

Abstract
Background
Burnout is a multidimensional psychological syndrome that arises from chronic workplace stress. Health care workers (HCWs), who operate in physically and emotionally exhausting work contexts, constitute a vulnerable group. This, coupled with its subsequent impact on patients and public economic resources, makes burnout a significant public health concern. Various self-care practices have been suggested to have a positive effect on burnout among HCWs. Of these, physical activity stands out for its ability to combine psychological, physiological, and biochemical mechanisms. In fact, it promotes psychological detachment from work and increases self-efficacy by inhibiting neurotransmitters and neuromodulators, increasing endorphin levels, enhancing mitochondrial function, and attenuating the hypothalamic pituitary-adrenal axis response to stress.
Objective
Our objective was to conduct a systematic review of the evidence on the association between physical activity and burnout among HCWs.
Methods
We considered HCWs, physical activity, and burnout, framing them as population, exposure, and outcome, respectively. We searched APA PsycArticles, MEDLINE, and Scopus until July 2022. We extracted relevant data on study design, methods to measure exposure and outcome, and statistical approaches.
Results
Our analysis encompassed 21 independent studies. Although 10% (2/21) of the studies explicitly focused on physical activity, the remaining investigations were exploratory in nature and examined various predictors, including physical activity. The most commonly used questionnaire was the Maslach Burnout Inventory. Owing to the heterogeneity in definitions and cutoffs used, the reported prevalence of burnout varied widely, ranging from 7% to 83%. Heterogeneity was also observed in the measurement tools used to assess physical activity, with objective measures rarely used. In total, 14% (3/21) of the studies used structured questionnaires to assess different types of exercise, whereas most studies (18/21, 86%) only recorded the attainment of a benchmark or reported the frequency, intensity, or duration of exercise. The reported prevalence of physically active HCWs ranged from 44% to 87%. The analyses, through a variety of inferential approaches, indicated that physical activity is often associated with a reduced risk of burnout, particularly in the domains of emotional exhaustion and depersonalization. Furthermore, we compiled and classified a list of factors associated with burnout.
Conclusions
Our comprehensive overview of studies investigating the association between physical activity and burnout in HCWs revealed significant heterogeneity in definitions, measurements, and analyses adopted in the literature. To address this issue, it is crucial to adopt a clear definition of physical activity and make thoughtful choices regarding measurement tools and methodologies for data analysis. Our considerations regarding the measurement of burnout and the comprehensive list of associated factors have the potential to improve future studies aimed at informing decision-makers, thus laying the foundation for more effective management measures to address burnout.
Keywords: burnout, Maslach Burnout Inventory, MBI, Copenhagen Burnout Inventory, CBI, Professional Fulfillment Index, PFI, physical activity, health care workers, public health policy
Introduction
Background
Burnout is a multidimensional psychological syndrome resulting from chronic workplace stress. It is characterized by feelings of energy depletion or exhaustion, increased mental distance from one’s own job or cynicism, and reduced professional efficacy [1].
Burnout is gaining attention as a major public health concern for the mental health challenges of health care workers (HCWs) [2]. It poses a threat to the quality of care delivery, especially in terms of patient safety [3], and results in high resource consumption to face its consequences [4,5]. This became even more evident during the COVID-19 pandemic [6], which tightened physicians’ work conditions [7,8], significantly increasing the share of physicians and nurses expressing an intention to leave the profession [9,10], and highlighted the frailty of health care systems in emergency management [11]. Although COVID-19 no longer constitutes a public health emergency [12], HCWs continue to be particularly vulnerable to burnout [13,14], with weakened abilities to manage the typical difficulties of care work and increased exposure to emotionally challenging situations [15]. This is especially true for those directly engaged in patient care given the demanding nature of their roles [16]. They often work long hours, experience sleep deprivation, contend with irregular schedules, and are exposed to emotionally challenging situations. In addition, they face the pressure to master a vast body of clinical knowledge [17]. Furthermore, HCWs are at high risk of workplace injuries [18] and assaults [19,20]. These challenges are compounded by common life stressors such as work-home conflicts, educational debts, relationship status, the age of their children, and the employment status of their partners [21]. As reported in a literature analysis [6], burnout can result in various negative outcomes and criticalities for HCWs, including anxiety, depressive disorders, alcohol abuse or dependence, and suicidal ideation. Burned-out workers experience poor mental health even without a clinically diagnosable disorder, as also proved by the fact that, within this group, there are more mental health problems than in most other occupational groups [22].
Within the broad spectrum of possible public health options to address burnout in HCWs, prioritizing measures to promote mental well-being has become paramount [23,24]. This entails addressing cultural factors, particularly those related to stigma; ensuring protected access to mental health care services; and implementing active policies to encourage healthy lifestyles [25,26]. Among these, physical activity is recognized worldwide as a key strategy for promoting mental well-being [27,28] in addition to helping prevent and manage noncommunicable diseases. However, unlike physical health [29], determining the “optimal dose” of physical activity—considering the combination of intensity, duration, and frequency [30]—for mental well-being remains uncertain and dependent on the specific domain of investigation [27].
A preliminary search of previous systematic reviews on the effects of physical activity on burnout was conducted in Scopus, PubMed, and PROSPERO and resulted in 2 different studies. Naczenski et al [31] found that physical activity was an effective strategy to reduce burnout among workers from various sectors. Regarding health professionals specifically, Bischoff et al [32] identified a potential beneficial effect in health professionals of mind-body practices such as yoga or qigong on occupational stress, one of the conditions for burnout [1].
Objectives
Our study systematically investigated how physical activity was incorporated into studies on burnout among HCWs. Recognizing that strategies created without evidence lead to ineffective programs, wasted resources, and persistently poor health outcomes [33], our ambition was to contribute to the development of evidence-based public health policies.
First, we aimed to provide insights into the reported level of participation in physical activity and the extent of participants at high risk of burnout. We also intended to verify whether a correlation emerges between levels of physical activity and burnout and whether a dose-response association exists.
Our second purpose was to thoroughly assess the quality of the available evidence in terms of collecting, compiling, managing, analyzing, and using health data. This assessment could also offer indications to generate hypotheses for further research to strengthen the body of evidence.
These are essential steps along the road that leads to shaping public health strategies and resource allocation for HCWs’ well-being.
Methods
As recommended for systematic reviews of association studies [34,35], we adopted the population, exposure, and outcome (PEO) approach by considering physical activity habits as the exposure factor and burnout as the outcome. To ensure accuracy and transparency, we followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [36] and the PRISMA-S (PRISMA literature search extension) [37] guidelines.
Eligibility Criteria
The eligibility criteria are detailed in Multimedia Appendix 1.
We included studies that examined the association between physical activity and burnout in health personnel directly involved in the provision of care services, such as physicians, nurses, and technicians, with no restrictions on demographics or workplace context. We considered both qualitative and quantitative measures of physical activity as eligible for inclusion. As we were interested in the association between physical activity and burnout, interventional studies were included regardless of the presence of a control group. A validated assessment tool for burnout (a general work-related stress outcome was not of interest) was mandatory for inclusion.
Our search was not limited by geographic context, funding source, or time horizon. We excluded studies in which physical activity was not distinct from other supportive strategies aimed at managing stress or building resilience or from other mindfulness practices. In addition, studies that focused on yoga or qigong were excluded as these are classified as meditation practices with only a light-intensity component of physical activity when performing respiration and poses [38-40].
Following the recommendation by Munn et al [35] to clearly report the exposure or risk factor and how it was measured or identified, we excluded studies that proposed only a simple question on physical activity without any reference to its frequency (eg, a generic “Yes/No” question on practicing “exercise” or even “regular exercise”). Furthermore, we excluded literature reviews, gray literature, conference proceedings, and unpublished material. Finally, we excluded studies that lacked a quantitative evaluation of the association.
Information Sources
We searched the following electronic databases up to July 2022: MEDLINE through the Ovid platform, APA PsycArticles, and Scopus. Using a “snowballing” approach, we manually screened the reference lists of included articles and conducted systematic citation tracking in Scopus, PubMed, and Google Scholar.
Search Strategy
In total, 2 authors, CGL and PM, developed search strings using the PEO framework to structure the research question. We selected search terms to identify HCWs, physical activity interventions, and burnout. Regarding burnout, to increase search sensitivity, we also considered terms related to the assessment instruments indicated by Rotenstein et al [41] and those identified in the more recent works by Edú-Valsania et al [42] and Shoman et al [43]. Moreover, to further increase the sensitivity of our search, we used the National Library of Medicine–controlled vocabulary thesaurus (Medical Subject Headings) with entry terms and synonyms. We limited the search to articles published in English. The complete search strategy can be found in Multimedia Appendix 2 [41-43].
Duplicates were removed by PM using an automatic procedure based on PubMed ID and digital object identifier, and this was performed in Microsoft Excel (Microsoft Corp).
Selection Process
Search results were retrieved from the databases and double screened independently by all the authors. The initial screening was based on the title and abstract using Rayyan (Rayyan Systems Inc) [44] for support. To refine and clarify the eligibility criteria, ensure consistency when applied by different reviewers, and train the team, a pilot phase was carried out on 500 works. The potentially relevant articles were retrieved for full-text screening, and their eligibility was determined as described in the previous step. Any disagreement was resolved through plenary discussion among all the authors until a consensus was reached.
Data Collection Process
Each selected study was randomly assigned to and independently evaluated by 2 authors to extract relevant data. Any disagreement was addressed as mentioned previously.
Data Items
We extracted 3 different types of information. First, we recorded the general characteristics, such as aim, context (country, workplace, and period), and population (type of HCW, number, and gender mix). Second, we summarized the methods used to measure burnout, the criteria used to quantitatively summarize the phenomenon in the study population, and a possible definition of severity. When possible, we included the frequency distributions of categorical outcomes and means of total scores with SDs. Third, we noted the methods adopted to measure physical activity, including the assessment of frequency, time, or intensity of activity and the percentage of participants practicing physical activity. Finally, we reported the adopted measures of the association between physical activity and burnout along with its strength (P values, odds ratios, and their 95% CIs), eventually derived by AB from published data, and a synthesis of the reported evidence. In addition, factors other than physical activity that are significantly associated with burnout were listed. A first list was drawn from bivariate analyses and reported only variables that were significantly associated (P<.05) with burnout. The consideration of even weak associations was hampered by the often incomplete presentation of these analyses. A second list came from multivariable analyses and included all the variables considered in the final (or presented) models regardless of whether physical activity was included in the model itself.
Synthesis of Evidence
The data are presented in a tabular form.
A narrative approach was adopted to provide an overall summary of the findings of the included studies and their biases, strengths, and limitations, with an in-depth discussion of the causes of heterogeneity.
Quality
The quality of the studies included in the analysis was assessed using the Joanna Briggs Institute Critical Appraisal Checklist for Cross-Sectional Studies [45]. This checklist consists of 8 items that are rated as “yes,” “no,” “unclear,” or “not applicable.” To further refine our judgment, we added “partial” as a fifth option.
Owing to the eligibility criteria adopted, 2 issues were always rated positively: item 1 (“Were the criteria for inclusion in the sample clearly defined?”), as we only considered studies that clearly reported associations in health personnel directly involved in the provision of care services, and item 4 (“Were objective, standard criteria used for measurement of the condition?”), as we only included studies that used validated questionnaires for burnout.
Item 2 allowed us to register whether a complete description of the participants and setting was provided. We assigned a score of “partial” or “no” if some or all the information was missing.
To assess whether the outcomes were measured in a valid and reliable way (item 7), we verified that the burnout measurement tools were used consistently with the dictates expressed by their developers.
We evaluated the validity and reliability of the exposure measurement (item 3) by positively appraising the use of structured questionnaires (eg, the International Physical Activity Questionnaire–Short Form [IPAQ-SF]) or automatic measurement devices such as pedometers, whereas the use of ad hoc questions to register the frequency or intensity of physical activity was considered a partial achievement.
Concerning the confounding factors, we did not assess how they were considered (item 5) and addressed in the statistical analyses (item 6) in studies exploring multiple wide-scope associations with burnout. On the other hand, we applied these items in studies that focused on a specific exposure factor (either physical activity or another variable of interest). In such cases, the use of statistical modeling, such as multivariable regression analysis, was considered a partial achievement in the absence of an advisable dedicated discussion on confounding factors.
For the appropriateness of the statistical analysis (item 8), a partial quality level was assigned if multivariable regression analysis, though possible, was not conducted or when it was conducted without an adequate method of model selection. Moreover, we assigned a partial level of quality if it was not possible to clearly understand all the details of the analyses because of omissions or results not being clearly reported.
Each study was evaluated for quality by 2 authors, and AB, a statistician, also reviewed items pertaining to statistics.
Discrepancies were resolved through plenary discussion among all authors until a consensus was reached. The quality assessment was not taken into account for eligibility purposes.
Results
Selected Studies
A total of 8937 records were identified, and after removing 2422 (27.1%) duplicates (Figure 1), 6515 (72.9%) publications remained following the initial screening. Of these 6515 publications, 6427 (98.65%) were excluded based on the title and abstract. These records were disregarded as they did not address physical activity, burnout, or health care personnel or because they were conference proceedings, reviews, or nonoriginal research (eg, letters or commentaries). Of the 88 studies selected for potential inclusion, 3 (3%) were not retrieved as they were published in journals not accessible through our organizations even after writing to the authors to request the accepted versions of their manuscripts [46-48]. Following full-text screening, 75% (64/85) of the records were excluded. Consequently, 21 independent studies involving 15,782 HCWs were included in this review (see Table 1 for details).
Figure 1.
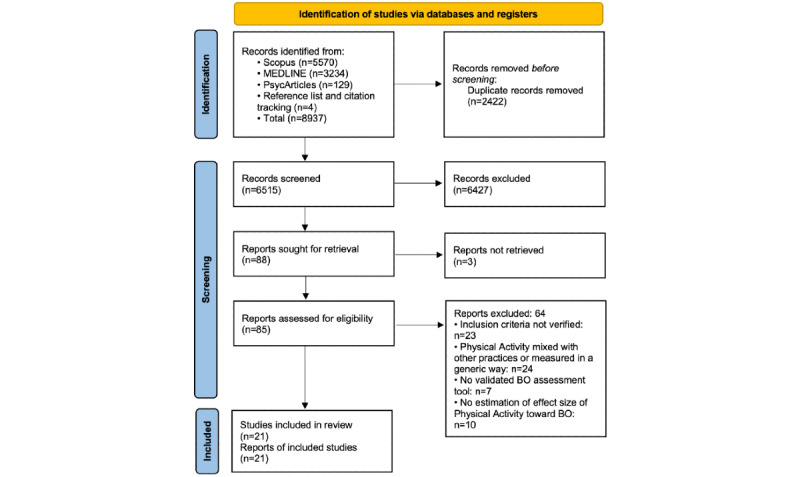
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 flow diagram. BO: burnout.
Table 1.
Characteristics of the included studies.
| Study, year | Aim | Country | Period of the survey | Type of HCWa | Sample size, N | Sex (female participants), % | Age (y) |
| Ajab et al [49], 2021 | To understand the availability of personal protective equipment and the levels of anxiety, depression, and burnout of HCWs | Asia; United Arab Emirates | From July 2020 to August 2020 | Physicians, nurses, allied health care professionals, and laboratory technicians; not specified occupation | 1290 | 78 | Mean 38.7 (SD 8.73)b |
| Alvares et al [50], 2020 | To assess the prevalence of and factors associated with burnout syndrome | America; Brazil | From November 2011 to June 2013 | Nurses and physicians in the ICUc | 125 nurses and 116 physicians | Nurses: 87.2d; physicians: 59.5d | Nurses: mean 36.5 (SD 8.2); physicians: mean 38.5 (SD 8.3) |
| Bin Dahmash et al [51], 2020 | To explore the prevalence of burnout and its predictors in radiology residents to minimize burnout rates and improve radiology residents’ well-being | Asia; Saudi Arabia | February 2019 | Radiology residents | 108 | 46.3 | Mean 27.2 (SD 1.83)b |
| Chokri et al [52], 2021 | To determine the prevalence of burnout among health care professionals and investigate the relationship between burnout and sociodemographic characteristics, working systems, and the level of physical activity in health care professionals | Africa; Morocco | February 2021 | Nurses, physicians, and health technicians | 145 | 70 | Mean 38.3 (SD 9.44)b |
| Portero de la Cruz et al [53], 2020 | To estimate the burnout, perceived stress, job satisfaction, coping, and general health levels experienced by nurses working in Spanish emergency departments and analyze the relationship between the sociodemographic, occupational, and psychological variables and the occurrence of burnout syndrome among these professionals | Europe; Spain | From March 2016 to December 2016 | Nurses | 171 | 73.1 | Mean 47.85 (SD 8.11) |
| Eckstein et al [54], 2022 | To examine how burnout is related to mindfulness, fulfillment, specialty choice, and other lifestyle factors | America; United States | From December 2019 to February 2020 | Physicians from different specialties (residents and attending physicians at an academic institution) | 60 | —e | Median 31 (range 25-70) |
| Feng et al [55], 2018 | To determine the prevalence of burnout among ophthalmology residents through a national survey and associate burnout with demographic factors, year in training, practice setting, self-reported workload physical activity, and sleep; in addition, this survey sought to solicit comments from ophthalmology residents regarding factors that they personally felt positively and negatively affected wellness and quality of life | America; United States | From January 17, 2017, to March 18, 2017 | Ophthalmology residents from PGY-2f to PGY-4g | 267 | 46.1 | Mean 29.7 (SD 2.3) |
| Ghoraishian et al [56], 2022 | To evaluate the frequency and factors associated with occupational burnout in orthopedic specialists and residents | Asia; Iran | 2019 | Orthopedic surgeons and residents | 180 | 5.6 | Mean 42.8 (SD 11.17) |
| Goldberg et al [57], 1996 | To measure the degree of burnout among emergency physicians and identify and rank predictive factors | America; United States | During the ACEPh Annual Scientific Assembly years 1992-1995 | Emergency physicians | 1272 | 25.7 | Mean 39 |
| Hu et al [58], 2021 | To investigate the severity of burnout and its associated factors among physicians and nurses in ICUs | Asia; China | From July 25, 2019, to July 30, 2019 | Physicians and nurses in ICUs | 2411 | 68.7 | Mean 33.5 (SD 5.95)b |
| Lebensohn et al [59], 2013 | To study the associations between commonly used indicators of well-being (perceived stress, depression, burnout, and satisfaction with life) and wellness behaviors at the start of family medicine residency | America; United States | At the beginning of PGY-1i in the graduating classes of 2012 and 2013 | PGY-1 family medicine (residents)b | 168 | 59.9 | Median 29 |
| McClafferty et al [60], 2021 | To document the concerning state of burnout in early pediatric trainees and examine the potential of the University of Arizona Center for Integrative Medicine PIMRj,k curriculum to provide interventions that address gaps in lifestyle behaviors with recognized association with burnout and how they might be introduced into residency training | America; United States | First trimester of residency in 4 consecutive years from 2012 to 2015 | First-year pediatric residents | 203 | 76 | Mean 28 |
| Ng et al [61], 2020 | To examine the prevalence and severity of burnout and explore the factors (sociodemographic, lifestyle behaviors, and career satisfaction) associated with burnout among medical graduates up to 20 y after graduation | Asia; Hong Kong | From January 29, 2016, to April 15, 2016 | Physicians entering medical school | 447 | 43.6 | Mean 34.1 (SD 6.0) |
| Olson et al [62], 2014 | To determine the association between achievement of national physical activity guidelines and burnout in internal medicine resident physicians | America; United States | From September 2012 to October 2012 | Internal medicine physicians (residents) | 76 | 47.3 | Mean 29.2 (SD 2.9) |
| Panse et al [63], 2020 | To assess burnout in plastic surgery residents | Asia; India | From March 2019 to April 2019 | Plastic surgery residents | 185 | 28.4 | — |
| Reed et al [64], 2020 | To explore the correlations between resident burnout and procedure volume, nonclinical responsibilities, and mindfulness practices along with gathering updated work hour data | America; United States | Not reported | Otolaryngology residents | 182 | — | — |
| Shanafelt et al [65], 2012 | To evaluate the health habits, routine medical care practices, and personal wellness strategies of American surgeons and explore associations with burnout and quality of life | America; United States | October 2010 | Surgeons | 7197 | 14.6 | Median 53 |
| Tiwari et al [66], 2020 | To investigate the prevalence of burnout among rheumatology practitioners and its associations | America; United Statesl | February 2019 | Rheumatology practitioners | 128 | 53.7 | Mean 49.9 (SD 12.0)b |
| Vinnikov et al [67], 2019 | To assess burnout prevalence in physicians and nurses of a cardiological hospital and ascertain whether smoking, alcohol, and physical activity may predict job-associated burnout | Asia; Kazakhstan | September 2018 | Cardiology personnel: physicians, nurses, and technical personnel | 259 | 82 | Median 34 |
| Vinnikov et al [68], 2021 | To verify the prevalence of occupational burnout in oncology physicians and nurses in a major cancer center and elucidate its predictors to plan future prevention activities | Asia; Kazakhstan | 2020 (before the breakout of COVID-19) | Oncology physicians and nurses | 256 | 62 | Median 37.5 |
| Yang et al [69], 2018 | To measure the prevalence of burnout and resilience levels in transplant nurses, identify any relationships between the 2 concepts, and determine whether demographic factors were associated with burnout in this group | Asia; China | From July 2015 to November 2015 | Transplant nurses | 536 | 96.3 | Mean 28.40 (SD 4.80) |
aHCW: health care worker.
bEstimated by the authors from grouped data.
cICU: intensive care unit.
dCalculated by the authors as, in the paper, the reported percentages were weighted for the unequal probabilities of participant selection.
eNot available.
fPGY-2: postgraduate at year 2.
gPGY-4: postgraduate at year 4.
hACEP: American College of Emergency Physicians.
iPGY-1: postgraduate at year 1.
jPIMR: Pediatric Integrated Medicine in Residency.
kThe 10-hour PIMR curriculum is designed in part to help pediatric programs meet new resident well-being requirements. The topics covered include self-nutrition and physical activity, mind-body therapies, dietary supplements, whole systems of medicine, and clinical applications.
lThe location of the conference where the survey was administered was considered to determine the country.
Although 10% (2/21) of the studies explicitly focused on exploring the association between physical activity and burnout [62,67], the remaining studies investigated the association among several factors, including physical activity. Most of the studies were conducted in America (10/21, 48%) and Asia (9/21, 43%), with only 10% (2/21) of the studies [49,52] being conducted after the spread of COVID-19. In total, 43% (9/21) of the studies [51,54-56,59,60,62-64] focused on residents. All the studies included in this review (21/21, 100%) had a cross-sectional design.
Demography of Study Populations
The study populations consisted of diverse groups of HCWs with varying proportions of women individuals, ranging from 5.6% to 96.3%. The professional categories represented included physicians, nurses, and technicians from different specialties, which were present in 90% (19/21), 38% (8/21), and 14% (3/21) of the studies, respectively. The sample sizes ranged from 60 to 7197 participants. The mean age varied from 27.2 (SD 1.83) years to 49.9 (SD 12.0) years, with a few studies (5/21, 24%) reporting the median ages, ranging from 29 to 53 years.
Measurement of Burnout
In terms of burnout measurement, the 22-item Maslach Burnout Inventory (MBI) was the most commonly used questionnaire. Some studies (3/21, 14%) used MBI-related measures based on fewer items [63-65]. In total, 10% (2/21) of the studies used different questionnaires: the Professional Fulfillment Index [54], which is designed to measure physician well-being [70], and the Copenhagen Burnout Inventory [61], which was proposed as an alternative tool to the MBI for measuring burnout [71] (see Multimedia Appendix 3 [49,51-53,55,56,58-63,66-69,72,73] for details).
The severity of the condition in the investigated population was reported in all the studies (21/21, 100%), albeit with differences in terms of the dimensions considered and the criteria used for deriving a summary assessment of burnout across the dimensions and, in some cases, by providing measures of location and scale parameters. Further details are provided in Table 2.
Table 2.
Burnout levels in the study populationsa.
| Study, year | Measure of burnout (MBIb) | Frequency distribution | Location and scale parameters | ||||||||
|
|
|
EEc | DPd | PAe | Criteria for burnout | Burnout | EE | DP | PA | Burnout | |
| Chokri et al [52], 2021 | MBI; normative data | 65%f, 15%, and 21% | 48%, 28%, and 23% | 32%, 25%, and 38% | 4 classes—high: EE+g, DP+, and PA−; moderate: 2 dimensions criticalh; low: 1 dimension critical; absent: no critical dimension | 11%, 41%, 32%, and 17% | Mean 31.03 (SD 15.5)i | Mean 9.8 (SD 6.0)i | Mean 34.3 (SD 8.0)i | N/Aj | |
| Portero de la Cruz et al [53], 2020 | MBI; normative data | 21%, 19%, and 60% | 43%, 28%, and 29% | 53%, 20%, and 26% | 3 classes—high: EE+, high DP+, and PA−; moderate: if not high and not absent; absent: EE−, DP−, and PA+ | 8%, 74%, and 18% | Mean 19.15 (SD 12.05)i | Mean 9.82 (SD 6.70)i | Mean 37.29 (SD 8.92)i | N/A | |
| Tiwari et al [66], 2020 | MBI; normative data | 38%, NRk, and NR | 31%, NR, and NR | NR, NR, and 21% | Binary classification: positive if EE+ or DP+ and PA− | 51% | NR | NR | NR | N/A | |
| Yang et al [69], 2018 | MBI; normative data | 37%, NR, and NR | 31%, NR, and NR | NR, NR, and 8% | Burnout score defined as the sum of the scores in the 3 dimensionsl | No threshold defined | Mean 24.38 (SD 9.38) | Mean 7.83 (SD 6.46) | Mean 29.38 (SD 8.53) | Mean 61.59 (SD 17.72) | |
| Lebensohn et al [59], 2013 | MBI; normative data | 14%, 28%, and 58% | 24%, 26%, and 51% | Not considered | 3 classes—high: EE+ and DP+; moderate: if not high and not low; low: EE− and DP− | 9%, 51%, and 41% | Mean 17.1 (SD 9.5) | Mean 6.38 (SD 4.7) | N/A | N/A | |
| McClafferty et al [60], 2021 | MBI; normative data | 20%, 25%, and 55% | 32%, 27%, and 42% | NR | 3 classes—high: EE+ and DP+; moderate: if not high and not low; low: EE− and DP− | 15%, 50%, and 35% | Mean 18.1 (SD 9.0) | Mean 7.4 (SD 4.9) | Mean 29.5 (SD 6.3) | N/A | |
| Olson et al [62], 2014 | MBI; normative data | NR, NR, and NR | NR, NR, and NR | Not considered | Binary classification: high if EE+ and DP+ | 54% | NR | NR | NR | N/A | |
| Bin Dahmash et al [51], 2020 | MBI; scoring key | 57%, NR, and NR | 32%, NR, and NR | NR, NR, and 65% | Binary classification: high if EE+ or DP+ and PA− | 24% | Mean 29.0 (SD 11.0) | Mean 9.60 (SD 6.08) | Mean 27.3 (SD 8.55) | N/A | |
| Feng et al [55], 2018 | MBI; scoring key | 55%i, 29%i, and 17%i | 46%i, 25%i, and 28%i | 71%i, 18%i, and 12%i | Binary classification: high if EE+ or DP+ and PA− | 63% | NR | NR | NR | N/A | |
| Hu et al [58], 2021 | MBI; scoring key | Physicians: 61%, 33%, and 6%; nurses: 57%, 37%, and 7% | Physicians: 37%, 36%, and 27%; nurses: 31%, 37%, and 32% | Physicians: 64%, 16%, and 20%; nurses: 66%, 14%, and 20% | Binary classification: high if EE+ or DP+ and PA− | Physicians: 71%; nurses: 68% | NR | NR | NR | N/A | |
| Vinnikov et al [67], 2019 | MBI; scoring key | Physicians: 32%, 29%, and 39%; nurses: 26%, 27%, and 47% | Physicians: 52%, 40%, and 8%; nurses: 45%, 37%, and 18% | Physicians: 16%, 16%, and 69%; nurses: 32%, 22%, and 46% | Not considered | N/A | Physicians: median 19 (IQR 15.8); nurses: median 18 (IQR 17) | Physicians: mean 14.1 (SD 6.4); nurses: median 12 (IQR 9) | Physicians: median 41 (IQR 9); nurses: median 38 (IQR 17) | N/A | |
| Vinnikov et al [68], 2021 | MBI; scoring key | Reported data were not consistent with the reported categorization | Reported data were not consistent with the reported categorization | Reported data were not consistent with the reported categorization | Not considered | N/A | Median 26 (IQR 19) | Median 15 (IQR 10) | Median 29 (IQR 15.8) | N/A | |
| Ajab et al [49], 2021 | MBI; Ajab et al [49] | 13%, 40%, and 47% | 4%, 23%, and 73% | 70%, 29%, and 1% | Not considered | N/A | NR | NR | NR | N/A | |
| Ghoraishian et al [56], 2022 | MBI; Ghoraishian et al [56] | 27%, 29%, and 43% | 16%, 19%, and 65% | 40%, 23%, and 37% | 4 classes—severe: EE+, DP+, and PA−; moderate: 2 dimensions critical; mild: 1 dimension critical; absent: no critical dimension | 7%, 16%, 27%, and 50% | NR | NR | NR | N/A | |
| Panse et al [63], 2020 | 9-item MBI (aMBIm) [74] | Moderate to severe: 64%; no to low: 36.2% | Moderate to severe: 26%; no to low: 74.1% | Moderate to severe: 91%; no to low: 9% | Burnout score defined as the sum of the scores in EE and DP and classified as binary (cutoff of ≥19; no reference provided for the validation of this cutoff) | 49% | NR | NR | NR | NR | |
| Goldberg et al [57], 1996 | MBI | Not considered | Not considered | Not considered | Binary classification: moderate to high levels of burnout according to the Golembiewski classificationn | 61% | Mean 23.31 (SD 8.55) | Mean 20.70 (SD 8.49) | Mean 24.72 (SD 9.17) | NR | |
| Alvares et al [50], 2020 | MBI | Physicians: 27%, NR, and NR; nurses: 31%, NR, and NR | Physicians: 7%, NR, and NR; nurses: 6%, NR, and NR | Physicians: NR, NR, and 9%; nurses: NR, NR, and 12% | Two binary classifications: (1) critical values in all the dimensions and (2) critical values in at least one dimension | Physicians: (1) 1% and (2) 34%; nurses: (1) 0% and (2) 39% | NR | NR | NR | N/A | |
| Shanafelt et al [65], 2012 | 2 single-item measures adapted from the MBI [75]o | EE reported at least weekly: 23% | DP reported at least weekly: 15% | N/A | Binary classificationi: high if EE+ or DP+ | 27% | N/A | N/A | N/A | N/A | |
| Reed et al [64], 2020 | 1 single question [76]p | N/A | N/A | N/A | N/A | 50% | N/A | N/A | N/A | N/A | |
aFrequency distribution from high to low. Independent of the way the authors reported the frequency distribution for PA, in accordance with Maslach et al [72], we considered low PA as a condition characterizing burnout. The numbers in the frequency distribution are rounded to percentage units.
bMBI: Maslach Burnout Inventory. In total, 3 categories were defined: emotional exhaustion, depersonalization, and PA. Most recent edition: Maslach et al [77].
cEE: emotional exhaustion.
dDP: depersonalization.
ePA: personal accomplishment.
fItalics indicate critical values for burnout.
gThe burnout dimension is in the high range (+) or low range (−).
hWhen referring to MBI and not otherwise specified, critical levels in burnout dimensions mean high in EE and DP and low in PA.
iAuthors’ interpretation.
jN/A: not applicable.
kNR: not reported.
lThe proposed burnout score does not consider that PA should be interpreted in the opposite direction from EE and DP as a low degree of burnout is reflected in high scores on PA [72].
maMBI: abbreviated Maslach Burnout Inventory.
nRaw data from the MBI used to divide the burnout process into 8 phases, with phases I-III representing a low degree and phases IV-V and VI-VIII representing moderate and high degrees, respectively [78].
oMBI adapted.
pMiniZ (adapted).
In two studies, authors adopted tools not referable to BMI. Ng et al [61] adopted the Copenhagen Burnout Inventory [71], which comprises 3 categories: personal, physical, and psychological exhaustion, work-related physical and psychological exhaustion, and patient-related physical and psychological exhaustion. The reported frequency distribution among study participants is 63%, 56%, and 35% respectively. No specific criteria were defined for burnout.
Eckstein et al [54] used the Professional Fulfillment Index [70], which consists of three response categories: Professional Fulfillment (PF), Interpersonal Disengagement, and Work Exhaustion (WE), employing 5-point Likert scales (“not at all true” to “completely true” for PF items and “not at all” to “extremely” for WE and Interpersonal Disengagement items). All responses are scored from 0 to 4. However, in the considered study, the PF domain was not taken into account. A binary classification (presence vs absence of burnout) is adopted according to the following criterion: the average score of Interpersonal Disengagement and WE ≥1.33 [70]. Participants meeting this criterion for burnout comprise 38%. Regarding Location and scale parameters, the median score for WE, Interpersonal Disengagement, and burnout is respectively 1.50, 0.83, and 1.00.
With due caution regarding the aforementioned heterogeneity of definitions and cutoffs, the percentage of participants classified as burned out varied from 7% to 83%.
Measurement of Physical Activity
None of the included studies used objective measurement tools, such as pedometers, to assess physical activity (Table 3).
Table 3.
Level of physical activity in the study populations.
| Study, year | Method used to measure physical activity | Percentage of HCWsa practicing physical activity | |
|
|
|
Criterion for prevalence | Prevalence, % |
| Olson et al [62], 2014 | IPAQ-SFb [79] | Compliance with the DHHSc benchmark: ≥150 min/wk [80] | 59 |
| Chokri et al [52], 2021 | Ricci-Gagnon scale [81] | Not inactive | 77 |
| McClafferty et al [60], 2021 | Arizona Lifestyle Inventory [82] | ≥1 d/wk for ≥30 min/session of moderate physical activity | 85 |
| Portero de la Cruz et al [53], 2020 | Question assessing a benchmark achievement | 7 d/wk | 49 |
| Ng et al [61], 2020 | Question assessing a benchmark achievement | Performing regular exercise: ≥5 d/wk for ≥10 min/session of any vigorous or moderate physical activities | 76 |
| Vinnikov et al [67], 2019 | Question assessing a benchmark achievement | Performing regular exercise: ≥3 d/wk for ≥40 min/session of any off-work physical activity | 34 |
| Vinnikov et al [68], 2021 | Question assessing a benchmark achievement | Performing regular exercise: ≥3 d/wk of any physical activity | 19 |
| Alvares et al [50], 2020 | Question assessing a benchmark achievement | Performing regular exercise: ≥3 d/wk of any physical activity | Nurses: 16d; physicians: 51.7d |
| Yang et al [69], 2018 | Question assessing a benchmark achievement | ≥1 d/wk | 46 |
| Panse et al [63], 2020 | Question assessing a benchmark achievement | ≥1 d for 2 wk | 35 |
| Shanafelt et al [65], 2012 | Frequency and intensity | >30 min/wk (moderately intense aerobic exercise) | ≥75 |
| Shanafelt et al [65], 2012 | Frequency and intensity | >30 min/wk (vigorously intense aerobic exercise) | 55 |
| Shanafelt et al [65], 2012 | Frequency and intensity | Compliance with the CDCe recommendation for aerobic exercise and muscle strength training [83] | 37 |
| Goldberg et al [57], 1996 | Frequency and time | ≥1 d/wk, ≥10 min/session | ≥78f; ≥79f |
| Feng et al [55], 2018 | Frequency | Compliance with the DHHS benchmark: ≥150 min/wk [80] | 35.2 |
| Ajab et al [49], 2021 | Frequency | ≥1 d/wk | 61 |
| Bin Dahmash et al [51], 2020 | Frequency | ≥1 d/wk | 44 |
| Eckstein et al [54], 2022 | Frequency | ≥1 d/wk | ≥78f |
| Hu et al [58], 2021 | Frequency | ≥1 d/wk | 56 |
| Lebensohn et al [59], 2013 | Frequency | ≥1 d/wk | 79 |
| Tiwari et al [66], 2020 | Frequency | ≥1 d/wk | 87 |
| Ghoraishian et al [56], 2022 | Frequency | A clear cutoff was not indicated | N/Ag |
| Reed et al [64], 2020 | Time | A clear cutoff was not indicated | N/A |
aHCW: health care worker.
bIPAQ-SF: International Physical Activity Questionnaire–Short Form.
cDHHS: US Department of Health and Human Services.
dCalculated by the authors as the percentages reported in the paper were weighted for the unequal probabilities of participant selection.
eCDC: Centers for Disease Control and Prevention.
fAuthors’ interpretation.
gN/A: not applicable.
Structured questionnaires that distinguished among different typologies of physical activity or ad hoc items were considered to investigate the habits of HCWs. The IPAQ-SF, the Ricci-Gagnon scale, and the Arizona Lifestyle Inventory were used in the studies by Olson et al [62], Chokri et al [52], and McClafferty et al [60], respectively. The IPAQ-SF was the only validated tool used, although it tends to overestimate actual physical activity levels [84]. A total of 33% (7/21) of the studies [50,53,61,63,67-69] used an ad hoc question to assess the achievement of a given benchmark, with a threshold frequency ranging from 1 day every 2 weeks [63] to every day [53]. In the remaining studies, physical exercise was measured in terms of frequency and intensity [65], frequency and time [57], only frequency [49,51,54-56,58,59,66], or only time [64]. When it was possible to report a distribution of frequencies or times, we considered the lowest category that did not indicate “no physical activity at all.” Whenever possible, we adopted the most widely used benchmark of physical exercise of “at least 1 day per week” to define physically active participants. Using this criterion, we found that the percentage of active workers ranged from 44% to 82% for residents and from 46% to 87% for the other categories.
Methods of Association Assessment
Bivariate associations between physical activity and burnout were assessed using usual methods. Table 4 provides further details. All studies except those by Olson et al [62], Vinnikov et al [67], Ghoraishian et al [56], Feng et al [55], and Tiwari et al [66] also conducted a multivariable regression analysis. In all 5 cases, a multivariable analysis could have been conducted to obtain adjusted odds ratios. Logistic and linear regression were equally used in 43% (9/21) and 33% (7/21) of the studies, respectively.
Table 4.
Association between physical activity and burnout.
| Study, year | Data analysis method | Bivariate analysis | Multivariable regression analysis |
| Ajab et al [49], 2021 | Bivariate analysis and multivariable linear regression | Low levels of EEa and DPb were significantly more frequent among HCWsc who performed physical activity almost every day than among HCWs who were not physically active the previous week (P<.001). High levels of personal accomplishment were significantly more frequent among HCWs who performed physical activity almost every day or every day than among HCWs not physically active the previous week (P<.001) | Not clearly reported and not coherent with the statistical methods declared |
| Alvares et al [50], 2020 | Chi-square and Fisher exact tests and multivariable logistic regression | Nurses: participants who did not exercise >3 d/wkd were at higher risk of high levelse of EE (ORf 7.36, 95% CI 1.14-47.32) and at lower risk of high levelse of DP (OR 0.05, 95% CI 0.004-0.61); physicians: crude ORs were not significant | Nurses: adjusted for other covariates, participants who did not exercise >3 d/wkd were at higher risk of high levels of EE (OR 11.01, 95% CI 2.73-44.39) and at lower risk of high levels of DP (OR 0.07, 95% CI 0.007-0.79) |
| Bin Dahmash et al [51], 2020 | Univariable and multivariable logistic regression | Participants who exercised ≥1 d/wk were significantly less at risk of having high DP (OR 0.33, 95% CI 0.13-0.78), low personal accomplishment (OR 0.43, 95% CI 0.19-0.97), or high burnout (OR 0.29, 95% CI 0.10-0.77; P=.01) than those who never exercised | Participants who exercised ≥1 d/wk were significantly less at risk of having high DP (aORg 0.38, 95% CI 0.15-1; P=.04) than those who never exercised |
| Chokri et al [52], 2021 | Chi-square test and multivariable linear regression | Degree of physical activity was not significantly associated with degree of EE (P=.86); it was weakly associated with DP and personal accomplishment (P=.09 and P=.08, respectively) | Physical activity not included in the model |
| Portero de la Cruz et al [53], 2020 | Bivariate analysis and univariable and multivariable linear regression | Those who did not take part in daily physical exercise had higher mean DP (P=.005) scores. There were no statistically significant differences in mean EE (P=.09) and mean personal accomplishment (P=.48) according to daily physical exercise | Adjusted for other covariates, the lack of daily physical activity was a significant predictor of higher DP values |
| Eckstein et al [54], 2022 | Univariable and multivariable logistic regression | Frequency of exercise not significantly associated with burnout | Physical activity not included in the model |
| Feng et al [55], 2018 | Bivariate analyses | The probability of low EE was significantly higher in participants who engaged in physical activity ≥150 min/wk (P=.02). No association was found with levels of DP (P=.32), personal accomplishment (P=.29), and burnout (P=.13) | NPh |
| Ghoraishian et al [56], 2022 | Chi-square test and univariable logistic regression | Participants who exercised ≤1 h/wk were at higher risk of burnout than those who exercised >1 h/wk (OR 2.3, 95% CI 1.24-4.48) | NP |
| Goldberg et al [57], 1996 | Chi-square test and multivariable logistic regression | Results of association analysis were inconsistent with the data. | Low levels of exercise were significantly associated with burnout |
| Hu et al [58], 2021 | Chi-square test and multivariable logistic regression | Not reported in the paper | Participants who exercised ≥1 d/wk were significantly at lower risk of burnout (once a week: OR 0.66, 95% CI 0.45-0.95; every 2 or 3 d: OR 0.56, 95% CI 0.39-0.80; every day: OR 0.52, 95% CI 0.36-0.75) than those who exercised less frequently or never |
| Lebensohn et al [59], 2013 | ANOVA and multivariable linear regression | Physical activity was not significantly associated with burnout | More frequent physical activity was a significant adjusted predictor of lower values of both EE and DP |
| McClafferty et al [60], 2021 | ANOVA and multivariable linear regression | Among individuals at high risk of burnout, the frequency of physical activity was lower than the group mean, whereas among individuals at low or moderate risk, the frequency was higher (P=.10) | Adjusted for other covariates, a higher frequency of exercise was a significant predictor of a higher score on personal accomplishment |
| Ng et al [61], 2020 | Univariable and multivariable linear regression | Practicing regular exercise significantly reduced CBIi-PeEj (slope: −9.882; P<.001) and CBI-PaEk (slope: −6.932; P=.004). It was not correlated with CBI-WrEl | Practicing regular exercise was a significant adjusted predictor of lower values of CBI-PeE and CBI-PaE |
| Olson et al [62], 2014 | Chi-square test and univariable logistic regression | Participants compliant with DHHSm guidelines were significantly less at risk of having high subscores in burnout (OR 0.38, 95% CI 0.147-0.99) than noncompliant HCWs | NP |
| Panse et al [63], 2020 | Univariable and multivariable logistic regression | Participants who performed any physical activity for fitness at least once in 2 weeks were significantly less at risk of high values of burnout (OR 0.41, 95% CI 0.22-0.77) than those who did not perform physical activity | Physical activity was not significantly associated with burnout |
| Reed et al [64], 2020 | Chi-square test, ANOVA, and multivariable logistic regression | Results of association analysis were inconsistent with the data | Physical activity was not significantly associated with burnout |
| Shanafelt et al [65], 2012 | Multivariable logistic regression | NP | Compliance with CDCn aerobic exercise and muscle strength training recommendations was not independently associated with burnout |
| Tiwari et al [66], 2020 | Univariable logistic regression | Participants who lacked exercise at least 1 d/wk were at higher risk of burnouto (OR 5.00, 95% CI 1.3-18.5) than participants who exercised | NP |
| Vinnikov et al [67], 2019 | Bivariate analysis | Physical activity was not significantly associated with any MBIp dimension | NP |
| Vinnikov et al [68], 2021 | Bivariate analysis and multivariable logistic regression | Participants who did not regularly exercise were at higher risk of high EE (OR 5.02d, 95% CI 2.25-12.42) and high DP (OR 2.37d, 95% CI 1.20-4.74) than those who regularly exercised | Participants who did not regularly exercise ≥3 d/wk were significantly more at risk of having high EE (aOR 9.91, 95% CI 2.92-27.2) than the other participants |
| Yang et al [69], 2018 | Multivariable linear regression | NP | Adjusted for other covariates, exercising every week was a significant predictor of lower values of EE and burnoutq. It was also a significant predictor of lower values of personal accomplishment |
aEE: emotional exhaustion.
bDP: depersonalization.
cHCW: health care worker.
dDerived by the authors.
eParticipants with moderate burnout in the dimension were excluded from the analysis.
fOR: odds ratio.
gaOR: adjusted OR.
hNP: not performed.
iCBI: Copenhagen Burnout Inventory. In total, 3 categories were defined: personal physical and psychological exhaustion, work-related physical and psychological exhaustion, and patient-related physical and psychological exhaustion.
jPeE: personal physical and psychological exhaustion.
kPaE: patient-related physical and psychological exhaustion.
lWrE: work-related physical and psychological exhaustion.
mDHHS: US Department of Health and Human Services. Its guidelines [80] set a benchmark of 150 minutes per week of physical activity.
nCDC: Centers for Disease Control and Prevention. It set recommendations for aerobic exercise and muscle strength training [83].
oThe definition of burnout adopted in the logistic regression was not clear.
pMBI: Maslach Burnout Inventory.
qThe result was reported for completeness even though we believe that the burnout score was meaningless as it did not consider that personal accomplishment should be interpreted in the opposite direction from EE and DP.
Existence and Degree of Association
Table 4 also presents the evidence of the association between physical activity and burnout. Owing to the high heterogeneity of the studies, a direct comparison of the results was not feasible. As previously mentioned, the 2 sources of heterogeneity were the diverse and sometimes vague definitions of physical activity used in the studies and the variations in the definitions and cutoffs for measuring burnout.
A total of 14% (3/21) of the studies [49,57,64] reported a few results that were not consistent with the data, and in one case [58], the authors referred to supplementary material that was not available on the journal web page. In total, 80% (4/5) [55,56,62,66] of the studies that presented only bivariate analyses indicated that a lack of physical activity was associated with high values of at least one component of the MBI. Similar results were reported by half (8/16, 50%) of the other studies that presented bivariate analyses regardless of the measure of burnout adopted.
In studies in which bivariate analysis was preparatory to multivariable regression analysis [50-54,58,61,63,68], physical activity may not have emerged as a predictor in the multivariable models [51,52,54,63,68]. This is sometimes due to the lack of a significant (albeit weak) association already in the bivariate analyses [52,54]. However, this result is also influenced by the different approaches to variable inclusion and selection. When conducting a bivariate analysis as a preliminary step for variable selection in the multivariable model, a less stringent significance criterion than P<.05 should be considered. Variables that show weak individual associations can become important predictors when considered jointly (eg, the study by Hosmer and Lemeshow [85]). Unfortunately, the selected studies used very different criteria, ranging from P<.05 for each variable to no preselection at all. In addition, methods for model selection were not always applied or clearly stated.
In cases in which physical activity was found to be a significant predictor in multivariate analyses, a protective effect was observed, especially against emotional exhaustion [50,59,61,68,69] and depersonalization [50,51,53,59]. This held true across a range of activity frequencies, from as little as 1 session per week to daily engagement.
For the sake of completeness, factors other than physical activity that showed a statistically significant association with burnout have been listed in 2 separate tables: one for bivariate analyses and the other for multivariable analysis (Tables S1 and S2 in Multimedia Appendix 4). The predictors were grouped by topic (demography, health conditions, lifestyle, personal attitude, work-life balance, work organization and environment, work profile, and self-perception at work) and ordered within each class according to their frequency.
Quality Evaluation
The risk of bias was assessed using the Joanna Briggs Institute tool, and the details are presented in Multimedia Appendix 5 [45,49-69].
All the studies provided detailed descriptions of participants and settings, with the exception of the studies by Eckstein et al [54], in which gender specifications were missing, and Reed et al [64], in which the period of the survey, gender mix, and age were not reported.
Regarding the assessment of physical activity, only a minority of studies (3/21, 14%) [52,60,62] adopted structured questionnaires and, therefore, received a positive evaluation. Most studies (18/21, 86%) only partially fulfilled this criterion, either relying on simple ad hoc questions to assess the activity frequency, time, or intensity or referring to meeting a threshold of activity. This limitation was observed even in studies that claimed to have a specific focus on physical activity [55,67].
Confounding was never explicitly addressed. As mentioned in the Methods section, we applied the dedicated items to the 14% (3/21) of studies that focused on a specific exposure [62,67,69]. All these papers touched on this issue through their conducted analyses and, therefore, obtained a “partial” rating for item 5. Of these studies, 33% (1/3) conducted only a bivariate analysis and, thus, did not comply with item 6 [62].
As for the use of the MBI, only a few studies (9/21, 43%) received a positive evaluation for item 7. Contrary to the explicit indications of the MBI developers [86], the authors of most studies (11/21, 52%) [50,51,55-58,62,63,66-68] adopted a categorical classification of participants based on burnout dimensions for descriptive as well as inferential purposes. Moreover, Yang et al [69], although correctly adopting the score to assess each MBI dimension, defined and adopted an overall burnout score as the raw sum of the scores in each dimension (as reported in Table 4, even without considering that personal accomplishment should be interpreted in the opposite direction from emotional exhaustion and depersonalization). In all these cases except the studies by Ghoraishian et al [56] and Panse et al [63], we assigned a partial achievement of the item. Indeed, these 2 studies were ranked with a “no” as they did not even provide the rationale behind their choice of ranges of scores in each dimension. Except for 14% (3/21) of the studies—Ajab et al [49] and Vinnikov et al [67,68]—all the other studies referring to the MBI or related multi-item measures introduced a definition of overall burnout. Despite this, studies that also adopted the total score of the burnout dimensions in their inferential analyses [52,53,59,60] were ranked with a “yes.” Ng et al [61] and Eckstein et al [54] were classified as “yes” as they correctly adopted the measurement tools—Copenhagen Burnout Inventory [73] and Professional Fulfillment Index [54], respectively.
Regarding item 8, statistical analysis was not considered appropriate in 10% (2/21) of the studies [50,58], in which the significant differences between physicians and nurses in the dimensions of the MBI were not adequately handled in the multivariable analysis. The analyses conducted in another 14% (3/21) of the studies [49,56,64] were rated as unclear either because the presented results were not coherent with the declared statistical methods [64] or because of unexplained methods [49,56]. Goldberg et al [57], Bin Dahmash et al [51], Shanafelt et al [65], Vinnikov et al [68], Portero de la Cruz et al [53], and Chokri et al [52] clearly explained their statistical methods and conducted comprehensive analyses, receiving a positive quality assessment. In the other cases, a better statistical methodology could have been applied by conducting a multivariable analysis, considering more suitable criteria to include the explanatory factors in the multivariable analysis, or again by applying model selection methods to obtain more parsimonious and general models.
Discussion
Principal Findings
The COVID-19 pandemic has taken a heavy toll on HCWs in terms of physical and mental health, and the long-term effects of the pandemic will further increase the burden of HCWs’ mental health disorders and burnout [87,88]. It has been argued that addressing burnout could serve as a nonstigmatized and systemic approach to address a long-standing issue in medicine through mental health initiatives, whether prevention oriented or treatment focused [89].
In addition to the personal consequences for HCWs experiencing burnout, it is important to consider its impact on patient care and resource consumption. Emotionally and physically healthy HCWs are among the most relevant factors influencing health care service quality [90]. All these considerations emphasize the importance of implementing strategies to prevent and manage burnout at an individual, organizational, and cultural level. The literature on burnout management primarily presents fragmented solutions that are infrequently tested in practice. These solutions often align with 1 of 2 predominant lines of intervention: one emphasizes strengthening individual capabilities to navigate the inherent challenges of health care work, whereas the other acknowledges work organization as a contributing factor and attempts to intervene at that level. However, there is a growing realization that individual and organizational well-being are intricately interconnected, thus necessitating systemic solutions. These comprehensive approaches encompass organizational interventions, instilling a culture of well-being in the workplace, and integrating well-being into health care education for true efficacy [24,91]. A recent meta-analysis of 20 controlled trials found that the most effective existing interventions for reducing burnout were those targeting multiple facets of well-being [92]. Regrettably, these systemic solutions are complex and often come at a significant cost [93-95]; therefore, it is particularly relevant for research to precisely identify the characteristics that specific interventions must have to succeed. This review focused on physical activity as an effective factor in fostering a culture of well-being among HCWs, which is crucial for tackling the physical and mental consequences of work-related stress [24]. Physical activity has enormous potential to mitigate the physical and mental impacts of work-related stress [96,97]. Indeed, it is suggested that it facilitates psychological detachment from work and enhance self-efficacy [53], providing an opportunity to divert attention from stressful thoughts [50]. It has also been shown that moderate-intensity exercise training programs improve feelings of vigor, energy, and vitality [98]. In particular, greater effects occurred when combining resistance exercise with aerobic exercise compared with aerobic exercise alone [98]. This finding is consistent with the World Health Organization recommendations for physical activity, which underlie the importance for adults of regularly performing both aerobic and muscle-strengthening activities to support health, including mental health outcomes [96]. With this review, we aimed to systematically assess the strength of the evidence and, eventually, the dose-response association between physical activity and burnout in a physically and emotionally exhausting work environment. However, it is essential to note that all studies included in our review had a cross-sectional design. As is well known, randomized controlled trials with a longitudinal perspective are the gold standard to highlight any potential cause-effect relationship between an exposure and an outcome. Nevertheless, the cross-sectional approach is useful in highlighting potential relationships between burnout and related factors, aiding in the identification of a multiplicity of risk factors and mitigation strategies, as the complexity of the phenomenon requires. This is particularly true in our case as most of the included studies (19/21, 90%) were exploratory investigations that examined various aspects potentially related to burnout rather than focusing specifically on physical activity. As shown in Tables S1 and S2 in Multimedia Appendix 4, a wide range of variables were considered in bivariate analyses (74 issues) and included in multivariable models (58 issues), reflecting the interplay between burnout and demographic characteristics, health, lifestyle, personal attitude, self-perception at work, work organization and environment, job profile, and work-life balance.
As mentioned previously, physical activity is considered a potential tool to cope with distress, and the PEO approach adopted in this study was specifically structured in this direction. However, it is important to recognize the possibility that high levels of burnout negatively influence the level of physical activity [99]. According to the study by Olson et al [62], the “lack of energy” among burned-out residents suggests that high levels of burnout lead HCWs to reduce the time dedicated to leisure activities, including physical exercise. Stults-Kolehmainen and Sinha [99] found a similar result in the literature, stating that stress hinders individuals from being more physically active and has a negative influence on other health behaviors, including smoking, alcohol, and drug use. We suggest that future studies include sections dedicated to exploring the reasons for individuals’ inability to meet their desired level of physical activity. Factors such as time constraints, lack of interest, or underlying health conditions should also be accounted for. The Barriers to Being Active Quiz developed by the US Centers for Disease Control and Prevention [100] is an example of a tool that may support the exploration of the dynamic interactions among personal, socioenvironmental, and behavioral factors, serving as a knowledge base for promoting more active and healthy lifestyles.
This study confirms that the dose-response relationship between physical activity and psychological well-being and health-related quality of life is far from being established. Significant mental health benefits could be achieved even at physical activity levels below the public health recommendations [101,102]. This also emerged from our study and has direct implications on healthy lifestyle recommendations, especially for inactive HCWs for whom incorporating brief bouts of physical activity into daily activities may be a more realistically achievable goal than meeting the guideline-recommended physical activity levels. This can be crucial to promote physical activity and, therefore, trigger a virtuous circle with benefits for burnout. In addition, it may have broader implications for the general population as there are indications that physicians’ involvement in physical activity is linked to their propensity to advise patients on the advantages of exercise [103,104]. Recognizing that any physical activity is better than none and considering engagement in physical activity as a modifiable behavior, adopting a strategy of gradually increasing activity through small habit changes is deemed effective for establishing a consistent exercise routine. This approach can be facilitated by the use of activity trackers [105,106].
This systematic review highlighted another general challenge in quantifying the strength of the physical activity–burnout association and establishing the dose-response curve, primarily as various methods were used to detect burnout. Different self-reporting tools are indeed available grounded on different theoretical bases [42]. Most of the studies in our review (19/21, 90%) proposed the 22-item MBI or MBI-related questionnaires (Table 2), confirming the substantial monopoly of this tool in burnout research. All these studies fell into some form of misuse of the index. The 3-factor structure of the MBI implies, on the one hand, that each dimension must be treated separately and, on the other hand, that none of them should be ignored. In contrast, in some studies where it would have made sense (3/17, 18%) [59,60,62], personal accomplishment was excluded from the analysis. This practice is not uncommon as several authors consider personal accomplishment not as a reaction to stressful situations but rather as a personality trait or coping resource and, therefore, as not contributing to the comprehensive concept of burnout [107]. Another misuse of the MBI is its diagnostic application, which erroneously considers the MBI dimensions as symptoms of burnout [71]. The 7-point scale (from Never to Every day) used to report the feelings experienced by the respondents was intended by Maslach and the coauthors of the tool as an operational simplification of the measurement of a dynamic phenomenon evolving continuously over time rather than as the assessment of a dichotomous condition (absent or present) defined through an arbitrary cutoff. Considering MBI scores for diagnostic purposes would inevitably invoke the wrong concept of burnout as a disease or disability, ignoring decades of research and the recent statement from the World Health Organization [1]. The MBI was not designed as a diagnostic tool [86], and the cutoff scores established to classify people at low, moderate, and high levels of burnout were “intended primarily as feedback for individual respondents.” These scores were published up to the third edition of the MBI Manual [72] accompanied, however, by a strong recommendation to use the original total scores for any statistical analysis. In the fourth edition released in 2018 [77], the categorization was finally removed. Therefore, it is surprising that, despite the extraordinary diffusion of the MBI, there was a failure to implement the correct instructions for its use. In fact, all studies except the one by Goldberg et al [57] considered some classification of the severity (sometimes referred to as risk) of burnout in each of the 3 MBI dimensions also for inferential purposes. Furthermore, a variety of classification criteria, even when taken from the same reference [72], and algorithms for combining dimensions into a single overall burnout indicator, typically a high score in at least one dimension and sometimes in all dimensions (reversing personal accomplishment, if considered), further increased the heterogeneity of the analyses. These methodological considerations become even more crucial in future research, particularly now that apps providing burnout self-diagnosis are available and transparency is needed in the adopted assessing algorithms [108].
Moving on to the evidence on the association between physical activity and burnout that emerged from this review, the most compelling results came from multivariable analyses that considered emotional exhaustion and depersonalization as the outcome. In these analyses, physical activity appeared to be associated with a reduction in critical conditions. However, it is still unclear whether this association depends on the type, intensity, duration, or frequency of physical activity, as previously mentioned. Some of the included studies (2/21, 10%) suggested that exercising for at least one day per week is sufficient to see a positive effect [58,69], whereas others (2/21, 10%) suggested a frequency of 3 days per week [50,68]. Lebensohn et al [59] observed that, the more frequently HCWs engaged in physical activity, the greater the positive effect.
It is worth noting that, in a few of the studies that considered a multivariable analysis (2/15, 13%), physical activity was not included among the predictors. However, this can sometimes be related to strict variable selection methods.
One limitation of most of the included studies (18/21, 86%) was related to the modality of physical activity measurement. Future studies should consider using objective measurement tools such as pedometers or validated questionnaires such as the International Physical Activity Questionnaire [79] even in its short version [84]. These approaches enhance the accuracy and reliability of data collection. On the other hand, relying on simple questions about regular physical activity or adherence to recommendations for a healthy lifestyle, although suitable for preliminary exploratory investigations, limits the comparability of studies.
The use of precise and detailed definitions to collect measures of intensity and frequency can prove to be a valuable strategy to delve deeper into the dose-response relationship.
Limitations
Our systematic review has some limitations that warrant consideration. First, our search was confined to 3 databases and only considered English-language articles. Moreover, we did not perform a rerun of the search shortly before submission. However, to mitigate the risk of overlooking relevant papers, we used forward and backward citation tracking, including the use of Google Scholar.
Another potential limitation arises from our eligibility criteria as we considered only HCWs in direct contact with patients and excluded practices with only a light component of physical exercise.
Finally, the heterogeneity in measurement methods and statistical analyses, which we have extensively covered in the Results section, made a meta-analysis inappropriate and precluded the determination of any pooled effect size.
Conclusions
Our comprehensive overview of studies exploring the association between physical activity and burnout in HCWs revealed a significant level of heterogeneity in definitions, measurements, and analyses adopted in the literature. Our work aimed to advance effective public health practices by addressing this critical issue in the existing evidence. It is important to adopt a clear definition of burnout and physical activity and make thoughtful choices regarding measurement tools and methodologies for data analysis. This becomes particularly crucial when considering that burnout is not a diagnosable disease but rather a multifaceted psychological syndrome that emerges in response to chronic interpersonal stressors in the workplace.
Our findings strongly emphasize the beneficial connection between physical activity and burnout when a statistically significant association is present in the analyses. However, they also highlight the importance of a more in-depth investigation of the specific dependencies on exercise type, intensity, duration, and frequency, knowledge that currently represents a research gap in the field of burnout studies. Moreover, our considerations regarding the measurement of burnout and the comprehensive list of associated factors have the potential to enhance the quality of future studies. Our findings have significant implications for policy makers and health care professionals, underlining the importance of promoting physical activity as an easily accessible mitigation strategy for the well-being of the workforce and the overall effectiveness of the health care system.
Acknowledgments
The authors would like to thank Roberto Guarino (National Research Council of Italy—Institute of Clinical Physiology, Lecce) for his technical support (informatics tools for document management and title and abstract screening). This study was conducted within the research agreement between the National Research Council of Italy—Institute of Clinical Physiology, National Research Council of Italy—Institute for Applied Mathematics and Information Technologies, “E. Magenes,” and National Research Council of Italy—Institute for Research on Population and Social Policies and the Brindisi Local Health Unit (CNR-IRPPS-547/2022; deliberazione ASL-BR-1027/2022). The agreement was executed for free.
Abbreviations
- HCW
health care worker
- IPAQ-SF
International Physical Activity Questionnaire–Short Form
- MBI
Maslach Burnout Inventory
- PEO
population, exposure, and outcome
- PF
Professional Fulfillment
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PRISMA-S
Preferred Reporting Items for Systematic Reviews and Meta-Analyses literature search extension
- WE
Work Exhaustion
Eligibility criteria.
Search strings.
Classification and interpretation of burnout scores.
Predictors adopted in bivariate analyses and in multivariable regression analyses (other than physical activity).
Quality assessment.
PRISMA checklist.
PRISMA-S Checklist.
Data Availability
All data generated or analyzed during this study are included in this published paper (and its supplementary information files).
Footnotes
Authors' Contributions: Conceptualization involved contributions from CGL and PM. Methodology development was the responsibility of AB, PM, and CGL. All the authors participated in conducting the literature search and extracting data. AB, CGL, and PM were involved in preparing the original draft of the manuscript. Reviewing and editing the manuscript was a collaborative effort among all the authors. Throughout the research process, supervision was provided by CGL and PM. All the authors have read and agreed to the published version of the manuscript.
Conflicts of Interest: None declared.
References
- 1.Burn-out an "occupational phenomenon": International Classification of Diseases. World Health Organization. 2019. [2024-02-20]. https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases .
- 2.Søvold LE, Naslund JA, Kousoulis AA, Saxena S, Qoronfleh MW, Grobler C, Münter L. Prioritizing the mental health and well-being of healthcare workers: an urgent global public health priority. Front Public Health. 2021;9:679397. doi: 10.3389/fpubh.2021.679397. https://europepmc.org/abstract/MED/34026720 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hodkinson A, Zhou A, Johnson J, Geraghty K, Riley R, Zhou A, Panagopoulou E, Chew-Graham CA, Peters D, Esmail A, Panagioti M. Associations of physician burnout with career engagement and quality of patient care: systematic review and meta-analysis. BMJ. 2022 Sep 14;378:e070442. doi: 10.1136/bmj-2022-070442. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=36104064 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Han S, Shanafelt TD, Sinsky CA, Awad KM, Dyrbye LN, Fiscus LC, Trockel M, Goh J. Estimating the attributable cost of physician burnout in the united states. Ann Intern Med. 2019 Jun 04;170(11):784–90. doi: 10.7326/M18-1422.2734784 [DOI] [PubMed] [Google Scholar]
- 5.Dewa CS, Jacobs P, Thanh NX, Loong D. An estimate of the cost of burnout on early retirement and reduction in clinical hours of practicing physicians in Canada. BMC Health Serv Res. 2014 Jun 13;14:254. doi: 10.1186/1472-6963-14-254. https://bmchealthservres.biomedcentral.com/articles/10.1186/1472-6963-14-254 .1472-6963-14-254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Leo CG, Sabina S, Tumolo MR, Bodini A, Ponzini G, Sabato E, Mincarone P. Burnout among healthcare workers in the COVID 19 era: a review of the existing literature. Front Public Health. 2021;9:750529. doi: 10.3389/fpubh.2021.750529. https://europepmc.org/abstract/MED/34778184 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shanafelt TD, West CP, Dyrbye LN, Trockel M, Tutty M, Wang H, Carlasare LE, Sinsky C. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clin Proc. 2022 Dec;97(12):2248–58. doi: 10.1016/j.mayocp.2022.09.002. https://linkinghub.elsevier.com/retrieve/pii/S0025-6196(22)00515-8 .S0025-6196(22)00515-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mollica RF, Fricchione GL. Mental and physical exhaustion of health-care practitioners. Lancet. 2021 Dec 18;398(10318):2243–4. doi: 10.1016/S0140-6736(21)02663-5. https://europepmc.org/abstract/MED/34922665 .S0140-6736(21)02663-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Poon YS, Lin YP, Griffiths P, Yong KK, Seah B, Liaw SY. A global overview of healthcare workers' turnover intention amid COVID-19 pandemic: a systematic review with future directions. Hum Resour Health. 2022 Sep 24;20(1):70. doi: 10.1186/s12960-022-00764-7. https://human-resources-health.biomedcentral.com/articles/10.1186/s12960-022-00764-7 .10.1186/s12960-022-00764-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rotenstein LS, Brown R, Sinsky C, Linzer M. The association of work overload with burnout and intent to leave the job across the healthcare workforce during COVID-19. J Gen Intern Med. 2023 Jun;38(8):1920–7. doi: 10.1007/s11606-023-08153-z. https://europepmc.org/abstract/MED/36959522 .10.1007/s11606-023-08153-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stephenson J. Study highlights effects of COVID-19 burnout on primary care physicians in 10 high-income countries. JAMA Health Forum. 2022 Nov 04;3(11):e225101. doi: 10.1001/jamahealthforum.2022.5101. https://jamanetwork.com/article.aspx?doi=10.1001/jamahealthforum.2022.5101 .2799069 [DOI] [PubMed] [Google Scholar]
- 12.Statement on the fifteenth meeting of the IHR (2005) emergency committee on the COVID-19 pandemic. World Health Organization. 2023. [2023-05-12]. https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the- international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic .
- 13.Ortega MV, Hidrue MK, Lehrhoff SR, Ellis DB, Sisodia RC, Curry WT, Del Carmen MG, Wasfy JH. Patterns in physician burnout in a stable-linked cohort. JAMA Netw Open. 2023 Oct 02;6(10):e2336745. doi: 10.1001/jamanetworkopen.2023.36745. https://europepmc.org/abstract/MED/37801314 .2810256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nigam JA, Barker RM, Cunningham TR, Swanson NG, Chosewood LC. Vital signs: health worker-perceived working conditions and symptoms of poor mental health - quality of worklife survey, united states, 2018-2022. MMWR Morb Mortal Wkly Rep. 2023 Nov 03;72(44):1197–205. doi: 10.15585/mmwr.mm7244e1. doi: 10.15585/mmwr.mm7244e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.López-Cabarcos MÁ, López-Carballeira A, Ferro-Soto C. The role of emotional exhaustion among public healthcare professionals. J Health Organ Manag. 2019 Sep 05;33(6):649–55. doi: 10.1108/JHOM-04-2019-0091. doi: 10.1108/JHOM-04-2019-0091. [DOI] [PubMed] [Google Scholar]
- 16.Montgomery A. The inevitability of physician burnout: implications for interventions. Burn Res. 2014 Jun;1(1):50–6. doi: 10.1016/j.burn.2014.04.002. doi: 10.1016/j.burn.2014.04.002. [DOI] [Google Scholar]
- 17.Barger LK, Weaver MD, Sullivan JP, Qadri S, Landrigan CP, Czeisler CA. Impact of work schedules of senior resident physicians on patient and resident physician safety: nationwide, prospective cohort study. BMJ Med. 2023;2(1):e000320. doi: 10.1136/bmjmed-2022-000320. https://europepmc.org/abstract/MED/37303489 .bmjmed-2022-000320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Strid EN, Wåhlin C, Ros A, Kvarnström S. Health care workers' experiences of workplace incidents that posed a risk of patient and worker injury: a critical incident technique analysis. BMC Health Serv Res. 2021 May 27;21(1):511. doi: 10.1186/s12913-021-06517-x. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-021-06517-x .10.1186/s12913-021-06517-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wang JF, Zeng QL, Wang YQ, Liao XQ, Xie CX, Wang GF, Zeng YL. Workplace violence and the risk of post-traumatic stress disorder and burnout among nurses: a systematic review and meta-analysis. J Nurs Manag. 2022 Oct;30(7):2854–68. doi: 10.1111/jonm.13809. [DOI] [PubMed] [Google Scholar]
- 20.Sahebi A, Golitaleb M, Moayedi S, Torres M, Sheikhbardsiri H. Prevalence of workplace violence against health care workers in hospital and pre-hospital settings: an umbrella review of meta-analyses. Front Public Health. 2022;10:895818. doi: 10.3389/fpubh.2022.895818. https://europepmc.org/abstract/MED/36003634 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018 Jun;283(6):516–29. doi: 10.1111/joim.12752. https://onlinelibrary.wiley.com/doi/10.1111/joim.12752 . [DOI] [PubMed] [Google Scholar]
- 22.Weaver MD, Vetter C, Rajaratnam SM, O'Brien CS, Qadri S, Benca RM, Rogers AE, Leary EB, Walsh JK, Czeisler CA, Barger LK. Sleep disorders, depression and anxiety are associated with adverse safety outcomes in healthcare workers: a prospective cohort study. J Sleep Res. 2018 Dec;27(6):e12722. doi: 10.1111/jsr.12722. https://europepmc.org/abstract/MED/30069960 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kuehn BM. Physicians are more burned out than ever-here's what can be done about it. JAMA. 2023 Mar 14;329(10):785–7. doi: 10.1001/jama.2023.1647.2802013 [DOI] [PubMed] [Google Scholar]
- 24.Stephenson J. National academy of medicine outlines plan to curb burnout, bolster health workforce well-being. JAMA Health Forum. 2022 Oct 07;3(10):e224549. doi: 10.1001/jamahealthforum.2022.4549. https://jamanetwork.com/article.aspx?doi=10.1001/jamahealthforum.2022.4549 .2797662 [DOI] [PubMed] [Google Scholar]
- 25.Grady C, Chênevert D, Coderre-Ball A. Exploring two psychosocial factors for health-care workers. Mental Health Commission of Canada. 2022. [2024-02-20]. https://mentalhealthcommission.ca/wp-content/uploads/2022/09/Psychosocial-factors-for-health-care-workers.pdf .
- 26.Mangurian C, Fitelson E, Devlin M, Pumar M, Epel E, Dahiya P, Mayer LE, Jackson-Triche M. Envisioning the future of well-being efforts for health care workers-successes and lessons learned from the COVID-19 pandemic. JAMA Psychiatry. 2023 Sep 01;80(9):962–7. doi: 10.1001/jamapsychiatry.2023.2355.2807609 [DOI] [PubMed] [Google Scholar]
- 27.Teychenne M, White RL, Richards J, Schuch FB, Rosenbaum S, Bennie JA. Do we need physical activity guidelines for mental health: what does the evidence tell us? Ment Health Phys Act. 2020 Mar;18:100315. doi: 10.1016/j.mhpa.2019.100315. doi: 10.1016/j.mhpa.2019.100315. [DOI] [Google Scholar]
- 28.Firth J, Solmi M, Wootton RE, Vancampfort D, Schuch FB, Hoare E, Gilbody S, Torous J, Teasdale SB, Jackson SE, Smith L, Eaton M, Jacka FN, Veronese N, Marx W, Ashdown-Franks G, Siskind D, Sarris J, Rosenbaum S, Carvalho AF, Stubbs B. A meta-review of "lifestyle psychiatry": the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020 Oct;19(3):360–80. doi: 10.1002/wps.20773. https://europepmc.org/abstract/MED/32931092 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.WHO guidelines on physical activity and sedentary behaviour. World Health Organization. 2020. [2024-02-20]. https://apps.who.int/iris/bitstream/handle/10665/336656/9789240015128-eng.pdf?sequence=1&isAllowed=y . [PubMed]
- 30.Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, Macera CA, Heath GW, Thompson PD, Bauman A. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007 Aug;39(8):1423–34. doi: 10.1249/mss.0b013e3180616b27.00005768-200708000-00027 [DOI] [PubMed] [Google Scholar]
- 31.Naczenski LM, Vries JD, Hooff ML, Kompier MA. Systematic review of the association between physical activity and burnout. J Occup Health. 2017 Nov 25;59(6):477–94. doi: 10.1539/joh.17-0050-RA. https://europepmc.org/abstract/MED/28993574 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Bischoff LL, Otto AK, Hold C, Wollesen B. The effect of physical activity interventions on occupational stress for health personnel: a systematic review. Int J Nurs Stud. 2019 Sep;97:94–104. doi: 10.1016/j.ijnurstu.2019.06.002.S0020-7489(19)30151-8 [DOI] [PubMed] [Google Scholar]
- 33.Naz O, Ibrahim M, Mohiuddin AF, Khan AA, Samad Z. Public health data quality and evidence use in developing countries: a call to action. Front Public Health. 2023;11:1194499. doi: 10.3389/fpubh.2023.1194499. https://europepmc.org/abstract/MED/37483937 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Moola S, Munn Z, Sears K, Sfetcu R, Currie M, Lisy K, Tufanaru C, Qureshi R, Mattis P, Mu P. Conducting systematic reviews of association (etiology): the Joanna Briggs Institute's approach. Int J Evid Based Healthc. 2015 Sep;13(3):163–9. doi: 10.1097/XEB.0000000000000064. [DOI] [PubMed] [Google Scholar]
- 35.Munn Z, Stern C, Aromataris E, Lockwood C, Jordan Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol. 2018 Jan 10;18(1):5. doi: 10.1186/s12874-017-0468-4. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/s12874-017-0468-4 .10.1186/s12874-017-0468-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. doi: 10.1136/bmj.n71. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=33782057 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rethlefsen ML, Kirtley S, Waffenschmidt S, Ayala AP, Moher D, Page MJ, Koffel JB, PRISMA-S Group PRISMA-S: an extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst Rev. 2021 Jan 26;10(1):39. doi: 10.1186/s13643-020-01542-z. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-020-01542-z .10.1186/s13643-020-01542-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Larson-Meyer DE. A systematic review of the energy cost and metabolic intensity of yoga. Med Sci Sports Exerc. 2016 Aug;48(8):1558–69. doi: 10.1249/MSS.0000000000000922.00005768-201608000-00016 [DOI] [PubMed] [Google Scholar]
- 39.Chen CH, Hung KS, Chung YC, Yeh ML. Mind-body interactive qigong improves physical and mental aspects of quality of life in inpatients with stroke: a randomized control study. Eur J Cardiovasc Nurs. 2019 Dec;18(8):658–66. doi: 10.1177/1474515119860232. [DOI] [PubMed] [Google Scholar]
- 40.Zeng ZP, Liu YB, Fang J, Liu Y, Luo J, Yang M. Effects of Baduanjin exercise for knee osteoarthritis: a systematic review and meta-analysis. Complement Ther Med. 2020 Jan;48:102279. doi: 10.1016/j.ctim.2019.102279.S0965-2299(19)30966-5 [DOI] [PubMed] [Google Scholar]
- 41.Rotenstein LS, Torre M, Ramos MA, Rosales RC, Guille C, Sen S, Mata DA. Prevalence of burnout among physicians: a systematic review. JAMA. 2018 Sep 18;320(11):1131–50. doi: 10.1001/jama.2018.12777. https://europepmc.org/abstract/MED/30326495 .2702871 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Edú-Valsania S, Laguía A, Moriano JA. Burnout: a review of theory and measurement. Int J Environ Res Public Health. 2022 Feb 04;19(3):1780. doi: 10.3390/ijerph19031780. https://www.mdpi.com/resolver?pii=ijerph19031780 .ijerph19031780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Shoman Y, Marca SC, Bianchi R, Godderis L, van der Molen HF, Guseva Canu I. Psychometric properties of burnout measures: a systematic review. Epidemiol Psychiatr Sci. 2021 Jan 13;30:e8. doi: 10.1017/S2045796020001134. https://europepmc.org/abstract/MED/33436137 .S2045796020001134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016 Dec 05;5(1):210. doi: 10.1186/s13643-016-0384-4. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-016-0384-4 .10.1186/s13643-016-0384-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, Currie M, Qureshi R, Mattis PF, Lisy K, Mu P. Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. Joanna Briggs Institute Reviewer's Manual. Adelaide, Australia: Joanna Briggs Institute; 2017. [DOI] [Google Scholar]
- 46.Shoureshi P, Guerre M, Seideman CA, Callejas DG, Amling CL, Bassale S, Chouhan JD. Addressing burnout in urology: a qualitative assessment of interventions. Urol Pract. 2022 Jan;9(1):101–7. doi: 10.1097/UPJ.0000000000000282. [DOI] [PubMed] [Google Scholar]
- 47.Chayu T, Kreitler S. Burnout in nephrology nurses in Israel. Nephrol Nurs J. 2011;38(1):65–78. [PubMed] [Google Scholar]
- 48.Fields AI, Cuerdon TT, Brasseux CO, Getson PR, Thompson AE, Orlowski JP, Youngner SJ. Physician burnout in pediatric critical care medicine. Crit Care Med. 1995 Aug;23(8):1425–9. doi: 10.1097/00003246-199508000-00018. [DOI] [PubMed] [Google Scholar]
- 49.Ajab S, Ádam B, Al Hammadi M, Al Bastaki N, Al Junaibi M, Al Zubaidi A, Hegazi M, Grivna M, Kady S, Koornneef E, Neves R, Uva AS, Sheek-Hussein M, Loney T, Serranheira F, Paulo MS. Occupational health of frontline healthcare workers in the United Arab Emirates during the COVID-19 pandemic: a snapshot of summer 2020. Int J Environ Res Public Health. 2021 Oct 29;18(21):11410. doi: 10.3390/ijerph182111410. https://www.mdpi.com/resolver?pii=ijerph182111410 .ijerph182111410 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Alvares ME, Thomaz EB, Lamy ZC, Nina RV, Pereira MU, Garcia JB. Burnout syndrome among healthcare professionals in intensive care units: a cross-sectional population-based study. Rev Bras Ter Intensiva. 2020 Jun;32(2):251–60. doi: 10.5935/0103-507x.20200036. https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-507X2020000200251&lng=en&nrm=iso&tlng=en .S0103-507X2020000200251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bin Dahmash A, Alorfi FK, Alharbi A, Aldayel A, Kamel AM, Almoaiqel M. Burnout phenomenon and its predictors in radiology residents. Acad Radiol. 2020 Jul;27(7):1033–9. doi: 10.1016/j.acra.2019.09.024.S1076-6332(19)30457-X [DOI] [PubMed] [Google Scholar]
- 52.Chokri A, Brouki Y, Elo'rdi A, Barkaoui M, Elgot A, Ouzir M. Burnout among healthcare professionals in Morocco: impact of physical activity and work-related factors during COVID-19. [2024-03-13];ResearchGate. 2021 https://www.researchgate.net/publication/354601250_Burnout_among_healthcare_professionals_in_Morocco_impact_of_physical_activity_and_work-related_factors_during_COVID-19 . [Google Scholar]
- 53.Portero de la Cruz S, Cebrino J, Herruzo J, Vaquero-Abellán M. A multicenter study into burnout, perceived stress, job satisfaction, coping strategies, and general health among emergency department nursing staff. J Clin Med. 2020 Apr 02;9(4):1007. doi: 10.3390/jcm9041007. https://www.mdpi.com/resolver?pii=jcm9041007 .jcm9041007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Eckstein J, Rana ZH, Caravan S, Sharma R, Potters L, Parashar B. Burnout in radiation oncology physician workforce: the effect of mindfulness and fulfillment. Adv Radiat Oncol. 2022;7(6):100971. doi: 10.1016/j.adro.2022.100971. https://linkinghub.elsevier.com/retrieve/pii/S2452-1094(22)00078-1 .S2452-1094(22)00078-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Feng S, Taravati P, Ding L, Menda S. Burnout in ophthalmology residency: a national survey. J Acad Ophthalmol. 2018 Jul 19;10(01):e98–107. doi: 10.1055/s-0038-1666850. [DOI] [Google Scholar]
- 56.Ghoraishian M, Zare Mehrjardi H, Askari J, Abrisham SM, Sobhan MR. The frequency of burnout among Iranian orthopedic surgeons and residents. Arch Bone Jt Surg. 2022 Jan;10(1):78–84. doi: 10.22038/abjs.2021.52914.2625. https://europepmc.org/abstract/MED/35291244 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Goldberg R, Boss RW, Chan L, Goldberg J, Mallon WK, Moradzadeh D, Goodman EA, McConkie ML. Burnout and its correlates in emergency physicians: four years' experience with a wellness booth. Acad Emerg Med. 1996 Dec;3(12):1156–64. doi: 10.1111/j.1553-2712.1996.tb03379.x. https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=1069-6563&date=1996&volume=3&issue=12&spage=1156 . [DOI] [PubMed] [Google Scholar]
- 58.Hu Z, Wang H, Xie J, Zhang J, Li H, Liu S, Li Q, Yang Y, Huang Y. Burnout in ICU doctors and nurses in mainland China-a national cross-sectional study. J Crit Care. 2021 Apr;62:265–70. doi: 10.1016/j.jcrc.2020.12.029. https://linkinghub.elsevier.com/retrieve/pii/S0883-9441(20)30823-6 .S0883-9441(20)30823-6 [DOI] [PubMed] [Google Scholar]
- 59.Lebensohn P, Dodds S, Benn R, Brooks AJ, Birch M, Cook P, Schneider C, Sroka S, Waxman D, Maizes V. Resident wellness behaviors: relationship to stress, depression, and burnout. Fam Med. 2013 Sep;45(8):541–9. https://www.stfm.org/familymedicine/vol45issue8/Lebensohn541 . [PubMed] [Google Scholar]
- 60.McClafferty H, Brooks AJ, Chen MK, Brenner M, Brown M, Esparham A, Gerstbacher D, Golianu B, Mark J, Weydert J, Yeh AM, Maizes V. Pediatric integrative medicine in residency program: relationship between lifestyle behaviors and burnout and wellbeing measures in first-year residents. Children (Basel) 2018 Apr 23;5(4):54. doi: 10.3390/children5040054. https://www.mdpi.com/resolver?pii=children5040054 .children5040054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Ng AP, Chin WY, Wan EY, Chen J, Lau CS. Prevalence and severity of burnout in Hong Kong doctors up to 20 years post-graduation: a cross-sectional study. BMJ Open. 2020 Oct 27;10(10):e040178. doi: 10.1136/bmjopen-2020-040178. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=33109674 .bmjopen-2020-040178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Olson SM, Odo NU, Duran AM, Pereira AG, Mandel JH. Burnout and physical activity in minnesota internal medicine resident physicians. J Grad Med Educ. 2014 Dec;6(4):669–74. doi: 10.4300/JGME-D-13-00396. https://europepmc.org/abstract/MED/26140116 .JGME-D-13-00396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Panse N, Panse S, Ravi S, Mankar H, Karanjkar A, Sahasrabudhe P. Burnout among plastic surgery residents in India: an observational study. Indian J Plast Surg. 2020 Dec;53(3):387–393. doi: 10.1055/s-0040-1719238. http://www.thieme-connect.com/DOI/DOI?10.1055/s-0040-1719238 .IJPS19100220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Reed L, Mamidala M, Stocks R, Sheyn A. Factors correlating to burnout among otolaryngology residents. Ann Otol Rhinol Laryngol. 2020 Jun;129(6):599–604. doi: 10.1177/0003489420903329. [DOI] [PubMed] [Google Scholar]
- 65.Shanafelt TD, Oreskovich MR, Dyrbye LN, Satele DV, Hanks JB, Sloan JA, Balch CM. Avoiding burnout: the personal health habits and wellness practices of US surgeons. Ann Surg. 2012 Apr;255(4):625–33. doi: 10.1097/SLA.0b013e31824b2fa0. [DOI] [PubMed] [Google Scholar]
- 66.Tiwari V, Kavanaugh A, Martin G, Bergman M. High burden of burnout on rheumatology practitioners. J Rheumatol. 2020 Dec 01;47(12):1831–4. doi: 10.3899/jrheum.191110.jrheum.191110 [DOI] [PubMed] [Google Scholar]
- 67.Vinnikov D, Dushpanova A, Kodasbaev A, Romanova Z, Almukhanova A, Tulekov Z, Toleu E, Ussatayeva G. Occupational burnout and lifestyle in Kazakhstan cardiologists. Arch Public Health. 2019;77:13. doi: 10.1186/s13690-019-0345-1. https://archpublichealth.biomedcentral.com/articles/10.1186/s13690-019-0345-1 .345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Vinnikov D, Romanova Z, Ussatayeva G, Tulekov Z, Dushimova Z, Khussainova I, Dushpanova A. Occupational burnout in oncologists in Kazakhstan. Occup Med (Lond) 2021 Nov 06;71(8):375–80. doi: 10.1093/occmed/kqab121.6359534 [DOI] [PubMed] [Google Scholar]
- 69.Yang G, Liu J, Liu L, Wu X, Ding S, Xie J. Burnout and resilience among transplant nurses in 22 hospitals in China. Transplant Proc. 2018 Dec;50(10):2905–10. doi: 10.1016/j.transproceed.2018.04.033.S0041-1345(18)30603-1 [DOI] [PubMed] [Google Scholar]
- 70.Trockel M, Bohman B, Lesure E, Hamidi MS, Welle D, Roberts L, Shanafelt T. A brief instrument to assess both burnout and professional fulfillment in physicians: reliability and validity, including correlation with self-reported medical errors, in a sample of resident and practicing physicians. Acad Psychiatry. 2018 Feb;42(1):11–24. doi: 10.1007/s40596-017-0849-3. https://europepmc.org/abstract/MED/29196982 .10.1007/s40596-017-0849-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen burnout inventory: a new tool for the assessment of burnout. Work Stress. 2005 Jul;19(3):192–207. doi: 10.1080/02678370500297720. [DOI] [Google Scholar]
- 72.Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual, 3rd edition. Washington, DC: Consulting Psychologists Press; 1996. [Google Scholar]
- 73.Borritz M, Kristensen TS, Villadsen E, Christensen KB. The Copenhagen burnout inventory: a new tool for the assessment of burnout. Work Stress. 2005 Jul;19(3):192–207. doi: 10.1080/02678370500297720. [DOI] [Google Scholar]
- 74.Riley MR, Mohr DC, Waddimba AC. The reliability and validity of three-item screening measures for burnout: evidence from group-employed health care practitioners in upstate New York. Stress Health. 2018 Feb;34(1):187–93. doi: 10.1002/smi.2762. [DOI] [PubMed] [Google Scholar]
- 75.West CP, Dyrbye LN, Sloan JA, Shanafelt TD. Single item measures of emotional exhaustion and depersonalization are useful for assessing burnout in medical professionals. J Gen Intern Med. 2009 Dec;24(12):1318–21. doi: 10.1007/s11606-009-1129-z. https://europepmc.org/abstract/MED/19802645 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Dolan ED, Mohr D, Lempa M, Joos S, Fihn SD, Nelson KM, Helfrich CD. Using a single item to measure burnout in primary care staff: a psychometric evaluation. J Gen Intern Med. 2015 May;30(5):582–7. doi: 10.1007/s11606-014-3112-6. https://europepmc.org/abstract/MED/25451989 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Maslach C, Leiter MP, Jackson SE. Maslach Burnout Inventory, 4th edition. Menlo Park, CA: Mind Garden; 2018. [Google Scholar]
- 78.Golembiewski RT, Munzenrider R, Carter D. Phases of progressive burnout and their work site covariants: critical issues in OD research and praxis. J Appl Behav Sci. 1983;19(4):461–81. doi: 10.1177/002188638301900408. [DOI] [PubMed] [Google Scholar]
- 79.Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003 Aug;35(8):1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB. [DOI] [PubMed] [Google Scholar]
- 80.2008 physical activity guidelines for Americans. U.S. Department of Health and Human Services. 2008. [2024-02-20]. http://www.health.gov/paguidelines/pdf/paguide.pdf .
- 81.Ricci J, Gagnon L. Evaluation du niveau d'activité physique et de condition physique. Questionnaire Ricci & Gagnon. 2016. [2023-05-18]. https://www.ameli.fr/sites/default/files/questionnaire-activite-physique_cpam-haute-savoie.pdf .
- 82.Brooks A, Dodds S, Cook P, Maizes V, Lebensohn P. Psychometric analyses of the Arizona Lifestyle Inventory: a multi-dimensional integrative medicine measure to assess wellness behaviors. J Altern Complement Med. 2014 May;20(5):A133. doi: 10.1089/acm.2014.5357.abstract. https://www.liebertpub.com/doi/10.1089/acm.2014.5357.abstract . [DOI] [Google Scholar]
- 83.How much physical activity do adults need? Centers for Disease Control and Prevention. 2022. Jun 02, [2023-05-18]. https://www.cdc.gov/physicalactivity/basics/adults/index.htm?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fphysicalactivity%2Feveryone%2Fguidelines%2Fadults.html .
- 84.Lee PH, Macfarlane DJ, Lam TH, Stewart SM. Validity of the international physical activity questionnaire short form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Act. 2011 Oct 21;8:115. doi: 10.1186/1479-5868-8-115. https://ijbnpa.biomedcentral.com/articles/10.1186/1479-5868-8-115 .1479-5868-8-115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Hosmer DW, Lemeshow S. Applied Logistic Regression, 2nd edition. Hoboken, NJ: John Wiley & Sons; 2005. [Google Scholar]
- 86.Maslach C, Leiter MP. How to measure burnout accurately and ethically. Harvard Business Review. 2021. Mar 19, [2023-02-22]. https://hbr.org/2021/03/how-to-measure-burnout-accurately-and-ethically .
- 87.Neria Y, Nandi A, Galea S. Post-traumatic stress disorder following disasters: a systematic review. Psychol Med. 2008 Apr;38(4):467–80. doi: 10.1017/S0033291707001353. https://europepmc.org/abstract/MED/17803838 .S0033291707001353 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Mitchell AE, Galli F, Keyworth C, Vegni E, Salas E. Editorial: coronavirus disease (COVID-19): the mental health, resilience, and communication resources for the short- and long-term challenges faced by healthcare workers. Front Psychol. 2022;13:904328. doi: 10.3389/fpsyg.2022.904328. https://air.unimi.it/handle/2434/923565 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.McFarland DC, Hlubocky F, Riba M. Update on addressing mental health and burnout in physicians: what is the role for psychiatry? Curr Psychiatry Rep. 2019 Oct 15;21(11):108. doi: 10.1007/s11920-019-1100-6. https://europepmc.org/abstract/MED/31617020 .10.1007/s11920-019-1100-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Mosadeghrad AM. Factors influencing healthcare service quality. Int J Health Policy Manag. 2014 Jul;3(2):77–89. doi: 10.15171/ijhpm.2014.65. https://europepmc.org/abstract/MED/25114946 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Lu DW. Sleep and burnout among health care professionals-the role of the individual. JAMA Netw Open. 2023 Nov 01;6(11):e2341882. doi: 10.1001/jamanetworkopen.2023.41882. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2023.41882 .2811328 [DOI] [PubMed] [Google Scholar]
- 92.Panagioti M, Geraghty K, Johnson J, Zhou A, Panagopoulou E, Chew-Graham C, Peters D, Hodkinson A, Riley R, Esmail A. Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern Med. 2018 Oct 01;178(10):1317–31. doi: 10.1001/jamainternmed.2018.3713. https://europepmc.org/abstract/MED/30193239 .2698144 [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 93.Panagioti M, Panagopoulou E, Bower P, Lewith G, Kontopantelis E, Chew-Graham C, Dawson S, van Marwijk H, Geraghty K, Esmail A. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017 Feb 01;177(2):195–205. doi: 10.1001/jamainternmed.2016.7674.2588814 [DOI] [PubMed] [Google Scholar]
- 94.Hassard J, Teoh K, Cox T, Dewe P, Cosmar M, Gründler R, Flemming D, Cosemans B, Van den Broek K. Calculating the cost of work-related stress and psychosocial risks: European risk observatory literature review. European Agency for Safety and Health at Work. 2014. [2024-02-20]. https://osha.europa.eu/sites/default/files/cost-of-work-related-stress.pdf .
- 95.Melnick ER, Sinsky CA, Shanafelt T. Funding research on health workforce well-being to optimize the work environment. JAMA. 2023 Apr 11;329(14):1145–6. doi: 10.1001/jama.2023.2073.2802011 [DOI] [PubMed] [Google Scholar]
- 96.Physical activity. World Health Organization. 2020. [2022-06-27]. https://www.who.int/news-room/fact-sheets/detail/physical-activity .
- 97.Josefsson T, Lindwall M, Archer T. Physical exercise intervention in depressive disorders: meta-analysis and systematic review. Scand J Med Sci Sports. 2014 Apr;24(2):259–72. doi: 10.1111/sms.12050. [DOI] [PubMed] [Google Scholar]
- 98.Wender CL, Manninen M, O'Connor PJ. The effect of chronic exercise on energy and fatigue states: a systematic review and meta-analysis of randomized trials. Front Psychol. 2022;13:907637. doi: 10.3389/fpsyg.2022.907637. https://europepmc.org/abstract/MED/35726269 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Stults-Kolehmainen MA, Sinha R. The effects of stress on physical activity and exercise. Sports Med. 2014 Jan;44(1):81–121. doi: 10.1007/s40279-013-0090-5. https://europepmc.org/abstract/MED/24030837 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Barriers to being active quiz. Center for Disease Control and Prevention. 2011. [2023-09-13]. https://agsci.oregonstate.edu/sites/agscid7/files/kbrec/pop.2.barriers_to_being_active.l2.pdf .
- 101.Pearce M, Garcia L, Abbas A, Strain T, Schuch FB, Golubic R, Kelly P, Khan S, Utukuri M, Laird Y, Mok A, Smith A, Tainio M, Brage S, Woodcock J. Association between physical activity and risk of depression: a systematic review and meta-analysis. JAMA Psychiatry. 2022 Jun 01;79(6):550–9. doi: 10.1001/jamapsychiatry.2022.0609. https://europepmc.org/abstract/MED/35416941 .2790780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Fluetsch N, Levy C, Tallon L. The relationship of physical activity to mental health: a 2015 behavioral risk factor surveillance system data analysis. J Affect Disord. 2019 Jun 15;253:96–101. doi: 10.1016/j.jad.2019.04.086.S0165-0327(19)30300-3 [DOI] [PubMed] [Google Scholar]
- 103.Selvaraj CS, Abdullah N. Physically active primary care doctors are more likely to offer exercise counselling to patients with cardiovascular diseases: a cross-sectional study. BMC Prim Care. 2022 Mar 29;23(1):59. doi: 10.1186/s12875-022-01657-3. https://europepmc.org/abstract/MED/35350999 .10.1186/s12875-022-01657-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Füzéki E, Weber T, Groneberg DA, Banzer W. Physical activity counseling in primary care in Germany-an integrative review. Int J Environ Res Public Health. 2020 Aug 04;17(15):5625. doi: 10.3390/ijerph17155625. https://www.mdpi.com/resolver?pii=ijerph17155625 .ijerph17155625 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Ringeval M, Wagner G, Denford J, Paré G, Kitsiou S. Fitbit-based interventions for healthy lifestyle outcomes: systematic review and meta-analysis. J Med Internet Res. 2020 Oct 12;22(10):e23954. doi: 10.2196/23954. https://www.jmir.org/2020/10/e23954/ v22i10e23954 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Ferguson T, Olds T, Curtis R, Blake H, Crozier AJ, Dankiw K, Dumuid D, Kasai D, O'Connor E, Virgara R, Maher C. Effectiveness of wearable activity trackers to increase physical activity and improve health: a systematic review of systematic reviews and meta-analyses. Lancet Digit Health. 2022 Aug;4(8):e615–26. doi: 10.1016/S2589-7500(22)00111-X. https://linkinghub.elsevier.com/retrieve/pii/S2589-7500(22)00111-X .S2589-7500(22)00111-X [DOI] [PubMed] [Google Scholar]
- 107.Schaufeli WB, Bakker AB, Hoogduin K, Schaap C, Kladler A. on the clinical validity of the maslach burnout inventory and the burnout measure. Psychol Health. 2001 Sep;16(5):565–82. doi: 10.1080/08870440108405527. [DOI] [PubMed] [Google Scholar]
- 108.Godia J, Pifarré M, Vilaplana J, Solsona F, Abella F, Calvo A, Mitjans A, Gonzalez-Olmedo MP. A free app for diagnosing burnout (BurnOut App): development study. JMIR Med Inform. 2022 Sep 06;10(9):e30094. doi: 10.2196/30094. https://medinform.jmir.org/2022/9/e30094/ v10i9e30094 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Eligibility criteria.
Search strings.
Classification and interpretation of burnout scores.
Predictors adopted in bivariate analyses and in multivariable regression analyses (other than physical activity).
Quality assessment.
PRISMA checklist.
PRISMA-S Checklist.
Data Availability Statement
All data generated or analyzed during this study are included in this published paper (and its supplementary information files).