

Abstract
Obstructive sleep apnea and vitamin D deficiency are associated with multiple complications with increased morbidity and mortality. However, the relationship between these two entities remains unclear, with clinical studies demonstrating contradictory results. This narrative review aims to present the current evidence and understanding of this relationship and discuss the possible mechanisms linking these two disease entities. Finally, we summarize and propose areas of opportunity for future research.
Keywords: apnea hypopnea index, cholecalciferol, continuous positive airway pressure, hypoxia, obesity, sleep disorders
The relationship between obstructive sleep apnea and vitamin D deficiency remains unclear. This review presents the current evidence and understanding of this relationship and discuss the possible mechanisms linking these two entities.
1. INTRODUCTION
Obstructive sleep apnea (OSA) is a chronic disease, characterized by recurrent partial or complete upper airway collapse during sleep leading to intermittent hypoxia and sleep disruption. 1 , 2 Abrupt oxygen desaturation during sleep leads to brief arousal from sleep in order to terminate the obstruction and restore normal breathing. 3 This causes substantial sleep fragmentation and impaired sleep quality. The prevalence of OSA has been increasing over the years, especially in developed countries. 4 , 5 OSA is commonly found in patients with obesity. This is believed to be due to fat deposits in the upper airway with reduction of muscle activity in that region leading to hypopneic and apneic episodes. 6 OSA has been demonstrated as an independent risk factor for cardiovascular diseases and is associated with increased cardiovascular morbidity and mortality. 7 , 8 This might be contributed by low‐grade inflammation and production of pro‐inflammatory cytokines causing endothelial dysfunction. 9 , 10 , 11 A recent meta‐analysis demonstrated that patients with OSA have higher level of renin‐angiotensin‐aldosterone system hormones, blood pressure, and heart rate compared with those without OSA, which may add on to the increased cardiovascular risks among this cohort. 12
Although traditionally, vitamin D is thought to play its main role in calcium homeostasis and regulation, there is now increasing evidence that low vitamin D level is associated with a multitude of cardio‐metabolic complications, which has sparked new interests in these extra‐skeletal associations. 13 Hypovitaminosis D is related to increased risks of cardiovascular diseases, metabolic dysfunctions, worse cardiovascular outcomes, and elevated all‐cause mortality. 14 , 15 , 16 , 17
Vitamin D levels are associated with respiratory function. 18 OSA and vitamin D deficiency seem to share common risk factors, such as obesity and increasing age. These two conditions have almost similar pathogenesis, such as involvement of inflammatory reactions and oxidative stress, although the exact mechanism is poorly understood. To date, studies examining the relationship between these two entities have shown contradictory results. The association is likely to be bi‐directional, multi‐factorial, and complex. To better comprehend the relationship between these two entities, this review aims to summarize the current evidence and to present the possible mechanisms and understanding of this association.
2. CLINICAL STUDIES OF OSA AND VITAMIN D
2.1. Vitamin D level in OSA
Among 139 patients with OSA, vitamin D level was significantly lower compared with 30 non‐apneic cohort (17.78 ± 7.8 vs. 23.9 ± 12.4 ng/mL, p = 0.019). However, those with OSA were older and had significantly higher body mass index (BMI), neck, waist, and hip circumferences, which could have contributed to the lower level of vitamin D. 19 Nevertheless, even among BMI‐matched obese male patients, vitamin D level was still significantly lower among those with OSA compared with those without, 20 , 21 suggesting a relationship between OSA and vitamin D deficiency irrespective of weight. In addition, vitamin D level was noted to have inverse correlation with sleep stage transitions, which are indicators of sleep continuity. 19 Furthermore, the level was demonstrated to be inversely correlated with disease severity even after multi‐variate analysis, 20 , 22 , 23 , 24 , 25 , 26 , 27 suggesting the role of sleep fragmentation in vitamin D deficiency. This may be the reason why lower level of vitamin D is more pronounced in severe OSA compared with those without OSA. 23 , 24
Similarly, the number of patients with vitamin D deficiency was reported to be higher in the OSA group compared with those without OSA. 24 , 25 Although few studies found no significant difference in vitamin D level between these two cohorts, these studies still demonstrated that the number of patients with vitamin D deficiency, especially at a level of <10 mcg/dL, was higher in the OSA group, and more pronounced with increasing disease severity, compared with those without OSA. 22 , 28 , 29
2.2. Vitamin D level in elderly
The difference in vitamin D level was not apparent among the elderly cohort. Among 72 hospitalized geriatric patients with mild dementia and confirmed OSA, vitamin D level was not significantly different compared with those without OSA (p = 0.082). 30 This could be due to less severe OSA encountered in this study. Nevertheless, the level of vitamin D was demonstrated to reduce with increasing OSA severity (mild OSA 13.5 ng/mL [8.7, 31.2]; moderate OSA 7.9 ng/mL [5.3, 22.6]).
Similarly, in a community‐dwelling elderly cohort with a wide range of BMI, there was no significant difference in the prevalence of vitamin D deficiency. Besides, no association was demonstrated between vitamin D level and apnea hypopnea index (AHI). 31 Nevertheless, those with lowest quartile of vitamin D concentrations had higher odds of severe sleep apnea. Sensitivity analysis suggested that this association was largely explained by greater BMI and larger neck circumference among men with hypovitaminosis D. 32
2.3. Vitamin D level in metabolic syndrome
Among patients with type 2 diabetes, there was no demonstrated significant difference in vitamin D level between those with OSA and those without (p = 0.086). 33 However, OSA patients with metabolic syndrome had higher prevalence of vitamin D deficiency, which is most pronounced among those with severe metabolic syndrome (metabolic index >3). 34 They also had significantly lower vitamin D level compared with those without metabolic syndrome (18 ± 8.6 vs. 23.9 ± 14.1 ng/mL, p = 0.012). 35 Low vitamin D level was noted to be associated with increased abdominal obesity, elevated triglyceride level, and reduced HDL‐cholesterol level, as well as diabetes mellitus in this cohort of patients. 36
2.4. Clinical characteristics
OSA patients with vitamin D deficiency were more likely to be females, older, African Americans, with higher BMI, and larger waist circumference compared with those who were vitamin D sufficient. 25 , 36 These individuals had concurrent metabolic syndrome and diabetes mellitus. There was no correlation found between vitamin D level and excessive daytime sleepiness. 22 , 37 The threshold AHI for vitamin D deficiency was reported to be 19.3 (sensitivity 55.8%, specificity 71.8%), 24 suggesting that vitamin D deficiency is more pronounced among those with moderate to severe OSA, and the level worsens with OSA severity.
The articles reviewed are summarized in Table 1.
TABLE 1.
Summary of papers reviewed.
| Study | Design | Objectives | Samples, n | Methodology | Results | Conclusion |
|---|---|---|---|---|---|---|
| Bozkurt 2012 | Cross‐sectional |
Vitamin D status of OSA Identify potential links between lower vitamin D levels and abnormal glucose metabolism |
143 non‐diabetic OSA versus 47 non‐diabetic non‐OSA Mean age 49.7 (9.8) versus 46.03 (10.8) |
Serum 25OHD, HbA1c, insulin levels, and 75‐g OGTT evaluated in all subjects | Serum 25OHD lower among OSA compared with controls; decrement of 25OHD parallel to severity of OSA; severe female OSA lowest serum 25OHD level, male controls highest serum 25OHD level; serum 25OHD of insulin resistant subjects lower than non‐insulin resistant subjects | Vitamin D deficiency may play a role and/or worsen OSA adverse outcomes on glucose metabolism |
| Mete 2013 | Cross‐sectional | Association between serum 25OHD and disease severity in OSA |
150 OSA versus 32 non‐OSA Mean age 47.21 (8.7) versus 46.94 (8.1) |
Serum 25OHD, PTH, calcium, and phosphorus evaluated in all subjects | No significant difference in serum 25OHD between groups; patients with severe OSA had lower serum 25OHD compared with OSA of other categories and control group; number of patients with vitamin D deficiency higher in OSA group than controls | Vitamin D deficiency more pronounced with increasing OSA severity |
| Goswami 2016 | Cross‐sectional | Determine if lower 25OHD concentration is associated with greater prevalence and increased severity of OSA, independent of established OSA risk factors |
2827 community‐dwelling elderly Mean age 76.4 (5.5) |
Analysis of serum 25OHD level, demographic and comorbidity data from Outcomes of Sleep Disorders in Older Men study | Subjects with lowest quartile of serum 25OHD had greater odds of severe sleep apnea compared with highest 25OHD quartile but confounded by larger BMI and neck circumference | Association between lower 25OHD and sleep apnea among community‐dwelling elderly largely explained by confounding by larger body mass index and neck circumference |
| Kerley 2016 | Cross‐sectional | 25OHD level in OSA and possible relationships to OSA severity, sleepiness, lung function, nocturnal heart rate, and body composition |
75 urban Caucasian OSA versus 31 urban Caucasian non‐OSA Median age 54.5 |
BMI, body composition, neck circumference, sleepiness, lung function, and vitamin D status compared across OSA severity categories and non‐OSA |
25OHD inversely correlated with BMI, percent body fat, AHI, and nocturnal heart rate 25OHD independently associated with AHI and nocturnal heart rate 25OHD significantly lower in OSA than non‐OSA |
25OHD and OSA are related |
| Salepci 2017 | Cross‐sectional | 25OHD level in OSA and identify associated risk factors for vitamin D deficiency |
162 OSA versus 19 non‐OSA Mean age 49 (12) |
25OHD level evaluated in all subjects |
74% of patients had vitamin D deficiency No significant difference in 25OHD level between OSA and non‐OSA and across all OSA severity categories No association between 25OHD level and AHI or BMI |
Large proportion of patients referred for OSA evaluation had vitamin D deficiency but did not differ by OSA diagnosis and disease severity |
| Archontogeorgis 2018 | Cross‐sectional | Association between 25OHD with anthropometric and sleep characteristics of OSA and compared with non‐OSA |
139 OSA versus 30 non‐OSA Mean age 53.9 (12.8) versus 44.9 (12.8) |
Serum 25OHD level lower in OSA than non‐OSA In OSA, 25OHD level negatively correlated with sleep stage transitions, AHI, oxygen desaturation index, percentage of time with oxyhemoglobin saturation <90%, positively correlated with average oxyhemoglobin saturation during sleep, forced expiratory volume in 1 s, and oxygen partial pressure |
25OHD level lower in OSA and correlated with indices of OSA severity | |
| Archontogeorgis 2018 | Cross‐sectional | 25OHD level according to presence of MetS and its components in OSA |
55 OSA with MetS versus 52 OSA without MetS Mean age 54.8 (12) versus 51.8 (13.5) |
25OHD level evaluated in all subjects |
25OHD level lower among OSA with MetS compared with OSA without MetS 25OHD level lower in OSA with higher metabolic score |
OSA with MetS has lower 25OHD level compared with OSA without MetS |
| Pazarli 2018 | Cross‐sectional | Association between bone mineral density and 25OHD level in OSA |
75 OSA versus 21 non‐OSA Mean age 48.55 (11.8) |
BMD and 25OHD level evaluated in all subjects |
No significant difference in BMD and 25OHD level in OSA severity categories No correlation between sleep indices and BMD parameters |
No relationship between OSA and BMD values |
| Qiao 2018 | Cross‐sectional | Relationship between OSA severity and bone metabolic markers |
87 OSA (32 mild‐to‐moderate, 55 severe) versus 32 obese non‐OSA Mean age 51.8 (8.1) versus 48.2 (9.9) versus 50.1 (7.3) |
BMD, t‐P1NP, N‐MID, beta‐CTX, 25OHD, and PTH evaluated in all subjects |
No significant differences in BMD Bone markers higher in severe OSA than control 25OHD lower in OSA than control; level decreased as OSA severity increased Serum PTH higher in severe OSA then mild‐to‐moderate OSA and control AHI correlated with t‐P1NP and PTH Minimum oxygen saturation level correlated with 25OHD and PTH |
Bone markers higher in severe OSA, severity of OSA correlated with bone metabolic markers |
| Ragia 2018 | Cross‐sectional | Impact of VDR gene polymorphic variation on 25OHD concentration and susceptibility to OSA |
144 OSA versus 32 non‐OSA Mean age 53.2 (12.4) versus 47.6 (14.3) |
Human genetic variation in VDR characterized in all subjects |
FokI CC genotype frequency higher in OSA than controls VDR FokI polymorphism explained 14.5% of 25OHD concentration variability and associated with excessive daytime sleepiness |
VDR FokI polymorphism associated with vitamin D concentration in OSA Interaction of vitamin D concentration with VDR FokI polymorphism associated with OSA adjusted for other risk factors |
| Gronewold 2019 | Cross‐sectional | Prevalence and severity of sleep disordered breathing in mild dementia and associations with severity of impairment in cognition, emotional function, and mobility |
101 elderly with dementia Mean age 84.1 (6.5) |
Daytime sleepiness, medical characteristics, cognition, emotional function, and mobility assessed in all subjects | Patients with AHI ≥ 15/h often presented with heart failure and vitamin D deficiency | |
| Kirac 2019 | Cross‐sectional | Association between VDR, VDBP mutations, vitamin D level, and risk factors with OSA |
50 OSA versus 50 non‐OSA Mean age 48.82 (11.03) versus 45.86 (8.51) |
VDR and VDBP mutations investigated with qPCR | CA genotype in VDBP, CC and AA genotypes in VDR were significant in OSA | VDR and VDBP mutations highly related with OSA |
| Bouloukaki 2020 | Cross‐sectional | 25OHD levels in OSA and possible correlations with clinical and PSG parameters |
617 OSA versus 68 non‐OSA Mean age 54 (15) |
25OHD level determined in all subjects |
OSA patients lower vitamin D levels than controls Lowest levels of vitamin D and higher prevalence for vitamin D deficiency in severe OSA Severe OSA independent association with risk of vitamin D deficiency |
Large proportion of patients referred for OSA evaluation had vitamin D deficiency and independently associated with severe OSA |
| Ma 2020 | Cross‐sectional | Association of 25OHD level with severity of OSA in T2D |
106 OSA and T2D versus 30 T2D non‐OSA Mean age 49.0 (14.0) |
25OHD level determined in all subjects |
No significant differences in 25OHD in all OSA severity categories 25OHD level not correlated with AHI or risk of OSA |
25OHD level not associated with AHI or risk of OSA in T2D |
| Siachpazidou 2020 | Prospective | 25OHD level in OSA and changes after 3 and 12 months of CPAP |
30 OSA versus 30 non‐OSA Mean age 50.3 (13.8) versus 56.1 (8.1) |
25OHD level at baseline, 3 and 12 months of CPAP in OSA |
No significant difference in 25OHD between OSA and control No change in 25OHD after 3 and 12 months of CPAP CPAP‐adherence patients less reduction in 25OHD compared with non‐adherent patients after 1 year 25OHD level correlated with higher daily CPAP usage at 3 and 12 months |
Good CPAP adherence and high daily CPAP usage positively affected 25OHD level in OSA |
| Bhatt 2021 | Cross‐sectional | Significance of vitamin D, PTH, VDR, PTH gene polymorphisms with body composition, and biochemical investigations in Asian Indian OSA |
120 OSA and obese versus 110 obese non‐OSA versus 70 non‐obese non‐OSA Mean age 43.5 (10.6) versus 42.6 (9.6) versus 42.6 (8.6) |
VDR and PTH genotyping with qPCR Clinical, body composition, anthropometry, and biochemical investigations |
OSA and obese lower 25OHD level, higher PTH level Indirect correlation between 25OHD level and OSA severity VDR and PTH genes significantly associated with OSA VDR haplotype combination variants more frequent in OSA and obesity |
Lower 25OHD level in OSA and correlate with disease severity VDR and PTH mutations highly related with OSA in Asian Indians |
| Sadaf 2021 | Prospective | Effect of OSA on BMD and serum 25OHD level |
59 OSA versus 34 non‐OSA Mean age 48.02 (4.35) versus 46.35 (7.29) |
BMD and 25OHD level assessed in all subjects |
Lower BMD and 25OHD level in OSA than control Negative correlation between AHI and BMD, AHI and 25OHD level |
OSA affects BMD |
Abbreviations: 25OHD, 25‐hydroxyvitamin D; AHI, apnea hypopnea index; beta‐CTX, beta‐C‐terminal telopeptide of type 1 collagen; BMD, bone mineral density; BMI, body mass index; CPAP, continuous positive airway pressure; MetS, metabolic syndrome; Mod, moderate; N‐MID, N‐terminal midfragment of osteocalcin; OGTT, oral glucose tolerance test; OSA, obstructive sleep apnea; PSG, polysomnography; PTH, parathyroid hormone; T2DM, type 2 diabetes mellitus; t‐P1NP, total procollagen type 1 N‐terminal propeptide; VDD, vitamin D deficiency; VDR, vitamin D receptor; VDBP, vitamin D binding protein.
2.5. Outcome of continuous positive airway pressure (CPAP) treatment on vitamin D level
Although treatment with CPAP among patients with moderate to severe OSA for 12 weeks did not significantly alter vitamin D level, some changes were seen at 24 weeks among those with severe OSA and with excessive sleepiness. 38 This suggests that CPAP may have late beneficial effect and exerts more benefit on vitamin D level particularly among those with severe OSA. Nevertheless, the median vitamin D level of this cohort falls within the sufficient range of 50.9 ng/mL, which may explain the non‐significant difference seen with CPAP treatment.
Further improvement of vitamin D level was demonstrated among male OSA patients who initially responded well to a year of adequate CPAP therapy usage. 39 These findings were consistent with another study that demonstrated that vitamin D levels were positively correlated with higher daily CPAP usage, especially among those who were adherent to CPAP therapy. 40 , 41 This suggests that improving hypoxia by normalizing nocturnal oxygen saturation may positively affect vitamin D level.
The studies examining effect of CPAP treatment on vitamin D level among patients with OSA are summarized in Table 2.
TABLE 2.
Effect of CPAP on 25OHD level among OSA.
| Study | Samples, n | CPAP duration | Findings |
|---|---|---|---|
| Haglow 2018 |
34 Mean AHI 39.9 |
24 weeks | Significant improvement of 25OHD |
| Liguori 2015 |
90 Mean AHI 49.7 |
Seven nights |
Significant improvement of vitamin D level in male OSA responders (residual AHI < 5 and CPAP usage >4 h per night) |
| Liguori 2017 |
39 Mean AHI 47.8 |
1 year (extension study from Liguori 2015) |
Significant improvement of 25OHD Obese OSA more frequently shifted from vitamin D level <20 to >20 ng/mL compared with non‐obese OSA Positive association between change in vitamin D level and BMI |
| Siachpazidou 2020 |
30 Mean AHI 40.4 |
1 year |
No significant improvement of 25OHD Patients with good CPAP adherence had higher 25OHD after 1 year compared with non‐adherent group Vitamin D level correlated with higher daily CPAP usage at 3 and 12 months |
Abbreviations: 25OHD, 25‐hydroxyvitamin D; AHI, apnea hypopnea index; BMI, body mass index; CPAP, continuous positive airway pressure; Mod, moderate; OSA, obstructive sleep apnea.
2.6. Outcome of vitamin D supplementation on OSA severity
The data of vitamin D supplementation use in patients with OSA are limited. There are only two studies identified, and both were limited by small sample sizes. Among 19 male patients with mild OSA who were not on CPAP, the use of vitamin D3 at 50 000 IU a week for total of 8 weeks significantly reduced OSA severity in terms of oxygen desaturation index, AHI, hypopnea index, and the number of OSA patients. 42 The second study evaluated the use of vitamin D3 at 4000 IU per day (n = 10) versus placebo (n = 9) for 15 weeks among patients with OSA of different severity categories and heterogenous CPAP usage. Significant improvement in LDL and lipoprotein‐associated phospholipase A2 was observed; however, post‐intervention OSA severity was not assessed. 43 In this respect, more robust studies are needed to study the effect of adequate vitamin D supplementation in patients with OSA.
3. POSSIBLE MECHANISMS
3.1. OSA causing vitamin D deficiency
3.1.1. Sleep duration and sun exposure
Sun exposure is essential in initiation of cutaneous vitamin D synthesis. However, patients with OSA experience nocturnal hypoxia and sleep fragmentation, which may lead to daytime drowsiness and fatigue. This may cause reduction in outdoor activities, leading to lack of sun exposure with subsequent reduction in vitamin D synthesis. 44 Indoor workers are consistently reported to experience vitamin D insufficiency or deficiency, suggesting the lack of exposure to ultraviolet light leading to reduction in vitamin D level. 45 In addition, short sleep duration of less than 6 h a night secondary to sleep fragmentation was reported to be associated with lower level of vitamin D. These individuals have twice increased odds of having vitamin D deficiency, independent of age, gender, seasonality, BMI, and ethnicity. 46 , 47
On the other hand, vitamin D deficiency, especially at a level of <20 ng/mL (<50 nmol/L), was shown to be associated with increased risk of sleep disorders, including poor sleep quality, shorter sleep duration, and sleepiness, 48 which could contribute to worsening of OSA. The use of vitamin D supplementation among patients with sleep disorders led to significant improvement of sleep quality, reduction of sleep latency, and increment of sleep duration. 49 , 50 This further strengthens the relationship between vitamin D deficiency and sleep disorders.
Older adults generally have lower vitamin D levels as old age is an independent risk factor for vitamin D deficiency. 51 , 52 , 53 , 54 The decline of vitamin D level in the aging process is associated with reduction in skin production of vitamin D, decreased vitamin D receptor (VDR), and reduced ability of renal production of active vitamin D. 55 This may explain the non‐significant difference seen between those with OSA and those without among the elderly.
3.1.2. Hypoxia
The association between vitamin D deficiency and OSA is also believed to be related to hypoxia involving hypoxia‐inducible factor 1‐α (HIF1‐α). 40 HIF1‐α is the main factor for oxygen metabolism homeostasis, and its expression is shown to increase in OSA. 56 The use of vitamin D3 reduced protein expression, transcriptional activity, and target genes of HIF1‐α in various human cancer cells, 57 substantiating the relationship between vitamin D deficiency and hypoxia. This is further proven with clinical studies, which demonstrated improvement of vitamin D level with attenuation of hypoxia in patients with OSA treated adequately with CPAP therapy. 38 , 39 , 40 , 41
3.1.3. Obesity
A high proportion of patients with OSA are overweight or obese. Observational studies have demonstrated the relationship between low vitamin D level and obesity to be bi‐directional. 58 Vitamin D deficiency increases risk of obesity, whereas obesity lowers vitamin D level. Being fat‐soluble, vitamin D is predominantly stored in adipose tissue. Moreover, VDR and the enzymes involved in producing the active form of vitamin D are also expressed in these adipose tissues. 40 Vitamin D is thus believed to be trapped in the adipose tissue, leading to reduced bioavailability and hence low level of vitamin D in the blood. 59 This is also contributed by an increased catabolism of vitamin D by local action of 24‐hydroxylase enzyme found in human adipose tissue. 27 In contrast, some believe that volumetric dilution of vitamin D, instead of sequestration, in the large adipose stores was the reason leading to low serum vitamin D level. 60 Nevertheless, both theories suggest that obesity plays an important role in vitamin D deficiency in patients with OSA. This is worsened by chronically raised abdominal pressure seen in those who are obese, which may also lead to gastro‐esophageal reflux and gastric ischemia, thereby affecting vitamin D absorption causing vitamin D deficiency. 27 , 61
Leptin is a type of adipokine that is a pro‐inflammatory factor predominantly formed by adipose cells. Increment of adipose tissue volume seen in obesity leads to adipocyte hypertrophy, which subsequently causes increment of leptin production. 62 High levels of leptin were shown to impair vitamin D metabolism by attenuating gene expression responsible for the activation of vitamin D. 63
On the other hand, the active form of vitamin D modulates adipogenesis and regulates adipocyte differentiation by binding to the nuclear VDR with high affinity. 64 Hence, a low vitamin D level causes adipose tissue dysregulation leading to obesity and thus increases the risk of OSA. 65 The use of active vitamin D in both animal and human tissues inhibited adipocyte differentiation, 64 depicting the role for low vitamin D status in development of obesity.
3.1.4. Metabolic syndrome
Vitamin D level is inversely associated with the presence of metabolic syndrome. 66 , 67 Low vitamin D status could magnify the adverse effects of obesity on the metabolic variables, including insulin resistance and hypertension. 36 , 68 Vitamin D‐deficient rats exhibited close to 50% reduction in insulin secretion compared with those which were replenished with activated vitamin D. 69 Pancreatic β cells express VDR, and the activated form of vitamin D is shown to stimulate insulin secretion. 70 Some longitudinal and observational studies have also demonstrated that low levels of vitamin D predict the risk of type 2 diabetes in Europeans, African Americans, South Asians, and native American children, suggesting that the evolution of diabetes may be influenced by low vitamin D level. 71 , 72 , 73 This may explain why there is no difference seen in vitamin D level between diabetic patients with and without OSA, as vitamin D deficiency is commonly seen in patients with type 2 diabetes regardless of age, gender, and insulin treatment. 33
Besides, vitamin D and VDR are demonstrated to be directly involved in the modulation and inflammatory pathways leading to the development of metabolic‐associated fatty liver disease (MAFLD), especially among the overweight and obese cohort. 74 This occurs via liver homeostasis, intra‐hepatic regulation of insulin sensitivity, fat accumulation, and gut homeostasis. 74 On the other hand, liver disease also impairs protein synthesis and reduces production of vitamin D binding protein (VDBP), leading to a decreased total vitamin D level. 75 As patients with OSA and metabolic syndrome are at higher risk of MAFLD, the reduction of vitamin D synthesis and VDBP could contribute to development of vitamin D deficiency. 76 , 77
The development of chronic kidney disease from the presence of concurrent diabetes and hypertension may also influence vitamin D status and function. 78 With deteriorating kidney function, there is a slow progressive decline in active vitamin D level due to reduction in renal mass, decreased glomerular filtration rate, and effect of fibroblast growth factor‐23 on the synthesis of active vitamin D. 79 The transport capacity for VDBP from the glomerular filtrate into the renal tubules is similarly reduced in chronic kidney disease. 75
3.1.5. Autonomic dysfunction
In healthy individuals, sympathetic neural activity decreases with a concurrent rise in parasympathetic activity during sleep. 80 However, in patients with OSA, upper airway obstruction and hypopnea are postulated to cause autonomic dysfunction, 81 with abnormal parasympathetic activity persisting beyond sleep. 82 As vagal nervous system plays a major role in gastrointestinal motility, abnormal parasympathetic activity in patients with OSA is believed to cause reduction in gastrointestinal motility and gastrointestinal hormone secretion leading to reduced vitamin D absorption. 44 , 83
3.2. Vitamin D deficiency worsening OSA
3.2.1. VDR gene polymorphism
VDRs are widely distributed throughout many tissues, including the brain regions, which are involved in sleep regulation. 84 , 85 Patients with OSA were found to have higher frequency of VDR FokI CC genotype, which was associated with lower vitamin D level, compared with non‐OSA controls. 86 In logistic regression analysis, the interaction of vitamin D with VDR FokI polymorphism was associated with higher risk of OSA occurrence after adjustment for various risk factors. 86 Furthermore, VDR FokI polymorphism could affect severity of OSA symptoms. A higher frequency of VDR FokI CC genotype was found in OSA patients with excessive daytime sleepiness. 86 Nevertheless, VDR activity may be confounded by ethnic variation. 86 , 87 In Asian and African populations, those with TT genotype were the ones associated with lower vitamin D level. 88 , 89 , 90 , 91 The underlying mechanism of this difference remains unclear.
3.2.2. Vitamin D and skeletal muscle
Vitamin D plays a role in active calcium transportation into muscle via Ca‐ATPase, as well as regulating muscular contractions. 92 Muscle weakness is one of the prominent features of vitamin D insufficiency. Chronically low vitamin D level may cause non‐inflammatory myopathy of upper airway muscle due to impaired cellular calcium transportation into the sarcoplasmic reticulum and mitochondria. 84 This leads to reduced pharyngeal patency and predisposes patients to apneic events during sleep. 93 Besides, vitamin D deficiency is reported to increase the risk of nasal airflow restriction, 84 hence further worsening sleep apnea.
3.2.3. Inflammatory cytokines
Chronic variations in vitamin D levels also affect humoral mechanisms as vitamin D harbors immuno‐modulatory properties. 94 A deficient in this vitamin causes immune dysregulation leading to a rise in inflammatory cytokines, including TNF‐α, which is shown to affect sleep architecture by enhancing slow‐wave sleep. 84 , 95 In healthy women, this cytokine was demonstrated to be inversely related to serum vitamin D level. 96 Interleukin‐17 (IL‐17), a pro‐inflammatory cytokine, was also found to be significantly elevated in patients with severe OSA compared with non‐OSA controls. 97 A negative correlation was demonstrated between IL‐17 and vitamin D level among those with severe OSA. 97 Additionally, people who have inadequate vitamin D are found to have increased risk of infection and inflammation of upper and lower airway. 84 This can cause adeno‐tonsillar hypertrophy, which can worsen airway obstruction in patients with OSA.
The proposed mechanisms of the bidirectional relationship are summarized in Figure 1.
FIGURE 1.
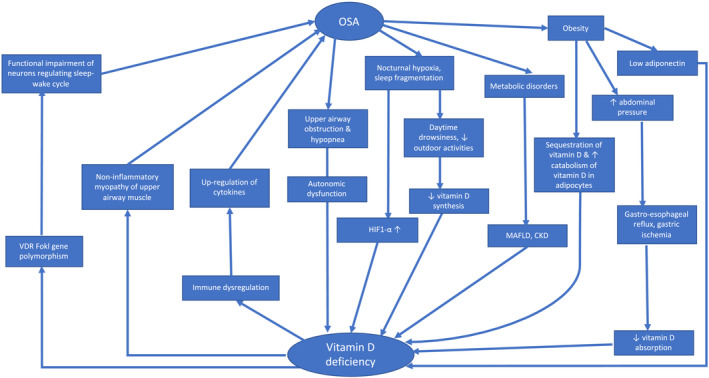
Relationship between obstructive sleep apnea and vitamin D deficiency. CKD, chronic k; HIF1‐α, hypoxia‐inducible factor 1‐alpha; MAFLD, metabolic‐associated fatty liver disease; OSA, obstructive sleep apnea; VDR, vitamin D receptor.
4. RESEARCH GAPS AND FUTURE DIRECTION
Despite the comprehensive summary of the clinical studies and possible mechanisms linking OSA and vitamin D deficiency, there remains gaps in the current literature in this area. Both of these increasingly common diseases are closely related to increased cardio‐metabolic risks with increased morbidity and mortality. 98 , 99 It remains unclear whether vitamin D deficiency is a risk factor for OSA or whether OSA is a risk factor for vitamin D deficiency, and the role of other confounding factors in these two disease entities. As clear relationship between OSA and vitamin D deficiency is yet to be established, larger prospective studies to examine the link between the two are needed. This is necessary to better understand the relationship, mechanism of vitamin D deficiency in patients with OSA, and the correlation between vitamin D levels and severity of OSA.
The effect of VDR and VDBP gene polymorphism in OSA remains unclear. Hence, research is needed to examine the role of VDR and VDBP genetic variants and possibly their mutations in OSA severity and OSA‐related metabolic disorders. Inter‐ethnic variations in this genetic polymorphism and mutations are also needed to understand the difference observed in the FokI genotype in different ethnic groups.
Other plausible mechanisms that warrant more robust future research include inflammatory pathways involved, associations with adipokines, and the role of autonomic dysfunction linking OSA and vitamin D deficiency.
Furthermore, the use of vitamin D supplement in the OSA cohort is very limited. Hence, prospective studies with bigger sample sizes are essential to determine the effect of vitamin D, as well as the dose and duration needed to bring benefits to patients with OSA. There is a lack of evidence in the role of vitamin D in improving OSA severity; whether vitamin D supplementation would alter the course of OSA, as well as its related metabolic disturbances, such as diabetes mellitus, hypertension, and dyslipidemia remains unanswered. Although current evidence suggests beneficial effects of CPAP therapy on vitamin D levels in patients with OSA, long‐term studies are lacking to better understand the benefits of CPAP on cardiovascular morbidity and mortality outcomes beyond improvement of vitamin D levels in these patients.
5. CONCLUSION
The present review aimed to collect and put into perspective current available literature regarding the association between OSA and vitamin D level. It focused on the potential relationship between these two entities and presented evidence for potential causal links and underlying mechanisms. Current evidence suggests a relationship between OSA and low levels of vitamin D via inflammatory and non‐inflammatory pathways, genetic polymorphisms of VDR and VDBP, and autonomic nervous system. The coexistence of obesity and hence increased adipose tissue contributes to the sequestration and catabolism of vitamin D and impaired adipokine function. Hypoxia secondary to sleep fragmentation leading to reduced outdoor activities and sun exposure may play a role linking these two disease entities as well. The presence of liver and kidney disease associated with metabolic disorders seen in these patients can lead to lower vitamin D level. Nevertheless, further robust prospective studies with larger sample sizes are needed to examine this link and the long‐term beneficial effect of OSA‐directed therapy in increasing vitamin D level. It is essential to determine the role of vitamin D supplementation in improving OSA severity and altering the course of OSA. Because untreated OSA and vitamin D deficiency independently lead to increased cardiovascular morbidity and mortality, early recognition through effective screening and diagnosis and a timely targeted treatment are necessary to reduce the risk of adverse sequelae related to OSA and vitamin D deficiency.
AUTHOR CONTRIBUTIONS
Huai Heng Loh conceived and designed the work; Norlela Sukor revised it critically for important intellectual content. Both authors read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
CONFLICT OF INTEREST
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials described in this manuscript.
ETHICS APPROVAL/PATIENT CONSENT
This article does not contain any studies with human participants performed by any of the authors.
ACKNOWLEDGMENTS
The authors would like to thank Universiti Malaysia Sarawak (UNIMAS) and National Universiy of Malaysia (UKM) for the financial support in the form of UNIMAS IMPACT Research Grant (F05/IMPACT/2122/2021) and the UKM Research Grant (FF‐2022‐066).
Loh HH, Sukor N. Obstructive sleep apnea and vitamin D level: Has the dust settled? Clin Respir J. 2024;18(3):e13593. doi: 10.1111/crj.13593.
Funding Information Universiti Malaysia Sarawak (UNIMAS) and National University of Malaysia (UKM) provided financial support in the form of UNIMAS IMPACT Research Grant (F05/IMPACT/2122/2021) and the UKM Research Grant (FF‐2022‐066), respectively. The sponsors had no role in the design or conduct of this review paper.
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
REFERENCES
- 1. Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long‐term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263‐276. doi: 10.5664/jcsm.27497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Rundo JV. Obstructive sleep apnea basics. Cleve Clin J Med. 2019;86(9 Suppl 1):2‐9. doi: 10.3949/ccjm.86.s1.02 [DOI] [PubMed] [Google Scholar]
- 3. Goyal M, Johnson J. Obstructive sleep apnea diagnosis and management. Mo Med. 2017;114(2):120‐124. [PMC free article] [PubMed] [Google Scholar]
- 4. Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population—a review on the epidemiology of sleep apnea. J Thorac Dis. 2015;7(8):1311‐1322. doi: 10.3978/j.issn.2072-1439.2015.06.11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Lykouras D, Theodoropoulos K, Sampsonas F, et al. The impact of obstructive sleep apnea syndrome on renin and aldosterone. Eur Rev Med Pharmacol Sci. 2015;19(21):4164‐4170. [PubMed] [Google Scholar]
- 6. Jehan S, Zizi F, Pandi‐Perumal SR, et al. Obstructive sleep apnea and obesity: implications for public health. Sleep Med Disord. 2017;1(4):00019. [PMC free article] [PubMed] [Google Scholar]
- 7. Parati G, Lombardi C, Hedner J, et al. Position paper on the management of patients with obstructive sleep apnea and hypertension: joint recommendations by the European Society of Hypertension, by the European Respiratory Society and by the members of European COST (COoperation in Scientific and Technological research) ACTION B26 on obstructive sleep apnea. J Hypertens. 2012;30(4):633‐646. doi: 10.1097/HJH.0b013e328350e53b [DOI] [PubMed] [Google Scholar]
- 8. Gottlieb DJ, Yenokyan G, Newman AB, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation. 2010;122(4):352‐360. doi: 10.1161/CIRCULATIONAHA.109.901801 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Unnikrishnan D, Jun J, Polotsky V. Inflammation in sleep apnea: an update. Rev Endocr Metab Disord. 2015;16(1):25‐34. doi: 10.1007/s11154-014-9304-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Garvey JF, Taylor CT, McNicholas WT. Cardiovascular disease in obstructive sleep apnoea syndrome: the role of intermittent hypoxia and inflammation. Eur Respir J. 2009;33(5):1195‐1205. doi: 10.1183/09031936.00111208 [DOI] [PubMed] [Google Scholar]
- 11. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736‐747. doi: 10.1016/S0140-6736(13)60734-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Loh HH, Lim QH, Chai CS, et al. Influence and implications of the renin‐angiotensin‐aldosterone system in obstructive sleep apnea: an updated systematic review and meta‐analysis. J Sleep Res. 2022;32(1):e13726. doi: 10.1111/jsr.13726 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Charoenngam N, Shirvani A, Holick MF. Vitamin D for skeletal and non‐skeletal health: what we should know. J Clin Orthop Trauma. 2019;10(6):1082‐1093. doi: 10.1016/j.jcot.2019.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Dobnig H, Pilz S, Scharnagl H, et al. Independent association of low serum 25‐hydroxyvitamin d and 1,25‐dihydroxyvitamin d levels with all‐cause and cardiovascular mortality. Arch Intern Med. 2008;168(12):1340‐1349. doi: 10.1001/archinte.168.12.1340 [DOI] [PubMed] [Google Scholar]
- 15. Liu LC, Voors AA, van Veldhuisen DJ, et al. Vitamin D status and outcomes in heart failure patients. Eur J Heart Fail. 2011;13(6):619‐625. doi: 10.1093/eurjhf/hfr032 [DOI] [PubMed] [Google Scholar]
- 16. Ginde AA, Scragg R, Schwartz RS, Camargo CA Jr. Prospective study of serum 25‐hydroxyvitamin D level, cardiovascular disease mortality, and all‐cause mortality in older U.S. adults. J Am Geriatr Soc. 2009;57(9):1595‐1603. doi: 10.1111/j.1532-5415.2009.02359.x [DOI] [PubMed] [Google Scholar]
- 17. Lavie CJ, Dinicolantonio JJ, Milani RV, O'Keefe JH. Vitamin D and cardiovascular health. Circulation. 2013;128(22):2404‐2406. doi: 10.1161/CIRCULATIONAHA.113.002902 [DOI] [PubMed] [Google Scholar]
- 18. Black PN, Scragg R. Relationship between serum 25‐hydroxyvitamin d and pulmonary function in the third national health and nutrition examination survey. Chest. 2005;128(6):3792‐3798. doi: 10.1378/chest.128.6.3792 [DOI] [PubMed] [Google Scholar]
- 19. Archontogeorgis K, Nena E, Papanas N, Steiropoulos P. The role of vitamin D in obstructive sleep apnoea syndrome. Breathe. 2018;14(3):206‐215. doi: 10.1183/20734735.000618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Qiao Y, Wang B, Yang JJ, et al. Bone metabolic markers in patients with obstructive sleep apnea syndrome. Chin Med J (Engl). 2018;131(16):1898‐1903. doi: 10.4103/0366-6999.238149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Bhatt SP, Guleria R, Vikram NK. The effect of the severity of obstructive sleep apnea on leukocyte telomere length, 25 hydroxy vitamin D, and parathyroid hormonal concentrations in Asian Indians. Front Neurol. 2021;12:682739. doi: 10.3389/fneur.2021.682739 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Kerley CP, Hutchinson K, Bolger K, McGowan A, Faul J, Cormican L. Serum vitamin D is significantly inversely associated with disease severity in Caucasian adults with obstructive sleep apnea syndrome. Sleep. 2016;39(2):293‐300. doi: 10.5665/sleep.5430 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Bozkurt NC, Cakal E, Sahin M, Ozkaya EC, Firat H, Delibasi T. The relation of serum 25‐hydroxyvitamin‐D levels with severity of obstructive sleep apnea and glucose metabolism abnormalities. Endocrine. 2012;41(3):518‐525. doi: 10.1007/s12020-012-9595-1 [DOI] [PubMed] [Google Scholar]
- 24. Mete T, Yalcin Y, Berker D, et al. Obstructive sleep apnea syndrome and its association with vitamin D deficiency. J Endocrinol Invest. 2013;36(9):681‐685. doi: 10.3275/8923 [DOI] [PubMed] [Google Scholar]
- 25. Bouloukaki I, Tsiligianni I, Mermigkis C, et al. Vitamin D deficiency in patients evaluated for obstructive sleep apnea: is it associated with disease severity? Sleep Breath. 2021;25(2):1109‐1117. doi: 10.1007/s11325-020-02142-w [DOI] [PubMed] [Google Scholar]
- 26. Sadaf S, Shameem M, Siddiqi SS, Anwar S, Mohd S. Effect of obstructive sleep apnea on bone mineral density. Turk Thorac J. 2021;22(4):301‐310. doi: 10.5152/TurkThoracJ.2021.20051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Archontogeorgis K, Nena E, Papanas N, et al. Vitamin D levels in middle‐aged patients with obstructive sleep apnoea syndrome. Curr Vasc Pharmacol. 2018;16(3):289‐297. doi: 10.2174/1570161115666170529085708 [DOI] [PubMed] [Google Scholar]
- 28. Siachpazidou DI, Stavrou V, Zouridis S, et al. 25‐Hydroxyvitamin D levels in patients with obstructive sleep apnea and continuous positive airway pressure treatment: a brief review. Sleep Sci. 2020;13(1):78‐83. doi: 10.5935/1984-0063.20190126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Salepci B, Caglayan B, Nahid P, et al. Vitamin D deficiency in patients referred for evaluation of obstructive sleep apnea. J Clin Sleep Med. 2017;13(4):607‐612. doi: 10.5664/jcsm.6554 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Gronewold J, Haensel R, Kleinschnitz C, Frohnhofen H, Hermann DM. Sleep‐disordered breathing in hospitalized geriatric patients with mild dementia and its association with cognition, emotion and mobility. Int J Environ Res Public Health [Electronic Resource]. 2019;16(5):863. doi: 10.3390/ijerph16050863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Goswami U, Ensrud KE, Paudel ML, et al. Vitamin D concentrations and obstructive sleep apnea in a multicenter cohort of older males. Ann Am Thorac Soc. 2016;13(5):712‐718. doi: 10.1513/AnnalsATS.201507-440OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Goswami U, Ensrud KE, Paudel ML, et al. Vitamin D concentrations and obstructive sleep apnea in a multicenter cohort of older males. Ann Am Thorac Soc. 2016;13(5):712‐718. doi: 10.1513/AnnalsATS.201507-440OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Ma D, Zheng X, Dong L, et al. The relationship of serum 25‐hydroxyvitamin‐D level with severity of obstructive sleep apnea in patients with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2020;13:1391‐1398. doi: 10.2147/DMSO.S250694 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Barcelo A, Elorza MA, Barbe F, Santos C, Mayoralas LR, Agusti AG. Angiotensin converting enzyme in patients with sleep apnoea syndrome: plasma activity and gene polymorphisms. Eur Respir J. 2001;17(4):728‐732. doi: 10.1183/09031936.01.17407280 [DOI] [PubMed] [Google Scholar]
- 35. Archontogeorgis K, Nena E, Papanas N, et al. Metabolic syndrome and vitamin D levels in patients with obstructive sleep apnea syndrome. Metab Syndr Relat Disord. 2018;16(4):190‐196. doi: 10.1089/met.2017.0181 [DOI] [PubMed] [Google Scholar]
- 36. Barcelo A, Esquinas C, Pierola J, et al. Vitamin D status and parathyroid hormone levels in patients with obstructive sleep apnea. Respiration. 2013;86(4):295‐301. doi: 10.1159/000342748 [DOI] [PubMed] [Google Scholar]
- 37. Šiarnik P, Jurík M, Hardoňová M, et al. Excessive daytime sleepiness in sleep apnea: any role of testosterone or vitamin D? Physiol Res. 2020;69(5):907‐917. doi: 10.33549/physiolres.934507 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Theorell‐Haglow J, Hoyos CM, Phillips CL, et al. Changes of vitamin D levels and bone turnover markers after CPAP therapy: a randomized sham‐controlled trial. J Sleep Res. 2018;27(4):e12606. doi: 10.1111/jsr.12606 [DOI] [PubMed] [Google Scholar]
- 39. Liguori C, Romigi A, Izzi F, et al. Continuous positive airway pressure treatment increases serum vitamin D levels in male patients with obstructive sleep apnea. J Clin Sleep Med. 2015;11(6):603‐607. doi: 10.5664/jcsm.4766 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Siachpazidou DI, Kotsiou OS, Stavrou V, et al. Serum vitamin D levels in patients with obstructive sleep apnea syndrome and level changes after continuous positive airway pressure therapy. Sleep Breath. 2021;25(2):657‐668. doi: 10.1007/s11325-020-02146-6 [DOI] [PubMed] [Google Scholar]
- 41. Liguori C, Izzi F, Mercuri NB, et al. Vitamin D status of male OSAS patients improved after long‐term CPAP treatment mainly in obese subjects. Sleep Med. 2017;29:81‐85. doi: 10.1016/j.sleep.2016.08.022 [DOI] [PubMed] [Google Scholar]
- 42. Ayyildiz F, Yildiran H, Afandiyeva N, Gulbahar O, Kokturk O. The effects of vitamin D supplemantation on prognosis in patients with mild obstructive sleep apnea syndrome. Turk J Med Sci. 2021;51(5):2524‐2533. doi: 10.3906/sag-2101-83 [DOI] [PubMed] [Google Scholar]
- 43. Kerley CP, Hutchinson K, Bramham J, McGowan A, Faul J, Cormican L. Vitamin D improves selected metabolic parameters but not neuropsychological or quality of life indices in OSA: a pilot study. J Clin Sleep Med. 2017;13(1):19‐26. doi: 10.5664/jcsm.6378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Maniero C, Fassina A, Guzzardo V, et al. Primary hyperparathyroidism with concurrent primary aldosteronism. Hypertension. 2011;58(3):341‐346. doi: 10.1161/HYPERTENSIONAHA.111.173948 [DOI] [PubMed] [Google Scholar]
- 45. Coppeta L, Papa F, Magrini A. Are shiftwork and indoor work related to D3 vitamin deficiency? A systematic review of current evidences. J Environ Public Health. 2018;2018:8468742. doi: 10.1155/2018/8468742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Bertisch SM, Sillau S, de Boer IH, Szklo M, Redline S. 25‐Hydroxyvitamin D concentration and sleep duration and continuity: multi‐ethnic study of atherosclerosis. Sleep. 2015;38(8):1305‐1311. doi: 10.5665/sleep.4914 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. de Oliveira DL, Dokkedal‐Silva V, Fernandes GL, Kim LJ, Tufik S, Andersen ML. Sleep duration as an independent factor associated with vitamin D levels in the EPISONO cohort. J Clin Sleep Med. 2021;17(12):2439‐2449. doi: 10.5664/jcsm.9452 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Gao Q, Kou T, Zhuang B, Ren Y, Dong X, Wang Q. The association between vitamin D deficiency and sleep disorders: a systematic review and meta‐analysis. Nutrients. 2018;10(10):1395. doi: 10.3390/nu10101395 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Huang W, Shah S, Long Q, Crankshaw AK, Tangpricha V. Improvement of pain, sleep, and quality of life in chronic pain patients with vitamin D supplementation. Clin J Pain. 2013;29(4):341‐347. doi: 10.1097/AJP.0b013e318255655d [DOI] [PubMed] [Google Scholar]
- 50. Mohammad Shahi M, Hosseini SA, Helli B, Haghighyzade MH, Abolfathi M. The effect of vitamin D supplement on quality of sleep in adult people with sleep disorders. Tehran Univ Med J. 2017;75(6):443‐448. [Google Scholar]
- 51. Chen J, Yun C, He Y, Piao J, Yang L, Yang X. Vitamin D status among the elderly Chinese population: a cross‐sectional analysis of the 2010‐2013 China national nutrition and health survey (CNNHS). Nutr J. 2017;16(1):3. doi: 10.1186/s12937-016-0224-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Forrest KY, Stuhldreher WL. Prevalence and correlates of vitamin D deficiency in US adults. Nutr Res. 2011;31(1):48‐54. doi: 10.1016/j.nutres.2010.12.001 [DOI] [PubMed] [Google Scholar]
- 53. Wei J, Zhu A, Ji JS. A comparison study of vitamin D deficiency among older adults in China and the United States. Sci Rep. 2019;9(1):19713. doi: 10.1038/s41598-019-56297-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Kweder H, Eidi H. Vitamin D deficiency in elderly: risk factors and drugs impact on vitamin D status. Avicenna J Med. 2018;8(4):139‐146. doi: 10.4103/ajm.AJM_20_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Gallagher JC. Vitamin D and aging. Endocrinol Metab Clin North Am. 2013;42(2):319‐332. doi: 10.1016/j.ecl.2013.02.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Gabryelska A, Szmyd B, Szemraj J, Stawski R, Sochal M, Bialasiewicz P. Patients with obstructive sleep apnea present with chronic upregulation of serum HIF‐1alpha protein. J Clin Sleep Med. 2020;16(10):1761‐1768. doi: 10.5664/jcsm.8682 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Ben‐Shoshan M, Amir S, Dang DT, Dang LH, Weisman Y, Mabjeesh NJ. 1Alpha,25‐dihydroxyvitamin D3 (calcitriol) inhibits hypoxia‐inducible factor‐1/vascular endothelial growth factor pathway in human cancer cells. Mol Cancer Ther. 2007;6(4):1433‐1439. doi: 10.1158/1535-7163.MCT-06-0677 [DOI] [PubMed] [Google Scholar]
- 58. Bennour I, Haroun N, Sicard F, Mounien L, Landrier JF. Vitamin D and obesity/adiposity–a brief overview of recent studies. Nutrients. 2022;14(10):2049. doi: 10.3390/nu14102049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Dix CF, Barcley JL, Wright ORL. The role of vitamin D in adipogenesis. Nutr Rev. 2018;76(1):47‐59. doi: 10.1093/nutrit/nux056 [DOI] [PubMed] [Google Scholar]
- 60. Drincic AT, Armas LA, Van Diest EE, Heaney RP. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity (Silver Spring). 2012;20(7):1444‐1448. doi: 10.1038/oby.2011.404 [DOI] [PubMed] [Google Scholar]
- 61. Yong CY, Reynaud E, Forhan A, et al. Cord‐blood vitamin D level and night sleep duration in preschoolers in the EDEN mother‐child birth cohort. Sleep Med. 2019;53:70‐74. doi: 10.1016/j.sleep.2018.09.017 [DOI] [PubMed] [Google Scholar]
- 62. Zakharova I, Klimov L, Kuryaninova V, et al. Vitamin D insufficiency in overweight and obese children and adolescents. Front Endocrinol (Lausanne). 2019;10:103. doi: 10.3389/fendo.2019.00103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Matsunuma A, Horiuchi N. Leptin attenuates gene expression for renal 25‐hydroxyvitamin D3‐1alpha‐hydroxylase in mice via the long form of the leptin receptor. Arch Biochem Biophys. 2007;463(1):118‐127. doi: 10.1016/j.abb.2007.02.031 [DOI] [PubMed] [Google Scholar]
- 64. Park CY, Han SN. The role of vitamin D in adipose tissue biology: adipocyte differentiation, energy metabolism, and inflammation. J Lipid Atheroscler. 2021;10(2):130‐144. doi: 10.12997/jla.2021.10.2.130 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Szymczak‐Pajor I, Miazek K, Selmi A, Balcerczyk A, Sliwinska A. The action of vitamin D in adipose tissue: is there the link between vitamin D deficiency and adipose tissue‐related metabolic disorders? Int J Mol Sci. 2022;23(2):956. doi: 10.3390/ijms23020956 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Reis JP, von Muhlen D, Miller ER 3rd. Relation of 25‐hydroxyvitamin D and parathyroid hormone levels with metabolic syndrome among US adults. Eur J Endocrinol. 2008;159(1):41‐48. doi: 10.1530/EJE-08-0072 [DOI] [PubMed] [Google Scholar]
- 67. Liu S, Song Y, Ford ES, Manson JE, Buring JE, Ridker PM. Dietary calcium, vitamin D, and the prevalence of metabolic syndrome in middle‐aged and older U.S. women. Diabetes Care. 2005;28(12):2926‐2932. doi: 10.2337/diacare.28.12.2926 [DOI] [PubMed] [Google Scholar]
- 68. Kayaniyil S, Vieth R, Retnakaran R, et al. Association of vitamin D with insulin resistance and beta‐cell dysfunction in subjects at risk for type 2 diabetes. Diabetes Care. 2010;33(6):1379‐1381. doi: 10.2337/dc09-2321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Norman AW, Frankel JB, Heldt AM, Grodsky GM. Vitamin D deficiency inhibits pancreatic secretion of insulin. Science. 1980;209(4458):823‐825. doi: 10.1126/science.6250216 [DOI] [PubMed] [Google Scholar]
- 70. Norman AW. Minireview: vitamin D receptor: new assignments for an already busy receptor. Endocrinology. 2006;147(12):5542‐5548. doi: 10.1210/en.2006-0946 [DOI] [PubMed] [Google Scholar]
- 71. Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM. Intake of vitamin D and risk of type 1 diabetes: a birth‐cohort study. Lancet. 2001;358(9292):1500‐1503. doi: 10.1016/S0140-6736(01)06580-1 [DOI] [PubMed] [Google Scholar]
- 72. Kwak JH, Choi YH, Paik JK. Vitamin D status, fiber intake, and type 2 diabetes in U.S. adults. J Med Food. 2020;23(7):711‐718. doi: 10.1089/jmf.2019.4528 [DOI] [PubMed] [Google Scholar]
- 73. Mitri J, Muraru MD, Pittas AG. Vitamin D and type 2 diabetes: a systematic review. Eur J Clin Nutr. 2011;65(9):1005‐1015. doi: 10.1038/ejcn.2011.118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Barchetta I, Cimini FA, Cavallo MG. Vitamin D and metabolic dysfunction‐associated fatty liver disease (MAFLD): an update. Nutrients. 2020;12(11):3302. doi: 10.3390/nu12113302 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Bikle DD, Schwartz J. Vitamin D binding protein, total and free vitamin D levels in different physiological and pathophysiological conditions. Front Endocrinol (Lausanne). 2019;10:317. doi: 10.3389/fendo.2019.00317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Li J, Byrne ME, Chang E, et al. 1Alpha,25‐dihydroxyvitamin D hydroxylase in adipocytes. J Steroid Biochem Mol Biol. 2008;112(1–3):122‐126. doi: 10.1016/j.jsbmb.2008.09.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Targher G, Bertolini L, Scala L, et al. Associations between serum 25‐hydroxyvitamin D3 concentrations and liver histology in patients with non‐alcoholic fatty liver disease. Nutr Metab Cardiovasc Dis. 2007;17(7):517‐524. doi: 10.1016/j.numecd.2006.04.002 [DOI] [PubMed] [Google Scholar]
- 78. Gonzalez EA, Sachdeva A, Oliver DA, Martin KJ. Vitamin D insufficiency and deficiency in chronic kidney disease. A single center observational study. Am J Nephrol. 2004;24(5):503‐510. doi: 10.1159/000081023 [DOI] [PubMed] [Google Scholar]
- 79. Al‐Badr W, Martin KJ. Vitamin D and kidney disease. Clin J Am Soc Nephrol. 2008;3(5):1555‐1560. doi: 10.2215/CJN.01150308 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Zwillich CW. Sleep apnoea and autonomic function. Thorax. 1998;53(Suppl 3):S20‐S24. doi: 10.1136/thx.53.2008.S20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Hemodynamic and autonomic changes in adults with obstructive sleep apnea. Adv Cardiol. 2011;46:171‐195. doi: 10.1159/000325109 [DOI] [PubMed] [Google Scholar]
- 82. Smith RP, Veale D, Pepin JL, Levy PA. Obstructive sleep apnoea and the autonomic nervous system. Sleep Med Rev. 1998;2(2):69‐92. doi: 10.1016/S1087-0792(98)90001-6 [DOI] [PubMed] [Google Scholar]
- 83. Li X, He J, Yun J. The association between serum vitamin D and obstructive sleep apnea: an updated meta‐analysis. Respir Res. 2020;21(1):294. doi: 10.1186/s12931-020-01554-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. McCarty DE, Chesson AL Jr, Jain SK, Marino AA. The link between vitamin D metabolism and sleep medicine. Sleep Med Rev. 2014;18(4):311‐319. doi: 10.1016/j.smrv.2013.07.001 [DOI] [PubMed] [Google Scholar]
- 85. Abu El Maaty MA, Hassanein SI, Gad MZ. Genetic variation in vitamin D receptor gene (Fok1:rs2228570) is associated with risk of coronary artery disease. Biomarkers. 2016;21(1):68‐72. doi: 10.3109/1354750X.2015.1118535 [DOI] [PubMed] [Google Scholar]
- 86. Ragia G, Archontogeorgis K, Simmaco M, et al. Genetics of obstructive sleep apnea: vitamin D receptor gene variation affects both vitamin D serum concentration and disease susceptibility. OMICS. 2019;23(1):45‐53. doi: 10.1089/omi.2018.0184 [DOI] [PubMed] [Google Scholar]
- 87. Norris KC, Williams SF. Race/ethnicity, serum 25‐hydroxyvitamin D, and heart disease. JAMA. 2013;310(2):153‐155. doi: 10.1001/jama.2013.7229 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Hossein‐Nezhad A, Eshaghi SM, Maghbooli Z, et al. The role of vitamin D deficiency and vitamin D receptor genotypes on the degree of collateralization in patients with suspected coronary artery disease. Biomed Res Int. 2014;2014:304250. doi: 10.1155/2014/304250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Rasheed H, Hegazy RA, Gawdat HI, et al. Serum vitamin D and vitamin D receptor gene polymorphism in mycosis fungoides patients: a case control study. PLoS ONE. 2016;11(6):e0158014. doi: 10.1371/journal.pone.0158014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Zhang Y, Zhu H, Yang X, et al. Serum vitamin D level and vitamin D receptor genotypes may be associated with tuberculosis clinical characteristics: a case‐control study. Medicine (Baltimore). 2018;97(30):e11732. doi: 10.1097/MD.0000000000011732 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Tayel SI, Soliman SE, Elsayed HM. Vitamin D deficiency and vitamin D receptor variants in mothers and their neonates are risk factors for neonatal sepsis. Steroids. 2018;134:37‐42. doi: 10.1016/j.steroids.2018.03.003 [DOI] [PubMed] [Google Scholar]
- 92. Pfeifer M, Begerow B, Minne HW. Vitamin D and muscle function. Osteoporos Int. 2002;13(3):187‐194. doi: 10.1007/s001980200012 [DOI] [PubMed] [Google Scholar]
- 93. Patil SP, Schneider H, Schwartz AR, Smith PL. Adult obstructive sleep apnea: pathophysiology and diagnosis. Chest. 2007;132(1):325‐337. doi: 10.1378/chest.07-0040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Gominak SC, Stumpf WE. The world epidemic of sleep disorders is linked to vitamin D deficiency. Med Hypotheses. 2012;79(2):132‐135. doi: 10.1016/j.mehy.2012.03.031 [DOI] [PubMed] [Google Scholar]
- 95. Shoham S, Davenne D, Cady AB, Dinarello CA, Krueger JM. Recombinant tumor necrosis factor and interleukin 1 enhance slow‐wave sleep. Am J Physiol. 1987;253(1 Pt 2):R142‐R149. doi: 10.1152/ajpregu.1987.253.1.R142 [DOI] [PubMed] [Google Scholar]
- 96. Peterson CA, Heffernan ME. Serum tumor necrosis factor‐alpha concentrations are negatively correlated with serum 25(OH)D concentrations in healthy women. J Inflamm (Lond). 2008;5(1):10. doi: 10.1186/1476-9255-5-10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Toujani S, Kaabachi W, Mjid M, Hamzaoui K, Cherif J, Beji M. Vitamin D deficiency and interleukin‐17 relationship in severe obstructive sleep apnea–hypopnea syndrome. Ann Thoracic Med. 2017;12(2):107‐113. doi: 10.4103/atm.ATM_301_16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Ge X, Han F, Huang Y, et al. Is obstructive sleep apnea associated with cardiovascular and all‐cause mortality? PLoS ONE. 2013;8(7):e69432. doi: 10.1371/journal.pone.0069432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Melamed ML, Michos ED, Post W, Astor B. 25‐Hydroxyvitamin D levels and the risk of mortality in the general population. Arch Intern Med. 2008;168(15):1629‐1637. doi: 10.1001/archinte.168.15.1629 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.