

Abstract
Children with eosinophilic esophagitis (EoE) are faced with ongoing treatments that can impact their wellbeing. There are no evidence-based resources that families can implement independently to cope with EoE-related stressors. This study aimed to examine acceptability, feasibility, and preliminary outcomes of the newly developed Cellie Coping Kit for Children with EoE intervention. Forty child-caregiver dyads completed a baseline assessment (T1) and initiated the intervention; 30 (75%) child participants and 33 (82.5%) caregivers were retained to follow-up (T2). Of those who completed the T2 assessment, most reported that the intervention was easy to use (>90%) and would recommend the intervention to others (>90%). The intervention was feasible: >70% used the kit, and most indicated they would use it again (>75%). More than half of families reported learning new information and/or coping strategies. No statistically significant changes were identified in comparing T1 and T2 coping and health-related quality of life. These findings suggest that the Cellie Coping Kit for Children with EoE is a promising intervention in that it was well accepted, feasible, and helped many families learn novel strategies on how to manage EoE challenges. Future research should examine how to strengthen the intervention to achieve longer-term targeted outcomes.
Keywords: Coping skills, Eosinophilic Esophagitis, pediatrics, quality of life
Introduction
Eosinophilic esophagitis (EoE) is a chronic inflammatory disease of the esophagus presenting with numerous gastrointestinal symptoms such as abdominal pain, heartburn, difficulty swallowing, and food impactions (Furuta et al., 2007). EoE affects about 10–50/100,000 children in the United States with increasing incidence and prevalence in recent years (Noel et al., 2004). EoE is associated with an immune response to food-related antigens leading to an eosinophil-predominant inflammatory response in the esophagus (Clayton and Peterson, 2018). Upper gastrointestinal endoscopy with esophageal biopsies remains the gold standard diagnostic method, and follow-up endoscopies are required to manage EoE (Richter, 2016). EoE treatment often involves food elimination diets, topical swallowed steroids, and closely endoscopically surveyed stepwise food reintroduction (Rossetti et al., 2020). No cures are currently available for EoE, and treatments can be challenging (Gonsalves and Aceves, 2020). Thus, there is a need to develop and test effective and affordable resources to help families manage these many challenges.
In addition to challenging symptoms and treatment regimens, children with EoE may encounter a myriad of emotional health symptoms (Taft et al., 2019). More specifically, children with EoE may experience anxiety, communication difficulties, depression symptoms, poor health-related quality of life (HR-QOL), and sleep problems (Harris et al., 2013; Klinnert et al., 2014). Many children with EoE may also encounter challenges related to social functioning, such as having difficulty making friends or having no friends (Harris et al., 2013). Feelings of isolation can arise if children are unable to take part in food-related activities with their peers or family (Klinnert et al., 2014).
How a child copes with their medical condition may impact their emotional health (Marsac et al., 2017). While parents are often key supports for their children, they may not know how to support their child’s coping in context of a medical condition, that is, how to provide coping assistance (Marsac et al., 2011). Currently, while there is a demonstrated need for mental health support for children with EoE, there are no evidence-based resources to help children and families cope with commonly experienced EoE-related stressors that families can use independently.
To help fill this need, a multidisciplinary team of pediatric EoE experts developed the Cellie Coping Kit for Children with EoE intervention. This intervention was adapted from an intervention originally developed for children with cancer (Marsac et al., 2012). The primary purpose of the Cellie Coping Kit intervention is to equip families with evidence-based coping strategies to help them manage the daily challenges of EoE. While research on the Cellie Coping Kit intervention for children with other medical conditions (e.g., cancer, food allergy, and injury) suggests promise, there is no data currently published on the Cellie Coping Kit for Children with EoE (e.g., Cole et al., 2017; Marsac et al., 2012). The unique challenges of EoE (e.g., food-related social impact, challenges with impaction, and frequent endoscopies) may affect how the intervention is accepted and used by families. Thus, we do not yet know how children and families will respond to this newly adapted intervention tool.
Study aim
To report initial Cellie Coping Kit for Children with EoE intervention acceptability, feasibility, and preliminary outcomes (i.e., change in EoE knowledge, increase in adaptive coping strategies, increase in coping assistance, and improved HR-QOL) in children with EoE and their caregivers.
Methods
Data were collected from two pediatric clinics in the Northeastern (Urban site) and Southeastern (Rural site) regions of the United States. The study was approved by the Institutional Review Board (IRB) at Children’s Hospital of Philadelphia (IRB 16–013571).
Children were eligible for the study if they (1) had a diagnosis of EoE, (2) were between the ages of 7 and 13 years old, (3) were actively engaged in a treatment regimen, (4) were able to read and understand English, (5) were cognitively able to answer study questions (as determined by the medical team), and (6) had a caregiver available to participate and to consent to their participation. Caregivers were eligible to participate if they were able to read and understand English, were cognitively able to answer study questions, and if their child participated. Those who did not meet inclusion criteria above were excluded from study participation.
Procedures
At each site, medical teams identified potential participants and notified the research team. A trained research assistant (RA) approached patients and their caregivers during an appointment to ascertain their interest in the study and to obtain consent and assent. At baseline (T1), caregivers completed a demographics questionnaire, parent-reported child HR-QOL measure, and a measure of coping assistance (i.e., how parents helped their child cope with EoE). Children completed measures of how they coped with EoE and a measure of HR-QOL.
Following completion of measures, a RA introduced the Cellie Coping Kit intervention and demonstrated how to use the kit (see below for further description of the intervention). More specifically, RAs worked with children and parents to identify at least one EoE-related challenge that the child struggled with (e.g., emotional reactions to EoE; difficulty with an elimination diet), found that challenge in the intervention materials, and guided families in how to select one or more evidence-based strategies to use for that particular challenge. This took approximately 5 to 10 min for each family.
During a 4-week follow-up phone assessment (T2), children and caregivers independently repeated baseline measures, responded to semi-structured interviews, and completed satisfaction questionnaires.
Description of the Cellie Coping Kit for Children with EoE intervention
The Cellie Coping Kit intervention includes a stuffed toy named “Cellie,” a deck of 46 coping cards, and a 45-page guide for caregivers. Intervention content was initially adapted from the cancer version of the kit (Marsac et al., 2012). Next, a literature review was conducted to identify additional EoE-specific challenges as well as effective strategies for managing these challenges. Finally, prior to conducting this study, the intervention materials were reviewed by a team of EoE experts from several institutions including gastroenterologists, social workers, psychologists, child life specialists, and nurses.
The purpose of the Cellie toy is to engage children in the intervention. The Cellie toy is also used in some of the recommended coping strategies (e.g., write your questions down and store them in Cellie’s mouth). The purpose of the coping cards is to provide the child with developmentally appropriate, evidence-based coping strategies for reducing common feelings of distress associated with EoE. The goal of the caregiver book is to provide evidence-based strategies that caregivers can use to support their child in dealing with the challenges of EoE.
Designed for children ages 6 to 13 years old, The Cellie Coping Kit for Children with EoE offers a variety of coping strategies for caregivers and children to choose from, allowing them to select and utilize the strategies that best fit their individual needs. Caregivers and children can use the kit as often or as little as necessary. Intervention materials include information on eating challenges, pain and discomfort, sleep challenges, medical care, emotional reactions, and family, friend, and school challenges. There are also special sections on food impactions, G-tubes, and anaphylaxis. In addition to the recommended strategies, families are encouraged to write their own ideas or ideas from their medical team onto the cards and/or book. Space is provided for new ideas on the child’s coping cards and in the caregiver’s guide. All items fit into a small backpack, making it easy for children to transport the kit for use outside of the home (e.g., at school, doctor appointments, and to the hospital). See Figure 1 for a sample coping card.
Figure 1.
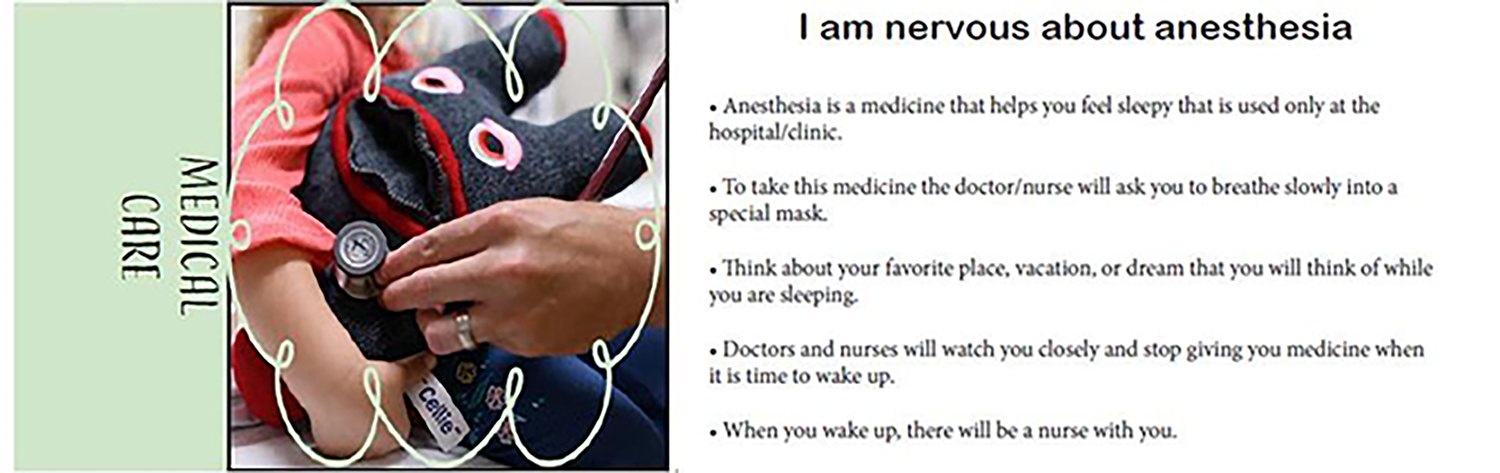
Sample coping card from the Cellie Coping Kit for children with EoE. This card is one of 45-cards from the Cellie Coping Kit for Children with EoE intervention. If a child was struggling with anesthesia, the child and their caregiver could find this card in the deck and select one of these strategies to try.
Measures
Semi-structured interview.
Caregivers and children independently completed a semi-structured interview (adapted from a previous study) used to assess intervention acceptability, feasibility, knowledge about EoE, and new coping strategies (Marsac et al., 2012). Sample questions include “Did you learn anything from using the Cellie Coping Kit? If so, what did you learn?” and “Was there anything that got in the way of using [or made it difficult for you to use] the Cellie Coping Kit?” Full interview guide is available upon request.
Satisfaction questionnaire.
Caregivers and children independently completed a Satisfaction Questionnaire (adapted from a previous study) to gauge families’ satisfaction with the Cellie Coping Kit for Children with EoE (Marsac et al., 2012). This measure included open-ended questions where participants commentated on strengths of the kit and areas for improvement. Additionally, participants completed 14 items (i.e., Yes/No; A Lot, Some, Not at All) to assess feasibility, usability, visual appeal, trustworthiness, and comprehensibility of the intervention materials.
How I Coped Under Pressure Scale (HICUPS).
Children completed the HICUPS as a measure of coping behaviors. Only the subscales that aligned with content addressed by the Cellie Coping Kit intervention were used in this study (Cognitive Restructuring, Avoidance, and Support Seeking). Participants were asked to respond on a four-point Likert scale from 0 (never) to 4 (most of the time). The HICUPS has been used with multiple children with medical conditions and consistently demonstrates acceptable psychometric properties (Ayers et al., 1996).
Parental Socialization of Coping Questionnaire (PSCQ).
Caregivers completed the PSCQ as a measure of parental coaching of child coping behaviors. The PSCQ parallels the HICUPS by asking parents to report on how much they encourage or discourage their child to use each coping strategy when experiencing EoE-related challenges. Similar to the HICUPS, only subscales that aligned with the intervention content were used (Cognitive Restructuring, Avoidance, Support Seeking). Answers are reported on a seven-point Likert scale ranging from 1 (strongly discouraged) to 7 (strongly encouraged). Psychometric properties for the PSCQ have been well-established (Miller et al., 1994).
Pediatric Quality of Life Inventory 3.0: Eosinophilic Esophagitis Module (PedsQL).
Children and caregivers completed the PedsQL 3.0 self-report or parent-proxy report as a measure of child HR-QOL. This version of the PedsQL was adapted specifically for children diagnosed with EoE (e.g., food gets stuck in my throat, I do not like getting an endoscopy) (Franciosi et al., 2012). Participants were asked to indicate how much of a problem each item had been for them in the past month using a five-point Likert scale from 0 (it is never a problem) to 4 (it is almost always a problem). Although psychometrics for the PedsQL 3.0 EoE Module have yet to be established, the PedsQL generally demonstrates strong internal consistency (α = 0.88–0.90; Varni et al., 2001).
Data analysis
IBM SPSS Statistics 27 was used for data management and analyses (IBM Corp, 2020). To assess acceptability and feasibility, categorical responses on the semi-structured interview and satisfaction questionnaire were presented as frequencies. When item-level data was missing, the participant was excluded from those specific analyses but retained in the overall study; thus, valid percentages are presented. Data from open-ended responses was used to help explicate quantitative results. Thus, sample quotes from participants are provided following the frequency analyses. Data from child and caregiver responses on the semi-structured interviews on intervention barriers are categorized with sample quotes provided.
For analyses that used subscales scores (i.e., mean differences between T1 and T2 on coping, coping assistance and HR-QOL), missing data were imputed for cases in which at least 50% of items on a given subscale was complete. When >50% of the items on a subscale were missing, the participant was excluded from those specific analyses but retained in the overall study. We conducted paired samples t tests for coping, coping assistance, and HR-QOL to examine differences between baseline assessments and post-intervention assessments. For some variables, data was not normally distributed; thus, we repeated analyses using nonparametric tests. Results did not change.
Results
Study participants
Forty children (median age 9.7 years) and one caregiver per child (median age 40.5 years) were initially enrolled in the study (T1). At follow-up (T2), 30 (75%) child participants and 33 (82.5%) caregivers completed questionnaires via phone or mail. Consistent with previously reported sex distribution of patients with EoE, our child population was composed of 31 (77.5%) male and 35 (87.5%) White participants. The majority of caregivers participating in the study were females (n = 38, 95%) (see Table 1 for additional demographic information).
Table 1.
Participants” Demographic Characteristics
| N = 40* | |
|---|---|
|
| |
| Child age | M (SD); MED |
| 9.7 (1.8); 10 | |
| Child sex | n (%) |
| Female | 9 (22.5) |
| Male | 31 (77.5) |
| Child race/ethnicity | n (%) |
| Black | 3 (7.5) |
| White | 35 (87.5) |
| Other | 2 (5.0) |
| Parent age | M (SD); MED |
| 40.5 (7.6); 41 | |
| Parent sex | n (%) |
| Female | 38 (95.0) |
| Male | 2 (5.0) |
Includes demographic characteristics at initial enrollment
Acceptability and feasibility
The majority of children and caregivers who completed the T2 assessment reported that they used the Cellie Coping Kit intervention and nearly all indicated that it was easy to use (see Table 2 for n’s and %s). However, one-fifth of children reported that there were too many words on the coping cards, and a few children indicated that the coping cards were confusing. Likewise, a few caregivers reported that the caregiver guide was confusing. As part of the acceptability evaluation, we also asked participants to rate the design and content of the Cellie Coping Kit. The majority of children and their caregivers reported liking the appearance of the Cellie toy and materials. Most children and caregivers also reported liking the coping strategies included in the coping cards and caregiver’s guide. Families also reported that the kit provided good advice and tips, and that the information in the kit was trustworthy. (see Table 2). One parent of a 10-year-old boy noted that it “helped with foods, [learning] what he can and can’t eat.” Most children and their caregivers indicated that they would recommend the kit to other children with EoE. Many participants also found that the kit was fun to use. For example, a 10-year-old boy said that he “played with Cellie, read the cards, and used it with friends.”
Table 2.
Acceptability and feasibility of the Cellie Coping Kit intervention for children with EoE: Child and caregiver report
| Child* | Caregiver* | |
|---|---|---|
|
| ||
| Acceptability | n (%) | n (%) |
| Used the Cellie Coping Kit | 20 (71.4) | 26 (86.7) |
| Child knows how to use Kit | 28 (93.3) | - |
| Coping Cards are easy to use | 27 (93.1) | 28 (93.3) |
| Coping Cards have too many words | 6 (20.0) | 4 (13.3) |
| Coping Cards directions are confusing | 4 (13.8) | - |
| Caregiver book is easy to use | - | 25 (100.0) |
| Caregiver book has too many words | - | 4 (14.3) |
| Likes appearance of Cellie | 26 (86.7) | 29 (93.5) |
| Likes the tips in Coping Cards/Caregivers' Guide | 28 (96.6) | 30 (100) |
| Kit is fun to use | 26 (89.7) | 24 (88.9) |
| Kit gives good advice / tips | 27 (100.0) | 29 (100.0) |
| Information in Kit is trustworthy / true | 29 (100.0) | 31 (100.0) |
| Would recommend the Kit to other kids / families | 26 (92.9) | 31 (100.0) |
| Feasibility | ||
| Frequency of use (for those who used it) | ||
| 1 time | 4 (17.4) | 6(21.4) |
| 2–5 times | 11 (47.8) | 12 (42.9) |
| 5–9 times | 5(21.7) | 3 (10.7) |
| 10 or more times | 3 (10.0) | 7 (25.0) |
| Locations in which Kit was used | ||
| Home | 22 (91.7) | 23 (82.1) |
| Hospital | 2 (8.3) | 2 (7.1) |
| Other | 0 (0.0) | 3 (10.7) |
| Would use the kit again | 27 (90.0) | 23 (76.7) |
Some data were missing at an item level, with sample size ranging from 23–31 participants; valid percentages are reported.
To assess feasibility of use, participants were asked how often they used the intervention, in which settings they used the intervention, and how they used the intervention (see Table 2 for n’s and %s). Of those who reported that they used the intervention, the frequency of use ranged from once to over ten times. During the intervention period, children and parents reported most commonly using the Cellie Coping Kit intervention two to five times and at home. Data from semi-structured interviews suggested that some children used the kit for comfort or when they were nervous before procedures. For example, a 7-year-old girl stated that she used the kit “when nervous, before surgery, [and] to sleep.” Another example is from a 12-year-old boy who stated that he “slept everywhere with Cellie, read the book and the flashcards.” Parents reported using the kit to facilitate communication and to learn new coping tips. For example, a parent of an 11-year-old boy noted using the kit “at restaurants, when [their child] was having anxiety.” Another parent of an 8-year-old boy said that “he used it to [teach about] his illness to teachers at school.”
Of those who completed the T2 assessment, the majority of children (n = 20; 72.0%) and caregivers (n = 15; 54.4%) reported that there were no barriers to using the intervention. Several participants noted that they did not need the intervention during the research study period (children n = 3, 10.8%; caregivers n = 2; 6.8%). Others indicated that they were too busy (n = 3; 10.8%; caregivers n = 5; 17.0%), that it wasn’t helpful (children n = 1, 3.6%; caregivers n = 1, 3.6%), that they didn’t like it (children n = 1, 3.6%), or that they were too old for it (children n = 1, 3.6%; caregivers n = 3, 10.2%). One caregiver also noted that their child liked to keep it in his room and would forget it (caregivers n = 1, 3.6%) and another commented on it not being durable enough (caregivers n = 1, 3.6%).
Preliminary outcomes
Many children (n = 22, 75.9%) and caregivers (n = 16, 64.0%) reported learning new coping strategies. The EoE-specific clinical content allowed parents to educate themselves on the disease. For example, the caregiver of a 7-year-old child expressed, “The [kit] had better terminology to understand his diagnosis.” Another caregiver noted that they learned “how to start checking ingredients [after using the Cellie Coping intervention].” Other caregivers learned how to better communicate with their child about EoE. For example, one mother shared that it helped her learn how to communicate with her son about his feelings about EoE. She stated that “He’s opened up tremendously.”
Coping strategies that were suggested for medical procedures also had an impact on children and parents. An 11-year-old boy mentioned how the Cellie Coping Kit helped him learn “how to cope with getting an IV.” Another child mentioned learning “That it’s easy to make it through having EoE.” One caregiver said that their family learned, “coping techniques, [about] anaphylaxis, communication, and [how to] calm [their] child.”
Some families particularly appreciated learning how to use the “Chef Card;” this card includes instructions to kitchen staff in how to keep their child’s food safe. The family writes the food allergens on the card with the instructions. This promotes the restaurant staff’s awareness about the seriousness of allergen exposure. One 8-year-old boy explained that he liked the Chef card part of the Cellie Kit sharing that “the Chef [card] is much better because they won’t forget, better than just telling them.”
The average scores for children’s self-reported coping behavior (as measured by the HICUPS), caregivers’ self-reported coping assistance (as measured by the PSCQ) and child HR-QOL (as measured by the PedsQL-EoE Module; child and caregiver report) at T1 and T2 are presented in Supplemental Table 1. There were no statistically significant differences pre to post-intervention for coping behavior, coping assistance or HR-QOL.
Discussion
In this study, we achieved our objective of evaluating the feasibility and acceptability of the Cellie Coping Kit for Children with EoE and exploring potential changes in coping, coping assistance, and child HR-QOL pre to post-intervention. Similar to Cellie Coping Kit intervention research with children and caregivers with other chronic medical conditions (e.g., cancer, food allergy; e.g., Cole et al., 2017;Marsac et al., 2012), the current study indicated strong intervention acceptability and feasibility, and identified knowledge gains in regards to EoE and how to cope with EoE-related challenges. However, no statistically significant differences were detected in comparing pre-intervention and post-intervention coping, coping assistance, or HR-QOL.
More specifically, regarding intervention feasibility and acceptability, most families who completed the follow-up assessment reported using the kit, noted some benefit from the intervention, and indicated that they would recommend the intervention to other children with EoE. Thus, the intervention can offer a low-cost avenue for medical teams to provide some initial support to children with EoE and their families, while requiring minimal additional time from the medical teams. Also consistent with other Cellie Coping Kit intervention studies (e.g., Marsac et al., 2018; Cole et al., 2017), a few children and caregivers indicated that the materials had too many words or were confusing. It may be that some families would benefit from intervention materials that are less reading focused, are aimed for a lower reading level, or that use more non-verbal techniques such as visual schedules or pictures of challenges and solutions. As was found in the Cellie Coping Kit intervention for Children with Injury, it may be that some families prefer having the opportunity for additional support in how to use the intervention (Marsac et al., 2018). Future research should investigate how to identify families that may need more support in using the intervention or who may need a different type of intervention.
While children and parents reported learning new EoE-relevant information and coping strategies in the semi-structured interview, no significant improvements in coping, coping assistance, or HR-QOL were detected. A number of factors may have contributed to this finding. In our pilot studies, we did not standardize when a family was introduced to the intervention; thus, some children were enrolled at a time where changes to dietary or medication therapies could have occurred and potentially influenced their reports of coping and/or HR-QOL. This is supported by research suggesting that there is a great degree of variability in HR-QOL due to changes in symptomatology and treatment methods (Lynch et al., 2018; Stern et al., 2018). Alternatively, it may be that a more intensive or different intervention is needed to achieve these intended outcomes.
Of note, over 70% of children and over 50% of parents who completed the follow-up assessment reported no intervention barriers. The most common barriers reported were busy schedules with a few families noting lack of need, child being too old, or general disinterest in the intervention. To address the competing demands on families’ time, incorporating the use of the intervention into medical care (e.g., having the family use it in the waiting rooms; referring to intervention content during medical appointments) could support its use. In addition, medical teams could also implement the Cellie Coping intervention into standard education programs at the time of a new diagnosis, which would help families get started on using it. As noted previously, future research is needed to determine child (e.g., time since EoE diagnosis, general emotional health and coping) and family characteristics (e.g., how caregivers typically support their child via medical interventions) that could be used to predict who could most benefit from the intervention and who might need a different intervention type.
Study limitations
While the study retained 75% of participants to follow-up, given the small sample size we are unable to make conclusions regarding the potential reasons for drop out. Future research should track child and family characteristics to further examine this. In addition, in this small study, we did not limit enrollment to families who were recently diagnosed with EoE; thus, children who had been diagnosed for a longer time may have already developed some adaptive coping strategies (Lee, et al., 2018). However, given that many families identified learning new strategies in response to open-ended questions, it may be that the assessment tools used lacked the sensitivity in detecting the types of coping changes that were observed.
Implications for practice
Currently, EoE is well-recognized in large scale centers across the country. However, some centers may have limited resources directed towards education of patients with EoE and their families (Chang et al., 2019). The treatment of EoE may require multiple adjustments to diet and medication, creating a burden not only to the child but to their caregivers (Hiremath et al., 2019). It is of great importance to provide a comprehensive support system that includes psychosocial resources for the child and their caregivers at the time of a new EoE diagnosis. While some centers have an established multidisciplinary team that includes child life therapists and psychologists specializing in EoE (Harris et al., 2013), children may need additional tools when undergoing medical procedures, while at home, or in school. While the Cellie Coping intervention is not a replacement for mental health care, this intervention may be a first step in laying a foundation to support EoE education and offer new adaptive coping strategies to families without adding much time for medical teams. Additionally, as suggested by Coyne and colleagues (2016), child-centered medical care should include the child’s perspectives and opinion about their medical care. This intervention provides children with the language needed to help them communicate with their families and medical teams about their challenges with their medical condition and care.
Conclusions
In summary, the Cellie Coping Kit for Children with EoE intervention is the first low cost, easy to use coping tool for children with EoE. Results from this study are promising, suggesting that the Cellie Coping Kit intervention provides acceptable, evidence-based coping strategies for children with EoE and their caregivers. Future research should examine child and family characteristics to determine who may benefit the most from the intervention. Future research should also consider how to strengthen the intervention intensity to better achieve intended outcomes of improved coping, coping assistance, and HR-QOL.
Supplementary Material
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number KL2TR001879 (AJB). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This study was also supported by the following NIH Grants: K08DK106444 (ABM), CEGIR (U54 AI117804) (ABM) as well as the Department of Pediatrics at University of Kentucky, Kentucky Children’s Hospital (MLM) and Substance Abuse and Mental Health Services Administration (U79SM080048).
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Marsac is a co-inventor of the Cellie Coping Kit and is the CEO of the Cellie Coping Company. It is possible that Dr. Marsac, the Children’s Hospital of Philadelphia, and the University of Kentucky will benefit financially from the kit. The research presented in the paper has been managed and approved by the University of Kentucky’s Conflict of Interest oversight committee.
Supplemental Material
Supplement material for this article is available in online.
References
- Ayers TS, Sandler IN, West SG, et al. (1996) A dispositional and situational assessment of children’s coping: testing alternative models of coping. Journal of Personality 64: 923–958. [DOI] [PubMed] [Google Scholar]
- Chang JW, Saini SD and Mellinger JL (2019) Management of eosinophilic esophagitis is often discordant with guidelines and not patient-centered: results of a survey of gastroenterologists. Diseases of the Esophagus: Official Journal of the International Society for Diseases of the Esophagus 32(6): doy133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clayton F and Peterson K (2018) Eosinophilic esophagitis: pathophysiology and definition. Gastrointestinal Endoscopy Clinics of North America 28: 1–14. [DOI] [PubMed] [Google Scholar]
- Cole D, Weiss D, Kohser KL, et al. (2017) The Cellie coping kit for children with food allergy: a pilot study. Pediatric Allergy, Immunology, and Pulmonology 30(1): 39–44. DOI: 10.1089/ped.2016.0698. [DOI] [Google Scholar]
- Coyne I, Hallström I and Söderbäck M (2016) Reframing the focus from a family-centred to a child-centred care approach for children’s healthcare. Journal of Child Health Care 20(4): 494–502. DOI: 10.1177/1367493516642744. [DOI] [PubMed] [Google Scholar]
- Franciosi JP, Hommel KA, Greenberg AB, et al. (2012) Development of the pediatric quality of life inventory eosinophilic esophagitis module items: qualitative methods. BMC Gastroenterology 12: 135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furuta GT, Liacouras CA, Collins MH, et al. (2007) Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology 133: 1342–1363. [DOI] [PubMed] [Google Scholar]
- Gonsalves NP and Aceves SS (2020) Diagnosis and treatment of eosinophilic esophagitis. Journal of Allergy and Clinical Immunology 145(1): 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris RF, Menard-Katcher C, Atkins D, et al. (2013) Psychosocial dysfunction in children and adolescents with eosinophilic esophagitis. Journal of Pediatric Gastroenterology and Nutrition 57: 500–505. [DOI] [PubMed] [Google Scholar]
- Hiremath G, Rogers E, Kennedy E, et al. (2019) A comparative analysis of eating behavior of school-aged children with eosinophilic esophagitis and their caregivers’ quality of life: perspectives of caregivers. Dysphagia 34(4): 567–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- IBM Corp (2020) IBM SPSS Statistics for Windows. Version 27.0. Armonk, NY: IBM Corp. [Google Scholar]
- Klinnert MD, Silveira L, Harris R, et al. (2014) Health-related quality of life over time in children with eosinophilic esophagitis and their families. Journal of Pediatric Gastroenterology and Nutrition 59: 308–316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee K, Furuta G and Nguyen N (2018) Eosinophilic esophagitis is an underlying cause for gastrointestinal concerns in children. Frontiers in Pediatrics 6: 113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynch MK, Barnes MJ, Dimmitt RA, et al. (2018) Disease-related predictors of health-related quality of life in youth with eosinophilic esophagitis. Journal of Pediatric Psychology 43: 464–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsac ML, Hildenbrand AK, Clawson K, et al. (2012) Acceptability and feasibility of family use of The Cellie Cancer Coping Kit. Supportive Care in Cancer 20: 3315–3324. [DOI] [PubMed] [Google Scholar]
- Marsac ML, Kassam-Adams N, Delahanty DL, et al. (2017) An initial application of a biopsychosocial framework to predict posttraumatic stress following pediatric injury. Health Psychology 36: 787–796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsac ML, Weiss D, Kohser KL, et al. (2018) The Cellie Coping Kit for children with injury: initial feasibility, acceptability, and outcomes. Child: Care, Health and Development 44: 599–606. [DOI] [PubMed] [Google Scholar]
- Marsac ML, Mirman JH, Kohser KL, et al. (2011) Child coping and parent coping assistance during the peritrauma period in injured children. Family Systems & Health 29: 279–290. [DOI] [PubMed] [Google Scholar]
- Miller PA, Kliewer W, Hepworth JT, et al. (1994) Maternal socialization of children’s postdivorce coping: development of a measurement model. Journal of Applied Developmental Psychology 15: 457–487. [Google Scholar]
- Noel RJ, Putnam PE and Rothenberg ME (2004) Eosinophilic esophagitis. The New England Journal of Medicine 351: 940–941. [DOI] [PubMed] [Google Scholar]
- Richter JE (2016) Current management of eosinophilic esophagitis 2015. Journal of Clinical Gastroenterology 50: 99–110. [DOI] [PubMed] [Google Scholar]
- Rossetti D, Isoldi S and Oliva S (2020) Eosinophilic esophagitis: update on diagnosis and treatment in pediatric patients. Paediatric Drugs 22(4): 343–356. [DOI] [PubMed] [Google Scholar]
- Stern E, Taft T, Zalewski A, et al. (2018) Prospective assessment of disease-specific quality of life in adults with eosinophilic esophagitis. Diseases of the Esophagus: Official Journal of the International Society for Diseases of the Esophagus 31: 1–7. [DOI] [PubMed] [Google Scholar]
- Taft TT, Guadagnoli L and Edlynn T (2019) Anxiety and depression in eosinophilic esophagitis: a scoping review and recommendations for future research. Journal of Asthma and Allergy 12: 389–399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varni JW, Seid M and Kurtin PS (2001) PedsQL 4.0: reliability and validity of the pediatric quality of life inventory version 4.0 generic core scales in healthy and patient populations. Medical Care 39: 800–812. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.