

Abstract
Background
Stage III lung cancer (LC) represents a heterogeneous group of diseases, and the optimal management is still a matter of debate. To date, only a few studies have assessed the role of multidisciplinary team (MDT) discussion in impacting survival of stage III LC. Hence, we aimed to reported the impact of the implementation of MDT discussion on long-term survival of stage III LC patients.
Methods
This is a retrospective, observational, single-centre cohort study evaluating data of consecutive patients with a clinical and pathological diagnosis of stage III LC treated before [2005–2011] and after [2012–2020] the implementation of MDT. The primary outcome was 5-year overall survival (OS).
Results
A total of 983 patients were enrolled with stage III LC, 411 (41.8%) pre-MDT and 572 (58.2%) post-MDT. The 5-year OS rates were 25.3% for the pre-MDT cohort and 33.9% for the post-MDT cohort (P=0.0008). Resected patients (n=670), who underwent trimodality therapy achieved a higher 5-year OS in both pre-MDT and post-MDT groups. An increased 5-year OS was observed in patients who underwent systemic therapy, from 28.2% in pre-MDT to 40.2% in post-MDT cohorts. In non-resected patients, there was an increased in 5-year OS in both systemic and chemoradiotherapy groups.
Conclusions
The implementation of an MDT increased the 5-year OS in both resected and non-resected stage III LC patients. Implementing MDT might be useful in improving the management of therapy with less invasive local and surgical strategies personalized for each LC patient.
Keywords: Stage III lung cancer (stage III LC), multidisciplinary team (MDT), trimodality therapy, systemic therapy
Highlight box.
Key findings
• The results showed that patients admitted post-multidisciplinary team (MDT) exhibited a better 5-year overall survival (OS) rates and also an improvement in the treatment management.
What is known and what is new?
• Limited studies have assessed the impact of MDT on outcomes of stage III lung cancer (LC), demonstrating an improvement in survival rates.
• This study showed that stage III LC patients’ prognosis has improved due to recent advancements in treatment strategies, especially systemic therapy, and their better integration within MDT.
What is the implication, and what should change now?
• The implication of the finding MDT improve OS rates for stage III LC patients is significant. It suggests that healthcare systems should prioritize the establishment and utilization of MDT in the treatment of this disease.
Introduction
Despite a significant decreases in mortality rates over the last decade, lung cancer (LC) still stands as the primary cause of cancer-related fatalities in the United States and Europe (1). Although strict guidelines suggest clearly the correct management of early and advanced stage LC, the optimal management of stage III is an ongoing source of debate. Stage III LCs are characterized by a high level of heterogeneity due various type of disease presentation (2). Hence, there is not a gold-standard management of stage III disease, with various treatment modalities proposed in the last 20 years.
The advent of targeted therapies (TT), immunotherapies (IT), and combination strategies provide significant advantages in the metastatic setting, but also in early and locally advanced LC. The high level of heterogeneity in stage III LC represent the main barrier in identify a single treatment pathway. In fact, despite these advances, the prognosis for patients with stage III LC remains poor, with a long-term survival rate ranging from 36–41% for stage IIIA patients, 24–26% in stage IIIB and 12–13% in stage IIIC (3-5).
The optimal management of stage III LC requires extensive knowledge of various therapeutic strategies, including surgery, systemic treatment, and radiotherapy (RT). Additionally, adopting discordant results promotes the adoption of neo-adjuvant (nadj) and adjuvant (adj) therapies in this setting.
Therefore, the introduction of a multidisciplinary team (MDT) decision path would integrate various expertise, perspectives, and methodologies to tackle this challenging disease. MDT allows for a holistic understanding of the disease and promotes more effective diagnostic and therapeutic approaches. To date, only a few studies have assessed the impact of MDT on outcomes of stage III LC, demonstrating an improvement in survival rates (6-10).
In the present paper, we conducted a real-world study at a high-volume centre in Italy with the aim of assessing the effectiveness of implement MDT discussion and its impact on long-term survival in stage III LC patients. We present this article in accordance with the STROBE reporting checklist (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-508/rc).
Methods
Study design and population
This is a retrospective, observational, single-centre cohort study collecting data of consecutive stage III LC patients admitted at the Fondazione IRCCS Istituto Nazionale dei Tumori di Milano (Milan, Italy) between January 01, 2005 to December 31, 2020.
All patients with stage IIIA/IIIB/IIIC LC were included. The 8th TNM (tumour nodes metastasis) edition and the American Joint Committee on Cancer was used for staging purpose (11). All patients diagnosed prior to 2017 were reclassified according to the 8th edition. Patients with a histological diagnosis of carcinoid tumors or unknown histology were excluded.
In 2012, the Thoracic Surgery Unit of the Fondazione IRCCS Istituto Nazionale dei Tumori di Milano, Italy, established a Lung-MDT, comprising thoracic surgeons, radiation oncologist, medical oncologist, pneumologists, radiologists, and pathologist. The primary goal of the MDT was to identify the most suitable treatment strategy for “difficult cases” and especially for all stage III LCs.
We divided patients into two cohorts: those diagnosed pre-MDT (from January 1, 2005 to December 31, 2011), and those post-MDT (from January 1, 2012 to December 31, 2020) (Figure 1). The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). Ethical approval was obtained from the Institutional Review Board of the Fondazione IRCCS Istituto Nazionale dei Tumori di Milano (INT 142/21; approval date: 27 May 2021). Informed consent was taken from all the patients.
Figure 1.
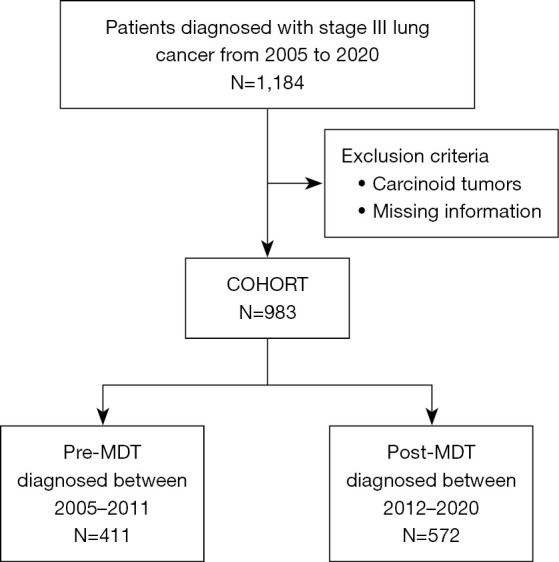
Flow-chart of the study. MDT, multidisciplinary team.
Data collection
Patient’s sociodemographic and clinical characteristics were collected from medical records. Each electronic or paper medical record for cases prior to 2009 was reviewed, and all clinical and demographic information was summarized within a database. The therapeutic path included surgical approach, chemotherapy (CT), RT, TT, and IT. We categorized surgeries as lobectomy (lobectomy and bilobectomy), pneumonectomy, and sublobar resection (segmentectomy and wedge resection). Histology was classified as adenocarcinoma, squamous and large cell neuroendocrine non-small cell lung cancer (NSCLC) carcinomas, and small cell lung cancer (SCLC). In Table S1 details on all different types of histology were reported. In Table S2 can be found details on how the different categories have been divided.
Outcomes
The primary outcome was the 5-year overall survival (OS) comparing the pre-MDT and post-MDT cohorts, which was defined, for resected patients from the date of surgical procedure and for non-resected patients from the date of diagnosis, to the date of death from any cause or last follow-up (May 2023). Disease-free survival (DFS) was estimated in patients who underwent surgery, and it was defined as the time from the surgical procedure to the first occurrence or death from any cause. Ten patients reported relapses, but unfortunately, the relapse dates were missing. Due to this missing information, these cases were excluded from the DFS curve analysis.
The secondary outcome was to evaluate the treatment modality received in the different groups (as defined in Table S2) and estimate 5-year OS across the different treatment modalities.
Sensitivity analyses were performed to evaluate pre-MDT and post-MDT in a selected cohort. We included only patients who received the same treatment modalities pre- and post-MDT. Therefore, we included for this analysis patients who received CT + surgery + RT; CT + RT + surgery; CT + surgery; surgery only; surgery + CT; surgery + RT; surgery + RT + CT; and for non-resected patients: CT; CT+RT; RT; no-therapy. For these cohort we evaluated 5-year OS.
The vital status was obtained through the Istituto Nazionale di Statistica (ISTAT, SIATEL 2.0 platform).
Statistical analysis
Descriptive statistics were used for reporting patient demographic and clinical characteristics for the two cohorts (pre- and post-MDT). The chi-square test was used to test differences between two cohorts. OS was estimated using Kaplan-Meier methods, and the log-rank trend test was used to test any trends in the survival curves. A multivariate Cox proportional hazard regression model was implemented to identify the prognostic factor for OS. Due to the nature of the study, we used a 1:1 propensity score matching to adjust for the effects of sex, age at the diagnosis, smoking status, histology type, and TNM stage. Patients admitted pre-MDT were matched to patients admitted post-MDT. For this analysis we used the SAS macro %psmatch_multi. A P value of <0.05 was considered statistically significant. Analyses were done using Statistical Analysis System Software (Release SAS: 9.04; SAS Institute, Cary, North Carolina, USA).
Results
Patients’ characteristics
Between 2005 and 2020, a total of 983 patients with stage III LC were enrolled. Among these patients, 41.8% (411/983) belonged to pre-MDT cohort, while 58.2% (572/983) to the post-MDT cohort.
Patients diagnosed with stage III LC post-MDT were older, with 50.5% (289/572) being current smokers, whereas in the pre-MDT cohort, 85.6% (352/411) were current smokers. The percentage of females was higher in the post-MDT cohort compared to the pre-MDT cohort (39.5% vs. 28.7%, P=0.0005).
Regarding tumor characteristics, 63.4% (623/983) were diagnosed with adenocarcinoma, and 4.7% (46/983) were diagnosed with SCLC. More adenocarcinoma (66.8% vs. 58.6%) and less SCLC (3.5% vs. 6.3%), were present in the post-MDT cohort compared to the pre-MDT (P=0.009). There were no significant differences in staging between the two cohorts (P=0.69).
Out of the total patient population, 670 patients (68.2%) underwent surgical procedures, while 313 patients (31.8%) were not eligible for surgical intervention. The proportion of patients who underwent surgery were statistically different between pre-MDT and post-MDT cohorts (72.7% vs. 64.9%, P=0.009).
For resected patients, the number of pneumonectomy performed decreased between the two cohorts (22.1% pre-MDT and 15.1% post-MDT), and the number of lobectomies and sublobar resections increased slightly (P=0.042).
In resected group, trimodality therapy were 30.1% and 39.6% in pre- and post-MDT, respectively. Surgery with systemic therapy was 34.4% in pre-MDT and 35.3% in post-MDT cohort.
Between pre-MDT and post-MDT, 40.8% and 36.7% of patients relapsed (P<0.0001).
While in non-resected group, patients treated with chemoradiotherapy were 20.5% in pre-MDT and 38.8% in post-MDT cohort (Table 1).
Table 1. Patient and clinical characteristics.
| Characteristics | Total, N=983 | Pre-MDT, N=411 | Post-MDT, N=572 | P |
|---|---|---|---|---|
| Patient’s characteristics | ||||
| Age at the diagnosis (years), n (%) | 0.004 | |||
| <55 | 137 (13.9) | 73 (17.8) | 64 (11.2) | |
| 55–74 | 683 (69.5) | 282 (68.6) | 401 (70.1) | |
| ≥75 | 163 (16.6) | 56 (13.6) | 107 (18.7) | |
| Sex, n (%) | 0.001 | |||
| Female | 344 (35) | 118 (28.7) | 226 (39.5) | |
| Male | 639 (65) | 293 (71.3) | 346 (60.5) | |
| Smoking status, n (%)a | <0.0001 | |||
| Current smoker | 641 (65.2) | 352 (85.6) | 289 (50.5) | |
| Ex-smoker | 222 (22.6) | 3 (0.7) | 219 (38.3) | |
| Never smoke | 113 (11.5) | 52 (12.7) | 61 (10.7) | |
| Tumor characteristics | ||||
| Histology type, n (%) | 0.009 | |||
| Adenocarcinoma | 623 (63.4) | 241 (58.6) | 382 (66.8) | |
| Squamous cell carcinoma | 198 (20.1) | 94 (22.9) | 104 (18.2) | |
| Large cell neuroendocrine carcinoma | 40 (4.1) | 12 (2.9) | 28 (4.9) | |
| Small cell lung cancer (SCLC) | 46 (4.7) | 26 (6.3) | 20 (3.5) | |
| Other tumor not otherwise classified | 76 (7.7) | 38 (9.2) | 38 (6.6) | |
| Stage TNM 8th edition, n (%) | 0.69 | |||
| IIIA | 725 (73.8) | 299 (72.7) | 426 (74.5) | |
| IIIB | 244 (24.8) | 107 (26) | 137 (24) | |
| IIIC | 14 (1.4) | 5 (1.2) | 9 (1.6) | |
| Therapeutic approach | ||||
| Surgery, n (%) | 0.009 | |||
| Yes | 670 (68.2) | 299 (72.7) | 371 (64.9) | |
| No | 313 (31.8) | 112 (27.3) | 201 (35.1) | |
| Resected only | 670 | 299 | 371 | |
| Type of surgical procedure, n (%) | 0.04 | |||
| Pneumonectomy | 122 (18.2) | 66 (22.1) | 56 (15.1) | |
| Lobectomy | 488 (72.8) | 211 (70.6) | 277 (74.7) | |
| Sublobar | 60 (9) | 22 (7.4) | 38 (10.2) | |
| Treatment modalities, n (%) | 0.006 | |||
| Trimodality therapy | 237 (40.7) | 90 (30.1) | 147 (39.6) | |
| Surgery + systemic therapy | 234 (34.9) | 103 (34.4) | 131 (35.3) | |
| Surgery +/− RT | 199 (29.7) | 106 (35.5) | 93 (25.1) | |
| Relapse, n (%) | <0.0001 | |||
| Yes | 258 (38.5) | 122 (40.8) | 136 (36.7) | |
| No | 213 (31.8) | 61 (20.4) | 152 (41.0) | |
| Unknown | 199 (29.7) | 116 (38.8) | 83 (22.4) | |
| Non-resected only | 313 | 112 | 201 | |
| Treatment modalities, n (%) | 0.004 | |||
| Chemoradiotherapy | 101 (32.3) | 23 (20.5) | 78 (38.8) | |
| Systemic therapy | 132 (41.9) | 54 (48.2) | 78 (38.8) | |
| No chemotherapy | 80 (25.6) | 35 (31.3) | 45 (22.4) |
a, 7 missing data. MDT, multidisciplinary team; TNM, tumour nodes metastasis; RT, radiotherapy.
In Table S2 are reported in detail all the treatment modalities received, stratified for resected and non-resected patients. The 1:1 propensity score matching analyses resulted in the selection of a pre-MDT cohort comprising 319 patients (Table S3).
Survival
The median follow-up time for the entire study population was 2.4 years, and 6.1 years for patients still alive at the end of the study. In the pre-MDT cohort, the median follow-up was 1.9 years, and 14.5 years for alive patients. For the post-MDT cohort, the median follow-up was 2.6 years, and 5.3 year for alive patients.
The 5-year OS rates were 25.3% for the pre-MDT and 33.9% for the post-MDT cohort (P=0.0008). Stratifying for resected and non-resected patients, we observed the same trend, 5-year OS rates were higher in post-MDT cohort for both resected (P=0.004) and non-resected (P=0.0001) patients (Figure 2). Figure S1 shows the 5-year DFS stratified only for resected patients, pre-MDT DFS was 23.7%, and DFS for post-MDT was 30.7% (P=0.03).
Figure 2.

Five-year survival in stage III lung cancer stratified by years, all patients, resected patients and non-resected patients. MDT, multidisciplinary team.
Figure 3 shows 5-year OS in resected patients pre-MDT and post-MDT categorized by treatment modalities. In both cohorts, treatment modalities exhibited statistically differences in survival (P=0.003 for pre-MDT; P=0.0004 for post-MDT). In pre-MDT cohort, patients who received trimodalities therapy achieved a higher 5-year survival rate (45.6%) compared to those who received systemic therapy (28.2%) or surgery with or without RT (26.4%). In the post-MDT cohort, the 5-year OS rates were 52.2% for patients treated with trimodalities therapy, 40.2% for those receiving systemic therapy, and 29.7% for patients who underwent surgery with or without RT.
Figure 3.

Five-year survival in stage III lung cancer stratified by treatments, for resected and non-resected patients pre- and post-MDT. MDT, multidisciplinary team; RT, radiotherapy.
Also, for non-resected patients, treatments modalities showed significant differences in both cohorts (Figure 3). In the pre-MDT cohort, 5-year survival rates were respectively 9.3% for patients who received systemic therapy, 4.3% for chemoradiotherapy, 2.9% for patients who did not received CT. In the post-MDT cohort, 5-year survival rates increased in patients who received chemoradiotherapy and systemic therapy, respectively 25.5% and 22.7%. For patients who did not received CT, 5-year survival rates were 2.2%.
We performed a Cox proportional model stratified for resected and non-resected patients (Table 2). In both groups, patients admitted post-MDT had a significantly lower risk of death than pre-MDT patients (resected patients aHR: 0.78, 95% CI: 0.64–0.95; non-resected patients aHR: 0.62, 95% CI: 0.48–0.80). For resected patients, patients treated with trimodality therapy had better survival than patients treated with surgery +/− RT (aHR: 0.55, 95% CI: 0.42–0.72), while no differences were observed between surgery +/− RT and surgery + systemic therapy (P=0.07). For non-resected patients, no differences were observed between patients treated with systemic therapy vs. chemoradiotherapy (P=0.28), while significant differences were observed between systemic therapy vs. No-CT (aHR: 3.99, 95% CI: 2.94–5.43).
Table 2. Cox regression model and propensity score analysis, stratified for resected and non-resected groups.
| Variables | Univariate analysis | Multivariate analysis* | Propensity score multivariate analysis | |||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | P | aHR (95% CI) | P | ps-aHR (95% CI) | P | |||
| Resected | ||||||||
| Period of surgery | ||||||||
| Pre-MDT | Ref | Ref | Ref | |||||
| Post-MDT | 0.75 (0.62–0.92) | 0.005 | 0.78 (0.64–0.95) | 0.01 | 0.73 (0.59–0.90) | 0.003 | ||
| Treatment | ||||||||
| Surgery +/− RT | Ref | Ref | Ref | |||||
| Trimodality therapy | 0.51 (0.40–0.65) | <0.0001 | 0.55 (0.42–0.72) | <0.0001 | 0.55 (0.42–0.74) | <0.0001 | ||
| Surgery + systemic therapy | 0.80 (0.64–1.00) | 0.06 | 0.80 (0.62–1.02) | 0.07 | 0.82 (0.63–1.07) | 0.14 | ||
| Non-resected | ||||||||
| Period of surgery | ||||||||
| Pre-MDT | Ref | Ref | Ref | |||||
| Post-MDT | 0.62 (0.48–0.79) | 0.0001 | 0.62 (0.48–0.80) | 0.0002 | 0.58 (0.44–0.77) | 0.0001 | ||
| Treatment | ||||||||
| Systemic therapy | Ref | Ref | Ref | |||||
| Chemoradiotherapy | 0.82 (0.61–1.10) | 0.19 | 0.85 (0.63–1.14) | 0.28 | 0.84 (0.61–1.14) | 0.35 | ||
| No chemotherapy | 4.11 (3.05–5.55) | <0.0001 | 3.99 (2.94–5.43) | <0.0001 | 4.16 (3.01–5.75) | <0.0001 | ||
*, adjusted for sex and age at the diagnosis. HR, hazard ratio; CI, confidence interval; MDT, multidisciplinary team; Ref, reference; RT, radiotherapy; ps-a, propensity score-adjustment.
Sensitivity analysis
Figure S2 shows a sensitivity analysis restricted only to patients who received the same treatment between pre-MDT and post-MDT. This analysis confirm that patients treated post-MDT had a higher 5-year OS, also stratified in resected and non-resected group.
The propensity score matched analysis showed similar results, indicating better survival in post-MDT compared to pre-MDT cohorts (resected patients psHR: 0.73, 95% CI: 0.59–0.90; non-resected patients psHR: 0.58, 95% CI: 0.44–0.77).
In SCLC patients, no significant survival difference was notice among pre-MDT and post-MDT cohorts (P=0.46, Figure S3). While comparing treatment modalities, patients with SCLC underwent surgical approach had 7.6% 5-year survival rate, while patients underwent chemoradiotherapy had a 13.9% 5-year survival rates (Figure S4, P<0.0001).
Discussion
Stage III LC is a highly heterogeneous disease, and the standard management in this setting is still being debated. To provide optimal management for each patient, the role of MDT has proven to be fundamental in establishing a clear diagnosis, staging and identifying the therapeutic options (12). This real-world study assessed long-term survival and different treatment modalities of patients with a diagnosis of stage III LC admitted pre-MDT and post-MDT. The higher 5-year OS rates in post-MDT cohort proved the biggest advantages obtained by employing a MDT approach suggesting the importance of this group in this heterogeneous stage. We also observed an improvement in the treatment management and the multidisciplinary influence in the post-MDT cohort. Specifically, the number of pneumonectomies decreased and the proportion of patients who received standard treatment, i.e. trimodality for the resected cohort and chemoradiotherapy for the non-resected cohort, increased. To mitigate the bias potentially introduced by the integration of IT, we performed a sensitivity analysis, focusing specifically on patients who received the same treatments, both pre- and post-MDT. The results demonstrated that the 5-year OS significantly improved in the post-MDT cohort, if compared to the pre-MDT one.
Innovative systemic treatment represented one of the variables that might influence OS rate in our post-MDT cohort patients. In particular, accumulating data showed that the implementation of IT and TT in the nadj and adj settings provided a significant improvement in stage I–III LC patients (13,14). In the IMpover010 study, adj atezolizumab in stage II–IIIA patients demonstrated a median DFS of 42.3 versus 35.3 months in the control arm (represented by best supportive care alone), with an estimated 34% reduction of relapse and death risk in patients treated with IT (HR 0.66, 95% CI: 0.50–0.98, P=0.0039) (13). On the other hand, in the PEARLS trial authors reported a slightly different median DFS of 53.6 months (95% CI: 39.2–NR) in patients treated with pembrolizumab versus 42 months (95% CI: 31.3–NR) in the placebo arm (HR 0.76, 95% CI: 063–0.91, P=0.0014) (14). Similarly, other studies showed the beneficial effect of adding IT and TT to CT in both nadj and adj settings (15-18).
Although surgery still remains the mainstay of treatment for most stage III LC, systemic treatment and RT are of paramount importance. Surgery allows tumour removal and the identification of risk factors for delivering adj therapies. Medical therapies and RT allow to reduce the risk of recurrence, mitigating worse disease characteristics, especially in patients with close or positive resection margins. As mentioned above, stage III LC management is characterized by a deep interconnection between different medical figures (i.e., surgeons, oncologists, radiotherapists), but consensus on optimal treatment of such disease is lacking, and historically concurrent chemoradiotherapy has been the preferred option. Hence, a personalized approach might be useful in providing a more effective treatment. While NSCLC landscape have rapidly changed, the local treatment for stage III SCLC have remained the same in the last 30 years highlighting the role of the aggressive biology of this disease and less potential for local control, especially surgery. In chemoradiotherapy candidate patients for limited disease SCLC, a recent study was concluded for which the results are awaited (ADRIATIC, NCT03703297) (19).
Globally, all this data is in line with the observations seen in our sample, and could help to explain the substantial survival improvement achieved in the last few years, together with the stable implementation of MDT. In addition, the OS differences seen between the two cohorts, would possibly broaden in the next future, following results of ongoing and just published clinical trials (13-17,20).
Of note, we have to remark the consistent reduction of pneumonectomy rate during the years observed in our sample, resulting in an improvement in life-quality for patients and a substantial reduction in treatment-related disability. Hopefully, the increasing knowledge about management of immune-related and TT-related toxicities will also help to enhance the quality-of-life after diagnosis of early-stage LC. In the next future, the potential use of chemo-free regimens in selected populations of patients could help to address this point.
In the cohort of non-resected patients, in the pre-MDT group we observed higher survival rates among those treated with systemic therapy compared to those treated with chemoradiotherapy. This effect was probably attributed to the use of pemetrexed as a companion agent to platinum-based therapy. In patients treated with systemic therapy, 13 (24%) were treated with pemetrexed, while in patients treated with chemoradiotherapy, pemetrexed it is not a regimen usually used and indicated.
In our study cohort, we also observed significant changes in the characteristics of patients admitted pre-MDT and post-MDT. It is widely known that men are more susceptible to developing LC than women (21). Our study confirmed this trend, as the incidence of stage III LC consistently remained higher in men than females in both cohorts. However, according to recent epidemiological observations, we observed a slight increase in the incidence of stage III LC among women. The slight increase could be attributed to changes in smoking habits (22,23). The prevalence of current smokers at the time of diagnosis decreased in post-MDT cohort, pointing out positive progress in tobacco control efforts. Both reasons probably explain also the increase of adenocarcinoma histology on the post-MDT cohort which is less (24,25). Moreover, this histology was recently proven to be related also with the air pollution (especially EGFR mut patients), which for sure increased in the last decade (26). However, it is important to note that the staging of diagnosed cases has remained unchanged, indicating that the disease is still being detected at similar stages despite changes in histological subtype reflecting the unchanged situation in screening programs, which is still, despite the advances, not a clinical practice reality.
The strength of this study was the large cohort and the 18-year study period. However, there were some limitations. First, our study was a single-centre, retrospective, observational, real-world study, which may limit the generalizability of the results. To address these limitations, we conducted a propensity score matching analysis to compare similar cohorts, that confirmed the results. Despite these limitations, our data indicate improved survival for patients treated within a MDT context with different expertise and the better adoption and “acceptance” of the innovative treatment strategies.
Conclusions
In conclusion, this study highlighted and demonstrated that the landscape of the III stage LC patients was not only improved due to the recent advances of treatment strategies, especially in terms of systemic therapy but also their adoption and use with a better sharing within a context of an MDT. Moreover, less invasive local strategies (e.g., RT vs. surgery or stereotaxic RT vs. traditional RT) have been easily endorsed, giving opportunity for a better survival also to frail patients. Finally, less invasive surgery strategies combined (lobectomy vs. pneumonectomy) with next-generation systemic therapy have led to a lower mortality, improving 5-year OS. All these changes are the result of the perfect combination between research advances but also to a better adoption within an MDT team.
Supplementary
The article’s supplementary files as
Acknowledgments
The authors thank Claudio Jacomelli for data management.
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). Ethical approval was obtained from the Institutional Review Board of the Fondazione IRCCS Istituto Nazionale dei Tumori di Milano (INT 142/21; approval date: 27 May 2021). Informed consent was taken from all the patients.
Footnotes
Reporting Checklist: The authors have completed the STROBE reporting checklist. Available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-508/rc
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-508/coif). The authors have no conflicts of interest to declare.
Data Sharing Statement
Available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-508/dss
References
- 1.Kratzer TB, Bandi P, Freedman ND, et al. Lung cancer statistics, 2023. Cancer 2024;130:1330-48. 10.1002/cncr.35128 [DOI] [PubMed] [Google Scholar]
- 2.Detterbeck FC, Boffa DJ, Kim AW, et al. The Eighth Edition Lung Cancer Stage Classification. Chest 2017;151:193-203. [DOI] [PubMed] [Google Scholar]
- 3.Gillaspie EA, Wigle DA. Management of Stage IIIA (N2) Non-Small Cell Lung Cancer. Thorac Surg Clin 2016;26:271-85. 10.1016/j.thorsurg.2016.04.001 [DOI] [PubMed] [Google Scholar]
- 4.Goldstraw P, Chansky K, Crowley J, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 2016;11:39-51. 10.1016/j.jtho.2015.09.009 [DOI] [PubMed] [Google Scholar]
- 5.Bardia A, Jhaveri K, Im S, et al. LBA11 - Datopotamab deruxtecan (Dato-DXd) vs chemotherapy in previously-treated inoperable or metastatic hormone receptor-positive, HER2-negative (HR+/HER2–) breast cancer (BC): Primary results from the randomised phase III TROPION-Breast01 trial. Ann Oncol 2023;34:S1254-S1335. [Google Scholar]
- 6.Boxer MM, Vinod SK, Shafiq J, et al. Do multidisciplinary team meetings make a difference in the management of lung cancer? Cancer 2011;117:5112-20. 10.1002/cncr.26149 [DOI] [PubMed] [Google Scholar]
- 7.Bydder S, Nowak A, Marion K, et al. The impact of case discussion at a multidisciplinary team meeting on the treatment and survival of patients with inoperable non-small cell lung cancer. Intern Med J 2009;39:838-41. 10.1111/j.1445-5994.2009.02019.x [DOI] [PubMed] [Google Scholar]
- 8.Pan CC, Kung PT, Wang YH, et al. Effects of multidisciplinary team care on the survival of patients with different stages of non-small cell lung cancer: a national cohort study. PLoS One 2015;10:e0126547. 10.1371/journal.pone.0126547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bilfinger TV, Albano D, Perwaiz M, et al. Survival Outcomes Among Lung Cancer Patients Treated Using a Multidisciplinary Team Approach. Clin Lung Cancer 2018;19:346-51. 10.1016/j.cllc.2018.01.006 [DOI] [PubMed] [Google Scholar]
- 10.Tamburini N, Maniscalco P, Mazzara S, et al. Multidisciplinary management improves survival at 1 year after surgical treatment for non-small-cell lung cancer: a propensity score-matched study. Eur J Cardiothorac Surg 2018;53:1199-204. 10.1093/ejcts/ezx464 [DOI] [PubMed] [Google Scholar]
- 11.Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J Clin 2017;67:93-9. [DOI] [PubMed] [Google Scholar]
- 12.Batra U, Munshi A, Kabra V, et al. Relevance of multi-disciplinary team approach in diagnosis and management of Stage III NSCLC. Indian J Cancer 2022;59:S46-55. 10.4103/ijc.IJC_51_21 [DOI] [PubMed] [Google Scholar]
- 13.Felip E, Altorki N, Zhou C, et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet 2021;398:1344-57. Correction appears in Lancet 2021;398:1686. [DOI] [PubMed]
- 14.O'Brien M, Paz-Ares L, Marreaud S, et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol 2022;23:1274-86. 10.1016/S1470-2045(22)00518-6 [DOI] [PubMed] [Google Scholar]
- 15.Wu YL, Tsuboi M, He J, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Engl J Med 2020;383:1711-23. 10.1056/NEJMoa2027071 [DOI] [PubMed] [Google Scholar]
- 16.Herbst RS, Wu YL, John T, et al. Adjuvant Osimertinib for Resected EGFR-Mutated Stage IB-IIIA Non-Small-Cell Lung Cancer: Updated Results From the Phase III Randomized ADAURA Trial. J Clin Oncol 2023;41:1830-40. 10.1200/JCO.22.02186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Deutsch JS, Cimino-Mathews A, Thompson E, et al. Association between pathologic response and survival after neoadjuvant therapy in lung cancer. Nat Med 2024;30:218-28. 10.1038/s41591-023-02660-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Awad MM, Forde PM, Girard N, et al. 1261O - Neoadjuvant nivolumab (N) + ipilimumab (I) vs chemotherapy (C) in the phase III CheckMate 816 trial. Ann Oncol 2023:34:S732-45. [Google Scholar]
- 19.Senan S, Shire N, Mak G, et al. ADRIATIC: A phase III trial of durvalumab 6 tremelimumab after concurrent chemoradiation for patients with limited stage small cell lung cancer. Ann Oncol 2019;30:II25. 10.1016/j.cllc.2019.12.006 [DOI] [PubMed] [Google Scholar]
- 20.Wakelee H, Liberman M, Kato T, et al. Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N Engl J Med 2023;389:491-503. 10.1056/NEJMoa2302983 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tolwin Y, Gillis R, Peled N. Gender and lung cancer-SEER-based analysis. Ann Epidemiol 2020;46:14-9. 10.1016/j.annepidem.2020.04.003 [DOI] [PubMed] [Google Scholar]
- 22.Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin 2023;73:17-48. 10.3322/caac.21763 [DOI] [PubMed] [Google Scholar]
- 23.Jemal A, Ma J, Rosenberg PS, et al. Increasing lung cancer death rates among young women in southern and midwestern States. J Clin Oncol 2012;30:2739-44. 10.1200/JCO.2012.42.6098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Toh CK, Gao F, Lim WT, et al. Never-smokers with lung cancer: epidemiologic evidence of a distinct disease entity. J Clin Oncol 2006;24:2245-51. 10.1200/JCO.2005.04.8033 [DOI] [PubMed] [Google Scholar]
- 25.Vasudevan S, Krishna V, Mehta A. Lung Cancer in Non-Smokers: Clinicopathological and Survival Differences from Smokers. Cureus 2022;14:e32417. 10.7759/cureus.32417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hill W, Lim EL, Weeden CE, et al. Lung adenocarcinoma promotion by air pollutants. Nature 2023;616:159-67. 10.1038/s41586-023-05874-3 [DOI] [PMC free article] [PubMed] [Google Scholar]