

Abstract
Background Up to now, it is unclear whether different medicinal cannabis (MC) strains are differently efficacious across different medical conditions. In this study, the effectiveness of different MC strains was compared depending on the disease to be treated.
Methods This was an online survey conducted in Germany between June 2020 and August 2020. Patients were allowed to participate only if they received a cannabis -based treatment from pharmacies in the form of cannabis flowers prescribed by a physician.
Results The survey was completed by n=1,028 participants. Most participants (58%) have used MC for more than 1 year, on average, 5.9 different strains. Bedrocan (pure tetrahydrocannabinol to pure cannabidiol [THC:CBD]=22:<1) was the most frequently prescribed strain, followed by Bakerstreet (THC:CBD=19:<1) and Pedanios 22/1 (THC:CBD=22:1). The most frequent conditions MC was prescribed for were different pain disorders, psychiatric and neurological diseases, and gastrointestinal symptoms. Overall, the mean patient-reported effectiveness was 80.1% (range, 0–100%). A regression model revealed no association between the patient-reported effectiveness and the variety. Furthermore, no influence of the disease on the choice of the MC strain was detected. On average, 2.1 side effects were reported (most commonly dry mouth (19.5%), increased appetite (17.1%), and tiredness (13.0%)). However, 29% of participants did not report any side effects. Only 398 participants (38.7%) indicated that costs for MC were covered by their health insurance.
Conclusions Patients self-reported very good efficacy and tolerability of MC. There was no evidence suggesting that specific MC strains are superior depending on the disease to be treated.
Keywords: medicinal cannabis, tetrahydrocannabinol, cannabidiol, patients’ experience, side effects
Introduction
There is increasing evidence that cannabis -based medicine (CBM) is efficacious in many different indications, mainly chronic pain, spasticity in multiple sclerosis, and palliative care 1 . After reintroduction in medicine, the number and type of available CBM constantly increased, ranging from pure tetrahydrocannabinol (THC) to pure cannabidiol (CBD), as well as cannabis extracts and flowers with very different THC:CBD ratios. In Germany, cannabis flowers and extracts were legalized for medical purposes in 2017. In limited exceptional cases and after approval (according to the Social Insurance Code), costs are covered by health insurance. Today (as of 2023), in Germany, more than 150 different cannabis flowers can be prescribed. However, it is largely unknown, whether particular strains and/or different concentrations of THC, CBD, other cannabinoids, and further ingredients, including terpenes and flavonoids, result in different effectiveness in different conditions.
So far, only a limited number of studies directly compared the effects of different cannabis strains in different indications 2 3 4 5 6 7 . According to data collected between 2009 and 2010 from 600 patients registered with the Vancouver Island Compassion Society and treated with medicinal cannabis (MC), the “more popular” Cannabis indica strains more effectively relieved pain compared to C. sativa strains 2 . Several characteristics were found to be similar for both species, e. g., trust in purity, route of administration, and reason for use (recreational vs. medicinal).
A study from the Netherlands, also published in 2014, explored patients’ views (n=102, in 76% use of cannabis flowers>1 year) on different cannabis strains, particularly with respect to concentrations of THC and CBD 4 . The most common indications for the use of cannabis flowers were chronic pain (53%) and multiple sclerosis (23%). Overall, 86% of patients were satisfied with the treatment. The higher the THC content the more often cannabis strains were used: (i) the high THC dominant strain Bedrocan (THC:CBD=22:<1) in 47.1%, (ii) the medium-high THC dominant strain Bedrobinol (THC:CBD=12:<1) in 28.4%, and (iii) the low THC balanced strain Bediol (THC:CBD=6:7.5) in 24.5%. Interestingly, no differences were detected between different strains with respect to dose and therapeutic satisfaction. However, high THC/low CBD strains caused increased appetite and higher levels of dejection and anxiety compared with the low THC/high CBD product.
Another study (n=837) investigating differences between different cannabis strains was conducted in Canada and published in 2017 7 . According to participants’ judgment, the balanced strain Midnight (8–11% THC, 11–14% CBD) was most effective for the management of pain, sleep, lack of appetite, and regulation of bowel function, whereas the THC dominant sativa strain Luminarium (25–28% THC, 0% CBD) was found to be the most effective to improve anxiety and depression and to regulate sexual problems. Improvement in concentration was attributed to the strain Cognitiva (13–17% THC, 0–0.5% CBD).
In 2018, an anonymous survey (n=455) on strain preferences was conducted in New England/USA 3 . At that time, a total of 1,987 strains were listed, of which 52% were hybrids, 29% were C. indica , and 19% C. sativa . The most common indications (multiple answers possible) were back/neck pain (60.3%), neuropathic pain (29.2%), posttraumatic stress disorder (PTSD, 26.4%), pain following trauma (18.6%) or surgery (16.5%), abdominal pain (13.5%), and cancer pain (1.9%). Interestingly, preferences were highly state/dispensary-specific. Many patients reported a time-dependent pattern with sativa use during the day and indica use at nighttime, and to improve sleep. In general, hybrid strains and C. indica were more commonly used than C. sativa . Determining if particular strains are perceived as more effective for particular conditions, the authors found very preliminary trends suggesting the hybrid strain Blue Dream for chronic pain, the hybrid strain Medibud for PTSD, and the Indica strain Mother of Berries (M.O.B.) for sleep.
Also, in 2018, data from the US were obtained from an electronic survey of MC patients (n=2,032) with various pain conditions 5 . Altogether, 42 different strains were preferred by patients, including C. indica , C. sativa , and hybrid strains, all with high THC/low CBD, as well as 3:1 and 1:1 CBD:THC strains. However, hybrid strains were most preferred by pain patients, and in particular, the strain OG Shark (with high THC/tetrahydrocannabinolic acid (THCA), low CBD/cannabidiolic acid (CBDA) and predominant terpenes β-caryophyllene and β-myrcene) 5 .
Using the mobile device software ReleafApp, in 2019, data from an observational study including 3,341 MC patients were collected in New Mexico/USA between 06/2016–05/2018 8 . Remarkably, flowers were not only the most commonly used CBM but also perceived as more efficacious than other CBMs. High THC strains, as well as C. indica (compared to C. sativa ), were reported to be more effective.
In a Canadian study published in 2021, data from 991 people were collected retrospectively via an app who used MC specifically for the management of insomnia 6 . Although all strain categories were perceived as efficacious, predominant indica strains were found to reduce insomnia symptomology more than CBD strains and predominant sativa strains.
The aim of this study was to present the basic characteristics of patients using MC from pharmacies prescribed by physicians in Germany and to determine if particular strains are perceived as more efficacious for particular conditions. In addition, we were interested in the kind and frequencies of indications, treatment duration, preferred strains, THC:CBD ratios, reimbursement rate by health insurance, and patients’ impressions with respect to taste, smell, side effect profile, and price-performance ratio. Our main research hypothesis was that different MC strains are differently effective in different indications.
Materials and Methods
Inclusion Criteria and Recruitment
We conducted an online survey in German language between 06/2020 and 08/2020. People fulfilling the following inclusion criteria were asked to participate: (i) age≥18 years, (ii) treatment with MC (alone or in combination with other CBM), (iii) indication for MC treatment confirmed by a physician, (iv) MC prescribed by the treating physician, and (v) use of MC from a German pharmacy. Patients with any indication were allowed to participate independently of whether costs for treatment were covered by the health insurance.
Patients were recruited from the clinic and practice of some of the authors (KMV, FG) through online newsletters of the German Association for Cannabis as Medicine (ACM), via German advocacy groups, social media, and specialized pharmacies. Data were collected exclusively online using SoSciSurvey (version 3.2.14i). Access was provided by the Hannover Medical School (MHH) in accordance with data protection laws. The study was approved by the Ethical Board at MHH (no. 9009_BO_K_2020).
Survey
The survey was composed of three parts: (i) information on previous MC use, including all previous and current indications and types of strains; (ii) information on current use, including main indication, type of strain(s), and dosing scheme. If a patient currently used MC for the treatment of different diseases (or symptoms), we asked to answer for the current main indication. We choose an effectiveness measure to reflect the patients’ perspective best. The outcome measure could be given as a number between 0% and 100% (scroll bar, 0%=“no effect”, 100%=“optimal effect/symptom free”). In the next step, we asked for the currently used cannabis strain(s). If more than one strain was currently used, participants were asked to answer all upcoming questions for the two mainly used strains separately. Finally, we asked about different related aspects, including side effects, costs, and cost coverage by insurance as well as smell and taste; and (iii) participants’ quality of life and sociodemographic profile. An overview of strains included in the study (n=43) is presented in Supplementary Table 1 .
Statistical Analyses
Power calculation (GPower 3.1) resulted in a minimum sample size of n=504. Statistical analysis was conducted with R software, version 3.6.3 (2020–02–29). For comparison of the effectiveness of different strains, we applied A-NOVA analysis, while we used multiple linear regression to establish the relationship between patients’ reported effectiveness and cannabis strains. To evaluate the relationship between the specific indication for MC use and the type of MC strain, we applied multinomial logistic regression. THC and CBD concentrations were evaluated according to the information provided by ACM and the German Pharmacy Apotheke Lux 99.
Results
Out of 1,621 people who opened the questionnaire, 1,028 completed the survey and were included in the analyses (n=856 males (83.3%), mean age 39.9 (+/-11.8) years, for further characteristics, see Table 1 ). While 65% of participants reported use of MC prescribed by a physician for≥1 year, 46% of participants reported a treatment period of>5 years if previous cannabis self-medication is also taken into consideration (for further details, see Table 1 ).
Table 1 Demographic characteristics of participants and duration of cannabis treatment, including self-medication as well as treatment duration for medicinal cannabis (MC) prescribed by physicians (N=1,028).
| Variable | N of participants (%) | ||
|---|---|---|---|
| All (mean age, SD [years]) | 1028 (100%) (39.9, 11.8) | ||
| Male sex | 856 (83.3%) | ||
| Country of origin | Germany | 1017 (98.9%) | |
| Austria | 5 (0.5%) | ||
| Switzerland | 1 (0.1%) | ||
| Other | 5 (0.5%) | ||
| Education | Primary education | 160 (16%) | |
| Lower secondary | 160 (16%) | ||
| Upper secondary | 349 (34%) | ||
| Postsecondary | 237 (23%) | ||
| University | 214 (21%) | ||
| Other | 43 (4%) | ||
| Treatment duration | MC use, including self-medication | MC from pharmacy prescribed by physicians | |
| <1 month | 11 (1%) | 41 (4%) | |
| 1–12 months | 133 (13%) | 319 (31%) | |
| 1–5 years | 417 (41%) | 596 (58%) | |
| 6–10 years | 204 (20%) | 68 (7%) | |
| >10 years | 263 (26%) | 4 (0%) | |
MC – medicinal cannabis, SD – standard deviation.
Altogether, 3,728 diagnoses (multiple answers possible, median=3.0, mean=3.6+/- 2.9, range, 1–19) were given for those whom MC treatment has ever been used. The most frequently selected indications (for both recent and current use) belonged to the following four diagnostic categories: pain conditions, psychiatric disorders, neurological disorders, and gastrointestinal problems ( Fig. 1 ). Concerning specific diagnoses ever treated with MC, the following diagnoses were most commonly mentioned (all mentioned>100 times, in descending order): musculoskeletal pain, chronic neuropathic pain, headache, migraine, depression, sleep disorders, attention-deficit/hyperactivity disorder (ADHD), anxiety disorder, PTSD, and irritable bowel syndrome. When being asked about the current main indication for MC use, the following specific diagnoses were indicated most commonly (all mentioned>100 times; the 10 most common are listed in descending order (for further details, see Supplementary Table 1 ): ADHD, musculoskeletal pain, chronic pain with somatic and psychological factors, migraine and other headaches, neuropathic pain, PTSD, depression, sleeping problems, restless legs syndrome (RLS), and fibromyalgia.
Fig. 1.
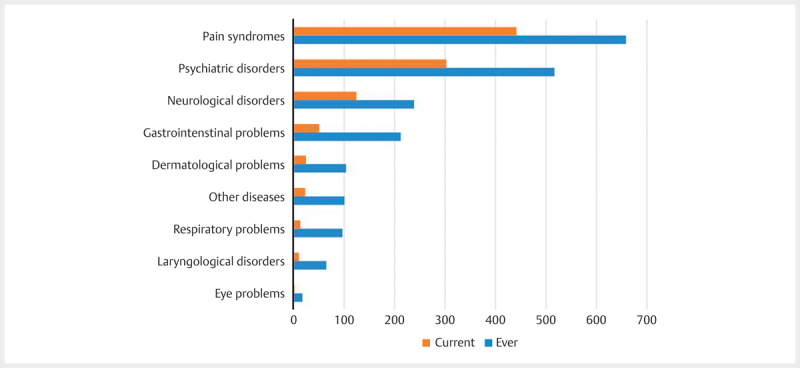
Self-reported indications for use of medicinal cannabis (MC) grouped by disease categories and treatment time (ever versus current; N=1,028 patients). Multiple answers only possible for ever.
Of 43 MC strains given for selection, only eight strains were chosen “frequently” (defined as being selected>30 times). On average, participants stated having used 5.9 different strains (SD=5.1, range, 1–36) with Bedrocan being by far the most frequently chosen strain (both ever used=750 times and currently used=285 times) followed by Bakerstreet (512 vs. 133), Pedanios 22/1 (480 vs. 105), Pedanios 20/1 (365 vs. 52), Red no 4 (389 vs. 42), Penelope (263 vs. 48), Pedanios 18/1 (256 vs. 43), and Red no 2 (322 vs. 42) (for further details consult Fig. 2 ). Altogether, 676 (66%) participants indicated currently using two different MC strains encompassing the same eight strains as mentioned above.
Fig. 2.
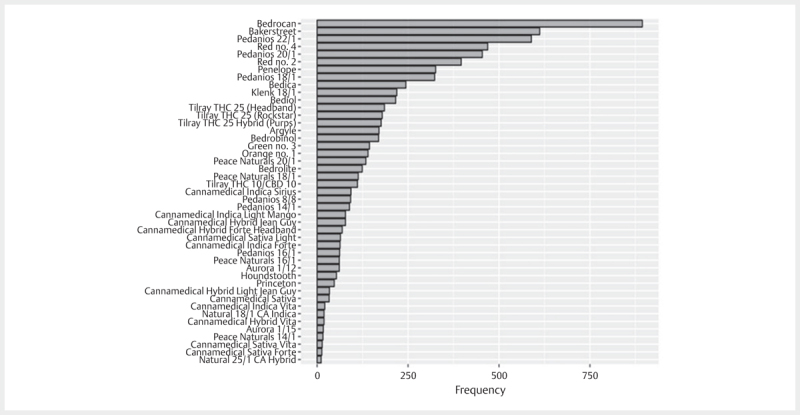
Frequencies of “ever use” of different cannabis strains (on average: 5.9 different strains) reported by N=1,028 patients (total mentionings: N=6041).
Considering THC and CBD concentrations, 34/43 (79%) were THC dominant, 6/43 (14%) were balanced products with equivalent THC:CBD ratios, and only 3/43 (7%) were CBD dominant strains. Among the eight “frequently” selected strains, seven had high THC concentrations (16%–22%), one was a balanced strain, and none were CBD dominant (see Supplementary Figure 1 ).
With respect to cannabis subspecies, 16/43 (37.2%) were hybrid strains, 15/43 (34.9%) were indica- and 10/43 (23.3%) sativa -based flowers (n=4 (9.3%) unknown category). Of those eight strains “frequently” used, four (50%) were C. indica , two (25%) were C. sativa , and two (25%) hybrid strains.
For the first- and second-choice MC strains, mean effectiveness was rated as being 80.1% (range, 6–100%) and 79% (range, 8%-100%), respectively, on a scale ranging from 0% (=no effect) to 100% (=optimal effect/symptom-free). Overall, for the eight most frequently chosen strains, no differences were detected with respect to patient-reported effectiveness (Supplementary Fig. 2 ).
Using a regression model looking for an association between patient-reported effectiveness and particular MC strains, we included the 14 most frequently ever reported indications for MC treatment (in descending order: musculoskeletal pain, depression, sleeping problems, chronic pain with somatic and psychological factors, neuropathic pain, ADHD, anxiety, migraine and other headaches, PTSD, irritable bowel syndrome, RLS, fibromyalgia, other pain syndromes) as well as five clustered categories based on these 14 indications (in descending order: pain, ADHD, psychiatric disorders, musculoskeletal symptoms, and chronic intestinal immune disorders) and the eight “frequently” used MC strains. In none of these analyses, an association between patient-reported effectiveness and particular MC strains was detected. Furthermore, the respective indication had no influence on the choice of the MC strain.
On average, participants reported 2.1 side effects (range, 0–12), but 29% of participants did not report any side effects. All in all, 1,028 participants listed 1,946 side effects for the first-choice strain, and 676 participants reported 1,245 side effects for the second-choice strain. For both the first- and the second-choice strain, the most commonly reported side effects were dry mouth (19.5%), increased appetite (17.1%), tiredness (13.0%), red eyes (12.4%), sleepiness (7.5%), and euphoria (6.5%). A summary of all reported side effects is presented in Table 2 .
Table 2 Self-reported side effects (multiple answers possible, in descending order, N=1,028).
| Side effect | N (%) |
|---|---|
| Dry mouth | 396 (20.3%) |
| Increased appetite | 364 (18.7%) |
| Red eyes | 240 (12.3%) |
| Tiredness | 225 (11.6%) |
| Euphoria | 131 (6.7%) |
| Sleepiness | 122 (6.3%) |
| Concentration problems | 74 (3.8%) |
| Thinking problems | 64 (3.3%) |
| Tiredness | 48 (2.5%) |
| Problems with attention | 47 (2.4%) |
| Gait problems | 35 (1.8%) |
| Reduced appetite | 26 (1.3%) |
| Hypotonia | 26 (1.3%) |
| Balance problems | 19 (1.0%) |
| Vertigo | 13 (0.7%) |
| Headache | 8 (0.4%) |
| General sensation of worsened health | 8 (0.4%) |
| Mood problems | 6 (0.3%) |
| Nausea | 5 (0.3%) |
| Diarrhea | 5 (0.3%) |
| Problems with sight | 5 (0.3%) |
| Vomiting | 2 (0.1%) |
In general, the taste and smell of MC strains were predominantly perceived as good or very good (n=730, 71.1%). Only a small proportion of participants (n=51, 5%) rated the currently used MC strains as bad or very bad with respect to taste and smell.
The price-performance ratio was rated as medium (23%), poor (20%), or very poor (21%), and only 309 participants (30%) were satisfied with the price-performance ratio (good: n=220 (21.4%), and very good: n=89 (8.6%)). Only 398/1,029 participants (38.7%) indicated that costs for MC treatment were fully or partially covered by their health insurance, 277 participants (27%) reported that an insurance verification request is currently being reviewed, and 353 participants (34.3%) stated not having submitted an application to the health insurance.
Discussion
We failed to confirm our main hypothesis that specific cannabis strains are more efficacious in specific indications. There was also no influence of the respective indication on the choice of the MC strain. Besides one strain, all strains preferred by participants were THC dominant with high THC concentrations. Self-reported effectiveness and tolerability of MC for the treatment of a variety of medical conditions were rated as excellent, with no relevant differences between C. sativa , indica , or hybrid. The majority of patients had used cannabis as a self-medication as well as MC prescribed by physicians for years. The overall profile of smell and taste was rated as very good. On the other hand, average cost-effectiveness was rated as poor, which is probably because the majority of patients did not get cost coverage from their health insurance.
This is the first large study exploring the effectiveness and tolerability of different cannabis strains prescribed by physicians in Germany. Previous studies demonstrated conflicting results 2 3 5 7 9 10 11 12 13 14 , but also differed in many ways with respect to the country studied, legality, access, costs, number and kind of available MC strains, standardization, characterization, and labeling of strains as well as the inclusion of patients using recreational cannabis as self-medication 2 3 15 .
In this study, we failed to show any relationship between MC strains and effectiveness in specific indications. Participants were able to select among 48 different conditions (clustered in 10 categories) for which MC had been used. When asked for conditions for which MC had ever been used, 45 conditions were marked, while currently MC was used for the treatment of 40 different disorders. Thus, in contrast to most recent studies 5 16 3 ] , in this study, participants with an extremely wide spectrum of disorders have been included.
In line with most recent studies 17 19 20 21 21 , we found that in Germany in 2020, MC is most commonly prescribed for different pain conditions, followed by psychiatric and neurological disorders. When looking at specific diagnoses according to ICD-10, however, ADHD was the most common current condition for MC, followed by different pain conditions (musculoskeletal pain, chronic pain with somatic and psychological factors, migraine, and other forms of headache, and neuropathic pain), three further psychiatric disorders (PTSD, depression, and sleep disorders), and RLS. This result is more remarkable since the database - and guidelines and treatment recommendations, respectively - for these different indications largely differ. While it is well known that a large number of patients with ADHD self-medicate with cannabis 22 , the database is weak, and so far, only one small controlled trial has been performed. Accordingly, most experts do not recommend CBM for the treatment of ADHD 23 . A similar situation can be found in all other commonly indicated psychiatric indications 24 . In contrast, in chronic pain several randomized controlled studies have been performed that clearly demonstrate the effectiveness of CBM in different pain conditions 23 25 . With respect to the most frequently used MC strains, seven out of eight “frequently” prescribed strains were THC dominant, with a THC content ranging between 16 and 22%. This finding is in line with patients’ reports and clinical trials. For example, patients with ADHD, in general, prefer CBM with high THC concentrations 22 . In a recent systematic review, it could be demonstrated that in patients with chronic pain, CBM with high THC-to-CBD ratios is more effective compared to CBM with comparable or low ratios .
By far, the most commonly prescribed cannabis flower was Bedrocan . This might be because Bedrocan was the first THC-dominant cannabis flower that became available for legal use for medicinal purposes in Germany (in 2007), and that supply bottlenecks occurred less frequently compared to most other products. Accordingly, Bedrocan is well-established in the German market. Alternatively, it can be speculated that the effectiveness and tolerability of Bedrocan are indeed superior compared to other THC-dominant strains with a similar THC:CBD ratio, which might be related to the specific type and terpene profile. The predominant terpenes in this sativa strain are β-myrcene, terpinolene, and cis-ocimen. However, in another large study including 2,032 patients with different pain syndromes, in contrast, the hybrid strain OG Shark containing predominantly the terpenes β-caryophyllene and β-myrcene was most preferred 5 , whereas according to a web survey, C. indica was preferred for pain control 2 . Based on this data, it seems unlikely that the type of MC ( sativa , indica , or hybrid) or the terpene profile influences effectiveness since in general, β-myrcene is the most prevalent terpene in MC 26 . Similarly, it seems to be unlikely that taste and smell had a relevant impact, since most of the participants rated taste and smell as good or very good. Although a substantial number of patients indicated that costs for MC treatment are not covered by their health insurance, we do not believe that costs significantly influenced the choice of MC. If costs are reimbursed by statutory health insurances, prices of MC from pharmacies are controlled by the German drug price regulation for prescription drugs, and therefore, do not differ significantly between different products and companies (at the time of the survey, on average, about € 17/g). Although prices may differ, if patients have to pay from their private funds, none of the strains included in this survey was much cheaper compared to others for a longer time period (at the time of the survey, on average, about € 19/g). Compared to street cannabis . Financial burden compared to street cannabis is relatively high, since at that time, average costs for street cannabis were about € 10/g.
This study has several strengths, including (i) a large sample size, (ii) a relatively short recruitment time, (iii) inclusion of only patients that used MC from pharmacies prescribed by physicians, (iv) patients with a wide spectrum of different indications, (v) relatively long time use of MC, and (vi) use of 5.9 different MC strains on average allowing comparison with respect to clinical effectiveness. However, the following limitations have to be addressed: (i) only German-speaking patients could be included, (ii) most participants came from Germany, and thus data represent only a small geographical region, (iii) only data for MC strains available in German pharmacies in 2020 could be collected; (iv) data were collected online based on self-reported diagnoses and treatment effects, (v) it cannot entirely be excluded that participants provided untruthful information. However, due to our recruitment strategy, we believe that most participants were highly motivated to further increase knowledge about the effects of MC, (vi) it has been suggested that long-term use of cannabis for medicinal purposes may cause cannabis use disorder (CUD) mainly in patients with “dual motives use” (medicinal and recreational use) and those who use illicit cannabis products 27 28 . In this study, however, we included only patients who reported medicinal use of cannabis prescribed and supervised by a physician. Since it was beyond the aim of this study, we did not ask for the current use of illicit cannabis products and did not include a questionnaire for CUD. Thus, we cannot entirely exclude that a proportion of participants used cannabis (at least in part) to substitute their CUD, and (vii) it cannot be excluded that mainly patients with beneficial effects of MC participated.
Contributors
KMV, FG, FH, and EB contributed to the conception and design of the study, organization of the database, collection, analysis, and interpretation of data. EB conducted the collection of the data, the organization of the database, and the statistical analysis, which was also the part of her master’s thesis. NS and KMV wrote the first draft of the manuscript. All authors contributed to the manuscript revision and approved the submitted version.
Acknowledgement
We acknowledge all patients who kindly participated in this trial.
Conflict of Interest Kirsten Müller-Vahl has received financial or material research support from EU (FP7-HEALTH-2011 No. 278367, FP7-PEOPLE-2012-ITN No. 316978), DFG: GZ MU 1527/3-1 and GZ MU 1527/3-2, BMBF: 01KG1421, National Institute of Mental Health (NIMH), Tourette Gesellschaft Deutschland e.V., Else-Kröner-Fresenius-Stiftung, GW pharmaceuticals, Almirall, Abide Therapeutics, Emalex Biosciences, Inc., Noema Pharma, CannaXan, and Therapix Biosiences. She has received consultant's and other honoraria from Abide Therapeutics, adjupharm, Alexion, AMP Alternative Medical Products GmbH, Ingelheim International GmbH, Bionorica Ethics GmbH, CannaMedical Pharma GmbH, Canopy Grouth, Columbia Care, CTC Communications Corp., Demecan, Enua pharma, Ethypharm GmbH, Eurox Group, Global Praxis Group Limited, Hormosan Pharma GmbH, Lundbeck, MCI Germany, Neuraxpharm, Noema Pharma, Sanity Group, Stadapharm GmbH, Synendos Therapeutics AG, Syqe, Tilray, and Zambon. She is an advisory/scientific board member for Alexion, Branchenverband Cannabiswirtschaft e.V. (BvCW), CannaMedical Pharma GmbH, Bionorica Ethics GmbH, CannaXan GmbH, Canopy Growth, Columbia Care, Ethypharm GmbH, Hormosan Pharma GmbH, IMC Germany, Leafly Deutschland GmbH, Neuraxpharm, Sanity Group, Stadapharm GmbH, Synendos Therapeutics AG, Syqe Medical Ltd., Therapix Biosciences Ltd., and Tilray. She has received speaker’s fees from Agaplesion Frankfurter Diakonie Kliniken gemeinnützige GmbH, Almirall, Aphria Deutschland GmbH, Arbeitsgemeinschaft Cannabis als Medizin (ACM), Astra Zeneca, Bedrocan, Branchenverband Cannabiswirtschaft e.V. (BvCW), Camurus, canymed GmbH, CEREBRO SPAIN BIDCO S.L, Cogitando GmbH, Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde (DGPPN), Diplomado Internacional de Endocannabinología (Programa Universitario de Investigación en Salud - PUIS, UNAM), Dresden International University (DIU), Emalex, Eurox Deutschland GmbH, Ever pharma GmbH, Georgia Medical Cannabis Project (GMCP), GROW, Hessische Landesstelle für Suchtfragen e.V. (HLS), LIO Pharmaceuticals GmbH, Medizinischer Dienst Westfalen Lippe, Meinhardt Congress GmbH, PR Berater, Spectrum Therapeutics GmbH, Swiss Alpinopharm, targoEvent GmbH, Takeda GmbH, Tilray, von Mende Marketing GmbH, and Wayland Group. She has received royalties from Deutsches Ärzteblatt, Der Neurologie und Psychiater, Elsevier, Medizinisch Wissenschaftliche Verlagsgesellschaft Berlin, and Kohlhammer. She served as a guest editor for Frontiers in Neurology on the research topic “The neurobiology and genetics of Gilles de la Tourette syndrome: new avenues through large-scale collaborative projects”, is an associate editor for “ Cannabis and Cannabinoid Research” and an Editorial Board Member of “Medical Cannabis and Cannabinoids” und “MDPI-Reports” and a Scientific board member for “Zeitschrift für Allgemeinmedizin”. FG has received fees for consulting or speaking engagements from the following companies active in the cannabis field:Bionorica SE, Canify A/S , CannaXan, Demecan Holding GmbH, Drapalin Pharmaceuticals GmbH , Four 20 Pharma GmbH, GECA Pharma GmbH, Heyday AG, Materia Deutschland, Medican Pharma GmbH, MYCB1, Nature Bloom GmbH, Neuraxpharm, Oxygen Handel GmbH, Spectrum Therapeutics GmbH, STADA Arzneimittel AG, Storz & Bickel GmbH & Co. KG, Swiss Organic Partners AG, THC Pharm GmbH, Vayamed GmbH FH has received consultant's and other honoraria from, Adjurpharm GmbH, Aurora Deutschland GmbH, Avextra, Dialectia, Columbia Care UK, Curaleaf, Dr. Reddeys, Enua, Ethypharm, Eumara, FAT-Moves UG, Grow Deutschland GmbH, Neuraxpharm, Nimbus Health GmbH, PR Berater, Remexian Pharma GmbH, Simon-Kucher and Partners, Stadapharm GmbH, Tilray Deutschland GmbH. He has received speaker’s fees from Canopy Growth Germany GmbH, Ethypharm, G. Pohl-Boskamp GmbH& Co. KG, INSIGHT Health GmbH, Medios AG, Neuraxpharm, Zambon GmbH EB worked for Anquor Pharmaceuticals between January 2020 to March 2020. NS has received financial and material research support by the research grant of the Medical University of Warsaw, Polish Ministry of Health, Polish Neurological Society, Foundation for Polish Research, European Stroke Organization, American Academy of Neurology, American Brain Foundation and Tourette Association of America. She has received honoraria from Biogen and 90 Consulting.
shared first authorship: N. Szejko, E. Becher
these two authors contributed equally: F. Grotenhermen, K. R. Müller-Vahl
Supplementary Material
References
- 1.Legare C A, Raup-Konsavage W M, Vrana K E. Therapeutic potential of cannabis , cannabidiol, and cannabinoid-based pharmaceuticals Pharmacology. 2022107131–149.Available from:www.karger.com/pha [DOI] [PubMed] [Google Scholar]
- 2.Pearce D D, Mitsouras K, Irizarry K J. Discriminating the effects of Cannabis sativa and Cannabis indica: A web survey of medical cannabis users Available from:www.liebertpub.com [DOI] [PubMed]
- 3.Piper B J. Mother of berries, ACDC, or chocolope?: Examination of the strains used by medical cannabis patients in New England J Psychoactive Drugs 20185095Available from:/pmc/articles/PMC6275121/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Brunt T M, van Genugten M, Höner-Snoeken K et al. Therapeutic satisfaction and subjective effects of different strains of pharmaceutical-grade cannabis. J Clin Psychopharmacol. 2014;34:344–349. doi: 10.1097/JCP.0000000000000129. [DOI] [PubMed] [Google Scholar]
- 5.Baron E P, Lucas P, Eades Jet al. Patterns of medicinal cannabis use, strain analysis, and substitution effect among patients with migraine, headache, arthritis, and chronic pain in a medicinal cannabis cohort Available from:https://doi.org/10.1186/s10194-018-0862-2 [DOI] [PMC free article] [PubMed]
- 6.Kuhathasan N, Minuzzi L, MacKillop Jet al. The use of cannabinoids for insomnia in daily life: Naturalistic study J Med Internet Res 20211423Available from:/pmc/articles/PMC8581757/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wan B A, Diaz P, Blake A et al. Efficacy of different varieties of medical cannabis in relieving symptoms . J Pain Manage. 2017;10:375–383. [Google Scholar]
- 8.Stith S S, Vigil J M, Brockelman Fet al. The Association between cannabis product characteristics and symptom relief Sci Rep 2019159Available from:https://pubmed.ncbi.nlm.nih.gov/30804402/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brunt T M, van Genugten M, Höner-Snoeken Ket al. Therapeutic satisfaction and subjective effects of different strains of pharmaceutical-grade cannabis J Clin Psychopharmacol 201434344–349.Available from:https://pubmed.ncbi.nlm.nih.gov/24747979/ [DOI] [PubMed] [Google Scholar]
- 10.Abuhasira R, Schleider LB L, Mechoulam Ret al. Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly Eur J Intern Med [Internet 20184944–50.Available from:http://www.ejinme.com/article/S0953620518300190/fulltext [DOI] [PubMed] [Google Scholar]
- 11.Rosenthal M S, Pipitone R N.Demographics, perceptions, and use of medical marijuana among patients in Florida Med Cannabis Cannabinoids 2021413–20.Available from:https://www.karger.com/Article/FullText/512342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brown J D, Costales B, van Boemmel-Wegmann Set al. Characteristics of older adults who were early adopters of medical cannabis in the Florida Medical Marijuana Use Registry J Clin Med 202091166Available from:https://www.mdpi.com/2077-0383/9/4/1166/htm [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Reinarman C, Nunberg H, Lanthier Fet al. Who are medical marijuana patients? Population characteristics from nine California assessment clinics J Psychoactive Drugs 201143128–135.Available from:https://www.tandfonline.com/doi/abs/10.1080/02791072.2011.587700 [DOI] [PubMed] [Google Scholar]
- 14.O’Connell T J, Bou-Matar C B. Long term marijuana users seeking medical cannabis in California (2001-2007): Demographics, social characteristics, patterns of cannabis and other drug use of 4117 applicants Harm Reduct J 200741–7.Available from:https://harmreductionjournal.biomedcentral.com/articles/10.1186/1477-7517-4-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Boehnke K F, Scott J R, Litinas Eet al. Cannabis use preferences and decision-making among a cross-sectional cohort of medical cannabis patients with chronic pain J Pain 2019201362–1372.Available from:https://pubmed.ncbi.nlm.nih.gov/31132510/ [DOI] [PubMed] [Google Scholar]
- 16.Belendiuk K A, Babson K A, Vandrey Ret al. Cannabis species and cannabinoid concentration preference among sleep-disturbed medicinal cannabis users Addict Behav 201550178–181.Available from:https://pubmed.ncbi.nlm.nih.gov/26151582/ [DOI] [PubMed] [Google Scholar]
- 17.Shiplo S, Asbridge M, Leatherdale S Tet al. Medical cannabis use in Canada: Vapourization and modes of delivery Harm Reduct J 2016131–10.Available from:https://harmreductionjournal.biomedcentral.com/articles/10.1186/s12954-016-0119-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kosiba J D, Maisto S A, Ditre J W. Patient-reported use of medical cannabis for pain, anxiety, and depression symptoms: Systematic review and meta-analysis Soc Sci Med 2019233181–192.Available from:https://pubmed.ncbi.nlm.nih.gov/31207470/ [DOI] [PubMed] [Google Scholar]
- 19.Bar-Lev Schleider L, Mechoulam R, Sikorin I et al. Adherence, safety, and effectiveness of medical cannabis and epidemiological characteristics of the patient population: A prospective study . Front Med (Lausanne) 2022;9:827849. doi: 10.3389/fmed.2022.827849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Whiting P F, Wolff R F, Deshpande Set al. Cannabinoids for medical use: A systematic review and meta-analysis JAMA 20153132456–2473.Available from:https://pubmed.ncbi.nlm.nih.gov/26103030/ [DOI] [PubMed] [Google Scholar]
- 21.Zürcher K, Dupont C, Weber Pet al. Use and caregiver-reported efficacy of medical cannabis in children and adolescents in Switzerland Eur J Pediatr 2022181335–347.Available from:https://link.springer.com/article/10.1007/s00431-021-04202-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stueber A, Cuttler C. Self-reported effects of cannabis on ADHD symptoms, ADHD medication side effects, and ADHD-related executive dysfunction 202126942–955.Available from:https://journals.sagepub.com/doi/abs/10.1177/10870547211050949?src=getftr&journalCode=jada [DOI] [PubMed] [Google Scholar]
- 23.Francisco A P, Lethbridge G, Patterson B et al. Cannabis use in attention – deficit/hyperactivity disorder (ADHD): A scoping review . J Psychiatr Res. 2023;157:239–256. doi: 10.1016/j.jpsychires.2022.11.029. [DOI] [PubMed] [Google Scholar]
- 24.McKee K A, Hmidan A, Crocker C E et al. Potential therapeutic benefits of cannabinoid products in adult psychiatric disorders: A systematic review and meta-analysis of randomised controlled trials. J Psychiatr Res. 2021;140:267–281. doi: 10.1016/j.jpsychires.2021.05.044. [DOI] [PubMed] [Google Scholar]
- 25.McDonagh M S, Morasco B J, Wagner Jet al. Cannabis -based products for chronic pain: A systematic review Ann Intern Med 20221751143–1153.Available from:https://www.acpjournals.org/doi/10.7326/M21-4520 [DOI] [PubMed] [Google Scholar]
- 26.Russo E B, Marcu J.Cannabis pharmacology: The usual suspects and a few promising l eads Adv Pharmacol 20178067–134.Available from:https://pubmed.ncbi.nlm.nih.gov/28826544/ [DOI] [PubMed] [Google Scholar]
- 27.Mills L, Lintzeris N, O’Malley Met al. Prevalence and correlates of cannabis use disorder among Australians using cannabis products to treat a medical condition Drug Alcohol Rev 2022411095–1108.Available from:https://onlinelibrary.wiley.com/doi/full/10.1111/dar.13444 [DOI] [PubMed] [Google Scholar]
- 28.Marie NS G, Taisir R, Sousa S et al. Prevalence of cannabis use disorder among individuals using medical cannabis at admission to inpatient treatment for substance use disorders . Addict Behav. 2023;142:107667. doi: 10.1016/j.addbeh.2023.107667. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.