

Abstract
Background and Aims
The preference of beauty seekers for noninvasive, convenient, and long‐lasting effective facial cosmetic techniques with minimal downtime and recovery time is obvious nowadays. As a part of traditional Chinese medicine, acupuncture has great advantages in solving these problems. This study aims to assess the effectiveness of two distinct acupuncture techniques for facial rejuvenation in treating nasolabial folds (NFs) and marionette lines (MLs).
Methods
One hundred beauty seekers who have received facial acupuncture cosmetic treatment in hospitals between June 1, 2020, and December 31, 2022, were selected randomly and inquired. Among them, 50 beauty seekers (Group Ⅰ) have received a normal facial traditional Chinese medicine acupuncture therapy, by inserting the needles perpendicularly into the acupoints. Meanwhile, another 50 beauty seekers (Group Ⅱ) were treated by needle knives, which were inserted parallelly under the dermis and basically along the meridians of Chinese medicine linked by the acupoints. The records of pain evaluation and adverse events on cases, subjective satisfactions, and objective evaluations of efficacy were summarized and statistically analyzed.
Results
The efficacy of Group Ⅱ is better than Group Ⅰ. The dermatologists' assessments for NF and ML show significant differences between Groups Ⅰ and Ⅱ after one course. The mean value of subjective satisfaction also obeys the rules above. Although Group Ⅱ exhibited the highest value of mean pain intensity, the adverse events were basically mild. Furthermore, Group Ⅱ showed higher willingness for additional treatments.
Conclusion
Only in terms of the wrinkle depth of NF and ML, the method of acupuncturing parallelly under the dermis by needle knife is safe and more successful.
Keywords: acupuncture, facial cosmetic, marionette lines, nasolabial folds, needle knife
1. INTRODUCTION
As aging occurs, our skin shows many changes. Due to the loss of elasticity resulting from the gradual decrease in moisture, lipids, skin collagen, and elastic fibers over time, the skin becomes saggy. 1 In addition, due to bone remodeling and deflation of fat pads, there is also a loss of volume in all layers of the anatomical facial structures. 2 , 3 The aforementioned processes start in the latter half of the second or third decade of life. When skin, fatty tissue, and facial muscles can no longer stay in the proper position, pigmentation, and wrinkles occur. Therefore, wrinkles are one of the most visible signs of physical aging. 4 Then, if wrinkles can be relieved greatly or removed, it is an important manifestation of facial rejuvenation. In addition, there is a growing trend among patients to look for natural effects that will help them relieve their anxiety when returning to social and professional life immediately. 5 For many side effects of plastic surgery which have been proven, 6 the choice of treatment for facial rejuvenation is also gradually developing and evolving from surgical treatment to minimally invasive technology. 7
Acupuncture has become more and more popular in recent years among people planning to improve their facial appearance. 8 , 9 , 10 Nevertheless, the methodology of acupuncture studies needs to be updated more rigorously (including the use of randomized, sham‐controlled trials with standardized interventions). 11 When referring to different applications of acupuncture, such as “facial revitalization acupuncture,” 12 “face‐lifting acupuncture,” 12 “thread embedding acupuncture,” 5 and so on, modern anatomy and physiology, combined with the theory of traditional Chinese medicine meridian, will be used simultaneously. When using Chinese medicine theories in cosmetic acupuncture, acupuncturists usually determine whether the skin laxity is caused by spleen and liver dysfunction based on patients' main complaints and symptoms, and carry out systemic treatment on the corresponding meridians as well as local areas experiencing sagging. 13 As for western medicine theories, cosmetic acupuncture is mainly guided by the principle of wound healing. It can be explained as that after being pierced into microscopic holes, the damaged skin during self‐healing will secrete growth factors to boost the quantity of collagen fibers and hyaluronic acid. Compared to a device called “Derma roller” equipped with multiple needles, 14 penetrations based on acupoints cause minimal trauma and inflammatory responses such as pain, bleeding, redness, and swelling, thereby alleviating the patient's burden. 13
In this paper, we give priority to and focus on the treatment effect of the cases of nasolabial folds (NFs) and marionette lines (ML), from the perspective of privacy protection and the degree of difficulty. Then, we aim to present and share two different acupuncture therapies in our hospital, and to discuss their efficacy. Since we have not used the facial contour measurement tool 15 or software 16 before, the assessment of the study's objectives need a comprehensive methodology, which includes beauty seekers' questionnaires and the rating of standardized processed pictures. Through this study, we hope to provide more ideas or choices for improving the efficacy and safety of facial rejuvenation with oriental characteristics.
2. METHODS
2.1. Study objective
Normally, NFs and MLs belong to the facial wrinkles around the mouth. The objective in this study was conducted to determine the efficacy on NF and ML of different acupuncture techniques based on the diverse concepts of cosmetic acupuncture.
2.2. Ethics approval and inclusion/exclusion criteria
We retrieved the list of clinic patients from medical cosmetology department in hospital, who had received facial acupuncture beauty treatments during hospital admissions for a period of 30 months (between June 2020 and December 2022). The eligible cases according to the criteria below were selected and collected a total number of 100 cases were collected. The cases belong to two groups using different acupuncture therapies in a ratio of 1:1. Each group includes 47 females and three males, whose age ranged from 35 to 70 years old.
Inclusion criteria are that the beauty seekers have not received any other plastic surgery or treatment affecting facial wrinkles or skin quality during one treatment course.
Exclusion criteria: (1) any existence of maxillofacial infections and tumors, facial trauma, and congenital facial deformity, which would affect the efficacy assessment; (2) body mass index (BMI) ≤ 18 or BMI ≥ 28 kg/m2, recorded during one treatment course; (3) any existence of metabolic diseases—diabetes included; (4) has not retained the imaging data in related with the treatment effects.
The study was performed under the guidelines and principles of the ethical standards set forth in the revised version of the Helsinki Declaration. The corresponding medical ethics committee approved this study. Furthermore, all individuals in the selected cases have signed the informed consent, which was also obtained before this study. All individuals in the selected cases have agreed to publish the results in academic papers.
2.3. Study design
The data used in all 100 cases came from the first one course in our hospital, which includes three sessions. The interval between two successive sessions is half a month. Usually, we will avoid the location of superficial arteries and veins when conduct superficial acupuncture in the nonacupoints area as far as possible. The disinfectant before and after treatment is iodophor. For Group Ⅰ, we selected the acupoints according to classical Chinese medicine acupuncture theory, and most beauty seekers who received this therapy mainly wanted facial maintenance, or physical and mental relaxation. As for Group Ⅱ, the acupoints act as anatomical marks of insertion to give mechanical acupuncture stimulation to the facial skin, not completely in relation to classical Chinese medicine acupuncture theory. The beauty seekers would receive this therapy, mainly because of appearance anxiety.
Group Ⅰ: Perform penetration by acupuncture needle (specification: 0.40 mm × 40 mm, as shown in Figure 1). The acupoints are divided into one route and one area, which aim to improve face sagging and face lift. 13 , 17 The area contains GB1‐Tóngzǐliáo, GB2‐Tīnghuì, GB14‐Yángbái, GB15‐Tóulínqì, EX‐HN4‐Yúyāo, EX‐HN5‐Tàiyáng, TE23‐Sīzhúkōng, and SI18‐Quánliáo. The route goes through ST2‐Sìbái, ST3‐Jùliáo, ST4‐Dìcāng, CV24‐Chéngjiāng, ST5‐Dàyíng, ST6‐Jiáchē, ST7‐Xiàguān, and ST8‐Tóuwéi. The inserting angle is basically normal to skin layer. The penetration depth is various and adjusted according to each acupoint. The specific technique is roughly illustrated in Figure 2A. In addition, the duration is half an hour.
Figure 1.
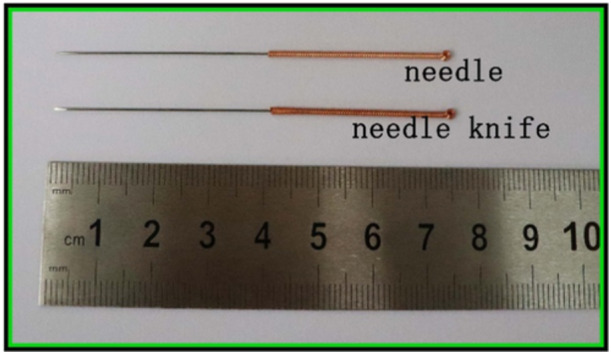
The specifications of the needle and the needle knife.
Figure 2.
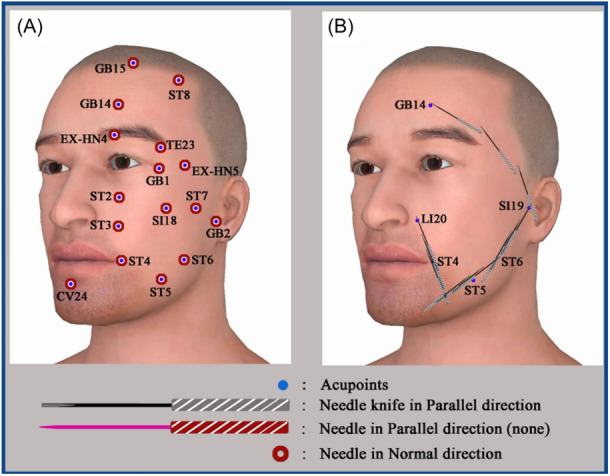
Acupuncture technique diagrams for different groups: (A) Ⅰ and (B) Ⅱ.
Group Ⅱ: This is the most commonly used and effective method in our hospital in the past 5 years, which performing penetration by needle knife (specification: 0.40 mm × 40 mm, as shown in Figure 1), along four line segments connecting two acupoints. The starting and ending acupoints of the four line segments are: ST4‐Dìcāng to LI20‐Yíngxiāng; ST5‐Dàyíng to ST6‐Jiáchē; ST6‐Jiáchē to SI19‐Tīnggōng; SI19‐Tīnggōng to GB14‐Yángbái; separately. Three successive needle knives were injected parallelly with the skin layer to the dermis at a depth of 1–2 mm. Each insertion position with the corresponding insertion angle between line segment and needle knife is illustrated in Figure 2B. The penetration distance for all needle knives is all into the skin. The duration of acupuncture is half an hour.
2.4. Efficacy assessments
2.4.1. Satisfaction with facial appearance
The records of telephone interviews with all individuals in the cases for satisfaction with the treatment, 3, 6, and 9 months after last treatment session, were used. The satisfaction with the total effect were recorded separately using a 5‐point Likert scale as shown in Table 1, with 5 being defined as very satisfied, 4 as somewhat satisfied, 3 as neither satisfied nor dissatisfied, 2 as somewhat dissatisfied, and 1 as very dissatisfied.
Table 1.
The satisfaction scales on the check sheet.
| Very dissatisfied | Somewhat dissatisfied | Neither satisfied nor dissatisfied | Somewhat satisfied | Very satisfied |
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 |
2.4.2. Pain rating scale
The overall pain experience for each case has been recorded using a visual analogue scale (VAS) questionnaire, immediately after the completion of three successive courses. The pain degree in a VAS questionnaire can be graded as 0 (no pain) to 10 (unbearable sharp pain).
2.4.3. Evaluation of geometric features of wrinkles
For the selected cases, standardized photographs have been taken at 0° using a digital camera (Canon EOS 200D‐, the equipment only for the medical cosmetology department in the hospital) during the treatment. Normally, the camera with a fixed focal distance was set at 1 meter away from the participant. The center of the camera was aligned with the center of the participant's face, and the Frankfurt plane was used as the horizontal plane. From the principle of double‐blind design, all participants in both Groups Ⅰ and Ⅱ should be randomly numbered and anonymously processed. Additionally, other characteristic parts of the face in their photographs, of before the beginning of the first session and immediately after the end of the last treatment session, were covered. Then, these photographs were given via us to another three specialized dermatologists from the department of dermatology in the hospital for the assessment of the quality of the wrinkles according to Merz esthetic scale. 18 Each scale value of FL and ML at a certain time node for each participant was the average of three dermatologists' assessments.
2.4.4. Adverse events
The records of adverse events in the period between the start of the first session and 3 months after the end of the last session mainly include bruises, engorgement, and fainting during acupuncture.
2.4.5. Statistical analysis
A mathematician from another institution performed the data analysis using SPSS 22.0 statistical software. The measurement data subject to normal distribution or approximate normal distribution were expressed as mean ± standard deviation (SD). For intragroup comparison, paired sample t test was used. Independent sample t test was used for comparison between Groups Ⅰ and Ⅱ. Thetwo‐side value of p < 0.05 was defined as the threshold for tests to be considered statistically significant, and exact p values were shown unless p < 0.001.
3. RESULTS
In particular, Figure 3 shows some representative photographs of the participants of different ages before the first session and after the last session in Group II. All other characteristics in Figure 3 that can expose the participant's identity are avoided as much as possible to ensure that only the specific biological characteristics displayed. In general, NF and ML were improved after treatment in Group II; in different individuals, the degree of improvement of different wrinkles was not always synchronized, because the initial condition of the individual physique and wrinkles before treatment was also different.
Figure 3.
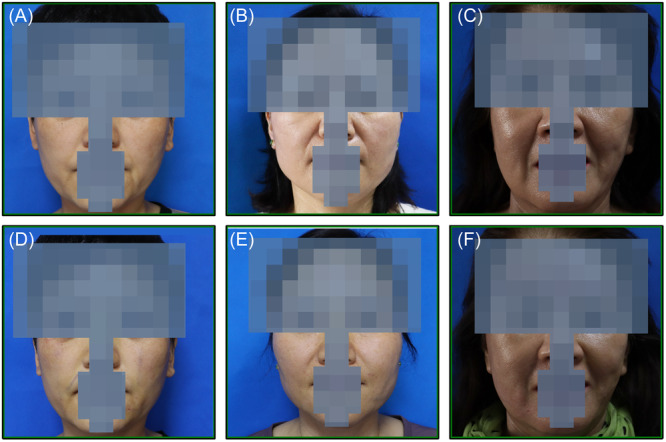
A 42‐year‐old woman in Group Ⅱ, (A) before treatment and (B) after the last session; a 51‐year‐old woman in Group Ⅱ, (C) before treatment and (D) after the last session; a 66‐year‐old woman in Group Ⅱ, (E) before treatment; and (F) after last session.
3.1. Subject satisfaction
The satisfaction and the likelihood to return for additional treatment of all participants were recorded in Table 2. The satisfaction score for Group Ⅱ was 4.58 ± 0.61, 3 months after last treatment session, which is obviously higher than Group Ⅰ (2.98 ± 0.59). Thus, there existed a high‐level significant difference between Group Ⅱ and Group Ⅰ (t = −13.356, p = 0.000 < 0.01). The high‐level significant difference was also kept, also 6 months after last treatment session (t = −12.241, p = 0.000) and 9 months after last treatment session (t = −14.571, p = 0.000). On the other hand, the satisfactions with the overall treatment effect of facial wrinkles, decreased more slowly over time after the last session in Group Ⅱ than in Group Ⅰ. The willingness of additional repeat treatments of Group Ⅱ, 9 months after last session, was also high (88%).
Table 2.
Independent sample t test for satisfaction questionnaire, with likelihood of returning for additional repeat treatments.
| Group (mean ± SD) | t | p | ||
|---|---|---|---|---|
| Ⅰ (n = 50) | Ⅱ (n = 50) | |||
| 3 months after | 2.98 ± 0.59 | 4.58 ± 0.61 | −13.356 | 0.000 |
| 6 months after | 2.48 ± 0.76 | 4.32 ± 0.74 | −12.241 | 0.000 |
| 9 months after | 2.28 ± 0.61 | 4.28 ± 0.76 | −14.571 | 0.000 |
| Likelihood to return after 9 months | 32% | 88% | ‐ | ‐ |
3.2. Pain assessment
On the day of the end of the first treatment session for each participant, the pain intensity was recorded and the results of the summary are listed in Table 3. Although, the average pain score in Group Ⅱ (3.80 ± 0.83) is obviously higher than Group Ⅰ (2.24 ± 0.89), which only belong to mild pain where pain score is 4. It means the pain in Group Ⅱ is also basically tolerable.
Table 3.
Independent sample t test for questionnaire of the pain during the treatment.
| Group (mean ± SD) | t | p | ||
|---|---|---|---|---|
| Ⅰ (n = 50) | Ⅱ (n = 50) | |||
| Pain score | 2.24 ± 0.89 | 3.80 ± 0.83 | 9.030 | 0.000 |
3.3. Objective assessment by dermatologist
The dermatologists' assessments before and after the whole treatment are summarized in Table 4. Before the beginning of the treatment, neither NF nor ML, has shown significant difference between Groups Ⅱ and Ⅰ for Merz esthetic score at rest. As for the dermatologists' assessments of response to the whole course, both NF (t = 3.069, p = 0.003 < 0.01) and ML (t = 2.115, p = 0.037 < 0.05) have shown significant differences between Groups Ⅱ and Ⅰ. When using the paired t test to study the difference of the assessments before and after the whole treatment with each group in Table 5, only NF (t = 3.072, p = 0.003 < 0.01) and ML (t = 2.147, p = 0.037 < 0.05) in Group Ⅱ have shown significant difference.
Table 4.
Merz aesthetic scores of wrinkles at rest (0–4) before the first session and after the last session, separately, with the independent t test between groups.
| Mean ± SD (before) | t | p | Mean ± SD (after) | t | p | |||
|---|---|---|---|---|---|---|---|---|
| Ⅰ (n = 50) | Ⅱ (n = 50) | Ⅰ (n = 50) | Ⅱ (n = 50) | |||||
| NF | 2.52 ± 0.81 | 2.24 ± 0.89 | 1.638 | 0.105 | 2.30 ± 0.99 | 1.62 ± 1.21 | 3.069 | 0.003 |
| ML | 2.40 ± 0.81 | 2.22 ± 1.07 | 0.947 | 0.346 | 2.22 ± 1.11 | 1.74 ± 1.16 | 2.115 | 0.037 |
Abbreviations: ML, marionette line; NF, nasolabial fold.
Table 5.
Paired t test for Merz aesthetic assessments in Table 4.
| Difference (Ⅰ) (before–after) | t | p | Difference (Ⅱ) (before–after) | t | p | |
|---|---|---|---|---|---|---|
| NF | 0.22 | 1.562 | 0.125 | 0.62 | 3.072 | 0.003 |
| ML | 0.18 | 1.000 | 0.322 | 0.48 | 2.147 | 0.037 |
Abbreviations: ML, marionette line; NF, nasolabial fold.
3.4. Adverse events and safety assessment
No serious adverse events or infections were reported at any of time points. For Group Ⅱ, most adverse events were recorded as mild to moderate ecchymosis (one moderate cases [3.4%] and seven mild cases [24.1%]). There was no case of ecchymosis for Group Ⅰ. Furthermore, the ecchymosis symptom of all cases would be resolved without intervention within 1 month. No nodules, granulomas, or other complications (edema and hematomas) were reported. Both Groups Ⅱ and Ⅰ were considered safe.
4. DISCUSSION AND CONCLUSION
The purpose of this experiment is to verify the effectiveness of Chinese acupuncture and the better choice of particular acupuncture method. Combining the subject satisfaction and objective assessment of wrinkles, the efficacy of Group Ⅱ is indeed more significant and long lasting. The procedure was also well tolerated by beauty seekers in Group Ⅱ. Furthermore, the downtime is minimal, since the duration of one session is just half an hour and there is no postprocedure loss of workdays.
The mechanisms of Group Ⅰ consist increasing or balancing “Qi” (considered by ancient Chinese as the energy moving in the Zang‐Fu organs and meridians), 9 , 19 increasing blood flow by inserting needles at certain acupoints, 9 , 20 stimulate secretion of collagen/elastin, 16 stimulate the production of endogenous opioids, 20 , 21 and decreasing facial muscle tone. 10 The needles in Group Ⅰ are inserted perpendicularly or a little obliquely with the tip toward the side of the head to a depth of approximately 0.5–10 mm according to different acupoints. Thus, in terms of muscle tone, Group Ⅰ involves both mimetic muscles, masticatory muscles, and the superficial musculoaponcurotic system (SMAS), in addition to the epidermis and dermis. From the viewpoint of the anatomical structure of the face, poor facial blood circulatory metabolism induced by wrinkles, and the chronic injury of facial muscles usually form a vicious circle. Due to the excessive pursuit of comprehensive treatment and the lack of treatment focus probably, the effect of Group Ⅰ seems too slow to alleviate wrinkles.
As for Group Ⅱ, the main mechanism should be closely related to SMAS under the dermis at a depth of 1–2 mm. As the independent tissue layer under facial subcutaneous fat, the SMAS fascia network connects facial mimetic muscles and transfers the contraction of some mimetic muscles to other ones to produce complex expressions. 22 , 23 The horizontal needle knife insertion along the segment between ST4‐Dìcāng and LI20‐Yíngxiāng is mainly to relax SMAS fascia connecting levator labii superioris alar muscles, levator labii superioris muscles, levator angularis muscles, zygomaticus minor muscle, and zygomaticus major muscle. Normally, the shortening of these radially arranged mimetic muscles around orbicularis oris muscle causes NFs and MLs. The rest three segments mainly focus on the improvement of skin sagging and face lift by helping the redistribution of SMAS tension. Besides, the use of needle knife, rather than ordinary needles, should also contribute to tissue regeneration.
There were also some limitations in this study. First, the retrospective nonrandomized design in this study is a key limitation. Since the therapeutic options of the cases depend on the treatment concept or the technical level of a specific acupuncturist, it may impact the findings through potential sample differences before the study between Groups Ⅰ and Ⅱ. Second, the acupuncturists need to use a variety of needles, be familiar with facial acupoints and anatomical stratification of facial muscles, simultaneously, which limit the promotion of technology in community hospitals. The acupuncturists involved in this study are clinicians with more than 5 years of work experience. Most traditional Chinese medicine clinicians in hospital can conduct the therapy by acupuncture needles easily in Group Ⅰ; however, when comes to the therapy by needle knife in Group Ⅱ, the clinicians should be proficient in anatomy operation skills, additionally. Third, we have not estimated the sample size.
Above all, the method that acupuncture under the dermis in parallel direction with the skin layer by needle knife is feasible and more effective on facial wrinkle removal, by releasing SMAS along meridian channels or connecting lines between acupoints. It meets the preference of beauty seekers for noninvasive, short‐recovery‐time procedures. Furthermore, there seems to exist a high degree of commonality between the diagnostic/therapeutic of modern myofascial trigger point and traditional Chinese medicine meridian theory. This treatment can propose a more convenient option and provide optimal ideas that imbibing and integrating various knowledge. Thus, a prospective randomized study in future is necessary to enhance our findings rigorously. Since this study only focused on the treatment of NF and ML currently, Our clinical team will continue to investigate the efficacy of the facial rejuvenation acupuncture method on the treatment of other facial wrinkles, such as horizontal forehead lines, glabellar lines, fishtail wrinkles, infraorbital hollow, and lip wrinkles. We will also continue to explore more principles and technical improvements for facial beauty, in addition to wrinkles.
AUTHOR CONTRIBUTIONS
Haowen Cheng: Investigation; writing—original draft; resources; conceptualization. Liangyu Xie: Writing—review and editing; methodology; validation. Tao Wang: Visualization; data curation; software; formal analysis. Bin Shi: Project administration; supervision; funding acquisition. The final version of this work has been read and approved by all authors. With full access to all of the study's data, Bin Shi assumes full accountability for the accuracy of the data analysis and the data's integrity.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
TRANSPARENCY STATEMENT
The lead author Bin Shi affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
ACKNOWLEDGMENTS
The collection, analysis, and interpretation of data; writing of the manuscript; and the publication fee of the manuscript, are supported by Key R&D Program of Shandong Province, China (No. 2022CXGC020510).
Cheng H, Xie L, Wang T, Shi B. Effectiveness of acupuncture therapy on improvement of nasolabial folds and marionette lines: a retrospective study. Health Sci Rep. 2024;7:e70014. 10.1002/hsr2.70014
DATA AVAILABILITY STATEMENT
Data is available on request from the authors.
REFERENCES
- 1. Gilbert E, Hui A, Waldorf HA. The basic science of dermal fillers: past and present part I: background and mechanisms of action. J Drugs Dermatol. 2012;11(9):1059‐1068. [PubMed] [Google Scholar]
- 2. Wan D, Amirlak B, Rohrich R, Davis K. The clinical importance of the fat compartments in midfacial aging. Plast Reconstr Surg Glob Open. 2013;1(9):e92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mendelson B, Wong CH. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic Plast Surg. 2012;36(4):753‐760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Yaar M, Eller MS, Gilchrest BA. Fifty years of skin aging. J Investig Dermatol Symp Proc. 2002;7(1):51‐58. [DOI] [PubMed] [Google Scholar]
- 5. Yun Y, Choi I. Effect of thread embedding acupuncture for facial wrinkles and laxity: a single‐arm, prospective, open‐label study. Integr Med Res. 2017;6(4):418‐426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bock JJ. A review of recent studies on cosmetic acupuncture. J Orient Obstet Gynecol. 2010;23(4):146‐154. [Google Scholar]
- 7. Ruan QZ, Chen AD, Tran BNN, et al. Integrative medicine in plastic surgery A systematic review of our literature. Ann Plast Surg. 2019;82(4):459‐468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Donoyama N, Kojima A, Suoh S, Ohkoshi N. Cosmetic acupuncture to enhance facial skin appearance: a preliminary study. Acupunct Med. 2012;30(2):152‐153. [DOI] [PubMed] [Google Scholar]
- 9. Doran VC. An introduction to facial revitalisation acupuncture. Eur J Orient Med. 2007;5:4‐8. [Google Scholar]
- 10. Lee KM, Lim SC, Kim JS, et al. A clinical study on facial wrinkles treated with miso facial acupuncture—measured by the facial skin photographing system. J Acupunct Res. 2010;27(1):101‐107. [Google Scholar]
- 11. Shin BC, Lim KT. Acupuncture for cosmetic use: a systematic review of prospective studies. Journal of Cosmetic Medicine. 2018;2(2):76‐84. [Google Scholar]
- 12. Kuge H, Mori H, Tanaka TH, Tsuji R. Reliability and validity of facial check sheet (FCS): checklist for self‐satisfaction with cosmetic acupuncture. Medicines. 2021;8(4):18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Orihashia K, Mitsunaga H, Kawai M, Kitagawa H, Zhou A, Tan Y. An overview of Japanese cosmetic acupuncture. World J Acupunct‐Mox. 2022;32(1):85‐88. [Google Scholar]
- 14. Tanaka I. About ICCO facial cosmetic acupuncture based on wound healing mechanism. Jpn J Acupunct Man Ther. 2019;178(2):72‐76. [Google Scholar]
- 15. Ahn S, Kim S, Lee H, Moon S, Chang I. Correlation between a cutometer and quantitative evaluation using Moire topography in age‐related skin elasticity. Skin Res Technol. 2007;13(3):280‐284. [DOI] [PubMed] [Google Scholar]
- 16. Cho JH, Lee HJ, Chung KJ, Park BC, Chang MS, Park SK. Effects of Jae‐Seng acupuncture treatment on the improvement of nasolabial folds and eye wrinkles. Evid Based Complement Alternat Med. 2015;2015:273909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Orihashi K, Mitsunaga H, Okamoto M, et al. Risk management of cosmetic acupuncture. World J Acupunct‐Mox. 2020;30(4):300‐303. [Google Scholar]
- 18. Alam M, Walter AJ, Geisler A, et al. Association of facial exercise with the appearance of aging. JAMA Dermatol. 2018;154(3):365‐367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Barrett J. Acupuncture and facial rejuvenation. Aesthet Surg J. 2005;25(4):419‐424. [DOI] [PubMed] [Google Scholar]
- 20. Chon TYandLee MC. Acupuncture. Mayo Clin Proc. 2013;88(10):1141‐1146. [DOI] [PubMed] [Google Scholar]
- 21. Eriksson SV, Lundeberg T, Lundeberg S. Interaction of diazepam and naloxone on acupuncture induced pain relief. Am J Chin Med. 1991;19(1):1‐7. [DOI] [PubMed] [Google Scholar]
- 22. Sykes JM, Riedler KL, Cotofana S, Palhazi P. Superficial and deep facial anatomy and its implications for rhytidectomy. Facial Plast Surg Clin North Am. 2020;28(3):243‐251. [DOI] [PubMed] [Google Scholar]
- 23. Gordon NA, Tower JI, Paskhover B. From the deep‐plane rhytidectomy to the vertical platysma advancement. Facial Plast Surg Clin North Am. 2020;28(3):311‐330. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data is available on request from the authors.