

Abstract
Background
Gastrointestinal bleeding (GIB) is a common complication after placement of a left ventricular assist device (LVAD). Some institutions attempt to mitigate post-LVAD GIB using preoperative endoscopy. Our study evaluated whether preoperative endoscopy was associated with a lower risk of post-LVAD GIB.
Methods
This was a multicenter cohort study of patients who underwent LVAD insertion from 2010-2019 at 3 academic sites. A total of 398 study participants were categorized based on whether they underwent preoperative endoscopy or not. The follow-up period was 1 year and the primary outcome was GIB. Secondary outcomes were severe bleeding and intraprocedural complications.
Results
A total of 114 patients experienced GIB within 1 year, with a higher rate in the endoscopy cohort (36.4% vs. 24.8%, P=0.015). After adjusting for covariables, the endoscopy cohort remained at increased risk of GIB (adjusted odds ratio 1.77, 95% confidence interval 1.05-2.976; P=0.032). Severe bleeding was common (47.4%). Arteriovenous malformations (48 cases) and peptic ulcer disease (17 cases) were the most identified sources of GIB. Only 1 minor adverse event occurred during preoperative endoscopy.
Conclusions
Our study suggests that pre-LVAD endoscopy is associated with a higher risk of GIB post LVAD, despite controlling for confounders. While this was an observational study and may not have captured all confounders, it appears that endoscopic screening may not be warranted.
Keywords: Heart-assist devices, gastrointestinal hemorrhage, endoscopy
Introduction
Left ventricular assist devices (LVADs) are increasingly used as life-prolonging therapy in advanced heart failure by serving as a bridge to cardiac transplantation, bridge to recovery or destination therapy [1]. Although LVAD insertions are associated with improved survival for patients with congestive heart failure, gastrointestinal bleeding (GIB) remains a common complication after LVAD placement, which contributes to significant morbidity and healthcare costs [2]. The etiology of GIB in LVAD recipients remains incompletely understood, but causative factors include use of anticoagulants and antiplatelet agents, development of acquired von Willebrand syndrome, and reduced pulse pressure with high shear stress [3]. Reported rates of GIB are high, ranging from 15-30% [4], with the main etiology being arteriovenous malformations (AVMs), which account for up to 44% of identified causes [5].
Patient-specific risk factors for post-LVAD GIB include older age, history of GIB, preimplant right ventricular (RV) dysfunction, chronic kidney disease (CKD), coronary artery disease (CAD), hyperglycemia, and elevated mean pulmonary arterial pressure [6]. Medical therapies have been shown to reduce the risk of bleeding in LVAD recipients [7], but to our knowledge no study has demonstrated any efficacy for preemptive endoscopy. Nevertheless, some medical centers, citing expert opinion [8], advocate for preoperative endoscopic evaluation of high-risk patients to mitigate bleeding associated with LVAD placement.
Our aim was to evaluate the efficacy of preoperative endoscopy in reducing the risk of post-LVAD GIB. Our hypothesis was that preoperative endoscopic evaluation does not reduce the risk of post-LVAD bleeding and may be associated with a higher rate of perioperative adverse events, given the more common comorbid diseases in this patient population.
Patients and methods
Study design, setting, and participants
We conducted a multicenter retrospective cohort study at 3 academic sites. Institutional LVAD databases were queried to find possible participants. Identified participants underwent LVAD insertion between 2010 and 2019. Adult patients (age ≥18 years) were eligible for inclusion. The minimum period of follow up was 1 year. Patients with less than 1 year of follow up were excluded. Study participants were categorized based on whether they underwent preoperative endoscopy or not (defined as upper endoscopy, colonoscopy or both, within 1 year prior to LVAD insertion). Indications for preoperative endoscopy were screening and diagnostic, at the discretion of the referring provider.
Data sources and variables
Data were collected from electronic medical records and endoscopy software. Baseline variables at the time of LVAD insertion were collected, including age, sex, race, prior history of GIB, outpatient proton pump inhibitor (PPI) use, antiplatelet agents, anticoagulants, coronary artery disease, chronic kidney disease, right ventricular dysfunction, and left ventricular (LV) distention. If patients underwent preoperative endoscopy, findings were collected and categorized into 5 groups: AVMs, peptic/mucosal disease (i.e., ulcers, erosions, gastritis), diverticulosis, polyps, and hemorrhoids. Amongst those who developed GIB, time to bleed (in days), presence of severe bleeding (defined as >3 g drops in hemoglobin on admission, or >3 packed red blood cell transfusions needed during hospitalization), supratherapeutic international normalized ratio (INR) (defined as INR >3 on admission), and source of bleeding were obtained and categorized according to the same groups. Procedure-related complications were categorized according to the established classification [9].
Statistical analysis
Descriptive statistics were tabulated and stratified according to screening status (Table 1). Continuous variables were presented as median with interquartile range (IQR), and Wilcoxon rank sum tests were employed for comparisons. Categorical variables were reported as frequencies (N) and percentages (%), and the chi-square test was used for comparative analysis. Univariate and multivariate logistic regressions were applied to further investigate the association between the primary outcome of “bleeding within 1 year” and the main predictor, screening status, while controlling for selected covariates. We controlled for preselected covariates, namely age, sex, race, prior history of GIB, coronary artery disease, chronic kidney disease, right ventricular dysfunction, outpatient PPI use, anticoagulants, and treatment centers. These covariates were chosen a priori, based on a review of the existing literature [6], to mitigate potential confounding factors. Model fit and assumptions were validated using diagnostics such as the Hosmer-Lemeshow goodness-of-fit test, and analysis of residuals. Any issues of multicollinearity among the variables were also assessed. The results from the finalized logistic regression model are presented in Table 2. Two supplementary analyses were performed to further investigate our findings. The first concentrated on individuals who underwent pre-LVAD endoscopy, and evaluated the association between their pre-LVAD findings and specific post-LVAD bleeding findings. We designed several plots to enhance comprehension and provide a visual representation of our findings. A bar chart was curated to elucidate the frequency distribution of both pre- and post-LVAD outcomes (Fig. 1). Twin upset plots delineated the frequency of various finding combinations spanning 5 distinct finding categories (Fig. 2,3). Lastly, an Alluvial diagram further encapsulated the progression from pre-LVAD screening discoveries to eventual post-LVAD bleeding events (Fig. 4). We also compared those who experienced severe bleeding to those with non-severe bleeding. Statistical significance was set at a 2-tailed P-value <0.05. All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). Specific R packages, including ggplot2, ComplexUpset, and ggalluvial, were used to generate graphical outputs.
Table 1.
Baseline variables and outcomes of unscreened and screened cohort of patients who underwent LVAD insertion
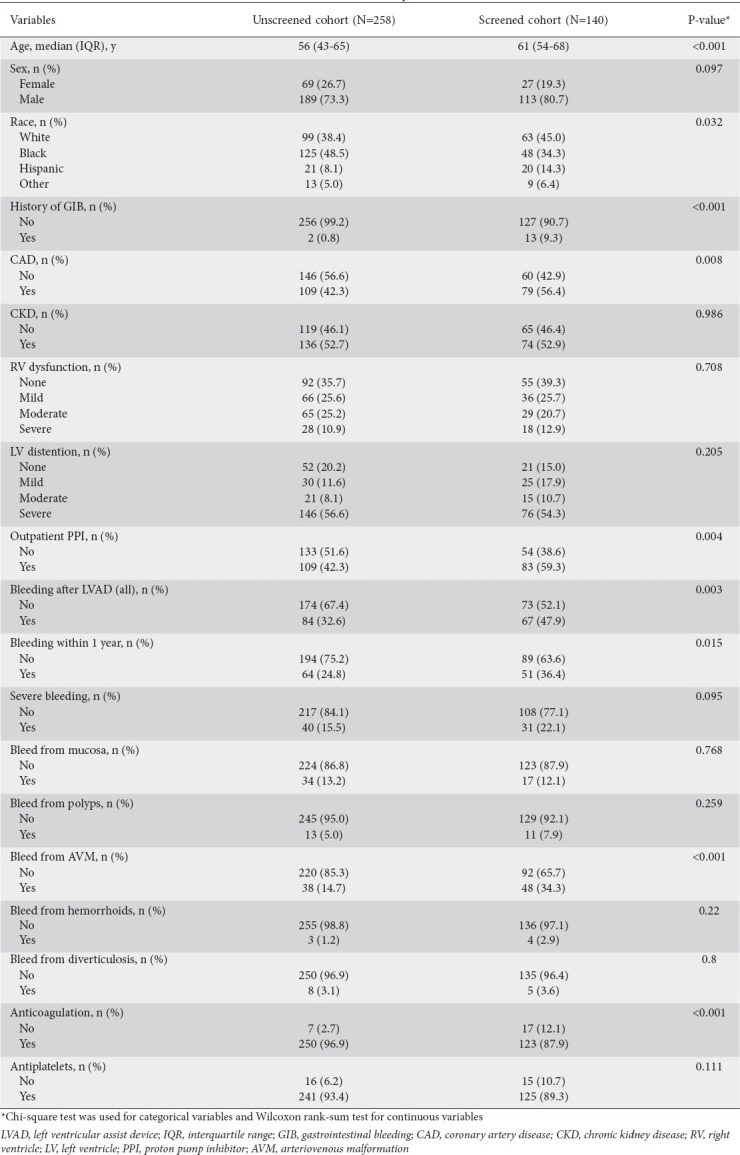
Table 2.
Univariate and multivariate logistic regression analyses of GIB at 1 year
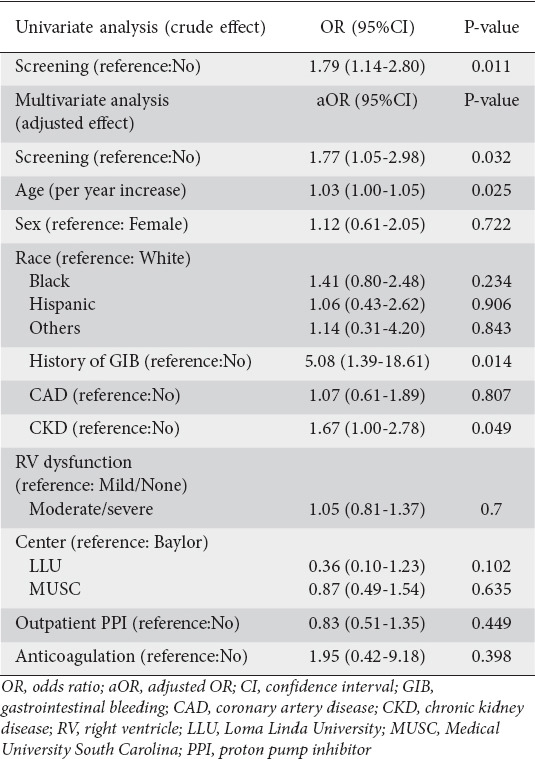
Figure 1.
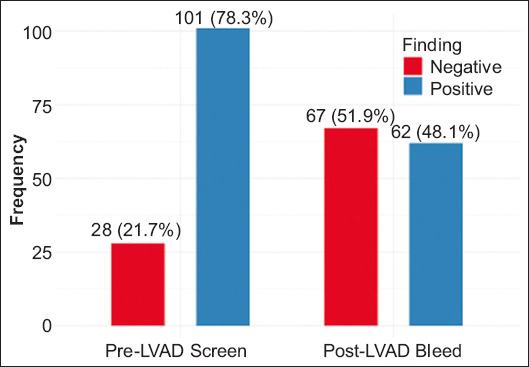
Frequency of positive and negative endoscopic findings among 129 patients, both pre- and post-LVAD implantation. In the pre-LVAD screening cohort, 101 patients (78.3%) exhibited positive findings. Conversely, in the post-LVAD bleeding cohort, 62 patients (48.1%) displayed positive findings
Figure 2.
Upset plot summarizing pre-LVAD endoscopic results for 129 patients with complete records. The plot reveals 101 patients (78.3%) with positive findings. The most common pattern of pre-LVAD screening finding was isolated polyps, which were found in 30 of 129 (23.3%) of all screened patients. An inset bar graph in the lower left corner shows that the most prevalent pathologic pre-LVAD finding was polyps (n=59, 58.4%), followed by diverticulosis (n=27, 26.7%), mucosal-related disorder (n=26, 25.7%), hemorrhoids (n=24, 23.8%), and AVMs (n=7, 6.9%)
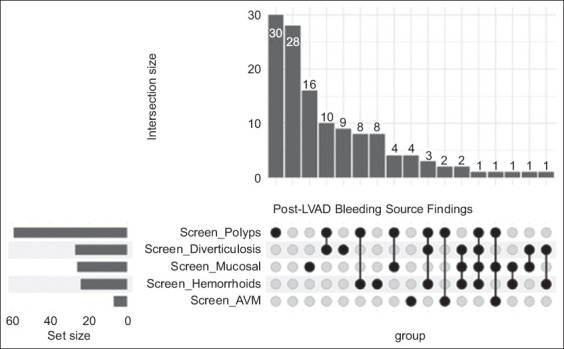
Figure 3.
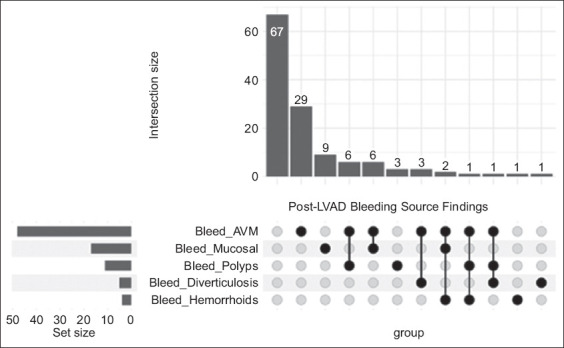
Upset plot summarizing post-LVAD GIB sources among 129 endoscopy cohort patients with complete records. The majority (n=67, 78.3%) did not experience GIB. Among the 62 patients with post-LVAD bleeding, isolated AVM-related bleeding was the predominant pattern, occurring in 29 of 62 cases (46.8%). An inset bar graph in the lower left corner shows the prevalent endoscopic sources of post-LVAD GIB: AVM-related (n=48, 77.4%), mucosal disorder-related (n=17, 27.4%), polyp-related (n=11, 17.7%), diverticulosis-related (n=5, 8.1%), and hemorrhoid-related (n=4, 6.5%)
Figure 4.
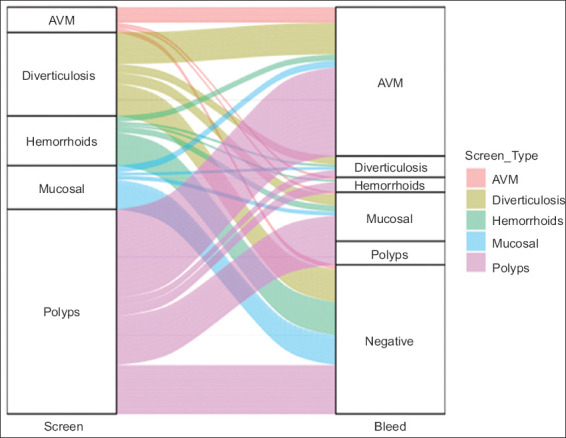
Alluvial diagram tracking the transition from pre-LVAD endoscopic findings to post-LVAD bleeding sources in a cohort of 101 patients with at least 1 positive screening result. The diagram quantitatively correlates these screening findings with subsequent bleeding sources post-LVAD implantation. The thickness of the bars and connecting lines is proportional to represent the number of occurrences of each finding (vertical bars) and the transitions between states (horizontal lines for pre- to post-LVAD transition)
LVAD, left ventricular assist device
LVAD, left ventricular assist device; AVM, arteriovenous malformation
LVAD, left ventricular assist device; GIB, gastrointestinal bleeding; AVM, arteriovenous malformation
LVAD, left ventricular assist device; AVM, arteriovenous malformation
Results
Preoperative endoscopy and no endoscopy cohorts
A total of 398 patients from 3 academic centers (176, 173 and 49, respectively) met the inclusion criteria. Of these, 140 underwent pre-LVAD endoscopy and 258 did not; 11 had missing or incomplete data. Table 1 summarizes the 2 cohorts. Of those who underwent preoperative endoscopy, 28 (20%) underwent esophagogastroduodenoscopy, 59 (42.14%) underwent colonoscopy and 53 (37.86%) had bidirectional endoscopy. The pre-LVAD endoscopy cohort were significantly older, of Caucasian and Hispanic race, with a history of GIB, preexisting CAD, PPI prescription at LVAD insertion and significantly less oral anticoagulation use at LVAD insertion.
GIB within 1 year of LVAD placement
GIB within 1 year occurred in 64 (24.8%) and 51 (36.4%) in the no-endoscopy and preemptive endoscopy groups, respectively (P=0.015). After adjusting for age, race, history of GIB, CAD, CKD, anticoagulation use, medical center, PPI use and RV dysfunction, GIB remained higher at 1-year in the preoperative endoscopy group (adjusted odds ratio [aOR] 1.77, 95% confidence interval [CI] 1.05-2.976; P=0.032) (Table 2). Time to bleed was earlier in the endoscopy cohort (median 76 [IQR 36-197] vs. 86 [IQR 38-197] days; 95%CI 3.81-6.55; P<0.001) (Supplementary Table 1 (220.4KB, pdf) and Supplementary Fig. 1 (220.4KB, pdf) ).
Severe GIB within 1 year of LVAD placement
Amongst those who developed GIB within 1 year, this was classified as severe in 29 (46.03%) and 25 (49.02%) in the no-endoscopy and preemptive endoscopy groups, respectively (P=0.574). On univariate analysis, a nonsignificant trend for greater LV distention (P=0.083) and supratherapeutic INR at admission during GIB (P=0.097) was seen in the severe GIB cohort at 1 year.
Risk factors for GIB within 1 year of LVAD placement
When factors associated with bleeding at 1 year were evaluated, age, history of GIB, CKD and pre-operative endoscopy were statistically significant. Conversely, preimplant RV dysfunction, sex, race, preexistent CAD, anticoagulation status, and medical center were not significant covariables (Table 2).
Endoscopy findings and etiology of bleeding
A total of 101 patients had at least 1 finding on preoperative endoscopy (Fig. 1), with the most common findings, in order of decreasing frequency, being polyps, diverticulosis, ulcers and erosions, hemorrhoids, and AVMs (Fig. 2). Amongst those who presented with GIB after LVAD, 62 patients had at least 1 positive finding on endoscopy (Fig. 1), with the most common findings, in order of decreasing frequency, being AVMs, erosions and ulcers, polyps, diverticulosis, and hemorrhoids (Fig. 3). Amongst the findings on screening endoscopy, the presence of AVMs was predictive of them as the source of GIB, if it occurred (Fig. 4).
Adverse events
Only 1 adverse event was reported during preoperative endoscopy (0.71%). The reported complication was minor by established severity criteria [9]: intraprocedural bleeding that resolved without intervention.
Discussion
We performed a multicenter retrospective study comparing the utility of preoperative endoscopy prior to LVAD placement on GIB outcomes. In our study, the preoperative endoscopy cohort had a greater incidence of GIB (36.4% vs. 24.8%) within 1 year of LVAD placement, even after controlling for known confounders. Fortunately, our study demonstrates that preoperative endoscopy is relatively safe, even though these patients are at high risk due to severe comorbidities.
The overall incidence of GIB in our study was 28.9% and 37.9% at 1 year and overall post LVAD placement, respectively—this is consistent with the existing literature [10-12]. Moreover, within the 1-year follow-up time period, 54/114 (47.4%) were hospitalized with severe bleeding—this is also consistent with available data: the mean hemoglobin decline from baseline in a previous study was 2.9±0.25 g/dL with 3.0 units of packed red blood cells transfused (IQR 2-4) per bleeding event [11]. Curiously, anticoagulation status did not affect bleeding severity, but a nonsignificant trend towards more severe bleeding was observed in those with supratherapeutic INR and greater LV distention on univariate analysis. It is known that supratherapeutic INR is associated with a greater severity of bleeding [13]. It is plausible that greater LV distention at the time of LVAD placement is associated with an increasingly narrow pulse pressure, which leads to more severe bleeding due to acquired von Willebrand disease.
In our cohort, an identified or suspected source of GIB was present in 62 (48.1%) patients, which is slightly lower than 71.5-79% reported in other studies [3,11,14]. Given that we did not collect procedure types in the bleeding cohort, it is plausible that a less aggressive evaluation could account for this lower positive rate. Nevertheless, AVMs were identified in 48 (37.2%) of those who underwent endoscopy, which is consistent with the available literature [5]. It is believed that AVM-associated bleeding is common in LVAD recipients, because of the relatively decompressed left ventricle with minimal opening of the aortic valve, which mimics flow patterns in aortic stenosis: Heyde postulated that this causes distention of the submucosal venous plexus in the gastrointestinal tract and leads to AVM formation and bleeding [15]. The other etiologies in our study, in decreasing order, were peptic disease, polyps, diverticulosis and hemorrhoids, compatible with available reports [16]. Sixty-seven (51.9%) patients did not have an identifiable source, although the data suggest that undiscovered AVMs are often the source of obscure overt GIB in this population [17]. Importantly, our data strongly suggests that a pre-LVAD finding of AVMs is predictive of AVMs as a source of GIB.
Our study confirmed known patient-specific risk factors for GIB in LVAD recipients, including age, history of GIB and presence of CKD. Given that AVMs represent a significant etiology of GIB in LVAD recipients, it is logical that age and CKD, known risk factors for AVMs, would be associated with an increased risk of gastrointestinal hemorrhage. Although PPIs are recommended for bleeding prevention [7], several studies, including ours, do not show a risk reduction, and this is understandable given that most bleeding etiologies are not prevented by PPIs.
We posit that our initial hypothesis that endoscopic evaluation would not reduce the risk of post-LVAD bleeding is logical, given that the bleeding etiologies in LVAD recipients are typically not preventable with preoperative endoscopy. Even the identification and treatment of AVMs pre-LVAD, while predictive of the potential source of GIB if it occurred in our study, are unlikely to be mitigated, because the risk factors for recurrent AVM formation and bleeding are exaggerated after LVAD placement.
Surprisingly, however, the preoperative endoscopy cohort had greater odds of bleeding after LVAD placement after controlling for known confounders. However, this probably represents a selection bias, and it is plausible that an additional unaccounted-for variable (e.g., use of non-steroidal anti-inflammatory drugs, severity of previous GIB episode) alerted the referring cardiologist/surgeon to screen the patients who are inherently at higher risk for long-term bleeding.
We acknowledge several limitations in the retrospective design of our study. For example, unaccounted-for variables may have contributed to the difference seen in bleeding events between the 2 cohorts, which affects the internal validity of the conclusions. We also relied on chart review, and did not ascertain outcomes actively (i.e., contact patients at 12 months), leaving the possibility of uncollected events outside of the medical record. Nevertheless, the strengths of our study include a relatively large cohort size in comparison to other available studies, and 3 separate institutions, which improves the potential external validity of our findings, as opposed to a single-center study. Moreover, there were few missing or incomplete variables, which mitigates the effects of information bias.
In conclusion, we conducted a multicenter retrospective study evaluating the impact of preoperative endoscopy on post-LVAD GIB and found screening was relatively safe, but was associated with a higher incidence of bleeding. Endogeneity probably accounts for this observed higher risk of GIB, but at the very least, pre-LVAD endoscopy does not appear to reduce bleeding after implantation. Further investigation is needed to identify the culprit variable(s) that can clarify the risk of bleeding after LVAD.
Summary Box
What is already known:
Gastrointestinal bleeding (GIB) is a common complication after placement of a left ventricular assist device (LVAD)
The main etiology of post-LVAD GIB is arteriovenous malformations (AVMs)
Although data to support this practice are lacking, some institutions try to mitigate post-LVAD GIB using preoperative endoscopy
What the new findings are:
Preoperative endoscopy prior to LVAD insertion was relatively safe
Preoperative endoscopic evaluation did not reduce the risk of post-LVAD bleeding
A pre-LVAD finding of AVMs was predictive of AVMs as a source of GIB
Biography
Loma Linda University Health, Loma Linda, California; Baylor College of Medicine, Houston, Texas; Prevea Health, Hobart, Wisconsin; University of Michigan, Ann Arbor, Michigan; Medical University of South Carolina, Charleston, South Carolina; University of California, Los Angeles, Los Angeles, California; The Texas Heart Institute, Houston, Texas; Baylor Scott and White Health, Central Texas Region; Michael E. DeBakey VA Medical Center, Baylor College of Medicine, Houston, Texas, USA
Footnotes
Conflict of Interest: SC has participated in advisory boards for Edwards Lifesciences, Baxter Pharmaceuticals, La Jolla Pharmaceutical Corp., & Eagle Pharmaceuticals. All other authors have no conflicts of interest
References
- 1.Chair SY, Yu DS, Ng MT, et al. Evolvement of left ventricular assist device:the implications on heart failure management. J Geriatr Cardiol. 2016;13:425–430. doi: 10.11909/j.issn.1671-5411.2016.05.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shah R, Qayed E. Outcomes and predictors of readmissions with GI bleeding in patients with left ventricular assist devices. South Med J. 2018;111:666–673. doi: 10.14423/SMJ.0000000000000883. [DOI] [PubMed] [Google Scholar]
- 3.Goldstein DJ, Aaronson KD, Tatooles AJ, et al. ADVANCE Investigators. Gastrointestinal bleeding in recipients of the HeartWare ventricular assist system. JACC Heart Fail. 2015;3:303–313. doi: 10.1016/j.jchf.2014.11.008. [DOI] [PubMed] [Google Scholar]
- 4.Malone G, Abdelsayed G, Bligh F, et al. Advancements in left ventricular assist devices to prevent pump thrombosis and blood coagulopathy. J Anat. 2023;242:29–49. doi: 10.1111/joa.13675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shrode CW, Draper KV, Huang RJ, et al. Significantly higher rates of gastrointestinal bleeding and thromboembolic events with left ventricular assist devices. Clin Gastroenterol Hepatol. 2014;12:1461–1467. doi: 10.1016/j.cgh.2014.01.027. [DOI] [PubMed] [Google Scholar]
- 6.Yin MY, Ruckel S, Kfoury AG, et al. Novel model to predict gastrointestinal bleeding during left ventricular assist device support. CircHeart Fail. 2018;11:e005267. doi: 10.1161/CIRCHEARTFAILURE.118.005267. [DOI] [PubMed] [Google Scholar]
- 7.Vedachalam S, Balasubramanian G, Haas GJ, Krishna SG. Treatment of gastrointestinal bleeding in left ventricular assist devices:A comprehensive review. World J Gastroenterol. 2020;26:2550–2558. doi: 10.3748/wjg.v26.i20.2550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Harvey L, Holley CT, John R. Gastrointestinal bleed after left ventricular assist device implantation:incidence, management, and prevention. Ann Cardiothorac Surg. 2014;3:475–479. doi: 10.3978/j.issn.2225-319X.2014.08.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events:report of an ASGE workshop. Gastrointest Endosc. 2010;71:446–454. doi: 10.1016/j.gie.2009.10.027. [DOI] [PubMed] [Google Scholar]
- 10.Dailey J, Nguyen L, Kohli A, et al. A multicenter study of left ventricular assist device-related gastrointestinal bleeding. Clin Transl Gastroenterol. 2022;13:e00526. doi: 10.14309/ctg.0000000000000526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jabbar HR, Abbas A, Ahmed M, et al. The incidence, predictors and outcomes of gastrointestinal bleeding in patients with left ventricular assist device (LVAD) Dig Dis Sci. 2015;60:3697–3706. doi: 10.1007/s10620-015-3743-4. [DOI] [PubMed] [Google Scholar]
- 12.John R, Kamdar F, Eckman P, et al. Lessons learned from experience with over 100 consecutive HeartMate II left ventricular assist devices. Ann Thorac Surg. 2011;92:1593–1599. doi: 10.1016/j.athoracsur.2011.06.081. [DOI] [PubMed] [Google Scholar]
- 13.Shingina A, Barkun AN, Razzaghi A, et al. Systematic review:the presenting international normalised ratio (INR) as a predictor of outcome in patients with upper nonvariceal gastrointestinal bleeding. Aliment Pharmacol Ther. 2011;33:1010–1018. doi: 10.1111/j.1365-2036.2011.04618.x. [DOI] [PubMed] [Google Scholar]
- 14.Morgan JA, Paone G, Nemeh HW, et al. Gastrointestinal bleeding with the HeartMate II left ventricular assist device. J Heart Lung Transplant. 2012;31:715–718. doi: 10.1016/j.healun.2012.02.015. [DOI] [PubMed] [Google Scholar]
- 15.Heyde EC. Gastrointestinal bleeding in aortic stenosis. N Engl J Med. 1958;259:196. [Google Scholar]
- 16.Draper KV, Huang RJ, Gerson LB. GI bleeding in patients with continuous-flow left ventricular assist devices:a systematic review and meta-analysis. Gastrointest Endosc. 2014;80:435–446. doi: 10.1016/j.gie.2014.03.040. [DOI] [PubMed] [Google Scholar]
- 17.Amornsawadwattana S, Nassif M, Raymer D, LaRue S, Chen CH. Video capsule endoscopy in left ventricular assist device recipients with obscure gastrointestinal bleeding. World J Gastroenterol. 2016;22:4559–4566. doi: 10.3748/wjg.v22.i18.4559. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.