

Abstract
Background
Frontotemporal lobar degeneration (FTLD) is a leading cause of dementia in individuals aged <65 years. Several challenges to conducting in-person evaluations in FTLD illustrate an urgent need to develop remote, accessible, and low-burden assessment techniques. Studies of unobtrusive monitoring of at-home computer use in older adults with mild cognitive impairment show that declining function is reflected in reduced computer use; however, associations with smartphone use are unknown.
Objective
This study aims to characterize daily trajectories in smartphone battery use, a proxy for smartphone use, and examine relationships with clinical indicators of severity in FTLD.
Methods
Participants were 231 adults (mean age 52.5, SD 14.9 years; n=94, 40.7% men; n=223, 96.5% non-Hispanic White) enrolled in the Advancing Research and Treatment of Frontotemporal Lobar Degeneration (ARTFL study) and Longitudinal Evaluation of Familial Frontotemporal Dementia Subjects (LEFFTDS study) Longitudinal Frontotemporal Lobar Degeneration (ALLFTD) Mobile App study, including 49 (21.2%) with mild neurobehavioral changes and no functional impairment (ie, prodromal FTLD), 43 (18.6%) with neurobehavioral changes and functional impairment (ie, symptomatic FTLD), and 139 (60.2%) clinically normal adults, of whom 55 (39.6%) harbored heterozygous pathogenic or likely pathogenic variants in an autosomal dominant FTLD gene. Participants completed the Clinical Dementia Rating plus National Alzheimer’s Coordinating Center Frontotemporal Lobar Degeneration Behavior and Language Domains (CDR+NACC FTLD) scale, a neuropsychological battery; the Neuropsychiatric Inventory; and brain magnetic resonance imaging. The ALLFTD Mobile App was installed on participants’ smartphones for remote, passive, and continuous monitoring of smartphone use. Battery percentage was collected every 15 minutes over an average of 28 (SD 4.2; range 14-30) days. To determine whether temporal patterns of battery percentage varied as a function of disease severity, linear mixed effects models examined linear, quadratic, and cubic effects of the time of day and their interactions with each measure of disease severity on battery percentage. Models covaried for age, sex, smartphone type, and estimated smartphone age.
Results
The CDR+NACC FTLD global score interacted with time on battery percentage such that participants with prodromal or symptomatic FTLD demonstrated less change in battery percentage throughout the day (a proxy for less smartphone use) than clinically normal participants (P<.001 in both cases). Additional models showed that worse performance in all cognitive domains assessed (ie, executive functioning, memory, language, and visuospatial skills), more neuropsychiatric symptoms, and smaller brain volumes also associated with less battery use throughout the day (P<.001 in all cases).
Conclusions
These findings support a proof of concept that passively collected data about smartphone use behaviors associate with clinical impairment in FTLD. This work underscores the need for future studies to develop and validate passive digital markers sensitive to longitudinal clinical decline across neurodegenerative diseases, with potential to enhance real-world monitoring of neurobehavioral change.
Keywords: digital, technology, remote, monitoring, cognition, neuropsychology, cognitive impairment, neurodegenerative, screening, clinical trials, mobile phone
Introduction
Background
Frontotemporal lobar degeneration (FTLD) is a common cause of dementia in individuals aged <65 years [1,2]. FTLD encompasses a group of neuropathologically distinct diseases that result in an overlapping set of dementia syndromes with heterogeneous symptoms, including those defined by primary behavior, language, or sensorimotor changes [3,4]. The timely detection of neurodegenerative diseases such as FTLD is a core public health strategy to reduce the individual, caregiver, and socioeconomic burden of dementia [5-7]. As we enter the era of disease-modifying treatments for neurodegenerative diseases, early detection is critical to identify those eligible for clinical trial participation and early treatment to slow or stop disease progression [8-10].
However, current assessment practices for detecting neurobehavioral changes associated with neurodegenerative disease are limited. In-person neuropsychological and neurological evaluations are the gold standard for determining the presence of cognitive impairment and identifying clinical phenotypes suggestive of an underlying neurodegenerative process; unfortunately, their high costs and restricted availability via specialty dementia clinics and research centers limit access for those with fewer financial resources and lower health literacy as well as those who reside in more remote geographic locations. In addition, evaluating a person at a single appointment provides only a snapshot of neurobehavioral functioning, which does not account for the dynamic nature of human behavior that fluctuates diurnally and is influenced by other dynamic factors (eg, sleep, fatigue, mood, and medications), limiting sensitivity for detecting early subtle declines [11,12]. Traditional neuropsychological assessment also lacks ecological validity because interpretations of functioning are based on task performance in a tightly controlled testing environment, which seldom reflects a patient’s typical daily experience.
Remote monitoring of health status and behavior through the use of digital health tools is a promising solution to overcome the numerous limitations of in-person assessment and has been identified as a priority by several leading health organizations, including the US Food and Drug Administration [13], the US Department of Health and Human Services [14], and the National Institutes of Health [15,16]. Passive digital monitoring in particular (ie, monitoring behavior passively and unobtrusively through remote sensors) represents a low-burden and highly scalable method for improved detection and monitoring of real-world neurobehavioral change in neurodegenerative disease. Naturalistic behavioral data collected via in-home remote sensors have shown sensitivity to clinical severity in Alzheimer disease [17-25]; for example, older adults with mild cognitive impairment exhibit significant declines in the number of days with computer use and daily time spent on the computer per day compared to those without cognitive impairment [18]. As an extension of this work, we aim to examine overall daily smartphone use and its association with clinical severity in FTLD. We focused on FTLD as a specific use case to study the construct of passively collected smartphone data in the context of a neurodegenerative disease that manifests with well-characterized neurobehavioral changes.
Objectives
Thus, the aims of this study were to (1) examine passively collected battery percentage trajectories as a proxy for smartphone use throughout the day and (2) test associations between daily battery percentage trajectories and measures of cognitive and functional impairment and neurodegeneration in FTLD. Time-stamped battery percentage data can be easily accessed through public application programming interfaces (APIs) for both iOS and Android devices and have previously been associated with smartphone use [26-28]. Although smartphone screen time or app use time may be a more face-valid measure of smartphone use, access to these data has historically been restricted on iOS devices. This has been a major barrier to accessibility in passive monitoring research because nearly 30% of smartphone users worldwide have iOS devices [29]. Thus, it is worthwhile to examine battery percentage as a more accessible proxy for overall smartphone use. Consistent with prior research on computer use in older adults with cognitive impairment, we hypothesized that individuals with greater FTLD overall disease severity (ie, more severe functional impairment, worse cognitive performance, greater neuropsychiatric symptoms, and more brain atrophy) would demonstrate lower levels of daily smartphone use.
Methods
Participants
Participants were enrolled in the ARTFL (Advancing Research and Treatment of Frontotemporal Lobar Degeneration) study and LEFFTDS (Longitudinal Evaluation of Familial Frontotemporal Dementia Subjects) Longitudinal Frontotemporal Lobar Degeneration (ALLFTD) Mobile App study through the multisite ALLFTD (NCT04363684) study and University of California San Francisco studies of FTLD (AG038791, AG062422, and AG019724), as described previously [30]. The participants were those who had a referring diagnosis of an FTLD clinical syndrome or those who were members of a family with a strong family history of an FTLD syndrome. Additional inclusion criteria were as follows: (1) aged ≥18 years, (2) access to a smartphone, and (3) English reported as the primary language. Participants were asked to use their own smartphones. Recruitment primarily targeted those with Clinical Dementia Rating Dementia Staging Instrument plus National Alzheimer’s Coordinating Center Frontotemporal Lobar Degeneration Behavior and Language Domains (CDR+NACC FTLD) global scores of <2, but participants who were more severely impaired were not excluded. Data for this study were collected from August 2020 to April 2023. During this period, 257 participants were enrolled and logged into the ALLFTD Mobile App on their personal smartphones. Participants were only included in this secondary analysis of the ALLFTD Mobile App study if they had at least 14 continuous days of passive smartphone monitoring data, consistent with prior digital phenotyping studies attempting to capture typical daily behavior [31]. Thus, of the initial 257 participants, 231 (89.9%) were included in the final sample after 26 (10.1%) participants were excluded because they first logged in <14 days before the date on which these data were pulled in April 2023. Of these 231 participants, 92 (39.8%) were classified as having neurobehavioral symptoms at the prodromal stage (ie, no functional impairment) or fully symptomatic (ie, with functional impairment) level of severity that are consistent with an FTLD-related clinical phenotype per conference consensus with neurologists and neuropsychologists following published criteria [32-35]. Participants who were symptomatic had either sporadic FTLD or a confirmed pathogenic or likely pathogenic variant in an autosomal dominant FTLD gene (ie, a pathogenic expansion in the chromosome 9 open reading frame 72 [C9orf72] gene or a known pathogenic or likely pathogenic variant in the progranulin (GRN) or microtubule-associated protein tau [MAPT] genes; conducted as described previously [36]). The remaining participants (139/231, 60.2%) were asymptomatic clinically normal family members of the prodromal or symptomatic individuals who (1) carried a pathogenic or likely pathogenic FTLD gene variant (55/139, 39.6%), (2) tested negative for known pathogenic or likely pathogenic FTLD variants (50/139, 36%), or (3) did not yet have results available from genetic testing (34/139, 24.5%).
Ethical Considerations
The study was approved by a centralized single institutional review board at Johns Hopkins Medicine (IRB # 20-29891), and all participants provided written informed consent.
Measures
Passively Monitored Smartphone Battery Percentage
We used the first 30 days of participants’ smartphone data for this study with the goal of understanding whether approximately 1 month of smartphone monitoring could reflect baseline neurobehavioral status without capturing longitudinal disease-related decline [18,37]. Participants downloaded the ALLFTD Mobile App onto their personal smartphones. The app is designed to deliver both active mobile cognitive assessments and passively collect smartphone use data [30], including battery percentage. The ALLFTD Mobile App was programmed to collect battery percentage every 15 minutes. Due to some variability around this timing in the actual data collected (ie, some missing data points and some data collected over shorter intervals), data were aggregated to reflect the average battery percentage per hour of each study day per participant. This resulted in a comparable number of data points per day across participants. The ALLFTD Mobile App also recorded information about participants’ smartphone model, which was used to estimate the age of the smartphone (ie, calculated on the basis of the smartphone model release date and the first date of participation in this study).
Functional, Cognitive, and Neuropsychiatric Assessment
All participants underwent comprehensive functional and cognitive assessment at a parent study visit at the beginning of their smartphone monitoring study period. Informant and participant interviews were conducted to characterize the level of cognitive and everyday functioning impairment using the CDR+NACC FTLD scale [38], which is a validated, modified version of the CDR [39] that has higher sensitivity to functional impairment in FTLD. CDR+NACC FTLD global scores [40] were used to categorize participants into disease severity groups: 0=unimpaired, 0.5=prodromal, and ≥1=symptomatic. Domain-specific cognitive functioning was assessed via a comprehensive battery of well-validated neuropsychological tests. The previously published Uniform Data Set (Version 3) Executive Function composite score was used as our measure of executive functioning, comprising Trail Making Test A and B, phonemic fluency (generating words beginning with F and L), number span backwards, and category fluency (animals and vegetables) [41,42]. Sample-based z scores were calculated for indices of memory, including immediate and delayed free recall on the California Verbal Learning Test-3 Brief Form [43], as well as Benson Complex Figure Delayed Recall [44,45]. A composite memory z score was created by taking the mean of the z scores across these memory tests. Language functioning was assessed via the Multilingual Naming Test [46]. Visuospatial functioning was assessed via the Benson Complex Figure Copy [45]. Informants also completed the Neuropsychiatric Inventory [47] to assess the presence and severity of neuropsychiatric symptoms in participants.
Neuroimaging
Of the 231 participants, a subset (n=189, 81.8%) completed neuroimaging. Participants were scanned on 3 Tesla magnetic resonance imaging (MRI) scanners. T1-weighted images were acquired as magnetization-prepared rapid gradient echo images using the following parameters: 240×256×256 matrix; approximately 170 slices; voxel size=1.05×1.05×1.25 mm3; and flip angle, echo time, and repetition time varied by vendor. A standard imaging protocol was used across all centers, and all images were reviewed for quality by a core group at the Mayo Clinic, Rochester, Minnesota, United States. Details of image acquisition, processing, and harmonization have been published elsewhere [48]. Total gray matter volume was used as the primary neuroimaging variable of interest. Total intracranial volumes were regressed out (using a simple linear regression with gray matter volume as outcome and total intracranial volume as the only predictor) before inclusion in analyses to account for interindividual volumetric differences in head size on gray matter volume.
Statistical Analyses
Differences in demographic and clinical characteristics across the CDR+NACC FTLD–defined disease severity groups were tested with 1-way ANOVA and chi-square tests for continuous variables and categorical variables, respectively. Raw battery percentage data were plotted against the time of day to inform statistical analysis. Linear mixed effects (LME) regression models were then used to model the linear, quadratic, and cubic effects of time (ie, hour of the day; 0=midnight; 23=11 PM) on battery percentage. Person-specific random intercepts and random effects of time (linear, quadratic, and cubic) were modeled. To determine whether daily patterns of battery percentage trajectories (ie, a proxy for smartphone use) varied as a function of FTLD disease severity, LME models examined linear, quadratic, and cubic effects of time and their interaction with each measure of disease severity separately (ie, CDR+NACC FTLD group, cognitive domain z scores, neuropsychiatric symptoms, and whole brain gray matter volumes). All LME models covaried for age, sex, smartphone type (iOS vs Android), and estimated smartphone age (calculated on the basis of the smartphone model release date and the first date of participation in this study). A post hoc sensitivity analysis was conducted in a subset of participants (162/231, 70.1%) whose age range was matched across the CDR+NACC FTLD groups. To understand whether subtle differences in neurobehavioral functioning related to daily smartphone battery use trajectories in an unimpaired sample, we conducted additional sensitivity analyses, which repeated all models in the subset of participants who were clinically normal (139/231, 60.2%). Regression estimates are reported as standardized betas, which represent the predicted change in the outcome as a function of each predictor in units of SDs. All analyses were performed using R (version 4.2.0; R Foundation for Statistical Computing). The lme4 package was used to conduct the LME regressions [49].
Results
Participant Characteristics
Table 1 shows demographic and clinical characteristics by disease severity group. Participants had a mean age of 52.5 (SD 14.9) years and a mean of 16 (SD 2.2) years of education. Of the 231 participants, 94 (40.7%) were men, and 223 (96.5%) identified as non-Hispanic White. Nearly three-fourths of the participants (171/231, 74%) had results of genetic testing available, of whom 45% (77/171) had heterozygous pathogenic or likely pathogenic variants in an FTLD gene. Clinically normal participants were statistically significantly younger (P<.001) and more likely to be women (P<.001) than those with prodromal or symptomatic FTLD, consistent with the larger parent study samples (ALLFTD Mobile App study [30]; ALLFTD [40,50]). There were no other clear imbalances in other demographic and clinical characteristics across the 3 groups. Overall, participants had a mean of 28.3 (SD 4.19; range 14-30) days of smartphone monitoring data. On average, participants’ smartphones were 2.8 (SD 1.53; range 0-7) years old.
Table 1.
Participant characteristics by disease severity group (n=231).
|
|
A (clinically normal; n=139) | B (prodromal; n=49) | C (symptomatic; n=43) | P value | Pairwise comparisonsa |
||||||||||||||||||
| Demographics | |||||||||||||||||||||||
|
|
Age (years), mean (SD) | 46.3 (13.9) | 59.7 (12.1) | 64.3 (9.3) | <.001 | A<B, C | |||||||||||||||||
|
|
Sex (male), n (%) | 41 (29.5) | 30 (61.2) | 23 (53.5) | <.001 | A<B, C | |||||||||||||||||
|
|
Education (years), mean (SD) | 16.3 (2.1) | 16.5 (2.4) | 16.7 (2.4) | .61 | N/Ab | |||||||||||||||||
|
|
Race and ethnicity (non-Hispanic White), n (%) | 134 (96.4) | 48 (98) | 41 (95.3) | .79 | N/A | |||||||||||||||||
| Study characteristics | N/A | ||||||||||||||||||||||
|
|
Total study days, mean (SD) | 28.3 (4.2) | 28.1 (4.3) | 28.6 (4.2) | .88 |
|
|||||||||||||||||
|
|
Smartphone type, n (%) | .42 |
|
||||||||||||||||||||
|
|
|
iOS | 97 (69.8) | 37 (75.5) | 27 (62.8) |
|
|
||||||||||||||||
|
|
|
Android | 42 (30.2) | 12 (24.5) | 16 (37.2) |
|
|
||||||||||||||||
|
|
Estimated smartphone age (years), mean (SD) | 2.7 (1.5) | 3.0 (1.5) | 2.9 (1.6) | .30 |
|
|||||||||||||||||
|
|
Genetic status |
|
|||||||||||||||||||||
|
|
|
Genetic testing results, n (%) | .56 |
|
|||||||||||||||||||
|
|
|
|
Not available | 34 (24) | 13 (26.5) | 13 (30.2) |
|
|
|||||||||||||||
|
|
|
|
Available | 105 (75.5) | 36 (73.5) | 30 (69.8) |
|
|
|||||||||||||||
|
|
|
|
|
Mutation carrier | 55 (52.4) | 15 (41.7) | 7 (23.3) |
|
|
||||||||||||||
|
|
|
|
|
|
C9orf72c | 29 (52.7) | 8 (53.3) | 3 (42.9) |
|
|
|||||||||||||
|
|
|
|
|
|
GRNd | 7 (12.7) | 1 (6.7) | 0 (0) |
|
|
|||||||||||||
|
|
|
|
|
|
MAPTe | 16 (29.1) | 6 (40) | 3 (42.9) |
|
|
|||||||||||||
|
|
|
|
|
|
Otherf | 3 (5.5) | 0 (0) | 1 (14.3) |
|
|
|||||||||||||
|
|
Clinical phenotype | N/A |
|
||||||||||||||||||||
|
|
|
Mild cognitive impairmentg | N/A | 39 (79.6) | N/A |
|
|
||||||||||||||||
|
|
|
bvFTDh | N/A | N/A | 25 (58.1) |
|
|
||||||||||||||||
|
|
|
svPPAi | N/A | N/A | 6 (14) |
|
|
||||||||||||||||
|
|
|
nfvPPAj | N/A | N/A | 3 (7) |
|
|
||||||||||||||||
|
|
|
lvPPAk | N/A | N/A | 1 (2.3) |
|
|
||||||||||||||||
|
|
|
PSP-RSl | N/A | 3 (6.1) | 4 (9.3) |
|
|
||||||||||||||||
|
|
|
CBSm | N/A | 2 (4.1) | 2 (4.7) |
|
|
||||||||||||||||
|
|
|
Othern | N/A | 5 (10.2) | 2 (4.7) |
|
|
||||||||||||||||
aPairwise comparisons were evaluated with the Tukey honestly significant difference test.
bN/A: not applicable.
cC9orf72: chromosome 9 open reading frame 72.
dGRN: progranulin.
eMAPT: microtubule-associated protein tau.
fIdentified pathogenic or likely pathogenic variants in genes less commonly identified as genetic causes of frontotemporal lobar degeneration (FTLD; ie, other than C9orf72, GRN, or MAPT). The specific genetic variant is not provided to protect participant anonymity.
gIncludes behavior-, cognitive-, and language-predominant mild cognitive impairment syndromes.
hbvFTD: behavioral variant frontotemporal dementia.
isvPPA: semantic variant primary progressive aphasia.
jnfvPPA: nonfluent variant primary progressive aphasia.
klvPPA: logopenic variant primary progressive aphasia.
lPSP-RS: progressive supranuclear palsy–Richardson syndrome.
mCBS: corticobasal syndrome.
nIncludes FTLD-amyotrophic lateral sclerosis or a change in neurobehavior that may not meet full diagnostic criteria for any particular FTLD syndrome.
Daily Smartphone Battery Percentage
Visualization of the raw battery percentage data by the time of day (Figure 1) shows a nonlinear trajectory such that, on average, battery percentage increased from midnight to approximately 6 AM, then decreased until about 7 PM, and then increased again through 11 PM. These temporal patterns presumably represent typical patterns of charging and charge use of the smartphone throughout the day. Multimedia Appendix 1 presents raw battery percentage data by disease severity group. The shape of these raw data motivated consideration of a cubic model. Thus, we first tested the fit of the LME regression modeling the linear, quadratic, and cubic effects of the time of day on battery percentage, covarying for age, sex, smartphone type, and estimated smartphone age. The cubic model’s conditional pseudo-R2 (ie, the proportion of variance explained by both fixed and random factors) was 0.37. The likelihood ratio tests indicated that the full cubic model had statistically significantly better fit than LME regressions modeling only the linear (χ22=4283.6; P<.001) and quadratic (χ21=4118.8; P<.001) effects of time.
Figure 1.
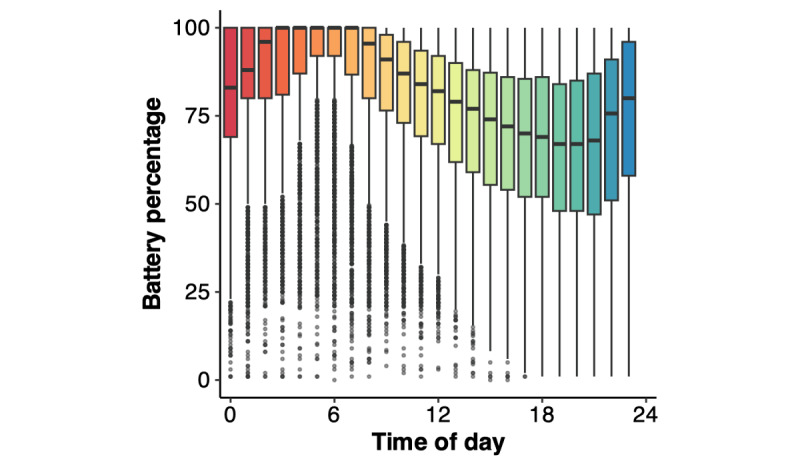
Visualization of raw battery percentage data for all participants binned by time of day (0=midnight; 23=11 PM).
LME regression indicated that the interactions between disease severity group and the linear, quadratic, and cubic effects of the time of day were associated with battery percentage (Table 2). Visualization of model results suggests that participants with prodromal FTLD and those with symptomatic FTLD had flatter battery curves throughout the day (ie, shallower decreases from maximum to minimum battery percentage as well as a higher minimum battery percentage; a proxy for less smartphone use) than clinically normal participants on average (Figure 2). Examination of pairwise disease severity group contrasts showed that participants with symptomatic FTLD also had significantly less battery use than participants with prodromal FTLD (P=.003 or P<.001 in all cases).
Table 2.
Linear mixed effects regression results showing significant relationships between disease severity groups and battery percentage trajectories throughout the day.
|
|
β (95% CI) | P value |
| Baseline age | .06 (.00 to .13) | .047 |
| Sex (reference: female) | −.03 (−.14 to .08) | .62 |
| Smartphone type (reference: Android) | .01 (−.11 to .12) | .89 |
| Estimated smartphone age | −.04 (−.08 to −.01) | .03 |
| Time of day (linear) | 1.74 (1.66 to 1.83) | <.001 |
| Time of day (quadratic) | −5.27 (−5.45 to −5.09) | <.001 |
| Time of day (cubic) | 3.28 (3.17 to 3.40) | <.001 |
| Prodromal (reference: normal) | .24 (.10 to .39) | .001 |
| Symptomatic (reference: normal) | .27 (.11 to .43) | .001 |
| Time of day (linear)×prodromal | −.23 (−.40 to −.07) | .006 |
| Time of day (linear)×symptomatic | −.56 (−.73 to −.38) | <.001 |
| Time of day (quadratic)×prodromal | .88 (.53 to 1.24) | <.001 |
| Time of day (quadratic)×symptomatic | 1.65 (1.29 to 2.01) | <.001 |
| Time of day (cubic)×prodromal | −.58 (−.81 to −.36) | <.001 |
| Time of day (cubic)×symptomatic | −.99 (−1.22 to −.76) | <.001 |
Figure 2.
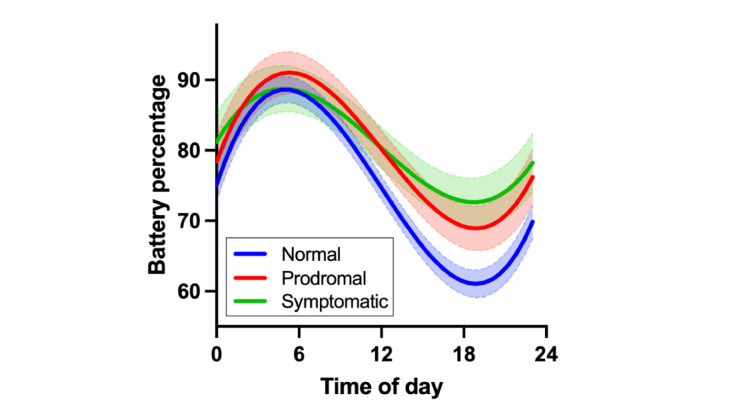
Participants with prodromal frontotemporal lobar degeneration (FTLD) and those with symptomatic FTLD had flatter battery curves throughout the day (ie, a proxy for less smartphone use) than clinically normal participants on average. Error bands represent pointwise 95% CIs.
Similar patterns emerged when examining all other indices of clinical severity. Each cognitive domain statistically significantly moderated the relationship between the time of day and battery percentage such that participants with worse cognitive functioning had flatter battery curves throughout the day, suggesting less smartphone use (Table 3 [executive functioning, memory, language, and visuospatial skills]; Figures 3A-3D). Neuropsychiatric symptom severity also moderated the relationship between the time of day and battery percentage such that participants with higher neuropsychiatric symptom ratings had flatter battery curves throughout the day, suggesting less smartphone use (Table 3 [neuropsychiatric symptoms]; Figure 3E). Examination of each Neuropsychiatric Inventory item (yes or no) in separate LME models suggested that participants with agitation, depression, apathy, disinhibition, irritability, motor disturbance, nighttime behaviors, and changes in appetite had less smartphone use (Table 4). Delusions, hallucinations, anxiety, and elation did not statistically significantly relate to battery use trajectories throughout the day (Table 4). Finally, total gray matter volume also moderated the relationship between the time of day and battery percentage such that participants with smaller gray matter volumes had flatter battery curves throughout the day, suggesting less smartphone use (Table 3 [gray matter volume]; Figure 3F). Of all indices of clinical severity presented in Table 3, executive functioning and total gray matter volume appeared to have the largest effect sizes on smartphone battery trajectories.
Table 3.
Results of separate linear mixed effects regression models showing significant relationships between battery percentage trajectories throughout the day and executive functioning, memory, language, visuospatial skills, neuropsychiatric symptoms, and whole brain gray matter volume (lower order terms and covariates are not displayed).
|
|
β (95% CI) | P value | |||
| Executive functioning | |||||
|
|
Time of day (linear)×UDS3-EFa composite score | .24 (.17 to .31) | <.001 | ||
|
|
Time of day (quadratic)×UDS3-EF composite score | −.65 (−.80 to −.50) | <.001 | ||
|
|
Time of day (cubic)×UDS3-EF composite score | .38 (.28 to .47) | <.001 | ||
| Memory | |||||
|
|
Time of day (linear)×memory z score | .21 (.13 to .28) | <.001 | ||
|
|
Time of day (quadratic)×memory z score | −.58 (−.74 to −.42) | <.001 | ||
|
|
Time of day (cubic)×memory z score | .34 (.24 to .44) | <.001 | ||
| Language | |||||
|
|
Time of day (linear)×MINTb z score | .07 (.00 to .15) | .05 | ||
|
|
Time of day (quadratic)×MINT z score | −.24 (−.40 to −.08) | .002 | ||
|
|
Time of day (cubic)×MINT z score | .15 (.05 to .25) | .004 | ||
| Visuospatial skills | |||||
|
|
Time of day (linear)×Benson Complex Figure Copy z score | .10 (.04 to .16) | .001 | ||
|
|
Time of day (quadratic)×Benson Complex Figure Copy z score | −.28 (−.38 to −.19) | <.001 | ||
|
|
Time of day (cubic)×Benson Complex Figure Copy z score | .19 (.13 to .25) | <.001 | ||
| Neuropsychiatric symptoms | |||||
|
|
Time of day (linear)×NPIc total score | −.06 (−.13 to .01) | .08 | ||
|
|
Time of day (quadratic)×NPI total score | .25 (.10 to .39) | .001 | ||
|
|
Time of day (cubic)×NPI total score | −.15 (−.25 to −.05) | .002 | ||
| Gray matter volume (n=189) | |||||
|
|
Time of day (linear)×gray matter volume | .22 (.14 to .29) | <.001 | ||
|
|
Time of day (quadratic)×gray matter volume | −.73 (−.88 to −.57) | <.001 | ||
|
|
Time of day (cubic)×gray matter volume | .45 (.35 to .55) | <.001 | ||
aUDS3-EF: Uniform Data Set (Version 3) Executive Function.
bMINT: Multilingual Naming Test.
cNPI: Neuropsychiatric Inventory.
Figure 3.
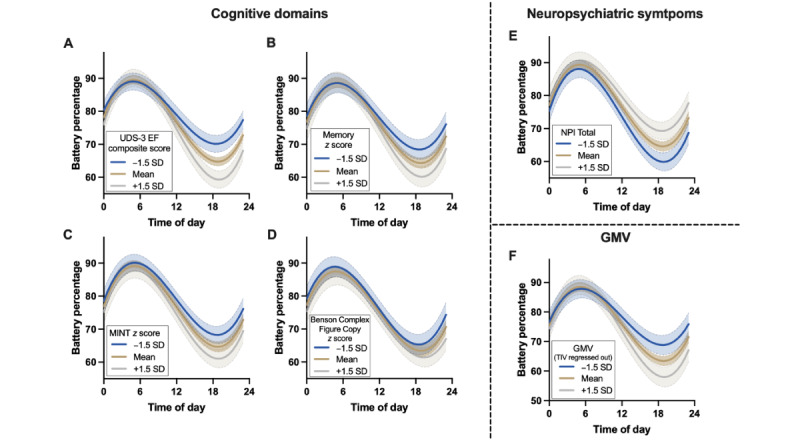
Daily battery percentage trajectories were significantly moderated by (A) executive functioning, (B) memory, (C) language, (D) visuospatial skills, (E) neuropsychiatric symptoms, and (F) total gray matter volumes. Participants with worse neurobehavioral outcomes had smaller daily decreases from peak to minimum battery percentage on average, suggesting less smartphone use throughout the day. GMV: gray matter volume; MINT: Multilingual Naming Test; NPI: Neuropsychiatric Inventory; TIV: total intracranial volume; UDS3-EF: Uniform Data Set (Version 3) Executive Function.
Table 4.
Results of separate linear mixed effects regression models examining relationships between battery percentage trajectories throughout the day and each neuropsychiatric symptom (NPS) captured on the Neuropsychiatric Inventory. Models covaried for age, sex, smartphone type, and estimated smartphone age.
|
|
Predictors modeling interactions with the time of day | ||
|
|
NPS×time of day (linear), β (SE) | NPS×time of day (quadratic), β (SE) | NPS×time of day (cubic), β (SE) |
| Delusions | −.12 (.25) | −.25 (.53) | .43 (.34) |
| Hallucinations | −.61 (.40) | 1.62 (.87) | −.78 (.55) |
| Agitation | −.36 (.10)a | 1.06 (.20)a | −.65 (.13)a |
| Depression | −.34 (.08)a | .92 (.17)a | −.64 (.11)a |
| Anxiety | .05 (.08) | −.20 (.17) | .15 (.11) |
| Elation | .12 (.13) | −.38 (.26) | .29 (.17) |
| Apathy | −.43 (.08)a | 1.32 (.17)a | −.81 (.11)a |
| Disinhibition | −.21 (.09)a | 1.14 (.18)a | −.86 (.12)a |
| Irritability | −.20 (.07)a | .78 (.16)a | −.49 (.10)a |
| Motor disturbance | −.44 (.11)a | 1.18 (.24)a | −.69 (.15)a |
| Nighttime behaviors | −.41 (.10)a | 1.20 (.22)a | −.74 (.14)a |
| Changes in appetite | −.16 (.09) | .86 (.20)a | −.61 (.13)a |
aP values met the threshold for significance.
Given the age difference across disease severity groups, we repeated the first LME model examining battery percentage trajectories by CDR+NACC FTLD group after restricting the age range of the clinically normal group to be identical to that of the group with prodromal FTLD and the group with symptomatic FTLD (participants aged 44-81 years in all groups; clinically normal: 70/139, 50.4%). The interactions between disease severity group and the linear, quadratic, and cubic effects of the time of day on battery percentage are fairly consistent, showing that the participants who were symptomatic had lower battery use than clinically normal participants (interaction with linear time: β=−.23, 95% CI −.40 to −.06; P=.009; interaction with quadratic time: β=.65, 95% CI .23 to 1.07; P=.003; interaction with cubic time: β=−.39, 95% CI −.66 to −.12; P=.004). However, the difference between the prodromal and clinically normal participants no longer reached statistical significance (interaction with linear time: β=−.05, 95% CI −.13 to .22; P=.586; interaction with quadratic time: β=−.07, 95% CI −.50 to .36; P=.76; interaction with cubic time: β=.05, 95% CI −.22 to .33; P=.70).
Sensitivity analyses conducted among the 139 clinically normal participants showed that the following neurobehavioral measures were associated with daily battery percentage trajectories: executive functioning (interaction with linear time: β=.21, 95% CI .12 to .30; P<.001; interaction with quadratic time: β=−.57, 95% CI −.76 to −.38; P<.001; interaction with cubic time: β=.34, 95% CI .21 to .46; P<.001); memory (interaction with linear time: β=.33, 95% CI .24 to .42; P<.001; interaction with quadratic time: β=−.83, 95% CI −1.02 to −.63; P<.001; interaction with cubic time: β=.47, 95% CI .35 to .60; P<.001), and total gray matter volume (interaction with linear time: β=.32, 95% CI .22 to .41; P<.001; interaction with quadratic time: β=−.84, 95% CI −1.03 to −.64; P<.001; interaction with cubic time: β=.48, 95% CI .36 to .61; P<.001). Language, visuospatial functioning, and neuropsychiatric symptoms did not strongly associate with daily battery percentage trajectories in clinically normal participants. The directions of associations in these clinically normal participants were consistent with relationships described in the entire sample.
Discussion
Principal Findings
This study is the first to our knowledge to examine passively collected smartphone use data in a sample with neurodegenerative disease. The results highlight an accessible, low-burden, and scalable remote monitoring method that captured behaviors associated with cognitive, neuropsychiatric, and brain health outcomes in a sample of participants with FTLD. The findings support a proof of concept that this passive digital monitoring approach, in combination with other methods, warrants further evaluation as a potential tool to augment screening and monitoring neurobehavioral change in clinical populations. Consistent with our hypotheses, we found that daily trajectories of smartphone battery use (a proxy for overall smartphone use) were associated with gold standard measures of clinical severity in FTLD such that those with more severe levels of impairment had less smartphone use throughout the day. Relationships between battery percentage trajectories and executive functioning, memory, and gray matter volume also held in the subset of clinically normal participants, suggesting potential sensitivity to subclinical neurobehavioral differences.
Comparison to Prior Work
These findings are consistent with previous studies showing that older adults with cognitive impairment have greater declines in everyday technology use compared to cognitively unimpaired older adults [18,51,52]. Other studies have shown that older adults with cognitive impairment report more difficulties using technology, representing a potential barrier to technology use [53,54]. Notably, the observed associations between battery percentage trajectories and cognitive functioning were not specific to particular cognitive domains, suggesting that the metrics of overall smartphone use may reflect a global transdiagnostic marker of functioning rather than a phenotype-specific marker (eg, executive functioning–predominant or language-predominant dysfunction). Thus, our findings may also not be specific to FTLD, and future work is needed to replicate findings in other populations with neurologic conditions. The use of a smartphone, like the use of a computer [18], is a cognitively complex task requiring the resources of many functions (eg, attention, executive function, working memory, and fine motor skill). As such, smartphone use patterns may be a particularly sensitive marker of early and subtle neurobehavioral change; however, additional research examining longitudinal changes in smartphone use over time is needed to support this hypothesis.
While this is the first study to our knowledge to report on passively collected smartphone use data in the context of neurodegenerative disease, there is a growing body of literature examining other passive streams of smartphone data as potential markers of neurobehavioral function in older adults; for example, passively collected data from smartphone accelerometers, GPS location, and touchscreen typing have been associated with symptom and disease severity in Parkinson disease, multiple sclerosis, and amyotrophic lateral sclerosis [55-64]. Future work should incorporate multiple passive smartphone data types for more comprehensive digital phenotyping and potentially improved clinical relevance in monitoring neurodegenerative disease.
Regarding the more technological aspects of passive smartphone data collection, previous studies have also reported similar variability around the frequency and timing of data collected per person. These studies have identified a number of factors that influence the collection and transfer of smartphone data to secure cloud-based servers, including smartphone hardware, data permissions, app engagement, wireless service, capacity of local data storage, data transmission limits, and even sociodemographic factors [65-67]. This has also been reported in other devices as well, including wearables [68-70]. Thus, thorough data cleaning is necessary to ensure that enough data points are captured to accurately represent activity for a given time period, as has been described previously [71,72].
Visualizing the raw battery percentage data was important for understanding daily patterns and supported the utility of daily smartphone battery percentage trajectories as a proxy for smartphone use. Average patterns in battery percentage appeared to track with typical diurnal sleep-wake rhythms: percentages increased up to morning (when mobile phones are likely charging) and decreased throughout the day (when participants were presumably awake and using their smartphones) until nighttime when percentages began to increase again. Careful examination of these raw data patterns, alongside measures of clinical severity, may support the development of specific metrics using battery percentage data that can be easily tracked over longer periods of time (eg, total battery drainage per day). Future work in this field should also consider examining the frequency and timing of smartphone battery charging as a way to track routine daily use patterns that may be clinically relevant. Tracking these metrics over many months or years would allow for future studies to examine person-specific changes in battery use over time and test longitudinal associations with neurodegenerative disease progression.
Strengths and Limitations
The strengths of this study include a large, extensively characterized cohort with FTLD; the reporting of novel smartphone use data; and the use of passive digital monitoring techniques. However, we also acknowledge several limitations. First, there are certainly caveats to our approach using battery percentage as a proxy for smartphone use, including factors that are difficult to quantify and adjust for, such as the impact of hardware, software, and service connection on battery life [73]. In addition, the ALLFTD Mobile App does not record when a smartphone may have been plugged in for charging, potentially preventing periods of battery decline even when the smartphone may have been in use. Even so, the robust relationships observed with gold standard measures of functional impairment, cognition, neuropsychiatric symptoms, and brain volumes are encouraging. Second, it is likely that the mobile cognitive testing sessions administered by the ALLFTD Mobile App contributed to some smartphone battery use and that battery use may subsequently be affected by adherence to the mobile cognitive testing protocol. However, we have previously reported on adherence to mobile cognitive testing through this app [30], which showed that cognitive testing completion rates among asymptomatic participants, participants with prodromal FTLD, and participants with symptomatic FTLD were 71.4%, 78.4%, and 59%, respectively. These adherence rates do not match the stairstep effect of battery use reported in this study whereby cognitively normal participants exhibited the highest smartphone battery use, participants with prodromal FTLD demonstrated intermediate smartphone battery use, and participants with symptomatic FTLD showed the lowest smartphone battery use, suggesting that our results are not simply driven by adherence to the mobile cognitive testing protocol. Third, although we importantly controlled for the effects of age, sex, smartphone type, and estimated smartphone age in our statistical analyses, further replication is needed in samples whose disease severity groups are demographically matched. Fourth, it is possible that a 30-day monitoring period may not be enough time to most accurately capture routine smartphone use behavior. Future studies are needed to evaluate the psychometrics of passive smartphone use metrics across different periods of time to identify optimal lengths of follow-up. Fifth, our sample was also limited in demographic diversity because participants mostly identified as non-Hispanic White and were highly educated, reflective of the cohort in the ALLFTD study [10]. This is a crucial consideration when examining new tools that require access to technology because the implementation of such digital tools may inadvertently increase disparities among those with fewer resources to obtain technology that meets required software specifications. However, with the steadily increasing rates of smartphone ownership worldwide in addition to the implementation of government-funded programs to provide access to technology (eg, the Lifeline Program or “Obama Phone” [74]), there is growing consensus that smartphone monitoring could become universally accessible.
Conclusions
In sum, our novel results demonstrate the feasibility of continuous, unobtrusive smartphone use monitoring, while also showing that smartphone use relates to the severity of neurobehavioral impairment in a sample with FTLD. We highlight these results as proof of concept because we believe that they support future research examining whether specific smartphone use metrics are clinically relevant and may have utility for monitoring clinical disease progression in FTLD and other neurodegenerative diseases. With continued validation, such passive monitoring methodologies for real-time, real-world, and remote monitoring have the potential to improve the monitoring of clinically meaningful neurobehavioral changes in individuals at risk for dementia.
Acknowledgments
This work was supported by the National Institutes of Health (AG063911, AG077557, AG62677, AG045390, NS092089, AG032306, AG021886, AG016976, AG058233, AG038791, AG02350, AG019724, AG062422, NS050915, AG032289-11, AG077557, K23AG061253, K24AG045333, K23AG59888, K23AG064029, and K23AG073514). This work was also supported by the Association for Frontotemporal Degeneration, the Bluefield Project to Cure Frontotemporal Dementia (FTD), the Rainwater Charitable Foundation, AlzOut, the John Douglas French Alzheimer’s Foundation, and the Alzheimer’s Association (AARF-22-974065, principal investigator: EWP; AARF-23-1145318, principal investigator: RS). The authors thank the organizers of the the International Society to Advance Alzheimer's Research and Treatment (ISTAART) Design and Data Analytics Professional Interest Area Workshop, Applying Novel Models for Longitudinal Outcomes, who provided consultation on the statistical analyses in this study.
The members of ALLFTD Consortium are Liana Apostolova, MD, Indiana University; Sami Barmada, MD, PhD, University of Michigan; Ece Bayram, MD, PhD, UCSD; Hugo Botha, MD, Mayo Clinic, Rochester; Andrea Bozoki, MD, University of North Carolina; Yann Cobigo, PhD, UCSF; Gregg S Day MD, MSc, Mayo Clinic Jacksonville; Dennis Dickson, MD, Mayo Clinic, Jacksonville; Kelley Faber, MS, Indiana University (NCRAD); Anne Fagan, PhD, Washington University, St. Louis; Jamie Fong, MS, UCSF; Tatiana Foroud, PhD, Indiana University (NCRAD); Douglas R. Galasko, MD, UCSD; Ralitza Gavrilova, MD, Mayo Clinic, Rochester; Tania Gendron, PhD, Mayo Clinic Jacksonville; Daniel Geschwind, MD, PhD, UCLA; Jill Goldman, MS, MPhil, Columbia University; Jonathan Graff-Radford, MD, Mayo Clinic, Rochester; Ian M. Grant, MD, Northwestern University; Murray Grossman, MD, EdD, University of Pennsylvania; Chadwick M. Hales, MD, PhD, Emory; Hilary W. Heuer, PhD, UCSF; Ging-Yuek (Robin) Hsiung, MD, University of British Columbia; Eric Huang, PhD, UCSF; David Irwin, MD, University of Pennsylvania; Noah Johnson, BA, Mayo Clinic, Rochester; David T. Jones, MD, Mayo Clinic, Rochester; Kejal Kantarci, MD, Mayo Clinic, Rochester; David Knopman, MD, Mayo Clinic, Rochester; Tyler Kolander, BA, Mayo Clinic, Rochester; Justin Kwan, MD, National Institutes of Health; Argentina Lario Lago, PhD, UCSF; Shannon B. Lavigne, PhD, UT Health San Antonio; Suzee Lee, MD, UCSF; Gabriel C. Léger, MD, UCSD; Peter Ljubenkov, MD, UCSF; Diane Lucente, MS, MGH; Masood Manoochehri, BA, Columbia University; Lauren Massimo, PhD, University of Pennsylvania; Scott McGinnis, MD, MGH; Corey T. McMillan, PhD, University of Pennsylvania; Joie Molden, PhD, University of Colorado; Chiadi Onyike, MBBS, MHS Johns Hopkins University; Alexander Pantelyat, MD, Johns Hopkins University; Henry Paulson, MD, PhD, University of Michigan; Leonard Petrucelli, PhD, Mayo Clinic Jacksonville; Rosa Rademakers, PhD, University of Antwerp; Vijay Ramanan MD, PhD, Mayo Clinic, Rochester; Meghana Rao, BS, MPH Mayo Clinic, Rochester; Katya Rascovsky, PhD, University of Pennsylvania; Kristoffer W. Rhoads, PhD, University of Washington; Aaron Ritter, MD, Cleveland Clinic Las Vegas; Erik D. Roberson MD, PhD, University of Alabama at Birmingham; Emily Rogalski, PhD, Northwestern University; Rodolfo Savica, MD, PhD, Mayo Clinic, Rochester; William Seeley, MD, UCSF; Allison Snyder, MD, National Institutes of Health; Anne C. Sullivan, PhD, UT Health San Antonio ; Jeremy M. Syrjanen, MS, Mayo Clinic, Rochester; M. Carmela Tartaglia, MD, University of Toronto; Philip W. Tipton, MD, Mayo Clinic Jacksonville; Marijne Vandebergh, PhD, University of Antwerp; Arthur Toga, PhD, Keck School of Medicine of University of Southern California; Sandra Weintraub, PhD, Northwestern University; Dylan Wint, MD, Cleveland Clinic Las Vegas; Amy Wolf, BS, UCSF; Jennifer Yokoyoma, PhD, UCSF.
Abbreviations
- ALLFTD
Advancing Research and Treatment of Frontotemporal Lobar Degeneration (ARTFL study) and Longitudinal Evaluation of Familial Frontotemporal Dementia Subjects (LEFFTDS study) Longitudinal Frontotemporal Lobar Degeneration
- API
application programming interface
- ARTFL
Advancing Research and Treatment of Frontotemporal Lobar Degeneration
- C9orf72
chromosome 9 open reading frame 72
- CDR+NACC FTLD
Clinical Dementia Rating Dementia Staging Instrument plus National Alzheimer’s Coordinating Center Frontotemporal Lobar Degeneration Behavior and Language Domains
- FTLD
frontotemporal lobar degeneration
- GRN
progranulin
- LEFFTDS
Longitudinal Evaluation of Familial Frontotemporal Dementia Subjects
- LME
linear mixed effects
- MAPT
microtubule-associated protein tau
- MRI
magnetic resonance imaging
Visualization of raw battery percentage data binned by time of day (0=midnight; 23=11 PM) by disease severity group: (A) clinically normal, (B) prodromal frontotemporal lobar degeneration (FTLD), and (C) symptomatic FTLD.
Footnotes
Conflicts of Interest: BA has received research funding from the National Institutes of Health (NIH), the Centers for Disease Control and Prevention, the CJD Foundation, Alector, and Ionis; consulting fees from Acadia, Ionis, Sangamo, Gate, and Merck; and royalties from Wolters Kluwer. GSD reports no conflicts of interest that are directly relevant to this work. His research is supported by the NIH (K23AG064029, U01AG057195, U01NS120901, and U19AG032438), the Alzheimer’s Association, and the Chan Zuckerberg Initiative. He serves as a consultant for Parabon Nanolabs Inc; as a topic editor (dementia) for DynaMed (EBSCO); and as the clinical director of the Anti-NMDA Receptor Encephalitis Foundation Inc, Canada (uncompensated). He is the co–project principal investigator for a clinical trial in anti–N-methyl-D-aspartate (NMDA) receptor encephalitis, which receives support from Horizon Pharmaceuticals. He has developed educational materials for PeerView, and Continuing Education Inc. He owns stock in ANI Pharmaceuticals. His institution has received support from Eli Lilly for development and participation in an educational event promoting early diagnosis of symptomatic Alzheimer disease and in-kind contributions of radiotracer precursors for tau–positron emission tomography (PET) neuroimaging in studies of memory and aging (via Avid Radiopharmaceuticals, a wholly owned subsidiary of Eli Lilly). NG has participated, or is currently participating, in clinical trials of antidementia drugs sponsored by Bristol Myers Squibb, Eli Lilly and Avid Radiopharmaceuticals, Janssen Immunotherapy, Novartis, Pfizer, and Wyeth, as well as the Study of Nasal Insulin to Fight Forgetfulness (SNIFF) and the Anti-Amyloid Treatment in Asymptomatic Alzheimer’s Disease (A4) trial. She receives research support from the Tau Consortium and the Association for Frontotemporal Dementia and is funded by the NIH. IL’s research is supported by the NIH (2R01AG038791-06A, U01NS100610, R25NS098999, U19 AG063911-1, and 1R21NS114764-01A1), the Michael J Fox Foundation, the Parkinson’s Foundation, the Lewy Body Dementia Association, CurePSP, Roche, Abbvie, Biogen, Centogene, EIP Pharma, Biohaven Pharmaceuticals, Novartis, United BioPharma, and UCB. She is a member of the scientific advisory board for Amydis but does not receive funds and from the Rossy Progressive Supranuclear Palsy Program at the University of Toronto. She receives her salary from the University of California San Diego and as chief editor of Frontiers in Neurology. JCR is the site principal investigator for clinical trials sponsored by Eli Lilly and Eisai. He receives consulting fees from Roon. LVV is the site principal investigator for clinical trials sponsored by Biogen and has consulted for Retrotope. All other authors declare no other conflicts of interest.
References
- 1.Knopman DS, Roberts RO. Estimating the number of persons with frontotemporal lobar degeneration in the US population. J Mol Neurosci. 2011 Nov 17;45(3):330–5. doi: 10.1007/s12031-011-9538-y. https://europepmc.org/abstract/MED/21584654 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hendriks S, Peetoom K, Bakker C, van der Flier WM, Papma JM, Koopmans R, Verhey FR, de Vugt M, Köhler S, Young-Onset Dementia Epidemiology Study Group. Withall A, Parlevliet JL, Uysal-Bozkir Ö, Gibson RC, Neita SM, Nielsen TR, Salem LC, Nyberg J, Lopes MA, Dominguez JC, De Guzman MF, Egeberg A, Radford K, Broe T, Subramaniam M, Abdin E, Bruni AC, Di Lorenzo R, Smith K, Flicker L, Mol MO, Basta M, Yu D, Masika G, Petersen MS, Ruano L. Global prevalence of young-onset dementia: a systematic review and meta-analysis. JAMA Neurol. 2021 Sep 01;78(9):1080–90. doi: 10.1001/jamaneurol.2021.2161. https://europepmc.org/abstract/MED/34279544 .2781919 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Perry D, Brown JA, Possin KL, Datta S, Trujillo A, Radke A, Karydas A, Kornak J, Sias AC, Rabinovici GD, Gorno-Tempini ML, Boxer AL, De May M, Rankin KP, Sturm VE, Lee SE, Matthews BR, Kao AW, Vossel KA, Tartaglia MC, Miller ZA, Seo SW, Sidhu M, Gaus SE, Nana AL, Vargas JN, Hwang JH, Ossenkoppele R, Brown AB, Huang EJ, Coppola G, Rosen HJ, Geschwind D, Trojanowski JQ, Grinberg LT, Kramer JH, Miller BL, Seeley WW. Clinicopathological correlations in behavioural variant frontotemporal dementia. Brain. 2017 Dec 01;140(12):3329–45. doi: 10.1093/brain/awx254. https://europepmc.org/abstract/MED/29053860 .4371604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Seo SW, Thibodeau MP, Perry DC, Hua A, Sidhu M, Sible I, Vargas JN, Gaus SE, Rabinovici GD, Rankin KD, Boxer AL, Kramer JH, Rosen HJ, Gorno-Tempini ML, Grinberg LT, Huang EJ, DeArmond SJ, Trojanowski JQ, Miller BL, Seeley WW. Early vs late age at onset frontotemporal dementia and frontotemporal lobar degeneration. Neurology. 2018 Mar 20;90(12):e1047–56. doi: 10.1212/wnl.0000000000005163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Black CM, Fillit H, Xie L, Hu X, Kariburyo MF, Ambegaonkar BM, Baser O, Yuce H, Khandker RK. Economic burden, mortality, and institutionalization in patients newly diagnosed with Alzheimer’s disease. J Alzheimers Dis. 2017 Nov 28;61(1):185–93. doi: 10.3233/jad-170518. [DOI] [PubMed] [Google Scholar]
- 6.Rasmussen J, Langerman H. Alzheimer's disease - why we need early diagnosis. Degener Neurol Neuromuscul Dis. 2019 Dec;9:123–30. doi: 10.2147/DNND.S228939. https://europepmc.org/abstract/MED/31920420 .228939 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wong W. Economic burden of Alzheimer disease and managed care considerations. Am J Manag Care. 2020 Aug 17;26(8 Suppl):S177–83. doi: 10.37765/ajmc.2020.88482. https://www.ajmc.com/pubMed.php?pii=88482 .88482 [DOI] [PubMed] [Google Scholar]
- 8.van Dyck CG, Swanson CJ, Aisen P, Bateman RJ, Chen C, Gee M, Kanekiyo M, Li D, Reyderman L, Cohen S, Froelich L, Katayama S, Sabbagh M, Vellas B, Watson D, Dhadda S, Irizarry M, Kramer LD, Iwatsubo T. Lecanemab in early Alzheimer's disease. N Engl J Med. 2023 Jan 05;388(1):9–21. doi: 10.1056/NEJMoa2212948. [DOI] [PubMed] [Google Scholar]
- 9.A study of PBFT02 in patients with frontotemporal dementia and progranulin mutations (FTD-GRN) (upliFT-D) National Institutes of Health U.S. National Library of Medicine. 2021. [2024-04-03]. https://clinicaltrials.gov/ct2/show/NCT04747431 .
- 10.Staffaroni AM, Quintana M, Wendelberger B, Heuer HW, Russell LL, Cobigo Y, Wolf A, Goh SY, Petrucelli L, Gendron TF, Heller C, Clark AL, Taylor JC, Wise A, Ong E, Forsberg L, Brushaber D, Rojas JC, VandeVrede L, Ljubenkov P, Kramer J, Casaletto KB, Appleby B, Bordelon Y, Botha H, Dickerson BC, Domoto-Reilly K, Fields JA, Foroud T, Gavrilova R, Geschwind D, Ghoshal N, Goldman J, Graff-Radford J, Graff-Radford N, Grossman M, Hall MG, Hsiung GY, Huey ED, Irwin D, Jones DT, Kantarci K, Kaufer D, Knopman D, Kremers W, Lago AL, Lapid MI, Litvan I, Lucente D, Mackenzie IR, Mendez MF, Mester C, Miller BL, Onyike CU, Rademakers R, Ramanan VK, Ramos EM, Rao M, Rascovsky K, Rankin KP, Roberson ED, Savica R, Tartaglia MC, Weintraub S, Wong B, Cash DM, Bouzigues A, Swift IJ, Peakman G, Bocchetta M, Todd EG, Convery RS, Rowe JB, Borroni B, Galimberti D, Tiraboschi P, Masellis M, Finger E, van Swieten JC, Seelaar H, Jiskoot LC, Sorbi S, Butler CR, Graff C, Gerhard A, Langheinrich T, Laforce R, Sanchez-Valle R, de Mendonça A, Moreno F, Synofzik M, Vandenberghe R, Ducharme S, Le Ber I, Levin J, Danek A, Otto M, Pasquier F, Santana I, Kornak J, Boeve BF, Rosen HJ, Rohrer JD, Boxer AL. Temporal order of clinical and biomarker changes in familial frontotemporal dementia. Nat Med. 2022 Oct;28(10):2194–206. doi: 10.1038/s41591-022-01942-9. https://europepmc.org/abstract/MED/36138153 .10.1038/s41591-022-01942-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Valdez P, Ramírez. García A. Circadian rhythms in cognitive performance: implications for neuropsychological assessment. ChronoPhysiol Ther. 2012 Dec;2:81–92. doi: 10.2147/cpt.s32586. [DOI] [Google Scholar]
- 12.McDermott LM, Ebmeier KP. A meta-analysis of depression severity and cognitive function. J Affect Disord. 2009 Dec;119(1-3):1–8. doi: 10.1016/j.jad.2009.04.022.S0165-0327(09)00170-0 [DOI] [PubMed] [Google Scholar]
- 13.Framework for FDA’s real-world evidence program. U.S. Food & Drug Administration. 2018. Dec, [2024-04-03]. https://www.fda.gov/media/120060/download .
- 14.National plan to address Alzheimer’s disease: 2022 update. U.S. Department of Health and Human Services. 2022. Dec 30, [2024-04-03]. https://aspe.hhs.gov/reports/national-plan-2022-update .
- 15.Workshop on applying digital technology for early diagnosis and monitoring of Alzheimer’s disease and related dementias. National Institutes of Health National Institute on Aging. [2024-04-03]. https://www.nia.nih.gov/research/dn/workshops/workshop-applying-digital-technology-early-diagnosis-and-monitoring .
- 16.National advisory neurological disorders and stroke council. National Institutes of Neurological Disorders and Stroke. [2024-04-03]. https://www.ninds.nih.gov/about-ninds/who-we-are/national-advisory-neurological-disorders-and-stroke-council .
- 17.Bernstein JP, Dorociak KE, Mattek N, Leese M, Beattie ZT, Kaye JA, Hughes A. Passively-measured routine home computer activity and application use can detect mild cognitive impairment and correlate with important cognitive functions in older adulthood. J Alzheimers Dis. 2021 Jun 01;81(3):1053–64. doi: 10.3233/jad-210049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kaye J, Mattek N, Dodge HH, Campbell I, Hayes T, Austin D, Hatt W, Wild K, Jimison H, Pavel M. Unobtrusive measurement of daily computer use to detect mild cognitive impairment. Alzheimers Dement. 2014 Jan 20;10(1):10–7. doi: 10.1016/j.jalz.2013.01.011. https://europepmc.org/abstract/MED/23688576 .S1552-5260(13)00043-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Seelye A, Hagler S, Mattek N, Howieson DB, Wild K, Dodge HH, Kaye JA. Computer mouse movement patterns: a potential marker of mild cognitive impairment. Alzheimers Dement (Amst) 2015 Dec 01;1(4):472–80. doi: 10.1016/j.dadm.2015.09.006. https://europepmc.org/abstract/MED/26878035 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Stringer G, Couth S, Heuvelman H, Bull C, Gledson A, Keane J, Rayson P, Sutcliffe A, Sawyer PH, Zeng XJ, Montaldi D, Brown LJ, Leroi I. Assessment of non-directed computer-use behaviours in the home can indicate early cognitive impairment: a proof of principle longitudinal study. Aging Ment Health. 2023 Jan 30;27(1):193–202. doi: 10.1080/13607863.2022.2036946. [DOI] [PubMed] [Google Scholar]
- 21.Gledson A, Asfiandy D, Mellor J, Ba-Dhfari TO, Stringer G, Couth S, Burns A, Leroi I, Zeng X, Keane J, Bull C, Rayson P, Sutcliffe A, Sawyer P. Combining mouse and keyboard events with higher level desktop actions to detect mild cognitive impairment. Proceedings of the IEEE International Conference on Healthcare Informatics (ICHI); ICHI 2016; October 4-7, 2016; Chicago, IL. 2016. [DOI] [Google Scholar]
- 22.Stringer G, Couth S, Brown LJ, Montaldi D, Gledson A, Mellor J, Sutcliffe A, Sawyer P, Keane J, Bull C, Zeng X, Rayson P, Leroi I. Can you detect early dementia from an email? A proof of principle study of daily computer use to detect cognitive and functional decline. Int J Geriatr Psychiatry. 2018 Jul 09;33(7):867–74. doi: 10.1002/gps.4863. https://europepmc.org/abstract/MED/29424087 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Piau A, Wild K, Mattek N, Kaye J. Current state of digital biomarker technologies for real-life, home-based monitoring of cognitive function for mild cognitive impairment to mild Alzheimer disease and implications for clinical care: systematic review. J Med Internet Res. 2019 Aug 30;21(8):e12785. doi: 10.2196/12785. https://www.jmir.org/2019/8/e12785/ v21i8e12785 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bayat S, Babulal GM, Schindler SE, Fagan AM, Morris JC, Mihailidis A, Roe CM. GPS driving: a digital biomarker for preclinical Alzheimer disease. Alzheimers Res Ther. 2021 Jun 14;13(1):115. doi: 10.1186/s13195-021-00852-1. https://alzres.biomedcentral.com/articles/10.1186/s13195-021-00852-1 .10.1186/s13195-021-00852-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Di X, Shi R, DiGuiseppi C, Eby DW, Hill LL, Mielenz TJ, Molnar LJ, Strogatz D, Andrews HF, Goldberg TE, Lang BH, Kim M, Li G. Using naturalistic driving data to predict mild cognitive impairment and dementia: preliminary findings from the longitudinal research on aging drivers (LongROAD) study. Geriatrics (Basel) 2021 Apr 23;6(2):45. doi: 10.3390/geriatrics6020045. https://www.mdpi.com/resolver?pii=geriatrics6020045 .geriatrics6020045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Li H, Liu X, Mei Q. Predicting smartphone battery life based on comprehensive and real-time usage data. arXiv. Preprint posted online January 12, 2018. 2024 https://arxiv.org/abs/1801.04069 . [Google Scholar]
- 27.Gower AD, Moreno MA. A novel approach to evaluating mobile smartphone screen time for iPhones: feasibility and preliminary findings. JMIR Mhealth Uhealth. 2018 Nov 19;6(11):e11012. doi: 10.2196/11012. https://mhealth.jmir.org/2018/11/e11012/ v6i11e11012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rahmati A, Tossell C, Shepard C, Kortum P, Zhong L. Exploring iPhone usage: the influence of socioeconomic differences on smartphone adoption, usage and usability. Proceedings of the 14th International Conference on Human-Computer Interaction with Mobile Devices and Services; MobileHCI '12; September 21-24, 2012; San Francisco, CA. 2012. [DOI] [Google Scholar]
- 29.Market share of mobile operating systems worldwide from 2009 to 2023, by quarter. Statista. [2024-04-03]. https://www.statista.com/statistics/272698/global-market-share-held-by-mobile-operating-systems-since-2009/
- 30.Taylor JC, Heuer HW, Clark AL, Wise AB, Manoochehri M, Forsberg L, Mester C, Rao M, Brushaber D, Kramer J, Welch AE, Kornak J, Kremers W, Appleby B, Dickerson BC, Domoto-Reilly K, Fields JA, Ghoshal N, Graff-Radford N, Grossman M, Hall MG, Huey ED, Irwin D, Lapid MI, Litvan I, Mackenzie IR, Masdeu JC, Mendez MF, Nevler N, Onyike CU, Pascual B, Pressman P, Rankin KP, Ratnasiri B, Rojas JC, Tartaglia MC, Wong B, Gorno-Tempini ML, Boeve BF, Rosen HJ, Boxer AL, Staffaroni AM. Feasibility and acceptability of remote smartphone cognitive testing in frontotemporal dementia research. Alzheimers Dement (Amst) 2023 May 9;15(2):e12423. doi: 10.1002/dad2.12423. https://europepmc.org/abstract/MED/37180971 .DAD212423 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bufano P, Laurino M, Said S, Tognetti A, Menicucci D. Digital phenotyping for monitoring mental disorders: systematic review. J Med Internet Res. 2023 Dec 13;25:e46778. doi: 10.2196/46778. https://www.jmir.org/2023//e46778/ v25i1e46778 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rascovsky K, Hodges JR, Knopman D, Mendez MF, Kramer JH, Neuhaus J, van Swieten JC, Seelaar H, Dopper EG, Onyike CU, Hillis AE, Josephs KA, Boeve BF, Kertesz A, Seeley WW, Rankin KP, Johnson JK, Gorno-Tempini ML, Rosen H, Prioleau-Latham CE, Lee A, Kipps CM, Lillo P, Piguet O, Rohrer JD, Rossor MN, Warren JD, Fox NC, Galasko D, Salmon DP, Black SE, Mesulam M, Weintraub S, Dickerson BC, Diehl-Schmid J, Pasquier F, Deramecourt V, Lebert F, Pijnenburg Y, Chow TW, Manes F, Grafman J, Cappa SF, Freedman M, Grossman M, Miller BL. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain. 2011 Sep;134(Pt 9):2456–77. doi: 10.1093/brain/awr179. https://europepmc.org/abstract/MED/21810890 .awr179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Gorno-Tempini ML, Hillis AE, Weintraub S, Kertesz A, Mendez M, Cappa SF, Ogar JM, Rohrer JD, Black S, Boeve BF, Manes F, Dronkers NF, Vandenberghe R, Rascovsky K, Patterson K, Miller BL, Knopman DS, Hodges JR, Mesulam MM, Grossman M. Classification of primary progressive aphasia and its variants. Neurology. 2011 Mar 15;76(11):1006–14. doi: 10.1212/wnl.0b013e31821103e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Höglinger GU, Respondek G, Stamelou M, Kurz C, Josephs KA, Lang AE, Mollenhauer B, Müller U, Nilsson C, Whitwell JL, Arzberger T, Englund E, Gelpi E, Giese A, Irwin DJ, Meissner WG, Pantelyat A, Rajput A, van Swieten JC, Troakes C, Antonini A, Bhatia KP, Bordelon Y, Compta Y, Corvol JC, Colosimo C, Dickson DW, Dodel R, Ferguson L, Grossman M, Kassubek J, Krismer F, Levin J, Lorenzl S, Morris HR, Nestor P, Oertel WH, Poewe W, Rabinovici G, Rowe JB, Schellenberg GD, Seppi K, van Eimeren T, Wenning GK, Boxer AL, Golbe LI, Litvan I. Clinical diagnosis of progressive supranuclear palsy: the movement disorder society criteria. Mov Disord. 2017 Jun;32(6):853–64. doi: 10.1002/mds.26987. https://europepmc.org/abstract/MED/28467028 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Armstrong MJ, Litvan I, Lang AE, Bak TH, Bhatia KP, Borroni B, Boxer AL, Dickson DW, Grossman M, Hallett M, Josephs KA, Kertesz A, Lee SE, Miller BL, Reich SG, Riley DE, Tolosa E, Tröster AI, Vidailhet M, Weiner WJ. Criteria for the diagnosis of corticobasal degeneration. Neurology. 2013 Jan 29;80(5):496–503. doi: 10.1212/wnl.0b013e31827f0fd1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ramos EM, Dokuru DR, Van Berlo V, Wojta K, Wang Q, Huang AY, Deverasetty S, Qin Y, van Blitterswijk M, Jackson J, Appleby B, Bordelon Y, Brannelly P, Brushaber DE, Dickerson B, Dickinson S, Domoto-Reilly K, Faber K, Fields J, Fong J, Foroud T, Forsberg LK, Gavrilova R, Ghoshal N, Goldman J, Graff-Radford J, Graff-Radford N, Grant I, Grossman M, Heuer HW, Hsiung GY, Huey E, Irwin D, Kantarci K, Karydas A, Kaufer D, Kerwin D, Knopman D, Kornak J, Kramer JH, Kremers W, Kukull W, Litvan I, Ljubenkov P, Lungu C, Mackenzie I, Mendez MF, Miller BL, Onyike C, Pantelyat A, Pearlman R, Petrucelli L, Potter M, Rankin KP, Rascovsky K, Roberson ED, Rogalski E, Shaw L, Syrjanen J, Tartaglia MC, Tatton N, Taylor J, Toga A, Trojanowski JQ, Weintraub S, Wong B, Wszolek Z, Rademakers R, Boeve BF, Rosen HJ, Boxer AL, ARTFL/LEFFTDS consortium. Coppola G. Genetic screening of a large series of North American sporadic and familial frontotemporal dementia cases. Alzheimers Dement. 2020 Jan;16(1):118–30. doi: 10.1002/alz.12011. https://europepmc.org/abstract/MED/31914217 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wakim NI, Braun TM, Kaye JA, Dodge HH, for ORCATECH Choosing the right time granularity for analysis of digital biomarker trajectories. Alzheimers Dement (N Y) 2020 Dec 18;6(1):e12094. doi: 10.1002/trc2.12094. https://europepmc.org/abstract/MED/33354618 .TRC212094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Knopman DS, Weintraub S, Pankratz VS. Language and behavior domains enhance the value of the clinical dementia rating scale. Alzheimers Dement. 2011 May;7(3):293–9. doi: 10.1016/j.jalz.2010.12.006. https://europepmc.org/abstract/MED/21575870 .S1552-5260(10)02535-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Morris JC. Clinical dementia rating: a reliable and valid diagnostic and staging measure for dementia of the Alzheimer type. Int Psychogeriatr. 1997 Jan 10;9 Suppl 1(S1):173–6; discussion 177. doi: 10.1017/s1041610297004870. [DOI] [PubMed] [Google Scholar]
- 40.Miyagawa T, Brushaber D, Syrjanen J, Kremers W, Fields J, Forsberg LK, Heuer HW, Knopman D, Kornak J, Boxer A, Rosen H, Boeve B, Appleby B, Bordelon Y, Bove J, Brannelly P, Caso C, Coppola G, Dever R, Dheel C, Dickerson B, Dickinson S, Dominguez S, Domoto-Reilly K, Faber K, Ferrell J, Fishman A, Fong J, Foroud T, Gavrilova R, Gearhart D, Ghazanfari B, Ghoshal N, Goldman JS, Graff-Radford J, Graff-Radford N, Grant I, Grossman M, Haley D, Hsiung R, Huey E, Irwin D, Jones D, Jones L, Kantarci K, Karydas A, Kaufer D, Kerwin D, Kraft R, Kramer J, Kukull W, Litvan I, Lucente D, Lungu C, Mackenzie I, Maldonado M, Manoochehri M, McGinnis S, McKinley E, Mendez MF, Miller B, Multani N, Onyike C, Padmanabhan J, Pantelyat A, Pearlman R, Petrucelli L, Potter M, Rademakers R, Ramos EM, Rankin K, Rascovsky K, Roberson ED, Rogalski E, Sengdy P, Shaw L, Tartaglia MC, Tatton N, Taylor J, Toga A, Trojanowski JQ, Wang P, Weintraub S, Wong B, Wszolek Z. Utility of the global CDR plus NACC FTLD rating and development of scoring rules: data from the ARTFL/LEFFTDS Consortium. Alzheimers Dement. 2020 Jan;16(1):106–17. doi: 10.1002/alz.12033. https://europepmc.org/abstract/MED/31914218 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Staffaroni AM, Asken BM, Casaletto KB, Fonseca C, You M, Rosen HJ, Boxer AL, Elahi FM, Kornak J, Mungas D, Kramer JH. Development and validation of the Uniform Data Set (v3.0) executive function composite score (UDS3-EF) Alzheimers Dement. 2021 Apr 20;17(4):574–83. doi: 10.1002/alz.12214. https://europepmc.org/abstract/MED/33215852 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Weintraub S, Besser L, Dodge HH, Teylan M, Ferris S, Goldstein FC, Giordani B, Kramer J, Loewenstein D, Marson D, Mungas D, Salmon D, Welsh-Bohmer K, Zhou XH, Shirk SD, Atri A, Kukull WA, Phelps C, Morris JC. Version 3 of the Alzheimer disease centers' neuropsychological test battery in the uniform data set (UDS) Alzheimer Dis Assoc Disord. 2018;32(1):10–7. doi: 10.1097/WAD.0000000000000223. https://europepmc.org/abstract/MED/29240561 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Delis DC, Kramer JH, Kaplan E, Ober BA. California Verbal Learning Test. San Antonio, TX: The Psychological Corporation; 1987. [Google Scholar]
- 44.Kramer JH, Jurik J, Sha SJ, Rankin KP, Rosen HJ, Johnson JK, Miller BL. Distinctive neuropsychological patterns in frontotemporal dementia, semantic dementia, and Alzheimer disease. Cogn Behav Neurol. 2003 Dec;16(4):211–8. doi: 10.1097/00146965-200312000-00002. [DOI] [PubMed] [Google Scholar]
- 45.Possin KL, Laluz VR, Alcantar OZ, Miller BL, Kramer JH. Distinct neuroanatomical substrates and cognitive mechanisms of figure copy performance in Alzheimer's disease and behavioral variant frontotemporal dementia. Neuropsychologia. 2011 Jan;49(1):43–8. doi: 10.1016/j.neuropsychologia.2010.10.026. https://europepmc.org/abstract/MED/21029744 .S0028-3932(10)00452-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Gollan TH, Weissberger GH, Runnqvist E, Montoya RI, Cera CM. Self-ratings of spoken language dominance: a Multilingual Naming Test (MINT) and preliminary norms for young and aging Spanish–English bilinguals. Bilingualism. 2011 Aug 01;15(3):594–615. doi: 10.1017/s1366728911000332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kaufer DI, Cummings JL, Ketchel P, Smith V, MacMillan A, Shelley T, Lopez OL. Validation of the NPI-Q, a brief clinical form of the neuropsychiatric inventory. J Neuropsychiatry Clin Neurosci. 2000 May 1;12(2):233–9. doi: 10.1176/appi.neuropsych.12.2.233. [DOI] [PubMed] [Google Scholar]
- 48.Olney NT, Ong E, Goh SY, Bajorek L, Dever R, Staffaroni AM, Cobigo Y, Bock M, Chiang K, Ljubenkov P, Kornak J, Heuer HW, Wang P, Rascovsky K, Wolf A, Appleby B, Bove J, Bordelon Y, Brannelly P, Brushaber D, Caso C, Coppola G, Dickerson BC, Dickinson S, Domoto-Reilly K, Faber K, Ferrall J, Fields J, Fishman A, Fong J, Foroud T, Forsberg LK, Gearhart DJ, Ghazanfari B, Ghoshal N, Goldman J, Graff-Radford J, Graff-Radford NR, Grant I, Grossman M, Haley D, Hsiung G, Huey ED, Irwin DJ, Jones DT, Kantarci K, Karydas AM, Kaufer D, Kerwin D, Knopman DS, Kramer JH, Kraft R, Kremers W, Kukull W, Lapid MI, Litvan I, Mackenzie IR, Maldonado M, Manoochehri M, McGinnis SM, McKinley EC, Mendez MF, Miller BL, Onyike C, Pantelyat A, Pearlman R, Petrucelli L, Potter M, Rademakers R, Ramos EM, Rankin KP, Roberson ED, Rogalski E, Sengdy P, Shaw LM, Syrjanen J, Tartaglia MC, Tatton N, Taylor J, Toga A, Trojanowski JQ, Weintraub S, Wong B, Wszolek Z, Boxer AL, Boeve BF, Rosen HJ. Clinical and volumetric changes with increasing functional impairment in familial frontotemporal lobar degeneration. Alzheimers Dement. 2020 Jan;16(1):49–59. doi: 10.1016/j.jalz.2019.08.196. https://linkinghub.elsevier.com/retrieve/pii/S1552-5260(19)35366-X .S1552-5260(19)35366-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. 2015;67(1):1–48. doi: 10.18637/jss.v067.i01. [DOI] [Google Scholar]
- 50.Toller G, Cobigo Y, Callahan P, Appleby BS, Brushaber D, Domoto-Reilly K, Forsberg LK, Ghoshal N, Graff-Radford J, Graff-Radford NR, Grossman M, Heuer HW, Kornak J, Kremers W, Lapid MI, Leger G, Litvan I, Mackenzie IR, Pascual MB, Ramos EM, Rascovsky K, Rojas JC, Staffaroni AM, Tartaglia MC, Toga A, Weintraub S, Wszolek ZK, Boeve BF, Boxer AL, Rosen HJ, Rankin KP. Multisite ALLFTD study modeling progressive empathy loss from the earliest stages of behavioral variant frontotemporal dementia. Alzheimers Dement. 2023 Jul 02;19(7):2842–52. doi: 10.1002/alz.12898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hedman A, Nygård L, Almkvist O, Kottorp A. Patterns of functioning in older adults with mild cognitive impairment: a two-year study focusing on everyday technology use. Aging Ment Health. 2013 Apr 03;17(6):679–88. doi: 10.1080/13607863.2013.777396. [DOI] [PubMed] [Google Scholar]
- 52.Hedman A, Nygård L, Almkvist O, Kottorp A. Amount and type of everyday technology use over time in older adults with cognitive impairment. Scand J Occup Ther. 2015 May 12;22(3):196–206. doi: 10.3109/11038128.2014.982172. [DOI] [PubMed] [Google Scholar]
- 53.Ikeda Y, Maruta M, Shimokihara S, Nakamura A, Han G, Tabira T. Difficulties in the use of everyday technology among older adults with subjective memory complaint and cognitive decline. Gerontology. 2022 Sep 2;68(6):655–63. doi: 10.1159/000518390.000518390 [DOI] [PubMed] [Google Scholar]
- 54.Malinowsky C, Almkvist O, Kottorp A, Nygård L. Ability to manage everyday technology: a comparison of persons with dementia or mild cognitive impairment and older adults without cognitive impairment. Disabil Rehabil Assist Technol. 2010 Jun 15;5(6):462–9. doi: 10.3109/17483107.2010.496098. [DOI] [PubMed] [Google Scholar]
- 55.Chen MH, Leow A, Ross MK, DeLuca J, Chiaravalloti N, Costa SL, Genova HM, Weber E, Hussain F, Demos AP. Associations between smartphone keystroke dynamics and cognition in MS. Digit Health. 2022 Dec 05;8:20552076221143234. doi: 10.1177/20552076221143234. https://journals.sagepub.com/doi/10.1177/20552076221143234?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_20552076221143234 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Hoeijmakers A, Meijer KA, Alfonso N, McConchie H, Lam KH, Killestein J. Motor- and non-motor symptoms can be passively and remotely monitored in people with multiple sclerosis by measuring keyboard interactions on a smartphone (4142) Neurology. 2021 Apr 13;96(15_supplement) doi: 10.1212/wnl.96.15_supplement.4142. [DOI] [Google Scholar]
- 57.Lam KH, Meijer KA, Loonstra FC, Coerver E, Twose J, Redeman E, Moraal B, Barkhof F, de Groot V, Uitdehaag B, Killestein J. Real-world keystroke dynamics are a potentially valid biomarker for clinical disability in multiple sclerosis. Mult Scler. 2021 Aug;27(9):1421–31. doi: 10.1177/1352458520968797. https://journals.sagepub.com/doi/abs/10.1177/1352458520968797?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Lam KH, Twose J, Lissenberg-Witte B, Licitra G, Meijer K, Uitdehaag B, De Groot V, Killestein J. The use of smartphone keystroke dynamics to passively monitor upper limb and cognitive function in multiple sclerosis: longitudinal analysis. J Med Internet Res. 2022 Nov 07;24(11):e37614. doi: 10.2196/37614. https://www.jmir.org/2022/11/e37614/ v24i11e37614 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Arroyo-Gallego T, Ledesma-Carbayo MJ, Sanchez-Ferro A, Butterworth I, Mendoza CS, Matarazzo M, Montero P, Lopez-Blanco R, Puertas-Martin V, Trincado R, Giancardo L. Detection of motor impairment in Parkinson's disease via mobile touchscreen typing. IEEE Trans Biomed Eng. 2017 Sep;64(9):1994–2002. doi: 10.1109/tbme.2017.2664802. [DOI] [PubMed] [Google Scholar]
- 60.Iakovakis D, Hadjidimitriou S, Charisis V, Bostantzopoulou S, Katsarou Z, Hadjileontiadis LJ. Touchscreen typing-pattern analysis for detecting fine motor skills decline in early-stage Parkinson's disease. Sci Rep. 2018 May 16;8(1):7663. doi: 10.1038/s41598-018-25999-0. doi: 10.1038/s41598-018-25999-0.10.1038/s41598-018-25999-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Lipsmeier F, Taylor KI, Postuma RB, Volkova-Volkmar E, Kilchenmann T, Mollenhauer B, Bamdadian A, Popp WL, Cheng WY, Zhang YP, Wolf D, Schjodt-Eriksen J, Boulay A, Svoboda H, Zago W, Pagano G, Lindemann M. Reliability and validity of the Roche PD Mobile Application for remote monitoring of early Parkinson's disease. Sci Rep. 2022 Jul 15;12(1):12081. doi: 10.1038/s41598-022-15874-4. doi: 10.1038/s41598-022-15874-4.10.1038/s41598-022-15874-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Papadopoulos A, Iakovakis D, Klingelhoefer L, Bostantjopoulou S, Chaudhuri K, Kyritsis K, Hadjidimitriou S, Charisis V, Hadjileontiadis LJ, Delopoulos A. Unobtrusive detection of Parkinson's disease from multi-modal and in-the-wild sensor data using deep learning techniques. Sci Rep. 2020 Dec 07;10(1):21370. doi: 10.1038/s41598-020-78418-8. doi: 10.1038/s41598-020-78418-8.10.1038/s41598-020-78418-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Johnson SA, Karas M, Burke KM, Straczkiewicz M, Scheier ZA, Clark AP, Iwasaki S, Lahav A, Iyer AS, Onnela JP, Berry JD. Wearable device and smartphone data quantify ALS progression and may provide novel outcome measures. NPJ Digit Med. 2023 Mar 06;6(1):34. doi: 10.1038/s41746-023-00778-y. doi: 10.1038/s41746-023-00778-y.10.1038/s41746-023-00778-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Karas M, Olsen J, Straczkiewicz M, Johnson SA, Burke KM, Iwasaki S, Lahav A, Scheier ZA, Clark AP, Iyer AS, Huang E, Berry JD, Onnela JP. Tracking ALS disease progression using passively collected smartphone sensor data. SSRN. Preprint posted online August 3, 2023. 2024 doi: 10.2139/ssrn.4526533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Kiang MV, Chen JT, Krieger N, Buckee CO, Alexander MJ, Baker JT, Buckner RL, Coombs G 3rd, Rich-Edwards JW, Carlson KW, Onnela JP. Sociodemographic characteristics of missing data in digital phenotyping. Sci Rep. 2021 Jul 29;11(1):15408. doi: 10.1038/s41598-021-94516-7. doi: 10.1038/s41598-021-94516-7.10.1038/s41598-021-94516-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Currey D, Torous J. Increasing the value of digital phenotyping through reducing missingness: a retrospective review and analysis of prior studies. BMJ Ment Health. 2023 Feb 17;26(1):e300718. doi: 10.1136/bmjment-2023-300718. http://mentalhealth.bmj.com/lookup/pmidlookup?view=long&pmid=37197799 .bmjment-2023-300718 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Barnett I, Torous J, Reeder HT, Baker J, Onnela JP. Determining sample size and length of follow-up for smartphone-based digital phenotyping studies. J Am Med Inform Assoc. 2020 Dec 09;27(12):1844–9. doi: 10.1093/jamia/ocaa201. https://europepmc.org/abstract/MED/33043370 .5920884 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Paolillo EW, Lee SY, VandeBunte A, Djukic N, Fonseca C, Kramer JH, Casaletto KB. Wearable use in an observational study among older adults: adherence, feasibility, and effects of clinicodemographic factors. Front Digit Health. 2022 Jun 10;4:884208. doi: 10.3389/fdgth.2022.884208. https://europepmc.org/abstract/MED/35754462 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Di J, Demanuele C, Kettermann A, Karahanoglu FI, Cappelleri JC, Potter A, Bury D, Cedarbaum JM, Byrom B. Considerations to address missing data when deriving clinical trial endpoints from digital health technologies. Contemp Clin Trials. 2022 Feb;113:106661. doi: 10.1016/j.cct.2021.106661. https://linkinghub.elsevier.com/retrieve/pii/S1551-7144(21)00397-9 .S1551-7144(21)00397-9 [DOI] [PubMed] [Google Scholar]
- 70.Tackney MS, Cook DG, Stahl D, Ismail K, Williamson E, Carpenter J. A framework for handling missing accelerometer outcome data in trials. Trials. 2021 Jun 05;22(1):379. doi: 10.1186/s13063-021-05284-8. https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-021-05284-8 .10.1186/s13063-021-05284-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Barnett I, Onnela JP. Inferring mobility measures from GPS traces with missing data. Biostatistics. 2020 Apr 01;21(2):e98–112. doi: 10.1093/biostatistics/kxy059. https://europepmc.org/abstract/MED/30371736 .5145908 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Langener AM, Stulp G, Jacobson NC, Costanzo A, Jagesar RR, Kas MJ, Bringmann LF. It’s all about timing: exploring different temporal resolutions for analyzing digital-phenotyping data. Adv Method Pract Psychol Sci. 2024 Jan 19;7(1) doi: 10.1177/25152459231202677. [DOI] [Google Scholar]
- 73.Pereira R, Matalonga H, Couto M, Castor F, Cabral B, Carvalho P, de Sousa SM, Fernandes JP. GreenHub: a large-scale collaborative dataset to battery consumption analysis of android devices. Empir Softw Eng. 2021 Mar 20;26:38. doi: 10.1007/s10664-020-09925-5. [DOI] [Google Scholar]
- 74.Ford GS. Subsidies and substitution: an empirical study of the lifeline program. Telecommun Policy. 2021 Feb;45(1):102075. doi: 10.1016/j.telpol.2020.102075. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Visualization of raw battery percentage data binned by time of day (0=midnight; 23=11 PM) by disease severity group: (A) clinically normal, (B) prodromal frontotemporal lobar degeneration (FTLD), and (C) symptomatic FTLD.