

Abstract
Background
Social desirability can negatively affect the validity of self-reported measures, including underreporting of stigmatized behaviors like alcohol consumption. The Marlowe-Crowne Social Desirability Scale (SDS) is widely implemented and comprised of Denial and Attribution Domains (i.e., tendencies to deny undesirable traits or attribute socially desirable traits to oneself, respectively). Yet, limited psychometric research has been conducted in sub-Saharan Africa, where the prevalence of unhealthy alcohol consumption is high as well as religiosity and hierarchical social norms. To address this gap, we (a) conducted an exploratory study assessing certain psychometric properties of the 28-item SDS (Runyankole-translated) among persons with HIV (PWH) in Uganda, and (b) examined the relationship between social desirability and self-reported alcohol use.
Methods
We pooled baseline data (N = 1153) from three studies of PWH engaged in alcohol use from 2017 to 2021. We assessed the translated scale’s construct validity (via confirmatory factor analysis), internal consistency, item performance, differential item functioning by gender, concurrent validity with the DUREL religiosity index domains, and the association between social desirability and self-reported alcohol use.
Results
Participants had a mean age of 40.42 years, 63% were men, and 91% had an undetectable HIV viral load. The 28-item SDS had satisfactory construct validity (Model fit indices: RMSEA = 0.07, CFI = 0.84, TLI = 0.82) and internal consistency (Denial Domain ΩTotal = 0.82, Attribution Domain ΩTotal = 0.69). We excluded Item 14 (“I never hesitate to help someone in trouble”) from the Attribution Domain, which mitigated differential measurement error by gender and slightly improved the construct validity (Model fit indices: RMSEA = 0.06, CFI = 0.86, TLI = 0.85) and reliability (Attribution Domain ΩTotal = 0.72) of the 27-item modified SDS. Using the 27-item SDS, we found that social desirability was weakly correlated with religiosity and inversely associated with self-reported alcohol use after adjusting for biomarker-measured alcohol use and other confounders (β = -0.05, 95% confidence interval: -0.09 to -0.01, p-value = 0.03).
Conclusions
We detected and mitigated measurement error in the 28-item Runyankole-translated SDS, and found that the modified 27-item scale had satisfactory construct validity and internal consistency in our sample. Future studies should continue to evaluate the psychometric properties of the Runyankole-translated SDS, including retranslating Item 14 and reevaluating its performance.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12889-024-18886-z.
Keywords: Internal consistency, Reliability, Validity, Measurement error
Background
Social desirability (the tendency for someone to present themselves in a generally favorable light) is a common phenomenon globally, although it likely manifests to differing degrees across cultures [1–3]. As an important source of confounding in behavioral health research, social desirability bias in research assessments can negatively affect the validity of self-reported measures [4–7] and has been found to increase underreporting of stigmatized behaviors like alcohol consumption [8–12]. This is particularly relevant in resource-limited settings like sub-Saharan Africa, where the prevalence of alcohol consumption and HIV are high and collecting self-reported data is more feasible compared to costly biospecimens [13, 14]. Moreover, religiosity and hierarchical social norms are prevalent in parts of sub-Saharan Africa, which may influence social desirability trends [15–20].
The Marlowe-Crowne Social Desirability Scale (SDS) is a commonly implemented measure to assess social desirability, and is comprised of two domains: denial (i.e., the tendency to deny undesirable characteristics that one has or, in other words, the tendency to avoid disapproval) and attribution (i.e., the tendency to attribute or amplify socially desirable characteristics to oneself or, in other words, the tendency to seek approval) [3, 21]. While it was developed among undergraduate students in the United States [21], it has been implemented in many settings and populations globally [22, 23]. In sub-Saharan Africa, the original 33-item SDS [21] was pilot-tested in different local languages in Uganda, Kenya, Ethiopia, and Mozambique [24]. Although the languages of the translations were not specified by the authors, they found that the original scale could be shortened to a 28-item scale to exclude items that were not as relatable to participants in their study settings in sub-Saharan Africa (example of omitted item: “I never make a long trip without checking the safety of my car”). Moreover, a study in Uganda using the 13-item Marlowe-Crowne SDS Short Form C found that social desirability was inversely associated with self-reported alcohol consumption among persons with HIV (PWH) [25].
Limited psychometric research has been conducted in sub-Saharan Africa in spite of the SDS being implemented in a notably different language, population, and region from which it was originally developed [24, 25]. A valid measure of social desirability could help us better statistically control for social desirability bias, particularly in similar resource-limited settings where self-reported measures continue to be the most cost- and resource-effective [26]. To address this knowledge gap, we conducted an exploratory study assessing certain psychometric properties of the 28-item Runyankole-translated Marlowe-Crowne SDS among PWH in Uganda. We also examined the association between social desirability and self-reported alcohol use in this setting.
Methods
Study design and population
This analysis used pooled baseline data from studies in Uganda, namely the Drinkers’ Intervention to Prevent Tuberculosis (TB, DIPT, Clinical Trials Registry NCT03492216 [Date of Registration: May 2018]) randomized controlled trial (RCT) [27], the Mobile Technology to Extend Clinic-Based Counseling for HIV + s in Uganda (Extend, Clinical Trials Registry NCT03928418 [Date of Registration: April 2019]) RCT [28], and the Alcohol Drinkers’ Exposure to Preventive Therapy for TB (ADEPT-T) observational study [29].
The DIPT RCT was conducted among heavy alcohol users with HIV and TB from 2018 to 2021 and aimed to evaluate the efficacy of incentive-based approaches to decrease alcohol use and improve isoniazid medication adherence (N = 680) [27, 30]. Recruitment and screening procedures are published in detail elsewhere [27, 30]. Enrolled participants received a 6-month course of isoniazid and pyridoxine (B6) and brief alcohol and medication adherence counseling based on Uganda’s standard of care. Participants underwent 1:1:1:1 randomization to one of the following interventions: no incentives (Arm 1, control), financial incentives for no recent alcohol use (Arm 2), financial incentives for recent isoniazid medication adherence (Arm 3), or financial incentives for decreasing alcohol use and increasing isoniazid medication adherence (Arm 4). Participants completed questionnaires and provided blood and urine samples, with data collection occurring at baseline and follow-up visits.
The Extend RCT evaluated the efficacy of counseling interventions to reduce alcohol use and increase HIV viral suppression among PWH who self-reported unhealthy alcohol use (N = 272) from 2019 to 2020, with screening procedures published elsewhere [28]. Eligible participants underwent 1:1:1 randomization to one of three study arms: brief advice based on Uganda’s standard of care (Arm 1, control), in-person counseling with interim boosters delivered by phone by the counsellor (Arm 2), or in-person counseling with interim boosters delivered by two-way automated systems (short messaging services [SMS] or interactive voice response [IVR], Arm 3). Participants completed questionnaires and provided blood samples at baseline and follow-up visits.
The ADEPT-T study was conducted between 2017 and 2020 and aimed to determine the incidence of isoniazid-related toxicity among PWH who consume alcohol and whether the rate of isoniazid-related toxicity varied by quantity of alcohol consumption (N = 301) [29]. Details pertaining to recruitment and screening procedures have been published elsewhere [29]. Participants were provided a 6-month course of isoniazid and pyridoxine (B6), completed questionnaires and provided blood samples at baseline and follow-up visits.
Participants provided written informed consent, and all study procedures were approved by the Ugandan National Council for Science and Technology, the Mbarara University of Science and Technology Research Ethics Committee, the Makerere University School of Medicine Research and Ethics Committee, and the institutional review boards (IRB) at the University of California San Francisco, Boston University, and Boston Medical Center.
Data collection
In each of the studies, a third-party native Runyankole-speaker forward translated the survey from English to Runyankole. Ugandan study staff who were fluent in both Runyankole and English then back translated the survey from Runyankole to English, and discussed translations that were unclear with native English-speaking study staff based in the United States. Native Runyankole-speaking interviewers administered the baseline survey to study participants in either Runyankole or English, depending on the participant’s preference. The survey collected data on social desirability, alcohol use, religiosity, and other variables (e.g., sociodemographics). These data were measured consistently across studies using the same survey questions.
Social desirability
We used the shortened 28-item Marlowe-Crowne SDS (which had previously been used in sub-Saharan Africa) [24] rather than the 33-item scale because our Ugandan research colleagues agreed that the items omitted from the original 33-item SDS [21] would not be as relevant to individuals in Uganda and also to minimize respondent burden. We measured social desirability using binary response options (i.e., true, false, Table 1), and calculated a summed score with higher scores indicating greater levels of social desirability (range = 0–28); the 14-item Denial and 14-item Attribution Domains each had a range of possible scores from 0–14.
Table 1.
English and Runyankole-translated items from the shortened 28-item Marlowe-Crowne Social Desirability Scale
| Item (Domain) | English (original) | Runyankole (translated) |
|---|---|---|
| 1 (D) | It is sometimes hard for me to go on with my work if I am not encouraged | Obumwe nobumwe nikingumira kugumizamu nemirimo yangye naba ntatungire obushagiki |
| 2 (D) | I sometimes feel resentful when I don’t get my way | Obumwe nimpurira nayeyanga naba ntakozire ekindikwenda |
| 3 (D) | On a few occasions, I have given up doing something because I thought too little of my ability | Ahamirundi mikye etari mingi, mpanikire kugira ekinakora kyona ahabwokugira ngu nkateekateeka ngu tindikukibaasa |
| 4 (D) | There have been times when I felt like rebelling against people in authority even though I knew they were right | Hariho emirundi emwe obunahuriire ninyenda ngu nyediimire abantu abari omubushoborozi nobu ndaabe nabeire nimanya ngu bahikire |
| 5 (A) | No matter who I’m talking to, I’m always a good listener | Tikiine kakwate yaaba ngamba nooha nari oha, ndi omuhurikiza murungi |
| 6 (D) | There have been occasions when I took advantage of someone | Habeireho obwire obu nyejuniise ondiijo muntu kwetungiramu omugasho nkomuntu |
| 7 (A) | I’m always willing to admit it when I make a mistake | Buriijo naba ndi omunshobi ningikiriza |
| 8 (D) | I sometimes try to get even rather than forgive and forget | Obumwe nobumwe ningyezaho kuhoora enzigu, okukira okusaasira nanokwebwa |
| 9 (A) | I am always courteous, even to people who are disagreeable | Buriijo nimpa abantu eifubo, nangwa nobubakuba abo abantu abatarikwikirizana |
| 10 (A) | I have never been irked when people expressed ideas very different from my own | Tinkagiraga kiniga abantu bahayo ebiteekateeko byabo biine entaniso mpango nebyangye |
| 11 (D) | There have been times when I was quite jealous of the good fortune of others | Hariho emirundi obunagirira eihari emigisha mirungi yabandi |
| 12 (D) | I am sometimes irritated by people who ask favors of me | Obumwe nishunguharira abantu abarikwenda ngu mbahwere |
| 13 (A) | I have never deliberately said something that hurt someone’s feelings | Tinkagambaga kintu kyona ngyendereire kutoneka ebiteekateeko by’omuntu |
| 14 (A) | I never hesitate to go out of my way to help someone in trouble | Tikirikuntwarira bwire kuruga omubyangye ebinaba ninkora okugira ngu mpwere ondiijo muntu ori omuburemeezi |
| 15 (A) | I have never intensely disliked anyone | Tinkangaga muntu weena ekirenga |
| 16 (D) | On occasion I have had doubts about my ability to succeed in life | Bumwe, nkagira okubanganisa omukubaasa kwangye kusingura omumagara gensi egi |
| 17 (A) | I am always careful about my manner of dress | Ninkira kwegyendesereza munonga omumijwarire yangye |
| 18 (D) | I like to gossip at times | Obumwe ninkira kugambukana / kukunda orugambo |
| 19 (D) | I can remember “playing sick” to get out of something | Nimbaasa kwijuka “kwerwaza” okugira ngu ndugye omuburemeezi |
| 20 (A) | I always try to practice what I preach | Ninkira kugyezaho kuta omunkora ebindikugamba |
| 21 (A) | I don’t find it particularly difficult to get along with loud mouthed, obnoxious people | Tindikukira kukitungamu buzibu okukwatagana nabantu abarikugamba busha, nabo abatari kwemerwa |
| 22 (A) | When I don’t know something I don’t at all mind admitting it | Kundikuba ntarikumanya kintu, tindikufayo nakakye kwikiriza ngu tindikukimanya |
| 23 (D) | At times I have really insisted on having things my own way | Hariho obwire obunyangisirize ngu ebintu bikorwe nkokundikwenda |
| 24 (D) | There have been occasions when I felt like smashing things | Hariho emirundi emwe obumpuriire ninyenda ngu nyate ebintu |
| 25 (A) | I would never think of letting someone else be punished for my wrongdoings | Tinkagiraga ekyetengo kyokugira ngu omuntu ondiijo afubirwe ahabwenshobi zangye |
| 26 (A) | I never resent being asked to return a favor | Tindikufayo kugira ngu nanye mpwere nkokunahwereirwe |
| 27 (A) | I have never felt that I was punished without cause | Tinkahuriraga okugira ngu nafubirirwa busha nteine mushango / orubanja |
| 28 (D) | I sometimes think when people have a misfortune they only got what they deserved | Heine obundikuteekateeka ngu abantu kubarikugira ebigwererezi nibaba bahoorwa |
Response options in English: true, false
Translated response options in Runyankole: namazima, tikihikire
Abbreviations: A Attribution Domain of the SDS where responding “true” would be the socially desirable response, D Denial Domain of the SDS where responding “false” would be the socially desirably response
Alcohol Use
We assessed alcohol consumption using both self-reported and biomarker-measured data. We assessed self-reported alcohol use in the past 3 months using the 3-item Alcohol Use Disorders Identification Test—Consumption (AUDIT-C) [31]. We calculated a summed score, with higher scores indicating more alcohol use (range = 0–12). We also measured alcohol use with an alcohol biomarker, phosphatidylethanol (PEth), a blood-based biomarker of past month alcohol use [32–34]. Higher PEth values (ng/mL) correspond to more alcohol consumption in the past month.
Religiosity
To measure religiosity, we used the 5-item Duke University Religion (DUREL) Index which measures religious involvement across three domains (i.e., organizational religious activity, non-organizational religious activity, and intrinsic religiosity) [35, 36]. The Organizational Religious Activity and Non-Organizational Religious Activity Domains consisted of a single item with 6-point Likert-type responses. The Intrinsic Religiosity Domain contained the remaining three items and used 5-point Likert-type responses. We calculated a summed score for this last domain, with higher scores indicating greater levels of intrinsic religiosity (range = 0–15). We assessed each DUREL Index domain separately as suggested by the developers of the scale [35].
Other covariates
We collected sociodemographic data on age (years), gender (men or women), and highest year of education. We measured social support using a modified 11-item version of the Duke University-University of North Carolina Social Support Scale [37]. We measured depression using the summed scores from the 20-item Center for Epidemiological Studies Depression (CESD) Scale [38]. Participants also provided biological specimens, including assessments of HIV viral load.
Statistical analysis
Of the participants with baseline data across each of the three studies (N = 1250), our pooled analysis was restricted to those with complete social desirability data in Runyankole (N = 1153). We excluded individuals who completed the survey in English (n = 55) because phrases can have different meanings or interpretations in other languages [39] and our key objective was to assess the performance of the SDS specifically in Runyankole.
Sample characteristics
We calculated descriptive statistics (i.e., means [standard deviation, SD] or medians [interquartile range, IQR; and minimum to maximum range] for continuous variables and proportions for categorical variables) to characterize the study population in the pooled sample overall and stratified by study.
Construct validity
As previously mentioned, the Marlowe-Crowne SDS was designed to measure social desirability by assessing two components related to social desirability, namely, the tendency to avoid disapproval (captured by items in the Denial Domain) and the tendency to seek approval (captured by items in the Attribution Domain) [3, 21]. We used confirmatory factor analysis to assess whether the SDS had an underlying two-factor structure as designed, specifically by confirming whether items designed to measure avoiding disapproval loaded strongly onto the Denial Domain and whether items designed to measure seeking approval loaded strongly onto the Attribution Domain as designed [39]. We used the cfa function in the lavaan package in R [40] to generate diagonally weighted least square standard parameter estimates. We used several model fit indices to determine whether a model was a good fit for the data: Root Mean Square Error of Approximation (RMSEA, 0.01 = excellent fit, 0.05 = good fit, 0.08 = mediocre fit), Comparative Fit Index (CFI, > 0.90 indicative of good fit) and Tucker-Lewis Index (> 0.90 indicative of good fit) [41].
Internal consistency
We assessed the internal consistency of the SDS using Cronbach’s alpha [42] (via the omega function in the psych package in R [43]), given its widespread use in the literature and to allow for comparison with other studies. Cronbach alpha values above 0.70 are considered indicative of good internal consistency [39, 44], although we were cautious to interpret our findings strictly from these cutoffs given the known limitations of Cronbach’s alpha and its sensitivity to assumption violations that lead to upwardly or downwardly biased reliability estimates [44, 45]. To better understand the Cronbach’s alpha correlation coefficient, we plotted the reliability function to assess the alpha value along the spectrum of SDS scores (instead of a single point estimate averaging the correlation coefficient across all SDS scores; Supplementary Fig. 2). We also assessed internal consistency using McDonald’s omega total [46, 47] (via the omega function in the psych package in R [43]) which is considered a more robust measure of reliability [44, 48].
Item Performance
We used option characteristic curves (OCCs) to determine how well each item was performing by examining each item’s discrimination and difficulty [39, 49]. An item’s discrimination assesses how well that particular item differentiates people with different levels of social desirability. Items with high discrimination (i.e., response curves with steep slopes) are more precise than those with low discrimination. An item’s difficulty estimates the location along the continuum of social desirability where there is more than a 50% probability of endorsing that item. To endorse a difficult item (i.e., one with a location parameter towards the right or higher end of the social desirability continuum), an individual would need to have high levels of social desirability whereas they would need little social desirability to endorse an easy item. In a sample of participants with ranging social desirability levels, many participants would likely endorse easier items but fewer would endorse difficult items. As such, scales with items ranging in difficulty are better able to assess and parse out which individuals have higher levels of social desirability. We estimated OCCs using the ksIRT function in the KernSmoorthIRT package in R [50].
Differential item functioning by gender
We assessed differential item functioning (DIF) by gender, which is a way to detect differential measurement error. Assessing DIF by gender allows us to detect whether participants with the same level of social desirability responded differently to specific items due to their gender. DIF analysis assumes unidimensionality, so we assessed DIF within each SDS domain. Likelihood ratio tests were employed, where a final anchored model estimated the magnitude of significant DIF across items. This allowed us to determine whether there were any significant differences in item responses in each domain, as well as whether any significant differences were also of large magnitude [51]. We then plotted expected scale scores to assess the impact of any notable DIF on the scale overall [52].
Concurrent validity
We assessed the correlations between the SDS and each domain of the DUREL religiosity index (as recommended by its developers [35, 36]) using the pwcorr statement in STATA. We evaluated whether correlation coefficients were weak (r < 0.3), moderate (r = 0.4 – 0.6), or strong (r > 0.7) [53].
Exploratory assessment of the association between SDS and self-reported alcohol use
We assessed the association between the Runyankole-translated SDS and self-reported alcohol use to determine whether the results were consistent with previous work in Uganda [25]. We first conducted regression diagnostics and found that there were no major violations to the linear regression assumptions of linearity, homoscedasticity, and normality. We then conducted linear regression modeling AUDIT-C summed scores as a function of SDS summed scores with a random effect to account for variability between studies. In our adjusted model, we additionally adjusted for age, gender, education, depression, religiosity, and biomarker-measured alcohol use (i.e., PEth). These covariates were identified a priori from expert knowledge, and associations between these variables (i.e., age [54–57], gender [57–60], education [57, 61], depression [62–64], and religiosity [65–69]), social desirability, and alcohol use have been documented in the literature. We also adjusted for the alcohol biomarker PEth to mitigate potential measurement issues in self-reported alcohol use assessments which are prone to underreporting [70–72]. Although we theorized that social support could confound the relationship between social desirability and self-reported alcohol use given its association with both [73–75], we did not include this covariate in our adjusted models as this variable was not collected in all of the studies. We also explored the association between SDS summed scores and self-reported alcohol use stratified by study (provided in Supplementary Material).
We conducted our analyses using STATA/SE 17.0 for Windows or R (Version 4.3.1) [76]. We assumed a two-sided p < 0.05 to be statistically significant.
Results
Sample characteristics
In our pooled baseline sample of PWH (N = 1153), participants had a mean age of 40.42 years (standard deviation [SD] = 9.89), 63% were men, 64% reported some primary school education, and most of the sample (91%) had an undetectable HIV viral load (< 40 copies/mL, Table 2). Participants self-reported a mean AUDIT-C score of 5.55 (SD = 3.12), while the median PEth concentration was 190 ng/mL (IQR = 34–474 ng/mL). As expected, given their differing study eligibility criteria, participants in ADEPT-T had lower PEth values compared to those in DIPT and Extend (medians of 15 ng/mL versus 264 ng/mL and 259 ng/mL, respectively). This corresponded with the trends in self-reported alcohol use, with those in ADEPT-T self-reporting lower alcohol use (mean AUDIT-C = 2.77) compared to the participants in the other studies (mean AUDIT-C scores of 6.34 and 6.89 in DIPT and Extend, respectively).
Table 2.
Sample characteristics of persons with HIV in Uganda overall and by study, n(%)
| Characteristics | Overall (N = 1153) | Study | ||
|---|---|---|---|---|
| DIPT (n = 599) | Extend (n = 261) | ADEPT-T (n = 293) | ||
| Age (years) | ||||
| Med (IQR) | 40 (32–47) | 39 (32–47) | 40 (33–46) | 40 (33–47) |
| Mean (SD) | 40.42 (9.89) | 40.40 (10.18) | 40.24 (9.49) | 40.61 (9.68) |
| Men | 721 (63) | 408 (68) | 169 (65) | 144 (49) |
| Highest level of education | ||||
| None | 141 (12) | 99 (17) | 14 (5) | 28 (10) |
| Some primary school | 733 (64) | 387 (65) | 160 (61) | 186 (63) |
| Some secondary school | 211 (18) | 92 (15) | 61 (23) | 58 (20) |
| Vocation school | 61 (5) | 20 (3) | 24 (9) | 17 (6) |
| University | 7 (1) | 1 (< 1) | 2 (1) | 4 (1) |
| Undetectable HIV viral load | 1021 (91) | 525 (90) | 234 (90) | 262 (92) |
| Recent alcohol use | ||||
| Self-reported AUDIT-C | ||||
| Med (IQR) | 5 (3.5–8) | 6 (4–8) | 7 (4–9) | 2 (0–4) |
| Mean (SD) | 5.55 (3.12) | 6.34 (2.45) | 6.89 (2.82) | 2.77 (2.88) |
| Biomarker-measured PEth (ng/mL) | ||||
| Med (IQR) | 190 (34–474) | 264 (93–583) | 259 (68–520) | 15 (1–188) |
| Mean (SD) | 342.07 (426.01) | 416.75 (457.41) | 387.01 (438.16) | 149.39 (257.07) |
| Depression (CESD) | ||||
| Med (IQR) | 6 (1–13) | 5 (1–10) | 13 (6–28) | 3 (0–10) |
| Mean (SD) | 9.66 (11.60) | 7.44 (8.69) | 18.37 (15.48) | 6.42 (8.63) |
| Religiosity (DUREL Index) | ||||
| Organizational religious activity | ||||
| Med (IQR) | 4 (3–5) | 4 (3–5) | 4 (3–5) | 5 (4–5) |
| Mean (SD) | 3.90 (1.40) | 3.78 (1.39) | 3.85 (1.39) | 4.18 (1.40) |
| Non-organizational religious activity | ||||
| Med (IQR) | 2 (1–5) | 2 (1–4) | 2 (1–4) | 4 (1–5) |
| Mean (SD) | 2.74 (1.67) | 2.49 (1.63) | 2.63 (1.59) | 3.32 (1.69) |
| Intrinsic religiosity | ||||
| Med (IQR) | 15 (12–15) | 15 (11–15) | 12 (12–15) | 15 (14–15) |
| Mean (SD) | 12.78 (3.29) | 12.34 (3.91) | 12.72 (2.19) | 13.76 (2.41) |
Abbreviations: ADEPT-T The Alcohol Drinkers’ Exposure to Preventive Therapy for TB Study, AUDIT-C Alcohol Use Disorders Identification Test – Consumption, CESD Center for Epidemiological Studies Depression, DIPT The Drinkers’ Intervention to Prevent Tuberculosis RCT, DUREL Duke University Religion Index, Extend The Mobile Technology to Extend Clinic-Based Counseling for HIV + s in Uganda RCT, IQR Interquartile range, med median, PEth Phosphatidylethanol
28-item Runyankole-translated SDS
The 28-item Runyankole-translated SDS had a mean summed score of 19.59 (SD = 3.51, range = 8–28), and a median score of 20 (IQR = 17–22). The 14-item Denial Domain had a mean summed score of 8.39 (SD = 3.32, range = 0–14) and a median score of 9 (IQR = 6–11); the 14-item Attribution Domain had a mean summed score of 11.20 (SD = 2.16, range = 0–14) and a median score of 11 (IQR = 10–13).
Construct validity and internal consistency
In our CFA of a two-factor structure, we determined that items had acceptable factor loadings in each domain (Denial Domain: 0.50 to 0.74, Attribution Domain: 0.34 to 0.76, Table 3) and multiple fit indices indicated a satisfactory model fit (RMSEA = 0.07, CFI = 0.84, TLI = 0.82). We found good internal consistency in the Denial Domain (Omega total [Ωtotal] of 0.82 and Cronbach’s α of 0.80) and satisfactory internal consistency in the Attribution Domain (Ωtotal of 0.69 and Cronbach’s alpha of 0.63). Plotting the reliability function for the Attribution Domain revealed that Cronbach alpha values were high (~ 0.80) among individuals with Attribution Domain scores below the mean (i.e., 11.20), but lower among individuals with domain scores above the mean (Supplementary Fig. 2).
Table 3.
Construct validity and internal consistency of the Runyankole-translated Marlowe-Crowne Social Desirability Scale among persons with HIV in Uganda
| 28-item SDS | 27-item SDS | |
|---|---|---|
| Construct validity via confirmatory factor analysis | ||
| Covariance between factors | -0.34 | -0.28 |
| Factor loadings range | ||
| Denial Domain | 0.50 to 0.74 | 0.50 to 0.72 |
| Attribution Domain | 0.34 to 0.76 | 0.42 to 0.80 |
| Model fit indices | ||
| RMSEA | 0.07 | 0.06 |
| CFI | 0.84 | 0.86 |
| TLI | 0.82 | 0.85 |
| Internal consistency | ||
| Omega’s total | ||
| Denial Domain | 0.82 | 0.82 |
| Attribution Domain | 0.69 | 0.72 |
| Cronbach’s alpha | ||
| Denial Domain | 0.80 | 0.80 |
| Attribution Domain | 0.63 | 0.67 |
Abbreviations: CFI Comparative Fit Index, RMSEA Root Mean Square Error of Approximation, TLI Tucker-Lewis Index, SDS Social Desirability Scale
Item-level performance
Most items had high discrimination, as depicted by the steep slopes of the response curves in Fig. 1. We also observed that most items had low or moderate difficulty in our sample. We observed that Item 14 (“I never hesitate to go out of my way to help someone in trouble”) had certain performance issues given the undulating slopes along the x-axis of the response curves (Fig. 2). OCCs for all items are presented in Supplementary Fig. 1.
Fig. 1.

Option characteristic curves for representative items from the Runyankole-translated Marlowe-Crowne SDS. Abbreviations: SDS = Social Desirability Scale. a Item 17 (“I am always careful about my manner of dress”) is part of the Attribution Domain of the SDS. Responding “true” to Item 17 indicates more social desirability. b Item 3 (“On a few occasions, I have given up doing something because I thought too little of my ability”) is part of the Denial Domain of the SDS. Responding “false” to Item 3 indicates more social desirability
Fig. 2.
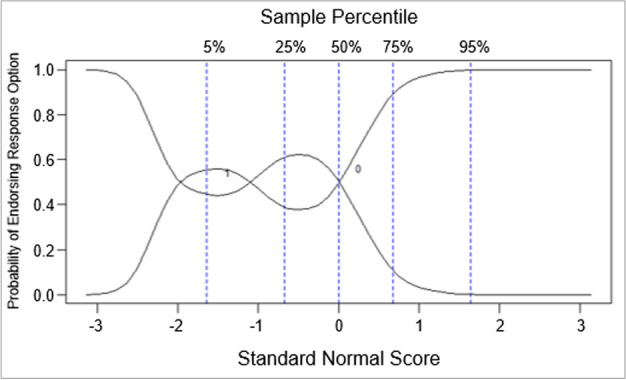
Option characteristic curve depicting performance issues in Item 14a from the Runyankole-translated Marlowe-Crowne Social Desirability Scale. a Item 14 (“I never hesitate to go out of my way to help someone in trouble”) is part of the Attribution Domain of the SDS. Responding “true” to Item 14 indicates more social desirability
Differential item functioning by gender
We did not find any notable DIF by gender in the Denial Domain, as indicated by the approximately overlapping slopes of expected test scores between men and women (Supplementary Table 3). However, we detected DIF by gender in the Attribution Domain (Table 4), and found that one particular item (i.e., Item 14) was driving this measurement error considering the significance and associated magnitude of its detected DIF (p-value = 0.002, DIF effect size = 0.678, Table 4). Given that this was the same problematic item that was identified when assessing item-level performance with OCCs, we removed it from the scale to mitigate the measurement error.
Table 4.
Assessing differential item functioning (DIF) by gender in the Attribution Domain of the Runyankole-translated Marlowe-Crowne Social Desirability Scale
| 14-item Attribution Domain | |||
| Item | P-value | DIF Effect Size | Expected Test Scores |
| 5 | 0.144 | -0.025 |
|
| 7 | 0.444 | 0.004 | |
| 9 | 0.291 | -0.163 | |
| 10 | 0.011 | -0.329 | |
| 13a | - | - | |
| 14 | 0.002 | 0.678 | |
| 15 | 0.783 | -0.189 | |
| 17 | 0.836 | -0.006 | |
| 20 | 0.960 | 0.242 | |
| 21 | 0.421 | -0.193 | |
| 22 | 0.056 | -0.053 | |
| 25a | - | - | |
| 26 | < 0.001 | 0.221 | |
| 27 | 0.502 | -0.061 | |
| Modified 13-item Attribution Domainb | |||
| Item | P-value | DIF Effect Size | Expected Test Scores |
| 5 | 0.136 | -0.020 |
|
| 7 | 0.603 | 0.029 | |
| 9 | 0.343 | -0.132 | |
| 10 | 0.023 | -0.283 | |
| 13a | - | - | |
| 15 | 0.535 | -0.142 | |
| 17a | - | - | |
| 20 | 0.945 | 0.250 | |
| 21 | 0.790 | -0.216 | |
| 22 | 0.279 | -0.078 | |
| 25 | 0.759 | 0.015 | |
| 26 | 0.006 | 0.297 | |
| 27 | 0.236 | -0.017 | |
aUsed as anchor item
bthe Attribution Domain was modified from a 14-item subscale to a 13-item subscale by removing problematic Item 14
Modified 27-item Runyankole-translated SDS
The 27-item Runyankole-translated SDS had a mean summed score of 18.95 (SD = 3.50, range = 7–27), and a median score of 19 (IQR = 16–22). The 14-item Denial Domain remained unchanged and, as such, had the same mean and median scores as reported above. After removing one item from the 14-item Attribution Domain, the subsequent 13-item Attribution Domain had a mean summed score of 10.56 (SD = 2.00, range = 0–13) and a median score of 11 (IQR = 10–12).
Construct validity and internal consistency
Excluding Item 14 seemed to slightly improve model fit in the CFA of a two-factor structure (RMSEA= 0.06, CFI = 0.86, TLI = 0.85, Table 3). Removing Item 14 (which was part of the Attribution Domain) slightly improved the internal consistency within the Attribution Domain (Ωtotal = 0.72 and Cronbach’s α = 0.67); as expected, the internal consistency coefficients from the Denial Domain remained unchanged given that no modifications were made to this domain (Ωtotal = 0.82 and Cronbach’s alpha = 0.80).
Differential item functioning by gender
We did not detect significant, notable DIF by gender in the Denial or Attribution Domains of the modified 27-item SDS (Table 4).
Concurrent validity
The modified 27-item SDS was weakly correlated (Pearson correlation coefficient = 0.08, p < 0.01) with the Organizational Religious Activity Domain of the DUREL religiosity index, as was the SDS’s 14-item Denial Domain (Pearson correlation coefficient = 0.07, p = 0.01, Table 5). The 27-item SDS’s Attribution Domain was weakly correlated (r = 0.07, p = 0.02) with the DUREL’s Intrinsic Religiosity Domain.
Table 5.
Concurrent validity between the modified 27-item Runyankole-translated Marlowe-Crowne Social Desirability Scale and the DUREL Index among persons with HIV in Uganda
| Modified 27-item SDS |
14-item Denial Domain |
Modified 13-item Attribution Domain |
||||
|---|---|---|---|---|---|---|
| Pearson correlation coefficient (r) | p-value | Pearson correlation coefficient (r) | p-value | Pearson correlation coefficient (r) | p-value | |
| DUREL Index | ||||||
| Organizational Religious Activity | 0.08 | < 0.01 | 0.07 | 0.01 | 0.03 | 0.34 |
| Non-Organizational Religious Activity | 0.00 | 0.90 | -0.02 | 0.57 | 0.03 | 0.24 |
| Intrinsic Religiosity | 0.02 | 0.48 | -0.02 | 0.51 | 0.07 | 0.02 |
Abbreviations: DUREL Duke University Religion Index, SDS Social Desirability Scale
Exploratory assessment of the association between the modified SDS and self-reported alcohol use
We found significant inverse associations between the 27-item SDS and self-reported alcohol use in our unadjusted (β = -0.08, 95% confidence interval [CI]: -0.13 to -0.04, p-value < 0.01) and adjusted (β = -0.05, 95% CI: -0.09 to -0.01, p-value = 0.03) mixed effects models (Table 6). Findings pertaining to these associations stratified by study are presented in Supplementary Table 4.
Table 6.
Mixed effectsa linear regression of the association between the modified 27-item Runyankole-translated Marlowe-Crowne Social Desirability Scale and self-reported alcohol use
| Unadjusted | Adjustedb | |||||
|---|---|---|---|---|---|---|
| β | 95% CI | p-value | β | 95% CI | p-value | |
| Self-reported alcohol use (AUDIT-C) | -0.08 | -0.13 to -0.04 | < 0.01 | -0.05 | -0.09 to -0.01 | 0.03 |
Abbreviations: AUDIT-C Alcohol Use Disorders Identification Test – Consumption, β beta coefficient, CI confidence interval
aBoth the unadjusted and adjusted models include a random effect to account for variability between studies
bAdjusted for age, gender, education, depression, religiosity, and the alcohol biomarker phosphatidylethanol
Discussion
We found that the 28-item Runyankole-translated SDS had satisfactory construct validity and internal consistency in our sample of PWH in Uganda, but discovered through further psychometric assessment that one problematic item (Item 14) was driving significant measurement error between men and women. Although removing this problematic item only marginally improved the scale’s construct validity and internal consistency, it attenuated the differential measurement bias that we detected which lends justification for using the modified 27-item SDS in this setting. Our study adds to the limited research regarding the validity and reliability of the SDS in Uganda given that we are the first to report the translated scale’s construct validity, the performance of individual items, differential item functioning by gender, and concurrent validity.
Our item-level analysis revealed a problematic item (Item 14) with subpar discrimination and difficulty, which was later identified as a key driver of differential measurement error by gender in one of the scale’s domains. Native Runyankole-speaking members of our team in Uganda provided important clarification that there may have been some translation issues with this particular item, which may have affected its performance in our sample. Through their feedback, we identified that the item in Runyankole was more translatable to “it does not take me a lot of time to stop what I am doing and help someone,” which likely altered some of the intended meaning from the original item in English (“I never hesitate to go out of my way to help someone in trouble”). The issues that we identified at the item- and scale-level justified our decision to remove Item 14 from the scale and proceed with a modified 27-item version of the translated scale. The mistranslation of Item 14 may have led to differential responses between women and men due to the subtle differences in meaning and the cultural and gender norms that are prevalent in Uganda [77–81]. The original item assesses whether someone would act “to help someone in trouble,” which is relatable to a more pressing situation where an individual might intervene to come to the aid of someone in a dire situation; this scenario may evoke a more consistent response between women and men who understand that the socially desirable response would be to always help someone in an urgent or heightened difficult situation. The subtle difference in phrasing of the Runyankole translation of Item 14, on the other hand, speaks more to an individual’s altruism in pausing their own routine (“it does not take me a lot of time to stop what I am doing…”) and support someone else (“… to help someone”); this may have been interpreted as supporting someone with something less urgent, given that people can need help for many things including minor, nonurgent tasks. Given the sociocultural norms in Uganda suggesting that women should be benevolent, submissive, nurturing, caring, and willing to prioritize the needs of their family or their community above their own, it is possible that women in our sample responded in the affirmative to this question compared to men who do not face the same type of societal expectations [77–81].
The observed mean score (18.95) for the modified 27-item SDS in our sample was comparable after rescaling (re-scaled mean score = 9.11) to the median score of 9.0 in a 2011–2014 study in Uganda using the 13-item SDS Short Form C [25]. Confirmatory factor analysis of the modified 27-item Runyankole-translated SDS suggested satisfactory construct validity, including marginally improved model fit indices compared to the 28-item SDS. Removing Item 14 also somewhat improved the scale’s reliability, indicated by the increased internal consistency coefficients in the Attribution Domain of the modified 27-item SDS. The Omega’s total (ΩTotal) coefficient for the modified 27-item SDS indicated satisfactory internal consistency, which is considered a more robust measure of reliability compared to Cronbach’s alpha [44, 48]. However, as Cronbach’s alpha is frequently cited in the literature, we further explored alpha internal consistency values in the Attribution Domain (which had a lower, average alpha value). We found fluctuations in internal consistency with better internal consistency among participants with less social desirability compared to the rest of our sample (i.e., those with scores below the mean) but lower internal consistency among participants with high levels of social desirability (i.e., those with scores above the mean). Most of our sample had high Attribution scores and Cronbach’s alpha is calculated partly as a function of the variance of individual items [42]. As such, it appears that there was low individual-item variance with which to differentiate the large proportion of our participants with high Attribution scores, which would have attenuated the alpha coefficient among this group of participants with high scores. This does not indicate that the Attribution Domain had poor internal consistency (particularly since the Omega total coefficient indicated good internal consistency), but may be more related to the method in which Cronbach’s alpha is calculated which can result in downwardly biased estimates. Future work assessing the internal consistency of the scale could consider implementing Likert-type response options (instead of the binary responses used in this study) or adding additional items to the scale, as both of these components could help to better differentiate individuals with high social desirability scores in this setting.
Using the modified 27-item SDS, we also found that social desirability was inversely associated with self-reported alcohol use (after adjusting for identified confounders including biomarker-measured alcohol use). Our findings are consistent with previous work in the same setting [25], and build on the other published evidence that social desirability is associated with misreporting [4–7].
This study had some limitations. Our study population was recruited via convenience sampling in healthcare clinics, which limits the generalizability of our findings. However, these methods were valuable to recruit a sufficient sample of our target population. Moreover, our study was not restricted to any particular setting; participants in our pooled sample were recruited across urban, semi-urban, and rural areas. We could not assess concurrent validity of the Marlowe-Crowne SDS with other social desirability measures because the studies in our pooled analysis were not designed for psychometric evaluation and these data were not collected. We assessed the concurrent validity of the SDS with religiosity, but the religiosity measure (i.e., DUREL) was not validated in Runyankole because its psychometric assessment was beyond the scope of our study. Also, we theorized that social support may confound the relationship between social desirability and self-reported alcohol use but did not adjust for this variable in our exploratory analyses because it was not collected in all of the studies. Despite these limitations, our study is a contribution to the limited psychometric research available pertaining to the Runyankole-translated SDS in this setting.
Conclusions
Although the 28-item Runyankole-translated SDS demonstrated satisfactory construct validity and internal consistency, we recommend that researchers using the current Runyankole translation of the scale remove Item 14 given that doing so mitigated observed differential measurement error by gender. The modified 27-item Runyankole-translated SDS had satisfactory construct validity and internal consistency in our sample, and can facilitate our understanding of the role of social desirability in underreporting of stigmatized behaviors like alcohol consumption in this setting. In addition to the more generalized social desirability measured in the Marlowe-Crowne SDS, it may be more nuanced to assess social desirability in relation to specific behaviors (e.g., sexual partnerships, condom use) which is an area for further research. Future studies should continue to evaluate the psychometric properties of the Runyankole-translated SDS, including evaluating whether implementing Likert-type response options or adding items to the scale may improve its performance. Although we conducted forward and back translations of the Marlowe-Crowne SDS to produce an appropriate Runyankole translation of the scale, phrases can often have different meanings or interpretations in translated languages and it would be useful for future qualitative work (including focus groups with individuals proficient in English and Runyankole) to assess whether the translated scale fully captures the intended meaning in English across all scale items or if improvements can be made. Qualitative work would also be beneficial in specifically retranslating Item 14, followed by quantitative psychometric analyses reevaluating whether its performance has improved. Although outside of the scope of this analysis, future work should consider whether the SDS performs differently in various regions in Uganda given cultural and tribal differences across the country.
Supplementary Information
Acknowledgements
We would like to thank the study participants and research staff, without whom this work would not have been possible. We would also like to thank Dr. David Strong for his methodological expertise and support.
Abbreviations
- ADEPT-T
Alcohol Drinkers’ Exposure to Preventive Therapy for TB Study
- AUDIT-C
Alcohol Use Disorders Identification Test—Consumption
- CFI
Comparative Fit Index
- DIF
Differential Item Functioning
- DIPT
Drinkers’ Intervention to Prevent Tuberculosis RCT
- DUREL
Duke University Religion Index
- Extend
Mobile Technology to Extend Clinic-Based Counseling for HIV + s in Uganda RCT
- IRB
Institutional Review Board
- IVR
Interactive voice response
- OCC
Option characteristic curve
- PEth
Phosphatidylethanol
- PWH
Persons with HIV
- RMSEA
Root Mean Square Error of Approximation
- SDS
Social Desirability Scale
- TLI
Tucker-Lewis Index
Authors’ contributions
CEDS made substantial contributions to the conception and design of the work, analysis and interpretation of the data, writing the original draft and reviewing and editing the manuscript. RF contributed to the analysis and interpretation of the data, and reviewing and editing the manuscript. NE, WM, JA, CN, AT, AKekibiina, KM, BB, NS, and AKatusiime contributed to the acquisition of the data, and reviewing and editing the manuscript. SRR and GC contributed to reviewing and editing the manuscript. JAH contributed to the conception and design of the work, interpretation of the data, and reviewing and editing the manuscript. All authors approved the submitted version of the manuscript.
Funding
This research was supported by the National Institute on Alcohol Abuse and Alcoholism with grant numbers R01AA029962, R01AA024990, U01AA026223, U01AA020776, K24AA022586, P01AA029541, and K24AA031211.
Availability of data and materials
The dataset generated for these analyses are available on reasonable request from the senior author.
Declarations
Ethics approval and consent to participate
Participants provided written informed consent for study procedures, which were approved by the Ugandan National Council for Science and Technology, the Mbarara University of Science and Technology Research Ethics Committee, the Makerere University Research Ethics Committee, and the institutional review boards (IRB) at the University of California San Francisco, Boston University, and Boston Medical Center. Research was performed in accordance with the Declaration of Helsinki.
Consent for publication
Participants provided written informed consent for study procedures, including publication of deidentified study findings.
Competing Interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Vesely S, Klöckner CA. Social desirability in environmental psychology research: three meta-analyses. Front Psychol. 2020;11:1395. doi: 10.3389/fpsyg.2020.01395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Johnson TP, Van de Vijver FJ. Social desirability in cross-cultural research. Cross-Cultural Surv Methods. 2003;325:195–204. [Google Scholar]
- 3.Holden RR, Passey J. Handbook of individual differences in social behavior. 2009. Social desirability; p. 441454. [Google Scholar]
- 4.Hewett PC, Mensch BS, Ribeiro MCSDA, Jones HE, Lippman SA, Montgomery MR, Wijgert JHVD. Using sexually transmitted infection biomarkers to validate reporting of sexual behavior within a randomized, experimental evaluation of interviewing methods. Am J Epidemiol. 2008;168(2):202–211. doi: 10.1093/aje/kwn113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mensch BS, Hewett PC, Abbott S, Rankin J, Littlefield S, Ahmed K, Cassim N, Patel S, Ramjee G, Palanee T. Assessing the reporting of adherence and sexual activity in a simulated microbicide trial in South Africa: an interview mode experiment using a placebo gel. AIDS Behav. 2011;15:407–421. doi: 10.1007/s10461-010-9791-z. [DOI] [PubMed] [Google Scholar]
- 6.Gnambs T, Kaspar K. Disclosure of sensitive behaviors across self-administered survey modes: a meta-analysis. Behav Res Methods. 2015;47:1237–1259. doi: 10.3758/s13428-014-0533-4. [DOI] [PubMed] [Google Scholar]
- 7.Nieuwkerk PT, de Boer-van der Kolk IM, Prins JM, Locadia M, Sprangers MA. Self-reported adherence is more predictive of virological treatment response among patients with a lower tendency towards socially desirable responding. London: SAGE Publications Sage UK; 2010. [DOI] [PubMed]
- 8.Tourangeau R, Yan T. Sensitive questions in surveys. Psychol Bull. 2007;133(5):859. doi: 10.1037/0033-2909.133.5.859. [DOI] [PubMed] [Google Scholar]
- 9.Vergés A. On the desirability of social desirability measures in substance use research. J Stud Alcohol Drugs. 2022;83(4):582–587. doi: 10.15288/jsad.2022.83.582. [DOI] [PubMed] [Google Scholar]
- 10.Davis CG, Thake J, Vilhena N. Social desirability biases in self-reported alcohol consumption and harms. Addict Behav. 2010;35(4):302–311. doi: 10.1016/j.addbeh.2009.11.001. [DOI] [PubMed] [Google Scholar]
- 11.Schell C, Godinho A, Cunningham JA. To thine own self, be true: Examining change in self-reported alcohol measures over time as related to socially desirable responding bias among people with unhealthy alcohol use. Substance abuse. 2021;42(1):87–93. doi: 10.1080/08897077.2019.1697998. [DOI] [PubMed] [Google Scholar]
- 12.McCambridge J, Saitz R. Rethinking brief interventions for alcohol in general practice. Bmj. 2017;356:j116. doi: 10.1136/bmj.j116. [DOI] [PubMed] [Google Scholar]
- 13.Milanzi EB, Ndasauka Y: Prevalence of alcohol addiction in Africa. In: Addiction in South and East Africa: Interdisciplinary approaches. Switzerland: Springer; 2019. p. 215–228.
- 14.World Health Organization: Alcohol - African Region. https://www.afro.who.int/health-topics/alcohol.
- 15.Uganda Bureau of Statistics. The National Population and Housing Census 2014 - Main Report. Kampala; 2016. https://www.ubos.org/wp-content/uploads/publications/03_20182014_National_Census_Main_Report.pdf.
- 16.Westoff CF, Bietsch K. Religion and reproductive behavior in sub-Saharan Africa. DHS Anal Stud. 2015(48):1–23.
- 17.Dasré A, Hertrich V. Addressing religious practices in Sub-Saharan Africa. Insights from a longitudinal study in rural Mali. Afr Popul Stud. 2020;34(1):4964–4977. [Google Scholar]
- 18.Nyakato V, RWABUKWALI CB. Couple relations, decision-making hierarchy and use of maternal health care in rural Uganda. 2013. [Google Scholar]
- 19.Bulthuis SE, Kok MC, Amon S, Agyemang SA, Nsabagasani X, Sanudi L, Raven J, Finn M, Gerold J, Tulloch O. How district health decision-making is shaped within decentralised contexts: a qualitative research in Malawi, Uganda and Ghana. Glob Public Health. 2021;16(1):120–135. doi: 10.1080/17441692.2020.1791213. [DOI] [PubMed] [Google Scholar]
- 20.Simpson S, Pérez Cañal R. Health and Hierarchy: Exploring Workforce Inequalities in Uganda and Somaliland. In: Women and Global Health Leadership: Power and Transformation. edn. Switzerland: Springer; 2022. p. 243–254.
- 21.Crowne DP, Marlowe D. A new scale of social desirability independent of psychopathology. J Consult Psychol. 1960;24(4):349. doi: 10.1037/h0047358. [DOI] [PubMed] [Google Scholar]
- 22.Perinelli E, Gremigni P. Use of social desirability scales in clinical psychology: a systematic review. J Clin Psychol. 2016;72(6):534–551. doi: 10.1002/jclp.22284. [DOI] [PubMed] [Google Scholar]
- 23.Lanz L, Thielmann I, Gerpott FH. Are social desirability scales desirable? A meta-analytic test of the validity of social desirability scales in the context of prosocial behavior. J Pers. 2022;90(2):203–221. doi: 10.1111/jopy.12662. [DOI] [PubMed] [Google Scholar]
- 24.Vu A, Tran N, Pham K, Ahmed S. Reliability of the Marlowe-Crowne social desirability scale in Ethiopia, Kenya, Mozambique, and Uganda. BMC Med Res Methodol. 2011;11(1):1–7. doi: 10.1186/1471-2288-11-162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Adong J, Fatch R, Emenyonu NI, Cheng DM, Muyindike WR, Ngabirano C, Kekibiina A, Woolf-King SE, Samet JH, Hahn JA. Social desirability bias impacts self-reported alcohol use among persons with HIV in Uganda. Alcohol Clin Exp Res. 2019;43(12):2591–2598. doi: 10.1111/acer.14218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mooney AC, Campbell CK, Ratlhagana M-J, Grignon JS, Mazibuko S, Agnew E, Gilmore H, Barnhart S, Puren A, Shade SB. Beyond social desirability bias: investigating inconsistencies in self-reported HIV testing and treatment behaviors among HIV-positive adults in North West Province, South Africa. AIDS and Behavior. 2018;22:2368–2379. doi: 10.1007/s10461-018-2155-9. [DOI] [PubMed] [Google Scholar]
- 27.Lodi S, Emenyonu NI, Marson K, Kwarisiima D, Fatch R, McDonell MG, Cheng DM, Thirumurthy H, Gandhi M, Camlin CS. The Drinkers’ Intervention to Prevent Tuberculosis (DIPT) trial among heavy drinkers living with HIV in Uganda: study protocol of a 2× 2 factorial trial. Trials. 2021;22(1):355. doi: 10.1186/s13063-021-05304-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hahn JA, Fatch R, Emenyonu NI, Sanyu N, Katusiime A, Levine B, Boscardin WJ, Chander G, Hutton H, Camlin CS. Effect of two counseling interventions on self-reported alcohol consumption, alcohol biomarker phosphatidylethanol (PEth), and viral suppression among persons living with HIV (PWH) with unhealthy alcohol use in Uganda: a randomized controlled trial. Drug Alcohol Depend. 2023;244:109783. doi: 10.1016/j.drugalcdep.2023.109783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hahn JA, Ngabirano C, Fatch R, Emenyonu NI, Cheng DM, Adong J, Tumwegamire A, Terrault NA, Linas BP, Jacobson KR. Safety and tolerability of isoniazid preventive therapy for tuberculosis for persons with HIV with and without alcohol use: a single arm trial. AIDS (London, England) 2023;37(10):1535. doi: 10.1097/QAD.0000000000003613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chamie G HJ, Kekibiina A, Emenyonu NI, Beesiga B, Marson K, Fatch R, Lodi S, Adong J, Thirumurthy H, McDonell MG, Gandhi M, Bryant K, Havlir DV, Kamya MR, Muyindike WR. Financial incentives for reduced alcohol use and increased isoniazid adherence during tuberculosis preventive therapy among people with HIV in Uganda: an open-label, factorial randomised controlled trial. Lancet Global Health Dec 2023:in press. [DOI] [PMC free article] [PubMed]
- 31.Bradley KA, DeBenedetti AF, Volk RJ, Williams EC, Frank D, Kivlahan DR. AUDIT‐C as a brief screen for alcohol misuse in primary care. Alcohol Clin Exp Res. 2007;31(7):1208–1217. doi: 10.1111/j.1530-0277.2007.00403.x. [DOI] [PubMed] [Google Scholar]
- 32.Hahn JA, Anton RF, Javors MA. The formation, elimination, interpretation and future research needs of phosphatidylethanol (PEth) for research studies and clinical practice. Alcohol Clin Exp Res. 2016;40(11):2292. doi: 10.1111/acer.13213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Helander A, Böttcher M, Dahmen N, Beck O. Elimination characteristics of the alcohol biomarker phosphatidylethanol (PEth) in blood during alcohol detoxification. Alcohol Alcohol. 2019;54(3):251–257. doi: 10.1093/alcalc/agz027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Luginbühl M, Wurst FM, Stöth F, Weinmann W, Stove CP, Van Uytfanghe K. Consensus for the use of the alcohol biomarker phosphatidylethanol (PEth) for the assessment of abstinence and alcohol consumption in clinical and forensic practice (2022 Consensus of Basel) Drug Test Anal. 2022;14(10):1800–1802. doi: 10.1002/dta.3340. [DOI] [PubMed] [Google Scholar]
- 35.Koenig HG, Büssing A. The Duke University Religion Index (DUREL): a five-item measure for use in epidemological studies. Religions. 2010;1(1):78–85. doi: 10.3390/rel1010078. [DOI] [Google Scholar]
- 36.Koenig H, Parkerson GR, Jr, Meador KG. Religion index for psychiatric research. 1997. [DOI] [PubMed] [Google Scholar]
- 37.Broadhead W, Gehlbach SH, De Gruy FV, Kaplan BH. The Duke-UNC functional social support questionnaire: measurement of social support in family medicine patients. Med Care. 1988;26:709–723. doi: 10.1097/00005650-198807000-00006. [DOI] [PubMed] [Google Scholar]
- 38.Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- 39.DeVellis RF, Thorpe CT. Scale development: Theory and applications. California: Sage Publications; 2021.
- 40.Rosseel Y. lavaan: an R package for structural equation modeling and more Version 0.5–10 (BETA) Ghent: Ghent University; 2010. [Google Scholar]
- 41.MacCallum RC, Browne MW, Sugawara HM. Power analysis and determination of sample size for covariance structure modeling. Psychol Methods. 1996;1(2):130. doi: 10.1037/1082-989X.1.2.130. [DOI] [Google Scholar]
- 42.Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297–334. doi: 10.1007/BF02310555. [DOI] [Google Scholar]
- 43.Revelle WR. psych: Procedures for personality and psychological research. 2017. [Google Scholar]
- 44.McNeish D. Thanks coefficient alpha, we’ll take it from here. Psychol Methods. 2018;23(3):412. doi: 10.1037/met0000144. [DOI] [PubMed] [Google Scholar]
- 45.Sijtsma K. On the use, the misuse, and the very limited usefulness of Cronbach’s alpha. Psychometrika. 2009;74:107–120. doi: 10.1007/s11336-008-9101-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.McDonald RP. Test theory: A unified treatment: psychology press. 2013. [Google Scholar]
- 47.Zinbarg RE, Revelle W, Yovel I, Li W. Cronbach’s α, Revelle’s β, and McDonald’s ω H: Their relations with each other and two alternative conceptualizations of reliability. Psychometrika. 2005;70:123–33. https://link.springer.com/article/10.1007/s11336-003-0974-7.
- 48.Hayes AF, Coutts JJ: Use omega rather than Cronbach’s alpha for estimating reliability. But…. Communication Methods and Measures 2020, 14(1):1–24.
- 49.Baker FB. The basics of item response theory. Maryland: ERIC; 2001.
- 50.Mazza A, Punzo A, McGuire B. KernSmoothIRT: An R package for kernel smoothing in item response theory. arXiv preprint arXiv:12111183 2012. https://arxiv.org/abs/1211.1183.
- 51.Meade AW. Guide to IRT invariance using the MIRT package in R. North Carolina State University. 2016. https://usermanual.wiki/Document/GuideToIRTinvarianceUsingMIRT10516.421019458.pdf.
- 52.Reise SP, Revicki DA. Handbook of item response theory modeling: Applications to typical performance assessment. New York and London: Routledge; 2014.
- 53.Akoglu H. User's guide to correlation coefficients. Turk J Emerg Med. 2018;18(3):91–93. doi: 10.1016/j.tjem.2018.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hitchcott PK, Penna MP, Fastame MC. Age trends in well-being and depressive symptoms: the role of social desirability. Psychiatr Q. 2020;91(2):463–473. doi: 10.1007/s11126-020-09711-y. [DOI] [PubMed] [Google Scholar]
- 55.Ausmees L, Kandler C, Realo A, Allik J, Borkenau P, Hřebíčková M, Mõttus R. Age differences in personality traits and social desirability: A multi-rater multi-sample study. J Res Pers. 2022;99:104245. doi: 10.1016/j.jrp.2022.104245. [DOI] [Google Scholar]
- 56.Keyes KM. Age, period, and cohort effects in alcohol use in the United States in the 20th and 21st centuries: Implications for the coming decades. Alcohol Res. 2022;42(1):02. doi: 10.35946/arcr.v42.1.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Burris JE, Johnson TP, O’Rourke DP. Validating self-reports of socially desirable behaviors. APOR; 2003. p. 32–36.
- 58.Dalton D, Ortegren M. Gender differences in ethics research: The importance of controlling for the social desirability response bias. J Bus Ethics. 2011;103:73–93. doi: 10.1007/s10551-011-0843-8. [DOI] [Google Scholar]
- 59.White AM. Gender differences in the epidemiology of alcohol use and related harms in the United States. Alcohol Res. 2020;40(2):01. doi: 10.35946/arcr.v40.2.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Bernardi RA, Nash J. The importance and efficacy of controlling for social desirability response bias. Ethics Behav. 2023;33(5):413–429. doi: 10.1080/10508422.2022.2093201. [DOI] [Google Scholar]
- 61.Christensen HN, Diderichsen F, Hvidtfeldt UA, Lange T, Andersen PK, Osler M, Prescott E, Tjønneland A, Rod NH, Andersen I. Joint effect of alcohol consumption and educational level on alcohol-related medical events: a Danish register-based cohort study. Epidemiology. 2017;28(6):872–879. doi: 10.1097/EDE.0000000000000718. [DOI] [PubMed] [Google Scholar]
- 62.Latkin CA, Edwards C, Davey-Rothwell MA, Tobin KE. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict Behav. 2017;73:133–136. doi: 10.1016/j.addbeh.2017.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Brière FN, Rohde P, Seeley JR, Klein D, Lewinsohn PM. Comorbidity between major depression and alcohol use disorder from adolescence to adulthood. Compr Psychiatry. 2014;55(3):526–533. doi: 10.1016/j.comppsych.2013.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.McHugh RK, Weiss RD. Alcohol use disorder and depressive disorders. Alcohol Res. 2019;40(1). https://arcr.niaaa.nih.gov/media/108/download?inline. [DOI] [PMC free article] [PubMed]
- 65.Sedikides C, Gebauer JE. Do religious people self-enhance? Curr Opin Psychol. 2021;40:29–33. doi: 10.1016/j.copsyc.2020.08.002. [DOI] [PubMed] [Google Scholar]
- 66.Sedikides C, Gebauer JE. Religiosity as self-enhancement: a meta-analysis of the relation between socially desirable responding and religiosity. Pers Soc Psychol Rev. 2010;14(1):17–36. doi: 10.1177/1088868309351002. [DOI] [PubMed] [Google Scholar]
- 67.Russell AM, Yu B, Thompson CG, Sussman SY, Barry AE. Assessing the relationship between youth religiosity and their alcohol use: A meta-analysis from 2008 to 2018. Addict Behav. 2020;106:106361. doi: 10.1016/j.addbeh.2020.106361. [DOI] [PubMed] [Google Scholar]
- 68.Lin H-C, Hu Y-H, Barry AE, Russell A. Assessing the associations between religiosity and alcohol use stages in a representative US sample. Subst Use Misuse. 2020;55(10):1618–1624. doi: 10.1080/10826084.2020.1756331. [DOI] [PubMed] [Google Scholar]
- 69.Meyers J, Brown Q, Grant B, Hasin D. Religiosity, race/ethnicity, and alcohol use behaviors in the United States. Psychol Med. 2017;47(1):103–114. doi: 10.1017/S0033291716001975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Hormes JM, Gerhardstein KR, Griffin PT. Under-reporting of alcohol and substance use versus other psychiatric symptoms in individuals living with HIV. AIDS Care. 2012;24(4):420–423. doi: 10.1080/09540121.2011.608795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Roux P, Cohen J, Lascoux-Combe C, Sogni P, Winnock M, Salmon-Ceron D, Spire B, Dabis F, Carrieri M. group A-C-Hs: Determinants of the underreporting of alcohol consumption by HIV/HCV co-infected patients during face-to-face medical interviews: the role of the physician. Drug Alcohol Depend. 2011;116(1–3):228–232. doi: 10.1016/j.drugalcdep.2010.09.025. [DOI] [PubMed] [Google Scholar]
- 72.Eyawo O, McGinnis KA, Justice AC, Fiellin DA, Hahn JA, Williams EC, Gordon AJ, Marshall BD, Kraemer KL, Crystal S. Alcohol and mortality: combining self-reported (AUDIT-C) and biomarker detected (PEth) alcohol measures among HIV infected and uninfected. JAIDS J Acquir Immune Defic Syndr. 2018;77(2):135–143. doi: 10.1097/QAI.0000000000001588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Lechner WV, Laurene KR, Patel S, Anderson M, Grega C, Kenne DR. Changes in alcohol use as a function of psychological distress and social support following COVID-19 related University closings. Addict Behav. 2020;110:106527. doi: 10.1016/j.addbeh.2020.106527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Cano MÁ, Sánchez M, Rojas P, Ramírez-Ortiz D, Polo KL, Romano E, De La Rosa M. Alcohol use severity among adult Hispanic immigrants: Examining the roles of family cohesion, social support, and gender. Subst Use Misuse. 2018;53(4):668–676. doi: 10.1080/10826084.2017.1356333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Cramer D. Social desirability, adequacy of social support and mental health. J Commun Appl Soc Psychol. 2000;10(6):465–474. doi: 10.1002/1099-1298(200011/12)10:6<465::AID-CASP571>3.0.CO;2-2. [DOI] [Google Scholar]
- 76.R Core Team . R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing; 2023. [Google Scholar]
- 77.Farago F, Eggum-Wilkens ND, Zhang L. Ugandan adolescents’ descriptive gender stereotypes about domestic and recreational activities, and attitudes about women. Youth & society. 2021;53(5):723–744. doi: 10.1177/0044118X19887075. [DOI] [Google Scholar]
- 78.Adams MK, Salazar E, Lundgren R. Tell them you are planning for the future: gender norms and family planning among adolescents in northern Uganda. Int J Gynecol Obstet. 2013;123:e7–e10. doi: 10.1016/j.ijgo.2013.07.004. [DOI] [PubMed] [Google Scholar]
- 79.Guloba DM, Katunze M, Ssewanyana DS, Ahikire P, Musiimenta DP, Boonabaana DB, Ssennono V. Gender roles and the care economy in Ugandan households: The case of Kaabong, Kabale and Kampala districts. Oxford: Oxfam; 2018.
- 80.Lundgren R, Burgess S, Chantelois H, Oregede S, Kerner B, Kågesten AE. Processing gender: lived experiences of reproducing and transforming gender norms over the life course of young people in Northern Uganda. Cult Health Sex. 2019;21(4):387–403. doi: 10.1080/13691058.2018.1471160. [DOI] [PubMed] [Google Scholar]
- 81.Vu L, Pulerwitz J, Burnett-Zieman B, Banura C, Okal J, Yam E. Inequitable gender norms from early adolescence to young adulthood in Uganda: tool validation and differences across age groups. J Adolesc Health. 2017;60(2):S15–S21. doi: 10.1016/j.jadohealth.2016.09.027. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The dataset generated for these analyses are available on reasonable request from the senior author.