

Abstract
This study tested whether effects of a preventive intervention delivered in elementary school showed benefits for the young adult offspring of intervention recipients over 20 years later. The Raising Healthy Children (RHC) intervention, trialed in in 18 public schools in Seattle, Washington, from 1980-1986 (grades 1-6), sought to build strong bonds to family and school to promote school success and avoidance of substance use and illegal behavior. Four intervention groups were constituted: Full, Late, Parent Training Only, and Control. Participants were followed through 2014 (age 39 years). Those who became parents were enrolled in an intergenerational study along with their oldest offspring (10 assessments between 2002 and 2018). This study includes young adult offspring (ages 18-25 years; n = 169; 52% Female; 4% Asian, 25% Black, 40% Multiracial, 4% Native American, 2% Native Hawaiian/Pacific Islander, 25% White; 14% Hispanic/Latinx) of participants in the original RHC trial. Offspring outcome measures included high school noncompletion, financial functioning, alcohol misuse, cannabis misuse, cigarette use, criminal behavior, internalizing behavior, social skills, and social bonding. A global test across all young adult outcome measures showed that offspring of parents who received the full RHC intervention reported better overall functioning compared to offspring of control group parents. Analyses of individual outcomes showed that offspring of full intervention group parents reported better financial functioning than offspring of control group parents. Findings show the potential of universal preventive interventions to provide long-term benefits that reach into the next generation. ClinicalTrials.gov Identifier: NCT04075019; retrospectively registered in 2019
Keywords: Cross-generational effects, young adult functioning, universal prevention
Over the past 30 years, several tested-effective preventive interventions that promote positive youth and young adult development have been developed (Blueprints for Healthy Youth Development, n.d.; Catalano et al., 2019; Washington State Institute for Public Policy, n.d.). Some of these interventions, including Raising Healthy Children (RHC; Hawkins, Guo, Hill, Battin-Pearson, & Abbott, 2001; Hawkins, Kosterman, Catalano, Hill, & Abbott, 2005, 2008; Kosterman et al., 2019) have shown benefits lasting years after the end of the intervention, even into adulthood (Kellam et al., 2014; Sandler, Schoenfelder, Wolchick, & MacKinnon, 2011). In addition to long-term effects, some preventive interventions also have demonstrated crossover effects, or beneficial effects that extend beyond the primary outcome(s) targeted by the intervention (King, Arango, & Foster, 2018; Vidot et al., 2016). For example, RHC sought to improve family management and bonding to school and to lower rates of adolescent substance use, but beneficial crossover effects on participant early pregnancy, mental health, and suicidal ideation also have been observed (Kosterman et al., 2019; Lonczak, Abbott, Hawkins, Kosterman, & Catalano, 2002). One possibility that has largely been unexamined is that benefits from preventive interventions may “cross over” into the next generation. This study tested whether the RHC intervention showed benefits for the young adult offspring of intervention recipients.
The Raising Healthy Children Intervention
The RHC intervention (Clinical-Trials.gov identifier: NCT04075019) has been described in detail previously (Hawkins et al., 2008; Hill et al., 2020; Kosterman et al., 2019). Briefly, RHC aimed to build strong prosocial bonds to family and school in order to promote school success and avoidance of substance use and delinquent behavior. It was delivered by trained staff at the classroom level, and consisted of teacher and parent workshops and child skill development (see Table 1). The study began as a randomized controlled trial in 1981 with treatment and control conditions. In 1985 as a condition of funding, two new intervention arms and additional control group participants were added, resulting in a nonrandomized controlled trial (see also Hawkins et al., 2008). Thus, four intervention conditions were implemented: a “full-intervention” group (n = 156) received the intervention from grades 1 through 6. A “late-intervention” group (n = 267) received the intervention in grades 5 and 6 only. A “parent-training-only” group (n = 141) was offered only the parent intervention components at fifth and sixth grades, and a control group (n = 220) received no intervention (see Figure 1 for CONSORT diagram). In past analyses, we have not identified benefits of the parent-training-only condition, likely because only 29% of parents attended 1 or more sessions (Hawkins, Catalano, Kosterman, Abbott, & Hill, 1999; Hawkins et al., 2005, 2008). Thus, this study compares the full- and late-treatment groups to the control group.
Table 1.
Components of the RHC intervention and grades they were administered
| Group | Intervention Components | Grades |
|---|---|---|
| Teachers | Proactive Classroom Management - establish clear rules and guidelines, recognize and reward good behavior, manage disruptions | 1-6 |
| Interactive Teaching - assess foundational knowledge, teach to learning objectives, model skills to be learned, monitor comprehension | ||
| Cooperative Learning - establish diverse student cooperative learning teams, recognize teams for improvement | ||
| Parents | Behavior Management Skills - identify desirable and undesirable child behaviors, establish clear rules and guidelines, consistent positive reinforcement for good behavior, consistent moderate consequences for bad behavior | 1-2 |
| Academic Support Skills - initiate contact with teachers, help with reading and math, create supportive home environment | 2-3 | |
| Skills to Reduce Drug Use - establish family drug use policy, practice refusal skills, reduce family conflict | 5-6 | |
| Children | Interpersonal Problem-Solving Skills - communication, decision making, negotiation, conflict resolution | 1 |
| Refusal Skills - recognize peer pressure, identify consequences of misbehavior, generate alternate activities - invite peers to join | 6 |
Figure 1.
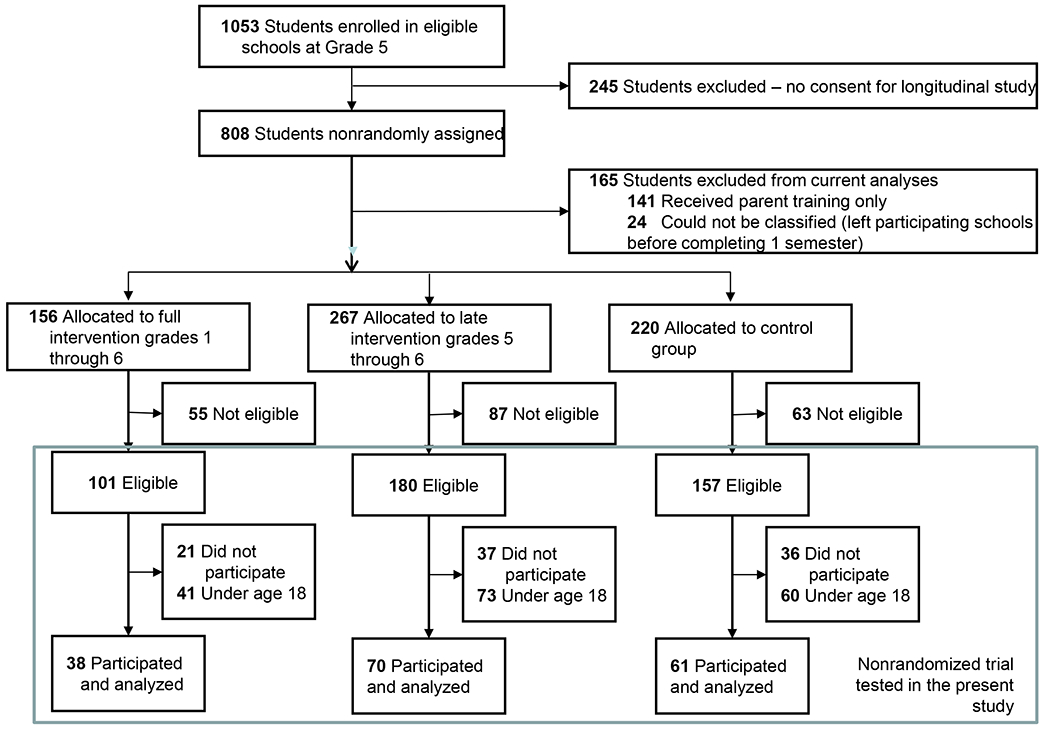
CONSORT diagram of analytic sample
It may seem unlikely that preventive interventions delivered to parents when they were in elementary school might have effects in the next generation. However, prior research shows that some childhood preventive interventions, including RHC, can help place individuals on a positive developmental trajectory into adulthood and are associated with improved adult functioning (Hawkins et al., 2001; Hawkins et al., 2005; Kosterman et al., 2019). For example, individuals in the full RHC intervention condition (compared to controls) were more likely to have graduated from high school (91% versus 81%) by age 21 (Hawkins et al., 2005) and had significantly higher lifetime academic attainment and better financial functioning (93% versus 84% above U.S. median socioeconomic status) at age 27 (Hawkins et al., 2008), with improved financial functioning persisting across the 30s (Kosterman et al., 2019). From ages 21 to 39, members of the full-intervention group compared to the control group reported better emotion regulation, fewer suicidal thoughts, and fewer symptoms of depression and anxiety (Hawkins et al., 2005, 2008; Kosterman et al., 2019). Similar evidence for long term effects on positive adult functioning, including among mothers specifically, has been observed for the FAST TRACK intervention (Dodge et al., 2015; Rothenberg et al., 2023).
Positive adult functioning among parents, in turn, may help parents create an environment conducive to the healthy development of their children (Cox & Harter, 2003; Duncan & Brooks-Gunn, 1997; Hawkins, Catalano, & Miller, 1992; Masten et al., 1999; Ramchandani, Stein, Evans, & O’Connor, 2005; Rothenberg et al., 2023). For example, prior studies show that higher levels of parent financial resources and education are associated with improved offspring functioning (Duncan & Brooks-Gunn, 1997; Hawkins et al., 1992; Sullivan et al., 2019). Similarly, many studies have demonstrated links between lower levels of parental depression and improved child outcomes (Netsi et al., 2018; Ramchandani et al., 2005; Sullivan et al., 2019). Thus, prior research supports the possibility of cross-generational intervention effects.
Published tests of cross-generational preventive intervention effects are virtually nonexistent. Using the current dataset, Hill and colleagues (2020) found that young children (ages 1-5 years) of parents who received the full RHC intervention had fewer developmental delays compared to children of control group parents. School-aged children of full-intervention group parents had higher teacher-rated cognitive and academic skills and lower levels of teacher-rated externalizing behavior compared to children of control group parents. Finally, children of parents who received the full RHC intervention were less likely to self-report having used alcohol, cigarettes, cannabis, or illegal drugs by age 18 (Hill et al., 2020).
The current study extends the Hill and colleagues (2020) study by testing cross-generational intervention effects on functioning among young adult offspring ages 18-25 years, including measures of financial functioning, substance use, antisocial behavior, social bonding, and emotion regulation. The choice of young adult outcomes was motivated by a) the original areas of focus of the RHC intervention experienced by parents (building social skills and bonding to family and school); b) areas of intervention impact in the parent generation as described above; and c) theory that emphasizes good physical and mental health, ethical behavior, healthy family relationships and social bonding, good financial functioning, and educational attainment as key dimensions of healthy young adult development (Benson, Scales, Hawkins, Oesterle, & Hill, 2004; Scales et al., 2016). The primary hypothesis was that there will be an overall cross-generational intervention benefit across all the outcomes examined (omnibus effect) in the full treatment group. Given the nature of the long-term effects of RHC on participants and prior findings in the Hill and colleagues (2020) study, effects on specific outcomes in the full treatment group were expected (secondary hypotheses), including lower levels of substance use, better financial functioning, and a higher prevalence of on-time high school completion among offspring of full-intervention parents compared to offspring of control group parents. Based on prior studies, no effects of the late treatment condition were hypothesized (Hawkins et al., 1999; Hawkins et al., 2005, 2008).
Methods
Sample and Procedures
The Seattle Social Development Project (SSDP), a nonrandomized controlled trial of the RHC intervention, included fifth-grade students (age 10, n = 808) recruited from 18 elementary schools serving higher crime neighborhoods in the Seattle School District in 1985. Students were surveyed 15 times through age 39 (2014). In 2002, recognizing that SSDP participants were becoming parents, we began SSDP – The Intergenerational Project (SSDP-TIP). SSDP and SSDP-TIP have been described elsewhere (Bailey, Hill, Epstein, Steeger, & Hawkins, 2018; Hawkins et al., 2008; Hill et al., 2020). The SSDP-TIP sample members included the parent participating in SSDP (SSDP parent), their eldest biological child (offspring), and an “other caregiver” (usually the spouse) identified by the SSDP parent. Data were collected using in-person interviews in respondents’ homes or another private location, over the phone, or over the web. Respondents were paid between $10 (young children) and $60 (parents) per survey. To date, 10 annual waves of data have been collected from families, which occurred in 2002-2005 (waves 1-4), 2009-2011 (waves 5-7), and 2015-2017 (waves 8-10). Families were eligible for SSDP-TIP if SSDP parents had face-to-face contact with the target child at least once a month. New families were recruited into each wave as more SSDP participants became parents for the first time. At the end of Wave 10, the cumulative sample included 426 families. Offspring (49% female) in the sample ranged in age from 1-29 years, and were racially and ethnically diverse: 12% Asian/Pacific Islander, 15% Black/African American, 34% multiracial, 4% Native American, and 36% White; 12% were Hispanic/Latinx. The median family income in 2017 was $75,001-$80,000.
Eligibility, recruitment, and retention analyses for SSDP-TIP included parent sex; marital status; receipt of financial assistance; cigarette use, cannabis use, and binge drinking in high school and at age 27 (SSDP-TIP baseline); free lunch eligibility in childhood; and race and ethnicity. None of these variables was related to eligibility by wave 10. Families were less likely to be recruited if the SSDP parent was male (72% versus 87% of females), Asian American (74% versus 86% of White parents), or received free/reduced-price school lunch in grades 5-7 (75% versus 85% of those not receiving free lunch). Retention from wave to wave averaged 90% and was not related to any of the variables tested. Tests of differential eligibility, recruitment, and retention in SSDP-TIP based on parent RHC treatment group membership showed no significant differences by group in whether SSDP parents were eligible for, recruited into, or retained during SSDP-TIP. This study included the n = 169 offspring (n = 38 full treatment, n = 70 late treatment, n = 61 control) who were surveyed at ages 18-25 years.
Measures
Self-reported young adult functioning measures were administered in each of waves 5-10 (2009-2017) unless otherwise noted. None of the offspring reached age 18 prior to 2009.
Education.
High school noncompletion (0 high school completed, 1 high school not completed) was based on offspring reports of the highest grade they had completed.
Financial functioning.
Any unemployment (waves 8-10) was coded as 1 if offspring reported at any wave being unemployed for 2 months or longer, despite wanting or needing a job (otherwise 0). Benefit receipt (waves 6-10) was coded as 1 if offspring reported at any wave receiving need-based government financial benefits (e.g., food stamps; otherwise 0). Respondents reported their household income range at each wave (waves 8-10; 1 less than $10,000 to 24 $200,001+), which was reverse coded so that higher scores indicated lower income. Average financial strain across waves 8-10 was created by averaging 8 items within survey year (e.g., In the past year have you: Changed food shopping or eating habits a lot to save money? Fell far behind in paying bills?; Cronbach’s alpha .78-.87) and then averaging across years. Except for unemployment, financial functioning assessments were limited to offspring who were not living with a parent. To reduce multiple testing, financial functioning measures were combined into a single latent factor.
Substance use.
At each wave, respondents reported their past-month frequency of alcohol use, typical number of drinks on drinking days, past-year frequency of cannabis and cigarette use, and whether they binge drank (5+ drinks during a single occasion) in the past year. A measure indicating any past-year cigarette use at any wave (0 no, 1 yes) was created. Any binge drinking was coded as 1 if respondents reported binge drinking in any year (otherwise 0). Past-month alcohol frequency and quantity and past-year cannabis use frequency were averaged, separately, across waves. At waves 6-10, respondents also reported whether they experienced problems related to their alcohol or cannabis use (separately; e.g., use caused problems in social relationships, hurt school/work performance; 9 items). Any alcohol problems and any cannabis problems were coded as 1 (otherwise 0) if respondents reported experiencing one or more problems at any wave. To reduce multiple testing, the four alcohol use outcomes (frequency, quantity, binge drinking, problem use) and the two cannabis use outcomes (frequency, problem use) were combined, respectively, into an alcohol misuse latent factor and a cannabis misuse latent factor.
Internalizing problems were measured using the Lengua scales (Lengua, Sadowski, Friedrich, & Fisher, 2001) empirically derived from the Achenbach Adult Self Report Form (Achenbach & Rescorla, 2003). Internalizing scores were calculated within wave (Cronbach’s alpha .80-.93) and then averaged across waves; higher scores indicate more problems.
Criminal behavior in the past year was assessed by asking whether respondents had engaged in a range of nonviolent, property, and violent crimes (e.g., hitting someone with the idea of seriously hurting them; giving false information on a job, loan, or bank account application or tax form). A variable indicating any criminal behavior at any wave (0 no, 1 yes) was created.
Social skills were measured in waves 8-10 only (Cronbach’s alpha .62-.74) using 5 items (e.g., How skilled are you at refraining from saying things that might cause a disagreement to build into a big fight?). Items were averaged within each wave and then across waves; higher scores indicate worse social skills.
Social bonding to a current romantic partner (if present), to two best friends, and to the parent who received the RHC intervention (separately) were reported by offspring. For each relationship, respondents reported whether, for example, they felt very close to (person) and would like to be the kind of person that (person) is. Reports for the two best friends were averaged. Scale scores were created by averaging items for partner, friends, and parent, separately, within wave (Cronbach’s alpha .71-.86) and then across waves. The three social bonding scales (partner, friends, parent) were not sufficiently correlated to combine into a latent factor, and were kept separate.
Controls.
Whether the SSDP parent had been born to a teen mother (1 yes, 0 no) was controlled to account for baseline differences in prevalence between control and full treatment groups in the original RHC trial. Parent sex, race, and childhood poverty were controlled to account for factors related to eligibility and recruitment into SSDP-TIP. Parent sex (1 male, 0 female) and race (1 Asian American, 0 Any other race) were self-reported, and childhood poverty (eligible for free/reduced-price lunch in grades 5, 6, or 7; 1 yes, 0 no) was taken from school records during the SSDP study. Parent marital status was assessed at each wave and was coded as married at any survey occasion (1 yes, 0 no). To account for the study’s accelerated longitudinal design, an offspring birth cohort variable was created based on offspring birth year.
Analysis
Intent-to-treat analyses used multivariable regression with observed and latent outcome variables in Mplus version 7.4. All tests were two-sided, with a significance criterion of p < .05 unless otherwise noted. Full Information Maximum Likelihood estimation was used to handle missing data. Weighted Least Squares Means-Variances estimation was used with categorical outcomes and latent factors with categorical indicators; Robust Maximum Likelihood was used with continuous outcomes. Both methods accurately model non-normally distributed variables (Muthén & Muthén, 1998-2017). Analyses proceeded in three steps. First and separately for the full- and late-intervention groups, a Global Test Statistic (Feng & Thompson, 2002) was used to test for an overall effect of intervention condition across all outcomes simultaneously, including control variables and accounting for clustering among offspring by birth cohort. Second, we tested associations between intervention condition (full treatment vs. control and late treatment vs. control) and specific young adult functioning indicators. Young adult functioning outcomes were regressed on full- and late-intervention group dummy variables, again including controls and accounting for clustering. After creation of latent factors, 11 total outcomes were examined. As a third step, we used a False Discovery Rate (FDR; Benjamini & Hochberg, 1995) procedure to adjust the critical p value within condition to minimize bias due to multiple testing.
Results
Table 2 shows the race and ethnic composition of the analytic sample. Means and prevalences for young adult functioning indicators are shown in Table 3. The financial functioning, alcohol misuse, and cannabis misuse indicators all loaded significantly on their respective latent factors (model fit statistics and factor loadings available online).
Table 2.
Race and ethnicity of included offspring.
| Race and ethnicity, N (%) | Prevalence |
|---|---|
| Ethnicity | |
| Hispanic/Latinx | 23 (14%) |
| Race | |
| Asian American | 6 (4%) |
| Black/African American | 42 (25%) |
| Multiracial | 68 (41%) |
| Native American/American Indian | 5 (3%) |
| Native Hawaiian/Pacific Islander | 4 (2%) |
| White/European American | 42 (25%) |
| Detailed information on multiracial individuals | |
| Asian American and Native Hawaiian/Pacific Islander | 3 (2%) |
| Asian American and Black/African American | 2 (1%) |
| Asian American and White/European American | 1 (<1%) |
| Black/African American and Native American | 4 (2%) |
| Black/African American and Native Hawaiian/Pacific Islander | 3 (2%) |
| Black/African American and White/European American | 23 (14%) |
| Native American/American Indian and White/European American | 11 (6%) |
| Native Hawaiian/Pacific Islander and White/European American | 3 (2%) |
| More than 2 races | 18 (11%) |
NOTE: Percentages for multiracial individuals are % of the total sample. Hispanic/Latinx is not mutually exclusive to race categories.
Table 3.
Descriptives for young adult functioning measures by intervention condition.
| Prevalence, N yes (% yes) | Mean (SD) | |||||
|---|---|---|---|---|---|---|
| Outcome | Full Tx | Late Tx | Control | Full Tx | Late Tx | Control |
| No on-time high school completion | 10 (26%) | 22 (30%) | 15 (23%) | |||
| Poor financial functioning | ||||||
| Unemployment, any | 17 (47%) | 28 (43%) | 24 (43%) | |||
| Benefit receipt, any | 6 (17%) | 15 (23%) | 15 (26%) | |||
| Low household income, mean (range 1-24) | 13.74 (6.51) | 15.17 (6.25) | 15.24 (6.70) | |||
| Financial strain, mean (range 0-1) | .23 (.27) | .30 (.25) | .29 (.24) | |||
| Alcohol misuse | ||||||
| Alcohol use frequency, mean (range 0-30) | 1.26 (1.57) | 2.30 (3.18) | 1.94 (3.34) | |||
| Alcohol quantity, mean (range 0-5) | 1.18 (1.26) | 1.71 (1.57) | 1.53 (1.59) | |||
| Binge drinking, any | 13 (34%) | 36 (51%) | 25 (40%) | |||
| Alcohol problems, any | 8 (21%) | 40 (56%) | 24 (39%) | |||
| Cannabis misuse | ||||||
| Cannabis use frequency, mean (range 0-3) | .79 (.88) | .83 (.93) | .71 (.87) | |||
| Cannabis problems, any | 5 (13%) | 14 (20%) | 11 (18%) | |||
| Cigarette use, any | 9 (24%) | 34 (48%) | 23 (37%) | |||
| Criminal behavior, any | 9 (24%) | 30 (42%) | 21 (34%) | |||
| Internalizing, mean (range 1-3) | 1.53 (.34) | 1.62 (.39) | 1.66 (.45) | |||
| Low social skills, mean (range 0-4) | 1.73 (.66) | 1.18 (.66) | 1.78 (.70) | |||
| Low bonding to partner, mean (range 0-4) | .56 (.46) | .34 (.46) | .64 (.38) | |||
| Low bonding to friends, mean (range 0-4) | .79 (.48) | .85 (.44) | .99 (.49) | |||
| Low bonding to parent, mean (range 0-4) | 1.14 (.59) | 1.30 (.64) | 1.24 (.60) | |||
NOTE: Tx = treatment.
Young adult offspring of parents receiving the full treatment reported significantly better functioning (i.e., less poor functioning) across all outcomes examined compared to young adult offspring of parents in the control group (Global Test Statistic T = −3.11, p = .003). Analyses of individual functioning indicators (Table 4) showed that young adult offspring of parents in the full treatment group reported significantly better financial functioning (i.e., less poor financial functioning) and less alcohol misuse compared to offspring of parents in the control group. No other significant differences between offspring of full-intervention and control parents were identified. Only the association between intervention status and financial functioning remained statistically significant after FDR adjustments. Neither the global test nor any tests of individual outcomes showed significant associations with the late-intervention condition (not shown).
Table 4.
Tests of association between intervention group (Full Treatment versus Control) and individual young adult functioning indicators (n = 147-169).
| Outcome | Unstand. Estimate (SE) | Stand. Estimate (SE) | p | FDR significance (p < .005) |
|---|---|---|---|---|
| No on-time high school completion | .15 (.16) | .14 (.15) | .360 | No |
| Poor financial functioning | −.51 (.16) | −.43 (.13) | .001 | Yes |
| Alcohol misuse | −.41 (.20) | −.39 (.19) | .040 | No |
| Cannabis misuse | −.02 (.34) | .02 (.34) | .947 | No |
| Cigarette use, any | −.42 (.28) | −.40 (.27) | .136 | No |
| Criminal behavior, any | −.25 (.28) | −.24 (.27) | .368 | No |
| Internalizing (range 1-3) | −.17 (.11) | −.42 (.25) | .107 | No |
| Low social Skills (range 0-4) | −.04 (.11) | −.06 (.16) | .717 | No |
| Low bonding to partner (range 0-4) | −.11 (.06) | −.26 (.15) | .068 | No |
| Low bonding to friends (range 0-4) | −.20 (.11) | −.41 (.24) | .096 | No |
| Low bonding to parent (range 0-4) | −.15 (.15) | −.25 (.26) | .315 | No |
NOTE: Bolding indicates statistical significance (p < .05). Unstand = unstandardized; Stand = standardized; FDR = false discovery rate. Estimates were adjusted for parent race, sex, marital status, childhood poverty, and whether the parent was born to a teen mother. Standardized estimates were standardized with respect to the outcome (STDY).
Discussion
This study tested whether the Raising Healthy Children intervention, a universal, school-based preventive intervention delivered in elementary school, showed benefits for young adult offspring of intervention recipients more than 20 years later. Results supported the hypothesis that young adult offspring of parents who received the full intervention as children would report better functioning overall compared to offspring of parents who did not receive the intervention. Specific hypotheses that offspring of full-intervention parents would report higher rates of high school completion and lower substance use were not supported after correction for multiple testing. However, offspring of parents who received the full intervention reported significantly better financial functioning in young adulthood compared to offspring of control group parents. Consistent with prior studies (Hawkins et al., 1999; Hawkins et al., 2005, 2008), no effects of the late intervention on offspring were identified, likely due to insufficient intervention dosage.
Young adulthood is a critical developmental period involving profound transitions that sets the stage for later positive adult functioning (Elder, 1998; Hser, Longshore, & Anglin, 2007; Schulenberg, Bryant, & O’Malley, 2004). At the same time, internalizing and mood disorders often onset in the 20’s (Burke, Burke, Regier, & Rae, 1990; Kessler et al., 2005). The early 20s also constitute the peak period for substance use and onset of substance use disorder (Burke et al., 1990; Johnston, O’Malley, Bachman, & Schulenberg, 2013; Johnston, O’Malley, Bachman, & Schulenberg, 2016; Kessler et al., 2005). Thus, navigating young adulthood is demanding, and many young adults struggle. Some preventive interventions promoting positive youth development have shown long-lasting beneficial effects in adulthood, with respect to academic attainment, employment, financial functioning, and mental health (Hawkins et al., 2005, 2008; Kosterman et al., 2019). In turn, adults with more positive functioning may be more likely to construct family environments that are healthier for their own children (Dodge et al., 2015; Rothenberg et al., 2023). Although knowledge about long-term intervention effects on recipients is growing, studies examining cross-generational intervention effects where outcomes are measured in the second generation are rare.
Our previous investigation of cross-generational benefits of the RHC intervention found that school-aged offspring of intervention recipients showed fewer developmental delays, lower teacher-rated behavior problems, higher teacher-rated academic skills, and less substance use by age 18 (Hill et al., 2020). The current analyses examined cross-generational intervention effects on global functioning, reflecting the complex, multidimensional, and summative nature of young adult functioning (Global Test Statistic), as well as effects on functioning in specific areas to provide information about where effects were observed and inform future intervention efforts. Findings suggest that some intervention benefits reached into young adulthood in the next generation, supporting positive young adult functioning overall and financial functioning specifically among offspring of intervention recipients. In fact, the effect size of this cross-generational protective association, ~.4 standard deviations, is quite large in comparison to the median effect size observed in the field of prevention science, which is typically in the range of .07 - .16 standard deviations (Tanner-Smith, Durlak, & Marx, 2018).
In the original trial, some of the most enduring effects of the RHC intervention on parents were on academic attainment and improved financial health (Hawkins et al., 2005, 2008; Kosterman et al., 2019). These enduring benefits to financial health through the 30s observed among parents who received the RHC intervention (Kosterman et al., 2019) seem likely to explain, at least partially, the cross-generational effects observed here, given prior studies showing intergenerational continuity in socioeconomic status (Mazmunder, 2005). Future papers will investigate mediating mechanisms for the observed cross generational effects, including parent financial health.
Limitations
The original RHC trial was a nonrandomized controlled trial, and included participants from a limited geographic area. Although extensive testing for baseline intervention group nonequivalence found only one difference (being born to a teen mother) that was controlled here, unmeasured baseline group differences may exist and could account in part for these findings. The sample size was small. Although coding decisions such as dichotomization and categorization of skewed distributions (e.g., binge drinking, cigarette use) greatly reduced any risk for bias due to outliers, even a small number of individuals responding differently within treatment groups could have altered prevalences and findings. Additionally, the small sample size raises the risk of Type II error. Several moderate to large but not statistically significant standardized effects in Table 4 suggest that some cross-generational intervention benefits may have been missed due to low power. Some of the financial functioning measures were available only in the last three waves of data collection, meaning that some offspring who experienced financial instability in earlier waves may have been missed. These limitations are balanced by important strengths, including the use of prospective, longitudinal data from parents and offspring; high retention rates; thorough checks for internal validity (eligibility, recruitment, retention); and correction for multiple testing.
Conclusions
Although adoption of evidence-based preventive interventions is becoming more common, such interventions are still underutilized. Significant barriers to adoption of prevention programming remain at family, school, community, and policy levels, including lack of awareness, low support among key stakeholders, and inadequate funding (Fagan et al., 2019; Fagan, Lewis, & Catalano, 2020). The current findings show the potential of RHC to provide long-term benefits that reach into the next generation, and constitute a powerful argument for expanded implementation of similar programs. Further, the late intervention (5th and 6th grade only) was not sufficient to yield either long-term or cross-generational benefits. In contrast to recent trends emphasizing highly focused and/or brief interventions that address a limited set of outcomes, the current study suggests that producing cross-generational preventive intervention effects may require more comprehensive, longitudinal interventions.
Supplementary Material
Acknowledgements
We gratefully acknowledge the Survey Research Division of the Social Development Research Group, who collected and managed study data, as well as the study participants, who generously shared their experiences.
Funding:
This manuscript was supported by grants from the National Institute on Drug Abuse (R01DA023089, R01DA053203, R01DA009679). The funding agency had no role in the design of the study; collection, analysis, or interpretation of data; writing of this report; or decision to submit this manuscript for publication. Conclusions reflect the points of view of the authors.
Footnotes
Disclosure of potential conflicts of interest: Dr. Hawkins is a co-developer of the intervention tested here, but has no financial disclosures or conflicts of interest to declare. All other authors state that they have no financial disclosures or conflicts of interest to declare.
Informed consent: Informed consent for adult participants, as well as parental permission and child assent for minor participants were obtained at study outset and at each data collection.
Ethical approval: Study procedures and materials were approved by the University of Washington Human Subjects review board, and were consistent with standards established by the 1964 Declaration of Helsinki and its later amendments.
References
- Achenbach TM, & Rescorla LA (2003). Manual for the ASEBA Adult Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families. [Google Scholar]
- Bailey JA, Hill KG, Epstein M, Steeger CM, & Hawkins JD (2018). Seattle Social Development Project – The Intergenerational Project (SSDP-TIP). In Eichelsheim VI & van de Weijer SGA (Eds.), Intergenerational continuity of criminal and antisocial behavior. An international overview of current studies (pp. 186–206). New York, NY: Routledge. [Google Scholar]
- Benjamini Y, & Hochberg Y (1995). Controlling the false discovery rate - a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society. Series B (Methodological), 57(1), 289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x [DOI] [Google Scholar]
- Benson PL, Scales PC, Hawkins JD, Oesterle S, & Hill KG (2004). Successful young adult development. A report submitted to The Bill & Melinda Gates Foundation. Retrieved from https://docs.gatesfoundation.org/Documents/SuccessfulDevelopment.pdf [Google Scholar]
- Blueprints for Healthy Youth Development. (n.d.). Retrieved from http://www.blueprintsprograms.com/ [Google Scholar]
- Burke KC, Burke JD, Regier DA, & Rae DS (1990). Age at onset of selected mental disorders in five community populations. Archives of General Psychiatry, 47(6), 511–518. doi: 10.1001/archpsyc.1990.01810180011002 [DOI] [PubMed] [Google Scholar]
- Catalano RF, Skinner ML, Alvarado G, Kapungu C, Reavley N, Patton GC, … Petroni S. (2019). Positive youth development programs in low- and middle-income countries: A conceptual framework and systematic review of efficacy. Journal of Adolescent Health, 65(1), 15–31. doi: 10.1016/j.jadohealth.2019.01.024 [DOI] [PubMed] [Google Scholar]
- Cox MJ, & Harter KS (2003). Parent-child relationships. In Bornstein MH, Davidson L, Keyes CLM, & Moore KA (Eds.), Well-being: Positive development across the life course (pp. 191–204). Mahwah, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Dodge KA, Bierman KL, Coie JD, Greenberg MT, Lochman JE, McMahon RJ, & Pinderhughes EE (2015). Impact of early intervention on psychopathology, crime, and well-being at age 25. The American Journal of Psychiatry, 172(1), 59–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duncan GJ, & Brooks-Gunn J (1997). Income effects across the life span: Integration and interpretation. In Duncan GJ & Brooks-Gunn J (Eds.), Consequences of growing up poor (pp. 596–610). New York, NY: Russell Sage Foundation. [Google Scholar]
- Elder GH Jr. (1998). The life course as developmental theory. Child Development, 69(1), 1–12. doi: 10.1111/j.1467-8624.1998.tb06128.x [DOI] [PubMed] [Google Scholar]
- Fagan AA, Bumbarger BK, Barth RP, Bradshaw CP, Cooper BR, Supplee LH, & Walker DK (2019). Scaling up evidence-based interventions in US public systems to prevent behavioral health problems: challenges and opportunities. Prevention Science, 20(8), 1147–1168. doi: 10.1007/s11121-019-01048-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fagan AA, Lewis AN, & Catalano RF (2020). Prevention of adolescent mental, emotional, and behavioral health disorders: a global perspective. In Hupp S & Jewell JD (Eds.), The Encyclopedia of Child and Adolescent Development. Hoboken, NJ: JohnWiley & Sons. [Google Scholar]
- Feng Z, & Thompson B (2002). Some design issues in a community intervention trial. Controlled Clinical Trials, 23(4), 431–449. doi: 10.1016/s0197-2456(02)00206-4 [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Kosterman R, Abbott R, & Hill KG (1999). Preventing adolescent health-risk behaviors by strengthening protection during childhood. Archives of Pediatrics and Adolescent Medicine, 153(3), 226–234. doi: 10.1001/archpedi.153.3.226 [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, & Miller JY (1992). Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance-abuse prevention. Psychological Bulletin, 112(1), 64–105. doi: 10.1037/0033-2909.112.1.64 [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Guo J, Hill KG, Battin-Pearson S, & Abbott RD (2001). Long-term effects of the Seattle Social Development intervention on school bonding trajectories. Applied Developmental Science, 5(4), 225–236. doi: 10.1207/S1532480XADS0504_04 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkins JD, Kosterman R, Catalano RF, Hill KG, & Abbott RD (2005). Promoting positive adult functioning through social development intervention in childhood: Long-term effects from the Seattle Social Development Project. Archives of Pediatrics and Adolescent Medicine, 159(1), 25–31. doi: 10.1001/archpedi.159.1.25 [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Kosterman R, Catalano RF, Hill KG, & Abbott RD (2008). Effects of social development intervention in childhood 15 years later. Archives of Pediatrics and Adolescent Medicine, 162(12), 1133–1141. doi: 10.1001/archpedi.162.12.1133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill KG, Bailey JA, Steeger CM, Hawkins JD, Catalano RF, Kosterman R, … Abbott RD. (2020). Outcomes of childhood preventive intervention across 2 generations: A nonrandomized controlled trial. JAMA Pediatrics, 174(8), 764–771. doi: 10.1001/jamapediatrics.2020.1310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hser YI, Longshore D, & Anglin MD (2007). The life course perspective on drug use: a conceptual framework for understanding drug use trajectories. Evaluation Review, 31(6), 515–547. doi: 10.1177/0193841X07307316 [DOI] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, & Schulenberg JE (2013). Monitoring the Future national survey results on drug use, 1975–2012: Volume 2, College students and adults ages 19–50. Ann Arbor, MI: Institute for Social Research, The University of Michigan. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, & Schulenberg JE (2016). Monitoring the Future National Survey Results on Drug Use, 1975–2015: Volume 2, College Students and Adults Aages 19–55. Retrieved from http://monitoringthefuture.org/pubs.html#monographs [Google Scholar]
- Kellam SG, Wang W, Mackenzie ACL, Brown CH, Ompad DC, Or F, … Windham A. (2014). The impact of the Good Behavior Game, a universal classroom-based preventive intervention in first and second grades, on high-risk sexual behaviors and drug abuse and dependence disorders into young adulthood. Prevention Science, 15(Suppl. 1), 6–18. doi: 10.1007/s11121-012-0296-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, & Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. doi: 10.1001/archpsyc.62.6.593 [DOI] [PubMed] [Google Scholar]
- King CA, Arango A, & Foster CE (2018). Emerging trends in adolescent suicide prevention research. Current Opinions in Clinical Psychology, 22, 89–94. doi: 10.1016/j.copsyc.2017.08.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kosterman R, Hawkins JD, Hill KG, Bailey JA, Catalano RF, & Abbott RD (2019). Effects of social development intervention in childhood on adult life at ages 30 to 39. Prevention Science, 20(7), 986–995. doi: 10.1007/s11121-019-01023-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lengua LJ, Sadowski CA, Friedrich WN, & Fisher J (2001). Rationally and empirically derived dimensions of children’s symptomatology: Expert ratings and confirmatory factor analyses of the CBCL. Journal of Consulting and Clinical Psychology, 69(4), 683–698. doi: 10.1037/0022-006X.69.4.683 [DOI] [PubMed] [Google Scholar]
- Lonczak HS, Abbott RD, Hawkins JD, Kosterman R, & Catalano RF (2002). Effects of the Seattle Social Development Project on sexual behavior, pregnancy, birth, and sexually transmitted disease outcomes by age 21 years. Archives of Pediatrics and Adolescent Medicine, 156(5), 438–447. doi: 10.1001/archpedi.156.5.438 [DOI] [PubMed] [Google Scholar]
- Masten AS, Hubbard JJ, Gest SD, Tellegen A, Garmezy N, & Ramirez M (1999). Competence in the context of adversity: Pathways to resilience and maladaptation from childhood to late adolescence. Development & Psychopathology, 11(1), 143–169. doi: 10.1017/s0954579499001996 [DOI] [PubMed] [Google Scholar]
- Mazmunder B (2005). Fortunate sons: New estimates of intergenerational mobility in the United States using social security earnings data. The Review of Economics and Statistics, 87, 235–255. doi: 10.1162/0034653053970249 [DOI] [Google Scholar]
- Muthén LK, & Muthén BO (1998-2017). Mplus User’s Guide (8th ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Netsi E, Pearson RM, Murray L, Cooper P, Craske MG, & Stein A (2018). Association of persistent and severe postnatal depression with child outcomes. JAMA Psychiatry, 75(3), 247–253. doi: 10.1001/jamapsychiatry.2017.4363 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ramchandani P, Stein A, Evans J, & O’Connor TG (2005). Paternal depression in the postnatal period and child development: A prospective population study. Lancet, 365(9478), 2201–2205. doi: 10.1016/s0140-6736(05)66778-5 [DOI] [PubMed] [Google Scholar]
- Rothenberg WA, Lansford JE, Godwin JW, Dodge KA, Copeland WE, Odgers CL, … Conduct Problems Prevention Research Group. (2023). Intergenerational effects of the Fast Track intervention on the home environment: A randomized control trial. Journal of Child Psychology and Psychiatry, 64(5), 820–830. doi: 10.1111/jcpp.13648 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sandler I, Schoenfelder E, Wolchick S, & MacKinnon D (2011). Long-term impact of prevention programs to promote effective parenting: lasting effects but uncertain processes. Annual Review of Psychology, 62, 299–329. doi: 10.1146/annurev.psych.121208.131619 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scales PC, Benson PL, Oesterle S, Hill KG, Hawkins JD, & Pashak TJ (2016). The dimensions of successful young adult development: A conceptual and measurement framework. Applied Developmental Science, 20(3), 150–174. doi: 10.1080/10888691.2015.1082429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schulenberg JE, Bryant AL, & O’Malley PM (2004). Taking hold of some kind of life: how developmental tasks relate to trajectories of well-being during the transition to adulthood. Development & Psychopathology, 16(4), 1119–1140. doi: 10.1017/S0954579404040167 [DOI] [PubMed] [Google Scholar]
- Sullivan AD, Benoit R, Breslend NL, Vreeland A, Compas B, & Forehand R (2019). Cumulative socioeconomic status risk and observations of parent depression: Are there associations with child outcomes? Journal of Family Psychology, 33(8), 883–893. doi: 10.1037/fam0000567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanner-Smith E, Durlak JA, & Marx RA (2018). Empirically Based Mean Effect Size Distributions for Universal Prevention Programs Targeting School-Aged Youth: A Review of Meta-Analyses. Prevention Science, 19, 1091–1101. doi: 10.1007/s11121-018-0942-1 [DOI] [PubMed] [Google Scholar]
- Vidot DC, Huang S, Poma S, Estrada Y, Lee TK, & Prado G (2016). Familias Unidas’ crossover effects on suicidal behaviors among Hispanic adolescents: results from an effectiveness trial. Suicide and Life-Threatening Behavior, 46(Suppl. 1), S8–S14. doi: 10.1111/sltb.12253 [DOI] [PubMed] [Google Scholar]
- Washington State Institute for Public Policy. (n.d.). Benefit-cost Results. Retrieved from http://www.wsipp.wa.gov/BenefitCost [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.