

ABSTRACT
Foreign bodies are commonly seen in children, here presenting a case of a male adult with an impacted thumb pin in the left lower lobe bronchus. Extraction required fiber-optic bronchoscopy, failure of which led to thoracotomy with bronchotomy.
KEY WORDS: Bronchotomy, fiber-optic bronchoscopy, foreign body, thumb pin
INTRODUCTION
Inhalations of foreign bodies are not uncommon to occur, and not only children but adults have also suffered from these accidents. There are a lot of commonly occurring endobronchial foreign bodies which need different instruments from fiber-optic to rigid bronchoscope along with the tools for extraction and sometimes even invasive surgeries. A thumb-pin foreign body in our case was impacted and was further complicated with forceps stuck into the sharp end of the pin.
CASE REPORT
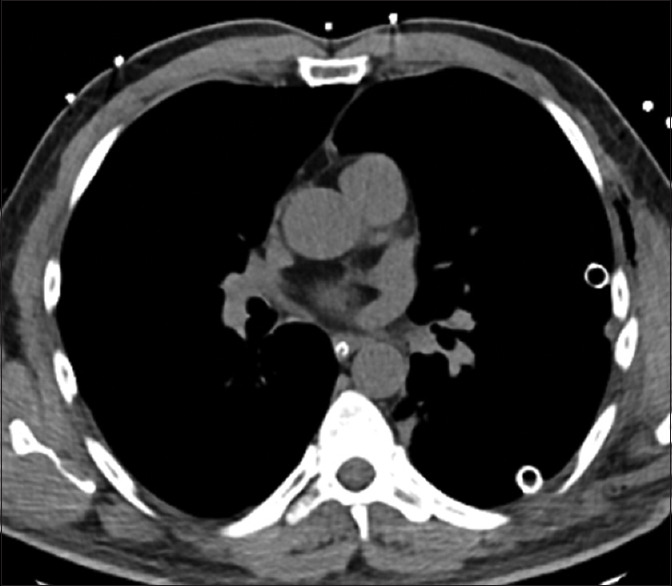
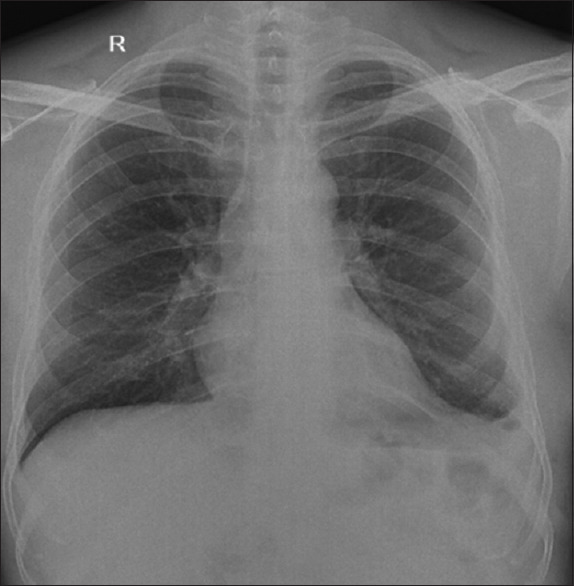
A 43-year-old male presented to Fortis Hospital Mohali after accidental ingestion of a thumb pin while working in his office. The patient came to the hospital within a few hours of the accident. The patient was not in distress but complained of a cough with one episode of streaky hemoptysis, chest discomfort, and throat pain. He is a known case of hypertension and was on medical management for the same. A chest X-ray was done which showed a metallic foreign body in the left main bronchus [Figure 1]. High resolution computed tomography (HRCT) chest was done to look for any trauma caused by the sharp end to the airways. HRCT shows [Figure 2] a linear metallic foreign body, measuring about 1.8 cm in length is seen in the left lower lobe bronchus. After baseline investigations, the patient was taken for fiber-optic bronchoscopy under conscious sedation after consent for the procedure. The foreign body was seen with the sharp end toward the scope impacted into the left lower lobe posterior basal segment. The traditional approach with the fiber-optic bronchoscope was chosen along with alligator biopsy forceps. A foreign body was identified [Figure 3] and an attempt was made to hold it between the jaws of forceps. Got hold of the sharp end and tried to pull out the pin but due to its tight impaction could not do so. Force is applied so that no injury to the airway should occur. Unfortunately, the sharp end got stuck to the forceps in such a manner that after many attempts it could not be released. So now, we have a thumb pin, onto that a biopsy forceps along with the fiber-optic bronchoscope into the left bronchial tree [Figure 4].
Figure 1.
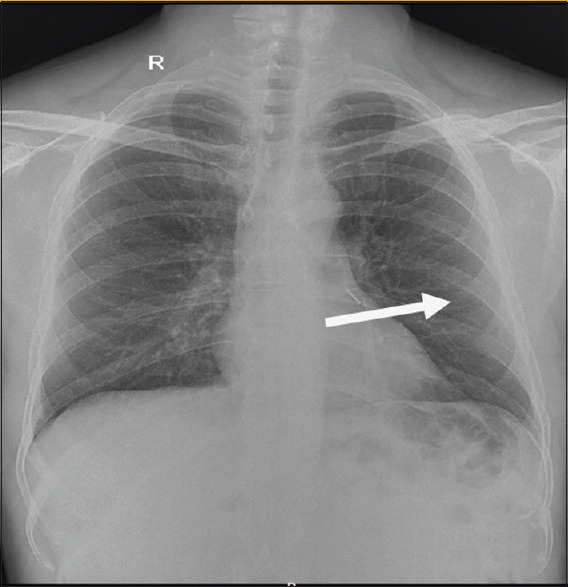
Xray left main Bronchus
Figure 2.
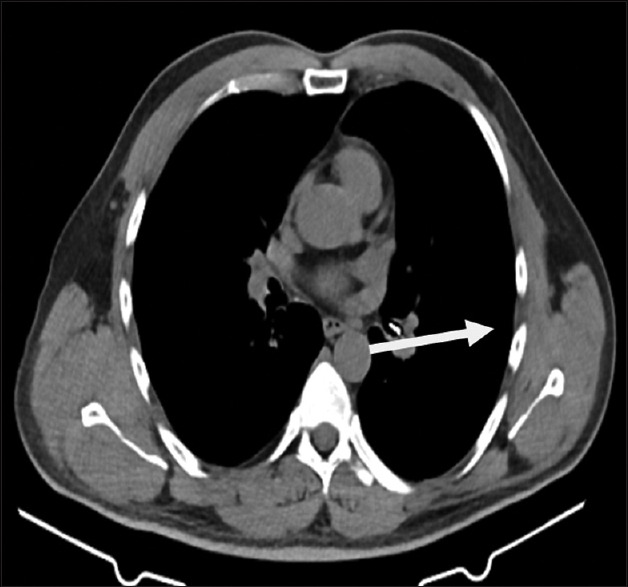
HRCT left lowe lobe Bronchus
Figure 3.
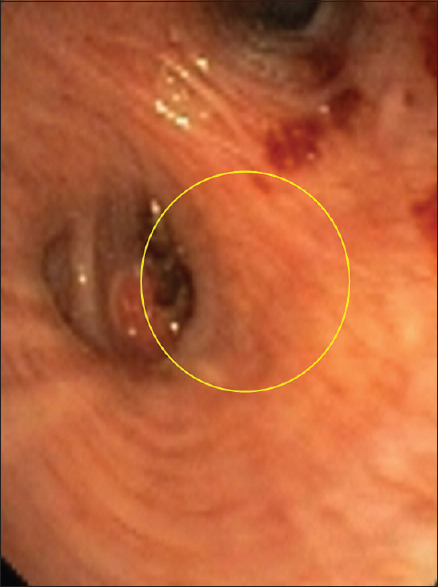
Fiber optic bronchoscope image
Figure 4.
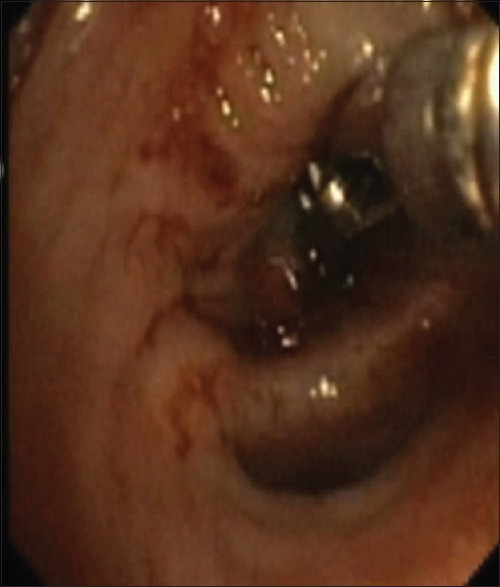
Fiber optic bronchoscope image with forceps
A thoracic surgeon was called and was asked for his opinion regarding the same. He suggested for thoracotomy followed by a bronchotomy for extraction. The outer end of the biopsy forceps was cut and the bronchoscope was removed, with the forceps hanging out of his mouth. The patient was shifted to the operation theater after all consent and plans for the invasive surgical procedure.
The patient was taken for left posterior-lateral thoracotomy, entered via the 5th intercostal space. Fine dissection was done around the left main stem bronchus at the hilar level, the bronchus was incised, and the foreign body was removed [Figure 5]. The incision was closed with interrupted prolene sutures and augmented with the bovine pericardial patch, the chest was closed in layers. Two chest tubes are seen in the left pleural cavity, no endobronchial foreign body is seen in the scan [Figure 6]. The patient was extubated the next day, and both intercostals chest drains were removed in the next 72 hours, patient was well mobilized. Chest X-ray [Figure 7] well expanded left lung, free of foreign body.
Figure 5.
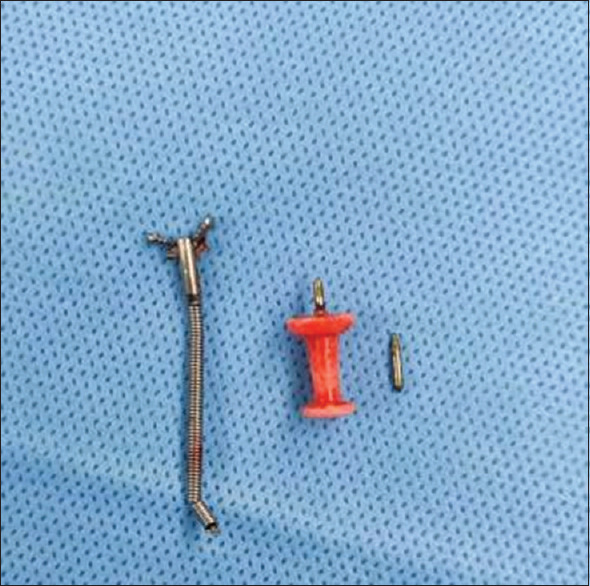
Foreign body
Figure 6.
HRCT scan with no endobronchial foreign body
Figure 7.
X ray chest with no foreign body
The patient was discharged on the 7th day of the procedure with a follow-up in OPD, doing well with no complaints and performing routine daily activities.
DISCUSSION
A rigid or flexible bronchoscopy can be performed whenever a foreign body is suspected or confirmed, although the debate for the optimal procedure continues.[1] Abundant case series and systemic reviews have recommended fiber-optic bronchoscopy as the choice of a procedure because it is simple, accessible, and also gives much more visual access to the airways. Useful even in patients with cervical injuries and those who are intubated and on mechanical ventilators.[2,3,4,5,6,7,8,9,10]
Flexible bronchoscopy is relatively easy and a safer procedure under experienced hands. The procedure is done under local anesthesia to visualize airways and can be opted for extraction of foreign bodies with lower cost, risk, and morbidity of secondary invasive procedures like rigid bronchoscopy which are done under general anesthesia.[11,12] In a few studies success rate of foreign body retrieval through flexible bronchoscope was about 79.1%. Open surgical procedures required were around 3.76% of patients in one and in another case, series were needed in more than 10%.[5,13]
Forceps are the most utilized and widely used tools for foreign body extraction.[2,14,15] There are multiple configurations of teeth and diameters to accommodate objects of varying size and texture and are best when objects with thin edges need extraction. Shark tooth, rat tooth, and alligator tips are used for the grasping of coins, plastic objects, and other non-crumbly organic foreign bodies such as bones. Rubberized tips are in use for grasping more delicate objects, and even sometimes the sharp objects, additionally give the benefit of protecting the airway mucosa. Standard cupped forceps used for endobronchial biopsy are not as useful as the previously listed forceps.
CONCLUSION
Foreign body aspiration is uncommon in adults, this makes an individual difficult to develop expertise with the procedure, techniques, and tools. The majority of the foreign bodies can be extracted safely with a flexible bronchoscope with the help of baskets and biopsy forceps. At times tools like rigid bronchoscopes or invasive surgeries by thoracic surgeons are needed. Hence, these foreign body extractions are to be done at a center with advanced tools and trained personnel.
Declaration of the patient consent
The authors certify that they have obtained all the appropriate patient consent forms. In the form, the patient has given consent for his images and other clinical information to be reported in this journal. The patient understands that their name and initials will not be published and due efforts will be made to conceal the identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest
REFERENCES
- 1.Bain A, Barthos A, Hoffstein V, Batt J. Foreign-body aspiration in the adult: Presentation and management. Can Respir J. 2013;20:e98–9. doi: 10.1155/2013/754121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sehgal IS, Dhooria S, Ram B, Singh N, Aggarwal AN, Gupta D, et al. Foreign body inhalation in the adult population: Experience of 25,998 bronchoscopies and systematic review of the literature. Respir Care. 2015;60:1438–48. doi: 10.4187/respcare.03976. [DOI] [PubMed] [Google Scholar]
- 3.Hsu AA. Endoscopic intervention of lower airway foreign matter in adults-A different perspective. J Thorac Dis. 2015;7:1870–7. doi: 10.3978/j.issn.2072-1439.2015.10.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mise K, Jurcev Savicevic A, Pavlov N, Jankovic S. Removal of tracheobronchial foreign bodies in adults using flexible bronchoscopy: Experience 1995–2006. Surg Endosc. 2009;23:1360–4. doi: 10.1007/s00464-008-0181-9. [DOI] [PubMed] [Google Scholar]
- 5.Ramos MB, Fernández-Villar A, Rivo JE, Leiro V, García-Fontán E, Botana MI, et al. Extraction of airway foreign bodies in adults: Experience from 1987–2008. Interact. Cardiovasc Thorac Surg. 2009;9:402–5. doi: 10.1510/icvts.2009.207332. [DOI] [PubMed] [Google Scholar]
- 6.Rodrigues AJ, Oliveira EQ, Scordamaglio PR, Gregório MG, Jacomelli M, Figueiredo VR. Flexible bronchoscopy as the first-choice method of removing foreign bodies from the airways of adults. J Bras Pneumol. 2012;38:315–20. doi: 10.1590/s1806-37132012000300006. [DOI] [PubMed] [Google Scholar]
- 7.Hewlett JC, Rickman OB, Lentz RJ, Prakash UB, Maldonado F. Foreign body aspiration in adult airways: Therapeutic approach. J Thorac Dis. 2017;9:3398–409. doi: 10.21037/jtd.2017.06.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Blanco Ramos M, Botana-Rial M, García-Fontán E, Fernández-Villar A, Gallas Torreira M. Update in the extraction of airway foreign bodies in adults. J Thorac Dis. 2016;8:3452–6. doi: 10.21037/jtd.2016.11.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fang YF, Hsieh MH, Chung FT, Huang YK, Chen GY, Lin SM, et al. Flexible bronchoscopy with multiple modalities for foreign body removal in adults. PLoS One. 2015;10:e0118993. doi: 10.1371/journal.pone.0118993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cravo J, Marques MAT. Endobronchial foreign bodies in adults—Flexible bronchoscopy as a first approach. Pulmonology. 2018;24:198–9. doi: 10.1016/j.pulmoe.2018.01.003. [DOI] [PubMed] [Google Scholar]
- 11.Du Rand IA, Blaikley J, Booton R, Chaudhuri N, Gupta V, Khalid S, et al. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: Accredited by NICE. Thorax. 2013;68((Suppl 1)):i1–44. doi: 10.1136/thoraxjnl-2013-203618. [DOI] [PubMed] [Google Scholar]
- 12.Dikensoy O, Usalan C, Filiz A. Foreign body aspiration: Clinical utility of flexible bronchoscopy. Postgrad Med J. 2002;78:399–403. doi: 10.1136/pmj.78.921.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chen CH, Lai CL, Tsai TT, Lee YC, Perng RP. Foreign body aspiration into the lower airway in Chinese adults. Chest. 1997;112:129–33. doi: 10.1378/chest.112.1.129. [DOI] [PubMed] [Google Scholar]
- 14.Dong YC, Zhou GW, Bai C, Huang HD, Sun QY, Huang Y, et al. Removal of tracheobronchial foreign bodies in adults using a flexible bronchoscope: Experience with 200 cases in China. Intern Med. 2012;51:2515–9. doi: 10.2169/internalmedicine.51.7672. [DOI] [PubMed] [Google Scholar]
- 15.Swanson KL, Prakash UB, McDougall JC, Midthun DE, Edell ES, Brutinel MW, et al. Airway foreign bodies in adults. J Bronchol. 2003;10:107–11. [Google Scholar]