures, pregnant women often experience cravings for various food items, including chocolate, fruits and fruit juices, sweet treats like ice cream and desserts, and to a lesser extent a range of meat and dairy products.22 In the current study, the analysis revealed that the most commonly craved food items were sweets and salts. In fact, the exact cause of food cravings during pregnancy is not fully understood; however, researchers propose that several factors contribute to their development, including cultural and societal influences, hormonal changes associated with pregnancy, food availability, and increased nutritional needs and energy requirements.22 24
The results from this study presented an association between mothers’ education and food cravings. In the present study, mothers’ educational level, mothers’ weight change and chronic diseases such as anaemia were found to be associated with pregnancy craving. A study found that food cravings during pregnancy were associated with excess weight gain and the development of obesity in pregnancy, which can be influenced by various factors, including educational level.23 Another study found that mothers’ educational level may have an impact on their young adult children’s fast-food consumption.25 However, further research is needed to fully understand the relationship between a mother’s education and food cravings. On the other hand, there is evidence that suggests an association between a mother’s weight change and food cravings. In a weight loss randomised controlled trial, it was found that decreasing the frequency of consuming food items was associated with decreases in cravings and weight loss.26 Another study found that food cravings are a desire for specific foods which, if uncontrolled, may lead to excess energy intake and weight gain.26 Additionally, a study investigated the prevalence of food cravings in pregnancy and found that food cravings may contribute to weight gain and the development of obesity in pregnancy.23 These findings are in line with our results.
In this study, no statistical association was found between food cravings and the gender of the babies. However, it is interesting to note that around 67% of mothers who craved caffeine and spicy foods gave birth to female babies. Similarly, a 2016 study published in the Journal of Human Nutrition and Dietetics also found no significant association between food cravings and the gender of the babies.23 In fact, increasing the number of participants recruited for this study may strengthen this hypothesis and establish a clearer correlation between such variables.
Furthermore, in this study, we explored the relationship between vitamins, minerals and the gender of the baby. It was observed that a significant proportion of pregnant women experiencing food cravings had mineral deficiencies, with iron deficiency being the most prevalent (40.6%). In effect, iron deficiency during pregnancy has been linked to pregnancy cravings, particularly for ice or non-food substances such as clay and chalk.27 28 This craving for non-food substances is known as pica and has been associated with iron deficiency anaemia.29 The exact mechanism behind this association is not yet fully understood, but it is thought that the body may be trying to compensate for the lack of iron by seeking out non-food substances that contain trace amounts of iron.29 However, it is important to note that not all pregnant women with iron deficiency experience pica cravings and not all women who experience pica have iron deficiency.30 Overall, while research suggests a correlation between iron deficiency and pregnancy cravings, more studies are needed to fully understand the relationship between the two. On the other hand, several previous studies discovered that vitamin D levels in plasma fluctuate during pregnancy, prepregnancy and childbirth. Vitamin D levels in plasma increase double early in pregnancy, peak in the third trimester and then return to normal or below normal during lactation.31–33 Our results revealed that vitamin D3 deficiency is the most prevalent vitamin deficiency during pregnancy among Jordanian women. It has been shown that vitamin D deficiency during pregnancy may lead to adverse pregnancy outcomes34; however, to date, there has been no direct association published between cravings during pregnancy and vitamin D deficiency.
Moreover, in this study, we examined the potential association between vitamins, minerals and the gender of the baby. Regrettably, our findings in this particular context did not demonstrate any correlation between the investigated vitamins and minerals and the gender of the baby. To provide a more definitive answer to this question, a long-term study with a larger population could be more suitable.
The study has several limitations worth considering. First, the use of convenience sampling through online questionnaires may introduce selection bias, capturing responses predominantly from certain demographic groups with better access to technology or stronger interest in the topic. This bias potentially restricts the generalisability of the findings to the broader population of pregnant women and mothers. Additionally, exclusion criteria such as non-Jordanian women and those unable to recall episodes of pregnancy cravings may further limit sample representativeness. Moreover, reliance on self-reported data introduces the possibility of response bias as participants may inaccurately recall or report information about their experiences and habits during pregnancy. Lastly, the study’s cross-sectional design restricts observation to associations at a single point in time, precluding the establishment of causality or exploration of temporal relationships between variables.
Considering the representativeness of the study sample is pivotal to understanding the generalisability of the findings. Focusing exclusively on pregnant women and mothers within a specific age range in Jordan may not accurately reflect experiences of broader populations. Additionally, the exclusion criteria and reliance on online surveys and social media recruitment may further diminish sample representativeness. Consequently, while the study offers valuable insights, its findings may not be broadly applicable. To enhance generalisability, future research should employ more diverse sampling methods and include a broader range of participants.
Conclusion
The prevalence of pregnancy cravings, specifically for food items, particularly sweets and salts, is evident among Jordanian women. These cravings are associated with factors such as the mother’s educational level, weight changes and the presence of anaemia. Furthermore, the study highlights the widespread health issues of iron and vitamin D deficiencies among women experiencing these cravings in the Jordanian context.
This research makes a significant contribution to the understanding of maternal health in Jordan, providing crucial insights into the specific factors influencing pregnancy cravings and shedding light on prevalent nutritional deficiencies among pregnant women. These findings offer valuable information for healthcare professionals, policymakers and researchers aiming to develop targeted interventions and improve maternal and fetal health outcomes in the region.
Supplementary Material
Footnotes
Contributors: SAB supervised the project. SMK and SAB collaborated in developing the questionnaire. SMK was responsible for data collection. SMK and SAB conducted the final statistical analyses and prepared the initial draft of the manuscript. SAB provided critical review, feedback and revisions to the manuscript. Both authors contributed to and approved the final version of the manuscript. SAB is the guarantor of the study.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Not required.
Ethics approval
This study involves human participants and was approved by Al-Balqa Applied University (IRB #1065/2/3/26). Data were collected through an online questionnaire, and participants had the option to choose whether or not to participate.
References
- 1.Morris W. American heritage dictionary of the English language; 1969.
- 2.Weingarten HP, Elston D. Food cravings in a college population. Appetite 1991;17:167–75. 10.1016/0195-6663(91)90019-o [DOI] [PubMed] [Google Scholar]
- 3.Weigel MM, Coe K, Castro NP, et al. Food aversions and cravings during early pregnancy: association with nausea and vomiting. Ecol Food Nutr 2011;50:197–214. 10.1080/03670244.2011.568906 [DOI] [PubMed] [Google Scholar]
- 4.Alderdice F, Lynn F, Lobel M. A review and psychometric evaluation of pregnancy-specific stress measures. J Psychosom Obstet Gynaecol 2012;33:62–77. 10.3109/0167482X.2012.673040 [DOI] [PubMed] [Google Scholar]
- 5.Orloff NC, Hormes JM. Pickles and ice cream! food cravings in pregnancy: hypotheses, preliminary evidence, and directions for future research. Front Psychol 2014;5:1076. 10.3389/fpsyg.2014.01076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fessler DM. Reproductive immunosuppression and diet: an evolutionary perspective on pregnancy sickness and meat consumption. Curr Anthropol 2002;43:19–61. 10.1086/324128 [DOI] [PubMed] [Google Scholar]
- 7.Hook EB. Dietary cravings and aversions during pregnancy. Am J Clin Nutr 1978;31:1355–62. 10.1093/ajcn/31.8.1355 [DOI] [PubMed] [Google Scholar]
- 8.Tierson FD, Olsen CL, Hook EB. Nausea and vomiting of pregnancy and association with pregnancy outcome. Am J Obstet Gynecol 1986;155:1017–22. 10.1016/0002-9378(86)90337-6 [DOI] [PubMed] [Google Scholar]
- 9.Whitehead SA, Andrews PLR, Chamberlain GVP. Characterisation of nausea and vomiting in early pregnancy: a survey of 1000 women. J Obstet Gynaecol 1992;12:364–9. 10.3109/01443619209025932 [DOI] [Google Scholar]
- 10.al-Kanhal MA, Bani IA. Food habits during pregnancy among saudi women. Int J Vitam Nutr Res 1995;65:206–10. [PubMed] [Google Scholar]
- 11.Bayley TM, Dye L, Jones S, et al. Food cravings and aversions during pregnancy: relationships with nausea and vomiting. Appetite 2002;38:45–51. 10.1006/appe.2002.0470 [DOI] [PubMed] [Google Scholar]
- 12.McKerracher L, Collard M, Henrich J. Food aversions and cravings during pregnancy on Yasawa Island, Fiji. Hum Nat 2016;27:296–315. 10.1007/s12110-016-9262-y [DOI] [PubMed] [Google Scholar]
- 13.Blau LE, Orloff N, Hormes JM. The Transdiagnostic nature of Cravings: smoking cessation and food craving in pregnancy. Midwifery 2020;87. 10.1016/j.midw.2020.102730 [DOI] [PubMed] [Google Scholar]
- 14.Mendes SG, Teixeira GP, Balieiro LCT, et al. Is the caloric midpoint associated with food cravings and food intake in pregnant women. J Am Nutr Assoc 2023;2023:1–8. 10.1080/27697061.2023.2255244 [DOI] [PubMed] [Google Scholar]
- 15.Kaiser L, Allen LH, American Dietetic Association . Position of the American dietetic association: nutrition and lifestyle for a healthy pregnancy outcome. J Am Diet Assoc 2008;108:553–61. 10.1016/j.jada.2008.01.030 [DOI] [PubMed] [Google Scholar]
- 16.Casas R, Castro Barquero S, Estruch R. Impact of sugary food consumption on pregnancy: a review. Nutrients 2020;12:3574. 10.3390/nu12113574 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Morris MJ, Na ES, Johnson AK. Salt craving: the psychobiology of pathogenic sodium intake. Physiol Behav 2008;94:709–21. 10.1016/j.physbeh.2008.04.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Worthington-Roberts B, Little RE, Lambert MD, et al. Dietary cravings and aversions in the postpartum period. J Am Diet Assoc 1989;89:647–51. [PubMed] [Google Scholar]
- 19.Pope JF, Skinner JD, Carruth BR. Cravings and aversions of pregnant adolescents. J Am Diet Assoc 1992;92:1479–82. [PubMed] [Google Scholar]
- 20.Gendall KA, Joyce PR, Sullivan PF. Impact of definition on prevalence of food cravings in a random sample of young women. Appetite 1997;28:63–72. 10.1006/appe.1996.0060 [DOI] [PubMed] [Google Scholar]
- 21.Tierson FD, Olsen CL, Hook EB. Influence of cravings and aversions on diet in pregnancy. Ecol Food Nutr 1985;17:117–29. 10.1080/03670244.1985.9990886 [DOI] [Google Scholar]
- 22.Fikrie A, Yalew A, Anato A, et al. Magnitude and effects of food cravings on nutritional status of pregnant women in Southern Ethiopia: a community-based cross sectional study. PLoS One 2022;17:e0276079. 10.1371/journal.pone.0276079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hill AJ, Cairnduff V, McCance DR. Nutritional and clinical associations of food cravings in pregnancy. J Hum Nutr Diet 2016;29:281–9. 10.1111/jhn.12333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yalew A, Tekle Silasie W, Anato A, et al. Food aversion during pregnancy and its association with nutritional status of pregnant women in boricha woreda, sidama regional state, Southern Ethiopia, 2019. A community based mixed crossectional study design. Reprod Health 2021;18:208. 10.1186/s12978-021-01258-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lee J, Allen J. Mother’s educational attainment and their young adult daughters' fast food intake: the role of race/ethnicity. Health Care Women Int 2020;41:169–87. 10.1080/07399332.2019.1669606 [DOI] [PubMed] [Google Scholar]
- 26.Myers CA, Martin CK, Apolzan JW. Food cravings and body weight: a conditioning response. Curr Opin Endocrinol Diabetes Obes 2018;25:298–302. 10.1097/MED.0000000000000434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Abu-Ouf NM, Jan MM. The impact of maternal iron deficiency and iron deficiency anemia on child’s health. Saudi Med J 2015;36:146–9. 10.15537/smj.2015.2.10289 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Malinowski AK, Murji A. Iron deficiency and iron deficiency anemia in pregnancy. CMAJ 2021;193:E1137–8. 10.1503/cmaj.210007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Means RT. Iron deficiency and iron deficiency anemia: implications and impact in pregnancy, fetal development, and early childhood parameters. Nutrients 2020;12:447. 10.3390/nu12020447 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Khairy M, Abdel-Rahman M, El-Raziky M, et al. Non-invasive prediction of hepatic fibrosis in patients with chronic HCV based on the routine pre-treatment workup. Hepat Mon 2012;12:e6718. 10.5812/hepatmon.6718 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cross NA, Hillman LS, Allen SH, et al. Calcium homeostasis and bone metabolism during pregnancy, lactation, and postweaning: a longitudinal study. Am J Clin Nutr 1995;61:514–23. 10.1093/ajcn/61.3.514 [DOI] [PubMed] [Google Scholar]
- 32.Bikle DD, Gee E, Halloran B, et al. Free 1, 25-dihydroxyvitamin D levels in serum from normal subjects, pregnant subjects, and subjects with liver disease. J Clin Invest 1984;74:1966–71. 10.1172/JCI111617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wilson SG, Retallack RW, Kent JC, et al. Serum free 1, 25‐dihydroxyvitamin D and the free 1, 25‐dihydroxyvitamin D index during a longitudinal study of human pregnancy and lactation. Clin Endocrinol (Oxf) 1990;32:613–22. 10.1111/j.1365-2265.1990.tb00905.x [DOI] [PubMed] [Google Scholar]
- 34.Chen B, Chen Y, Xu Y. Vitamin D deficiency in pregnant women: influenced by multiple risk factors and increase the risks of spontaneous abortion and small-for-gestational age. Medicine (Baltimore) 2021;100:e27505. 10.1097/MD.0000000000027505 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2023-078082supp001.pdf (2.9MB, pdf)
bmjopen-2023-078082supp002.pdf (303.5KB, pdf)
Data Availability Statement
Data are available upon reasonable request.