

Abstract
Some children socially transition genders by changing their pronouns (and often names, hairstyles, clothing) from those associated with their assigned sex at birth to those associated with their gender identity. We refer to children who have socially transitioned as transgender children. In a prospective sample of children who socially transitioned during childhood (at or before the age of 12; Mage of transition = 6.82), we tested whether the parent-reported internalizing symptoms of transgender children were different before vs. after they socially transitioned. The children were predominantly white (70.6% white) and girls (76.5% transgender girls, 23.5% transgender boys). Their parents tended to have high levels of education (74.5% Bachelor’s degree or above) and lived in families with high household incomes (62.7% with household incomes of $75,000 or above). On average, youth showed lower levels of internalizing symptoms after socially transitioning vs. before, suggesting a possible mental health benefit of these transitions.
Social transitions describe the nonmedical process of changing one’s pronouns, and often name, hairstyle, clothing, etc., in order to live as a different gender than the one assigned at birth (Gülgöz et al., 2019; Kuvalanka et al., 2017). Children who have made social transitions can be described as transgender children. Some authors have hypothesized that making a social transition may benefit mental health in children who express the desire to do so (Sherer, 2016; Turban & Ehrensaft, 2018). This potential benefit is difficult to test methodologically, given that random assignment cannot be used to examine the outcomes of social transitions (i.e., it would not be ethical to randomly assign children to transition, or not; not all gender diverse children wish to socially transition). The next best option is to prospectively follow a group of gender diverse children—who have not, at least initially—socially transitioned and then observe levels of psychopathology over time in the youth who socially transition. In the present work, we report on the first such prospective study, in which we examine anxiety and depression symptoms in transgender youth before and after they made binary social transitions (youth who adopted the binary gendered pronouns “opposite” their assigned sex at birth) in childhood, at age 12 or younger.
There are a variety of ways that childhood social transitions could impact internalizing psychopathology. Social transitions might reduce levels of anxiety and depression, as living and being regarded by others as the gender with which you identify, in itself, may enhance wellbeing and reduce distress (Sherer, 2016; Turban, 2017). Another reason childhood social transitions could plausibly reduce psychopathology is that they may be a marker of, and/or a key way to confer, family support for a child’s gender identity. Family support for one’s LGBT identity has been shown to be associated with lower levels of psychopathology in samples of LGBT youth (Pariseau et al., 2019; Ryan et al., 2010), as well as in transgender children specifically (Durwood et al., 2021).
On the other hand, it is also possible that social transitions in childhood have no impact on internalizing symptoms, or could even result in an increase in internalizing symptoms. For children who are fully supported in their gender expressions, transition-related reductions in internalizing symptoms may be unlikely. Further, some children may experience new stressors after transitioning, such as bullying and/or discrimination, which could offset any benefits of the transition itself. In line with this idea, LGBT adults show elevated levels of internalizing psychopathology due to minority stress (Bockting et al., 2013; Hatzenbuehler, 2009; Pellicane & Ciesla, 2022), and some data indicates that gay men who have recently come out are more likely to have anxiety or depression diagnoses than closeted men (Pachankis et al., 2015). Additionally, it is possible that any potential benefits of a social transition simply appear in domains other than anxiety and depression symptoms, such as in the realms of self-esteem, feelings of belongingness, performance at school, or life satisfaction.
Some empirical evidence is consistent with social transitions either improving, or having no effect on a child’s mental health, though this work has all been cross-sectional. A handful of studies of internalizing symptoms in socially-transitioned transgender youth have reported normative levels of depression and normative or only slightly elevated levels of anxiety (Durwood et al., 2017; Gibson et al., 2021; Kuvalanka et al., 2017; Olson et al., 2016). Some other studies have compared binary, socially transitioned children to gender-diverse children who have not made binary social transitions. The findings in this literature are mixed, with some work suggesting fewer internalizing symptoms in gender diverse children who have (vs. have not) socially transitioned (Kuvalanka et al., 2017), and other work showing no differences between groups (Morandini et al., 2023; Sievert et al., 2021; Wong et al., 2019). While comparing internalizing symptoms in gender diverse children who have vs. have not made binary social transitions lends some insight, these findings are also challenging to interpret, as the two groups being compared may systematically differ in meaningful ways besides social transition status; for example, youth who have not transitioned may differ from youth who have transitioned in terms of how they identify (whether they identify as transgender or not), aspects of their social context, etc. Supporting this possibility, one qualitative study suggested that many gender diverse youth who have not socially transitioned simply did not want to according to their parents (Olson et al., 2019), and a prospective study found that gender diverse children who later went on to socially transition showed more “cross-sex” identification and preferences than did gender diverse youth who did not go on to transition, suggesting these are distinct groups of youth (Rae et al., 2019). This work suggests simple comparisons between children who have vs. have not socially transitioned in childhood are difficult to interpret because the groups might differ in many other important ways. Despite the limitations of existing work, those findings suggest that social transitions in gender diverse children may reduce, or have no effect on, psychopathology.
In the present work, we report the first prospective data comparing the anxiety and depression symptoms of 51 youth before vs. after making childhood social transitions.
Transparency and Openness
This study was not preregistered. Code and data are provided here https://osf.io/rjxp6/. Because of identifiability concerns, shared files do not include (a) demographic information or (b) information about which youth retransitioned. Supplemental Materials for this paper are posted on the journal’s website. We report in this paper how we determined our sample size, all data exclusions, and all measures in the study. As this is an observational study, there were no manipulations. This work was approved by the Institutional Review Boards of the University of Washington and Princeton University and adhered to the Declaration of Helsinki’s 2008 Sixth Revision.
Methods
Participants.
Participants in this study are parents of gender diverse youth who were asked to report on anxiety and depression symptoms in their children. Both the parents and their children are part of a large, national, longitudinal study of North American gender diverse youth and their families, which began in 2013. This study recruited families of gender diverse children who had not made a binary social transition by the time of their first visit, N = 142 (if they used the binary pronouns “opposite” their assigned sex at the time of their first visit, they were recruited for a separate longitudinal study of binary transgender youth; Gülgöz et al., 2019). Parents were recruited to the study via support groups, conferences, and camps for gender diverse youth, as well as through clinicians, word-of-mouth, internet searches, and through media stories. Parents are only included in the study if their child was willing to participate in an initial study session (at some later points, parents were asked to participate without simultaneous youth participation). Youth needed to be between the ages of 3 and 12 at their first participation for families to participate. The recruitment period for the larger longitudinal sample took place between July 2013 and February 2020. Data collection for the present analyses (i.e., our cut-off date) ended on July 1st, 2021.
Of the 142 gender diverse youth in the longitudinal study, our primary group of interest are the 51 youth who made binary social transitions at or before the age of 12, during their participation in our study. We defined binary social transitions as youth having changed their pronouns to those stereotypically associated with the binary gender “opposite” their assigned sex at birth (e.g., for assigned male children, adopting “she/her” pronouns, and for assigned female children, adopting “he/him” pronouns) across contexts. If youth changed their pronouns first in certain contexts (e.g., at home) and later in other contexts (e.g., at school), we considered the later of those times the age at which they socially transitioned. Of the 51 youth who made binary social transitions, three had gone on to have another social transition (i.e., changed pronouns again, here called “retransitioning,” Olson et al., 2022) by our cut-off date. Because these retransition trajectories could be related to how one responds to an initial social transition, we include analyses both retaining and excluding these three retransitioners. Demographics for the central analytic sample are shown in Table 1.
Table 1.
Demographics of Main Sample.
| N = 51 | |
|---|---|
|
| |
| Child Gender (after transition) | n (%) |
| Girl | 39 (76.5%) |
| Boy | 12 (23.5%) |
| Child Race | |
| Asian | 2 (3.9%) |
| Black | 1 (2.0%) |
| Multiracial | 8 (15.7%) |
| White, Hispanic | 4 (7.8%) |
| White, non-Hispanic | 36 (70.6%) |
| Parent 1 Highest Level of Education | |
| High School Diploma | 2 (3.9%) |
| Some college/Associate’s degree | 9 (17.6%) |
| College/Bachelor’s degree | 12 (23.5%) |
| Advanced degree (MA, MD, etc.) | 26 (51.0%) |
| Unknown | 2 (3.9%) |
| Geographic Region of the United States, or Canada | |
| Midwest | 12 (23.5%) |
| Northeast | 6 (11.8%) |
| South | 10 (19.6%) |
| West | 22 (43.1%) |
| Canada | 1 (2.0%) |
| Annual Family Income | |
| less than $25,000 | 1 (2.0%) |
| $25,001-$50,000 | 8 (15.7%) |
| $50,001-$75,000 | 10 (19.6%) |
| $75,001-$125,000 | 15 (29.4%) |
| greater than $125,000 | 17 (33.3%) |
Note: Income and education were determined by the first available response.
Procedure.
Parents were periodically invited to participate in the longitudinal study via an in-person visit, virtual visit, or online survey once approximately every 1–2 years, though not all parents participated every time they were invited.1 Parents were compensated for each participation, between $5-$20 depending on the duration of the participation. All parents provided consent.
The mean transition age was 6.82 years, with the youngest transition at age 3 and the oldest at age 12 (age at first visit ranged from 3–11, M = 6.18). Per child, the average number of visits at which internalizing symptoms were reported by a parent was 4.73 (range from 2 to 8). Parents of 46 children (90%) reported on their children’s mental health at three or more visits. Of the 241 total time points with mental health data reported by parents, 78 (32%) were before the child’s social transition was completed (Mvisits before transition = 1.5, range 1–4), and 163 (68%) were after transition (Mvisits after transition = 3.2, range 1–7).
Measures.
Parents reported on their child’s anxiety and depression symptoms, using the NIH Patient-Reported Outcomes Measurement Information System (PROMIS) parent proxy scales for Anxiety and Depression (Anxiety Short Form 8a v2.0; Depressive Symptoms Short Form 6a v2.0; forms in English; Anxiety: A Brief Guide to the PROMIS Anxiety Instruments, 2019; Depression: A Brief Guide to the PROMIS Depression Instruments, 2019; Irwin et al., 2012; Varni et al., 2012; Varni, Thissen, et al., 2014). These scales ask parents to report on the youth’s anxiety and depression symptoms in the past 7 days. Example items from the parent scales include, “My child felt nervous,” and “My child felt sad.” Parents selected responses from a 5-point Likert scale of responses: “never,” “almost never,” “sometimes,” “often,” and “almost always.” We used summed score conversion to determine t-scores, with 50 representing the middle score in a reference sample (Varni et al., 2014; missing items, which were exceedingly rare, were replaced with the parent’s mean response on the rest of the short form items).
However, we note that these short forms were developed for parents of children aged 5–17, while 28 of our visits included data about children aged 3 or 4 (13 children transitioned before age 5). We therefore adopt a secondary scoring approach, based on a recent publication in which researchers expanded the use of the PROMIS parent proxy measures to early childhood (age 1–5; Cella et al., 2022; Lai et al., 2022; Sherlock et al., 2022). This process involved adapting existing parent proxy items, such as the ones included in our measures. Of our eight Anxiety items, eight very similar items are included in the new Early Childhood anxiety item bank (ex: “My child felt nervous” converted into “My child seemed nervous”). Of our six Depressive Symptom items, two very similar items are included in the new Early Childhood depressive symptom item bank (ex: “It was hard for my child to have fun” converted into “My child had a hard time having fun”). Though these items do not constitute existing subscales of the PROMIS early childhood measures, the PROMIS system allows for the scoring of custom short forms. We therefore used the HealthMeasures Scoring Service to determine additional age-adjusted t-scores for those 28 visits according to the Early Childhood item banks (Cella et al., 2020). We note that the correlation between Early Childhood and general Parent Proxy t-scores is extremely high (ranxiety(26) = 0.99, p < 0.01; rdepression(26) = 0.90, p < 0.01), while Early Childhood scoring was also systematically higher than the general Parent Proxy scoring (tanxiety(27) = 24.02, p < 0.001; tdepression(27) = 12.297, p < 0.001). For maximum transparency, we report results using the age-adjusted t-scores for the visits at ages 3 and 4 and results when we use the full short forms.
All 51 youth had parent-reported scores for depressive symptoms from before and after their child’s transition. All but one of the youth had parent-reported scores for anxiety symptoms from both before and after their child’s transition. Youth themselves also completed a self-report for visits when they were present beginning at age nine; however, given the young age of the children in this study, there were not enough pre-transition data to conduct analyses using child report. If two parents completed the PROMIS scales at a given time point (92 visits), we use the mean of those two parent reports. In these cases, the two parents report similar levels of internalizing symptoms (raw correlations: ranxiety(90) = 0.57, p < 0.001; rdepression(90) = 0.54, p < 0.001).
COVID-19.
The onset of the global COVID-19 pandemic took place during our ongoing data collection. The COVID-19 pandemic negatively impacted child mental health broadly (Racine et al., 2020), and as a result, we had concerns that including data from the COVID-period could impact our primary question of interest—particularly as all data collected during COVID were post-transition. Because only a small proportion of our transitioners’ data was collected during COVID-19 (35 visits), we could not conduct a strong test of whether COVID-19 impacted results among our transitioning sample. Therefore, in order to assess whether COVID-19 might be expected to influence our data, we examined PROMIS data from N = 178 other gender diverse youth collected by our lab. We found that their mental health was negatively impacted by COVID (for full details, see Supplementary Materials). Given this, we decided to conduct parallel analyses including and excluding data collected after the onset of COVID (i.e., after February 1, 2020).
Results
All analyses were conducted in R (Wickham et al., 2019), with models fit using the lme4, lmerTest and sjPlot packages (Bates et al., 2014; Kuznetsova et al., 2017; Lüdecke et al., 2022), and significance for fixed effects evaluated using the Satterthwaite approximation (packages knitr and parameters were also used in the process of displaying results: Lüdecke et al., 2020; Xie, 2023).
Transition-Related Changes in Mental Health.
Linear mixed-effects models were used to estimate changes in anxiety and depression t-scores as a function of whether the data were collected before or after transition. There are four analytic decision points in this project where we considered multiple decisions equally reasonable. We therefore took a multiverse approach to testing whether social transition predicted significant mental health differences (Steegen et al., 2016). This approach is considered helpful when there are multiple reasonable analytic decisions one could make. Interpretation then relies on understanding the degree to which the results are or are not contingent upon any particular analytic decision; significant results that are present across different analytic decisions are thought to be more robust than those that are only significant in rare instances.
In our multiverse analyses we include four independent analytic decisions. First, we include or exclude data gathered after the onset of the COVID-19 pandemic. Second, we include or exclude data from retransitioners (N = 3). Third, we code visits under age 5 according to the full short forms we used (developed for children aged 5–17), or according to closely-related Early Childhood measures as described above.
Fourth, we have multiple options for model specification. In all models, we take a multi-level modeling approach, including a random intercept of youth to account for the non-independent nature of within-youth measures. The decision point centers around controlling for other variables related to childhood mental health. Based on extant literature, there is reason to believe that both gender and age (Steensma et al., 2014) can be relevant to internalizing symptoms in gender diverse youth. For age, it is further reasonable to expect either linear (e.g., children’s mental health getting worse as they get older) or quadratic (e.g., a period of relatively little change followed by a period of quicker change) effects. We therefore consider six possible models, including combinations of these effects. In Model A, our only fixed effect is that of social transition (contrast coded: pre-transition = −0.5, post-transition = 0.5) – we do not control for other variables. In Model B, we include gender as a control variable (post-transition binary gender, contrast coded: girl = −0.5, boy = 0.5). In Model C, we control for a linear effect of age. In Model D, we control for both gender and linear age. In Model E, we include linear and quadratic age as control variables. In Model F, we include linear age, quadratic age, and gender as control variables. In all models including age, we use age in months as a predictor and center it on the mean as calculated across all included visits.
Based on these four decision points, there are 48 models we consider reasonable when assessing transition-related change in anxiety and depression. For interpretation, we focus on the overall pattern of social transition effects as displayed in Figure 1 (Ns and mean anxiety and depressive symptoms pre- and post-transition for each analytic approach can be seen in Table 2; full results of each model can be seen in the supplementary materials). This forest plot displays the estimated t-score difference between pre-transition and post-transition visits, along with the confidence interval of that estimate. Negative values represent mental health improvements, and confidence intervals which do not overlap with zero show that the estimate is statistically significant.
Figure 1.
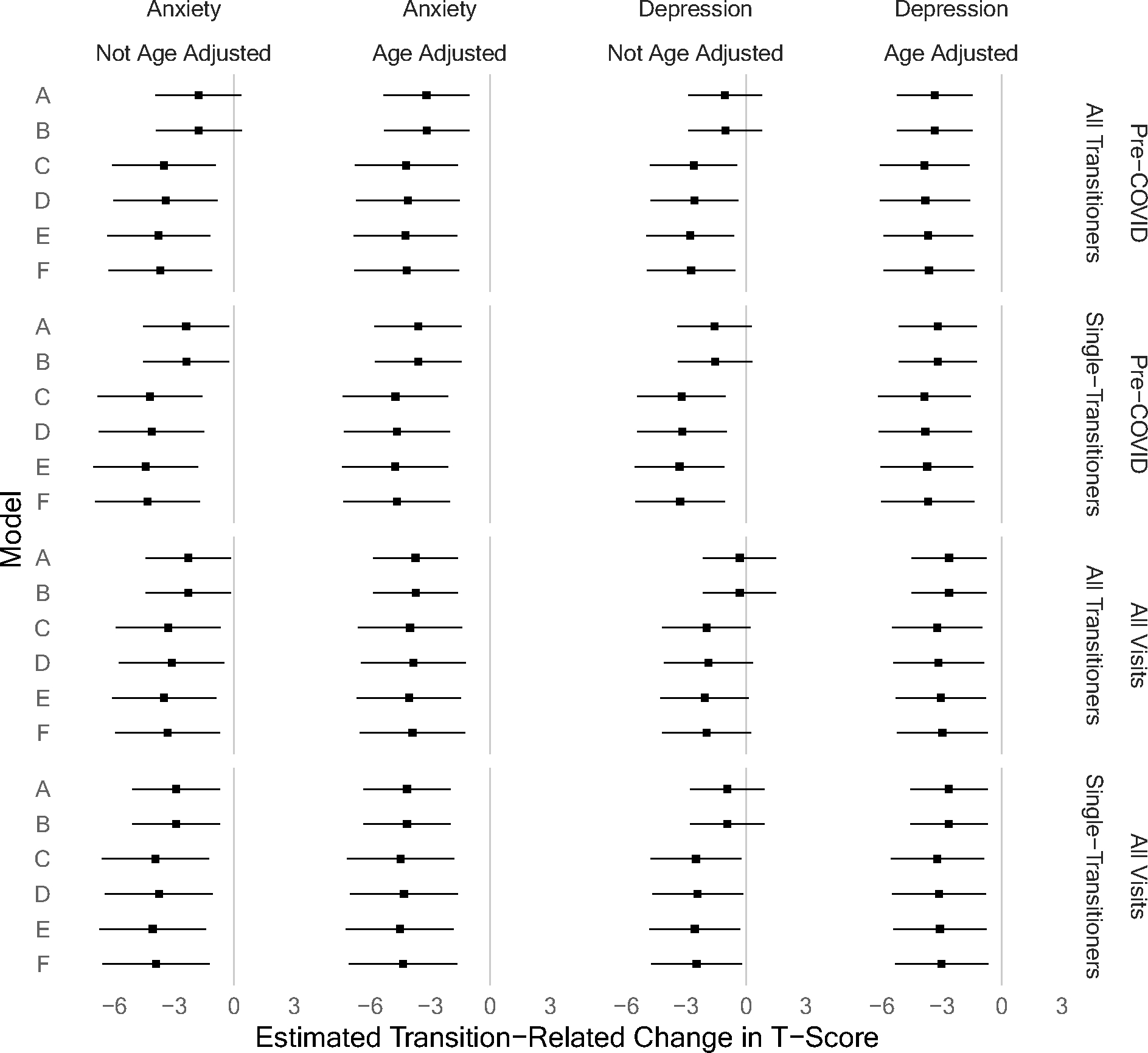
Forest Plot of Transition-Related Mental Health Change Estimates. In each graph, the dot represents the point estimate of mental health change between pre-transition and post-transition visits. The error bars represent confidence intervals (calculated using the Satterthwaite method); error bars that do not overlap with zero show significant effects. Across a variety of analytic approaches, we see that anxiety and depression are improved (46 out of 48 analyses for anxiety; 36 out of 48 analyses for depression) or unchanged (2 out of 48 analyses for anxiety; 12 out of 48 analyses for depression) after transition relative to before transition. We saw no analytic conditions under which post-transition mental health was worse than pre-transition mental health.
Table 2.
Mean Anxiety and Depressive Symptoms Before and After Social Transition. In this table, we display mean values of internalizing symptoms before and after social transition (with standard deviations in parentheses). This is done separately for each applicable multiverse definition (e.g., including or not including data gathered during COVID). In each case, participant-level mental health before and after transition is calculated as the mean t-score across all visits (i.e., if a participant has three post-transition visits, we define their post-transition anxiety t-score as the mean of their t-scores at those three visits). We here report the means and standard deviations of those values across included participants.
| Anxiety | Depressive Symptoms | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Not Age Adjusted | Age Adjusted | Not Age Adjusted | Age Adjusted | ||||||||
|
|
|
||||||||||
| N | Pre-Trans. | Post-Trans. | Pre-Trans. | Post-Trans. | N | Pre-Trans. | Post-Trans. | Pre-Trans. | Post-Trans. | ||
|
| |||||||||||
| Pre-COVID | All Transitioners | 45 | 55.36 (9.49) | 53.72 (9.48) | 57.07 (8.98) | 54.05 (9.26) | 46 | 54.28 (7.83) | 52.89 (8.20) | 56.92 (7.26) | 53.39 (8.04) |
|
| |||||||||||
| Only Single-Transitioners | 42 | 55.70 (9.42) | 53.70 (9.81) | 57.30 (8.99) | 54.06 (9.58) | 43 | 54.48 (7.68) | 52.78 (8.48) | 56.70 (7.33) | 53.31 (8.31) | |
|
| |||||||||||
| All Visits | All Transitioners | 50 | 55.61 (9.37) | 53.62 (8.19) | 57.34 (8.92) | 53.83 (8.02) | 51 | 53.88 (8.04) | 53.22 (7.06) | 56.48 (7.75) | 53.53 (6.92) |
|
| |||||||||||
| Only Single-Transitioners | 47 | 55.93 (9.30) | 53.56 (8.44) | 57.56 (8.92) | 53.78 (8.27) | 48 | 54.05 (7.93) | 52.92 (7.11) | 56.25 (7.83) | 53.24 (6.98) | |
We found that post-transition anxiety was significantly lower than pre-transition anxiety in 46 of 48 models. We found that post-transition depressive symptoms were significantly lower than pre-transition depressive symptoms in 36 of 48 models. All analytic approaches showed either transition-related improvement in mental health or no significant transition-related change – no analyses showed transition-related decrements in mental health. As a demonstrative visual, we include Figure 2, which shows each youth’s level of anxiety and depression before and after social transition. This figure includes data from all visits and uses age-adjusted t-scores for visits where children were aged 3 or 4.
Figure 2.
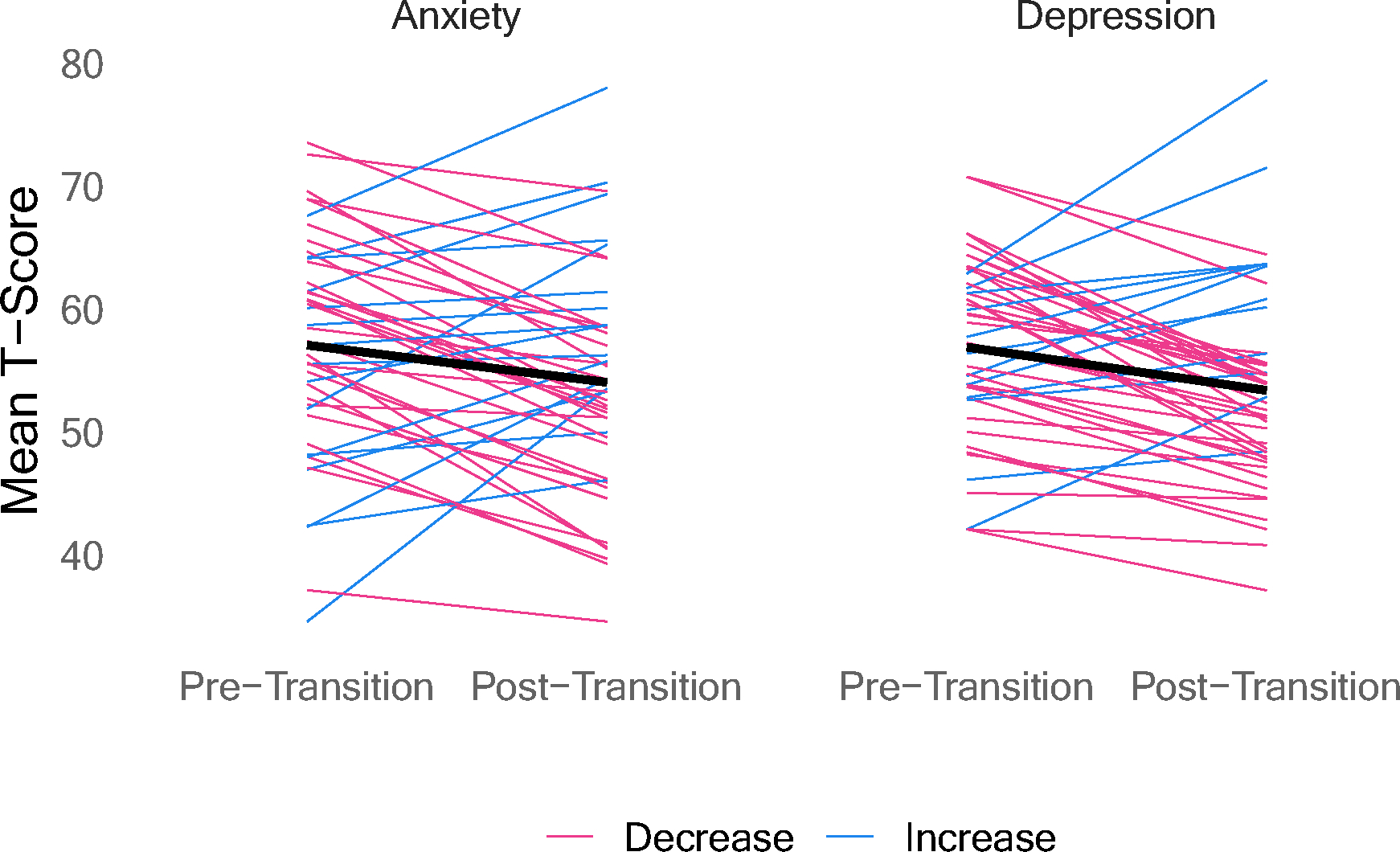
Anxiety and Depression T-Scores Before and After Transition. Across a variety of individual trajectories, most youth had lower anxiety and depression after transition. These visualizations show participants’ mean pre-transition and post-transition internalizing symptoms (All Data, Age Adjusted T-Scores for 3-year-olds and 4-year-olds). The black line shows the across-subjects mean.
Comparison with Non-Transitioning Gender Diverse Youth.
Much research studying the mental health of gender diverse youth focuses on comparison, looking at the relative mental health of transgender youth (e.g., Olson et al., 2016). In this project, we were instead able to measure within-person mental health changes related to social transition. On the suggestion of reviewers, we additionally explored a comparison between our 51 transitioning youth and their counterparts who did not transition. We note that these samples differ in many potential ways (e.g., they may differ in a desire to transition, Olson et al., 2019; degree of gender nonconformity, Rae et al., 2019; parents’ tolerance of social transition; or other as-yet-unknown ways) and therefore direct comparison of these groups should not be interpreted as a difference merely in whether they socially transitioned or not. Of the original 142 youth, we include 87 in our nontransitioning sample (3 youth socially transitioned after the age of 12, so they are not included in either our main sample or this comparison sample; 1 youth did not transition but their parents have not reported any internalizing data; the other 51 are in the transitioning group).
This comparison sample includes 29 children who were assigned female at birth, and 58 who were assigned male at birth (this ratio is not significantly different from our main sample; χ2(df = 1) = 1.048, p = 0.31). These youth were older than the transitioning group when their parents first provided PROMIS data (Mtransitioners = 79.61 months, SDtransitioners = 26.93; Mnon-transitioners = 93.00 months, SDnon-transitioners = 28.69; t(110.27) = 2.751, p = 0.007). These youth also have fewer visits with PROMIS data in this time period (Mtransitioners = 4.73 visits, SDtransitioners = 1.58; Mnon-transitioners = 3.39 visits, SDnon-transitioners = 1.57; t(104.69) = −4.806, p < 0.001). For additional demographics about this sample, see Table 3.
Table 3.
Demographics of Non-Transitioning Comparison Sample.
| N = 87 | |
|---|---|
|
| |
| Child Sex Assigned at Birth | n (%) |
| Male | 58 (66.7%) |
| Female | 29 (33.3%) |
| Child Race | |
| Asian | 2 (2.3%) |
| Black | 2 (2.3%) |
| Multiracial | 10 (11.5%) |
| Native American | 1 (1.2%) |
| White, Hispanic | 8 (9.2%) |
| White, non-Hispanic | 63 (72.4%) |
| Not Reported | 1 (1.2%) |
| Parent 1 Highest Level of Education | |
| High School Diploma | 2 (2.3%) |
| Some college/Associate’s degree | 8 (9.2%) |
| College/Bachelor’s degree | 31 (35.6%) |
| Advanced degree (MA, MD, etc.) | 43 (49.4%) |
| Unknown | 3 (3.5%) |
| Geographic Region of the United States, or Canada | |
| Midwest | 18 (20.7%) |
| Northeast | 13 (14.9%) |
| South | 13 (14.9%) |
| West | 42 (48.3%) |
| Canada | 1 (1.2%) |
| Annual Family Income | |
| less than $25,000 | 4 (4.6%) |
| $25,001-$50,000 | 9 (10.3%) |
| $50,001-$75,000 | 17 (19.5%) |
| $75,001-$125,000 | 28 (32.2%) |
| greater than $125,000 | 28 (31.2%) |
| Unknown | 1 (1.2%) |
Note: Income and education were determined by the first available response.
We cannot directly compare the effect of social transition between the two groups, as the comparison group has not undergone social transition. Instead, we look at whether transition status at a particular visit (non-transitioner, pre-transition transitioner, post-transition transitioner) predicts mental health. As with our central analyses, we take a multiverse approach to this analysis with respect to inclusion of COVID data, inclusion of multiple transitioners in the transitioning sample, and scoring of visits where the child was age 3 or 4. In all cases, we use the same linear-multi-level model predicting internalizing scores (Anxiety or Depressive Symptoms). Our fixed effect of interest is transition status, with visits from non-transitioners used as the reference. We additionally include a random intercept for youth to account for within-youth dependency and a fixed effect of age (in months, centered across the dataset) to control for between-group differences in age.
We focus on the overall pattern of visit-type effects as displayed in Figure 3 (full model results can be seen in the supplementary materials). This forest plot displays the estimated t-score difference between (a) pre-transition transitioners and non-transitioners and (b) post-transition transitioners and non-transitioners. Positive values mean that the transitioners had elevated (i.e., worse) anxiety or depressive symptoms relative to the non-transitioners, while negative values mean that the transitioners had reduced (i.e., better) anxiety or depressive symptoms relative to the non-transitioners. The graph displays point estimates and confidence intervals. In 15 of 16 cases, we see no significant difference between pre-transition transitioners and non-transitioners. In all cases, we see no significant difference between post-transition transitioners and non-transitioners. Visual inspection of the graph indicates that the youth who transitioned had scores that were (non-significantly) worse than the non-transitioners before transitioning and scores that were (non-significantly) better than the non-transitioners after. While the transitioners showed significant differences based on transition status, the non-transitioners’ average scores fell in between, and transitioner-nontransitioner differences were non-significant.
Figure 3.
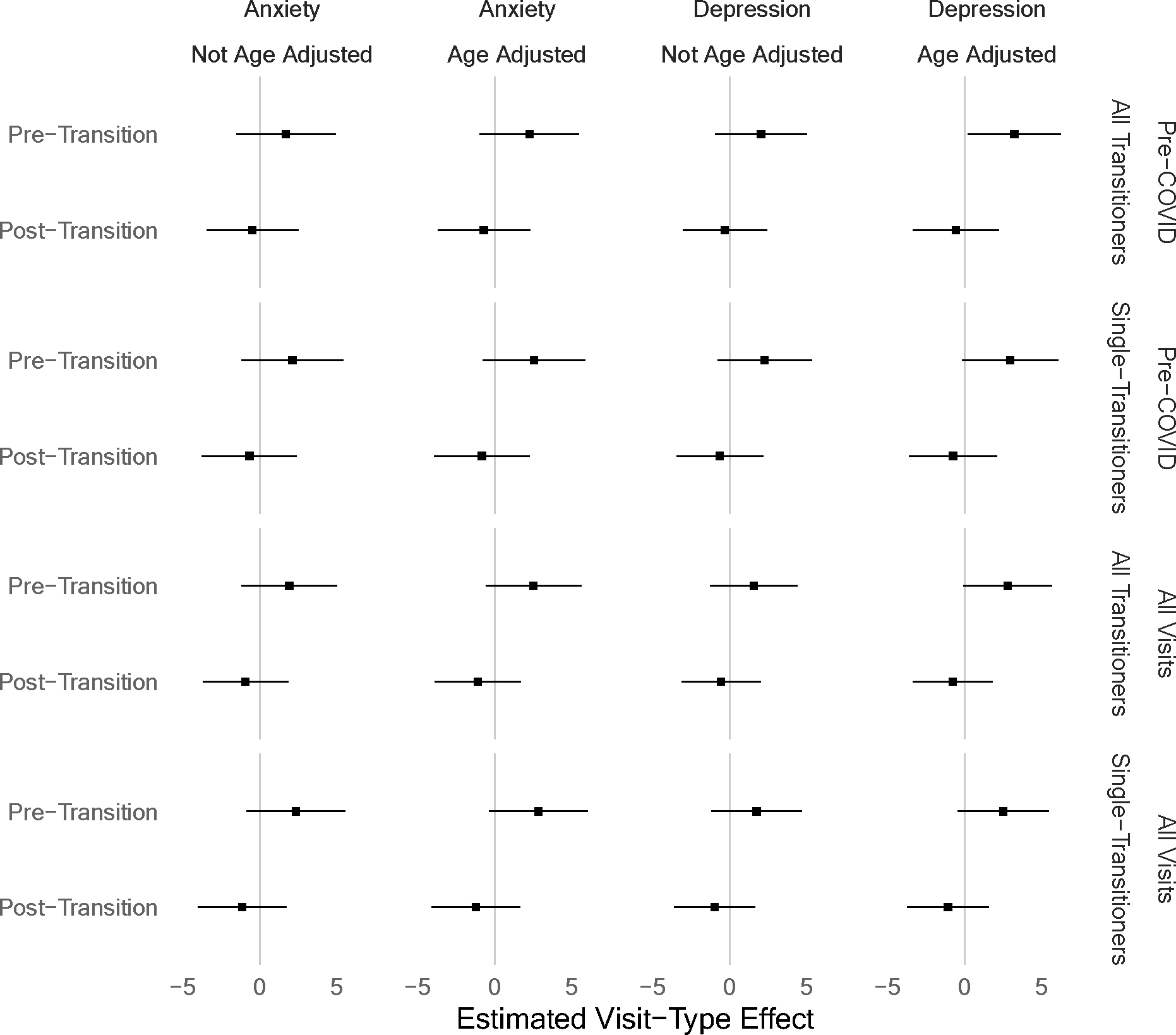
Forest Plot of Visit-Type Mental Health Difference Estimates. In each graph, we see two effects: one comparing pre-transition transitioners with non-transitioners and one comparing post-transition transitioners with non-transitioners. Each point estimate is shown, along with confidence intervals (calculated using the Satterthwaite method); error bars that do not overlap with zero show statistically significant effects. Positive values indicate that the transitioners had mental health decrements relative to the non-transitioners, while negative values indicate that the transitioners had mental health benefits relative to the non-transitioners. All effects are from analyses controlling for age, to account for age differences between groups. In 31 of 32 cases, the transitioners do not differ significantly from the non-transitioners (regardless of transition status). We additionally note that the consistent pattern in which pre-transition estimates are negative and post-transition estimates are positive is consistent with our main finding that social transition is associated with mental health improvements.
Discussion
The question of whether childhood social transitions impact psychopathology is exceedingly hard to test methodologically, given that using random assignment would be both unethical and implausible (Drescher & Byne, 2012; Green, 2017; Olson-Kennedy et al., 2016; Turban & Ehrensaft, 2018; Zucker, 2020). Using the next best option, a prospective design, we found that youth generally showed decreases in anxiety and depression after transitioning relative to before. The results were especially consistent for anxiety, though the depression results were fairly robust as well. For both types of internalizing symptoms, differences were especially strong when we used age-adjusted subscale scoring for parent reports about children under age 5, when we excluded data gathered during the onset of the COVID-19 pandemic, and when we controlled for any effects of age; however, these effects were significant in most models, regardless. These findings suggest that childhood social transitions on average reduce internalizing symptoms in youth who identify as the binary gender other than the one assigned to them at birth. These findings contribute to a longstanding discussion around childhood social transitions and whether they can be beneficial (Sherer, 2016; Steensma & Cohen-Kettenis, 2011), and broadly, they provide support for childhood social transitions. Critically, we do not interpret these results to mean that all gender diverse youth would benefit from social transitions (for example, we might not expect male children who like to wear stereotypically feminine clothing, but do not identify as girls, to benefit from a transition), especially as past work suggests many gender nonconforming youth who have not transitioned simply do not want to transition (Olson et al., 2019).
Our finding that youth who did not transition did not differ in their mental health from those who did is consistent with some past cross-group comparisons (Morandini et al., 2023; Sievert et al., 2021; Wong et al., 2019). However, because these studies focused on cross-sectional data they were unable to address the key question here: whether those who socially-transition show an improvement in mental health across this transition. Our results comparing internalizing symptoms before vs. after transitions suggest that social transitions in childhood may, in fact, reduce internalizing psychopathology for many transgender youth, at least in the short-to-medium term (final visits in the data set were M = 3.55 years since the child’s social transition; SD = 1.3 years, range 1–6 years); whether this improvement holds in the long term is unknown. We expect that our findings apply specifically to youth who identify as the binary gender other than the one assigned to them at birth, who wish to live as that gender, who have parental support for that decision, and who live in environments where it is safe to transition.
These findings do not illuminate the mechanism by which this improvement in internalizing symptoms across transitions occurred. It is possible that living, and being seen by others, as the gender with which a child identifies in itself enhances that child’s wellbeing. It also tends to be the case that children who make binary socially transitions (as these children did—that is, they live as boys or girls, rather than nonbinary) are often perceived by others as being gender nonconforming before socially transitioning (e.g., being perceived by others as a boy who wears dresses and plays with dolls) and gender conforming after socially transitioning (e.g., being perceived by others as a girl who wears dresses and plays with dolls). Thus, it is possible that some children actually experienced less victimization after transitioning than before, and this could also explain, in part or in full, the reduction in symptoms. These and other potential mechanisms should be explored in future work. Additionally, in the present study we did not capture the specific reason(s) that each child transitioned. It is possible that some children transition because they, their parents, or a clinician believe their mental health will improve after doing so, and that others may transition for other reasons. It would be interesting in future work to investigate whether certain reasons for transitioning are linked with a greater benefit of transition than others.
As with all findings, strong conclusions must be tempered by the limitations of the study itself. First, while the primary analyses are within-youth—and therefore statistical power is greater as compared to between-subjects designs—a sample size of 51 still is not large. Replication in a second, ideally larger and independent sample would lend greater confidence to the findings. These prospective studies are challenging to conduct, however, because researchers cannot know how many initially-recruited gender nonconforming children will ultimately transition, and therefore, a very large sample is needed to capture even a small number of youth who will later transition. Second, as discussed in the results section, this study utilized a measure for parents of youth aged five and above with some parents of youth aged three and four. Given that the results held and were stronger when using age-adjusted measures, we think this concern is minimized. Nonetheless we encourage future researchers to use the version of the measure that now exists for younger children in this age group. Third, this sample is predominantly white and high income, with high levels of parental education. It is possible that the impact of social transitions would be different for families who experience more prejudice and discrimination on other dimensions of identity, and/or who have fewer financial resources. Additional work with more demographically representative samples is needed. Fourth, our sample included predominantly parents of youth assigned male at birth, rather than parents of youth who were assigned female at birth. This ratio is in line with other studies of gender diverse children (Gibson et al., 2021; Kuvalanka et al., 2017; Steensma et al., 2014). but it is not in line with many recent samples of gender diverse adolescents, many of which include more youth who are assigned female at birth (Arnoldussen et al., 2020; Chen et al., 2023). More work, in older samples, and with different gender breakdowns, is needed to assess the generalizability of the current findings.
Another limitation of this study is that it utilized parent report. Children may have different views of their mental health than do their parents; parents could either under- or overestimate their child’s anxiety and depression symptoms, compared to children’s own perceptions. Past work with a separate sample of transgender youth, though, showed that parents and youth reported similar levels of internalizing symptoms, with parents reporting slightly higher levels of anxiety than do children (Durwood et al., 2017). Given that young children below around 8 years of age are too young to complete many validated self-report scales of psychopathology, and/or the same scales are not validated for use from 3 to 12 (Ebesutani et al., 2011; Varni et al., 2012), gauging child-reported anxiety and depression both before and after a social transition in early childhood presents a challenge. Nonetheless, readers should keep in mind that youth could have different views of their mental health than do their parents.
One final limitation is that we treated social transitions as a single moment in time based on the time point at which a child had changed pronouns across their social contexts (e.g., at school, at home, with strangers). In reality, social transitions often take place over extended periods of time, during which children might make certain changes (e.g., wearing different clothing, changing pronouns) in some contexts but not others (Kuper et al., 2019). Qualitative work following youth as they go through the process of transition can provide important nuance on the process of transitioning that these categorical, quantitative data cannot.
It is important to note that, as with all life experiences, the impact of social transitions found here was not identical for everyone. As can be seen in Figure 2, some youth’s symptoms decreased, while others’ increased after transition relative to before. There are a variety of possible explanations for this. Some youth could have experienced higher levels of gender-related social rejection and/or bullying after transitioning compared to before, which could have led to mental health decrements. Some youth may have experienced other stressors completely unrelated to gender (e.g., their family had a change in socioeconomic status) that could have influenced their wellbeing. It is also possible that social transitions are simply not beneficial for all youth who undertake them. We saw that the models generally showed larger effects of transition when the three children who later retransitioned were excluded; though it is hard to draw conclusions based on three individuals, this may suggest that for these children, social transitions were not helpful, and may have worsened their mental health (importantly, other work shows that children can retransition without distress, and thus if a social transition does not seem to benefit a child, the child can retransition; (Durwood et al., 2022). An interesting future topic of research would be to examine for whom transitioning may be more or less helpful, or what other factors may co-occur with transitioning (e.g., an increase in bullying, a change in one’s ability to participate on sports teams) that could offset positive impacts of transitioning for some youth. A key point to note here is that, while it is instructive to learn about whether social transitions impact mental health, as we have done here, a mental health benefit is not necessary to justify an individual’s decision to transition. A person may wish to transition simply because they wish to viewed and treated by others in a way that is consistent with how they identify—just as many lesbian, gay, or bisexual people likely decide to come out without the expressed purpose of improving their levels of anxiety and depression (though of course some may show such an improvement). Thus, while these data happened to show that many children’s mental health improved with socially transitioning, we do not mean to imply that such a benefit is necessary to justify such a transition, or that the lack of such an improvement would suggest someone should not transition.
Conclusion
Using a prospective sample of gender diverse children who made binary social transitions, we found, on average, a significant decrease in anxiety and depression symptoms across transitions. These are the first quantitative data to test the impact of childhood social transitions on internalizing symptoms in gender diverse youth.
Supplementary Material
Funding.
Author time and data collection for this paper were supported through grants including National Institute of Child Health and Development under award R01HD092347, the National Science Foundation under award BCS-1523632, and through funding from the Arcus Foundation. We would also like to thank the Whiteley Center for hosting us for discussions and protected writing time that ultimately led to this paper. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders. Additionally, Dr. Olson receives funding from the MacArthur Foundation.
Footnotes
Conflicts of Interest. KRO received grant funding or fellowship support from the National Institute of Health, National Science Foundation, and MacArthur Foundation. KRO served as a paid consultant at Sesame Workshop, an entertainment production company, and as a subject expert panelist for SAMHSA; her travel was paid for to interview with Kensington Communications. LD provided paid feedback on a textbook chapter for Pearson and also received honoraria for invited lectures in an undergraduate course at UCLA, and at the UW Medicine Harborview Medical Center.
Parents might not participate in a particular study visit/survey because they were too busy at the time of the invitation, but they wished to stay in the longitudinal study and participate in the future. For in person visits, parents sometimes did not participate because they were out of town when the study team was in their area, sick, or because they had other conflicting commitments.
Supplemental Material: Supplemental Material are posted on the journal’s website.
References
- Anxiety: A brief guide to the PROMIS Anxiety instruments. (2019). [Patient-Reported Outcomes Measurement Information System: Dynamic Tools to Measure Health Outcomes from the Patient Perspective]. [Google Scholar]
- Arnoldussen M, Steensma TD, Popma A, Van Der Miesen AIR, Twisk JWR, & De Vries ALC (2020). Re-evaluation of the Dutch approach: Are recently referred transgender youth different compared to earlier referrals? European Child & Adolescent Psychiatry, 29(6), 803–811. 10.1007/s00787-019-01394-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bates D, Mächler M, Bolker B, & Walker S (2014). Fitting Linear Mixed-Effects Models using lme4. arXiv:1406.5823 [Stat]. http://arxiv.org/abs/1406.5823 [Google Scholar]
- Bockting WO, Miner MH, Swinburne Romine RE, Hamilton A, & Coleman E (2013). Stigma, Mental Health, and Resilience in an Online Sample of the US Transgender Population. American Journal of Public Health, 103(5), 943–951. 10.2105/AJPH.2013.301241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cella D, Blackwell CK, & Wakschlag LS (2022). Bringing PROMIS to Early Childhood: Introduction and Qualitative Methods for the Development of Early Childhood Parent Report Instruments. Journal of Pediatric Psychology, 47(5), 500–509. 10.1093/jpepsy/jsac027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cella D, Gershon R, Bass M, & Rothrock N (2020). Assessment Center Scoring Service User Manual (v1.8). https://www.assessmentcenter.net/ac_scoringservice/templates/UserManual.pdf [Google Scholar]
- Chen D, Berona J, Chan Y-M, Ehrensaft D, Garofalo R, Hidalgo MA, Rosenthal SM, Tishelman AC, & Olson-Kennedy J (2023). Psychosocial Functioning in Transgender Youth after 2 Years of Hormones. New England Journal of Medicine, 388(3), 240–250. 10.1056/NEJMoa2206297 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Depression: A brief guide to the PROMIS Depression instruments. (2019). [Patient-Reported Outcomes Measurement Information System: Dynamic Tools to Measure Health Outcomes from the Patient Perspective]. [Google Scholar]
- Drescher J, & Byne W (2012). Gender Dysphoric/Gender Variant (GD/GV) Children and Adolescents: Summarizing What We Know and What We Have Yet to Learn. Journal of Homosexuality, 59(3), 501–510. 10.1080/00918369.2012.653317 [DOI] [PubMed] [Google Scholar]
- Durwood L, Eisner L, Fladeboe K, Ji C. (Gabriella), Barney S, McLaughlin KA, & Olson KR (2021). Social Support and Internalizing Psychopathology in Transgender Youth. Journal of Youth and Adolescence, 50(5), 841–854. 10.1007/s10964-020-01391-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durwood L, Kuvalanka KA, Kahn-Samuelson S, Jordan AE, Rubin JD, Schnelzer P, Devor AH, & Olson KR (2022). Retransitioning: The experiences of youth who socially transition genders more than once. International Journal of Transgender Health, 23(4), 409–427. 10.1080/26895269.2022.2085224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durwood L, McLaughlin KA, & Olson KR (2017). Mental Health and Self-Worth in Socially Transitioned Transgender Youth. Journal of the American Academy of Child & Adolescent Psychiatry, 56(2), 116–123.e2. 10.1016/j.jaac.2016.10.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ebesutani C, Bernstein A, Martinez JI, Chorpita BF, & Weisz JR (2011). The Youth Self Report: Applicability and Validity Across Younger and Older Youths. Journal of Clinical Child & Adolescent Psychology, 40(2), 338–346. 10.1080/15374416.2011.546041 [DOI] [PubMed] [Google Scholar]
- Gibson DJ, Glazier JJ, & Olson KR (2021). Evaluation of Anxiety and Depression in a Community Sample of Transgender Youth. JAMA Network Open, 4(4), e214739–e214739. 10.1001/jamanetworkopen.2021.4739 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green R (2017). To Transition or Not to Transition? That Is the Question. Current Sexual Health Reports, 9(2), 79–83. 10.1007/s11930-017-0106-5 [DOI] [Google Scholar]
- Gülgöz S, Glazier JJ, Enright EA, Alonso DJ, Durwood LJ, Fast AA, Lowe R, Ji C, Heer J, Martin CL, & Olson KR (2019). Similarity in transgender and cisgender children’s gender development. Proceedings of the National Academy of Sciences of the United States of America, 116(49), 24480–24485. 10.1073/pnas.1909367116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatzenbuehler ML (2009). How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychological Bulletin, 135(5), 707–730. 10.1037/a0016441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Irwin DE, Gross HE, Stucky BD, Thissen D, DeWitt E, Lai J, Amtmann D, Khastou L, Varni JW, & DeWalt DA (2012). Development of six PROMIS pediatrics proxy-report item banks. Health and Quality of Life Outcomes, 10(1), 22. 10.1186/1477-7525-10-22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuper LE, Lindley L, & Lopez X (2019). Exploring the gender development histories of children and adolescents presenting for gender affirming medical care. Clinical Practice in Pediatric Psychology, 7(3), 217–228. 10.1037/cpp0000290 [DOI] [Google Scholar]
- Kuvalanka KA, Weiner JL, Munroe C, Goldberg AE, & Gardner M (2017). Trans and gender-nonconforming children and their caregivers: Gender presentations, peer relations, and well-being at baseline. Journal of Family Psychology, 31(7), 889–899. 10.1037/fam0000338 [DOI] [PubMed] [Google Scholar]
- Kuznetsova A, Brockhoff PB, & Christensen RHB (2017). lmerTest package: Tests in linear mixed effects models. Journal of Statistical Software, 82(13). [Google Scholar]
- Lai J-S, Kallen MA, Blackwell CK, Wakschlag LS, & Cella D (2022). Psychometric Considerations in Developing PROMIS® Measures for Early Childhood. Journal of Pediatric Psychology, 47(5), 510–522. 10.1093/jpepsy/jsac025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lüdecke D, Bartel A, Schwemmer C, Powell C, Djalovski A, & Titz J (2022). sjPlot: Data Visualization for Statistics in Social Science (2.8.11) [Computer software]. https://CRAN.R-project.org/package=sjPlot [Google Scholar]
- Lüdecke D, Ben-Shachar MS, Patil I, & Makowski D (2020). Parameters: Extracting, Computing and Exploring the Parameters of Statistical Models using R. Journal of Open Source Software, 5(53). 10.21105/joss.02445 [DOI] [Google Scholar]
- Morandini JS, Kelly A, De Graaf NM, Malouf P, Guerin E, Dar-Nimrod I, & Carmichael P (2023). Is Social Gender Transition Associated with Mental Health Status in Children and Adolescents with Gender Dysphoria? Archives of Sexual Behavior, 52(3), 1045–1060. 10.1007/s10508-023-02588-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olson KR, Blotner C, Alonso D, Lewis K, Edwards D, & Durwood L (2019). Family discussions of early childhood social transitions. Clinical Practice in Pediatric Psychology, 7(3), 229–240. 10.1037/cpp0000289 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olson KR, Durwood L, DeMeules M, & McLaughlin KA (2016). Mental Health of Transgender Children Who Are Supported in Their Identities. Pediatrics, 137(3), e20153223. 10.1542/peds.2015-3223 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olson KR, Durwood L, Horton R, Gallagher NM, & Devor A (2022). Gender Identity 5 Years After Social Transition. Pediatrics, 150(2), e2021056082. 10.1542/peds.2021-056082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olson-Kennedy J, Cohen-Kettenis PT, Kreukels BPC, Meyer-Bahlburg HFL, Garofalo R, Meyer W, & Rosenthal SM (2016). Research priorities for gender nonconforming/transgender youth: Gender identity development and biopsychosocial outcomes. Current Opinion in Endocrinology & Diabetes and Obesity, 23(2), 172–179. 10.1097/MED.0000000000000236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pachankis JE, Cochran SD, & Mays VM (2015). The mental health of sexual minority adults in and out of the closet: A population-based study. Journal of Consulting and Clinical Psychology, 83(5), 890–901. 10.1037/ccp0000047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pariseau EM, Chevalier L, Long KA, Clapham R, Edwards-Leeper L, & Tishelman AC (2019). The relationship between family acceptance-rejection and transgender youth psychosocial functioning. Clinical Practice in Pediatric Psychology, 7(3), 267–277. 10.1037/cpp0000291 [DOI] [Google Scholar]
- Pellicane MJ, & Ciesla JA (2022). Associations between minority stress, depression, and suicidal ideation and attempts in transgender and gender diverse (TGD) individuals: Systematic review and meta-analysis. Clinical Psychology Review, 91, 102113. 10.1016/j.cpr.2021.102113 [DOI] [PubMed] [Google Scholar]
- Racine N, Cooke JE, Eirich R, Korczak DJ, McArthur B, & Madigan S (2020). Child and adolescent mental illness during COVID-19: A rapid review. Psychiatry Research, 292, 113307. 10.1016/j.psychres.2020.113307 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rae JR, Gülgöz S, Durwood L, DeMeules M, Lowe R, Lindquist G, & Olson KR (2019). Predicting Early-Childhood Gender Transitions. Psychological Science, 30(5), 669–681. 10.1177/0956797619830649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan C, Russell ST, Huebner D, Diaz R, & Sanchez J (2010). Family Acceptance in Adolescence and the Health of LGBT Young Adults. Journal of Child and Adolescent Psychiatric Nursing, 23(4), 205–213. 10.1111/j.1744-6171.2010.00246.x [DOI] [PubMed] [Google Scholar]
- Sherer I (2016). Social Transition: Supporting Our Youngest Transgender Children. Pediatrics, 137(3), e20154358. 10.1542/peds.2015-4358 [DOI] [PubMed] [Google Scholar]
- Sherlock P, Blackwell CK, Kallen MA, Lai J-S, Cella D, Krogh-Jespersen S, Luby JL, Buss KA, Burns J, & Wakschlag LS (2022). Measuring PROMIS® Emotional Distress in Early Childhood. Journal of Pediatric Psychology, 47(5), 547–558. 10.1093/jpepsy/jsac029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sievert ED, Schweizer K, Barkmann C, Fahrenkrug S, & Becker-Hebly I (2021). Not social transition status, but peer relations and family functioning predict psychological functioning in a German clinical sample of children with Gender Dysphoria. Clinical Child Psychology and Psychiatry, 26(1), 79–95. 10.1177/1359104520964530 [DOI] [PubMed] [Google Scholar]
- Steegen S, Tuerlinckx F, Gelman A, & Vanpaemel W (2016). Increasing Transparency Through a Multiverse Analysis. Perspectives on Psychological Science, 11(5), 702–712. 10.1177/1745691616658637 [DOI] [PubMed] [Google Scholar]
- Steensma TD, & Cohen-Kettenis PT (2011). Gender Transitioning before Puberty? Archives of Sexual Behavior, 40(4), 649–650. 10.1007/s10508-011-9752-2 [DOI] [PubMed] [Google Scholar]
- Steensma TD, Zucker KJ, Kreukels BPC, VanderLaan DP, Wood H, Fuentes A, & Cohen-Kettenis PT (2014). Behavioral and Emotional Problems on the Teacher’s Report Form: A Cross-National, Cross-Clinic Comparative Analysis of Gender Dysphoric Children and Adolescents. Journal of Abnormal Child Psychology, 42(4), 635–647. 10.1007/s10802-013-9804-2 [DOI] [PubMed] [Google Scholar]
- Turban JL (2017). Transgender Youth: The Building Evidence Base for Early Social Transition. Journal of the American Academy of Child & Adolescent Psychiatry, 56(2), 101–102. 10.1016/j.jaac.2016.11.008 [DOI] [PubMed] [Google Scholar]
- Turban JL, & Ehrensaft D (2018). Research Review: Gender identity in youth: treatment paradigms and controversies. Journal of Child Psychology and Psychiatry, 59(12), 1228–1243. 10.1111/jcpp.12833 [DOI] [PubMed] [Google Scholar]
- Varni JW, Magnus B, Stucky BD, Liu Y, Quinn H, Thissen D, Gross HE, Huang I-C, & DeWalt DA (2014). Psychometric properties of the PROMIS® pediatric scales: Precision, stability, and comparison of different scoring and administration options. Quality of Life Research, 23(4), 1233–1243. 10.1007/s11136-013-0544-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varni JW, Thissen D, Stucky BD, Liu Y, Gorder H, Irwin DE, DeWitt EM, Lai J-S, Amtmann D, & DeWalt DA (2012). PROMIS® Parent Proxy Report Scales: An item response theory analysis of the parent proxy report item banks. Quality of Life Research, 21(7), 1223–1240. 10.1007/s11136-011-0025-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varni JW, Thissen D, Stucky BD, Liu Y, Magnus B, Quinn H, Irwin DE, DeWitt EM, Lai J-S, Amtmann D, Gross HE, & DeWalt DA (2014). PROMIS® Parent Proxy Report Scales for children ages 5–7 years: An item response theory analysis of differential item functioning across age groups. Quality of Life Research, 23(1), 349–361. 10.1007/s11136-013-0439-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wickham H, Averick M, Bryan J, Chang W, McGowan LD, François R, Grolemund G, Hayes A, Henry L, Hester J, Kuhn M, Pedersen TL, Miller E, Bache SM, Müller K, Ooms J, Robinson D, Seidel DP, Spinu VS, … Yutani H (2019). Welcome to the tidyverse. Journal of Open Source Software, 4(43). [Google Scholar]
- Wong WI, van der Miesen AIR, Li TGF, MacMullin LN, & VanderLaan DP (2019). Childhood social gender transition and psychosocial well-being: A comparison to cisgender gender-variant children. Clinical Practice in Pediatric Psychology, 7(3), 241–253. 10.1037/cpp0000295 [DOI] [Google Scholar]
- Xie Y (2023). knitr: A General-Purpose Package for Dynamic Report Generation in R (R package version 1.42) [Computer software]. https://yihui.org/knitr/ [Google Scholar]
- Zucker KJ (2020). Debate: Different strokes for different folks. Child and Adolescent Mental Health, 25(1), 36–37. 10.1111/camh.12330 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.