

Abstract
Objectives:
This study developed a causal relationship model of herb use from observational data and analyzed the direct and indirect effects of herb use on health according to the model.
Methods:
A cross-sectional study was conducted with 400 participants aged 26-59 years, selected through multistage random sampling. The instruments used for data collection included demographic information, herb use, health literacy (HL), perceived social support, societal values, and attitudes toward herb use. The conceptual model, hypothesized based on prior evidence, was tested using confirmatory factor analysis through structural equation modeling. Path coefficients were estimated using the maximum likelihood method.
Results:
The final model utilized empirical data, which showed that perceived social support had the most significant impact on herb use. This was followed by HL, positive attitudes toward herbal remedies, and societal values, with coefficients of 0.31, 0.18, and 0.16, respectively. When analyzing variables that indirectly affected herb use, it was clear that positive attitudes, perceived social support, and societal values significantly influenced herb use through HL, with influence coefficients of 0.08, 0.16, and 0.04, respectively. Together, these variables accounted for 68% of the variance in herb use.
Conclusions:
The findings from this study can be utilized to develop and implement strategies that guide the use of herbal products, ultimately aiming to improve human health.
Keywords: Adult, Attitude, Health literacy, Herbal, Social support
GRAPHICAL ABSTRACT

INTRODUCTION
The global spread of diseases has increased interest in herbal remedies for self-care, driven by factors such as cost and accessibility [1]. Although distinct from modern treatments, herbal medicines are still subject to efficacy testing. The use of herbal remedies aims to improve overall well-being, including immunity and disease management, by utilizing readily available herbs [2]. Herbal use, steeped in theory and history, has been transmitted across generations [3]. Working adults with disposable income often fall prey to misleading marketing of herbal dietary supplements, leading to incorrect usage that can be more detrimental than beneficial to their health. Recognizing patterns of herb use is crucial in highlighting the dangers of misuse. Misuse can be exacerbated by misleading information and a lack of adequate health literacy (HL) [4]. Factors such as individual circumstances and HL levels can influence such behaviors [5].
HL can be defined as the ability to locate, comprehend, assess, and utilize health-related information to prevent illness and enhance overall health. It serves as a bridge connecting various factors to health outcomes, helping individuals make informed decisions about the use of herbal health remedies [6]. This involves understanding health systems, interpreting information, and making independent health decisions in collaboration with healthcare providers [7]. Research has shown that HL significantly affects herb use, with some studies indicating that it influences as much as 89.5% of herb use among individuals with chronic illnesses [8].
Sørensen et al. [9]’s integrated model of HL posits that HL is a process involving the comprehension, assessment, and implementation of health-related information in a way that promotes healthy behavior. Mancuso [10]’s model additionally highlights that HL serves as a mediator between upstream factors and health behaviors. The 3 determinants of these upstream factors are intrapersonal, interpersonal, and environmental.
Intrapersonal factors relate to the characteristics and beliefs of individuals. Research has demonstrated that attitudes significantly impact the use of herbal remedies. For example, Soltanipour et al. [11] found that adults who held positive attitudes toward herbal remedies were more likely to use them. Likewise, a study conducted in northeastern Bulgaria showed that attitudes toward herb use markedly affected the consumption of herbal medicines and supplements [12].
Environmental factors encompass a range of conditions related to an individual’s birth, growth, living, working, and aging. Social values, which encompass social and environmental determinants, are often regarded as virtuous or worthy of being passed down [13]. Historically, the use of herbs for medical care, treatment, or health promotion has been widely accepted and practiced. It has been observed that social values influence herb uses for health, as they affect personal choices and are recognized by the social environment [14].
Interpersonal factors involve interactions with both individuals and the physical environment. Research has shown that social support plays a significant role in influencing herb use for health purposes. For example, a study conducted by Guo et al. [15] demonstrated that social support had a direct impact on adherence to herb use, even after adjusting for age and marital status. Furthermore, social support also indirectly affected adherence through its relationship with HL.
In accordance with Bandura [16]’s social cognitive learning theory, which posits that behavior can change due to personal and environmental factors, this study acknowledges that elements such as interpersonal, intrapersonal, and environmental influences can modify behavior. The research found that HL, attitudes, and contextual variables, including social support and societal values, all impact the behavior of individuals using medicinal products. Mancuso [10]’s concept was employed in this study to develop a causal model of HL, which was integrated with Bandura [16]’s theory to create a causal model of herb use.
Herbal drugs and supplements are commonly used for primary healthcare and treatment worldwide. Manufacturers typically highlight the benefits, but incorrect use or abuse can lead to adverse effects, particularly if not customized to an individual’s biological circumstances. Users often possess limited knowledge regarding the suitability and safety of herbal products [17]. Therefore, minimizing the risk of toxicity-related harm requires appropriate HL.
While the consumption of herbal products is increasing in Thailand, there is a significant lack of research on its prevalence and the factors associated with it, especially among working-age adults. This study seeks to fill this void by using a HL model to explore attitudes, social support, and literacy related to herbal product use. Conducted in Nakhon Nayok Province, which is known for its abundant natural resources and traditional remedies, the research focuses on identifying personal, interpersonal, and environmental factors that influence herbal consumption. By understanding these factors, the study aims to promote responsible use of herbal products, thereby enhancing proper usage and dietary habits for health benefits. The findings could provide valuable insights into fostering sustainable herbal practices that benefit individuals, communities, and the nation as a whole.
METHODS
Study Population
The study utilized a descriptive cross-sectional survey methodology and was conducted from August 2023 to October 2023. The population consisted of Thai working-age adults in Nakhon Nayok Province. A multistage random sampling method was used to select participants from the population served by each health service facility. This approach is particularly useful when it is costly or inefficient to sample every element from the selected clusters, and it is often adopted when a complete list of the population is not available or practical. The initial cluster random selection included 4 districts with similar characteristics: Mueang Nakhon Nayok District, Pak Phli District, Ban Na District, and Ongkharak District. From these, Ongkharak and Mueang Nakhon Nayok were randomly selected. Within each district, the population was stratified to evenly represent both urban and rural areas, both inside and outside the municipality. Participants eligible for the study were individuals aged 26 to 59 who had previously used herbal health products, had no communication barriers, had resided in their current urban or rural location for at least 10 years, were free from serious illnesses, had no history of allergic reactions to herbs, and were willing to provide informed consent. Individuals who might find it difficult to understand and respond to the questionnaire, even with assistance from the facilitator, were excluded from the study.
Structural equation modeling (SEM) was employed to explore the mediation effect. Previous research indicates that SEM requires a sample size of 10-15 times the number of variables [18]. After accounting for a 20% non-response rate, the final sample size was determined to be 400 respondents, which is recommended for SEM when using the maximum likelihood estimation approach [19].
Questionnaire
Demographic characteristics
Data on various demographic qualities, including gender, age, education, health, occupation, income, family history, and herbal product usage, were collected as these factors can influence individuals’ preferences for using herbal medicines.
Herb use
Herb use was evaluated using a modified version of the “Behavior of Using Herbs for Self-Care” questionnaire [20]. This questionnaire was translated into Thai through translation and back-translation and comprised 14 items that evaluated herb use in 2 distinct categories: treatment of health problems and disease, and prevention of disease and health promotion. Responses were collected using a 5-point Likert scale, where higher scores indicated more frequent use of herbal products for health promotion. A score of 1 corresponded to “never,” and a score of 5 to “always.” The content validity of the questionnaire was established by a panel of 3 experts, with Index of Item Objective Congruence (IOC) scores ranging from 0.60 to 1.00. Cronbach’s alpha for the questionnaire was 0.97, indicating high reliability. The model demonstrated a good fit with the empirical data according to the confirmatory factor analysis (CFA) results (chi-square=108.15, degrees of freedom [df]=43, chi-square/df=2.52, root-mean squared error of approximation [RMSEA]=0.06, standardized root mean residual [SRMR]=0.04, goodness-of-fit index [GFI]=0.96, comparative fit index [CFI]=0.99, and normed fit index [NFI]=0.98). The factor loadings for all questions met the standard criteria, with values ranging from 0.58 to 0.86.
HL
The HL assessment evaluated 3 components: (1) accessing health information and services, (2) evaluating health information and services, and (3) managing one’s health. It utilized a modified version of the Thai HL scales for adults [21]. Each item on the questionnaire demonstrated a Cronbach’s alpha ranging from 0.87 to 0.91, with discriminant power between 0.56 and 0.76. The overall reliability coefficient for the questionnaire was 0.94. The model exhibited a good fit with the empirical data according to CFA (chi-square=486.45, df=218, chi-square/df=2.31, RMSEA=0.05, SRMR=0.05, GFI=0.90, CFI=0.99, and NFI=0.98). The factor loadings for all questions met the standard criteria, with values ranging from 0.59 to 0.85.
Social support perceptions
Perceptions of social support were measured using a modified version of the Multidimensional Scale of Perceived Social Support (MSPSS) developed by Zimet et al. [22]. The MSPSS was translated into Thai following standard procedures. The scale included items that assessed support from friends and family, which were rated on a 5-point Likert scale from 1 (no support) to 5 (a lot of support). Content validity was established by experts, and the Cronbach’s alpha coefficient was 0.95.
Social values
Social values were assessed using a modified scale created by Chartprasert and Deedenkeeratisakul [23]. The questionnaire comprised ten items, and participants rated each item on a 5-point Likert scale, where 1 represents strong disagreement and 5 represents strong agreement. Higher scores signified a greater level of social values. Content validity was established by experts, with IOC values ranging from 0.60 to 1.00, indicating satisfactory validity. The scale demonstrated high reliability, evidenced by a reliability coefficient of 0.95.
Attitudes toward the use of herbal products
Attitudes toward herbal product usage were assessed using 10 items adapted from Udompitayson [24]’s survey. These items measured feelings, beliefs, knowledge, opinions, and behavioral habits associated with the use of herbal products. Responses were recorded on a 5-point Likert scale, where 1 represents strong disagreement and 5 represents strong agreement, with higher scores indicating more positive attitudes. Content validity was established by experts, with IOC values ranging from 0.60 to 1.00, demonstrating satisfactory validity. The reliability coefficient for the scale was 0.95.
Data collection procedure
Participants were required to review and consent to the terms and conditions, providing an electronic signature before accessing the questionnaire. The survey collected demographic details and information on herbal product usage, HL, social support, societal values, and attitudes toward the use of herbal products for health. On average, completing the questionnaire took about 30 minutes.
Statistical Analysis
Data were analyzed using SPSS version 21 (IBM Corp., Armonk, NY, USA). Skewness and kurtosis were investigated to evaluate the data for normality, and missing values were inferred using the median. Data preprocessing included screening with indicators. Subsequently, the measurement model and structural equations were analyzed using LISREL software.
The chi-square test, along with several other indices, was employed to evaluate the model’s fit. These indices included the CFI, GFI, NFI, and RMSEA. Additionally, 90% confidence intervals were used. A non-significant chi-square test, GFI, CFI, and NFI values above 0.95, and an RMSEA below 0.06 were deemed to indicate a well-fitting model [25].
Ethics Statement
The study received approval from the Ethics Committee of Srinakharinwirot University (SWUEC 082/2566 E). All participants capable of doing so provided written informed consent, while those unable to write gave their consent verbally. Data collection was conducted anonymously and excluded any personal identifiers.
RESULTS
A total of 400 participants completed the data collection questionnaire. Among them, 62.5% were female, 52.7% were married, and 33.2% fell within the 41-50 age bracket. Additionally, 27.0% were employed, 42.2% had completed high school education, and 41.2% either considered their income sufficient or did not have savings. Furthermore, 63.0% had some knowledge of alternative medicine, and 82.7% reported no underlying diseases. Analysis of the data distributions for the variables under investigation indicated that the data generally followed a normal distribution. These findings are presented in Table 1.
Table 1.
The mean, standard deviation (SD), skewness, and kurtosis of the data obtained from measuring the variables after standardization
| Variables | Mean±SD | Skewness | Kurtosis | p-value |
|---|---|---|---|---|
| Access to health information and services | 3.69±0.71 | -0.27 | -0.51 | 0.85 |
| Examination of health information and services | 3.85±0.65 | -0.65 | -0.92 | 0.53 |
| Decision-making in using herbal products for health care | 3.82±0.65 | -0.62 | -1.08 | 0.46 |
| Behavior of using herbal products to promote health | 4.00±0.64 | -0.56 | -1.06 | 0.49 |
| Behavior of using herbal products for disease treatment | 3.81±0.74 | -0.63 | -0.98 | 0.51 |
| Societal values toward the use of herbal products | 4.20±0.57 | -1.03 | -1.70 | 0.14 |
| Positive attitudes toward the use of herbal products | 3.85±0.63 | -0.13 | -0.84 | 0.97 |
| Perceived social support | 3.62±0.72 | -0.16 | -0.78 | 0.14 |
Correlations of Variables
The researchers analyzed the relationships among variables using the Pearson product-moment correlation coefficient, identifying statistically significant correlations at the 0.05 level. The strongest correlations observed were between “examination of health information and services” and “decision-making in using herbal products for health care” (0.76), and between “behavior of using herbal products to promote health” and “behavior of using herbal products for disease treatment” (0.76). The weakest correlation was found between “cultural values” and “social support” (0.32).
The relationships between variables were examined through bivariate analysis, which involved calculating the Pearson product-moment correlation coefficient. The analysis revealed that no values exceeded 0.80, confirming the suitability of the data for further analysis using SEM [26], as detailed in Table 2.
Table 2.
Correlations of variables
| Variables | HL1 | HL2 | HL3 | HB1 | HB2 | SV | AT | SS |
|---|---|---|---|---|---|---|---|---|
| HL1 | 1.00 | |||||||
| HL2 | 0.82* | 1.00 | ||||||
| HL3 | 0.65* | 0.67* | 1.00 | |||||
| HB1 | 0.52* | 0.52* | 0.51* | 1.00 | ||||
| HB2 | 0.58* | 0.57* | 0.53* | 0.76* | 1.00 | |||
| SV | 0.37* | 0.39* | 0.36* | 0.46* | 0.34* | 1.00 | ||
| AT | 0.59* | 0.57* | 0.46* | 0.59* | 0.60* | 0.57* | 1.00 | |
| SS | 0.64* | 0.69* | 0.55* | 0.61* | 0.68 | 0.32* | 0.57 | 1.00 |
HL1, access to health information and services; HL2, examination of health information and services; HL3, decision-making in using herbal products for health care; HB1, behavior of using herbal products to promote health; HB2, behavior of using herbal products for disease treatment; SV, societal values toward the use of herbal products; AT, positive attitudes toward the use of herbal products; SS, perceived social support.
p<0.05.
The relationship estimated according to the study hypothesis demonstrated a relatively low goodness-of-fit for the model, which was developed based on the study’s conceptual framework (chi-square=162.74, df=20, chi-square/df=8.14, RMSEA=0.13, GFI=0.92, CFI=0.97, and NFI=0.97).
To achieve an acceptable GFI, the model was adjusted by correlating the errors of certain observed variables. Following this adjustment, the model’s fit was evaluated and found to be satisfactory. The GFI values were deemed acceptable (chi-square=13.46, df=10, chi-square/df=1.35, RMSEA=0.03, GFI=0.99, CFI=1.00, and NFI=1.00), as shown in Figure 1 and Table 3.
Figure. 1.
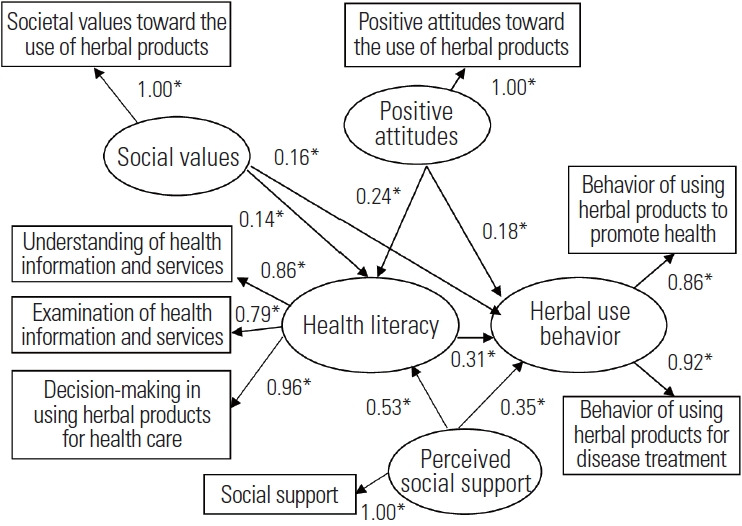
Structural equation modeling with standardized regression coefficients. *p<0.05.
Table 3.
Coefficient of influence (β) of the predictor variable on the outcome variable in the causal relationship model of herbal medicine use for health
| Variables | Health literacy (R2=0.58) |
Herbal health behavior (R2=0.68) |
||||
|---|---|---|---|---|---|---|
| DE | IE | TE | DE | IE | TE | |
| Health literacy | - | - | - | 0.31* | - | 0.31* |
| Societal values toward the use of herbal products | 0.14* | - | 0.14* | 0.16* | 0.04* | 0.20* |
| Positive attitudes toward herb use | 0.24* | - | 0.24* | 0.18* | 0.08* | 0.26* |
| Perceived social support | 0.53* | - | 0.53* | 0.35* | 0.16* | 0.51* |
| χ2=13.46, df=10, p-value=0.19, χ2/df=1.35, RMSEA=0.03, SRMR=0.01, GFI=0.99, CFI=1.00, NFI=1.00 | ||||||
DE, direct effect; IE, indirect effect; TE, total effect; df, degrees of freedom; RMSEA, root-mean squared error of approximation; SRMR, standardized root mean residual; GFI, goodness-of-fit index; CFI, comparative fit index; NFI, normed fit index.
p<0.05.
The variable that had the most substantial and direct impact on the behavior of using herbs for health was social support, with a path coefficient of 0.35 and a significance level of p-value <0.05. The study also explored the indirect effects of various variables on the use of herbs for health, finding significant influences from HL, Thai values, and positive attitudes toward Thai herbal products, with path coefficients of 0.31, 0.18, and 0.16, respectively (p<0.05). These factors together explained 68% of the variance in HL.
The most significant variable directly influencing HL was found to be social support (path coefficient=0.53; p<0.05). Thai values (path coefficient=0.24; p<0.05) and a positive attitude toward the use of Thai herbal products (path coefficient=0.14; p<0.05) also played influential roles. Together, these factors accounted for 58% of the variance in HL.
DISCUSSION
This study employed Bandura [16]’s concept and Mancuso [10]’s HL structure to investigate the factors influencing herb use. According to the results, the model fit the actual data quite well. HL indirectly affected herb use, whereas individual, contextual, and social/environmental variables had a direct impact.
Social support had the most significant direct impact, with individuals frequently seeking information about herbal medicines from family and friends. Users commonly trusted the perceived benefits of herb use, particularly when recommended by close acquaintances. This finding is consistent with that of Woradet et al. [27], who identified a positive relationship between social support and herb use. Additionally, social support indirectly influenced herb use through the HL of Thai herbs.
HL significantly influenced herb use, as individuals considered it a crucial factor in making decisions to enhance their health. This finding is consistent with prior studies that have shown the impact of HL on herb use. Khampang et al. [28] explained that HL, particularly the ability to acquire appropriate health-related information about herbal products, directly affects their use for health purposes. Similarly, Pitug et al. [29] discovered that adequate levels of HL, especially in terms of accessing and evaluating health information, can influence the consumption of herbal supplements.
Attitudes toward herb use significantly influenced herb use, with positive attitudes often leading to increased consumption of herbs for health purposes. The decision to use herbs and supplements is shaped by one’s attitudes and beliefs [30]. This observation aligns with the findings of Nguyen et al. [31], who noted that the perceived safety of herbal medicines, along with their fewer side effects compared to modern medicines, contributes to their increased use for health purposes. Thongruang [32] also reported that a broadly positive attitude toward herbal products tends to increase their use in healthcare settings. Additionally, the affordability of domestic herbs, which is attributed to cost-effective production methods, chemical-free ingredients, and a longstanding tradition of herb use passed down through generations, positively influences herb use [33].
Social values significantly influence herb use, as supported by Lasmono [34], who noted that cultural values profoundly shape health-related herb uses. Additionally, emerging social values can play a role in promoting Thai traditional medicines. Individuals frequently consider perceived social values an important factor in their decision-making processes, particularly when selecting herbs [35]. Thai social values foster a sense of identity, instilling beliefs, preferences, and emotions such as nostalgia and pride in being Thai. Consequently, this encourages the adoption of Thai herb use behaviors that are compatible with their lifestyle and readily accessible.
Social support has been identified as the most influential factor affecting HL, primarily because it facilitates the transfer of relevant health information and monitors behaviors and practices across various population groups. Research has shown that there is a direct and positive relationship between HL and social support. Pa-in et al. [36] also recognized social support as a situational determinant of HL, highlighting its critical role in the dissemination of appropriate health information. When higher levels of social support were provided, individuals demonstrated an enhanced ability to obtain and understand health information, and were more effectively able to utilize the healthcare system to their benefit [37].
The cross-sectional design of this study limits the causal inferences that can be drawn; therefore, future research should aim to validate these causal relationships. A more robust approach would involve conducting a longitudinal study and collecting data at multiple time points. The contributors were recruited from a health service center, which restricted the sample size and may not have adequately represented the broader population. In future studies, we plan to increase the sample size and recruit participants from a wider community.
In summary, this study established that HL correlates with social values, attitudes toward herb use, and social support, quantifying these relationships. Healthcare professionals and policymakers can use these findings to develop targeted and effective strategies that promote the use of herbal products, thereby improving healthcare outcomes. To improve their value and medical benefits, ensure public availability, and monitor health impacts, particularly in Nakhon Nayok or similar areas, the government should support the use of local economic plants as herbal medicine.
Acknowledgements
We extend our sincere appreciation to all individuals who contributed to this research.
Footnotes
Conflict of Interest
The authors have no conflicts of interest associated with the material presented in this paper.
Funding
Support for this study was provided by the Graduate School of Srinakharinwirot University.
Author Contributions
Conceptualization: Intarakamhang U, Prapasiri S, Prasittichok P. Data curation: Prasittichok P, Duangchan P. Formal analysis: Prasittichok P, Duangchan P. Funding acquisition: Prasittichok P. Methodology: Intarakamhang U, Prapasiri S, Prasittichok P. Project administration: Prasittichok P, Duangchan P. Writing – original draft: Intarakamhang U, Prapasiri S, Prasittichok P. Writing – review & editing: Duangchan P, Prasittichok P.
REFERENCES
- 1.Lee EL, Richards N, Harrison J, Barnes J. Prevalence of use of traditional, complementary and alternative medicine by the general population: a systematic review of national studies published from 2010 to 2019. Drug Saf. 2022;45(7):713–735. doi: 10.1007/s40264-022-01189-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kanjanahattakij N, Kwankhao P, Vathesatogkit P, Thongmung N, Gleebbua Y, Sritara P, et al. Herbal or traditional medicine consumption in a Thai worker population: pattern of use and therapeutic control in chronic diseases. BMC Complement Altern Med. 2019;19:258. doi: 10.1186/s12906-019-2652-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sam S. Importance and effectiveness of herbal medicines. J Pharmacogn Phytochem. 2019;8(2):354–357. [Google Scholar]
- 4.Mazrouei NA, Meslamani AZ, Alajeel R, Alghadban G, Ansari N, Kaabi MA, et al. The patterns of herbal medicine use in the United Arab Emirates; a national study. Pharm Pract (Granada) 2022;20(3):2698. doi: 10.18549/PharmPract.2022.3.2698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80. doi: 10.1186/1471-2458-12-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Intarakamhang U, Prasittichok P. Health literacy in dietary supplement use among working-age groups: systematic review and meta-analysis. Heliyon. 2022;8(8):e10320. doi: 10.1016/j.heliyon.2022.e10320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liu C, Wang D, Liu C, Jiang J, Wang X, Chen H, et al. What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam Med Community Health. 2020;8(2):e000351. doi: 10.1136/fmch-2020-000351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Khattiya S, Fongkerd S, Santayakorn P. Health literacy factors affecting herb use toward self-care among patients with chronic diseases who come to the services at Huai Koeng hospital, Udonthani province. UDRU Hum Social Sc J. 2021;10(1):127–144. (Thai) [Google Scholar]
- 9.Sørensen K, Levin-Zamir D, Duong TV, Okan O, Brasil VV, Nutbeam D. Building health literacy system capacity: a framework for health literate systems. Health Promot Int. 2021;36(Supplement_1):i13–i23. doi: 10.1093/heapro/daab153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mancuso JM. Health literacy: a concept/dimensional analysis. Nurs Health Sci. 2008;10(3):248–255. doi: 10.1111/j.1442-2018.2008.00394.x. [DOI] [PubMed] [Google Scholar]
- 11.Soltanipour S, Keihanian F, Saeidinia A. Knowledge, attitude and practice of physicians towards herbal remedies in Rasht, north of Iran. Medicine (Baltimore) 2022;101(47):e31762. doi: 10.1097/MD.0000000000031762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Agova N, Petrova G, Georgieva S, Kumanov I. Consumers attitudes toward the use of herbal medicines and herbal supplements in Northeastern Bulgaria. J IMAB. 2020;26(3):3278–84. doi: 10.5272/jimab.2020263.3278. [DOI] [Google Scholar]
- 13.Whyle E, Olivier J. Social values and health systems in health policy and systems research: a mixed-method systematic review and evidence map. Health Policy Plan. 2020;35(6):735–751. doi: 10.1093/heapol/czaa038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Purwoko P, Wijaya T. Consumer value and lifestyle as a predictor of herbal medicine purchase intention in Surakarta-Indonesia. Glob J Health Sci. 2019;11(4):69. doi: 10.5539/gjhs.v11n4p69. [DOI] [Google Scholar]
- 15.Guo A, Jin H, Mao J, Zhu W, Zhou Y, Ge X, et al. Impact of health literacy and social support on medication adherence in patients with hypertension: a cross-sectional community-based study. BMC Cardiovasc Disord. 2023;23(1):93. doi: 10.1186/s12872-023-03117-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bandura A. Social foundation of thought and action: a social cognitive theory. Upper Saddle River: Prentice Hall; 1986. p. 24. [Google Scholar]
- 17.Ekor M. The growing use of herbal medicines: issues relating to adverse reactions and challenges in monitoring safety. Front Pharmacol. 2014;4:177. doi: 10.3389/fphar.2013.00177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jackson DL. Sample size and the number of parameter estimates in maximum likelihood confirmatory factor analysis: a Monte Carlo investigation. Struct Equ Modeling. 2001;8:205–223. doi: 10.1207/S15328007SEM0802_3. [DOI] [Google Scholar]
- 19.Kim GS. AMOS 18.0 structural equation model analysis. Seoul: Hannarae Academy. 2013. (Korean)
- 20.Ruangsongkram S, Promsorn T. Factors related to the behavior of using herb for self-care of people in Prachinburi Province in the pandemic situation of coronavirus disease 2019. Thai J Public Health Health Sci. 2023;6(1):99–113. (Thai) [Google Scholar]
- 21.Intarakamhang U, Khammungkul J, Boocha P. General health literacy scale for Thais and comparison between age groups. Heliyon. 2022;8(5):e09462. doi: 10.1016/j.heliyon.2022.e09462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52:30–41. doi: 10.1207/s15327752jpa5201_2. [DOI] [PubMed] [Google Scholar]
- 23.Chartprasert DK, Deedenkeeratisakul K. Domestic customers’ perceived value toward Thai cultural products. J Manag Sci Chiangrai Rajabhat Univ. 2022;17(2):31–58. (Thai) [Google Scholar]
- 24.Udompitayson J. Use of herbs for medical purposes: attitudes and behaviors of local people in Ban Nai Lum, Kantang District, Trang Province. J Lib Arts. 2020;1(1):1–7. (Thai) [Google Scholar]
- 25.Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- 26.Kumari SS. Multicollinearity: estimation and elimination. J Contemp Res Manage. 2008;3(1):87–95. [Google Scholar]
- 27.Woradet S, Chaimay B, Salaea R, Kongme Y. Factors associated with herbal used behavior toward self-care among village health volunteers in Krung La district, Phatthalung Province. J Health Sci. 2015;24(1):50–59. (Thai) [Google Scholar]
- 28.Khampang R, Kloyiam S, Butchon R. Relationship between socioeconomic, demographic, health and social characteristics and ability to access reliable information on herbal and food supplements: analysis of Thai Health Literacy Survey 2019. BMC Public Health. 2022;22(1):1054. doi: 10.1186/s12889-022-13454-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pitug W, Laohasiriwong W, Senahad N, Soeung KP. Health literacy and dietary supplement consumption among northeasterners of Thailand. Indian J Public Health Res Dev. 2020;11(7):1482–7. doi: 10.37506/ijphrd.v11i7.10305. [DOI] [Google Scholar]
- 30.Soltani A, Jaam M, Nazar Z, Stewart D, Shaito A. Attitudes and beliefs regarding the use of herbs and supplementary medications with COVID-19: a systematic review. Res Social Adm Pharm. 2023;19(3):343–355. doi: 10.1016/j.sapharm.2022.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Nguyen PH, Tran V, Pham DT, Dao TN, Dewey RS. Use of and attitudes towards herbal medicine during the COVID-19 pandemic: a cross-sectional study in Vietnam. Eur J Integr Med. 2021;44:101328. doi: 10.1016/j.eujim.2021.101328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Thongruang C. Consumer purchasing behavior for herbal medicine in drugstore in Bangkok. Naresuan Univ J. 2013;16(3):195–202. [Google Scholar]
- 33.Logiel A, Jørs E, Akugizibwe P, Ahnfeldt-Mollerup P. Prevalence and socio-economic factors affecting the use of traditional medicine among adults of Katikekile Subcounty, Moroto District, Uganda. Afr Health Sci. 2021;21(3):1410–1417. doi: 10.4314/ahs.v21i3.52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lasmono SL. Phenomenological research on the values systems of the Indonesian traditional herb consumer. Int J Res Innov Soc Sci. 2022;6(7):126–132. [Google Scholar]
- 35.Tam YA. Profiling herbal medicine use by transtheoretical model and perceived value: a case study of young adults in Malaysia. Int J Account. 2021;6(37):48–63. [Google Scholar]
- 36.Pa-in P, Wonghongkul T, Khampolsiri T, Chintanawat R. Causal model of health literacy in Thai older adults with knee osteoarthritis. Pac Rim Int J Nurs Res. 2023;27(2):303–316. doi: 10.60099/prijnr.2023.262040. [DOI] [Google Scholar]
- 37.Chen WL, Zhang CG, Cui ZY, Wang JY, Zhao J, Wang JW, et al. The impact of social capital on physical activity and nutrition in China: the mediating effect of health literacy. BMC Public Health. 2019;19(1):1713. doi: 10.1186/s12889-019-8037-x. [DOI] [PMC free article] [PubMed] [Google Scholar]