

Abstract
Pregnant, postpartum, and lactating people, and infants have unique needs during public health emergencies, including nuclear and radiological incidents. This report provides information on the CDC Division of Reproductive Health’s emergency preparedness and response activities to address the needs of women of reproductive age (aged 15–49 years), people who are pregnant, postpartum, or lactating, and infants during a radiation emergency. Highlighted preparedness activities include: (1) development of a quick reference guide to inform key questions about pregnant, postpartum, and lactating people, and infants during radiation emergencies; and (2) exercising the role of reproductive health experts during nuclear and radiological incident preparedness activities.
Keywords: emergency preparedness, radiation and nuclear emergencies, women of reproductive age, maternal and infant health, reproductive health
Introduction
Pregnant, Postpartum, and lactating people and infants have unique needs during public health emergencies, including nuclear and radiological incidents.1 Radiation emergencies may vary in scale and severity, and include nuclear emergencies (e.g., detonation of a nuclear weapon or improvised nuclear device), detonation of a radiological dispersal device (also known as a dirty bomb), and accidental incidents, such as nuclear power plant incidents or transportation accidents involving radioactive materials.2 Exposure to radioactive materials can lead to internal contamination (through swallowing or breathing in radioactive materials) and external contamination (through radioactive dust, powder, or liquid coming in contact with hair, skin, or clothing).3
The U.S. Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 classifies people who are pregnant, postpartum, and lactating, and infants as populations at risk for adverse health outcomes related to emerging public health threats.1 During and after radiation emergencies, people who are pregnant, postpartum, or lactating or have infants are advised to consult a physician to understand the extent of exposure and possible contamination4
Health effects from radiation emergencies depend on the type of radioactive material, dose (amount of radiation received), total time it took for that dose to accumulate, and whether there is internal or external contamination. People with radiation contamination, including women of reproductive age (WRA), can develop acute radiation syndrome (if a high radiation dose is accrued over a very short time), cutaneous radiation injury (skin injury after exposure), psychological distress, and possible cancer later in life.2,5,6
Previous research describes the acute and long-term effects of internal or external contamination for the general adult population.5,7 For most external radiation exposures, the radiation dose to the fetus is lower than the dose to the woman.8 A pregnant woman’s abdomen partially protects the fetus from radiation sources that are outside her body. If a pregnant woman swallows or breathes in radioactive materials, these may be absorbed into her bloodstream.
From the woman’s blood, radioactive materials may pass through the umbilical cord to the fetus or concentrate in areas of the mother’s body near the womb and expose the fetus to radiation. Health effects to the fetus from radiation exposure can be severe, even at radiation doses too low to make the mother sick. These health effects can include miscarriage, stunted growth, deformities, abnormal brain function, and cancer.4,8
A fetus is most sensitive to radiation between weeks 2 and 18 of pregnancy. A fetus will become less sensitive to radiation during later stages of pregnancy. In addition, radioactive material can be passed to babies through breast milk of mothers with internal contamination, through contaminated water mixed with infant formula.9 And while being held and fed if their caregiver has radioactive material on their skin or clothing (external contamination). Babies may swallow or breathe in these materials while feeding and can become internally contaminated.10
The absorbed dose of radiation is measured in rad or Gray (Gy) (100 rad = 1 Gy).10 There is a dose-response effect for severity of symptoms or illness by Gy absorption with duration of exposure. For example, nausea and vomiting are unlikely to occur at low doses (≤1 Gy) but with high doses (>8 Gy) they occur 90%–100% of the time within 2 h of exposure.10
Similar trends have been documented for central nervous system dysfunction, risk of cancer, and death; the higher the absorption dose, the more likely and severe the symptom or illness.10 For example, lifetime cancer risk for low-dose exposure (≤1 Gy) is 0.06 to 8% but increases to >40% for high-dose exposure (above ≥6 Gy).10 For adults, exposures ≥8 Gy are lethal.10 For a pregnant person, health effects from radiation on the pregnancy can range from no effects to miscarriage or stillbirth—depending on magnitude and duration of exposure.4,11 For the fetus and infants, the effects can include abnormal growth, congenital malformations, abnormal brain function, and cancer in the future.4,11
In 2016, the CDC established a Nuclear/Radiological Training and Exercise Preparedness Program for its workforce to better prepare for and respond to a radiation emergency.7 To develop a radiation-knowledgeable workforce, the CDC conducted agency-wide and inter-agency preparedness exercises and workshops, created a resource library for clinicians, public health professionals, and first responders, and developed trainings for public health professionals and clinicians.12,13
The CDC’s Division of Reproductive Health (DRH) has been active in radiation preparedness activities since 2016.14 The DRH has been engaged in the planning and execution of agency-wide and interagency emergency preparedness activities, including drills and tabletop exercises, to better prepare for and respond to needs of WRA and infants in an emergency. To optimize staff response readiness for radiation emergencies, the DRH developed and maintained subject matter expertise, and collaborated with external and internal partners to increase capacity of radiation emergency preparedness efforts.
This report provides an overview of DRH’s emergency preparedness and response activities for radiation emergencies, including development of a quick reference guide on what is known about radiation emergencies and reproductive health, and participation in preparedness activities.
Development of a Radiation Emergency Quick Reference Guide for Women’s Reproductive Health
To strengthen the DRH’s nuclear and radiation preparedness activities and inform internal resource development, increase preparedness to develop messaging, or answer questions from the general public during radiation emergencies, the DRH developed the Radiation Emergency Quick Reference Guide to provide information about the needs of pregnant, postpartum, and lactating people, and infants during a radiation emergency.
We assessed what is known about the effects of nuclear and radiological emergencies on WRA based on published literature and existing web resources, and used our guiding principles for addressing the needs of pregnant people as a framework.14,15 Detailed methods about the development of the Radiation Emergency Quick Reference Guide for WRA are described in the Table 1.
TABLE 1.
Selected References for Public Health Practitioners: Outcomes Among Women of Reproductive Age After Radiation Emergencies
| Country/countries | Exposure incident | Elevated risk for the following outcome(s) and recommendations | Reference(s) |
|---|---|---|---|
| Q1. Are people who are pregnant more susceptible to the effects of nuclear radiation exposure, such as an increased risk for severe illness or death? | |||
| Japan | Atomic bombing | No evidence that radiation causes increased illness severity (e.g., worse acute radiation syndrome symptoms such as vomiting) among pregnant women compared with other WRA | 16 |
| Q2. Are people who are pregnant at increased risk for pregnancy complications and adverse pregnancy outcomes after a radiation emergency? | |||
| Finland | Chernobyl | Spontaneous abortion or miscarriage | 32,47 |
| Norway | Chernobyl | Spontaneous abortion or miscarriage | 17,18,48 |
| Japan | Atomic bombing | Spontaneous abortion or miscarriage | 49 |
| Ukraine | Chernobyl | Spontaneous abortion or miscarriage | 17 |
| United States | Three Mile Island Accident | Spontaneous abortion or miscarriage | 50 |
| United States | N/A | Spontaneous abortion or miscarriage | 4 |
| Finland | Chernobyl | Stillbirth | 17 |
| Germany | Chernobyl | Stillbirth | 17 |
| Greece, Hungary, Poland, Sweden | Chernobyl | Stillbirth | 17 |
| Japan | Atomic bombing | Stillbirth | 49,51 |
| Germany | Chernobyl | Perinatal death | 17,32 |
| Belarus | Chernobyl | Perinatal death | 17,19 |
| Ukraine | Chernobyl | Perinatal death | 17 |
| Japan | Fukushima accident | Perinatal death | 20 |
| Belarus | Chernobyl | Pregnancy complications (pre-eclampsia) | 19 |
| Q3. Are there special considerations for treatment, prophylaxis, and/or interventions for people who are pregnant and postpartum? | |||
| United States | N/A | Treatment for pregnant people can cross placenta | 22,52,53 |
| United States | N/A | Treatment for lactating people detected in breastmilk | 22,52,53 |
| United States | N/A | Safe treatments for pregnant people and specialist follow-up | 21–24,52,54 |
| United States | N/A | Safe treatments for lactating people and infants | 21–24,52 |
| Q4. Are exposed WRA at increased risk for negative long-term health outcomes such as cancer or infertility? | |||
| Belarus | Chernobyl | Breast cancer | 27 |
| Russia | Chernobyl | Breast cancer | 28 |
| Japan | Atomic bombing | Ovarian cancer | 55 |
| Israel | Chernobyl | Increased fertility treatments among exposed immigrants from Belarus and Ukraine | 30 |
| China | Xinhou accident | Impaired fertility | 56 |
| Japan | Atomic bombing | Transient amenorrhea | 29 |
| Q5. Are infants with exposure in utero at increased risk for death, disability, or severe illnesses? | |||
| Belarus | Chernobyl | Congenital malformations | 17,19 |
| Belarus, Berlin, Scotland | Chernobyl | Congenital malformations—Down’s syndrome | 32 |
| Bulgaria | Chernobyl | Congenital malformations—heart and central nervous system | 17,32 |
| Germany | Chernobyl | Congenital malformations—cleft lip and palate | 17 |
| Turkey | Chernobyl | Congenital malformations—neural tube defects | 17,32,57 |
| Ukraine | Chernobyl | Congenital malformations | 17,58 |
| United States | N/A | Congenital malformations | 4 |
| Ukraine | Chernobyl | Impaired growth | 34 |
| United States | N/A | Impaired growth | 4 |
| Belarus | Chernobyl | Neurodevelopmental delays | 38 |
| Belarus, Russia, Ukraine | Chernobyl | Neurodevelopmental delays | 17,19 |
| Japan | Atomic bombing | Neurodevelopmental delays | 33,35,59,60 |
| United States | N/A | Neurodevelopmental delays | 4 |
| Germany | Chernobyl | Infant death | 17 |
| Japan | Atomic bombing | Infant death | 29,61 |
| Poland | Chernobyl | Infant death | 17 |
| Russia | Techa River Wastewater Contamination | Infant death | 62 |
| Ukraine | Chernobyl | Infant death | 17 |
| United States | N/A | Infant death | 4 |
| Japan | Atomic bombing | Cancer | 36,63 |
| Japan | Atomic bombing | Cancer—childhood leukemia | 59 |
| Germany, Greece, the United Kingdom | Chernobyl | Cancer—childhood leukemia | 17,64 |
| Europe | Chernobyl | Cancer—childhood leukemia | 65 |
| Ukraine | Chernobyl | Cancer—thyroid | 37 |
| Q6. Are there infant feeding considerations for exposed postpartum and lactating people? | |||
| United Kingdom | Chernobyl | Radionuclides detected in breast milk | 66 |
| Japan | Fukushima accident | Radionuclides detected in breast milk | 40 |
| Italy | Chernobyl | Radionuclides detected in breast milk | 39,67 |
| United States | N/A | Recommendations on infant feeding | 9,42 |
N/A, Not Applicable; WRA, women of reproductive age.
We adapted our guiding principles for addressing the needs of pregnant people into six questions specific to the needs of WRA and infants during radiation emergencies: (1) Are people who are pregnant more susceptible to the effects of nuclear radiation exposure, such as an increased risk for severe illness or death? (2) Are people who are pregnant at increased risk for pregnancy complications and adverse pregnancy outcomes after a radiation emergency? (3) Are there special considerations for treatment, prophylaxis, and/or interventions for people who are pregnant, postpartum, and lactating? (4) Are exposed WRA at increased risk for negative long-term health outcomes such as cancer or infertility? (5) Are infants with exposure in utero at increased risk for death, disability, or severe illnesses? (6) Are there infant feeding considerations for exposed postpartum and lactating people?14,15
We searched MEDLINE, Embase, CINAHL, and Scopus databases to identify relevant literature published from January 1950 to March 2022. Search strategy included terms related to nuclear accidents, radiation exposure, radiation effects, pregnancy, and birth. We limited our review to English language, original research, case reports, review articles, and government websites or reports.
We reviewed over 3800 articles, and excluded literature about medical/radiation therapy, nuclear medicine procedures, and radiation exposure of pregnant health care workers (Fig. 1). A total of 200 articles on WRA and their infants were included from the literature search. In addition, we scanned more than 20 government websites and reports to supplement results from our literature search to add to the quick reference guide.
FIG. 1.
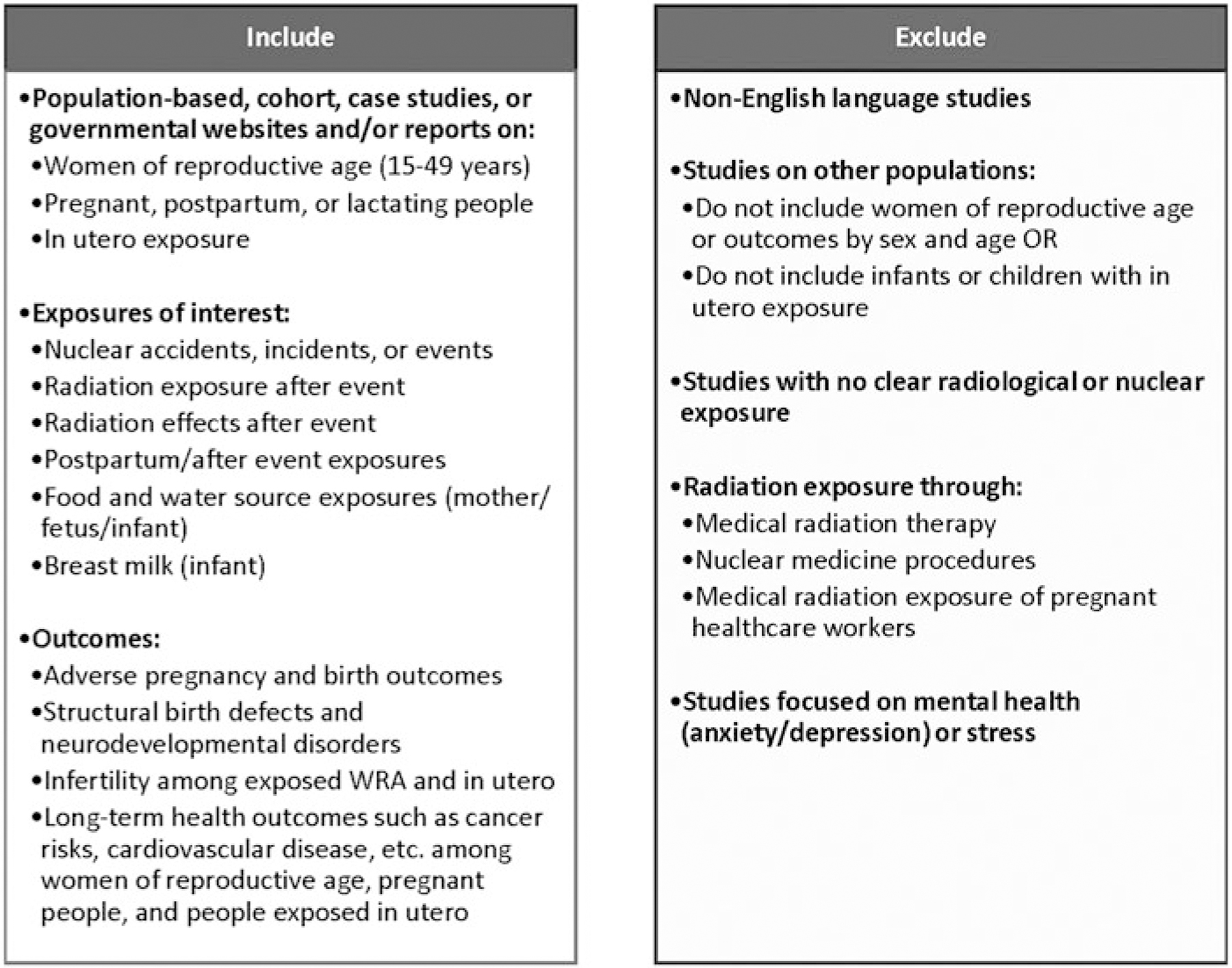
Radiation emergency quick reference guide about WRA, including pregnant, postpartum, and lactating people, and infants’ inclusion criteria. WRA, women of reproductive age.
Summary of Findings on the Effects of Nuclear Radiation on WRA and Infants Provided in the Radiation Emergency Quick Reference Guide
The purpose of the quick reference guide is to highlight select references addressing the six major WRA questions, including pregnant, postpartum, and lactating people (15–49 years), and infants. These questions were adapted from our previously published guiding principles for assessing potential and emerging threats to WRA during emergencies.
We added two questions related to infant considerations after exposure that include feeding during emergencies and long-term outcomes of infants exposed in utero.14,15 The results of the literature review include the following number of articles per question: are pregnant women more suceptible to nuclear radiation (n = 1); are pregnant women more likely to have pregnancy complications (n = 26); special treatment considerations for WRA and infants (n = 0); long-term outcomes after radiation exposure for WRA (n = 14); increased risk of disability, illness, or death for people with in utero radiation exposure (n = 155); and infant feeding considerations (n = 15).
Of these, a total of 38 articles and eight governmental websites are highlighted to address the six questions on the potential exposure risk to WRA and infants. These 38 articles were selected to highlight the outcomes of interest among WRA, including people who are pregnant, postpartum, and lactating, or infants because they discussed an original finding, provided an estimated level exposure, summarized two or more outcomes, and/or had a large sample size. Whenever needed, we supplemented information from eight governmental websites for populations of interest.
Are people who are pregnant more susceptible to the effects of nuclear radiation exposure, such as an increased risk for severe illness or death?
A study with evidence to determine whether people who are pregnant have increased radiosensitivity after exposure from a radiation incident compared with other WRA.16 One study of non-cancer biomarkers indicative of long-term radiation effects did not detect a statistically significant difference between people who were pregnant and those who were not at the time of the Hiroshima and Nagasaki bombings in 1945.16
Biomarkers included serum cholesterol, white blood cell count, erythrocyte sedimentation rate, hemoglobin level, chromosome aberration frequency, glycophorin A locus mutation rate, and naive CD4 T cell count. No studies were found that assessed the risk of death due to acute radiation syndrome among people who are pregnant and WRA.
Are people who are pregnant at increased risk for pregnancy complications and adverse pregnancy outcomes after a radiation emergency?
There was evidence of increased adverse reproductive health outcomes after radiological exposure following the Chernobyl accident in Europe according to several ecological studies.17 Adverse reproductive health outcomes included spontaneous abortion, stillbirth, and perinatal deaths.17 In the 1st year after the Chernobyl accident, spontaneous abortions (i.e., miscarriage, defined here as pregnancy losses up to 16 weeks) in Norway increased from 7.4% in the 12 months before the accident to 8.3% after the accident.18 Some studies suggest that risk for adverse pregnancy outcomes may be related to concentration and duration of radiation dosage.19,20
Another study assessed pregnancy complications after radiation exposure during Chernobyl. People who were pregnant and lived in heavily contaminated areas in Belarus had an increase in maternal morbidity due to higher rates of anemia, renal insufficiency (i.e., kidney disease, defined by elevated creatinine and blood or serum urea nitrogen levels in the circulation), and pre-eclampsia compared with less exposed areas in Belarus after Chernobyl.19
Are there special considerations for treatment, prophylaxis, and/or interventions for people who are pregnant, postpartum, or lactating?
There are several medical countermeasures for internal radiation contamination depending on the dose and radioactive isotope involved. Potassium Iodide (KI), Prussian Blue, and Diethylenetriamine Pentaacetate (DTPA) are common treatments for internal contamination; however, the treatment choice differs by the exposure and certain risk factors (e.g., age, radioactive dose, thyroid exposure/cancer risk, pregnancy/lactation status).21,22
In 2001, the United States Federal Drug Administration (FDA) reviewed data from Chernobyl on the relationship between radioactive dose and thyroid cancer risks. KI is a type of iodine that is not radioactive and can be used to help block one type of radioactive material, radioactive iodine, from being absorbed by the thyroid.22 The FDA revised its recommendations for the administration of based on age, predicted thyroid exposure, and pregnancy and lactation status.22
Iodine, whether stable or radioactive, can cross the placenta in pregnant people and can be detected in breast milk of lactating people. When treating pregnant and lactating people after radiation exposure, one dose of potassium iodine (130 mg) is recommended at the lowest threshold exposure of >5 Gy to minimize the risk of blocking thyroid function in the fetus or nursing infant.19 In cases of severe contamination in lactating people, repeat dosing may be given and nursing neonates should be monitored for signs of illness.22
DTPA is a chelating agent used to counteract the effects of radioactive metals such as plutonium, americium, and curium.23 There are special considerations for DTPA treatment for people who are pregnant. If available, it is recommended to use pentetate zinc trisodium injection (Zn-DTPA) rather than pentetate calcium trisodium injection (Ca-DTPA) for pregnant women.21 The main side of effect of Ca-DTPA is a loss of essential metals, such as zinc, and should only be used for pregnant women to only treat very high levels of internal radioactive contamination.21 Either Zn-DTPA or Ca-DTPA (with vitamins and a zinc supplement) are safe to use to treat people who are lactating.21
Finally, Prussian Blue is a chelator that is used to remove radioactive cesium (Cs) and thallium (TI) from inside a person’s body. Prussian Blue is safe for use with people who are pregnant, postpartum, lactating, and infants.24 Due to these special considerations, after contamination and treatment, people who are pregnant are advised to visit a maternal-fetal specialist for an assessment of risk to the fetus and multidisciplinary management of related hematopoietic, gastrointestinal, central nervous system, and subcutaneous syndromes.23
Are exposed WRA at increased risk for negative long-term health outcomes, such as cancer or infertility?
People who receive high doses of radiation, including WRA, could have a greater risk of developing cancer (e.g., thyroid cancer) later in life compared with the general adult population, depending on radiation exposure.25,26 There is evidence of an increased risk of breast cancer among exposed WRA based on dose level.27 There may be an elevated risk of breast cancer from a radiation emergency among lactating women compared with the general population.28
Literature on future fertility effects among WRA after radiation emergencies is sparse. However, temporary amenorrhea (up to 18 months) was reported after Hiroshima, and increased use of fertility treatments have been reported among exposed WRA after Chernobyl.29,30 There are other non-cancer effects for adults, including WRA, such as cardiovascular disease and cataracts.31
Are infants with exposure in utero at increased risk for death, disability, or severe illnesses?
The fetal health consequences of exposure at doses greater than 0.5 Gy can be severe, depending on the stage of fetal development—even if such a dose is too low to cause an immediate effect for the pregnant person.4 In utero radiation exposure can lead to the development of congenital malformations such as Down’s syndrome, neural tube defects, cleft lip and palate, and/or infant death.4,17,32,33 Infants with in utero exposure can also experience poor long-term outcomes such as: adverse growth, developmental or neurological outcomes, and cancer.4,17,34–38 Risk is highest if exposure occurs during early fetal development, between 2 and 18 weeks of gestation.4
Are there feeding considerations for infants of exposed postpartum and lactating people?
In a radiation emergency, lactating people can pass radioactive materials to their infants through breastmilk if they are externally exposed to radiation, or become internally contaminated through eating or drinking contaminated food or water, or breathing contaminated air.39 A study after the Fukushima nuclear accident found that radionuclides can be detected in breast milk, and in some cases, at higher levels than tap water in their area.40
Further, lactating people with thyroid conditions transfer radionuclides into breast milk at a higher rate than those without a thyroid condition, increasing the exposure risk to the infant.41 It is important to note that formula feeding can also result in exposure to the infant if mixed with water from a contaminated source.9,42 Recommendations for infant feeding could vary depending on the radiation exposure type, dose absorbed, and access to resources (e.g., breast milk expressed before the emergency, ready-to-feed infant formula, safe drinking water for mixing infant formula).9,42
DRH Participation in Preparedness Training and Exercises
As part of the CDC’s Training and Exercise Preparedness Program, the DRH has collaborated with staff across CDC programs to design and implement preparedness and response training and exercises. In 2017, the CDC participated in the Gotham Shield Exercise, which included both a weeklong full-scale emergency simulation and brief half-day tabletop exercises, beginning with an alert of a nuclear-radiological incident.
This exercise simulated emergency response operations to detonation of a nuclear device in a large U.S. city in Federal Emergency Management Agency (FEMA) Region II. During the 4 days of the exercise, the CDC simulated activities focused on the following objectives: (1) assessing the CDC’s ability to activate staff and equip the CDC Incident Management System for a nuclear incident; (2) verify information flow plans, policies, and procedures during a nuclear radiological incident; (3) assess the CDC’s ability to share timely information with relevant partners; and (4) assess the ability to identify and report on the status of CDC assets and personnel in a region affected by a nuclear-radiological incident.
Trained response team members from DRH were actively engaged, responding to hypothetical scenarios introduced throughout the course of the exercise. Activities included estimating the number of pregnant people in the affected area using DRH Pregnancy Estimator, responding to national inquiries relating to the health of maternal and infant populations, developing emergency risk communication messages, and providing technical expertise to support early surveillance activities.43
This active engagement allowed the CDC to optimize DRH staff capacity for radiation emergency responses, practice the application of reproductive health subject matter expertise to management of nuclear-radiological emergencies, identify gaps in data to inform guidance for people who are pregnant, postpartum, or lactating, and better streamline processes and procedures for responding to public health needs of people who are pregnant, postpartum, or lactating during a radiation emergency.
The DRH has continued collaborating with interdisciplinary staff (e.g., clinicians, epidemiologists, data managers, health communicators, and health physicists) across the agency to address the needs of WRA, including people who are pregnant, postpartum, or lactating, and infant health populations, during a radiation emergency.
Nearly 5 years later, the CDC participated in the 2022 Cobalt Magnet exercise. Cobalt Magnet was a full-scale simulation of a Radiological Dispersal Device in FEMA Region VI, enabling response personnel to practice protecting public health and safety, providing emergency relief to affected populations, and restoring essential services. The 4-day exercise was held May 16–20, 2022. More than 30 local, state, and federal agencies, and hospitals were involved in the exercise.
The DRH team activated for the exercise as part of the CDC’s At-Risk Task Force, an all-hazards preparedness and response team focusing on the needs of populations with access and functional needs in emergencies, including infants and people who are pregnant, postpartum, or lactating. Specifically, DRH staff answered questions, and prepared partner e-mails, talking points, and social media risk communication messages for people who are pregnant, postpartum, or lactating; they also developed a 100-day strategic plan for surveillance of adverse outcomes among people who are pregnant, postpartum, or lactating.44
The DRH has also supported state and regional nuclear radiation exercises. In July 2022, DRH staff supported a readiness response exercise in FEMA Region IV, both on-site and virtually. Participants from local, state, and federal agencies assisted with the exercise at a mock community reception center (CRC), which is expected to be erected after a nuclear power plant emergency and used for individual screening, evaluation, and decontamination.44
As part of the exercise, state and local staff evaluated potentially affected people for medical treatment due to radioactive contamination, scanned individuals’ bodies and recorded the radiation contamination levels, and counseled people on potential long-term health effects. More than 150 participants underwent contamination screening, decontamination showering, and registration.
During the simulation, it was found that information on pregnancy status was not routinely collected from people arriving at the CRC, despite several scenarios where the participants actively disclosed that they were pregnant. The DRH staff provided feedback during an after-action review of the exercise to include a standard question on the screening questionnaire about pregnancy and infant feeding.
Discussion
People who are pregnant, postpartum, or lactating, and infants, have unique needs and risks for adverse outcomes during radiation emergencies. Due to these unique needs and potential risks, it is critical to incorporate questions about pregnancy, lactation status, and infant feeding into any data collection effort. Information about pregnancy status (Y/N) and estimated date of delivery is needed for pregnant people.
For people with infants, information on typical infant feeding practices (breastfeeding, formula feeding, or mixed feeding) is needed. There is also a need for linked longitudinal data to provide surveillance and monitoring of pregnancy and infant outcomes after nuclear or radiological incidents.45
The DRH collaborated across CDC on nuclear radiation activities to address the needs of WRA, including people who are pregnant, postpartum, or lactating, and infants. One of the activities included developing an internal resource guide that included six questions that staff should ask individuals who are screened during a radiation emergency. Two of the questions specifically addressed infants’ exposure and feeding. The DRH then developed activities and exercises to train inter-agency staff for radiation emergencies and incorporated this information into the resource guide.
The DRH participation in functional exercises highlighted the need for (1) clear information on what is known about pregnant people at the beginning of an emergency; (2) specific questions about pregnancy status and infant feeding practices and incorporating responses into any data collection efforts; (3) long-term monitoring of health needs and outcomes of people who are pregnant, postpartum, or lactating, and their infants; and (4) collaborations across the agency to address the special needs of these populations (e.g., working with the CDC’s Division of Nutrition, Physical Activity, and Obesity or the National Center on Birth Defects and Developmental Disabilities to highlight risks for pregnant, postpartum, and lactating people and infants).
During an emergency, WRA and people who are pregnant, postpartum, or lactating are advised to follow the same protective instructions as everyone else (e.g., shelter in place until it is safe to go outside).8,9 If referred to a CRC for screening, it is recommended that on arrival at the facility they notify staff members that they are pregnant, postpartum, or lactating and how they are feeding their infant.8,9 The CRC evaluation process often includes referrals for medical care.8,9
Once safe to do so, pregnant, postpartum, or lactating people should seek medical attention to continue prenatal or postpartum care. In addition, guidance is available for infant feeding during emergencies, and specifically during radiation emergencies, that can serve as a resource to public health responders.9,46
It is important to include reproductive health subject matter experts in planning for and response to radiation emergencies to ensure that data collection is adapted to the needs of WRA and infants. The results of our literature search found that there are unique considerations for WRA and infants after radiation emergencies. Our analysis had some limitations.
First, our search included articles only in the English language, which could introduce bias due to some incidents taking place in countries where English is not the primary language. Second, multiple studies assessed the same disaster and outcomes. Third, most studies did not have a direct measure of radiological exposure. Fourth, some studies had small sample sizes. Finally, we excluded studies that solely assessed mental health outcomes, such as anxiety or stress during or after radiation emergencies due to the complex relationship of mental health with exposure and our outcomes of interest. Further, we considered it a topic that deserves its own literature search.
Public health surveillance and research on reproductive health outcomes should be initiated as soon as possible after an incident. The Radiation Emergency Quick Guide is intended to be a resource that can be used to quickly assess the literature on the unique considerations of WRA during radiation emergencies. More information is needed for a more robust assessment of the potential impacts of radiation emergencies on pregnant, postpartum, and lactating people, and infants.
When planning and responding to nuclear emergencies, considerations for the unique needs of WRA and infants are important. The DRH will continue to support emergency planning and preparedness activities (e.g., drills, state, and federal functional exercises). We will develop and maintain subject matter expertise. We will also work collaboratively (e.g., across the CDC, federal government, and state and local partners) to develop and update tailored communication materials for different audiences on the special circumstances that nuclear and radiological emergencies pose to WRA, pregnant, postpartum, or lactating people, and infants.
Supplementary Material
Acknowledgments
Members of the Division of Reproductive Health Emergency Preparedness and Response Team: Mehreen Meghani, MPH and Maria Rivera, MPH.
Funding Information
No funding was received for this article.
Footnotes
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.
Author Disclosure Statement
The authors did not report any potential conflicts of interest.
Supplementary Material
References
- 1.US. Congress, 116 sess (Sen. Burr RR-N 2019). S. 1379, Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019. 2019. Available from: https://www.congress.gov/113/plaws/publ5/PLAW-113publ5.pdf [Last accessed: October 7, 2022].
- 2.Centers for Disease Control and Prevention National Center for Environmental Health. Acute Radiation Syndrome: A Fact Sheet for Clinicians. 2018. Available from: https://www.cdc.gov/nceh/radiation/emergencies/arsphysicianfactsheet.htm [Last accessed: September 27, 2022].
- 3.Centers for Disease Control and Prevention. National Center for Environmental Health. Types of Radiation Emergencies. 2018. Available from: https://www.cdc.gov/nceh/radiation/emergencies/typesofemergencies.htm [Last accessed: September 27, 2022].
- 4.Centers for Disease Control and Prevention National Center for Environmental Health. Radiation and Pregnancy: A Fact Sheet for Clinicians. 2020. Available from: https://www.cdc.gov/nceh/radiation/emergencies/prenatalphysician.htm [Last accessed: September 27, 2022].
- 5.Centers for Disease Control and Prevention. National Center for Environmental Health. Contamination vs. Exposure. 2022. Available from: https://www.cdc.gov/nceh/radiation/emergencies/contamination.htm [Last accessed: September 27, 2022].
- 6.Centers for Disease Control and Prevention. National Center for Environmental Health. Possible health effects of radiation exposure and contamination. 2018. Available from: https://www.cdc.gov/nceh/radiation/emergencies/healtheffects.htm [Last accessed: July 10, 2023].
- 7.Salame-Alfie A, Whitcomb RC, Evans CL, et al. Developing a radiation-savvy public health workforce. Environ Adv 2022;9:100269; doi: 10.1016/j.envadv.2022.100269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Centers for Disease Control and Prevention. National Center for Environmental Health. Radiation Emergencies. Radiation Emergencies & Your Health—Pregnancy. 2022. Available from: https://www.cdc.gov/nceh/radiation/emergencies/prenatal.htm [Last accessed: September 30, 2022].
- 9.Centers for Disease Control and Prevention. National Center for Environmental Health. Radiation Emergencies. Radiation Emergencies & Your Health—Infant Feeding. 2023. Available from: https://www.cdc.gov/nceh/radiation/emergencies/breastfeeding.html [Last accessed: July 10, 2023].
- 10.Department of Homeland Security. Quick Reference Guide: Radiation Risk Information for Responders Following a Nuclear Detonation. 2016. Available from: https://www.dhs.gov/sites/default/files/publications/Quick%20Reference%20Guide%20Final.pdf [Last accessed: December 09, 2022].
- 11.ICRP (International Commission on Radiological Protection). Pregnancy and medical radiation. ICRP Publication 84. Ann. ICRP 30 (1). 2000. [DOI] [PubMed] [Google Scholar]
- 12.Centers for Disease Control and Prevention National Center for Environmental Health. Radiation Emergencies Resource Library. 2022. Available from: https://www.cdc.gov/nceh/radiation/emergencies/resourcelibrary/all.htm [Last accessed: September 27, 2022].
- 13.Centers for Disease Control and Prevention National Center for Environmental Health. Radiation Emergency Training, Education, and Tools. 2022. Available from: https://www.cdc.gov/nceh/radiation/emergencies/training.htm [Last accessed: September 27, 2022].
- 14.Perez M, Galang RR, Snead MC, et al. Emergency preparedness and response: Highlights from the Division of Reproductive Health, 2011–2021. J Womens Health 2021; 30(12):1673–1680; doi: 10.1089/jwh.2021.0553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Watson AK, Ellington S, Nelson C, et al. Preparing for biological threats: Addressing the needs of pregnant women. Birth Defects Res 2017;109(5):391–398; doi: 10.1002/bdr2.1016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Miles EF, Tatsukawa Y, Funamoto S, et al. Biomarkers of radiosensitivity in a-bomb survivors pregnant at the time of bombings in hiroshima and nagasaki. ISRN Obstet Gynecol 2011;2011:264978; doi: 10.5402/2011/264978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Busby C, Lengfelder E, Pflugbeil S, et al. The evidence of radiation effects in embryos and fetuses exposed to Chernobyl fallout and the question of dose response. Med Conflict Surv 2009;25(1):20–40. [DOI] [PubMed] [Google Scholar]
- 18.Irgens LM, Lie RT, Ulstein M, et al. Pregnancy outcome in Norway after Chernobyl. Biomed Pharmacother 1991; 45(6):233–241. [DOI] [PubMed] [Google Scholar]
- 19.Petrova A, Gnedko T, Maistrova I, et al. Morbidity in a large cohort study of children born to mothers exposed to radiation from Chernobyl. Stem Cells 1997;15(Suppl. 2): 141–150. [DOI] [PubMed] [Google Scholar]
- 20.Scherb HH, Mori K, Hayashi K. Increases in perinatal mortality in prefectures contaminated by the Fukushima nuclear power plant accident in Japan: A spatially stratified longitudinal study. Medicine (Baltimore) 2016;95(38): e4958; doi: 10.1097/MD.0000000000004958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.National Center for Environmental Health. Medical Countermeasures (Treatments) for Radiation Exposure and Contamination. 2022. Available from: https://www.cdc.gov/nceh/radiation/emergencies/countermeasures.htm [Last accessed: October 17, 2022].
- 22.Food and Drug Administration. Guidance Potassium Iodide as a Thyroid Blocking Agent in Radiation Emergencies. 2001. Available from: https://www.fda.gov/media/72510/download [Last accessed: September 27, 2022].
- 23.National Center for Environmental Health. DTPA (Diethylenetriamine pentaacetate). 2018. Available from: https://www.cdc.gov/nceh/radiation/emergencies/dtpa.htm [Last accessed: October 17, 2022].
- 24.National Center for Environmental Health. Prussian Blue. 2022. Available from: https://www.cdc.gov/nceh/radiation/emergencies/prussianblue.htm [Last accessed: October 7, 2022].
- 25.Centers for Disease Control and Prevention. National Center for Environmental Health. Cancer and Long-Term Health Effects of Radiation Exposure and Contamination. 2018. Available from: https://www.cdc.gov/nceh/radiation/emergencies/cancer.htm [Last accessed: September 30, 2022].
- 26.Richardson DB. Exposure to ionizing radiation in adulthood and thyroid cancer incidence. Epidemiology 2009; 20(2):181–187. [DOI] [PubMed] [Google Scholar]
- 27.Rivkind N, Stepanenko V, Belukha I, et al. Female breast cancer risk in Bryansk Oblast, Russia, following prolonged low dose rate exposure to radiation from the Chernobyl power station accident. Int J Epidemiol 2020;49(2):448–456; doi: 10.1093/ije/dyz214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cahoon EK, Preston D, Zhang R, et al. Breast cancer risk in residents of Belarus exposed to Chernobyl fallout while pregnant or lactating: Standardized incidence ratio analysis, 1997 to 2016. Int J Epidemiol 2021;23:23; doi: 10.1093/ije/dyab226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tabuchi A, Horii E, Nishida S, et al. Obstetric-gynecological investigation on the exposed. Hiroshima J Med Sci 1955;4(2–3):223–236. [Google Scholar]
- 30.Cwikel J, Sergienko R, Gutvirtz G, et al. Reproductive effects of exposure to low-dose ionizing radiation: A long-term follow-up of immigrant women exposed to the Chernobyl accident. J Clin Med 2020;9(6):08; doi: 10.3390/jcm9061786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.National Cancer Institute. Accidents at Nuclear Power Plants and Cancer Risk. 2022. Available from: https://www.cancer.gov/about-cancer/causes-prevention/risk/radiation/nuclear-accidents-fact-sheet [Last accessed: October 7, 2022].
- 32.Dubrova YE. Long-term genetic effects of radiation exposure. Mutat Res 2003;544(2–3):433–439; doi: 10.1016/j.mrrev.2003.05.003. [DOI] [PubMed] [Google Scholar]
- 33.Otake M, Schull WJ. Radiation-related small head sizes among prenatally exposed A-bomb survivors. Int J Radiat Biol 1993;63(2):255–270; doi: 10.1080/09553009314550341. [DOI] [PubMed] [Google Scholar]
- 34.Hatch M, Little MP, Brenner AV, et al. Neonatal outcomes following exposure in utero to fallout from Chernobyl. Eur J Epidemiol 2017;32(12):1075–1088; doi: 10.1007/s10654-017-0299-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Otake M, Schull WJ. Radiation-related brain damage and growth retardation among the prenatally exposed atomic bomb survivors. Int J Radiat Biol 1998;74(2):159–171; doi: 10.1080/095530098141555. [DOI] [PubMed] [Google Scholar]
- 36.Sugiyama H, Misumi M, Sakata R, et al. Mortality among individuals exposed to atomic bomb radiation in utero: 1950–2012. Eur J Epidemiol 2021;36(4):415–428; doi: 10.1007/s10654-020-00713-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hatch M, Brenner AV, Cahoon EK, et al. Thyroid cancer and benign nodules after exposure in utero to fallout from Chernobyl. J Clin Endocrinol Metab 2019;104(1):41–48; doi: 10.1210/jc.2018-00847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kolominsky Y, Igumnov S, Drozdovitch V. The psychological development of children from Belarus exposed in the prenatal period to radiation from the Chernobyl atomic power plant. J Child Psychol Psychiatry Allied Discip 1999;40(2):299–305. [PubMed] [Google Scholar]
- 39.Giussani A, Risica S. Validation of the ICRP model for caesium intake by lactating mothers with Italian data after the Chernobyl fallout. Environ Int 2012;39(1):122–127; doi: 10.1016/j.envint.2011.10.010. [DOI] [PubMed] [Google Scholar]
- 40.Unno N, Minakami H, Kubo T, et al. Effect of the Fukushima nuclear power plant accident on radioiodine 131I content in human breast milk. J Obstet Gynaecol Res 2012; 38(5):772–779; doi: 10.1111/j.1447-0756.2011.01810.x. [DOI] [PubMed] [Google Scholar]
- 41.Simon SL, Luckyanov N, Bouville A, et al. Transfer of 131I of 131I into human breast milk and transfer coefficients for radiological dose assessments. Health Phys 2002; 82(6):796–806. [DOI] [PubMed] [Google Scholar]
- 42.Mountford PJ, Coakley AJ. A review of the secretion of radioactivity in human breast milk: Data, quantitative analysis and recommendations. Nuclear Med Commun 1989; 10(1):15–27; doi: 10.1097/00006231-198901000-00003. [DOI] [PubMed] [Google Scholar]
- 43.Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion. Division of Reproductive Health. Toolkits for Emergency Planning and Response. Pregnancy Estimator. Available from: https://www.cdc.gov/reproductivehealth/emergency/tools.html [Last accessed: July 18, 2023].
- 44.Centers for Disease Control and Prevention. Center for Preparedness and Response. 2023. Available from: https://www.cdc.gov/cpr/index.htm [Last accessed: July 11, 2023].
- 45.Woodworth KR, Reynolds MR, Burkel V, et al. A preparedness model for mother–baby linked longitudinal surveillance for emerging threats. Matern Child Health J 2021; 25(2):198–206; doi: 10.1007/s10995-020-03106-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion. Division of Nutrition, Physical Activity, and Obesity. Infant and young child feeding in emergencies toolkit. 2022. Available from: https://www.cdc.gov/nutrition/emergencies-infant-feeding/index.html [Last accessed: September 27, 2022].
- 47.Auvinen A, Vahteristo M, Arvela H, et al. Chernobyl fallout and outcome of pregnancy in Finland. Environ Health Perspect 2001;109(2):179–185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ulstein M, Jensen TS, Irgens LM, et al. Outcome of pregnancy in one Norwegian county 3 years prior to and 3 years subsequent to the Chernobyl accident. Acta Obstetr Gynecol Scand 1990;69(4):277–280. [DOI] [PubMed] [Google Scholar]
- 49.Tabuchi A A study of the productivity and offspring of women exposed to the atomic bomb. Hiroshima J Med Sci 1957;5(4):309–316. [Google Scholar]
- 50.Goldhaber MK, Staub SL, Tokuhata GK. Spontaneous abortions after the Three Mile Island nuclear accident: A life table analysis. Am J Public Health 1983;73(7):752–759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Scherb H, Weigelt E, Bruske-Hohlfeld I. European stillbirth proportions before and after the Chernobyl accident. Int J Epidemiol 1999;28(5):932–940. [DOI] [PubMed] [Google Scholar]
- 52.Food and Drug Administration. Frequently Asked Questions on Potassium Iodide (KI). 2011. Available from: https://www.fda.gov/drugs/bioterrorism-and-drug-preparedness/frequently-asked-questions-potassium-iodide-ki [Last accessed: September 27, 2022].
- 53.International Atomic Energy Agency. Radiation protection of pregnant women in nuclear medicine. 2022. Available from: https://www.iaea.org/resources/rpop/health-professionals/nuclear-medicine/pregnant-women [Last accessed: October 7, 2022].
- 54.Waselenko JK, MacVittie TJ, Blakely WF, et al. Medical management of the acute radiation syndrome: Recommendations of the Strategic National Stockpile Radiation Working Group. Ann Intern Med 2004;140(12):1037–1051. [DOI] [PubMed] [Google Scholar]
- 55.Utada M, Brenner AV, Preston DL, et al. Radiation risk of ovarian cancer in atomic bomb survivors: 1958–2009. Radiat Res 2021;195(1):60–65; doi: 10.1667/RADE-20-00170.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Zhang ZH, Liang L, Zhang SL, et al. Follow-up study of a pregnant woman 16 years after exposure in the Xinzhou radiation accident. J Radiol Prot 2011;31(4):489–494; doi: 10.1088/0952-4746/31/4/N01. [DOI] [PubMed] [Google Scholar]
- 57.Caglayan S, Kayhan B, Mentesoglu S, et al. Changing incidence of neural tube defects in Aegean Turkey. Paediatr Perinat Epidemiol 1989;3(1):62–65. [DOI] [PubMed] [Google Scholar]
- 58.Volosovets OP, Kryuchko TO, Veselskyi VL, et al. Congenital anomalies in children of Ukraine: 25-Year monitoring of morbidity and prevalence. Wiadomosci Lekarskie 2020;73(10):2193–2197. [PubMed] [Google Scholar]
- 59.McCollough CH, Schueler BA, Atwell TD, et al. Radiation exposure and pregnancy: When should we be concerned? Radiographics 2007;27(4):909–917; discussion 917. [DOI] [PubMed] [Google Scholar]
- 60.Miller RW. Delayed effects of external radiation exposure: A brief history. Radiat Res 1995;144(2):160–169. [PubMed] [Google Scholar]
- 61.Yamazaki JN, Wright SW, Wright PM. A study of the outcome of pregnancy in women exposed to the atomic bomb blast in Nagasaki. J Cell Comparat Physiol 1954; 43(Supp, 1):319–328. [DOI] [PubMed] [Google Scholar]
- 62.Ostroumova E, Akleyev A, Hall P. Infant mortality among offspring of individuals living in the radioactively contaminated Techa river area, Southern Urals. Acta Med Nagasakiensia 2005;50(Suppl. 1):23–28. [Google Scholar]
- 63.Preston DL, Cullings H, Suyama A, et al. Solid cancer incidence in atomic bomb survivors exposed in utero or as young children. J Natl Cancer Inst 2008;100(6):428–436; doi: 10.1093/jnci/djn045. [DOI] [PubMed] [Google Scholar]
- 64.Busby CC. Very low dose fetal exposure to Chernobyl contamination resulted in increases in infant leukemia in Europe and raises questions about current radiation risk models. Int J Environ Res Public Health 2009;6(12):3105–3114; doi: 10.3390/ijerph6123105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Hoffmann W Has fallout from the Chernobyl accident caused childhood leukaemia in Europe? A commentary on the epidemiologic evidence. Eur J Public Health 2002; 12(1):72–76. [DOI] [PubMed] [Google Scholar]
- 66.Gall M, Mahler S, Wirth E. Transfer of 137Cs into mother’s milk. J Environ Radioact 1991;14(4):331–339; doi: 10.1016/0265-931X(91)90023-9. [DOI] [Google Scholar]
- 67.Venuti GC, Risica S, Rogani A. Radioactive caesium contamination in human milk in Italy after the Chernobyl accident. Radiat Protect Dosimetry 1991;37(1):43–49. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.