

Abstract
Background There is no normative study of transregional grip strength data available from India. Hence, a multicenter study is designed to obtain reference value.
Materials and Methods This is a prospective observational study conducted as a part of the Indian normative data project of the Indian Society for Surgery of the Hand. The study included three participating centers: one from the northern part and two from the southern part. Certified calibrated Jamar dynamometer and Jamar pinch gauge were used to measure the grip strength, key pinch strength, tip pinch strength, and tripod pinch strength as per the guidelines of the American Society of Hand Therapists.
Results A total of 1,019 volunteers in the age group of 18 to 60 years were studied. The mean grip strength in males and females was 38.18 and 24.06 kg, respectively. The mean key pinch strength was 8.52 kg in males and 5.97 kg in females. The mean tip pinch strength was 4.86 kg in males and 3.59 kg in females. The mean tripod pinch strength was 5.41 kg in males and 4.16 kg in females.
Conclusions All four strengths were lower in value when compared with American and other populations. The men had more strength than women. There was no relation to hand dominance. There was a correlation for age and height but no correlation with body mass index (BMI).
Keywords: grip strength, key pinch strength, tip pinch strength, tripod pinch strength, normative data, reference values
Introduction
The grip strength and pinch strength are the most important quantitative assessments for the function of the hand as a whole. They play a role in diagnosing a hand disorder when there is a discrepancy in comparison with the contralateral hand strength. They help in assessing the progress in recovery after surgery and therapy. Moreover, hand grip strength is a health indicator for frailty and risk of disability among the elderly, allowing early risk identification and intervention. 1 These form the important outcome measure following therapeutic intervention.
The grip strength and pinch strength are affected by various factors including ethnicity. 2 The reference value of one population cannot be held as good for another population. The purpose of this study is to derive age- and gender-wise normative data for grip strength and pinch strength in the Indian population.
Materials and Methods
The study included 1,019 volunteers aged 18 to 60 years. In this multicentric study, involving three tertiary care centers, 200 volunteers participated from Tamil Nadu, 200 volunteers participated from Karnataka, and 619 volunteers participated from Chandigarh. The volunteers in the age group of 18 to 60 years who were willing to participate in the study were included. Informed consent was taken from all participants. Institutional ethics committees of all three participating hospitals approved the study. The volunteers comprised patient attendees, students, nursing staff, and security and housekeeping personnel. Volunteers who had any history of injury to the hand, pain or numbness in the hand, diabetes, acute edematous, vascular, or inflammatory condition of the hand were excluded as these factors might reduce the grip strength.
The demographic data collected were name, age, gender, hand dominance, height in centimeters, and weight in kilograms. Power grip strength was measured using a Jamar dynamometer and pinch strengths were measured using a Jamar pinch gauge. The equipment of all three centers was calibrated before the start of the study and recalibrated when needed.
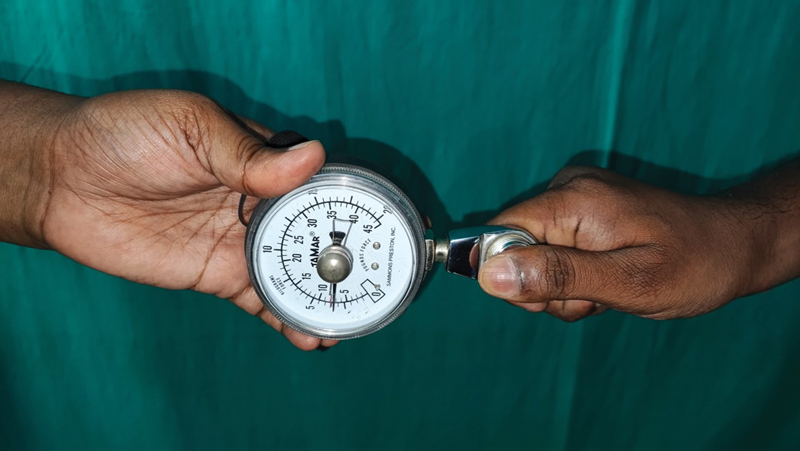
The strengths were measured as per the American Society of Hand Therapists 3 recommendations. The procedure was explained to the volunteer and was seated on a chair without arms with the feet flat on the floor. The shoulder was kept in adduction and neutral rotation, the elbow in 90-degree flexion, the forearm in the neutral position, wrist between 0 and 30 degrees of extension, and 0 to 15 degrees of ulnar deviation ( Figs. 1 and 2 ).
Fig. 1.

Position to measure grip strength.
Fig. 2.
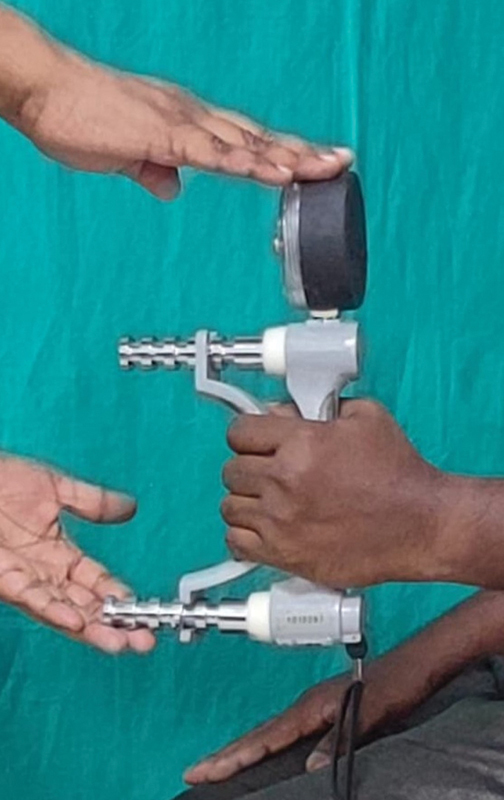
Jamar dynamometer is set in the second handle and supported by the examiner.
Grip strength: The dynamometer was set at the position of the second handle and the equipment was stabilized by the examiner.
Key pinch strength (lateral pinch strength): Thumb pulp to lateral aspect of the proximal interphalangeal joint of the index finger, and the other three fingers flexed ( Fig. 3 ).
Fig. 3.
Key pinch (lateral pinch).
Tip pinch strength: Thumb pulp to index pulp, and the other three fingers flexed ( Fig. 4 ).
Fig. 4.

Tip pinch.
Tripod pinch strength (chuck pinch strength/palmar pinch strength): Thumb pulp to index and middle pulp, and the other two fingers flexed ( Fig. 5 ).
Fig. 5.

Tripod pinch (chuck pinch or palmar pinch).
Three consecutive measurements were taken for all measurements and the mean was calculated and recorded. 4 The data collected from the three tertiary care centers were analyzed by the corresponding author.
Statistical Analysis
The mean, median, and standard deviation were calculated for all continuous data. Percentage was computed for all categorical data. Independent t -tests for two groups and one-way analysis of variance (ANOVA) tests for more than two groups were done to find significant differences. Correlation analysis was done using the Pearson correlation test. SPSS version 20 was used and p -value less than 0.05 was considered significant.
Results
A total of 1,019 volunteers were examined. Grip strength and key pinch strength were recorded in all the volunteers. Tip pinch strength and tripod pinch strength were recorded in 400 volunteers. The average age of the participants was 37.73 years (range: 18–60 years). Of these volunteers, 510 were females and 509 were males. Their strengths are depicted in Table 1 .
Table 1. Gender-wise mean value of grip and pinch strengths.
| Strength | Men ( n = 509) | Women ( n = 510) | ||||
| Mean (kg) | Standard deviation | Standard error, mean | Mean (kg) | Standard deviation | Standard error, mean | |
| Grip strength, right | 38.77 | 8.40 | 0.37 | 24.81 | 8.67 | 0.38 |
| Grip strength, left | 37.59 | 7.74 | 0.34 | 23.31 | 8.09 | 0.36 |
| Key pinch, right | 8.77 | 2.63 | 0.12 | 6.23 | 1.99 | 0.09 |
| Key pinch, left | 8.26 | 2.49 | 0.11 | 5.72 | 1.91 | 0.08 |
| Strength | Men ( n = 200) | Women ( n = 200) | ||||
| Mean (kg) | Standard deviation | Standard error, mean | Mean (kg) | Standard deviation | Standard error, mean | |
| Tip pinch, right | 5.01 | 1.40 | 0.09 | 3.73 | 1.16 | 0.08 |
| Tip Pinch, left | 4.72 | 1.43 | 0.10 | 3.45 | 1.22 | 0.09 |
| Tripod pinch, right | 5.58 | 1.42 | 0.10 | 4.45 | 1.75 | 0.12 |
| Tripod pinch, left | 5.23 | 1.41 | 0.10 | 3.87 | 1.19 | 0.08 |
The mean grip strength in males was 38.18 kg and the mean grip strength in females was 24.06 kg. The mean key pinch strength in males was 8.52 kg and the mean key pinch strength in females was 5.97 kg. The mean tip pinch strength in males was 4.86 kg and the mean tip pinch strength in females was 3.59 kg. The mean tripod pinch strength in males was 5.41 kg and the mean tripod pinch strength in females was 4.16 kg. All four strengths were more in men and it was statistically significant.
The participants were further subdivided into five groups based on age: (1) 18 to 20 years, (2) 21 to 30 years, (3) 31 to 40 years, (4) 41 to 50 years, and (5) 51 to 60 years. The mean value of strengths in the age group is depicted in Table 2 . The grip strength and key pinch strength were maximum in the 18- to 20-year age group and they were statistically significant. The tip pinch strength was maximum in the age group of 41 to 50 years and the tripod pinch strength was maximum in the 21- to 30-year age group, but both were not statistically significant.
Table 2. Age-wise distribution of the mean of strengths recorded in kilogram.
| Age group & n (no. of hands) | Grip strength (kg) | Key pinch strength (kg) | Age group & n (no. of hands) | Tip pinch strength (kg) | Tripod pinch strength (kg) |
|---|---|---|---|---|---|
| 18–20 ( n = 86) | 35.80 | 8.77 | 18–20 ( n = 0) | 0 | 0 |
| 21–30 ( n = 568) | 32.28 | 7.29 | 21–30 ( n = 400) | 4.07 | 4.88 |
| 31–40 ( n = 566) | 31.21 | 7.41 | 31–40 ( n = 400) | 4.29 | 4.64 |
| 41–50 ( n = 396) | 28.89 | 6.75 | 41–50 ( n = 400) | 4.31 | 4.87 |
| 51–60 ( n = 422) | 30.54 | 7.09 | 51–60 ( n = 400) | 4.23 | 4.73 |
The left hand was found to be dominant in 7.26% (74 persons) participants. The mean value of strengths as per handedness is depicted in Table 3 . In right-handed individuals, the grip, key pinch, tip pinch, and tripod pinch strengths were higher in the dominant hand, but it was not statistically significant ( p > 0.05). In left-handed individuals, the grip strength and key pinch strength were higher in their dominant hand and the tip pinch and tripod pinch strengths were higher in the nondominant hands. However, the variations of strength due to handedness were not statistically significant. On comparing the dominant side for grip strength, it was more in the left-handed individuals, but the difference was not statistically significant. The right-handed individuals when compared with left-handed individuals had more key pinch, tip pinch, and tripod pinch strengths in their dominant hand, but the difference was not statistically significant ( p > 0.05).
Table 3. Strength as per the handedness (strength in kilogram).
| n (no. of persons) | Grip strength (kg) | Key pinch strength (kg) | n (no. of persons) | Tip pinch strength (kg) | Tripod pinch strength (kg) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| D | ND | D | ND | D | ND | D | ND | ||||
| Right-handed | 945 | 31.86 | 30.27 | 7.54 | 6.96 | Right-handed | 382 | 4.40 | 4.10 | 4.99 | 4.56 |
| Left-handed | 74 | 32.65 | 30.79 | 7.36 | 6.93 | Left-handed | 18 | 3.74 | 3.80 | 4.38 | 5.34 |
Abbreviations: D, dominant hand; ND, nondominant hand.
The strengths based on occupation are depicted in Table 4 . All strengths were more in skilled job occupations when compared and were statistically significant.
Table 4. Strengths based on occupation.
| Occupation | n | Grip strength (kg) | Key pinch strength (kg) | n | Tripod pinch strength (kg) | Tip pinch strength (kg) |
|---|---|---|---|---|---|---|
| Administrator | 10 | 33.833 | 6.017 | 10 | 4.933 | 4.4585 |
| Agriculturist | 15 | 31.066 | 7.621 | 15 | 5.7895 | 4.947 |
| Business | 10 | 27.574 | 6.665 | 10 | 4.2145 | 3.9645 |
| Clerical job | 37 | 28.3975 | 7.0465 | 37 | 5.073 | 4.4605 |
| Homemaker | 58 | 22.963 | 5.862 | 58 | 4.706 | 3.908 |
| Nurse | 47 | 21.87 | 5.1785 | 47 | 4.4555 | 3.887 |
| Physiotherapist | 29 | 24.8335 | 6.768 | 29 | 4.8045 | 4.0015 |
| Professional | 3 | 35.7775 | 7.111 | 3 | 7.028 | 5.5555 |
| Skilled Job | 296 | 36.058 | 9.076 | 59 | 4.374 | 4.2605 |
| Student | 62 | 22.8945 | 5.6505 | 62 | 4.5625 | 3.847 |
| Unskilled Job | 61 | 29.2545 | 6.366 | 61 | 5.1595 | 4.8605 |
| White collar | 391 | 31.995 | 6.786 | 9 | 5.3725 | 4.361 |
| Total | 1,019 | 400 |
The mean height was 161.14 cm and the standard deviation was 10.27. The mean weight was 63.41 kg and the standard deviation was 11.15. There was a significant positive correlation between height and weight for all four strengths as depicted in Table 5 . The average body mass index (BMI) was 24.36 kg/m 2 (range: 14.45–43.57 kg/m 2 ). There was a weak correlation between age and BMI for all four strengths and it was significant for key pinch strength alone.
Table 5. Correlation analysis of strengths with weight, height, body mass index (BMI), and age.
| Correlation analysis | r -Value | |||
|---|---|---|---|---|
| Height (cm) | Weight (kg) | BMI (kg/m 2 ) | Age (y) | |
| Grip strength, right | 0.473 | 0.305 | –0.0603 | –0.0429 |
| Grip Strength, left | 0.49 | 0.33 | –0.0439 | –0.042 |
| Key pinch, right | 0.347 | 0.158 | –0.133 | 0.0757 |
| Key pinch, left | 0.345 | 0.161 | –0.124 | –0.0659 |
| Tripod pinch, right | 0.203 | 0.168 | 0.0476 | –0.0292 |
| Tripod pinch, left | 0.345 | 0.23 | 0.0169 | –0.0185 |
| Tip pinch, right | 0.304 | 0.275 | 0.0941 | 0.0741 |
| Tip pinch, left | 0.297 | 0.246 | 0.0691 | 0.0412 |
Discussion
Surgery of the hand addresses not only the removal or rectification of the problem but also the betterment of hand function. Measurements of grip and pinch strengths give visual feedback to the patient, thereby encouraging them to undergo therapy well. Also, the nominal value of grip strength and pinch strength allows the therapist and surgeon to compare and infer the present condition and the future progress. Apart from this, hand grip strength is correlated with diabetes, chronic anemia, dyslipidemia, cardiovascular diseases, and male cancer. 5 6 A low hand grip strength is an indicator of frailty and risk of disability among the elderly and allows early risk identification and intervention. 1 The usage of percentile from the normative value of hand grip strength to diagnose sarcopenia adds more importance to the study of a normative value. 6 7
Although there are few studies from India, they have limitations like measuring in the standing position, 8 less age group range, 9 10 female gender alone, 11 12 and of the same region. 8 13 It has been established that grip strength was higher for individuals who stood than for those who sat in a chair and in individuals with a 90-degree flexed elbow than in those with an extended elbow. 14 Also, in many studies grip strength alone was measured. In our study, participants were recruited from three states and the strength measurements were taken as per the recommendation of the American Society of Hand Therapists in calibrated machines. To our knowledge, this is the first study to include participants from different regions of the country.
The hand grip strengths and pinch strengths of the study population were lower than those of the American and European populations. This finding is similar to that of previous studies from Asia. 1 2 8 15 In the present study, the mean grip strength is 38.18 kg in males and 24.06 kg in females, when compared with the mean grip strength of 44.77 kg in males and 26.47 kg in females in the United States 16 and the mean grip strength of 44.62 kg in males and 27.17 kg in females in the United Kingdom. 3 Of pinch strengths measured, key pinch strength was the highest, followed by tripod strength and tip strength, respectively, which is in accordance with many reported studies 3 16 except for the study done by Shaheen et al who reported a higher tripod pinch strength. 17 Most of the studies ignored the hand dominance as the left-hand dominance was less than 10% 16 and reported as the mean of the strength. In the present study, we followed the same criteria.
Previous studies have shown that men have more power in all four strengths compared with women 3 16 and the present study's inference is the same. Most of the studies showed that the hand strengths either increased with increasing age 18 19 20 having a linear inverse relationship or peaked somewhere between 25 and 50 years and decreased thereafter 3 16 21 having a curvilinear relationship. The present study did not fall under either category and showed that the grip strength declined with increasing age and showed an increase in strength in the 51- to 60-year age group. Key pinch strength also showed a similar pattern. A possible explanation for this could be exclusion of participants with diabetes and the fact that most of the participants were working, hence representing the healthier set of people in that age group. In the present study, the change in tip pinch strength and tripod pinch strength with age was not statistically significant.
The left hand was the dominant hand in 7.26% of the participants. Left-hand dominance was 9.4% in Saudi Arabia, 5 7% in Malaysia, 6 11% in Greece, 10% in Australia, 7 7% in one study from the United States, 8 and 18% in another study from the United States. 9 Similar to other studies, there was no statistically significant association with handedness.
Participants doing skilled jobs had more strength than those in other jobs. We were not able to infer a more meaningful relationship with job as the physical demands of each person were not categorized. Many studies found that with increasing levels of occupational and hobby-related demands, the strengths also increased. 22 23
In the present study, there is a significant correlation between height and weight and a weak correlation with BMI. Similar results were seen in the study by Kamarul et al 15 and Anjum et al. 2
The limitation of the study is that though occupation has been taken into account, the nature of occupation was not segregated based on the scale of physical demand. Also, hobbies and measurement of palm width and upper limb were not recorded and analyzed.
Conclusion
This multicentric study provides reference data for grip and pinch strengths in the Indian population. It can be used as a reference value for diagnosing disease and quantifying prognosis or risk. It will play a great role in the rehabilitation of the hand in the Indian population.
Acknowledgments
The authors would like to acknowledge Dr. Senthilvadivu for her help in statistical analysis. We would like to acknowledge hand therapists Ms. Sandhiya Jaichandran and Mr. Venubabu from the corresponding author's institute. We would like to thank the members of the Indian Society for Surgery of the Hand and the Normative Data Research Group of ISSH for their support and guidance.
Funding Statement
Funding None.
Conflict of Interest None declared.
Institutional Review Board Approval
Institutional review board clearance was obtained for the study individually at three participating centers where the study was performed and the study protocols conformed to the Declaration of Helsinki.
Authors' Contributions
Su.R. was the Principal Investigator for the project as a whole and for the project in Tamil Nadu, and also contributed to data collection and writing of the manuscript. M.P.G. was the Principal Investigator for the project in Karnataka and contributed to data collection. V.V. was the Principal Investigator for the project in Chandigarh and contributed to data collection. Sr.R. and S.G. provided logistical support and contributed to editing of the manuscript. A.B. contributed to designing the methodology and editing the manuscript, and was the coordinator of the ISSH Normative data project. M.T. was a patron of the ISSH Normative data project and contributed to editing the manuscript.
References
- 1.Lam N W, Goh H T, Kamaruzzaman S B, Chin A V, Poi P J, Tan M P. Normative data for hand grip strength and key pinch strength, stratified by age and gender for a multiethnic Asian population. Singapore Med J. 2016;57(10):578–584. doi: 10.11622/smedj.2015164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Anjum S N, Choudary P, Dimri R, Ankarath S. Comparative evaluation of grip and pinch strength in an Asian and European population. Hand Ther. 2012;17:11–14. [Google Scholar]
- 3.Gilbertson L, Barber-Lomax S. Power and pinch grip strength recorded using the hand-held Jamar® Dynamometer and B+L hydraulic pinch gauge: British Normative Data for Adults. Br J Occup Ther. 1994;57:483–488. [Google Scholar]
- 4.Mathiowetz V. Effects of three trials on grip and pinch strength measurements. J Hand Ther. 1990;3:195–198. [Google Scholar]
- 5.Li S, Zhang R, Pan G, Zheng L, Li C. Handgrip strength is associated with insulin resistance and glucose metabolism in adolescents: evidence from National Health and Nutrition Examination Survey 2011 to 2014. Pediatr Diabetes. 2018;19(03):375–380. doi: 10.1111/pedi.12596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lee S Y. Handgrip strength: an irreplaceable indicator of muscle function. Ann Rehab Med. 2021;45:167–169. doi: 10.5535/arm.21106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chen L K, Woo J, Assantachai P et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(03):300–30700. doi: 10.1016/j.jamda.2019.12.012. [DOI] [PubMed] [Google Scholar]
- 8.Mullerpatan R P, Karnik G, John R. Grip and pinch strength: normative data for healthy Indian adults. Hand Ther. 2013;18:11–16. [Google Scholar]
- 9.Vishwanath S, Vishal K. Normative data of grip and pinch strengths in healthy adults of Indian population. Indian J Physiother Occup Ther. 2021;15(03):178–183. [Google Scholar]
- 10.Koley S, Melton S A. Age-related changes in handgrip strength among healthy Indian males and females aged 6-25 years. J Life Sci. 2010;2:73–80. [Google Scholar]
- 11.Koley S, Kaur N, Sandhu J S. A study on hand grip strength in female labourers of Jalandhar, Punjab, India. J Life Sci. 2009;1(01):57–62. [Google Scholar]
- 12.Kaur M. Age-related changes in hand grip strength among rural and urban Haryanvi Jat females. Homo. 2009;60(05):441–450. doi: 10.1016/j.jchb.2009.06.002. [DOI] [PubMed] [Google Scholar]
- 13.Walankar P, Verma C, Mehta A, Author C. Study of hand grip strength in Indian population. Int J Health Sci Res. 2016;6:11. [Google Scholar]
- 14.Balogun J A, Akomolafe C T, Amusa L O. Grip strength: effects of testing posture and elbow position. Arch Phys Med Rehabil. 1991;72(05):280–283. [PubMed] [Google Scholar]
- 15.Kamarul T, Ahmad T S, Loh W Y. Hand grip strength in the adult Malaysian population. J Orthop Surg (Hong Kong) 2006;14(02):172–177. doi: 10.1177/230949900601400213. [DOI] [PubMed] [Google Scholar]
- 16.Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, Rogers S. Grip and pinch strength: normative data for adults. Arch Phys Med Rehabil. 1985;66(02):69–74. [PubMed] [Google Scholar]
- 17.Shaheen A AM, Omar M TA, Ali O I. Normative values of handgrip and pinch strengths in healthy female college students in Riyadh, Saudi Arabia: a cross-sectional study. Bull Fac Phys Ther. 2021;26:1. [Google Scholar]
- 18.Kellor M, Frost J, Silberberg N, Iversen I, Cummings R. Hand strength and dexterity. Am J Occup Ther. 1971;25(02):77–83. [PubMed] [Google Scholar]
- 19.Thorngren K G, Werner C O. Normal grip strength. Acta Orthop Scand. 1979;50(03):255–259. doi: 10.3109/17453677908989765. [DOI] [PubMed] [Google Scholar]
- 20.Schmidt R T, Toews J V. Grip strength as measured by the Jamar dynamometer. Arch Phys Med Rehabil. 1970;51(06):321–327. [PubMed] [Google Scholar]
- 21.Fraser C, Benten J. A study of adult hand strength. Br J Occup Ther. 1983;46(10):296–299. [Google Scholar]
- 22.Werle S, Goldhahn J, Drerup S, Simmen B R, Sprott H, Herren D B. Age- and gender-specific normative data of grip and pinch strength in a healthy adult Swiss population. J Hand Surg Eur Vol. 2009;34(01):76–84. doi: 10.1177/1753193408096763. [DOI] [PubMed] [Google Scholar]
- 23.Crosby C A, Wehbé M A, Mawr B. Hand strength: normative values. J Hand Surg Am. 1994;19(04):665–670. doi: 10.1016/0363-5023(94)90280-1. [DOI] [PubMed] [Google Scholar]