

Abstract
BACKGROUND:
Due to the physical demands of work, blue-collar workers (BCW) frequently experience fatigue, musculoskeletal pain, and burnout. The purpose of this study was to determine the feasibility and utility of introducing yoga-based loosening exercises (YLE) at the workplace for improving fatigue, musculoskeletal pain, and burnout among BCW.
MATERIALS AND METHODS:
One hundred and twenty-eight BCW were randomized into a yoga group that received 40 minutes of supervised YLE daily, 5 days a week, for 1 month, followed by 1 month of unsupervised practice at home or a waitlisted control group. The Chalder Fatigue Scale (CFS), Visual Analog Scale for pain, Oldenburg Burnout Inventory (OLBI), sit-and-reach test (SRT), handgrip strength dynamometer, and the Short Form-8 (SF-8) questionnaire were measured at baseline, at the end of the first month, and at follow-up after the first month.
RESULTS:
All the participants adhered well to the YLE (≈86% at the workplace, ≈70% at home). Compared to the controls, the yoga group reported significant reductions in fatigue, pain, and burnout and significant improvements in flexibility, strength, and quality of life (P < 0.001) at all the time points.
CONCLUSION:
Our findings demonstrate that workplace yoga programs for BCW are feasible and can considerably reduce fatigue, pain, and burnout and improve their quality of life.
Keywords: Blue-collar workers, fatigue, occupational stress, quality of life, yoga
Introduction
Blue-collar workers (BCW) are primarily involved in heavy manual and repetitive work that requires a lot of physical strength.[1] Due to the nature of their work, they are often reported to have mental and physical health issues.[2,3] Fatigue, musculoskeletal pain, sleep disturbances, loss of flexibility, weakness, etc., are common in this vulnerable population,[2,3] but they go largely unaddressed. Various studies report significant absenteeism among BCW due to sickness and/or work-related strains.[4,5] BCW are being reported to have doubled the prevalence of occupational diseases compared to white-collar workers. Further, it is also postulated that the BCW from lower socioeconomic positions are likely to suffer from more work-related diseases compared to those from higher socioeconomic positions. BCW are reported to have higher odds of getting back pain, arthrosis of joints, repetitive strain injuries, burnouts, and other immune-related disorders.[6]
Besides this, the psychosocial stressors among this vulnerable population significantly contribute to both physical and economic burdens, which can impact the individual and the nation's productivity at large.[6] Therefore, job stress is considered a significant threat to the development and health of the employers, employees, and the country.[7,8] Occupational health is a significant problem in India as well, where reports suggest that Indian workers suffer from musculoskeletal disorders, respiratory disorders, ophthalmic issues, and skin disorders. Unfavorable work environments, poor lifestyles, ergonomic hazards, and demographic features such as age, sex, long working hours, and unstable economic status are attributed to be the reasons for increased occupational distress among Indian BCW.[7]
According to the International Labour Organization, almost 313 million blue-collar employees worldwide become subjected to non-life-threatening occupational hazards or diseases.[9] Therefore, restoring employees’ physical and mental health remains a primary requirement, as it can significantly boost the healthcare system and economy. Physical activity at the workplace is gaining attention across the globe as it is associated with reduced stress, absenteeism, increased job satisfaction, productivity, and well-being.[10] Additionally, a recent study suggests that physical activity after work hours improves the self-efficacy and focus on work of the employees.[11] Progressive resistance exercises, elastic band exercises, stretching exercises, and yoga are the most commonly used physical activity programs at the workplace.[12,13]
Yoga is an evidence-based mind–body practice that has been shown to have a multidimensional impact on the physical and mental health. Regular yoga practice has been shown to improve the emotional status and mental resilience, reduce stress, and negate negative psychological effects, which offer rest, relaxation, and an enhanced sense of well-being.[14,15,16] The biological processes underlying yoga's impact are mostly attributable to immunomodulation and regulatory action on the posterior hypothalamus.[17] Furthermore, yoga also has been shown to reduce the physical stress by improving the strength, flexibility, physical vigor, and sleep quality.[14,15,16,18]
Recent systematic reviews and meta-analyses on the usefulness of imparting yoga classes at the workplace have shown that yoga can reduce workplace stress and improve health-related outcomes.[19,20,21] This has been verified and validated by numerous previous studies that have reported yoga as a feasible mind–body modality that can be practiced in the workplace, as well as effective in relieving workplace stress and pain and improving psychological well-being.[13,22,23] Most of these studies published discuss either corporate wellness programs, industrial workers, or higher socioeconomic populations. No studies have been conducted to date to investigate the feasibility and effectiveness of yoga for BCW serving in informal workplaces who suffer from significant occupational health problems.
The purpose of this study was to investigate the feasibility and effectiveness of a yoga-based loosening exercises (YLE) program implemented at the workplace to reduce fatigue, pain, and burnout and improve strength, flexibility, and quality of life among BCW.
Materials and Methods
Study design and setting
This study was conducted at a private medical college in India and used a randomized waitlist control design. There were two groups: the yoga group and the waitlisted control group.
Screening criteria and randomization
All the consented participants were screened using the Chalder Fatigue Scale (CFS)[24] and those participants who had a CFS score greater than 15 were randomized to a YLE group (sukshmavyayama) or to a waitlisted control group. The randomization was conducted using the computed random software, and sequentially numbered, opaque, sealed envelope (SNOSE) technique was used to conceal the random allocation.
Intervention
The yoga group was then offered a 4-week YLE (sukshmavyayama) program, 40 minutes daily, 5 days per week, after their work hours in the evening during May/June 2022. The participants were advised to attend all the sessions, and their attendance was monitored by one of the investigators. Further, all the yoga group participants were advised to mark their own attendance at home practice in a diary during the follow-up period.
The YLE program included six sets of practices, namely: (a) neck strengthening exercises; (b) upper limb strengthening exercises; (c) chest strengthening exercises; (d) abdomen strengthening exercises; (e) waist strengthening exercises; and (f) lower limb strengthening exercises.[25] The control group did not receive any intervention during the entire trial period. They were engaged in their regular routine day-to-day activity. Both groups were followed up for a month after active intervention, during which the yoga group was advised to practice the YLE at home.
Study participants and sampling
In May 2022, BCW (housekeeping staff, gardeners, multitasking staff, and cooks) who belong to a low socioeconomic background classified using the Kuppuswamy socioeconomic scale,[26] working as a daily wager at the study site for more than 5 years, aged 25–50 years, were invited to participate in this study. Participants with a CFS score of 15, those taking analgesics, and those who already practice yoga, yoga-related activities, or any other type of exercise program once a week or more were excluded from the study.
Sample size
The study included a total of 128 participants, equally allocated between the two groups: the yoga group and the waitlisted control group [see Figure 1]. The sample size was calculated using G Power software version 3.1, by setting the alpha (α) to 0.05, the power (β) to 0.80, and the effect size to 0.5.
Figure 1.
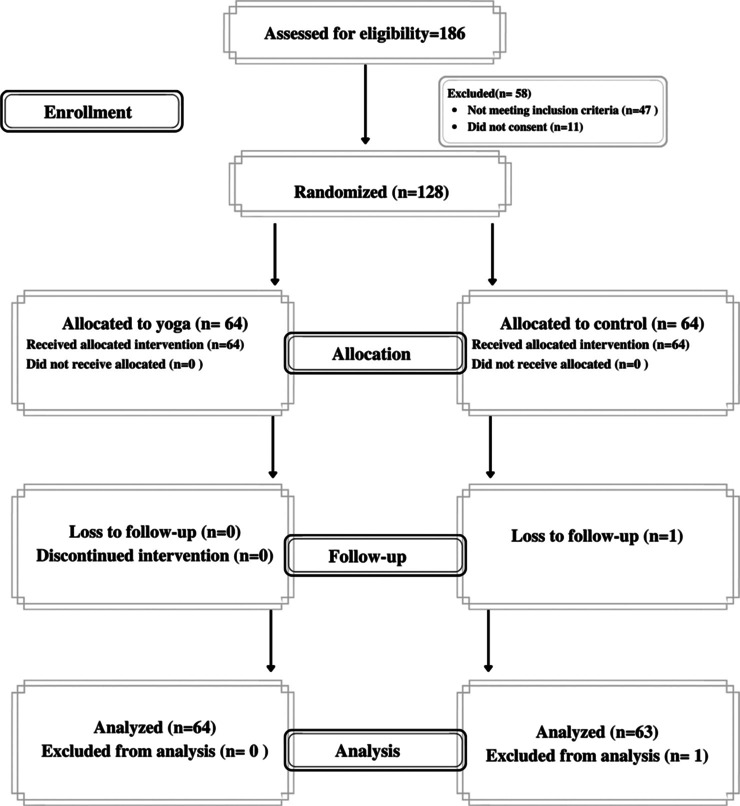
Trial profile
Data collection tool and technique
Outcome measures for fatigue (CFS), quality of life (the Short Form-8 (SF-8) questionnaire), burnout (the Oldenburg Burnout Inventory (OLBI)), hand strength (the hand grip dynamometer), and flexibility (the sit-and-reach test (SRT)) were recorded from participants from both yoga and control groups at baseline (before the first YLE class), at the end of 1 month (at the end of the last YLE class), and after 1 month.
The CFS is a self-administered, 11-item instrument commonly used in occupational research. CFS measures both physical and psychological fatigue, with higher scores indicating greater fatigue.[24] The OLBI is a 16-item inventory used to measure work-related burnout in two dimensions: exhaustion and disengagement from work, where a higher score indicates extreme burnout.[27] Both CFS and OLBI have shown strong internal validity and reliability.[24,27]
A handgrip strength dynamometer (Fitness Grips, New Delhi, India) was used to assess the handgrip strength (HGS) in both hands. HGS is used as a functional assessment tool for different muscles and is an indicator for quality daily living.[28] The SRT was performed with the participant sitting on the floor with legs stretched to the sides and then trying to stretch forward and reach as far as possible on an inch-tape. The participants were instructed to stay in the final position for 2 seconds, and the total distance reached was recorded. SRT is an indicator of hamstring and low back flexibility.[29]
The SF-8,[30] a validated questionnaire that captures the health-related quality of life under eight domains namely “general health, physical functioning, role physical, bodily pain, vitality, social functioning, mental health, and role emotional,” was used to record the quality of life of the study participants. Before the analysis, Cronbach's alpha was computed to assess the internal reliability of each of the tools, which were found to be greater than the threshold of 0.70, indicating an acceptable internal reliability.
Statistical analysis
The data were captured at baseline, post-intervention, and at 1-month follow-up in the intervention and non-intervention groups. The captured data were entered into Microsoft Excel and were exported to the Statistical Package for the Social Sciences (SPSS) version 27, for cleaning and analysis. Descriptive statistics, that is, mean, standard deviation, frequencies, and percentages, were used to descriptively report the characteristics of the sample in intervention and control groups. Before the analysis, the normality of the outcome variables (i.e. CFS score, SRT, burnout score, VAS score, HGS-right, HGS-left, SF-8 quality of life (PCS), and SF-8 quality of life (MCS)) was assessed using Kolmogorov–Smirnov test for normality. Levene's test was used to assess the homogeneity of variance in the outcome variables across intervention and control groups.
Generalized linear models (GLM) were used to capture the effect of intervention (i.e. yoga) on the study parameters. We used GLM as our data did not fit in the assumptions of normal distribution and homogeneity of variance, which are essential for parametric statistical tests such as t-test and analysis of variance (ANOVA). A total of eight GLM were developed with the post-intervention and follow-up scores as dependent variables and intervention as independent variables. The individual GLM were offset for the baseline scores of the respective outcome variables. As we used only one independent variable (i.e. intervention) in the model, we computed the main effects of yoga intervention on the post-intervention and follow-up scores. Adjusted mean difference (β) was computed to report the magnitude of intervention after offsetting for baseline differences between the groups. The significance level (α) was set at 0.05.
Ethical consideration
The study was approved by the Institutional Ethics Committee of the private medical college, and all the participants signed a written informed consent before their enrollment. The trial was registered in the Clinical Trial Registry of India (CTRI/2022/04/042083).
Results
Participant characteristics
All the participants from the yoga arm completed the study, whereas there was one dropout in the control group. The study group consisted of 81.3% females, whereas the control group had only 44.4% female participants. All the participants were married in the study group, whereas in the control group, 11% of participants were not married. According to the Kuppuswamy scale, the majority of participants in both groups belonged to the upper lower class.[31] Participants in the yoga group completed an average of 17.18 ± 2.44 yoga classes out of 20 during the study period and 13.92 ± 2.44 classes at home during the follow-up period. The detailed baseline characteristics of the group are outlined in Table 1.
Table 1.
Baseline characteristics of the study participants
| Variables | Yoga group n=64 | Waitlisted Control Group n=63 |
|---|---|---|
| Age in completed years (mean±SD) | 39.42±6.86 | 37.65±5.77 |
| Marital status | ||
| Married | 64 (100%) | 56 (88.9%) |
| Unmarried | 0 (0.0%) | 7 (11.1%) |
| Gender | ||
| Male | 12 (18.8%) | 35 (55.6%) |
| Female | 52 (81.3%) | 28 (44.4%) |
| Socioeconomic status* | ||
| Upper middle class | 0 (0.00%) | 1 (1.6%) |
| Upper lower class | 64 (100%) | 62 (98.4%) |
| Condition of pain | ||
| Upper extremity pain | 19 | 17 |
| Lower extremity pain | 40 | 36 |
| No pain | 5 | 10 |
| Sleep duration in hours (mean±SD) | 6.71±0.70 | 7.00±0.56 |
| Habits | ||
| Tea | 60 (93.75%) | 51 (80.95%) |
| Tobacco and alcohol | 0 (0.00%) | 6 (9.52%) |
| None | 4 (6.25%) | 6 (9.52%) |
| Daily working hours | 13.98±1.49 | 13.82±1.12 |
| Number of children | ||
| Up to 2 children | 48 (75.0%) | 56 (92%) |
| 3 and above | 16 (25.0%) | 7 (8%) |
SD=standard deviation, *socioeconomic status was computed based on modified Kuppuswamy scale
Changes in fatigue, burnout, and pain
GLM showed that the yoga group had significant reductions in fatigue (P < 0.001), burnout (P = 0.009), and pain (P < 0.001) compared to the waitlisted control group. These changes were consistent even after a 1-month follow-up, where the yoga group significantly had less fatigue (P < 0.001), burnout (P = 0.001), and pain (P < 0.001) compared to their controls [see Table 2].
Table 2.
Comparison of changes between the yoga group and the control group across the time points
| Study variables | Yoga group (n=64) Mean (±SD) | Control group (n=63) Mean (±SD) | Adjusted mean difference* (β) | P |
|---|---|---|---|---|
| Chalder Fatigue Scale score | ||||
| Baseline | 20.94 (±4.27) | 18.46 (±2.46) | ||
| Post-intervention | 15.55 (±2.85) | 18.67 (±1.98) | -4.86 | 0.000 |
| Follow-up | 14.70 (±4.69) | 17.75 (±1.98) | -4.76 | 0.000 |
| Sit-and-reach test | ||||
| Baseline | 32.95 (±5.54) | 31.65 (±3.84) | ||
| Post-intervention | 39.89 (±5.38) | 31.37 (±4.38) | 6.74 | 0.000 |
| Follow-up | 40.28 (±4.51) | 31.78 (±3.63) | 6.88 | 0.000 |
| Burnout score# | ||||
| Baseline | 37.44 (±4.44) | 39.46 (±4.76) | ||
| Post-intervention | 33.72 (±3.28) | 38.35 (±5.78) | -2.41 | 0.009 |
| Follow-up | 32.84 (±5.22) | 37.95 (±3.86) | -3.48 | 0.000 |
| VAS score | ||||
| Baseline | 4.58 (±2.01) | 3.54 (±2.09) | ||
| Post-intervention | 2.66 (±1.63) | 3.97 (±2.19) | -2.04 | 0.000 |
| Follow-up | 2.11 (±1.48) | 3.68 (±2.02) | -2.34 | 0.000 |
| Handgrip dynamometer-right | ||||
| Baseline | 16.73 (±10.54) | 24.27 (±13.63) | ||
| Post-intervention | 22.09 (±10.12) | 23.59 (±12.17) | 5.61 | 0.000 |
| Follow-up | 23.00 (±10.57) | 23.90 (±11.68) | 6.12 | 0.000 |
| Handgrip dynamometer-left | ||||
| Baseline | 13.78 (±9.90) | 22.70 (±14.64) | ||
| Post-intervention | 18.27 (±9.71) | 21.84 (±13.48) | 4.79 | 0.000 |
| Follow-up | 19.19 (±10.06) | 21.90 (±13.09) | 5.43 | 0.000 |
| SF-8TM health-related quality of life (PCS) | ||||
| Baseline | 9.09 (±2.42) | 10.67 (±2.41) | ||
| Post-intervention | 13.34 (±1.90) | 11.02 (±2.05) | 3.32 | 0.000 |
| Follow-up | 13.38 (±2.65) | 11.37 (±1.95) | 3.43 | 0.000 |
| SF-8TM health-related quality of life (MCS) | ||||
| Baseline | 11.23 (±2.39) | 12.70 (±2.37) | ||
| Post-intervention | 14.04 (±2.26) | 12.75 (±1.42) | 2.15 | 0.000 |
| Follow-up | 14.25 (±1.39) | 12.78 (±1.71) | 2.41 | 0.000 |
SD=standard deviation, VAS=Visual Analog Scale; SF-8=Short Form-8; PCS=physical component summary, MCS=mental component summary; #burnout was measured using Oldenburg Burnout Inventory (OLBI); the adjusted mean difference (β) represents the effectiveness of the intervention after adjusting for the baseline differences in the study variables and effect of differences in sex of participants between the groups
Changes in flexibility and strength
The yoga group had shown significant improvement in flexibility (SRT after intervention and follow-up, P < 0.001) and grip strength (HGS right and left hands, after intervention, and follow-up, P < 0.001) compared to the waitlisted group [see Table 2].
Changes in quality of life
It was also observed that there was a significant improvement both in the quality-of-life physical component score (P < 0.001) and quality-of-life mental component score (P < 0.001) at post-intervention and follow-up in the group receiving yoga intervention compared to waitlisted control.
Discussion
The results of this trial showed that a 4-week supervised YLE program resulted in significant reductions in fatigue, burnout, and pain and improved flexibility, HGS, and quality of life among a randomized group of BCW from low socioeconomic backgrounds working at a private educational institute. The effects of yoga were consistent even after 1 month of intervention, where the participants followed the same practice at home.
While yoga is well known to reduce workplace stress and pain and improve the psychological well-being,[13,32,33] no studies have evaluated the feasibility of a yoga program among BCW from low socioeconomic backgrounds to our knowledge. Further, there exist significant barriers to implementing yoga programs among low-income adults, such as unfavorable work schedules, a lack of self-confidence to practice yoga, and perceptions about the safety of yoga practices.[34] The present program was offered free of cost and was led by a team of physicians experienced in yoga. This may have motivated the participants to adhere and participate in the program.
Furthermore, poor economic conditions and a lack of physical and emotional well-being are associated with higher work-related burnout.[35] This study indicates that 40 minutes of simple YLE practice is beneficial in reducing work-related burnout. This finding may be considered important as the need for interventions that can relieve burnout among BCW is less understood and acknowledged.[36]
Our finding suggests a significant impact of YLE on the fatigue levels of the participants. This finding is interesting as YLE for 40 minutes is well accepted and did not burden the participants’ energy levels; rather, it has been shown to reduce their fatigue levels. Given the high prevalence of fatigue among BCW,[37] our findings suggest that implementing YLE can be an effective option for relieving fatigue and potentially improving work efficiency.
High physical work demands among BCW are often associated with musculoskeletal pain.[38] YLE has demonstrated that it significantly reduces pain among the study participants compared to their controls. The findings are consistent with an earlier study that found yoga can reduce pain in people suffering from chronic pain.[39] These results are further suggestive of the usefulness of YLE among BCW.
Weak HGS is often correlated with weak body strength among BCW.[40] Similarly, awkward postures, repetitive movements, etc., are reckoned to reduce flexibility and lead to musculoskeletal disorders among heavy workers.[41] Our finding suggests that YLE significantly improves both flexibility and HGS among BCW. Earlier studies also reported that introducing yoga-based stretches at the workplace can improve flexibility and HGS and may contribute to a reduction in musculoskeletal symptoms.[42]
Occupational stress and mental health have a significant role to play in improving the work ability and quality of life among BCW.[43] Furthermore, quality of life is considered an independent motivator for the employees that catalyzes their work spirit and strengthens their work capacity.[44] Our study participants reported significant improvement in both physical and mental quality of life which signifies the positive role of yoga in ameliorating occupational stress.
This study demonstrates the effectiveness of yoga program both at workplace (supervised) and at home (self-practice) on a larger sample of the vulnerable population. Attendance rates of the supervised YLE sessions (≈86%) and self-practice sessions at home (≈70%) in this study indicate that YLE is accepted by most of the study participants as a feasible and beneficial practice. Given the obstacles to implementing yoga practice among the low-socioeconomic, blue-collar population,[34] the findings of this study suggest that if yoga practices can be simplified to meet the needs of the participants, we can improve acceptability and adherence.
The plausible mechanisms by which YLE have impacted our study cohort may be through the known effects of yoga practices such as (1) immunomodulation which helps in counteracting the flight-or-fight stress response[45]; (2) stimulation of median forebrain that stimulates the centers for improved mental state[46]; (3) modulation of oxidative stress[47]; (4) and improving cardiopulmonary function by upregulating circulation and breathing.[48] However, this needs to be validated through future studies, as this study has used only a single component of yoga, that is, loosening exercises.
Limitation and recommendation
There are some limitations to this study. We used a simple random technique in this study, due to which we have an underrepresentation of men in the yoga group. This may have an effect on the outcome metrics. Further, the effect of yoga may also be confounded by the additional support, attention, and positive environment created by the introduction of yoga or by the yoga instructor. The difference in the marital status of the study group may also have influenced the outcome measures and hence may be considered a confounder.
We did not collect any data on any treatment (if undergone) outside their work hours, which may also influence the end-program scores. Additionally, we did not collect any data on the benefit of these outcomes on work efficiency and savings for the employers. This study lasted 1 month with a subsequent 1-month follow-up; however, this may not be adequate to generalize the long-term advantages as well as the sustainability of the YLE benefits. This calls for longer-term investigations with more follow-up. Further, we did not collect any data regarding the factors associated with adherence to the YLE. This could be considered a limitation. Furthermore, these data are restricted to a specific study environment, limiting the generalizability of the current findings. Despite these limitations, these study results are encouraging for introducing YLE among BCW, whose health issues are seldom addressed.
Future research may examine the usefulness of yoga using stratified randomized control designs, as well as the cost-effectiveness, economic benefits, and savings for employers. Further, it is imperative to measure whether the effectiveness of yoga programs will enhance if provided within the work hours of blue-collar employees, as in this study, the participants had to stay for an additional 40 minutes outside their work hours, which may be considered a significant factor when designing yoga programs for BCW at their workplace. Future studies may also explore about the health benefits of imparting yoga in workplace such as reduction in absenteeism due to sickness, reduction in total medical expenditures, and improvement in health behaviors. Furthermore, studies including diverse BCW from all sorts of work settings should be conducted to better understand the opportunities and obstacles of implementing YLE across the blue-collar community.
Conclusion
According to the findings of this study, simple yoga practices such as loosening exercises can be easily integrated into workplaces and have been shown to reduce fatigue, pain, and burnout, as well as improve flexibility, strength, and quality of life among BCW who are more vulnerable to occupational health hazards. Furthermore, this is the first study to show the feasibility of establishing modified yoga programs for blue-collar employees, which may have significant healthcare and economic implications.
Ethical consideration
The study was approved by the Institutional Ethics Committee of the Sant Hirdaram Medical College of Naturopathy and Yogic Sciences, Bhopal, and all the participants signed a written informed consent before their enrollment. The trial was registered in the Clinical Trial Registry of India (CTRI/2022/04/042083).
Author's contribution
Pradeep MK Nair, Jyoti Keswani, Hemanshu Sharma, Gulab Rai Tewani, and Kavita Fogawat conceptualized the study. Pradeep MK Nair, Jyoti Keswani, Kavita Fogawat, and Prakash Babu Kodali curated the data. Pradeep MK Nair and Prakash Babu Kodali performed formal analysis. Pradeep MK Nair, Jyoti Keswani, and Kavita Fogawat investigated the study. Pradeep MK Nair, Jyoti Keswani, Hemanshu Sharma, Gulab Rai Tewani, Kavita Fogawat, and Prakash Babu Kodali designed the methodology. Pradeep MK Nair, Jyoti Keswani, and Kavita Fogawat administrated the project. Hemanshu Sharma provided resources. Pradeep MK Nair, Jyoti Keswani, Hemanshu Sharma, and Gulab Rai Tewani supervised the study. Pradeep MK Nair and Prakash Babu Kodali wrote the original draft of the manuscript. Pradeep MK Nair, Jyoti Keswani, Hemanshu Sharma, Gulab Rai Tewani, Kavita Fogawat, and Prakash Babu Kodali wrote, reviewed, and edited the manuscript.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Detaille S, Reig-Botella A, Clemente M, López-Golpe J, De Lange A. Burnout and time perspective of blue-collar workers at the shipyard. Int J Environ Res Public Health. 2020;17:1–10. doi: 10.3390/ijerph17186905. doi: 10.3390/IJERPH 17186905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Åkerstedt T, Discacciati A, Häbel H, Westerlund H. Psychosocial work demands and physical workload decrease with ageing in blue-collar and white-collar workers: A prospective study based on the SLOSH cohort. BMJ Open. 2019;9:e030918. doi: 10.1136/bmjopen-2019-030918. doi: 10.1136/BMJOPEN-2019-030918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Roquelaure Y, LeManach AP, Ha C, Poisnel C, Bodin J, Descatha A, et al. Working in temporary employment and exposure to musculoskeletal constraints. Occup Med (Chic Ill) 2012;62:514–8. doi: 10.1093/occmed/kqs004. [DOI] [PubMed] [Google Scholar]
- 4.Manjunatha R, Kiran D, Thankappan KR. Sickness absenteeism, morbidity and workplace injuries among iron and steel workers-A cross sectional study from Karnataka, Southern India. Australas Med J. 2011;4:144–7. doi: 10.4066/AMJ.2011.576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Alexopoulos EC, Burdorf A. Prognostic factors for respiratory sickness absence and return to work among blue collar workers and office personnel. Occup Environ Med. 2001;58:246–52. doi: 10.1136/oem.58.4.246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.van der Molen HF, de Vries S, Sluiter JK. Occupational diseases among workers in lower and higher socioeconomic positions. Int J Environ Res Public Heal. 2018;15:2849. doi: 10.3390/ijerph15122849. doi: 10.3390/IJERPH 15122849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hwang WJ, Kim JA, Ha JS. Effects of a yoga program in reducing cardiovascular disease risk factors in workers of small workplaces: A pilot test. Sustain. 2020;12:10038. doi: 10.3390/SU122310038. [Google Scholar]
- 8.Habibi E, Hassanzadeh A, Mahaki B, Safari S, Dehghan H. Effects of work-related stress on work ability index among refinery workers. J Educ Health Promot. 2014;3:18. doi: 10.4103/2277-9531.127598. doi: 10.4103/2277-9531.127598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Walter D. International Labour Organization; May 20, 2019. India must seize the opportunity to create safe and healthy workplace. Published. Available from: http://www.ilo.org/newdelhi/info/public/fs/WCMS_703534/lang--en/index.htm . [Last accessed on 2023 Apr 18] [Google Scholar]
- 10.Marshall AL. Challenges and opportunities for promoting physical activity in the workplace. J Sci Med Sport. 2004;7:60–6. doi: 10.1016/s1440-2440(04)80279-2. [DOI] [PubMed] [Google Scholar]
- 11.ten Brummelhuis LL, Calderwood C, Rosen CC, Gabriel AS. Is physical activity before the end of the workday a drain or a gain? Daily implications on work focus in regular exercisers. J Appl Psychol. 2022;107:1864–77. doi: 10.1037/apl0000976. [DOI] [PubMed] [Google Scholar]
- 12.Todorovic N, Stajer V, Harrison B, Korovljev D, Maksimovic N, Ostojic SM. Advancing health-enhancing physical activity at workplace: Sport4Heath 2020 scientific forum. BMC Proc. 2020;14(Suppl 16):13. doi: 10.1186/s12919-020-00196-y. doi: 10.1186/S12919-020-00196-Y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hartfiel N, Burton C, Rycroft-Malone J, Clarke G, Havenhand J, Khalsa SB, et al. Yoga for reducing perceived stress and back pain at work. Occup Med (Chic Ill) 2012;62:606–12. doi: 10.1093/occmed/kqs168. [DOI] [PubMed] [Google Scholar]
- 14.Duan-Porter W, Coeytaux RR, McDuffie JR, Goode AP, Sharma P, Mennella H, et al. Evidence map of yoga for depression, anxiety, and posttraumatic stress disorder. J Phys Act Health. 2016;13:281–8. doi: 10.1123/jpah.2015-0027. doi: 10.1123/JPAH.2015-0027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Raub JA. Psychophysiologic effects of Hatha Yoga on musculoskeletal and cardiopulmonary function: A literature review. J Altern Complement Med. 2002;8:797–812. doi: 10.1089/10755530260511810. [DOI] [PubMed] [Google Scholar]
- 16.Tran MD, Holly RG, Lashbrook J, Amsterdam EA. Effects of hatha yoga practice on the health-related aspects of physical fitness. Prev Cardiol. 2001;4:165–70. doi: 10.1111/j.1520-037x.2001.00542.x. [DOI] [PubMed] [Google Scholar]
- 17.Riley KE, Park CL. How does yoga reduce stress? A systematic review of mechanisms of change and guide to future inquiry. Health Psychol Rev. 2015;9:379–96. doi: 10.1080/17437199.2014.981778. [DOI] [PubMed] [Google Scholar]
- 18.Donesky-Cuenco DA, Nguyen HQ, Paul S, Carrieri-Kohlman V. Yoga therapy decreases dyspnea-related distress and improves functional performance in people with chronic obstructive pulmonary disease: A pilot study. J Altern Complemnatry Med. 2010;15:225–34. doi: 10.1089/acm.2008.0389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Valle E Della, Palermi S, Aloe I, Marcantonio R, Spera R, Montagnani S, et al. Effectiveness of workplace yoga interventions to reduce perceived stress in employees: A systematic review and meta-analysis. J Funct Morphol Kinesiol. 2020;5:33. doi: 10.3390/jfmk5020033. doi: 10.3390/JFMK5020033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Puerto Valencia LM, Weber A, Spegel H, Bögle R, Selmani A, Heinze S, et al. Yoga in the workplace and health outcomes: A systematic review. Occup Med (Chic Ill) 2019;69:195–203. doi: 10.1093/occmed/kqz033. [DOI] [PubMed] [Google Scholar]
- 21.Shete SU, Verma A, Kulkarni DD, Bhogal RS. Effect of yoga training on inflammatory cytokines and C-reactive protein in employees of small-scale industries. J Educ Health Promot. 2017;6:76. doi: 10.4103/jehp.jehp_65_17. doi: 10.4103/jehp.jehp_65_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hartfiel N, Havenhand J, Khalsa SB, Clarke G, Krayer A. The effectiveness of yoga for the improvement of well-being and resilience to stress in the workplace. Scand J Work Environ Health. 2011;37:70–6. doi: 10.5271/sjweh.2916. [DOI] [PubMed] [Google Scholar]
- 23.Ofei-Dodoo S, Cleland-Leighton A, Nilsen K, Cloward JL, Casey E. Impact of a mindfulness-based, workplace group yoga intervention on burnout, self-care, and compassion in health care professionals: A pilot study. J Occup Environ Med. 2020;62:581–7. doi: 10.1097/JOM.0000000000001892. [DOI] [PubMed] [Google Scholar]
- 24.Jackson C. The chalder fatigue scale (CFQ 11) Occup Med (Chic Ill) 2015;65:86. doi: 10.1093/occmed/kqu168. doi: 10.1093/OCCMED/KQU168. [DOI] [PubMed] [Google Scholar]
- 25.Dhirendra B. 1st. Dhirendra Yoga Publications; 1953. Yogic Sukshma Vyayam. [Google Scholar]
- 26.Saleem SM. Modified Kuppuswamy socioeconomic scale updated for the year 2021. Indian J Foransic Community Med. 2021;8:1–3. doi: 10.18231/J.IJFCM.2021.001. [Google Scholar]
- 27.Demerouti E, Bakker AB, Vardakou I, Kantas A. The convergent validity of two burnout instruments. Eur J Psychol Assess. 2006;19:12–23. [Google Scholar]
- 28.Yorke AM, Curtis AB, Shoemaker M, Vangsnes E. The impact of multimorbidity on grip strength in adults age 50 and older: Data from the health and retirement survey (HRS) Arch Gerontol Geriatr. 2017;72:164–8. doi: 10.1016/j.archger.2017.05.011. [DOI] [PubMed] [Google Scholar]
- 29.Baltaci G, Un N, Tunay V. Comparison of three different sit and reach tests for measurement of hamstring flexibility in female university students. Br J Sport Med. 2003;37:59–61. doi: 10.1136/bjsm.37.1.59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Yiengprugsawan V, Kelly M, Tawatsupa B. SF-8TM health survey. Encycl Qual Life Well-Being Res. 2014:5940–2. [Google Scholar]
- 31.Sood P, Bindra S. Modified Kuppuswamy socioeconomic scale: 2022 update of India. Int J Community Med Public Heal. 2022;9:3841–4. [Google Scholar]
- 32.Hartfiel N, Havenhand J, Khalsa SB, Clarke G, Krayer A. The effectiveness of yoga for the improvement of well-being and resilience to stress in the workplace. Scand J Work Environ Health. 2011;37:70–6. doi: 10.5271/sjweh.2916. [DOI] [PubMed] [Google Scholar]
- 33.Wolever RQ, Bobinet KJ, McCabe K, Mackenzie ER, Fekete E, Kusnick CA, et al. Effective and viable mind-body stress reduction in the workplace: A randomized controlled trial. J Occup Health Psychol. 2012;17:246–58. doi: 10.1037/a0027278. [DOI] [PubMed] [Google Scholar]
- 34.Spadola CE, Rottapel R, Khandpur N, Kontos E, Bertisch SM, Johnson DA, et al. Enhancing yoga participation: A qualitative investigation of barriers and facilitators to yoga among predominantly racial/ethnic minority, low-income adults. Complement Ther Clin Pract. 2017;29:97. doi: 10.1016/j.ctcp.2017.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Soares JJF, Grossi G, Sundin Ö. Burnout among women: Associations with demographic/socio-economic, work, life-style and health factors. Arch Womens Ment Health. 2007;10:61–71. doi: 10.1007/s00737-007-0170-3. [DOI] [PubMed] [Google Scholar]
- 36.Malkinson R, Kushnir T, Weisberg E. Stress management and burnout prevention in female blue-collar workers: Theoretical and practical implications. Int J Stress Manag. 1997;4:183–95. [Google Scholar]
- 37.Tang FC, Li RH, Huang SL. The association between job-related psychosocial factors and prolonged fatigue among industrial employees in Taiwan. PLoS One. 2016;11:e0150429. doi: 10.1371/journal.pone.0150429. doi: 10.1371/JOURNAL.PONE.0150429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lagersted-Olsen J, Bay H, Jørgensen MB, Holtermann A, Søgaard K. Low back pain patterns over one year among 842 workers in the DPhacto study and predictors for chronicity based on repetitive measurements. BMC Musculoskelet Disord. 2016;17:1–11. doi: 10.1186/s12891-016-1307-1. doi: 10.1186/S12891-016-1307-1/TABLES/5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Schmid AA, Fruhauf CA, Sharp JL, Van Puymbroeck M, Bair MJ, Portz JD. Yoga for people with chronic pain in a community-based setting: A feasibility and pilot RCT. J Evidence-based Integr Med. 2019:24. doi: 10.1177/2515690X19863763. doi: 10.1177/2515690X19863763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Koley S, Kaur N, Sandhu JS. A study on hand grip strength in female labourers of Jalandhar, Punjab, India. J Life Sci. 2017;1:57–62. [Google Scholar]
- 41.Soares CO, Pereira BF, Pereira Gomes MV, Marcondes LP, De Campos Gomes F, De Melo-Neto JS. Preventive factors against work-related musculoskeletal disorders: Narrative review. Rev Bras Med do Trab. 2019;17:415–30. doi: 10.5327/Z1679443520190360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.De Oliveira Martins PF, Zicolau EAA, Cury-Boaventura MF. Stretch breaks in the work setting improve flexibility and grip strength and reduce musculoskeletal complaints. Mot Rev Educ Física. 2015;21:263–73. [Google Scholar]
- 43.Yi X, Yang J, Gao X, Li F. The relationship between occupational stress, mental health and work ability of coal chemical workers in Xinjiang. Front Psychiatry. 2022;13:1848. doi: 10.3389/fpsyt.2022.903534. doi: 10.3389/FPSYT.2022.903534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Leitão J, Pereira D, Gonçalves Â. Quality of work life and organizational performance: Workers’ feelings of contributing, or not, to the organization's productivity. Int J Environ Res Public Health. 2019;16:3803. doi: 10.3390/ijerph16203803. doi: 10.3390/ijerph 16203803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Arora S, Bhattacharjee J. Modulation of immune responses in stress by Yoga. Int J Yoga. 2008;1:45–55. doi: 10.4103/0973-6131.43541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Woodyard C. Exploring the therapeutic effects of yoga and its ability to increase quality of life. Int J Yoga. 2011;4:49–54. doi: 10.4103/0973-6131.85485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Martarelli D, Cocchioni M, Scuri S, Pompei P. Diaphragmatic breathing reduces exercise-induced oxidative stress. Evidence Based Complement Altern Med. 2011;2011:932430. doi: 10.1093/ecam/nep169. doi: 10.1093/ECAM/NEP169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Divya TS, Vijayalakshmi M, Mini K, Asish K, Pushpalatha M, Suresh V. Cardiopulmonary and metabolic effects of yoga in healthy volunteers. Int J Yoga. 2017;10:115. doi: 10.4103/0973-6131.186162. doi: 10.4103/0973-6131.186162. [DOI] [PMC free article] [PubMed] [Google Scholar]