

Abstract
Background
Fibrotic interstitial lung diseases (fILDs) are a heterogeneous group of lung diseases associated with significant morbidity and mortality. Despite a large increase in the number of clinical trials in the last 10 years, current regulatory-approved management approaches are limited to two therapies that prevent the progression of fibrosis. The drug development pipeline is long and there is an urgent need to accelerate this process. This manuscript introduces the concept and design of an innovative research approach to drug development in fILD: a global Randomised Embedded Multifactorial Adaptive Platform in fILD (REMAP-ILD).
Methods
Description of the REMAP-ILD concept and design: the specific terminology, design characteristics (multifactorial, adaptive features, statistical approach), target population, interventions, outcomes, mission and values, and organisational structure.
Results
The target population will be adult patients with fILD, and the primary outcome will be a disease progression model incorporating forced vital capacity and mortality over 12 months. Responsive adaptive randomisation, prespecified thresholds for success and futility will be used to assess the effectiveness and safety of interventions. REMAP-ILD embraces the core values of diversity, equity, and inclusion for patients and researchers, and prioritises an open-science approach to data sharing and dissemination of results.
Conclusion
By using an innovative and efficient adaptive multi-interventional trial platform design, we aim to accelerate and improve care for patients with fILD. Through worldwide collaboration, novel analytical methodology and pragmatic trial delivery, REMAP-ILD aims to overcome major limitations associated with conventional randomised controlled trial approaches to rapidly improve the care of people living with fILD.
Keywords: Connective tissue disease associated lung disease, Hypersensitivity pneumonitis, Idiopathic pulmonary fibrosis, Interstitial Fibrosis, Rheumatoid lung disease
Background
Interstitial lung diseases (ILDs) are a group of pulmonary disorders that occur due to a variety of causes, including many different environmental and genetic factors.1–4 ILDs are often subcategorised as fibrotic, inflammatory or fibroinflammatory based on clinical and radiological features, and in some cases, supplemented with immunological and histological data. Patients with fibrotic ILD (fILD) typically have a poor prognosis, with significant morbidity and mortality.5–8 There is an urgent unmet need for better pharmacological and non-pharmacological therapies for patients affected by fILD.9
Standard of care for fILD varies substantially, even for those fILDs where guidelines exist. The heterogeneity in the management of fILD reflects the lack of robust evidence in the field.10–13 Conversely, development of new therapeutic agents has been limited by the complexity and heterogeneity of disease pathophysiology. These challenges require changes to conventional drug development, including other non-pharmacological treatment modalities.
Previous clinical trial designs in fILD
Previous clinical trials in fILD have typically been conventional placebo-controlled randomised controlled trials (RCTs) that usually evaluated a single investigational product, with a treatment and a control arm, and a prespecified fixed sample size. Previous RCTs initially focused on idiopathic pulmonary fibrosis (IPF),14 15 with more recent attention on non-IPF fILD.16–18 However, the traditional research protocol misses several opportunities to increase efficiency such as investigating multiple interventions simultaneously, testing for interaction among treatment combinations and early stopping for non-promising interventions (tables 1 and 2).19–21 Alternative study designs such as the Randomised Embedded Multifactorial Adaptive Platform (REMAP) trials may be better equipped to efficiently explore potential treatments. Adaptive platform trials have successfully been implemented to investigate treatments in pancreatic cancer,22 Alzheimer’s disease,23 amyotrophic lateral sclerosis,19 community-acquired pneumonia (CAP) and COVID-19.24
Table 1.
Limitations of traditional randomised controlled trials in interstitial lung disease
| Typical limitations | |
| Trial design |
|
| Operational factors |
|
| Patient factors |
|
Table 2.
Key features of REMAP trials
| Key features | Description | |
| R | Randomised | Patients are randomised to all interventions for which they are eligible and consent to. |
| E | Embedded | The study protocol is embedded within routine clinical care, reflecting standard practice,and minimising additional study procedures. |
| M | Multifactorial | Multiple interventions (factors) are tested concurrently, with patients randomised to multiple treatment domains, increasing the probability of receiving at least one active treatment rather than control. |
| A | Adaptive | Information acquired during the trial is used to adaptively determine how the study should progress based on prespecified procedures in the protocol, such as a randomisation algorithm to determine randomisation weights to factors and stopping rules defining early success or futility. |
| P | Platform | A perennial infrastructure is developed with the objective to generate a continuous learning system. |
REMAP trials as a solution to challenges in identifying effective ILD treatments
REMAP trials are characterised by five key features as described in table 2. These key features provide multiple advantages over conventional RCTs, collectively maximising trial efficiency and supporting rapid generation of new knowledge.25 These advantages are particularly impactful for rare diseases such as fILD that have a poor prognosis, few evidence-based treatment options and numerous potential treatments/interventions at the clinical trial phase of development.26
Terminology
The distinct features of REMAP trials necessitate precise and standardised terminology. As defined in table 3, REMAP trials contain multiple mutually exclusive treatment factors. A factor describes the intervention being studied, which could be a medicinal or non-medicinal product. Examples of factors include existing standard of care treatments or active treatments. One or more factors may be grouped together into a treatment domain, with a domain describing a specific approach to clinical management. For example, an antifibrotic domain could include standard of care and one or more antifibrotic treatments, while an immunomodulatory domain could contain standard of care and one or more immunomodulatory treatments. A patient is randomised to a single factor within each domain of the adaptive platform trial and receives treatments in active domains for which they are eligible. Thus, a patient can be randomised to multiple factors across multiple domains. This collection of factors coming from separate domains administered to the individual patient is referred to as that patient’s regimen (figure 1). A stratum (for example, a diagnosis of IPF) captures a specific baseline disease characteristic that makes patients eligible or ineligible for particular domains, and can be used for stratified randomisation and/or strata-specific analyses. This means that not all patients entering the platform are eligible to be randomised to all platform domains. For example, an immunomodulatory domain is made unavailable for patients with IPF. REMAP trials also possess specific analytical characteristics, as described below, that can increase study efficiency.
Table 3.
Common terminology used in REMAP trials
| Term | Definition | Examples |
| Factor | The mutually exclusive interventions, categorised within domains, to which a patient can be randomised. |
|
| Domain | A distinct category of mutually exclusive interventions called factors; patients can be randomised to receive a factor from a domain for which they are eligible. |
|
| Regimen | The collection of factors that a patient is randomised to across domains; patients receive one unique factor from each domain for which they are eligible. |
|
| Stratum | Baseline disease characterisation that defines which domain(s) a patient is potentially eligible to participate in; strata can be used for stratified randomisation and strata-specific analyses. |
|
fILD, fibrotic interstitial lung disease; IPF, idiopathic pulmonary fibrosis; REMAP, Randomised Embedded Multifactorial Adaptive Platform.
Figure 1.
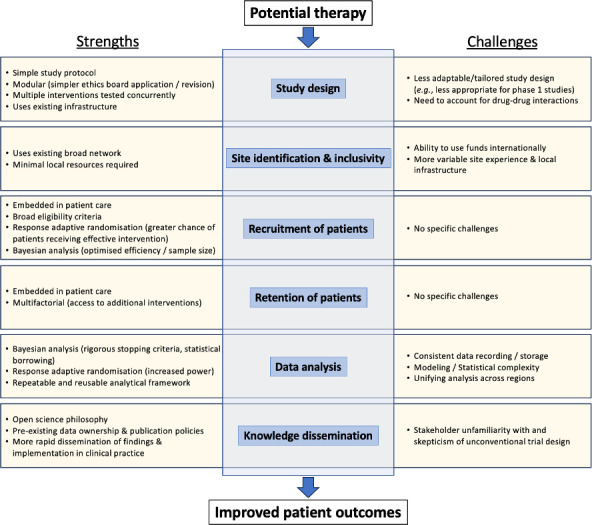
Strengths and challenges of REMAP trials as compared with conventional randomised controlled trials. REMAP, Randomised Embedded Multifactorial Adaptive Platform.
Principles of REMAP trials
REMAP trials are intended to operate as a perennial platform where new domains and/or factors (interventions) are added when understood to be a research priority and when additional funding to support such an addition is acquired (figure 2). They are randomised clinical trials centred around a core protocol that is embedded in routine patient care,15 17 reducing recruitment burden and increasing recruitment rate.27 The core protocol provides global details on trial design and conduct that is supplemented with domain-specific and region-specific appendices. These appendices describe prespecified protocol details for specific interventions and geographical regions; for example, details may include adaptations to treatment-specific exclusion criteria or specific healthcare system requirements.15 This modular structure allows rapid and efficient modification to individual components of the study with minimal disruption to overall study conduct, which includes the addition of new interventions or removal of ineffective interventions.
Figure 2.

Study overview. Patients with fibrotic ILD will be assessed for platform eligibility criteria (step 1), after which, screening for domain-specific eligibility criteria will be performed (step 2). Patients who meet eligibility criteria for at least one domain will be randomised to an intervention (factor) from each domain (step 3), which could include a variety of different options depending on the available interventions (indicated by subscripts). Patients would then be initiated on therapy and complete study assessments that allow analysis of efficacy, safety and cost-effectiveness outcomes (step 4). Predefined stopping criteria for each intervention will be assessed throughout the study (step 5), with termination of completed interventions (factors) and/or domains and initiation of new interventions (factors) and/or domains. Patients will be continuously assessed throughout their participation in the study for eligibility of previously existing and newly added domains. Domain refers to a group of interventions that are mutually exclusive. Interventions are called factors in the REMAP terminology. Ctrl, control arm; ILD, interstitial lung disease; REMAP, Randomised Embedded Multifactorial Adaptive Platform.
Multifactorial design
The multifactorial aspect of a REMAP trial permits simultaneous assessment of several interventions across multiple therapeutic domains and different disease strata.25 28 Multifactorial designs facilitate efficient use of resources, leveraging patient data across multiple domains and providing support for important, but potentially less commercially appealing, research questions enabling these research questions to be answered simultaneously with questions for which funding may be more readily obtainable. A patient can be assigned to the control arm in one domain but to active treatments in other domains. This patient-centred approach decreases the number of trial participants who receive only standard of care or placebo, ensuring that more patients receive active treatments, which appeals to patients and increases trial attractiveness.
Adaptive features
REMAP trials, like all RCTs, require a comprehensive statistical analysis plan (SAP) addressing typical issues, while also requiring additional work to arrive at the best adaptive features to be used prior to initiation of the trial. These design decisions are informed by extensive simulations whenever possible using real-world data.25 Design decisions are supported by the analysis of the trial performance characteristics under different simulated circumstances.
Multiple adaptive features can be employed, with the Bayesian statistical framework leveraging all available data, naturally enabling prespecified adaptations. These adaptive features include response-adaptive randomisation (RAR), which concentrates recruitment to therapies that appear to be beneficial, while minimising resource use and risks for enrolled patients.28 There is also greater potential to terminate a given factor or domain based on predetermined thresholds for success or futility.29 Similarly, should targeted therapies become available at some time in the future, the protocol can be adapted to incorporate stratified randomisation. All of these adaptive features are supported within a platform infrastructure that, once study start-up and site initiation are established, leverages the ongoing infrastructure to assess numerous therapies over time.
Recruitment and retention of patients
Not infrequently many patients are excluded from traditional clinical trials due to extensive inclusion and exclusion criteria.30 REMAP trials typically have broad eligibility criteria and simple study procedures that maximise patient recruitment while also retaining the ability to test heterogeneity of treatment effects across prespecified strata.29 Embedding the trial in routine clinical practice with minimal additional study visits also increases the likelihood that patients residing in more remote areas can participate. The simplified study protocol embedded within routine clinical care and the ability to randomise patients to multiple domains facilitate the retention of patients by reducing the burden of study visits and increasing the incentive to ongoing participation, respectively. To ensure that patients from low/middle-income countries can participate in REMAP-ILD, the core protocol is pragmatic, with minimally required data collection required to ensure successful delivery of the trial. This will reduce the burden of delivery and cost to ensure that more people can participate even in resource-scarce scenarios. All information and data collection tools will be translated into the languages of participating centres.
Data analysis
Initial power calculations and number needed to recruit are based whenever possible on simulated trials using real-world data. REMAP trials include frequent prespecified adaptive analyses, the timing and frequency of which are based on data obtained from simulated trials.28 Bayesian statistical methods are used during the trial to make prespecified changes to the protocol based on accruing data, including evaluation of differential treatment effects within prespecified strata, evaluation of prespecified intervention–intervention interactions and testing of multiple interventions.
An RAR algorithm may be used to preferentially randomise patients to interventions that have demonstrated a suggested benefit compared with other factors within a domain based on prespecified criteria that are assessed at interim analyses.28 The study continues until a statistical stopping rule for success, futility or harm has been triggered, or until complete follow-up for the predefined maximum sample size has been reached. Although a priori sample size estimates are generated, the exact sample size of REMAP trials is not fixed as in conventional RCTs. Instead, predefined minimum and maximum sample sizes are defined, with the potential to quickly declare success or futility, using prespecified statistical rules, based on accumulating data. Reaching study conclusions before reaching the maximum sample size, through triggering a prespecified statistical rule for success or futility, allows more efficient use of funding and leads to better patient care.21 31 32 This is an important advantage of REMAP trials, although it requires that regulatory agencies accept the employed analytical techniques.33
Funding structure
Funding global perennial adaptive platforms is a challenge as the current model for most funding organisations precludes fully integrated global collaboration by limiting the funds that can be transferred internationally. The funding structure is even more challenging for less-resourced countries and centres, as research funding is itself a source of research inequity. Further contributing to this challenge is the limited term for most funding sources, resulting in the need to frequently reapply for funding of a perennial international platform that tests multiple interventions over many years. Despite that, REMAP-CAP,24 an investigator-initiated global platform, was able to thrive and succeed. REMAP-ILD is being planned to adapt the learning and principles of REMAP-CAP to investigate therapies for fILD as outlined below. As per January 2024, various funding applications have been submitted. A REMAP trial design proposal has been submitted to the National Institute for Health and Care Research (UK). An investigator-initiated interventional trial activating the steroid domain has been submitted to the Swiss National Science Foundation (SNF) (Switzerland). A proposal to activate the antifibrotic and steroid domain is under negotiation with the Brazilian Ministry of Health, PROADI-SUS Programme (Brazil). In addition, the European Patient-driven Research Hub for Effective Interventions in Interstitial Lung Diseases analogue to the REMAP-ILD structure has been proposed in a first stage Horizon call submission (HORIZON-HLTH-2024-DISEASE-03-08-two-stage Comparative effectiveness research for healthcare interventions in areas of high public health need—European Union (EU)). The respective responses are currently pending. Additional submissions are currently under way to fund this global initiative and further sources of funding will be sought depending on the outcomes of these applications.
Knowledge dissemination
Governance policies within platform trials emphasise rapid and widespread dissemination of new knowledge through agreements on data sharing, data ownership and publication. The potential to reach earlier conclusions for success or futility contributes to the timely dissemination of evidence-based knowledge.
Randomised Embedded Multifactorial Adaptive Platform in fILD
Mission and values
REMAP-ILD is an international collaborative network (see online supplemental file 1) with the goal of rapidly and efficiently testing treatment options for patients with fILD, particularly therapies that are suitable for repurposing and thus less likely to be prioritised by pharmaceutical companies. REMAP-ILD is also interested in testing new drugs through phase II studies, which may be nested in the platform once it is established. The primary objective of REMAP-ILD is to test the effectiveness and safety of potential pharmacological and non-pharmacological treatments for fILD. Secondary objectives include assessment of specific subgroups of interest (eg, IPF vs non-IPF fILD) and cost-effectiveness, the latter will be specifically adapted at each regional level.
thorax-2023-221148supp001.pdf (108.9KB, pdf)
REMAP-ILD embraces the core values of diversity, equity and inclusion (DEI), and prioritises an open-science approach to data sharing and dissemination of results (see online supplemental file 2 for REMAP-ILD DEI statement).34 There are four key principles underpinning the work performed by the REMAP-ILD consortium: first, DEI is at the core, and as such REMAP-ILD has embedded these values throughout the study. REMAP-ILD policies, documents and a governance structure prioritise DEI for participants, staff and collaborators. Second, non-discrimination in any form. We will be proactive in fostering inclusion both for patient participants and research staff and collaborators. Third, global involvement and representation. We will actively engage with under-represented communities worldwide. Fourth, accountability and continuous improvement. We will work across the board to gain feedback and iteratively improve our efforts.
thorax-2023-221148supp002.pdf (51.9KB, pdf)
Patient population
REMAP-ILD will aim to focus on all adults with fILD, using eligibility criteria that are as broad and inclusive as possible. To ensure the presence of clinically meaningful fibrosis, patients will be required to have CT evidence of pulmonary fibrosis (ie, traction bronchiectasis, or reticulation, and/or honeycombing) affecting ≥10% of the lungs on CT visual assessment. Patients will not be required to have evidence of progression, which simplifies enrolment and broadens application to a clinically relevant patient population. Of note, the implications of including progressive and non-progressive fILD on trial design are being carefully simulated and will be described in a separate manuscript and in the SAP. Stable background therapy for ≥8 weeks will be required to minimise the influence of recently adjusted treatment. Exclusion criteria for the core protocol are minimal, with exclusion of only inflammatory-predominant ILD requiring urgent treatment, sarcoidosis or asbestosis as the primary ILD diagnosis, inability to perform forced pulmonary function test manoeuvres and expected survival <3 months. The exclusion of asbestosis and sarcoidosis is due to preliminary data demonstrating difference in disease progression in these groups compared with others. All other exclusion criteria will be in relation to patient safety. Domain-specific exclusions will apply.
Multifactorial design in REMAP-ILD
REMAP-ILD is intended to have multiple concurrently enrolling domains, each testing a distinct set of mutually exclusive interventions (figure 2). Patients will be randomised within each domain, receiving interventions for which they are eligible, potentially receiving multiple interventions (from different domains) under study. Several funding applications are under review across several countries, intended to initially support testing of antifibrotic therapy (pirfenidone and nintedanib), oral corticosteroids, immunomodulatory drugs (mycophenolate and azathioprine) and senolytics (metformin). Additional planned domains (eg, antitussive, pulmonary rehabilitation, diet, pulmonary vasodilators and possibly palliative care) will be activated as funding becomes available.
Primary outcome
The primary outcome will be a disease progression model over 12 months that incorporates measures of forced vital capacity (FVC) and mortality.
Study measurements
Protocol-specific tests will be minimal and will relate only to the baseline and 1-year assessments. All other study measurements will be those embedded in standard clinical care to minimise the burden on patients and healthcare staff, increase patient recruitment and retention, and reduce costs. These most notably include pulmonary function tests, patient-reported outcome measures (PROMs) and adverse effect monitoring. PROMs focus on dyspnoea, cough and quality of life, including health utilities that support cost-effectiveness analyses. Additional domain-specific protocolised measurements may be required. Adverse effects will be monitored and reported throughout the study and will be intervention dependent as performed in conventional trials.
Statistical analysis
REMAP-ILD will use RAR and prespecified rules for early stopping for success, harm or futility during preplanned interim analyses. REMAP-ILD power calculations and design decisions/choices are being informed by extensive simulations using real-world data coming from the PROFILE, INJUSTIS and CARE-PF Studies.35–37 The primary analysis for these domains is a joint model of the FVC per cent-predicted trajectory combined with the HR for mortality and will be detailed in future publications.
Governance structure
The governance structure of REMAP-ILD facilitates oversight and management of all aspects of the study (figure 3). The International Trial Steering Committee takes overall responsibility for the trial design and conduct. An international Domain-Specific Working Group exists for each domain and is responsible for design and oversight of each domain, while a Regional Management Committee takes primary responsibility for trial execution in each participating region and any adaptations that are described in the corresponding regional-specific appendix. While interim analyses and assessment of potential stopping rules will be overseen by an independent Data Safety Monitoring Board (DSMB), the DSMB will not make design decisions unless the trial’s algorithms are no longer acceptable from an ethical, safety or scientific point of view. To ensure appropriate prioritisation of interventions for REMAP-ILD domains, evidence will be assessed by an independent Therapy Prioritisation Advisory Group. Additional groups are responsible for other aspects of trial success (eg, DEI committee, health economics committee, patient and public advisory board) and all groups meet regularly to support study design and delivery. Patient participants are embedded throughout these committees and provided a platform for input on study design and conduct. REMAP-ILD is committed to adhering to all relevant data privacy regulations and guidelines to maintain patient confidentiality. Protection of patient data from unauthorised access will be ensured through the use of encrypted data collection tools such as OpenClinica, but with a federated data sharing model where regions own their own data. Overall, this integrated and scalable structure is designed to support REMAP-ILD’s mission of rapidly answering clinically relevant questions and facilitates the continual evolution required to meet the needs of people living with fILD.
Figure 3.

REMAP-ILD governance structure and their related documents. Dotted line boxes: desirable but not yet activated. Embedding refers to scenarios where REMAP-ILD will be embedded in clinical registries. Of note, if we succeed to embed REMAP-ILD in a clinical registry, patients will still be randomised to interventions within the registry. ILD, interstitial lung disease; REMAP, Randomised Embedded Multifactorial Adaptive Platform; Stats, statistical.
Challenges
Regulatory approvals
A major challenge associated with global platform trials such as REMAP relates to harmonisation of regulatory, data protection, ethical and governance procedures. Each region will have its own process for regulating trial conduct (eg, Food and Drug Administration, USA; European Medicine Agency, EU; Medicines and Healthcare products Regulatory Agency, UK) as well as procedures for implementation (eg, National Institute for Health and Care Excellence). Furthermore, implementation will depend on health economic assessments which will also be dependent on the nature of the intervention (high-cost therapy under patent vs repurposed generic drug vs non-pharmacological therapy). To overcome these challenges, numerous regional and special interest working groups are required (described in the Governance structure section) as well as iterative discussions with regulatory bodies to ensure that the simplest, most broadly applicable protocols align with their requirements.
Funding
Most funding agencies allow use of allocated funds only within specific regions, which presents a major challenge for a global investigator-driven network such as REMAP-ILD. This may lead to some components of the study being activated in only distinct regions depending on funding opportunities. This also highlights the need for improved international collaboration among funding organisations, particularly in the study of rare diseases such as fILD, so that international networks such as REMAP-ILD can function on a global scale. It is anticipated that initiation of REMAP-ILD and other similar platform trials will call attention to the need for major granting agencies to support research for rare diseases in a more sustainable and globally equitable manner.
Conclusion
REMAP-ILD is an innovative and efficient approach for investigating treatment efficacy and safety in fILDs, which will result in improved, evidence-based patient care. Through global collaboration, novel analytical methodology and pragmatic clinical trial delivery, we anticipate that the REMAP-ILD design will overcome major limitations associated with conventional development of therapeutic and non-pharmacological strategies in fILD, thereby improving the care of patients living with fILD across the world.
thorax-2023-221148supp003.pdf (107KB, pdf)
thorax-2023-221148supp004.pdf (99.7KB, pdf)
thorax-2023-221148supp005.pdf (90.4KB, pdf)
Footnotes
@leticiakawano, @tkulkarn1, @ILDIPFDoc_NI, @LucillaPiccari, @kaminskimed
LK-D, TK and CJR contributed equally.
WA and GJ contributed equally.
Collaborators: Members of the REMAP-ILD consortium are listed in online supplemental file 1.
Contributors: LK-D, TK, CJR, GJ, VC and WA were responsible for the conceptual design of the manuscript. BW, TJ, MQ and RL were responsible for the statistical analysis section. PR-O, BGB, NC, MF-C, A-MH-V, KAJ, YHK, SBM, LP, HP, MM-M, JST, IB-V, SR, JJ, DR, LGS, MK, ACG, FJM, NK and VC provided critical input to the manuscript and are active members of REMAP-ILD consortium. All members listed in the REMAP-ILD consortium (online supplemental file 1) agreed with the content of the manuscript.
Funding: This study was funded by Efficacy and Mechanism Evaluation Programme (NIHR154383).
Competing interests: LK-D—research grants from Boehringer Ingelheim and Bristol-Myers-Squibb, research grant from the Brazilian Ministry of Health (PROADI-SUS), non-financial research support from Fisher & Paykel; personal fees from Sarava and Boehringer Ingelheim. TK—personal fees from Boehringer Ingelheim, United Therapeutics, Puretech and Veracyte. CJR—research grant from Boehringer Ingelheim; personal fees from Boehringer Ingelheim, Pliant Therapeutics, AstraZeneca, Trevi Therapeutics, Hoffmann La Roche and Cipla. PR-O—research grants from Boehringer Ingelheim, Hoffmann La Roche, CSL Behring, FibroGen, Vicore Pharma, Gilead, Galecto and Chiesi; personal fees from Boehringer Ingelheim, Hoffmann La Roche, Cipla, Tecnofarma, Respiratory Effectiveness Group and The Limbic. NC—personal fees from Boehringer Ingelheim, Liminal Biosciences, Vicor Pharma, Bridge Biotherapeutics and Transcrip. MF-C—research grants from CSL Behring, Boehringer Ingelheim and Roche; personal fees from Boehringer Ingelheim, MSD, AstraZeneca and GSK. A-MH-V—research grants from Boehringer Ingelheim and Janssen; personal fees from ARXX, Boehringer Ingelheim, Janssen, Medscape, Roche, Genentech, Bayer, Lilly and Merck Sharp & Dohme. KAJ—research grants from University Hospital Foundation and Three Lakes Foundation; personal fees from Boehringer Ingelheim, Pliant, Thyron, Brainomix and Hoffman La Roche. YHK—research grants from NHMRC, MRFF, Air Liquide Healthcare, Austin Medical Research Foundation, Lung Foundation Australia/Thoracic Society of Australia and New Zealand, and RACP. SBM—research grants from Three Lakes Foundation, NIH/NHLBI, Merck, Boehringer Ingelheim, Pliant Therapeutics, American Thoracic Society, and National Scleroderma Foundation; personal fees from Wolters Kluwer, Roche, DevPro Biopharma, Gilead, Accendatech, Cowen and APIE Therapeutics. LP—research grants from Janssen and Ferrer; personal fees from Janssen, Ferrer, United Therapeutics, MSD and Liquidia. HP—research grants from Boehringer Ingelheim, AstraZeneca and Siemens; personal fees from Boehringer Ingelheim, Sanofi, Janssen, MSD, AstraZeneca and Chiesi. MM-M—research grants from Boehringer Ingelheim and Roche; personal fees from Boehringer Ingelheim, Ferrer and Chiesi. JST—research grant from Boehringer Ingelheim; personal fees from Boehringer Ingelheim and Aflofarm. SR—personal fees from Cipla and Boehringer Ingelheim. JJ—research grants from Gilead, Microsoft research and GSK; personal fees from Boehringer Ingelheim, Roche, GSK and Takeda. DR—research grants from NIHR; personal fees from OMass Therapeutics, Sosei Heptares and GSK. LGS—personal fees from Daiichi Sankyo and Chiesi. MK—research grants from Boehringer Ingelheim and Roche; personal fees from Nichtraucherhelden/Sanero, Boehringer Ingelheim and Roche. NK—research grants from Veracyte, Boehringer Ingelheim, BMS and non-financial support from AstraZeneca; scientific founder at Thyron; personal fees from Boehringer Ingelheim, Pliant, AstraZeneca, RohBar, Veracyte, Augmanity, CSL Behring, Splisense, Galapagos, Fibrogen, GSK, Merck and Thyron; and reports Equity in Pliant and Thyron. RL—senior consultant for Berry Consultants. WA—personal fees from Boehringer Ingelheim. GJ—research grants from AstraZeneca, Biogen, Galecto, GSK, Nordic Biosciences, RedX and Pliant; personal fees from Apollo Therapeutics, AstraZeneca, Brainomix, Bristol-Myers-Squibb, Chiesi, Cohbar, Daewoong, Veracyte, GSK, Resolution Therapeutics, Pliant, Hoffmann La Roche, PatientMPower, Pinsent Masons, Galapagos and Vicore Pharma. BGB, IB-V, BW, TJ, MQ and VC have no conflicts to declare.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Contributor Information
Collaborators: REMAP-ILD consortium, Amanda Bravery, Amanda Goodwin, Ana Etges, Ana Boshoff, Andreas Günther, Andrew Briggs, Andrew Palmer, Andrew Wilson, Anjali Crawshaw, Anna-Maria Hoffmann-Vold, Anne Bergeron, Anne Holland, Anthony C Gordon, Antje Prasse, Argyris Tzouvelekis, Athina Trachalaki, Athol Wells, Avinash Anil Nair, Ayodeji Adegunsoye, Barbara Wendelberger, Ben Hope-Gill, Bhavika Kaul, Bibek Gooptu, Bruno Guedes Baldi, Bruno Crestani, Carisi Anne Polanczyk, Carlo Vancheri, Carlos Crobal, Charlotte Summers, Chris Grainge, Chris J Ryerson, Christophe von Garnier, Christopher Huntley, Claudia Ravaglia, Claudia Valenzuela, Conal Hayton, Cormac McCarthy, Daniel Chambers, Daphne Babalis, David Thicket, David Turner, Deepak Talwar, Devaraj Anand, Devesh Dhasmana, Dhruv Parek, Diane Griffiths, Diego Castillo Villegas, Duncan Richards, Eliana Santucci, Elisabeth Bendstrup, Elisabetta Balestro, Eliza Tsitoura, Emanuela Falaschetti, Ena Gupta, Erica Farrand, Fasihul Khan, Fernando J Martinez, Francesco Bonella, Francesco Lombardi, Gary M Hunninghake, Gauri Saini, Gisli Jenkins, Gunnar Gudmundsson, Harold Collard, Helen Parfrey, Helmut Prosch, Hernan Fainberg, Huzaifa Adamali, Iain Stewart, Ian Forrest, Ian Glaspole, Iazsmin Bauer-Ventura, Imre Noth, Ingrid Cox, Irina Strambu, Jacobo Sellares, James Eaden, Janet Johnston, Jeff Swigris, John Blaikley, John S Kim, Jonathan Chung, Joseph A Lasky, Joseph Jacob, Joyce Lee, Juergen Behr, Karin Storrer, Katarzyna Lewandowska, Kate Johnson, Katerina Antoniou, Katrin Hostettler, Kerri A Johannson, Killian Hurley, Kirsty Hett, Larissa Schwarzkopf, Laura Fabbri, Laura Price, Laurence Pearmain, Leticia Kawano-Dourado, Liam Galvin, Lisa G Spencer, Lisa Watson, Louise Crowley, Luca Richeldi, Lucilla Piccari, Manuela Funke-Chambour, Maria Molina-Molina, Mark Jones, Mark Spears, Mark Toshner, Marlies Wijsenbeek-Lourens, Martin Brutsche, Martina Vasakova, Melanie Quintana, Michael Gibbons, Michael Henry, Michael P Keane, Michael Kreuter, Milena Man, Mohsen Sadatsafavi, Naftali Kaminski, Nazia Chaudhuri, Nick Weatherley, Nik Hirani, Ovidiu Fira Mladinescu, Paolo Spagnolo, Paul Beirne, Peter Bryce, Peter George, Philip L Molyneaux, Pilar Rivera-Ortega, Radu Crisan-Dabija, Rahul Maida, Raphael Borie, Reoto Takei, Roger Lewis, Rui Rolo, Sabina Guler, Sabrina Paganoni, Sally Singh, Sara Freitas, Sara Piciucchi, Shama Malik, Shaney Barratt, Simon Hart, Simone Dal Corso, Sophie V Fletcher, Stefan Stanel, Stephen Bianchi, Steven Jones, Steven Nathan, Sujeet Rajan, Surinder Birring, Sydney B Montesi, Takei Reoto, Tamara J Corte, Tanzira Zaman, Tejaswini Kulkarni, Timothy Gatheral, Tom Jensen, Tom McMillan, Valerie Quinn, Venerino Poletti, Victoria Cornelius, Vincent Cottin, Wendy Adams, Wim Wuyts, Yasuhiro Kondoh, Yasunari Miyazaki, Yet Hong Khor, and Yussef Haider
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
Not applicable.
References
- 1. Travis WD, Costabel U, Hansell DM, et al. An official American Thoracic society/European respiratory society statement: update of the International multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2013;188:733–48. 10.1164/rccm.201308-1483ST [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Newton CA, Oldham JM, Ley B, et al. Telomere length and genetic variant associations with interstitial lung disease progression and survival. Eur Respir J 2019;53:1801641. 10.1183/13993003.01641-2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Dressen A, Abbas AR, Cabanski C, et al. Analysis of protein-altering variants in telomerase genes and their association with MUC5B common variant status in patients with idiopathic pulmonary fibrosis: a candidate gene sequencing study. Lancet Respir Med 2018;6:603–14. 10.1016/S2213-2600(18)30135-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Abramson MJ, Murambadoro T, Alif SM, et al. Occupational and environmental risk factors for idiopathic pulmonary fibrosis in Australia: case–control study. Thorax 2020;75:864–9. 10.1136/thoraxjnl-2019-214478 [DOI] [PubMed] [Google Scholar]
- 5. Khor YH, Ng Y, Barnes H, et al. Prognosis of idiopathic pulmonary fibrosis without anti-fibrotic therapy: a systematic review. Eur Respir Rev 2020;29:157. 10.1183/16000617.0158-2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Fernández Pérez ER, Kong AM, Raimundo K, et al. Epidemiology of hypersensitivity pneumonitis among an insured population in the United States: a claims-based cohort analysis. Ann Am Thorac Soc 2018;15:460–9. 10.1513/AnnalsATS.201704-288OC [DOI] [PubMed] [Google Scholar]
- 7. Adegunsoye A, Oldham JM, Bellam SK, et al. Computed tomography honeycombing identifies a progressive fibrotic phenotype with increased mortality across diverse interstitial lung diseases. Ann Am Thorac Soc 2019;16:580–8. 10.1513/AnnalsATS.201807-443OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Raimundo K, Solomon JJ, Olson AL, et al. Rheumatoid arthritis–interstitial lung disease in the United States: prevalence, incidence, and healthcare costs and mortality. J Rheumatol 2019;46:360–9. 10.3899/jrheum.171315 [DOI] [PubMed] [Google Scholar]
- 9. Tikellis G, Tong A, Lee JYT, et al. Top 10 research priorities for people living with pulmonary fibrosis, their caregivers, healthcare professionals and researchers. Thorax 2021;76:575–81. 10.1136/thoraxjnl-2020-215731 [DOI] [PubMed] [Google Scholar]
- 10. Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 2018;198:e44–68. 10.1164/rccm.201807-1255ST [DOI] [PubMed] [Google Scholar]
- 11. Raghu G, Remy-Jardin M, Ryerson CJ, et al. Diagnosis of hypersensitivity pneumonitis in adults. an official ATS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 2020;202:e36–69. 10.1164/rccm.202005-2032ST [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Raghu G, Montesi SB, Silver RM, et al. Treatment of systemic sclerosis-associated interstitial lung disease: evidence-based recommendations. an official American Thoracic society clinical practice guideline. Am J Respir Crit Care Med 2024;209:137–52. 10.1164/rccm.202306-1113ST [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Raghu G, Remy-Jardin M, Richeldi L, et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 2022;205:e18–47. 10.1164/rccm.202202-0399ST [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. King TE, Bradford WZ, Castro-Bernardini S, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med 2014;370:2083–92. 10.1056/NEJMoa1402582 [DOI] [PubMed] [Google Scholar]
- 15. Richeldi L, du Bois RM, Raghu G, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med 2014;370:2071–82. 10.1056/NEJMoa1402584 [DOI] [PubMed] [Google Scholar]
- 16. Maher TM, Corte TJ, Fischer A, et al. Pirfenidone in patients with unclassifiable progressive fibrosing interstitial lung disease: a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet Respir Med 2020;8:147–57. 10.1016/S2213-2600(19)30341-8 [DOI] [PubMed] [Google Scholar]
- 17. Flaherty KR, Wells AU, Cottin V, et al. Nintedanib in progressive fibrosing interstitial lung diseases. N Engl J Med 2019;381:1718–27. 10.1056/NEJMoa1908681 [DOI] [PubMed] [Google Scholar]
- 18. Behr J, Prasse A, Kreuter M, et al. Pirfenidone in patients with progressive fibrotic interstitial lung diseases other than idiopathic pulmonary fibrosis (RELIEF): a double-blind, randomised, placebo-controlled, phase 2B trial. Lancet Respir Med 2021;9:476–86. 10.1016/S2213-2600(20)30554-3 [DOI] [PubMed] [Google Scholar]
- 19. Paganoni S, Berry JD, Quintana M, et al. Adaptive platform trials to transform amyotrophic lateral sclerosis therapy development. Ann Neurol 2022;91:165–75. 10.1002/ana.26285 [DOI] [PubMed] [Google Scholar]
- 20. Broglio K, Meurer WJ, Durkalski V, et al. Comparison of Bayesian vs frequentist adaptive trial design in the stroke hyperglycemia insulin network effort trial. JAMA Netw Open 2022;5:e2211616. 10.1001/jamanetworkopen.2022.11616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Berry SM, Connor JT, Lewis RJ. The platform trial: an efficient strategy for evaluating multiple treatments. JAMA 2015;313:1619–20. 10.1001/jama.2015.2316 [DOI] [PubMed] [Google Scholar]
- 22. Picozzi VJ, Duliege A-M, Collisson EA, et al. Precision promise (PrP): an adaptive, multi-arm registration trial in metastatic pancreatic ductal adenocarcinoma (PDAC). JCO 2022;40:TPS4188-TPS. 10.1200/JCO.2022.40.16_suppl.TPS4188 [DOI] [Google Scholar]
- 23. Bateman RJ, Benzinger TL, Berry S, et al. The DIAN-TU next generation Alzheimer’s prevention trial: adaptive design and disease progression model. Alzheimers Dement 2017;13:8–19. 10.1016/j.jalz.2016.07.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Angus DC, Berry S, Lewis RJ, et al. The REMAP-CAP (randomized embedded multifactorial adaptive platform for community-acquired pneumonia) study. Rationale and design. Ann Am Thorac Soc 2020;17:879–91. 10.1513/AnnalsATS.202003-192SD [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Adaptive Platform Trials Coalition . Adaptive platform trials: definition, design, conduct and reporting considerations. Nat Rev Drug Discov 2019;18:797–807. 10.1038/s41573-019-0034-3 [DOI] [PubMed] [Google Scholar]
- 26. White ES, Thomas M, Stowasser S, et al. Challenges for clinical drug development in pulmonary fibrosis. Front Pharmacol 2022;13:823085. 10.3389/fphar.2022.823085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Chaudhari N, Ravi R, Gogtay NJ, et al. Recruitment and retention of the participants in clinical trials: challenges and solutions. Perspect Clin Res 2020;11:64–9. 10.4103/picr.PICR_206_19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Viele K, Saville BR, McGlothlin A, et al. Comparison of response adaptive randomization features in multiarm clinical trials with control. Pharm Stat 2020;19:602–12. 10.1002/pst.2015 [DOI] [PubMed] [Google Scholar]
- 29. Saville BR, Berry SM. Efficiencies of platform clinical trials: a vision of the future. Clin Trials 2016;13:358–66. 10.1177/1740774515626362 [DOI] [PubMed] [Google Scholar]
- 30. Khor YH, Schulte M, Johannson KA, et al. Eligibility criteria from pharmaceutical randomised controlled trials of idiopathic pulmonary fibrosis: a registry-based study. Eur Respir J 2023;61:2202163. 10.1183/13993003.02163-2022 [DOI] [PubMed] [Google Scholar]
- 31. Berry DA. Adaptive clinical trials in oncology. Nat Rev Clin Oncol 2011;9:199–207. 10.1038/nrclinonc.2011.165 [DOI] [PubMed] [Google Scholar]
- 32. Bhatt DL, Mehta C. Adaptive designs for clinical trials. N Engl J Med 2016;375:65–74. 10.1056/NEJMra1510061 [DOI] [PubMed] [Google Scholar]
- 33. Services USDoHaH, (FDA) FaDA, Health CfDaR, Research CfBEa . Adaptive designs for medical device clinical studies guidance for industry and food and drug administration staff [FDA]. 2016. Available: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/adaptive-designs-medical-device-clinical-studies
- 34. Versavel S, Subasinghe A, Johnson K, et al. Diversity, equity, and inclusion in clinical trials: a practical guide from the perspective of a trial sponsor. Contemp Clin Trials 2023;126:107092. 10.1016/j.cct.2023.107092 [DOI] [PubMed] [Google Scholar]
- 35. Maher TM, Oballa E, Simpson JK, et al. An epithelial biomarker signature for idiopathic pulmonary fibrosis: an analysis from the multicentre PROFILE cohort study. Lancet Respir Med 2017;5:946–55. 10.1016/S2213-2600(17)30430-7 [DOI] [PubMed] [Google Scholar]
- 36. Khan F, Stewart I, Howard L, et al. The its not JUST idiopathic pulmonary fibrosis study (INJUSTIS): description of the protocol for a multicentre prospective observational cohort study identifying biomarkers of progressive fibrotic lung disease. BMJ Open Respir Res 2019;6:e000439. 10.1136/bmjresp-2019-000439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Ryerson CJ, Tan B, Fell CD, et al. The Canadian registry for pulmonary fibrosis: design and rationale of a national pulmonary fibrosis registry. Can Respir J 2016;2016:3562923. 10.1155/2016/3562923 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
thorax-2023-221148supp001.pdf (108.9KB, pdf)
thorax-2023-221148supp002.pdf (51.9KB, pdf)
thorax-2023-221148supp003.pdf (107KB, pdf)
thorax-2023-221148supp004.pdf (99.7KB, pdf)
thorax-2023-221148supp005.pdf (90.4KB, pdf)