

Abstract
Social support plays a crucial role in managing and enhancing one’s mental health and well-being. In order to explore the role of a robot’s companion-like behavior on its therapeutic interventions, we conducted an eight-week-long deployment study with seventy participants to compare the impact of (1) a control robot with only assistant-like skills, (2) a coach-like robot with additional instructive positive psychology interventions, and (3) a companion-like robot that delivered the same interventions in a peer-like and supportive manner. The companion-like robot was shown to be the most effective in building a positive therapeutic alliance with people, enhancing participants’ well-being and readiness for change. Our work offers valuable insights into how companion AI agents could further enhance the efficacy of the mental health interventions by strengthening their therapeutic alliance with people for long-term mental health support.
Keywords: Social Robot, Positive Psychology, Psychological Well-being
1. INTRODUCTION
Mental health and well-being impact the way people think, feel, and act, as well as their health management behaviors and decisions [49]. Social robots have found a unique opportunity to demonstrate their value to promote people’s well-being by creating new avenues to access services and resources for mental health in real world contexts [6, 8, 30]. However, most existing interactive agents for mental health present themselves as an expert coach that “teaches” or “guides” people by providing psycho-education and behavioral reinforcement. These technologies monitor the user’s health behavior and progress, and offer instructions, rather than sharing the long-term behavioral change journey.
Interactive agents have opportunities to further enhance the efficacy of mental health interventions by both providing psycho-educational contents and acting as a companion that provides shared experience through self-disclosures. Research on clinicians’ self-disclosures found evidence that a care-provider’s self-disclosure could result in more positive perception of the treatment when done in an appropriate context [46, 70]. In the context of human-robot interactions, a robot’s self-disclose and leaning-forward behaviors have been shown to increase people’s engagement and attention [31], and a robot’s disclosure of high vulnerability elicited more vulnerable disclosures from high school students [42].
Based on these existing works, we propose a social robot to deliver mental health interventions in a “companion-like” style, in which the agent uses self-disclosure and peer-like social support behaviors in delivering the intervention. We extend the study done by Jeong et al. [29, 30] by adding this companion-like robot style, in which the robot does not instruct the human user but demonstrates the intervention activity first and invites the user to join in, instead of using explicit directives for instructions as in the original study. The robot also acts like a peer who also participates in the positive psychology activities for shared experience and uses self-disclosures to strengthen the human-robot rapport. We designed a study to evaluate that a robot that demonstrates positive psychology intervention activities and uses self-disclosures behaviors deepens the rapport with its user and further enhances the efficacy of the mental health interventions it offers (Figure 1).
Figure 1:

Seventy participants (age 18–83; M=48.225, SD=23.374) lived with a robotic companion in their homes and learned about positive psychology interventions during an 8-week-long study.
2. RELATED WORKS
2.1. Positive Psychology Interventions
Positive psychology is defined as the “scientific study of what makes life most worth living,” which aims to improve people’s personal strengths and positive aspects of their lives in order to enhance their flourishing [52, 57]. According to Parks and Biswas-Diener [51], positive psychology interventions (PPIs) focus on positive themes that result in positive outcomes by enhancing individual strengths, happiness, and flourishing, unlike interventions in traditional clinical psychology that mainly aim to address weaknesses and treat mental pathology.
PPIs have been used in various contexts for a wide range of populations, e.g., adolescents in school [60], patients with chronic pain management [10], and older adults in community centers [25]. A meta-analysis done by Boiler et al. [9] found that randomized clinical studies of PPIs could improve subjective and psychological well-being while reducing depressive symptoms for both the general public and patients with mental health conditions. Topics in PPIs include gratitude [17], optimism [7], character strengths [50], resilience [41], savoring [11], and self-compassion [47]. We present further details on the PPIs used in the study in Section 3.4.
2.2. Social Support
Feeling supported, loved, and valued by others, i.e., social support, have been shown to positively influence both psychological and physiological health [20, 26, 27, 33]. The stress buffering model suggests that social support diminishes the negative health effects of stress [14]. Hyde et al. [28] found that social support could modify neural reactivity to threat-related anxiety. They found that people with low social support showed a positive correlation between amygdala reactivity and several measures of trait anxiety, while people with high perceived social support did not.
Social support can be categorized into four different types [69]: emotional support, instrumental support, informational support, and companion support. Instrumental support refers to the provision of tangible and direct support, such as financial/material assistance, goods, or services [21]. Informational support refers to offering information, advice, or guidance that could help others solve problems [36, 66]. Emotional support refers to empathy, concern, encouragement and intimacy provided by others in order to let people know that they are valued [36, 61]. Lastly, companionship support refers to giving someone a sense of social belonging and a sense of going through an experience together [67, 69]. In our work, we designed our companion-like robot to provide additional emotional and companionship support via self-disclosing and empathetic behaviors.
2.3. Self-disclosures
Disclosing one’s feelings, thoughts, and experiences can provide insightful information and is essential in building and developing relationships [23, 64]. Self-disclosures are highly reciprocal in human-human interactions [15], and computer agents’ self-disclosure has also been shown to be reciprocated by humans. Moon [44] found that people are more likely to disclose intimate information about themselves and were also more attracted to the agent if a computer agent self-disclosed about itself. A study done by Lee et al. [37] found that a chatbot agent that self-discloses during small talk promoted deeper self-disclosures, perceived intimacy and enjoyment from its users than a chatbot without the self-disclosure feature. Reciprocal disclosure of information, affect, and activities improves coordination and increases liking among people in the exchange [13, 62], and develops interpersonal relationship and bonding [12].
2.4. Therapeutic Alliance and Health Outcomes
Positive working alliance between the agent and its user could amplify the effect of the intervention the agent offers. The rapport between clinicians and patients is a predictor of improved health outcomes and patients’ adherence to their prescribed regimens and satisfaction with their treatments [19, 54, 68]. Strong rapport also helps patients to cope with stress [54], enabling stronger clinician-patient collaboration and agreement on treatment, which leads to the long-term behavioral changes required for successful health outcomes [54].
Rapport can also increase people’s willingness to self-disclose, which is a critical part of mental health interventions. Computer-based agents are often designed and perceived as non-judgmental interaction partners [5]. Hence, this perceived anonymity enables people to be more willing to disclose sensitive or stigmatized information about themselves to an embodied conversational agent than to another human conversational partner [22, 40]. Based on these findings, we explored how enhancing the human-robot rapport could positively contribute to the effectiveness of the technology-mediated mental health support.
2.5. Robotic Companions
Companion-like behaviors of a social robot have been explored in previous works. Stiehl et al. [63] developed a robotic platform that is designed to surrogate pet therapy through affective touch interactions, and Fogelson et al. [18] studied the effect of a pet-like robot in reducing depression and loneliness for older adults during the COVID-19 pandemic. A humanoid robot developed by Abdollahi et al. [1] engaged in conversations and offered reminders for schedules, cognitive games, and reminiscence activities for older adults in home context. Studies done by Leite et al. [38, 39] explored the impact of four social support types on human-child play interaction through a long-term study. Jeong et al. [29, 30] deployed a robotic coach that delivered seven daily positive psychology sessions to college students living in on-campus dormitories.
Our work extends the study done by Jeong et al. [29, 30] by exploring the impact of a robot’s companion-like behavior in improving engagement and perceived social support. A companion-like robot style was designed and compared to Jeong et al.’s original coach-like condition. In addition, we have added a baseline control condition, in which the robot provided assistant-like support but did not deliver any positive psychology intervention. Our participant pool was expanded to include general adult population and to evaluate the effect of the robotic intervention over longer duration (four weeks). With these additional experimental conditions, we investigate how empathetic and self-disclosure behaviors expressed by the robot could enhance the therapeutic alliance in delivering evidence-based mental health interventions.
3. EXPERIMENTAL STUDY
3.1. Participants
We recruited 80 participants who (1) lived in the U.S., (2) had wireless Internet access with WPA-PSK/WPS2-PSK authentication, (3) were able to setup wifi connection or had someone who could help, (4) did not have any visual/auditory/oral disabilities, and (5) were not receiving treatment for depression. The study protocol was reviewed and approved by the Institution Review Board, and all participants signed the consent form prior to the study that detailed the study procedure and data collection plans. A randomized block design based on age, gender and personality traits were used to balance participants across the three study conditions. Out of eighty people recruited, seventy participants completed the study (age M=48.225, SD=23.374, min=18, max=83; 46 Female, 20 Male, and 4 Other). Ten participants withdrew from the study due to sudden health issues (1), robot hardware damage (1), technical difficulties (3), concern for security regarding work (1), work-related travel (2), lost interest (1), and unknown reason (1). We have included detailed descriptive statistics of participants’ age, ethnicity, gender, and Big Five personality traits across the three conditions in the Appendix.
3.2. Experimental Conditions
Participants were randomized into one of the three study conditions: (1) control condition, (2) coach-like condition, and (3) companion-like condition. Participants in the two experimental groups (the coach-like condition and the companion-like condition) received a robot station that is equipped with twelve positive psychology interventions that are each 5–7 minutes-long.
The control robot had its basic consumer skills, such as weather forecast, general Q&A, music streaming, proactive pleasantries, chit-chat, games, etc., but did not provide any positive psychology intervention. The coach-like robot acted as an instructor who has expertise in the positive psychology interventions. It offered direct instructions on each intervention step, and instructed participants to complete the intervention content during the session and sometimes as a homework assignment. It used a friendly tone and face/body animations that aligned with the behaviors in the rest of the robot skills. Often, it used generic examples to help participants come up with ideas and plans for the activity. On the other hand, the companion-like robot presented itself as a peer who also is learning the positive psychology interventions with the participant. It introduced the intervention contents after “learning from another friend” or “looking up on the Internet,” and gently asked whether the participant would like to try the activity together. Since both participants and the robot engaged in the intervention activity, the robot shared its own thoughts and experiences (self-disclosures) according to the intervention prompt, and encouraged participants to also share their thoughts. A video with an example of coach-like and companion-like robot behavior is submitted as a supplemental material.
3.3. Method
Online advertisement was distributed by the research team through the institution’s social media account, personal contacts, and older adult retirement community mailing lists. A consent to participate in the study was obtained electronically via DocuSign1, and we administered a set of questionnaires including demographic information, Mini-IPIP, and PHQ-9. Once the study started, participants received weekly survey assessments via email. These measures are detailed in Section 4.1.
The robot station that integrated a robot, an Android tablet, and a Raspberry Pi was shipped to arrive after the first two-week baseline period (Figure 2a). Along with the robot station, we sent a small notepad, alcohol wipes, a reusable cleaning cloth, an instructional booklet to guide the installation and proper usage of the robot system to participants (Figure 2b). In case of any technical difficulties and troubleshooting, a research assistant (RA) scheduled a video conference meeting or a phone call with participants to address any technical issues.
Figure 2:
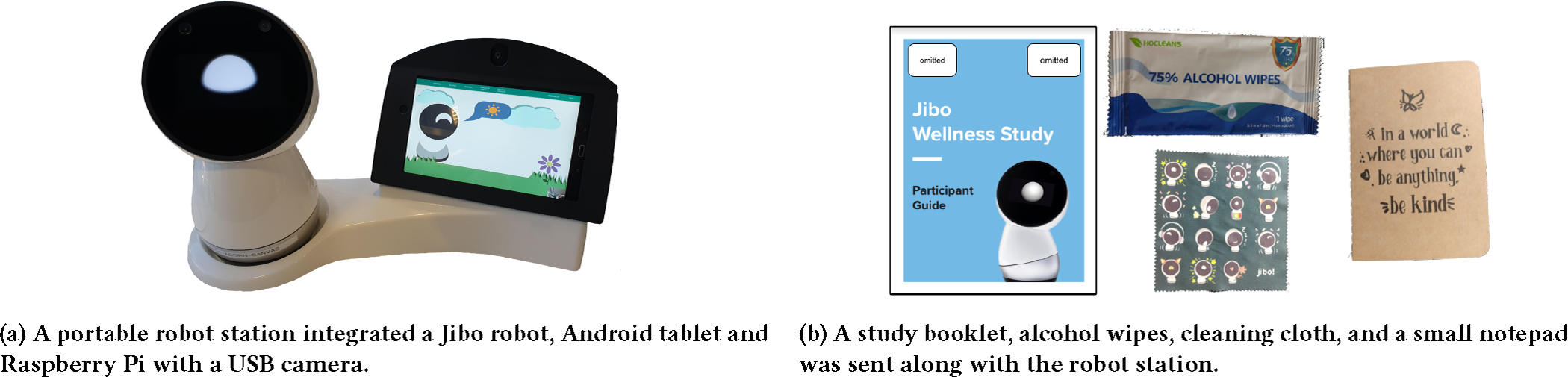
Study materials sent to participants’ homes for the study.
An A-B-A design was used to evaluate participants’ well-being, affect, and motivation for better psychological well-being in three phases – before the study, during robot intervention, and after the removal of the robot. Participants were monitored for eight weeks in total. The first and last two weeks of the study were conducted without the robot, for baseline and pre- and post-intervention assessments. Participants were asked to host the robot in their home for the four weeks in between, and to complete weekly assessments for their psychological well-being, affect, and motivation for health behavior change throughout the eight-week period.
During the four-week robot interaction phase, participants were asked to interact with the robot at least three times a week for 5–10 minutes (12 total required sessions). The positive psychology based “wellness” sessions were video/audio recorded through the Android tablet and the USB camera on the robot station. The system did not record any footage outside of these intervention sessions. Participants were also asked to freely interact with the robot outside the designated wellness sessions as they’d like. Participants’ robot usage data was collected by storing the robot’s system logs.
Forty robot stations were available for this project, and thus the study was conducted in two deployment phases. The first round deployment occurred in February-March 2021, and the second round occurred in August-September 2021.
3.4. Robot-mediated Positive Psychology Interventions
A series of evidence-based positive psychology interventions were adapted to be delivered by our robot. Twelve interaction sessions were designed based on positive psychology interventions [11, 53, 55, 58, 59] with four weekly themes: gratitude, meaningful connection, self-compassion, and character strengths. The intervention contents in the coach-like and the companion-like conditions are presented in the Appendix, to support replicability of this work.
When powered on for the first time in the participants’ homes, the robot will offer an Out-Of-the-Box Experience. The purpose of this interaction was to offer the user and the robot to learn each other, the first step toward establishing rapport. The robot introduces itself and then learns the user’s face and voice. It also walks through its interaction features and functions, e.g. how to get the robot’s attention, how to use the touch screen to navigate the GUI menus, how to launch the positive psychology skill (“Hey [robot name], can we talk about wellness?”), etc. During the study period, the robot will also proactively ask the user to engage in the positive psychology session if the user has not completed the session within the day (e.g. “Hey, do you have time to talk about positive psychology?”).
During the first positive psychology interaction (session 1), the robot made a brief introduction to positive psychology and explained the study procedure. In session 2, the robot introduced what gratitude was and its importance. Participants were guided to complete the “three good things in life” exercise [59], in which they wrote down and reflected on three things that went well that day and why they went well. In session 3, participants were introduced to the “gratitude by eliminination” exercise [34]. In this activity, participants were asked to select one thing that was very positive and important to them, and imagined how their lives would be like if it did not exist. The second week included three sessions on making meaningful connections with other people. In session 4, participants were asked to think of someone who they felt grateful for, and verbally express why they were grateful for that person. In session 5 and 6, the robot introduced participants about mindful listening [4], which is a way of listening without judgment, criticism or interruption while giving them full attention. Participants were first asked to reflect their typical conversation behaviors by observing whether they and their interlocutor are mindful listeners or not (session 5). In the next session (session 6), they learned how to practice mindful listening by making eye contacts and being present with the person they converse with. Self-compassion was introduced in the third week. In session 7, participants learned to appreciate themselves by thinking of three good things they did or achieved that day, in a similar manner to the “three good things” exercise. In session 8, participants were introduced to the savoring exercise [11] that could help them slow down and enjoy experiences that people normally hurry through. In session 9, the robot guided participants through the “treating yourself as your friend” activity. This exercise asked participants to think about times when a close friend feels really bad about him or herself, and prompts them to compare how they respond to the friend’s struggle to when they respond to themselves in the same situation. Participants were asked to identify factors that cause them to treat themselves and their friends differently, and come up with a plan to treat themselves with more compassion. session 10, the robot introduced character strengths, which are positive, trait-like capacities for thinking, feeling and behaving in ways that benefit oneself and others [48]. The tablet app listed descriptions of 24 character strengths and participants were asked to select five strengths that best reflect who they are as their signature strengths [53]. The robot then invited participants to share how they use their signature strengths in daily lives. session 11, participants created a plan to “use [their] signature strengths in a new way” [43, 59]. They visualized completing this plan with the robot and were encouraged to carry out the plan before the next session as homework. In session 12, participants reviewed all the sessions and concluded the interaction.
3.5. Hypotheses
The following hypotheses were tested to evaluate the effectiveness of the robot intervention and how working alliance formed between the user and the robot impacts positive psychology outcomes.
H1. Participants in the coach-like condition and the companion-like condition will show improved psychological well-being, affect, and readiness to change after the study, while participants in the control condition will not show any significant change.
H1a. Also, the companion-like robot will result in higher improvement in well-being, affect, and readiness to change than the coach-like robot.
H2. Participants’ working alliance with the robot will be positively correlated with their improvement in psychological well-being, overall affect, and readiness to change.
H2a. And participants in the companion-like condition will report the highest working alliance with the robot, followed by participants in the coach-like condition, and participants in the control condition.
4. DATA COLLECTION AND MEASURES
4.1. Self-report Measures
For pre-screening procedure, the Mini-IPIP [16] and the PHQ-9 [35] were administered to measure potential participants’ personality traits and risk for depression. The Mini-IPIP (International Personality Item Pool) scale [16] is a 20-item short form of the 50-item of IPIP that measures Big Five personality traits, and consist of phrases describing a behaviour or a trait (conscientiousness, agreeableness, neuroticism, openness to experience and extroversion).
During the study, three self-report questionnaires were administered to measure study participants’ psychological well-being (Ryf’s Psychological Well-being Scale [32]), affect (Positive and Negative Affect Schedule Short Form [65]), and readiness to change (Readiness Ruler [24]) on a weekly basis. The Ryf’s Psychological Well-being Scale (RPWS) [56] was used to measure participants’ psychological well-being with six sub-scales (autonomy, environmental mastery, personal growth, positive relations with others, purpose in life and self-acceptance). The Positive and Negative Affect Schedule-Short Form (PANAS-SF) is a 20-item scale that is widely used to measure mood or emotion with ten items for measuring positive affect (e.g., excited, inspired) and ten items measuring negative affect (e.g., upset, afraid). The Readiness Ruler (RR) is commonly used to measure participants’ willingness and motivation to make behavior changes for better well-being. We asked participants’ perceived importance and confidence to make behavior change for better well-being. For the importance to change (RR_imp), we asked “how important it is for you to make behavior change for better well-being?” and the confidence to change (RR_conf) asked “how confident are you about making behavior change for better well-being?”, all on a scale of zero to ten.
At the end of the study, participants completed the Working Alliance Inventory-Short Revised (WAI-SR) [45] to evaluate their perceived rapport with the robot. The WAI-SR assesses the extent of collaboration between a clinician/therapist and a client on three sub-scales (bond, goals and tasks).
4.2. Video and Audio Data
The positive psychology sessions with the robot were video/audio recorded via the Android tablet and the USB camera connected to the Raspberry Pi on the robot station. Whenever the system was recording, the Android application displayed a live video feed at the bottom right corner on the tablet screen to notify the recording status. Once the session with the robot was completed, the tablet application uploaded the recorded data with other relevant meta data to Amazon S3, and the local data was deleted from the tablet. After the study, the audio data was transcribed by a professional transcription vendor2.
4.3. Post-study interview
We conducted a semi-structured interview with each participant at the end of the study to gain more qualitative feedback on the interaction. During the interview, participants shared their overall experience with the study, things they liked/disliked about the robot and the intervention sessions. We also asked whether they would continue practicing the positive psychology activities after the study, and whether there were any features they would like to see in robots in the future. The whole list of the interview questions are as below in the Appendix, to support replicability of this work. All interview responses were audio-recorded and transcribed for qualitative analysis.
5. RESULTS
We present the results from our analyses in this section. The acronyms refer to the following: RPWS_total, overall well-being; RPWS_A, autonomy; RPWS_EM, environmental mastery; RPWS_PG: personal growth; RPWS_PR, positive relations with others; RPWS_PL, purpose in life; RPWS_SA, self-acceptance. PANAS_total refers to overall affect; PANAS_PA, positive affect; PANAS_NA, negative affect; RR_imp, importance for well-being change; RR_conf, confidence for well-being change. The PANAS_total is calculated by PANAS_PA-PANAS_NA.
5.1. Impact of Robot Intervention on Well-being, Affect, and Readiness to Change
Linear mixed effect regression models showed that experimental conditions made significant impact on participants’ well-being, affect, and readiness to change. For the control condition, negative affect showed statistically significant decrease over time (PANAS_NA, coef=−0.050, p=0.009). For the coach-like condition, overall well-being (RPWS_total, coef=0.023, p=0.048) and overall affect (PANAS_total, coef=0.074, p=0.004) showed significant improvement and negative affect (PANAS_NA, coef=−0.050, p=0.004) showed significant reduction. For the companion-like condition, overall well-being (RPWS_total, coef=0.033, p=0.030), personal growth (RPWS_PG, coef=0.038, p=0.036), self-acceptance (RPWS_SA, coef=0.047, p=0.014), and confidence for change (RR_change, coef=0.105, p=0.010) showed statistically significant improvement and negative affect (PANAS_NA, coef=−0.036, p=0.004) showed statistically significant decrease during the study. Overall, we found that both coach-like and companion-like conditions made positive impacts on intervention outcomes but the companion-like robot resulted in the biggest change in psychological well-being. Table 1 shows the results from the linear mixed regression models and Figure 3 show plots of statistically significant results.
Table 1:
Results from the linear mixed regression model. Coef refers to the coefficient value and SE is the standard error of the week term.
| Control | Coach-like | Companion-like | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Measurement | Coef | SE | z | p | Coef | SE | z | p | Coef | SE | z | p |
|
| ||||||||||||
| RPWS_total | 0.007 | 0.016 | 0.453 | 0.651 | 0.023 | 0.011 | 1.980 | 0.048* | 0.033 | 0.015 | 2.167 | 0.030* |
| RPWS_A | 0.008 | 0.021 | 0.387 | 0.699 | 0.049 | 0.030 | 1.618 | 0.106 | 0.029 | 0.027 | 1.087 | 0.277 |
| RPWS_EM | 0.028 | 0.036 | 0.793 | 0.428 | 0.027 | 0.027 | 1.000 | 0.317 | 0.037 | 0.030 | 1.246 | 0.213 |
| RPWS_PG | −0.025 | 0.018 | −1.388 | 0.165 | 0.003 | 0.024 | 0.136 | 0.892 | 0.038 | 0.018 | 2.092 | 0.036* |
| RPWS_PR | 0.002 | 0.025 | 0.085 | 0.932 | 0.025 | 0.020 | 1.254 | 0.210 | 0.019 | 0.023 | 0.838 | 0.402 |
| RPWS_PL | 0.021 | 0.023 | 0.912 | 0.362 | 0.018 | 0.020 | 0.879 | 0.379 | 0.031 | 0.021 | 1.430 | 0.153 |
| RPWS_SA | 0.014 | 0.021 | 0.683 | 0.495 | 0.022 | 0.019 | 1.182 | 0.237 | 0.047 | 0.019 | 2.451 | 0.014* |
|
| ||||||||||||
| PANAS_total | 0.030 | 0.034 | 0.875 | 0.382 | 0.074 | 0.026 | 2.888 | 0.004** | 0.019 | 0.027 | 0.690 | 0.490 |
| PANAS_PA | −0.019 | 0.022 | −0.844 | 0.399 | 0.019 | 0.020 | 0.919 | 0.358 | −0.017 | 0.019 | −0.868 | 0.385 |
| PANAS_NA | −0.050 | 0.019 | −2.620 | 0.009** | −0.050 | 0.017 | −2.881 | 0.004** | −0.036 | 0.013 | −2.852 | 0.004** |
|
| ||||||||||||
| RR_imp | −0.018 | 0.052 | −0.336 | 0.737 | −0.027 | 0.038 | −0.724 | 0.469 | 0.043 | 0.040 | 1.065 | 0.287 |
| RR_conf | −0.016 | 0.054 | −0.288 | 0.773 | 0.025 | 0.051 | 0.498 | 0.618 | 0.105 | 0.041 | 2.584 | 0.010* |
Figure 3:
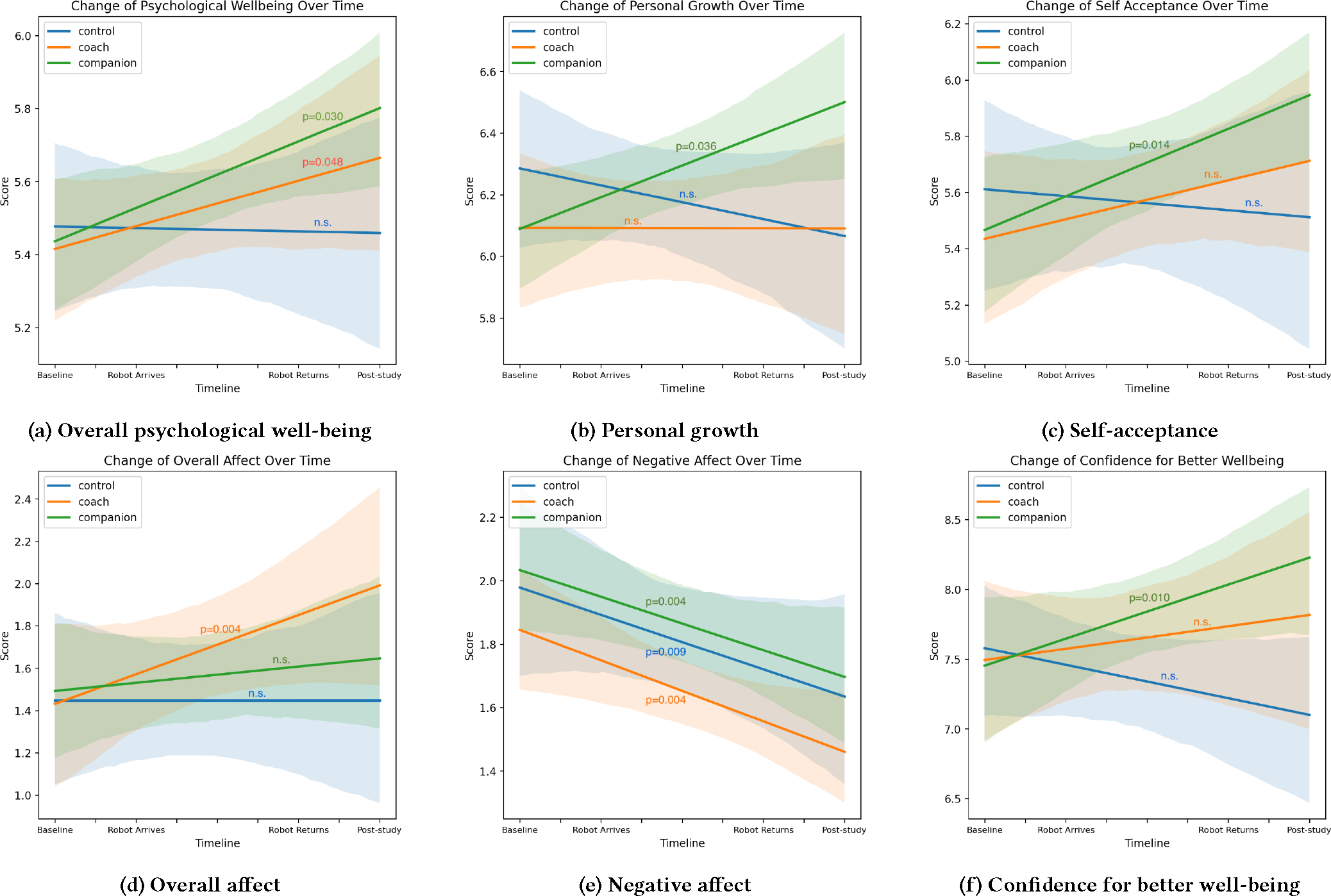
The companion-like condition showed a statistically significant improvement in overall psychological well-being, personal growth, self-acceptance, and confidence for better well-being. The coach-like condition showed significant improvement in overall well-being and overall affect. All three conditions showed significant reduction in negative affect. [Graph interpretation: increasing trend is better except negative affect, which decreasing trend is better.
5.2. Impact of Working Alliance on Intervention Outcomes
A Kruskal-Wallis test showed that there were significant differences among participants’ working alliance with the robot across the three experimental conditions: control MD=1.958, coach-like MD=3.333, companion-like MD=3.750; χ2(2)=14.409, p<0.001. Post-hoc Dunn tests showed that the control condition was significantly lower than the coach-like (p=0.005) and the companion-like (p<0.001) condition.
Further analyses were conducted to investigate the differences in three elements (Goal, Task, and Bond) of the WAI-SR. Kruskal-Wallis tests on each element showed that all three elements were significantly different across the conditions: WAI-SR Goal, χ2(2)=15.191, p<0.001; WAI-SR Task, χ2(2)=17.966, p<0.001; WAI-SR Bond, χ2(2)=7.509, p=0.023. The medians for the WAI-SR Goal are: control MD=1.500, coach-like MD=3.250, companion-like MD=3.500. The medians for the WAI-SR Task are: control MD=2.000, coach-like MD=3.250, companion-like MD=3.375. The medians for the WAI-SR Bond are: control MD=2.375, coach-like MD=4.000, companion-like MD=4.500 (Figure 4).
Figure 4:
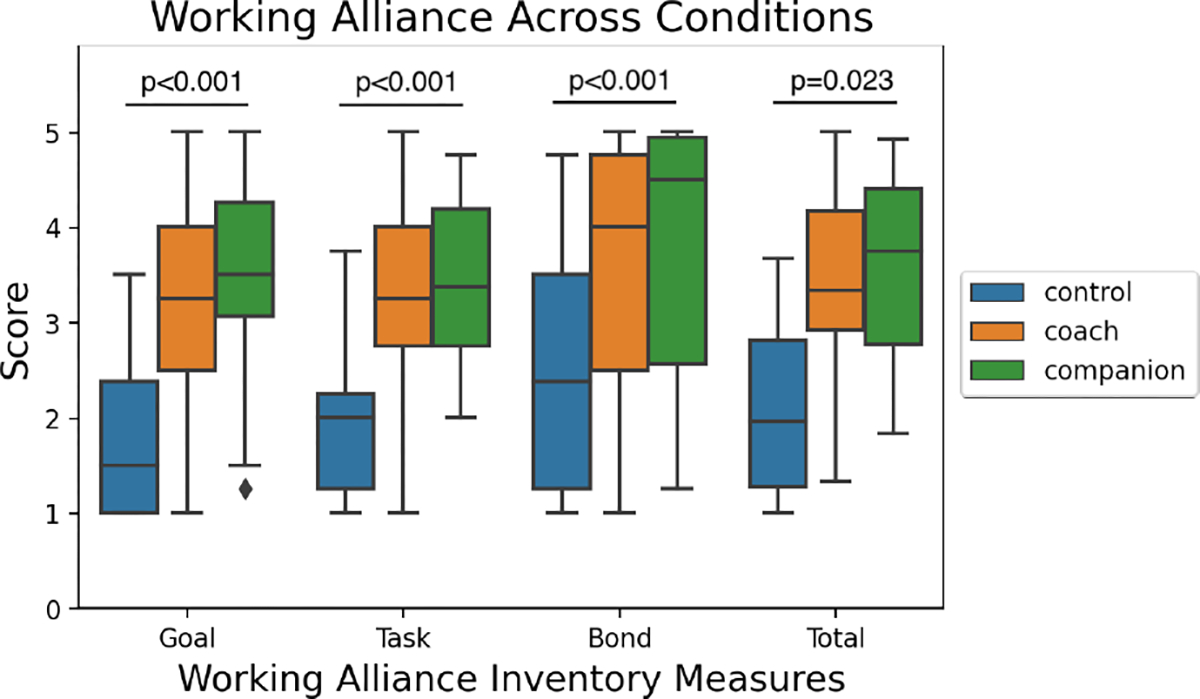
Participants’ working alliance with the robot showed statistically significant differences among the three experimental conditions.
Post-hoc Dunn tests were conducted for pairwise comparisons. For the WAI-SR Goal, the control condition was significantly lower than the coach-like (p=0.010) and the companion-like condition (p<0.001) conditions. For the WAI-SR Task, the control condition was lower than the coach-like condition (p<0.001) and the companion-like condition (p<0.001). For the WAI-SR Bond, the control condition was significantly lower than the companion-like condition (p=0.026) but was not significantly different from the coach-like condition (p=0.067).
Although there was no significant difference between the coach-like and companion-like conditions, a contrast coded generalized linear regression model showed a statistically significant trend of increase in the level of working alliance across the three experimental condition (control < coach-like < companion-like) for the overall working alliance and each WAI-SR element: WAI-SR Total p<0.0001; WAI-SR Goal p<0.0001; WAI-SR Task, p<0.0001; WAI-SR Bond, p=0.012.
Spearman’s correlation coefficients between participants’ working alliance and study outcomes were calculated to test for H2. The goal and task factors of participants’ working alliance were positively correlated with their change in well-being (ΔRPWS_total). However, overall affect or readiness to change were not associated with participants’ self-reported alliance with the robot (Table 2).
Table 2:
Spearman’s correlations between participants’ working alliance and study outcomes.
| WAI_SF Item | Study Outcome | ρ | p-value |
|---|---|---|---|
| W AI_goal | ΔRPWS_total | 0.302 | 0.038* |
| ΔPANAS_total | 0.043 | 0.773 | |
| ΔRR_imp | −0.015 | 0.916 | |
| ΔRR_conf | 0.065 | 0.663 | |
| W AI_task | ΔRPWS_total | 0.337 | 0.020* |
| ΔPANAS_total | 0.257 | 0.080 | |
| ΔRR_imp | 0.071 | 0.634 | |
| ΔRR_conf | 0.161 | 0.277 | |
| W AI_bond | ΔRPWS_total | 0.169 | 0.256 |
| ΔPANAS_total | 0.012 | 0.932 | |
| ΔRR_imp | −0.084 | 0.572 | |
| ΔRR_conf | 0.070 | 0.637 |
5.3. Post-study Interview
Overall, participants enjoyed engaging in the wellness activities with the robot (85%). Participants most enjoyed (1) the opportunities to reflect and introspect on their own experiences/well-being, (2) the robot’s positivity and behavioral reinforcement on intervention materials, and (3) the overall positive psychology intervention contents. The study sparked curiosity for participants to learn more about well-being activities and motivated them to continue practicing them after the study. Several participants mentioned that they were willing to keep practicing and utilizing the intervention activities they learned from the study even after the robot was no longer with them. P20 noted that she shared one of the interventions she learned from the study with a friend who asked for help.
The robot’s guidance with the wellness program was also appreciated. P06 said “I found that part [gratitude session] really profound because geez, I could list about 30 or 40 things that I’m grateful for. Um, and COVID has made life very difficult for all of us and, um, I just feel like my life has just literally been a miracle. It’s, it, it went from 0 all the way around to 360. So, um, I very much enjoyed that.” P23 and P46 noted it was easy to understand the intervention materials and the assigned exercises were easily comprehended and implemented in their daily lives, and P20 appreciated the examples and anecdotes the robot shared.
However, some participants said it took some time to get accustomed to having the robot in their homes. P06 said, “I mean, I had to get used to him. (laughing). He’s just a typical kid that, you know, somebody drop, your friend you haven’t seen in 10 years and they drop of their son say-Can he stay with you for a week, something’s come up? And so you have to get used to the kid, right?”.
6. DISCUSSION
Our long-term home deployment study showed that the positive psychology intervention delivered by our robots made a positive impact on participants’ well-being, affect, and readiness to change (H1), which align with the previous finding from Jeong et al. [29]. Overall, we found that the companion-like robot was the most effective (H1a). Participants who lived with the companion-like robot showed significant improvements in their psychological well-being (RPWS_total), personal growth (RPWS_PG), self-acceptance (RPWS_SA), and confidence for well-being change (RR_conf). With the coach-like robot, participants showed improved overall psychological well-being (RPWS_total) and overall affect (PANAS_total).
Interestingly, participants in the experimental condition reported higher therapeutic alliance with the robot compared to participants in the control condition in all three categories (goal, task, and bond), and a consistent trend of the companion-like robot being rated higher than the coach-like robot was observed (H2a). Correlation analyses between the intervention outcomes and working alliance found that participants’ rapport with the robot was positively associated with improvement in psychological well-being (H2). This result suggests that the human-robot rapport could either impact or indicate the effectiveness of the well-being interventions delivered through the robot, just as clinician-patient rapport is repeatedly shown to be a predictor for treatment outcomes in prior literature.
Jeong et al. [29, 30] showed that positive psychology interventions delivered by a coach-like robot are associated with college students’ improved well-being outcomes. Results from our study suggest that the human-robot alliance and rapport could amplify the positive therapeutic impact on people’s well-being outcomes and their motivation for behavior change. In addition, an exploratory analysis on non-verbal cues observed during human-robot interactions found that relaxed vocal expression, positive facial expression, and physical engagement behaviors were associated with the intervention outcomes [30]. Results from these two studies suggest that there is an opportunity for an interactive agent to observe users’ behavior and infer how well the interaction is going, in order to continuously personalize and adapt its relationship with the user to enhance the intervention effect.
Evaluating the effect of a long-term robot intervention in the real world is challenging since it is impossible to isolate the effect of other external factors. For example, participants in all three conditions showed a significant trend of negative affect decreasing over time. This shows that the effect must have come outside the positive psychology intervention the experimental condition robots (coach-like and companion-like) provided. The co-presence of the robot could have contributed to the reduction of negative affect, but other factors such as the weather (winter to spring, spring to summer) could have attributed to the trend. While it is impossible to control all the external variables, we attempted to balance out their effect by fairly but randomly distributing participants across conditions based on their age, gender, and personality traits. Even so, we acknowledge that our results could have been influenced by factors other than the positive psychology interventions provided by the robot.
One limitation in our work is that only self-reported measures and interview data were used to evaluate the effect of our robot intervention. Although the self-reported questionnaires used in the study were previously validated and are widely used in clinical settings, they may contain response bias and inaccurate reflection of participants’ internal state [2]. Future studies that use a multi-method assessment approach that combines both self-reported responses and objective physiological measures would allow improved evaluation of the intervention and provide a more accurate and holistic understanding of its impact.
Our future work will focus on investigating how people’s linguistic, verbal, and non-verbal behaviors change over time as they develop relationship and rapport with the agent, and what behavioral signs indicate and inform the growth or decay of the human-agent alliance through long-term interactions and data collection. Social penetration theory [3] proposes that the breadth and depth of self-disclosures moves from shallow/non-intimate topics to deeper/more-intimate ones as interpersonal relationship develops. We believe some of negative feedback on the robot’s behavior could have stemmed from the mismatch between the participant’s perceived relationship with the robot and the robot’s prosocial and self-disclosure behavior, which was viewed as a violation of social norm. In order to mitigate such mismatch between the robot’s behavior and a user’s perceived relationship with the robot, the robot should continuously monitor and manage its rapport with people.
7. CONCLUSION
In this work, we present a novel companion-like robot that delivered interactive positive psychology interventions along with other useful skills during the COVID-19 pandemic. Our long-term deployment study showed that a social robot delivered positive psychology sessions were effective at improving people’s psychological well-being, affect, and motivation for behavior change, and that the effect was greater when users have built therapeutic alliance with the agent. While both the robot’s coach-like and companion-like interaction styles were effective, our results show that the companion-like robot style formed tighter working alliance with the users and produced the best intervention outcomes. These results suggest that it is important to design an interactive agent as a helpful and supportive companion that can build long-term rapport and therapeutic alliance in order to improve the efficacy of its health interventions. Our work contributes to studying how to design companion AI agents that can support people’s long-term well-being goals in daily lives.
Supplementary Material
CCS CONCEPTS.
• Human-centered computing → Empirical studies in HCI; Empirical studies in interaction design.
ACKNOWLEDGMENTS
This work was supported by the Information and Communication Technology (ICT) R&D program of the Ministry of Science and Institute for Information and Communication Technology Promotion of Republic of Korea under grant 2017-0-00162, “Development of Human-Care Robot Technology for Aging Society”. SJ was supported by the T32 MH115822 grant from the National Institute of Mental Health (NIMH). LA-F was supported by the Ramón y Cajal Fellowship Program (ref. RYC-2016-19770), funded by Agencia Estatal de Investigación, Ministerio de Ciencia, Innovación y Universidades, and the European Social Fund.
Footnotes
Contributor Information
Sooyeon Jeong, Northwestern University, Chicago, Illinois, USA.
Laura Aymerich-Franch, Pompeu Fabra University, Barcelona, Spain.
Sharifa Alghowinem, MIT Media Lab, Cambridge, MA, USA.
Rosalind W. Picard, MIT Media Lab, Cambridge, MA, USA
Cynthia L. Breazeal, MIT Media Lab, Cambridge, MA, USA
Hae Won Park, MIT Media Lab, Cambridge, MA, USA.
REFERENCES
- [1].Abdollahi Hojjat, Mollahosseini Ali, Lane Josh T, and Mahoor Mohammad H. 2017. A pilot study on using an intelligent life-like robot as a companion for elderly individuals with dementia and depression. In 2017 IEEE-RAS 17th International Conference on Humanoid Robotics (Humanoids). IEEE, 541–546. [Google Scholar]
- [2].Althubaiti Alaa. 2016. Information bias in health research: definition, pitfalls, and adjustment methods. Journal of multidisciplinary healthcare 9, 211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Altman Irwin and Taylor Dalmas A. 1973. Social penetration: The development of interpersonal relationships. Holt, Rinehart & Winston. [Google Scholar]
- [4].Anderson William Todd. 2012. Mindful listening instruction: Does it make a difference. Contributions to Music Education, 13–30. [Google Scholar]
- [5].Aymerich-Franch Laura and Ferrer Iliana. 2022. Investigating the use of speech-based conversational agents for life coaching. International Journal of Human-Computer Studies 159, 102745. [Google Scholar]
- [6].Aymerich-Franch Laura and Ferrer Iliana. 2022. Liaison, safeguard, and well-being: Analyzing the role of social robots during the COVID-19 pandemic. Technology in Society, 101993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Bailey Thomas C, Eng Winnie, Frisch Michael B, and Snyder CR. 2007. Hope and optimism as related to life satisfaction. The Journal of Positive Psychology 2, 3, 168–175. [Google Scholar]
- [8].Björling Elin A, Ling Honson, Bhatia Simran, and Dziubinski Kimberly. 2020. The Experience and Effect of Adolescent to Robot Stress Disclosure: A Mixed-Methods Exploration. In International Conference on Social Robotics. Springer, 604–615. [Google Scholar]
- [9].Bolier Linda, Haverman Merel, Westerhof Gerben J, Riper Heleen, Smit Filip, and Bohlmeijer Ernst. 2013. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC public health 13, 1, 1–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Braunwalder Céline, Rachel Müller Marija Glisic, and Fekete Christine. 2022. Are positive psychology interventions efficacious in chronic pain treatment? A systematic review and meta-analysis of randomized controlled trials. Pain medicine 23, 1, 122–136. [DOI] [PubMed] [Google Scholar]
- [11].Bryant Fred B and Verof Joseph. 2017. Savoring: A new model of positive experience. Psychology Press. [Google Scholar]
- [12].Carpenter Amanda and Greene Kathryn. 2015. Social penetration theory. The international encyclopedia of interpersonal communication, 1–4. [Google Scholar]
- [13].Chartrand Tanya L and Van Baaren Rick. 2009. Human mimicry. Advances in experimental social psychology 41, 219–274. [Google Scholar]
- [14].Cohen Sheldon and Wills Thomas A. 1985. Stress, social support, and the buffering hypothesis. Psychological bulletin 98, 2, 310. [PubMed] [Google Scholar]
- [15].Cozby Paul C. 1972. Self-disclosure, reciprocity and liking. Sociometry, 151–160. [PubMed] [Google Scholar]
- [16].Donnellan M Brent, Oswald Frederick L, Baird Brendan M, and Lucas Richard E. 2006. The mini-IPIP scales: Tiny-yet-effective measures of the Big Five factors of personality. Psychological assessment 18, 2, 192. [DOI] [PubMed] [Google Scholar]
- [17].Emmons Robert A and Shelton Charles M. 2002. Gratitude and the science of positive psychology. Handbook of positive psychology 18, 459–471. [Google Scholar]
- [18].Fogelson Donna M, Rutledge Carolyn, and Zimbro Kathie S. 2021. The Impact of Robotic Companion Pets on Depression and Loneliness for Older Adults with Dementia During the COVID-19 Pandemic. Journal of Holistic Nursing, 08980101211064605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Fuertes Jairo N, Mislowack Alexa, Bennett Jennifer, Paul Laury, Gilbert Tracey C, Fontan Gerardo, and Boylan Laura S. 2007. The physician–patient working alliance. Patient education and counseling 66, 1, 29–36. [DOI] [PubMed] [Google Scholar]
- [20].Ganster Daniel C and Victor Bart. 1988. The impact of social support on mental and physical health. British Journal of Medical Psychology 61, 1, 17–36. [DOI] [PubMed] [Google Scholar]
- [21].Glanz Karen, Rimer Barbara K, and Viswanath Kasisomayajula. 2008. Health behavior and health education: Theory, research, and practice. John Wiley & Sons. [Google Scholar]
- [22].Gratch Jonathan, Lucas Gale M, King Aisha Aisha, and Morency Louis-Philippe. 2014. It’s only a computer: The impact of human-agent interaction in clinical interviews. In Proceedings of the 2014 international conference on Autonomous agents and multi-agent systems. 85–92. [Google Scholar]
- [23].Haker H, Lauber C, and Rössler W. 2005. Internet forums: A self-help approach for individuals with schizophrenia? Acta Psychiatrica Scandinavica 112, 6, 474–477. [DOI] [PubMed] [Google Scholar]
- [24].Hesse Morten. 2006. The Readiness Ruler as a measure of readiness to change poly-drug use in drug abusers. Harm reduction journal 3, 1, 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Ho Henry CY, Yeung Dannii Y, and Kwok Sylvia YCL. 2014. Development and evaluation of the positive psychology intervention for older adults. The Journal of Positive Psychology 9, 3, 187–197. [Google Scholar]
- [26].Holt-Lunstad Julianne, Smith Timothy B, Baker Mark, Harris Tyler, and Stephenson David. 2015. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspectives on psychological science 10, 2, 227–237. [DOI] [PubMed] [Google Scholar]
- [27].Holt-Lunstad Julianne, Smith Timothy B, and Layton J Bradley. 2010. Social relationships and mortality risk: A meta-analytic review. PLoS medicine 7, 7, e1000316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Hyde Luke W, Gorka Adam, Manuck Stephen B, and Hariri Ahmad R. 2011. Perceived social support moderates the link between threat-related amygdala reactivity and trait anxiety. Neuropsychologia 49, 4, 651–656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Jeong Sooyeon, Alghowinem Sharifa, Aymerich-Franch Laura, Arias Kika, Lapedriza Agata, Picard Rosalind, Park Hae Won, and Breazeal Cynthia. 2020. A Robotic Positive Psychology Coach to Improve College Students’ Wellbeing. In 2020 29th IEEE International Conference on Robot and Human Interactive Communication (RO-MAN). IEEE, 187–194. [Google Scholar]
- [30].Jeong Sooyeon, Aymerich-Franch Laura, Arias Kika, Alghowinem Sharifa, Lapedriza Agata, Picard Rosalind, Park Hae Won, and Breazeal Cynthia. 2022. Deploying a robotic positive psychology coach to improve college students’ psychological well-being. User Modeling and User-Adapted Interaction, 1–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Johanson Deborah L, Ahn Ho Seok, MacDonald Bruce A, Ahn Byeong Kyu, Lim JongYoon, Hwang Euijun, Sutherland Craig J, and Broadbent Elizabeth. 2019. The effect of robot attentional behaviors on user perceptions and behaviors in a simulated health care interaction: Randomized controlled trial. Journal of medical Internet research 21, 10, e13667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Kállay Éva and Rus Claudia. 2014. Psychometric properties of the 44-item version of Ryf’s Psychological Well-Being Scale. European Journal of Psychological Assessment. [Google Scholar]
- [33].Kaplan Berton H, Cassel John C, and Gore Susan. 1977. Social support and health. Medical care 15, 5, 47–58. [DOI] [PubMed] [Google Scholar]
- [34].Koo Minkyung, Algoe Sara B, Wilson Timothy D, and Gilbert Daniel T. 2008. It’s a wonderful life: Mentally subtracting positive events improves people’s affective states, contrary to their affective forecasts. Journal of personality and social psychology 95, 5, 1217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Kroenke Kurt and Spitzer Robert L. 2002. The PHQ-9: A new depression diagnostic and severity measure. [DOI] [PMC free article] [PubMed]
- [36].Langford Catherine Penny Hinson, Bowsher Juanita, Maloney Joseph P, and Lillis Patricia P. 1997. Social support: A conceptual analysis. Journal of advanced nursing 25, 1, 95–100. [DOI] [PubMed] [Google Scholar]
- [37].Lee Yi-Chieh, Yamashita Naomi, Huang Yun, and Fu Wai. 2020. “ I Hear You, I Feel You”: Encouraging Deep Self-disclosure through a Chatbot. In Proceedings of the 2020 CHI conference on human factors in computing systems. 1–12. [Google Scholar]
- [38].Leite Iolanda, Castellano Ginevra, Pereira André, Martinho Carlos, and Paiva Ana. 2012. Long-term interactions with empathic robots: Evaluating perceived support in children. In International Conference on Social Robotics. Springer, 298–307. [Google Scholar]
- [39].Leite Iolanda, Castellano Ginevra, Pereira André, Martinho Carlos, and Paiva Ana. 2014. Empathic robots for long-term interaction. International Journal of Social Robotics 6, 3, 329–341. [Google Scholar]
- [40].Gale M Lucas Albert Rizzo, Gratch Jonathan, Scherer Stefan, Stratou Giota, Boberg Jill, and Morency Louis-Philippe. 2017. Reporting mental health symptoms: breaking down barriers to care with virtual human interviewers. Frontiers in Robotics and AI 4, 51. [Google Scholar]
- [41].Luthar Suniya S, Lyman Emily L, and Crossman Elizabeth J. 2014. Resilience and positive psychology. In Handbook of developmental psychopathology. Springer, 125–140. [Google Scholar]
- [42].Martelaro Nikolas, Victoria C Nneji Wendy Ju, and Hinds Pamela. 2016. Tell me more designing HRI to encourage more trust, disclosure, and companionship. In 2016 11th ACM/IEEE International Conference on Human-Robot Interaction (HRI). IEEE, 181–188. [Google Scholar]
- [43].Mongrain Myriam and Anselmo-Matthews Tracy. 2012. Do positive psychology exercises work? A replication of Seligman et al. (2005). Journal of clinical psychology 68, 382–389. [DOI] [PubMed] [Google Scholar]
- [44].Moon Youngme. 2000. Intimate exchanges: Using computers to elicit self-disclosure from consumers. Journal of consumer research 26, 4, 323–339. [Google Scholar]
- [45].Munder Thomas, Wilmers Fabian, Leonhart Rainer, Linster Hans Wolfgang, and Barth Jürgen. 2010. Working Alliance Inventory-Short Revised (WAI-SR): Psychometric properties in outpatients and inpatients. Clinical Psychology & Psychotherapy: An International Journal of Theory & Practice 17, 3, 231–239. [DOI] [PubMed] [Google Scholar]
- [46].Myers David and Hayes Jefrey A. 2006. Effects of therapist general self-disclosure and countertransference disclosure on ratings of the therapist and session. Psychotherapy: Theory, Research, Practice, Training 43, 2, 173. [DOI] [PubMed] [Google Scholar]
- [47].Nef Kristin and Knox Marissa C. 2016. Self-compassion. Mindfulness in positive psychology: The science of meditation and wellbeing 37, 1–8. [Google Scholar]
- [48].Niemiec Ryan M. 2013. VIA character strengths: Research and practice (The first 10 years). In Well-being and cultures. Springer, 11–29. [Google Scholar]
- [49].World Health Organization et al. 2018. Mental health: strengthening our response.
- [50].Park Nansook and Peterson Christopher. 2008. Positive psychology and character strengths: Application to strengths-based school counseling. Professional school counseling 12, 2, 2156759X0801200214. [Google Scholar]
- [51].Parks Acacia C and Biswas-Diener Robert. 2013. Positive interventions: Past, present and future. Mindfulness, acceptance, and positive psychology: The seven foundations of well-being, 140–165. [Google Scholar]
- [52].Peterson Christopher. 2009. Positive psychology. Reclaiming children and youth 18, 2, 3. [Google Scholar]
- [53].Peterson Christopher and Seligman Martin E. P.. 2004. Character strengths and virtues a handbook and classification. American Psychological Association. [Google Scholar]
- [54].Qina’au Joanne and Masuda Akihiko. 2020. Cultural considerations in the context of establishing rapport: A contextual behavioral view on common factors. In Handbook of Cultural Factors in Behavioral Health. Springer, 75–92. [Google Scholar]
- [55].Rashid Tayyab. 2015. Positive psychotherapy: A strength-based approach. The Journal of Positive Psychology 10, 25–40. 10.1080/17439760.2014.920411 [DOI] [Google Scholar]
- [56].Ryf Carol D and Keyes Corey Lee M. 1995. The structure of psychological well-being revisited. Journal of personality and social psychology 69, 4, 719. [DOI] [PubMed] [Google Scholar]
- [57].Seligman Martin EP and Csikszentmihalyi Mihaly. 2014. Positive psychology: An introduction. In Flow and the foundations of positive psychology. Springer, 279–298. [Google Scholar]
- [58].Seligman Martin EP, Rashid Tayyab, and Parks Acacia C. 2006. Positive psychotherapy. American psychologist 61, 8, 774. [DOI] [PubMed] [Google Scholar]
- [59].Seligman Martin EP, Steen Tracy A, Park Nansook, and Peterson Christopher. 2005. Positive psychology progress: Empirical validation of interventions. American psychologist 60, 5, 410. [DOI] [PubMed] [Google Scholar]
- [60].Shoshani Anat and Steinmetz Sarit. 2014. Positive psychology at school: A school-based intervention to promote adolescents’ mental health and well-being. Journal of Happiness Studies 15, 6, 1289–1311. [Google Scholar]
- [61].Slevin ML, Nichols SE, Downer SM, Wilson P, Lister TA, Arnott S, Maher J, Souhami RL, Tobias JS, Goldstone AH, et al. 1996. Emotional support for cancer patients: What do patients really want? British journal of cancer 74, 8, 1275–1279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [62].Sprecher Susan and Treger Stanislav. 2015. The benefits of turn-taking reciprocal self-disclosure in get-acquainted interactions. Personal Relationships 22, 3, 460–475. [Google Scholar]
- [63].Stiehl Walter Dan, Lieberman Jef, Breazeal Cynthia, Basel Louis, Lalla Levi, and Wolf Michael. 2005. The Design of the Huggable: A Therapeutic Robotic Companion for Relational, Affective Touch.. In AAAI Fall Symposium: Caring Machines. 91–98. [Google Scholar]
- [64].Tamir Diana I and Mitchell Jason P. 2012. Disclosing information about the self is intrinsically rewarding. Proceedings of the National Academy of Sciences 109, 21, 8038–8043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [65].Thompson Edmund R. 2007. Development and validation of an internationally reliable short-form of the positive and negative affect schedule (PANAS). Journal of cross-cultural psychology 38, 2, 227–242. [Google Scholar]
- [66].Tilden Virginia P and Weinert Clarann. 1987. Social support and the chronically ill individual. The Nursing Clinics of North America 22, 3, 613–620. [PubMed] [Google Scholar]
- [67].Uchino Bert N. 2008. Social support and physical health. Yale university press. [Google Scholar]
- [68].Wampold Bruce E. 2015. How important are the common factors in psychotherapy? An update. World Psychiatry 14, 3, 270–277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [69].Wills Thomas Ashby. 1991. Social support and interpersonal relationships. Prosocial behavior. [Google Scholar]
- [70].Zink Korie L, Perry Marcia, London Kory, Floto Olivia, Bassin Benjamin, Burkhardt John, and Santen Sally A. 2017. “Let me tell you about my... ” Provider self-disclosure in the emergency department builds patient rapport. Western Journal of Emergency Medicine 18, 1, 43. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.