

Abstract
Background:
Many rural-urban indexes are utilized in cancer research. This variation introduces inconsistencies between studies. Recommendations on index use have prioritized geographical unit over feasibility of inclusion in analysis. We evaluated rural-urban indexes and recommend one for use to increase comparability across studies.
Methods:
We assessed 9 US rural-urban indexes regarding their respective rural and urban code ranges; geographical unit, land area, and population distributions; percent agreement; suitability for analysis; and integration feasibility for national, state, and local cancer research. We referenced 1569 Wisconsin Pancreatic Cancer Registry patients to demonstrate how index choice affects patient categorization.
Results:
Six indexes categorized rural and urban areas. Indexes agreed on binary rural-urban designation for 88.8% of the US population. As ternary variables, they agreed for 83.4%. For cancer registry patients, this decreased to 73.4% and 60.4% agreement, respectively. Rural-Urban Continuum Codes (RUCC) performed the best in differentiating metropolitan, micropolitan, and rural counties; availability for retrospective and prospective studies; and continuous coding for analysis.
Conclusions:
Urban/rural patient categorization changed with index selection. We conclude that RUCC is an appropriate and feasible rural-urban index to include in cancer research, as it is standardly available in national cancer registries, can be matched to patient’s county of residence for local research, and it had the least amount of fluctuation of the indices analyzed. Utilizing RUCC as a continuous variable across studies with a rural-urban component will increase reproducibility and comparability of results and eliminate rural-urban index choice as a potential source of discrepancy between studies.
BACKGROUND
Rurality predicts later stages of cancer diagnosis,1 lower rates of therapies,2 less effective therapies,3 shorter survival,4 and higher mortality.5 Stage at diagnosis is an important indicator of cancer patient outcomes and survival, and studies have shown that rural patients are diagnosed at a later stage than their metro counterparts.1,4,5 Rurality may impact patients’ access to specific or specialist therapies, such as access to radiation therapy for breast cancer2 or definitive surgical treatment for prostate cancer.3 Rurality also may delay access to treatments, including for rural patients with gastric cancers where they waited longer receive surgery and had a higher percentage of positive surgical margins than their metro counterparts.4 Rural pancreatic cancer patients were less likely to undergo pancreatectomy5 and have poorer overall survival6,7 and 1-year mortality.5 These trends persist across geographical regions and cancer types.3,8 However, variation in treatment and outcomes between rural and urban patients also exist,2,9 resulting from community,10 demographic,11 and health care differences.12
Differences in identifying rurality produce inconsistencies in disparities.9 More than 9 rural-urban indexes are used and based on differing geographic units, including census tract, ZIP code, and county. Indexes differ in their inclusion criteria, incorporating factors like population, commuting percentage, and adjacency to urban areas. Additionally, there is confusion over terms equating urban and metropolitan, despite being distinct terms. Furthermore, in reviewing rural cancer studies, we identified gaps in rural-urban index deployment, including incorrect index identification, omission of index,13 and outdated indexes.14 Researchers often focus on geographical community measures – specifically census tract-based indexes, the smallest area measurement. This is detrimental to index availability in data sources.1,9
We evaluated indexes on their categorization across the rural-urban continuum. We examined indexes across their rural and urban code ranges; geographical unit, land area, and population distributions; suitability as continuous variables in analysis; and feasibility for integration into cancer research. We utilized the UW Health Pancreatic Cancer Registry patient cohort to demonstrate how index choice influences patient categorization. Pancreas cancer was chosen for study because it is one of the few cancers in Wisconsin that is increasing in frequency, its urgency in treatment, and the known effect of access to higher volume centers on outcomes.
METHODS
Rural-Urban Indexes
We identified 9 rural-urban indexes between 2000–2020: Urban Rural Classification of Urban Areas and Urban Clusters (UACE);15 Core Based Statistical Areas (CBSA);16 Frontier and Remote Area Codes (FAR);17 Rural-Urban Commuting Area Codes (RUCA);18 Aging, Independence, and Disability Rural-Urban Commuting Area Codes at the ZIP Code Tabulation Area level (RUCA[z]);19,20 Rural-Urban Continuum Codes (RUCC);21 Urban Influence Codes (UIC);22 National Center for Health Statistics (NCHS) Urban-Rural Classification Scheme for Counties;23 and the Index of Relative Rurality (IRR).24 We retrieved indexes spanning 1980–2013 from publishers’ websites. Each index is described elsewhere.1,9,10,25
Land Area and Population Data
We acquired land area and population at the geographical unit of each index to compare land area and population distributions. Geographical units included census block (UACE), census tract (RUCA), ZIP Code Tabulation Area (FAR, RUCA[z]), and county (RUCC, UIC, NCHS, IRR, CBSA). UACE, RUCA, and FAR indexes included 2010 population and land area variables in their source files. We obtained 2010 county-level population and land area data from the 2010 Census of Population Summary File 1 for RUCC, UIC, NCHS, IRR, and CBSA. The RUCA(z) index is based on approximate boundaries of 2013 ZIP Code Tabulation Areas (ZCTA).24 Since these boundaries fluctuate over time, we were unable to obtain the 2013 ZCTA population or land area on which RUCA(z) was based. Therefore, we excluded this index from parts of our analysis.
To demonstrate how index choice may affect categorization, 1569 patients from the UWHealth pancreatic cancer registry diagnosed during 2004–2016 with pancreatic ductal adenocarcinoma (PDAC) served as a reference population. This includes all patients diagnosed with PDAC at UW Health during this time-frame. Mean age at diagnosis was 66.7 years (SD 10.8 years); 54.4% of patients were male; and 86% of patients identified as non-Hispanic White. Patients presented with the following: local disease 10.9%, regional disease 45.7%, and distant disease 38.6%.
We evaluated differences in rurality via percent agreement across county and ZCTA-based binary and ternary indexes. We compared the change in each index’s median and interquartile range and mean over time.
Comparing Rural-Urban Indexes
In comparing indexes, we evaluated the extent to which rural and urban communities are differentiated – and the extent to which distinctions are made within communities. Supplemental Table 1 shows the 9 indexes by geographical unit, classification of urban/rural, the amount and percentage of land area, geographical units, and population each index classifies as urban/rural (2010 versions) for the US, midwestern states, and Wisconsin.
We excluded indexes that simply distinguished rural from urban communities (UACE, CBSA, and FAR) (Supplemental Table 1). We included the remaining indexes in the full analysis. We transformed these to binary indexes (metropolitan and non-metropolitan) and to ternary indexes (metropolitan, micropolitan/urban, and noncore/small town/rural). Because IRR is a continuous variable, we established divisions between metropolitan and nonmetropolitan counties at IRR = 0.50 and further subdivided nonmetropolitan counties into micropolitan/urban and rural counties at IRR = 0.60.25
We calculated Cohen’s kappa, with an ordinal weight, to evaluate the level of agreement across indexes in their binary and ternary forms by geographical units, land area, and population. We also compared the percentage agreement of geographical units, land area, and population (Table 1, Supplemental Table 2). We compared the distribution via median, interquartile range, mean, and standard deviation. We examined these trends visually via violin plots, with indexes standardized to illustrate transitions along a rural-urban interface (Figure 1, Supplemental Figure 1).
Table 1.
Agreement Between Binary and Ternary Rural-Urban Indexes at the US Population and UW Health Pancreatic Cancer Registry (n = 1539 Patients) Levels
| Variable Type | Indexes Included | Agreement/Disagreement | Rural-Urban Category | US Population | Registry Patientsa | ||||
|---|---|---|---|---|---|---|---|---|---|
| Count | % | % Agreement/Disagreement | Count | % | % Agreement Disagreement | ||||
| Binary | RUCC, UIC, NCHS, IRRb, RUCA | Agree | Metropolitan | 247 994 082 | 80.3 | 88.8 | 908 | 59.0 | 73.4 |
| Nonmetropolitan | 26 248 722 | 8.5 | 222 | 14.4 | |||||
| Disagree | Metropolitan and nonmetropolitan | 34 347 840 | 11.1 | 11.1 | 408 | 26.5 | 26.5 | ||
| Binary | RUCC, RUCA | Agree | Metropolitan | 252 306 164 | 81.7 | 94.9 | 920 | 59.8 | 91.0 |
| Nonmetropolitan | 40 789 077 | 13.2 | 480 | 31.2 | |||||
| Disagree | Metropolitan and nonmetropolitan | 15 650 297 | 5.1 | 5.1 | 138 | 9.0 | 9.0 | ||
| Ternary | RUCC, UIC, NCHS, IRR,b RUCA | Agree | Metropolitan | 247 994 082 | 80.3 | 83.4 | 908 | 59.0 | 60.4 |
| Micropolitan | 8 722 475 | 2.8 | 21 | 1.4 | |||||
| Rural/Noncore | 886 289 | 0.3 | 1 | 0.1 | |||||
| Disagree-1 level | Metropolitan and micropolitan | 24 208 656 | 7.8 | 13.2 | 244 | 15.9 | 28.8 | ||
| Micropolitan and rural/noncore | 16 639 958 | 5.4 | 200 | 13.0 | |||||
| Disagree-2 levels | Metropolitan and rural/noncore | 4 639 840 | 1.5 | 1.5 | 28 | 1.8 | 1.8 | ||
| Disagree-all levels | Metropolitan, micropolitan, and rural/noncore | 5 499 314 | 1.8 | 1.8 | 136 | 8.8 | 8.8 | ||
| Ternary | RUCC, RUCA | Agree | Metropolitan | 252 306 164 | 88.4 | 88.8 | 920 | 59.8 | 74.9 |
| Micropolitan | 405 347 | 0.1 | 184 | 12.0 | |||||
| Rural/Noncore | 827 415 | 0.3 | 49 | 3.2 | |||||
| Disagree-1 level | Metropolitan and micropolitan | 10 777 424 | 3.8 | 9.5 | 87 | 5.7 | 21.7 | ||
| Micropolitan and rural/noncore | 16 270 060 | 5.7 | 247 | 16.0 | |||||
| Disagree-2 levels | Metropolitan and rural/noncore | 4 872 873 | 1.7 | 1.7 | 51 | 3.3 | 3.3 | ||
RUCA(z) was used in place of RUCA for the Registry patients since patient ZIP codes were available in the registry and census tracts were not.
The Index of Relative Rurality (IRR) was missing data for 0.1% of the US population and Registry patients.
Figure 1.

Comparison of Rural-Urban Index DIstributions (A) Across the US Population, (B) Wisconsin Population, and (C) UW Health Pancreatic Cancer Registry Patients
Each index is standardized such that the “Rural-Urban Interface” line lies between those values that the index designated as urban (left of line) and rural (right of line). Center points indicate the median of the index, boxes indicate the interquartile range, and spikes indicate the upper- and lower-adjacent values (1.5 times the interquartile range).
a RUCA(z) is based on 2013 ZCTAs. US and Wisconsin population data are not available at the ZCTA level for 2013; therefore, those distributions are excluded from the Figure.
We used STATA Version 16.1 (StataCorp LLC, College Station, Texas) to complete the analysis and ArcGIS Version 10.7 (Environmental Systems Research Institute, Redlands, California) to create maps.
RESULTS
Inconsistency and Agreement Across Binary Rural-Urban Designations
Supplemental Table 1 displays the geographical unit, rural-urban delineation, and rural-urban categorization of land area, geographical units, and total population for each index. Two methods exist to designate between rural or urban in RUCA and RUCA(z), both shown in Figures 2 and 3.
Figure 2.
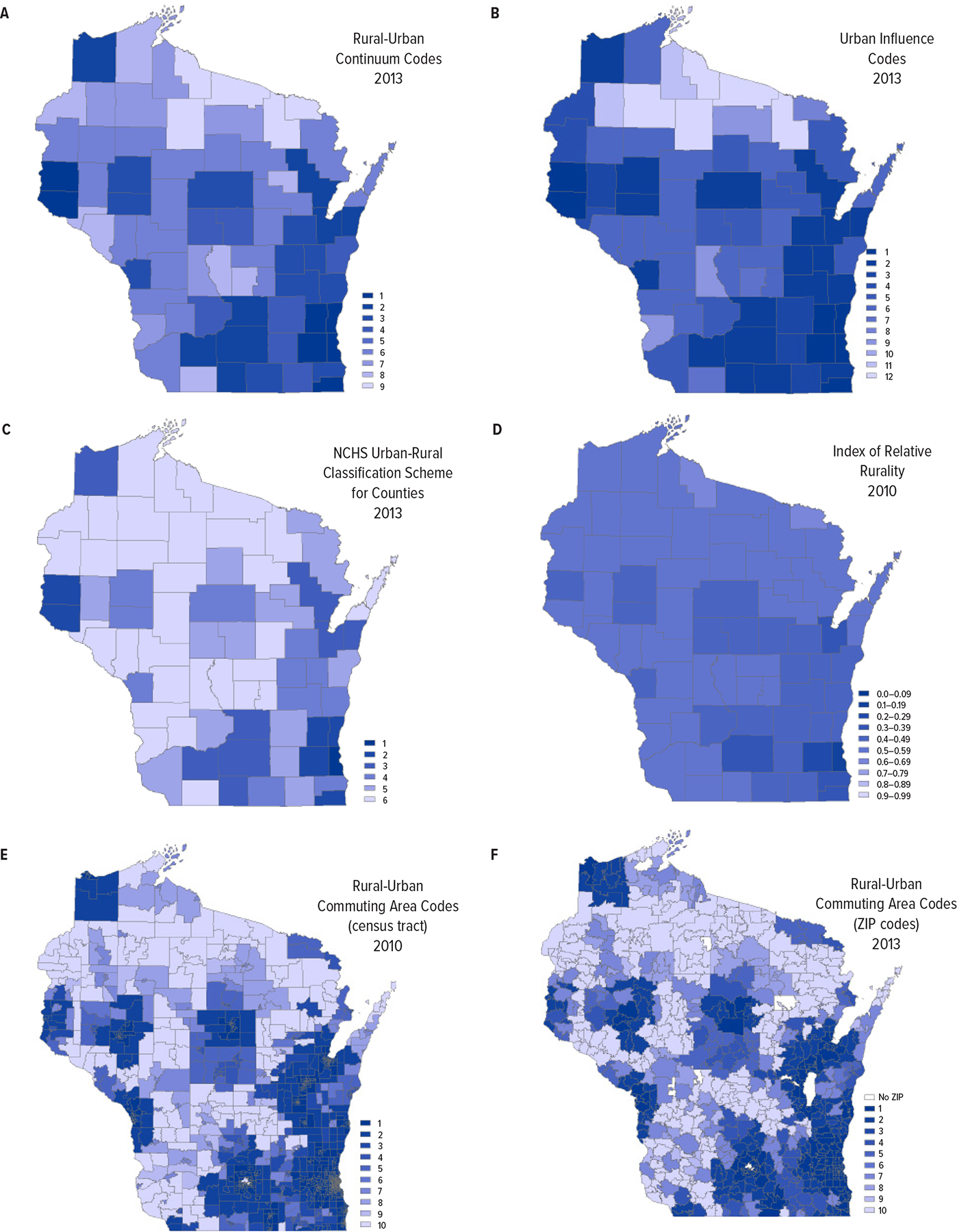
Maps of Wisconsin Rurality by Six Different Rural-Urban Indexes
Darker colors indicate more urban areas, and lighter colors indicate more rural areas. Rural-Urban Continuum Codes (A), Urban Influence Codes (B), National Center for Health Statistics (NCHS) Urban-Rural Classification Scheme for Counties (C), and Index of Relative Rurality (D) maps are at the county level. Rural-Urban Commuting Area map (E) is at the census tract level. ZIP Code Tabulation Area (ZCTA) Rural-Urban Commuting Area (F) map is at the ZCTA level.
Figure 3.
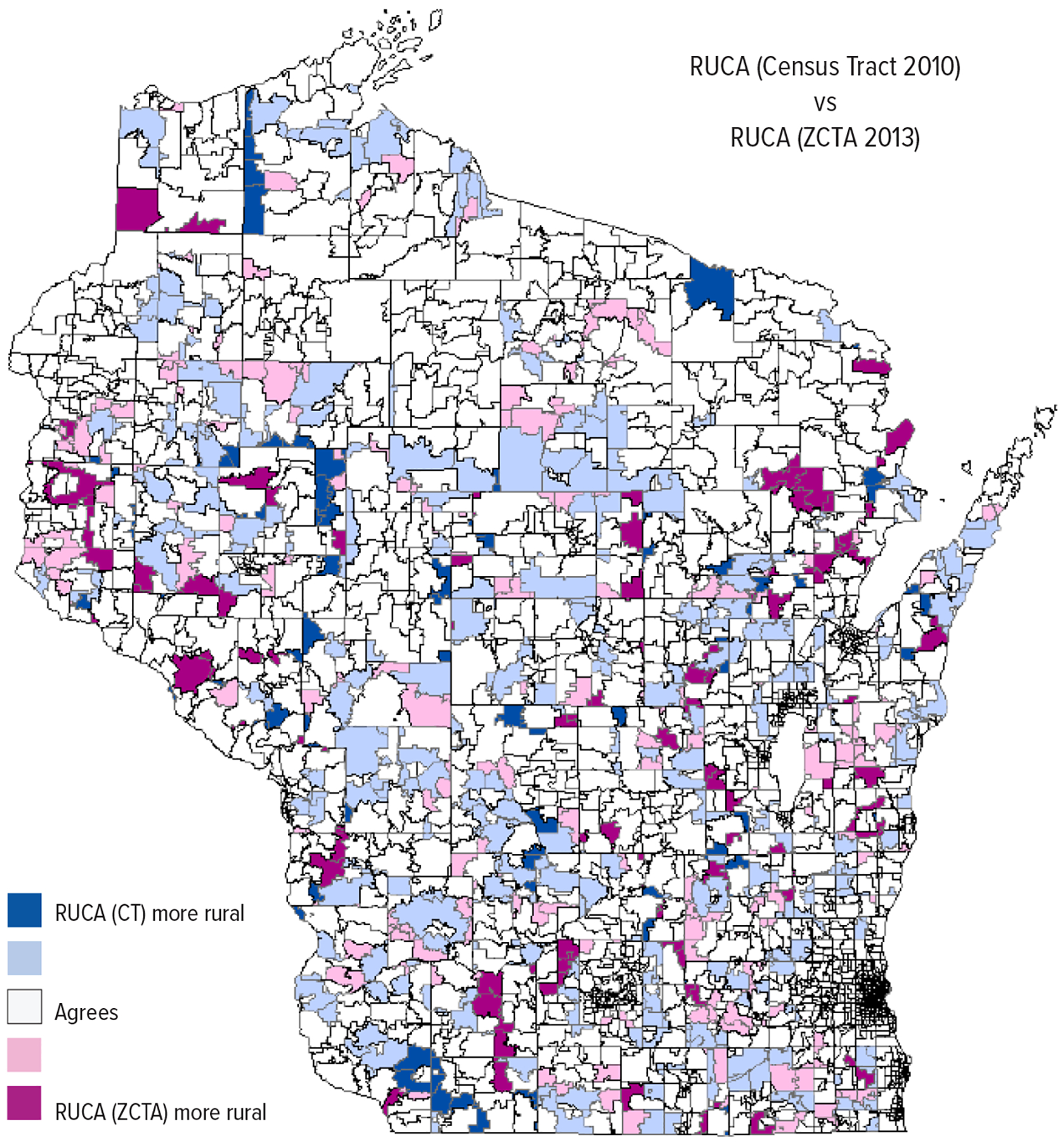
Comparing Rural Urban Commuting Area (RUCA) Indexes (primary codes only) Based on Census Tract (CT) and ZIP Code Tabulated Area (ZCTA) Across Wisconsin
Dark blue indicates Census Tract-based RUCA (RUCA [CT]) categorized areas as more rural than ZCTA-based RUCA (RUCA [ZCTA]) by a code difference of 5 to 9 (2.6% of land area). Light blue indicates RUCA (CT) categorized areas as more rural than RUCA (ZCTA) by a code difference of 1 to 4 (16.3% of land area). Deep pink indicates RUCA (ZCTA) categorized areas as more rural than RUCA (CT) by a code difference of 5 to 9 (3.9% of land area). Light pink indicates RUCA (ZCTA) categorized areas as more rural than RUCA (CT) by a code difference of 1 to 4 (6.2% of land area). RUCA (CT) and RUCA (ZCTA) agreed for white areas (71.1% of land area).
Accompanied by a difference across rural/urban communities, there is also a distribution within rural areas across indexes. The percentage of rural communities (by geographical unit) in the US ranged from 17.5% of ZCTAs (RUCA [option 2]) to 63.0% of counties (IRR) (Supplemental Table 1). By comparison, the difference in percentage of rural communities is even larger across Wisconsin communities (13.2% to 63.9%). The percentage of rural land area ranged from 52% (FAR) to 97% (UACE). Variation in land area was smaller across indexes categorizing both rural and urban areas. Similarly, the rural US population in indexes categorizing rural or urban areas is 3.9% (FAR) to 19.3% (UA) of the US population compared to indexes categorizing rural and urban areas allocating 11.5% (IRR) to 16.5% (RUCA [option 1]).
Binary rural or urban designations agreed across RUCA, RUCC, UIC, NCHS, and IRR indexes for 88.8% of the US population (Table 1, Supplemental Table 2). RUCC and RUCA – the 2 most employed indexes in cancer research – agreed on 94.9% of the population. Of Registry patients classifications, 73.4% agreed across binary RUCC, UIC, NCHS, IRR, and RUCA(z) indexes. This increased to 91.0% when comparing RUCC and RUCA(z) only. We included RUCA(z) as patient ZIP codes were known.
Cohen’s kappa ranged from 0.60 when comparing IRR with RUCC, UIC, and NCHS to 0.81 when comparing RUCA with RUCC, UIC, and NCHS, indicating moderate-to-very good agreement between indexes. We excluded RUCA(z) from this analysis as ZCTAs cannot be matched one-to-one with census tracts or counties.
Agreement Decreased Across Ternary Metropolitan, Micropolitan, and Rural Designations
RUCA, RUCC, UIC, NCHS, and IRR indexes agreed on ternary metropolitan, micropolitan, and rural designations for 83.4% of the US population (Table 1, Supplemental Table 2). These indexes simultaneously designate 6.0% of land area and 1.8% of US population as rural, micropolitan, and metropolitan depending on the index used. Adding further confusion, while some indexes designate 5.3% of land area and 1.5% of total population as rural, other indexes designate these same areas and people as metropolitan. Again, there is higher agreement across designation among RUCC and RUCA indexes, with 88.8% of US population in agreement. Within the Registry patients, 60.4% agreed across these indexes for ternary metropolitan, micropolitan, or rural communities, increasing to 74.9% when limited to RUCC and RUCA(z). RUCA(z) was included in the Registry patient analysis since patient ZIP codes were known. Cohen’s kappa ranged across indexes from 0.53 for IRR compared to UIC and NCHS to 0.77 for RUCC and RUCA compared to UIC and NCHS, indicating moderate-to-good agreement as ternary indexes.
Differences in Discrete or Continuous Index Geographical Units, Land Area, and Population Distributions
Figure 1 and Supplemental Figure 1 show RUCC, UIC, NCHS, IRR, RUCA, and RUCA(z) total population, geographical units, and land area distributions across the US and Wisconsin. Maps of Wisconsin based on each index are shown in Figure 2; the discrepancy between RUCA and RUCA(z) in Wisconsin is shown in Figure 3. The median geographical unit across the US is urban for RUCA and RUCA(z); conversely, the median is rural for RUCC, UIC, NCHS, and IRR. The median land area distribution is rural for the 5 county and census tract-based indexes, and the median population distribution is urban for the same indexes. RUCA(z) was excluded from the land area and population distribution analysis since 2013 ZCTA-based land area and population totals were unavailable. The rural-urban distribution of Registry patients followed Wisconsin population distribution trends.
Changes in Discrete or Continuous Index Distributions Over Time
RUCC, RUCA, UIC, NCHS, and RUCA(z) indexes captured changes in rural-urban community designations over time (Figure 4, Supplemental Figure 2). RUCC changes on a per-county basis are mapped in Figure 5. The mean rural-urban value across counties, ZCTAs, and census tracts for each index decreased over time. The distributions highlight where indexes underwent methodological changes (Figure 4, Supplemental Figure 2).
Figure 4.
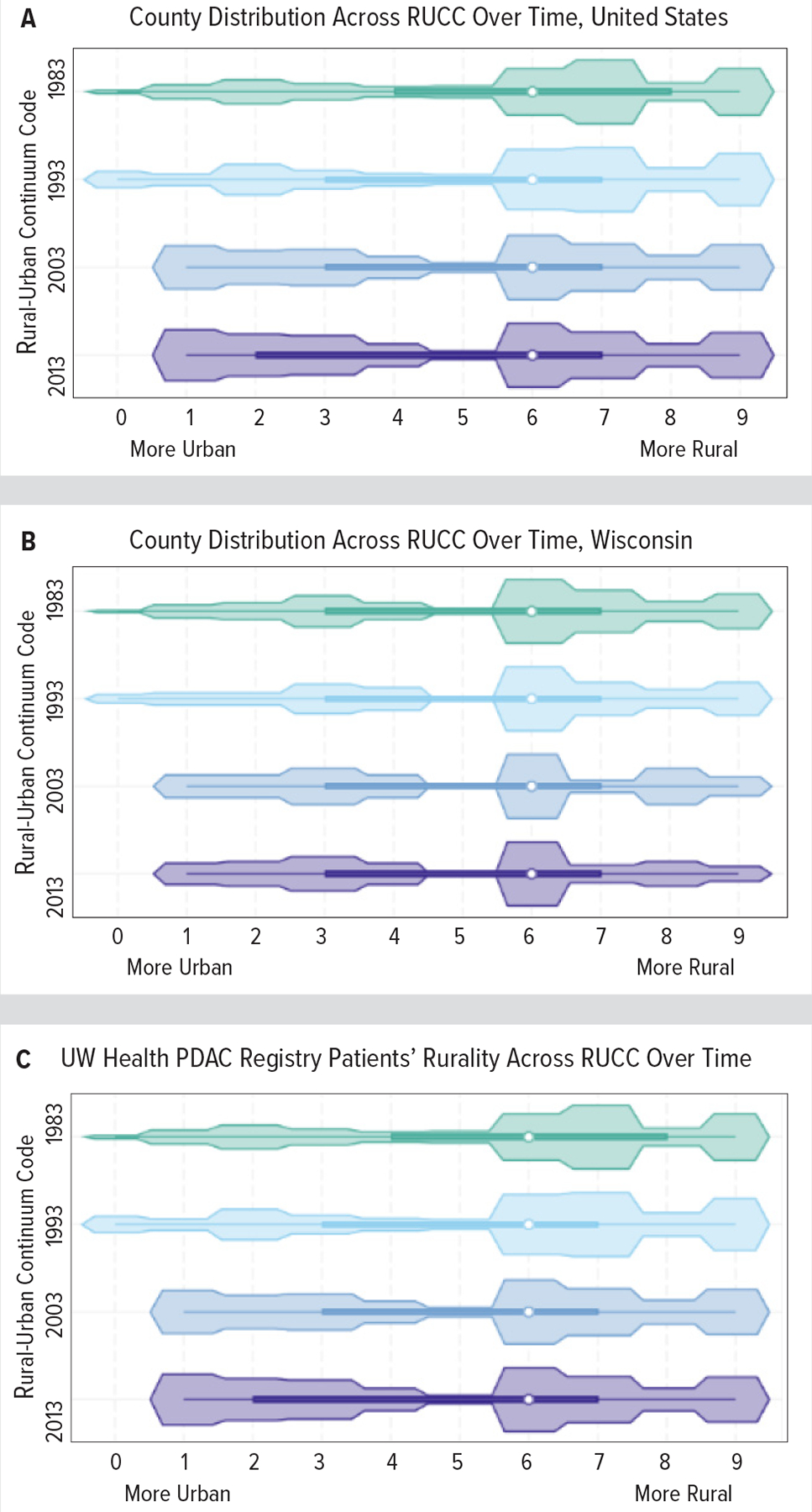
Rurality Over Time: Rural-Urban Continuum Code (RUCC) Geographical Unit Distributions Across the US (A), Wisconsin (B), and UW Health Pancreatic Cancer Registry Patients (C).
Abbreviation: PDAC, pancreatic ductal adenocarcinoma.
Geographical unit is measured at the county level for RUCC. Center points indicate the median code of the index, boxes indicate the interquartile range, and spikes indicate the upper- and lower-adjacent values (1.5 times the inter-quartile range). Changes in the RUCC range between 1993 and 2003 reflect methodology changes.
Figure 5.
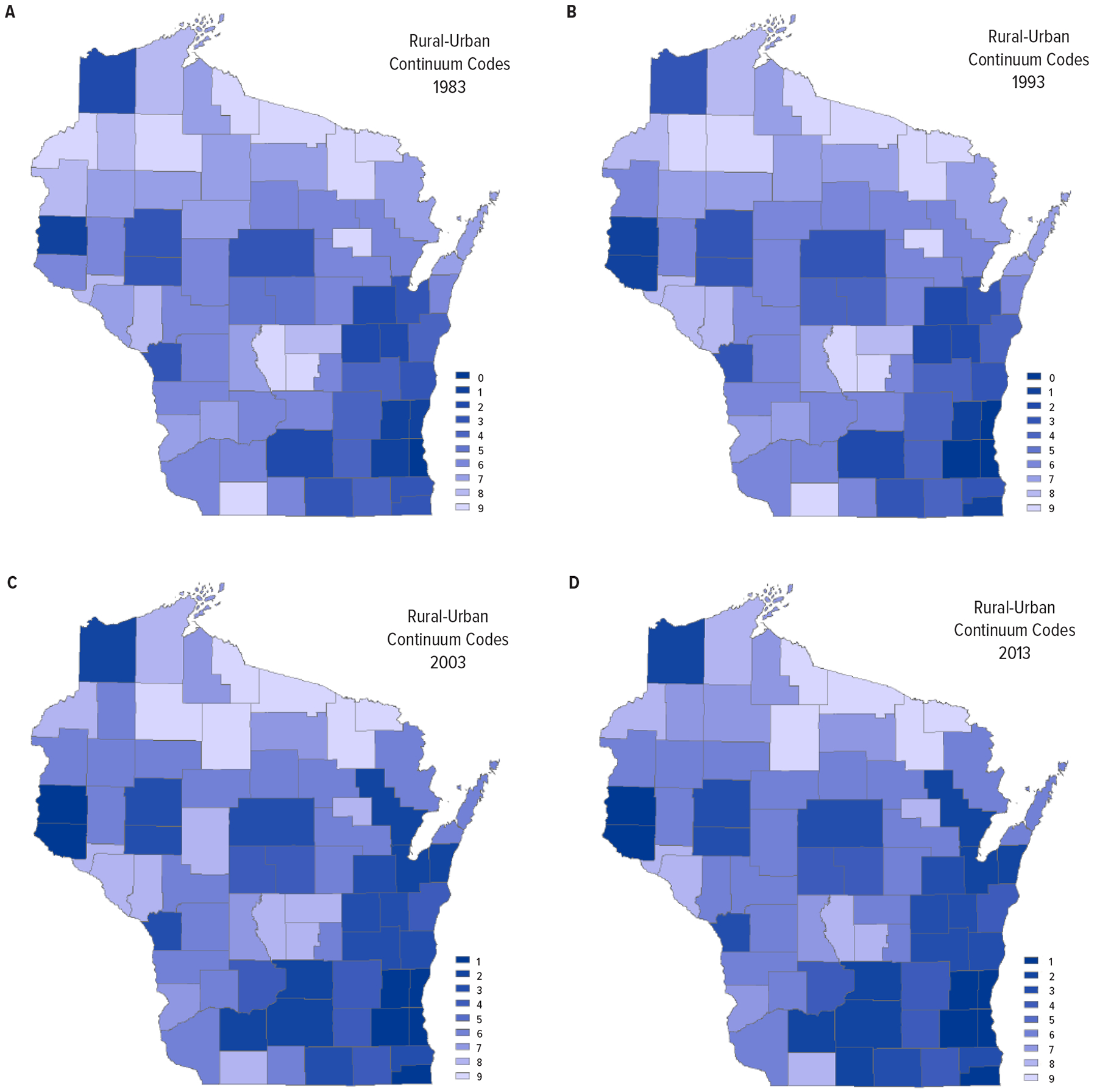
Rural-Urban Continuum Code (RUCC) Changes Across Wisconsin Over Time
Darker colors indicate more urban areas, and lighter colors indicate more rural areas. Maps are at the county level.
DISCUSSION
Categorizing Rural and Urban Communities
Indexes must categorize both rural and urban areas to accurately study the rural-urban continuum. UACE and CBSA (urban) and FAR (rural) only categorize one or the other, making them unsuitable. The remaining 6 indexes categorize across metropolitan, micropolitan, and rural areas.
Comparability of Research Based on Different Indexes
RUCC, UIC, and NCHS are county-level indexes based on OMB metropolitan and non-metropolitan definitions,21–23 making them comparable in terms of rurality research (Supplemental Table 1). UIC and NCHS further divide nonmetropolitan counties into micropolitan and rural. These 3 indexes employ different methodologies to subdivide counties within 3 categories. They also emphasize different subsets of counties; RUCC identifies 3 metropolitan levels, 4 urban levels, and 2 rural levels;21 UIC designates 7 of 12 codes as rural;22 and NCHS designates 4 of 6 codes as metropolitan.23
RUCA and RUCA(z) also stem from OMB metropolitan and nonmetropolitan categories18,20 subdivided into 2 to 4 categories across 10 primary codes and 21 secondary codes (2010 index). Some researchers create a binary variable based on the primary codes (option 1) and others group counties with a secondary code of x.1 with metropolitan counties to create a different binary variable (option 2). Due to these different methodologies, research based on binary RUCA or RUCA(z) variables may not be directly comparable. This problem is exacerbated when researchers do not disclose their method of creating a binary RUCA variable.27
The high population percent agreement between RUCC and RUCA at binary (94.9%) and ternary (88.8%) levels suggests less variability than expected. However, the percent agreement between RUCC and RUCA(z) decreased to 91.0% (binary) and 74.9% (ternary) when compared for the Registry patients (Table 2). This may be specific to this patient population or may be further evidence of RUCA(z) being a poor RUCA approximation (Figure 3). Patient-specific census tract, ZIP code, and county is necessary to further explore this question. The differences in percent agreement between national and local populations highlight that national trends may not replicate local health-system trends. Local health system geographical population trends will be highly dependent on the immediate population and area under study. Areas that match national geographical distributions more closely will be better aligned with national population data, and areas that trend more rural or urban than national geographical distributions will differ more from the national trends. Similarly, the smaller the population studied, the more variation with national trends one can expect. In our case, our relatively small catchment area may contribute to the difference in percent agreement found between indexes at the registry patient level versus the national level.
Comparing Indexes by Geographical Unit, Land Area, and Population Distributions
Indexes varied in the number of their individual codes used. Counties and land area were distributed across RUCC, though few counties are categorized as RUCC 5 (Supplemental Figures 1A and 1B), creating a natural binary division that does not follow the index’s other designations. UIC counties clustered within the urban group (Supplemental Figure 1A) and cannot be interpreted across a continuum since micropolitan (codes 3, 5, and 8) and rural categories (codes 4, 6, 7, 9, 10, 11, 12) are not sequential.22 NCHS counties clustered by its only rural category (Supplemental Figures 1A and 1C). IRR showed normal distributions across all factors considered, as it is a relative measure (Figure 1A, Supplemental Figures 1A and 1C).
Census tract and population distributions clustered in RUCA’s most urban code, due to smaller and denser tracts in more populated areas (Figure 1A, Figure 2E, Supplemental Figure 1A). Inversely, RUCA land area clustered in its most rural code (Figure 2E, Supplemental Figure 1C). RUCA(z) separated to its most urban and rural ZCTAs. Differences between the RUCA and RUCA(z) distribution suggest that RUCA(z) may not approximate RUCA (Figure 3, Supplemental Figure 1A).
National trends were magnified when viewed for Wisconsin (Figure 1B). The population distribution was spread more evenly across RUCC and UIC metropolitan codes for Wisconsin than for the US. Population distribution was almost consistent across all NCHS codes. IRR showed an urban cluster (Milwaukee metropolitan area) separating itself from the rest of Wisconsin and remained similar for RUCA in Wisconsin compared to the US. Within the Registry, patients were divided into 2 populations by RUCC and UIC and 4 populations by RUCA(z) (Figure 1C). These differences highlight how the rural-urban composition of participants may differ based on a study’s geographical reach.
Maps of Wisconsin by RUCC, UIC, NCHS, IRR, RUCA, and RUCA(z) compare across multiple land units (Figure 2). IRR and NCHS tended to homogenize rurality. IRR designated most counties as micropolitan and used few values for Wisconsin counties (Figure 2D). Due to its normal distribution, IRR draws a large distinction between the most urban and rural counties, homogenizing between those extremes. NCHS classified 32 of 72 counties into its 1 rural code, preventing distinction between patients who live in different rural communities (Figure 2C). In terms of cancer care, this homogenization of rural counties masks differences in access to care between patients who live in rural counties that are more or less densely populated or further or closer to metropolitan counties. Differences include distances patients are required to travel to receive oncology and surgical consultations, receive specialty care, and access second opinions. UIC showed divergence in rurality, though recall its codes do not sequentially identify metropolitan, micropolitan, and rural counties (Figure 2B). RUCC, RUCA, and RUCA(z) showed divergences in rurality across their respective code ranges, depicting their utility in measuring rurality across a continuum (Figures 2A, 2E, and 2F).
Index Suitability as a Continuous Variable
In moving away from binary rural-urban designations towards a rural-urban continuum, indexes must be conducive to continuous or multilevel ordinal coding. Binary rural-urban designations may mask outcome variation within groups, while continuous variables may expose nonlinear trends across the rural-urban continuum.12 As continuums become more commonly employed, a consensus index becomes important for research congruity (Table 2).
RUCC, NCHS, IRR, RUCA (option 1), and RUCA(z) (option 1) are ordinal indexes that may be coded as continuous variables. UIC does not divide its nonmetropolitan codes sequentially,22 and NCHS only designates 1 code for micropolitan counties and rural/noncore counties, respectively, restricting distinction between rurality levels.23 IRR effectively homogenizes rurality status, blurring the line between counties of different rurality on regional or local scales.
RUCA (option 2) and RUCA(z) (option 2), which includes the x.1 secondary code as metropolitan, blur the most appropriate way to order codes continuously. If RUCA and RUCA(z) are used as continuous variables, it should be based on primary RUCA codes only. RUCC includes multiple sequential codes for metropolitan, micropolitan, and rural designations, making it conducive to use as a continuous variable in analysis.
Index Feasibility to be Used in Cancer Research
The National Cancer Database, North American Association of Central Cancer Registries, and Surveillance, Epidemiology, and End Results Program registries include RUCC and RUCA indexes. RUCC is included in its original 9-code form, and RUCA is included as a binary rural-urban variable. Registry inclusion makes RUCC and RUCA accessible to researchers, though recoding RUCA into a binary variable limits its use. This recoding is to prevent case identification. Therefore, RUCC is the most accessible and specific index available for registry-based cancer research.
Counties and ZIP codes are standard fields in electronic health records; thus, researchers use county or ZIP code-based indexes. However, ZIP codes change frequently, and RUCA(z) versions are only available for noncensus years (1998, 2004, 2006, 2013).26 Researchers risk excluding cases if a patient’s ZIP code is unmatched in the chosen file. Thus, it is preferable to avoid ZIP code and ZCTA-based indexes.28 County-based indexes (RUCC) are preferred for health system and local level research.
Indexes Over Time
The hypothesized role of rurality should determine the index studied. Rurality as an exposure is calculated on a past version of an index, whereas rurality as an enabler/barrier to care should be calculated from a relevant version to the year(s) of study. When rurality is investigated as an exposure, patients may be misclassified as they move. This may obstruct the rurality designation of interest.
Absolute changes in rurality are masked by IRR’s relative nature, making this index inappropriate for longitudinal studies.
Considerations for RUCA(z) and ZCTAs
RUCA(z) is a RUCA approximation. ZCTAs approximate ZIP codes, and it is possible for a patient’s ZIP code and ZCTA to differ. ZIP codes are subject to change, as evidenced by the regular updates released by the US Postal Service, so a patient’s ZIP code at diagnosis versus year of study may differ despite not moving. The difference between RUCA and RUCA(z) geographical unit distributions across the US and Wisconsin show RUCA(z) may not approximate RUCA (Figure 3, Supplemental Figure 1A and 1B). The RUCA(z) map shows irregular ZCTA boundaries, affirming caution over using ZCTAs as a geographical unit (Figure 2F).28 Furthermore, RUCA(z) is not published by a government agency, making its ongoing availability less assured.
Limitations
We evaluated indexes for their categorization of cancer patients across the rural-urban continuum. However, we did not have access to patient-specific ZIP codes, census tracts, and counties. County, ZCTA, and census tract land area varies by state; thus, we did not evaluate land area on a per-state level. This is especially important for states with fewer and larger counties.
CONCLUSIONS
Utilizing the Rural-Urban Continuum Code (RUCC) index across cancer research will increase comparability of results. Counties are a stable geographic unit and are readily available within many data sources. RUCC includes codes across metropolitan, micropolitan, and rural communities and can be grouped into a binary or ternary variable. RUCC indexes for 1993, 2003, and 2013 are available in several national registries at a discrete level, enabling residence study across a continuum. ZCTA-based indexes should be avoided as ZCTAs approximate actual ZIP code boundaries and change frequently. Government agencies should procure a census block measure of rurality without compromising patient confidentiality. The precise unit of geographical analysis, thus minimizing masking trends. Finally, researchers should include social, economic, and health-related variables alongside rurality to understand the many factors affecting cancer disparities.
Supplementary Material
Box.
Terms and Abbreviations
| UACE | Urban Rural Classification of Urban Areas and Urban Clusters |
| CBSA | Core Based Statistical Areas |
| FAR | Frontier and Remote Area Codes |
| RUCA | Rural-Urban Commuting Area Codes |
| RUCA(z) | Aging, Independence, and Disability Rural-Urban Commuting Area Codes at the ZIP Code Tabulation Area Level |
| RUCC | Rural-Urban Continuum Codes |
| UIC | Urban Influence Codes |
| NCHS | National Center for Health Statistics Urban-Rural Classification Scheme for Counties |
| IRR | Index of Relative Rurality |
| ZCTA | ZIP Code Tabulation Area |
Acknowledgements:
The authors would like to thank the University of Wisconsin Carbone Cancer Center Pancreas Cancer Task Force for the funds to complete this project.
Funding/Support:
This project was supported by P30 CA014520 (CCSG Cancer Center Support Grant, University of Wisconsin Carbone Cancer Center), R01 CA211082 (NIH/NCI), R01 CA211082-03S1 (NIH/NCI), and the University of Wisconsin Carbone Cancer Center (UWCCC) Pancreas Cancer Task Force.
Footnotes
Ethics Approval:
The pancreas cancer registry data use was exempt as human subjects research by the University of Wisconsin Health Sciences IRB, ID # 2019–0155, expiration April 26, 2024.
Financial Disclosures:
None declared.
Appendix: Supplemental Tables and Figures are available at www.wmjonline.org
Availability of Data and Materials:
The datasets generated and/or analyzed during the current study are not publicly available due to HIPAA restrictions with personal health information for the registry patients but are available from the corresponding author on reasonable request. The other datasets analyzed are publicly available and are referenced as such in the manuscript.
REFERENCES
- 1.Pruitt SL, Eberth JM, Morris ES, Grinsfelder DB, Cuate EL. Rural-urban differences in late-stage breast cancer: do associations differ by rural-urban classification system? Tex Public Health J. 2015;67(2):19–27. [PMC free article] [PubMed] [Google Scholar]
- 2.Baldwin LM, Patel S, Andrilla CH, Rosenblatt RA, Doescher MP. Receipt of recommended radiation therapy among rural and urban cancer patients. Cancer. 2012;118(20):5100–5109. doi: 10.1002/cncr.27488 [DOI] [PubMed] [Google Scholar]
- 3.Baldwin LM, Andrilla CH, Porter MP, Rosenblatt RA, Patel S, Doescher MP. Treatment of early-stage prostate cancer among rural and urban patients. Cancer. 2013;119(16):3067–3075. doi: 10.1002/cncr.28037 [DOI] [PubMed] [Google Scholar]
- 4.Rana N, Gosain R, Lemini R, et al. Socio-demographic disparities in gastric adenocarcinoma: a population-based study. Cancers (Basel). 2020;12(1):157. doi: 10.3390/cancers12010157 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brooks GA, Tomaino MR, Ramkumar N, et al. Association of rurality, socioeconomic status, and race with pancreatic cancer surgical treatment and survival. J Natl Cancer Inst. 2023;115(10):1171–1178. doi: 10.1093/jnci/djad102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bertens KA, Massman JD 3rd, Helton S, et al. Initiation of adjuvant therapy following surgical resection of pancreatic ductal adenocarcinoma (PDAC): are patients from rural, remote areas disadvantaged? J Surg Oncol. 2018;117(8):1655–1663. doi: 10.1002/jso.25060 [DOI] [PubMed] [Google Scholar]
- 7.Ganga A, Kim EJ, Mintzer GL, et al. Disparities in primary pancreatic adenocarcinoma survival by Medicaid-status: a national population-based risk analysis. Eur J Surg Oncol. 2023;49(7):1242–1249. doi: 10.1016/j.ejso.2023.02.002 [DOI] [PubMed] [Google Scholar]
- 8.Hashibe M, Kirchhoff AC, Kepka D, et al. Disparities in cancer survival and incidence by metropolitan versus rural residence in Utah. Cancer Med. 2018;7(4):1490–1497. doi: 10.1002/cam4.1382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Meilleur A, Subramanian SV, Plascak JJ, Fisher JL, Paskett ED, Lamont EB. Rural residence and cancer outcomes in the United States: issues and challenges. Cancer Epidemiol Biomarkers Prev. 2013;22(10):1657–1667. doi: 10.1158/1055-9965.EPI-13-0404 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yaghjyan L, Cogle CR, Deng G, et al. Continuous rural-urban coding for cancer disparity studies: is it appropriate for statistical analysis? Int J Environ Res Public Health. 2019;16(6):1076. doi: 10.3390/ijerph16061076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Delavar A, Feng Q, Johnson KJ. Rural/urban residence and childhood and adolescent cancer survival in the United States. Cancer. 2019;125(2):261–268. doi: 10.1002/cncr.31704 [DOI] [PubMed] [Google Scholar]
- 12.McLafferty S, Wang F. Rural reversal? Rural-urban disparities in late-stage cancer risk in Illinois. Cancer. 2009;115(12):2755–2764. doi: 10.1002/cncr.24306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Swords DS, Mulvihill SJ, Skarda DE, et al. Hospital-level variation in utilization of surgery for clinical stage I-II pancreatic adenocarcinoma. Ann Surg. 2019;269(1):133–142. doi: 10.1097/SLA.0000000000002404 [DOI] [PubMed] [Google Scholar]
- 14.Zahnd WE, Davis MM, Rotter JS, et al. Rural-urban differences in financial burden among cancer survivors: an analysis of a nationally representative survey. Support Care Cancer. 2019;27(12):4779–4786. doi: 10.1007/s00520-019-04742-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.2010 census urban and rural classification and urban area criteria. United States Census Bureau. Published 2019. Accessed March 13, 2020. https://www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural/2010-urban-rural.html [Google Scholar]
- 16.Core based statistical areas (CBSAs), metropolitan divisions, and combined statistical areas (CSAs). United States Census Bureau. Published 2013. Accessed March 12, 2020. https://www.census.gov/geographies/reference-files/time-series/demo/metro-micro/delineation-files.html [Google Scholar]
- 17.Frontier and remote area codes. United States Department of Agriculture Economic Research Service. Published 2015. Accessed March 31, 2020. https://www.ers.usda.gov/data-products/frontier-and-remote-area-codes/
- 18.Rural-urban commuting area codes. United States Department of Agriculture Economic Research Service. Published 2019. Accessed December 19, 2019. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes/ [Google Scholar]
- 19.RUCA data: ZIP code RUCA approximation. WWAMI Rural Health Research Center. Published 2007. Accessed December 19, 2019. https://depts.washington.edu/uwruca/ruca-approx.php [Google Scholar]
- 20.Rural-urban commuting area (RUCA) codes, zip code file: version 3.10. Administration for Community Living: AGing, Independence, and Disability Program. Published 2013. Accessed March 31, 2020. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes/ [Google Scholar]
- 21.Rural-urban continuum codes. United States Department of Agriculture Economic Research Service. Published 2013. Accessed December 13, 2019. https://www.ers.usda.gov/data-products/rural-urban-continuum-codes/ [Google Scholar]
- 22.Urban influence codes. United States Department of Agriculture Economic Research Service. Published 2013. Accessed December 13, 2019. https://www.ers.usda.gov/data-products/urban-influence-codes/ [Google Scholar]
- 23.NCHS urban-rural classification scheme for counties. National Center for Health Statistics. Published 2017. Accessed March 13, 2020. https://www.cdc.gov/nchs/data_access/urban_rural.htm [Google Scholar]
- 24.Waldorf B, Kim A. The Index of Relative Rurality (IRR): US county data for 2000 and 2010. Purdue University Research Repository. April 18, 2018. Accessed April 1, 2024. https://purr.purdue.edu/publications/2960/1 [Google Scholar]
- 25.Waldorf B, Kim A. Defining and Measuring Rurality in the US: From Typologies to Continuous Indices. Department of Agricultural Economics, Purdue University; 2015. Accessed April 1, 2024. http://sites.nationalacademies.org/cs/groups/dbassesite/documents/webpage/dbasse_168031.pdf [Google Scholar]
- 26.United States Summary: 2010, Population and Housing Unit Counts: 2010 Census of Population and Housing. US Census Bureau; 2012. Accessed April 1, 2024. https://www2.census.gov/library/publications/decennial/2010/cph-2/cph-2-1.pdf [Google Scholar]
- 27.Freeman AT, Kuo M, Zhou L, et al. Influence of treating facility, provider volume, and patient-sharing on survival of patients with multiple myeloma. J Natl Compr Canc Netw. 2019;17(9):1100–1108. doi: 10.6004/jnccn.2019.7298 [DOI] [PubMed] [Google Scholar]
- 28.Krieger N, Waterman P, Chen JT, Soobader MJ, Subramanian SV, Carson R. Zip code caveat: bias due to spatiotemporal mismatches between zip codes and US census-defined geographic areas--the Public Health Disparities Geocoding Project. Am J Public Health. 2002;92(7):1100–1102. doi: 10.2105/ajph.92.7.1100 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to HIPAA restrictions with personal health information for the registry patients but are available from the corresponding author on reasonable request. The other datasets analyzed are publicly available and are referenced as such in the manuscript.