

Abstract
Higher concentrations of ambient air pollutants, including PM2.5 and NO2, and other pollutants have been found near active oil and gas wells and may be associated with adverse COVID‐19 outcomes. We assessed whether residential exposure to nearby oil and gas production was associated with higher rates of the respiratory infection COVID‐19 and related mortality using a population‐based ecological study in California. Using gridded population estimates, we estimated area‐level exposure to annual average oil and gas production volume from active wells within 1 kilometer (km) of populated areas within census block groups from 2018 to 2020. We geocoded confirmed cases and associated deaths to assess block group case and mortality rates from COVID‐19 from February 2020 to January 2021. We fit hierarchical Poisson models with individual and area covariates (e.g., age, sex, socioeconomic disadvantage), and included time and other interactions to assess additional variation (e.g., testing, reporting rates). In the first 4 months of the study period (February–May 2020), block groups in the highest tertile of oil and gas production exposure had 34% higher case rates (IRR: 1.34 95% CI: 1.20, 1.49) and 55% higher mortality rates (MRR: 1.52 95%: CI: 1.14, 2.03) than those with no estimated production, after accounting for area‐level covariates. Over the entire study period, we observed moderately higher mortality rates in the highest group (MRR: 1.16 95%: CI: 1.01, 1.33) and null associations for case rates.
Keywords: environmental epidemiology, oil production, gas production, COVID‐19, air pollution, pandemic preparedness
Key Points
Using gridded population estimates, we estimated exposure to oil and gas production in areas within 1 km of an active well
We observed higher reported case and mortality rates in areas with higher estimated oil and gas production from February to May 2020
We geocoded COVID‐19 cases and deaths to census block groups and estimated age and sex‐specific mortality rates from February 2020 to January 2021
1. Background
Between December 2019 and May 2022, there were an estimated 82 million reported cases of COVID‐19, the disease caused by SARS‐CoV‐2, and approximately 1 million linked deaths in the United States (U.S.) (Tanne, 2022). Geographic variability in the distribution of infection and associated mortality, particularly along racial and economic lines, encourages study of the systemic and environmental factors that promote severe disease (Abedi et al., 2020; Brakefield et al., 2022; Park et al., 2021). Prior research has found that environmental hazards are associated with higher risk of SARS‐CoV‐2 exposure, infection, and poorer outcomes, including mortality (Frank & Wali, 2021; Weaver et al., 2022). For example, the co‐occurrence of air pollution and higher rates of reported COVID‐19 has been suggested to partially account for differential rates of disease observed across communities as early as 1 year into the pandemic (Bourdrel et al., 2021; Carballo et al., 2022; English et al., 2022; Fairburn et al., 2019). A common but understudied environmental exposure is the drilling and operation of oil and gas wells, which have been found to result in higher concentrations of ambient air pollutants (Deziel, McKenzie, et al., 2022; Garcia‐Gonzales, Shonkoff, et al., 2019; Gonzalez, Francis, et al., 2022), including contaminants previously associated with elevated COVID‐19 risks such as nitrous dioxide (NO2) and fine particulate matter (PM2.5) (Bourdrel et al., 2021; English et al., 2022; Meo et al., 2021). In addition to air pollutants, oil drilling has been associated with transmission of water and soil and pollutants (Johnston et al., 2019) and associated activities such as transport and waste disposal, including additional noise, lighting, and other stressors (Birkholzer et al., 2015; Tran et al., 2020).
In the United States, an estimated 17.6 million residents lived within one mile (1.6 kilometers (km)) of active oil and gas wells in 2017 (Czolowski et al., 2017). Several studies have reported associations between residing near oil and gas wells and higher risk of several adverse respiratory and cardiovascular outcomes, including asthma, cancers, immunodeficiency, heart failure, higher diastolic blood pressure, and upper respiratory disease (Denham et al., 2021; Gonzalez et al., 2020; Johnston et al., 2019, 2021; Tran et al., 2020). Underlying comorbidities, and particularly cardiovascular disease, are highly associated with the development of severe COVID‐19 (Zhang et al., 2023). To our knowledge, no prior studies have examined whether exposure to oil and gas development is associated with higher rates of COVID‐19 or other respiratory infections. Furthermore, recent studies have called attention to the environmental justice dimensions of oil and gas well siting, including higher rates of siting in neighborhoods subject to historical racial discrimination from housing policy in California (Gonzalez, Nardone, et al., 2022; González et al., 2023; Kroepsch et al., 2019).
Since the beginning of the pandemic, researchers and practitioners have built substantial knowledge of effective COVID‐19 prevention, treatment, and mitigation strategies. However, further work is needed to improve understanding of critical risk factors underlying health disparities with respect to the distribution and severity of COVID‐19 infection and mortality, and to support identification and mitigation of community‐level risk factors in pandemic preparedness efforts (Curtis, 2021; Frank & Wali, 2021; Frumkin, 2021).
In the current study, our aim was to evaluate whether, in the first year of the pandemic, communities located near active oil and gas wells had higher reported COVID‐19 case rates and associated mortality. We leveraged data on the locations of oil and gas wells and diagnosed COVID‐19 cases across California, which are common: in 2020, California was the fifth most productive state for crude oil (U.S. Energy Information Administration, 2022). Approximately 1.1 million California residents live within 1 km of active wells, with disproportionately high exposure among Black, Hispanic, and socioeconomically marginalized people (González et al., 2023). During the first year of the pandemic, as the most populous state in the U.S., California accounted for approximately 13% of reported COVID‐19 cases and 9% of reported mortalities (CDC, 2020). In this study, we considered environmental, social, and individual health factors to investigate if differential exposure to oil and gas drilling may partially explain variations in COVID‐19 rates in California communities.
A list of environmental epidemiology terms used in this paper is included in Supporting Information S1.
2. Materials and Methods
2.1. Study Design and Data Sources
We conducted an ecological study to assess the association between area‐level oil and gas production and corresponding area‐level COVID‐19 case and COVID‐19 mortality rates in California. To match case data to active drilling sites, we obtained COVID‐19 case data with residential addresses, which was available for the reporting period of 1 February 2020–31 January 2021. The unit of observation for the analysis was the 2010 census block group, a geographic unit nested within census tracts and typically including 600 to 3,000 residents (U.S. Census Bureau, 2021).
We integrated data from multiple sources, including the COVID‐19 case records and area‐level hospitalization and emergency department visit rates from the California Department of Public Health (CDPH), oil and gas location and production data from the California Geologic Energy Management Division (CalGEM), and publicly available area‐level demographic and economic data from the American Community Survey (ACS) (American Community Survey, 2019), the US Census (U.S. Census Bureau, 2021), and the University of Wisconsin Neighborhood Atlas (Butler et al., 2013).
We restricted our study population to census block groups with at least 1 active oil and gas well within 10 km and at least 50 residents. Our intention was to limit unmeasured confounding under the assumption that people living within 10 km of a well are more likely to be comparable to each other than to people living 10 km or further from wells (Tran et al., 2020). As described by Deziel, Clark, et al. (2022), we used an “activity‐based metric” of total estimated production across all wells linked to a block group as an aggregated measure of physical, chemical or other stressors associated with production.
2.2. Exposure Assessment
We identified active oil and gas wells using data from the California Geologic Energy Management Division (CalGEM) (CalGEM, 2024) from 2018 to 2020, which regulates drilling and operation of wells in California. Data on oil and gas location and production volume included the coordinates for each oil and gas well, well status (e.g., active, idle, plugged), and monthly production volume in barrels of oil equivalent (BOE). We were interested in assessing exposure to oil and gas development during, and in the 2 years leading up, the COVID‐19 pandemic. We assumed that production would serve as a measure of long‐term cumulative exposure to the potential air, soil, water and other pollutants associated with oil and gas drilling over this time. We included active‐producing wells for which >0 BOE of production was reported for any month between January 2018 and December 2020.
To assess exposure to specific oil and gas wells, we first identified populated areas within census block groups using a dasymetric spatial data set produced by Depsky et al. (2022). Briefly, the authors developed a spatial layer using a statewide database of tax parcel boundaries (which are smaller than census blocks) from DMP LightBox (Nationwide Parcel Data & Property Level Geocodes|SmartParcels, 2018), a layer of building footprints for nearly 11 million buildings in California (US Building Footprints, 2019), and census block population counts to apportion the population within block groups into 100‐m population grids. Using the identified well locations from CalGEM (CalGEM, 2024), we generated 1‐, 3‐, and 10‐km buffers around each well coordinate and included all block groups where the 10‐km buffer intersected with at least one populated area within a block group (n = 8,560). This dasymetric approach to exposure assessment has been previously used to estimate area‐level exposures to oil and gas development (Casey et al., 2021; Clough & Bell, 2016).
To assign production exposure to block groups, we created three groups based on the distance from the populated areas to the identified active oil and gas wells: within 1 km (“0–1 km”), within 3 but more than 1 km (“1–3 km”), and within 10 but more than 3 km from a well (“3–10 km”) (Tran et al., 2021). Following previous approaches to measuring exposure to oil and gas production, we hypothesize that people living within 1 km of a well are very likely to be exposed production and considered this our “exposed” group. Similarly, we hypothesized that those living more than 3 km away are much less likely to be exposed and considered this our “unexposed” group. Finally, we considered the 1–3 km group to be “intermediately exposed” and included these block groups in our analyses as a comparison group for our “exposed” and “unexposed” block groups. Using these criteria, we identified 1,193 “exposed” block groups (0–1 km), 2,339 “intermediate” block groups, and 5,028 “unexposed” block groups with at least one active well 3–10 km from populated areas (Figure 1).
Figure 1.
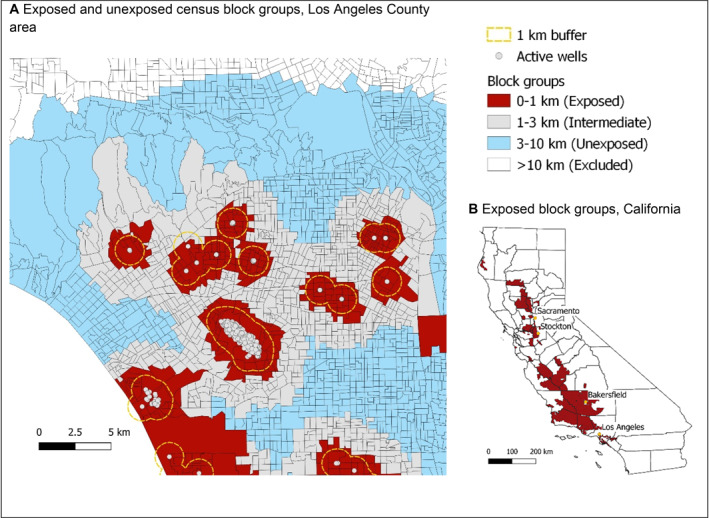
Example of exposure assignment of active oil and gas wells (2018–2020) to California census block groups using 1, 3, and 10 km radii. Panel (a) map showing the distribution of block groups assigned to the exposed group with populated areas within 1 km of an active oil or gas well (shown in red) in the Los Angeles County area. Those block groups with populated areas within 3‒10 km of an active well were considered unexposed (blue). Block groups with populated areas within 1‒3 km of an active well were intermediately exposed (grey). Block groups with populated areas greater than >10 km from an active oil or gas well were not included in analysis to reduce unmeasured confounding (white). Populated areas within census block groups are not shown in the map, only the whole census block group. Panel (b) map shows the distribution of exposed block groups groups across the state of California, and several major cities.
Finally, for all “exposed” block groups, we identified all wells within 1 km of populated areas and identified annual oil and gas production (in BOE) at these actively producing wells between January 2018 and December 2020. We then estimated the cumulative sum of total estimated BOE across all wells within 1 km of populated areas for each block group. As the exposure distribution was highly right skewed, we then created tertiles of BOE exposure to assess differential exposure to oil and gas production. This approach is similar to those used in other studies of residential proximity to oil production (Johnston et al., 2019; Tran et al., 2020).
2.3. Outcome Assessment
Confirmed and probable COVID‐19 cases and COVID‐19‐related deaths among California residents registered in the surveillance system and with residential address data were available from the California Department of Public Health (CDPH) from 1 February 2020 to 31 January 2021. Using the approach of English et al. (2022), we identified cases with age, sex, and residential address data, and used geocoding to generate point locations and identify each study subject's block group of residence at the time of diagnosis using 2010 census block group boundaries (U.S. Census Bureau, 2021). To allow for at least 30 days of follow up, we only included deaths among COVID‐19 cases identified by 31 December 2020. We also excluded residents with a reported age over 110 years (<0.01%).
To estimate the total population at risk within our block groups, we collected age and sex‐stratified population denominators from the American Community Survey (ACS) 2019 5‐year estimates (American Community Survey, 2019). We assigned 1 year of person‐time per resident to each block group to estimate COVID‐19 incidence rates. As we only included deaths for an 11‐month period (February 2020–December 2020), we assigned 0.9 years of person‐time per resident to each block group to calculate COVID‐19 mortality rates.
2.4. Covariates
Covariates of interest were identified a priori based on existing research on risk factors for infection and severity of COVID‐19, as well as for ambient air pollution exposure and poor health outcomes (Gonzalez, Francis, et al., 2022; Gonzalez et al., 2020). A Directed Acyclic Graph is included in Supporting Information S1.
Individual‐level covariates: Individual age at infection, self‐reported sex, and dates of infection and death were obtained from CDPH case records. As we could not directly measure key temporal factors, including changes in COVID‐19 testing availability and use, shifts in public awareness and behaviors at the relevant geographic scale, we assessed time trends in our models by grouping outcomes into three time periods based on nationwide disease trends, similar to the approach of Lipsitt et al. (2021). We established three 4‐month periods: February–May 2020 (early pandemic period), June–September 2020 (summer surge), and October–January 2021 (fall surge); these dates aligned with patterns observed in our data (Figure S1 in Supporting Information S1). For analyses investigating the rates of COVID‐19 mortality, we shortened the final period to October–December 2020, to allow for 30 days of follow up as specified previously. We further grouped cases and deaths by age group and binary sex (male/female) to generate stratified estimates. To avoid generating too many empty strata in areas with a small population, we grouped age into four categories consistent with COVID‐19 risk thresholds (CDC, 2022): 0–19, 20–44, 45–65, >65 years. Accordingly, we generated up to 24 strata per block group (ex: “February–May 2020/female/0–19 years old,” “February–May 2020/male/0–19 years old,” etc.).
Block‐group level covariates: We measured race and ethnicity demographics at the block group level due to high missingness in the case data (>75%) and research linking area demographics with disproportionate rates of COVID‐19 mortality and oil and gas exposure (Abedi et al., 2020; Brakefield et al., 2022; Glance et al., 2021; González et al., 2023). Specifically, we determined the proportion of block group populations who were Hispanic/Latino of any race, non‐Hispanic Asian, non‐Hispanic Black, non‐Hispanic White, or who identified with another racial/ethnic group not covered by those categories. Based on prior studies of oil and gas extraction activities in rural versus urban areas, we categorized block groups as urban if they had at least 60% overlap with census‐defined urban areas and as rural otherwise. Finally, we collected 2018 Area Deprivation Index (ADI) ranking for California block groups from the University of Wisconsin's Neighborhood Atlas (Butler et al., 2013; Kind & Buckingham, 2018; University of Wisconsin, 2020), which includes factors for theoretical domains of income, education, employment, and housing quality, given prior research linking economic disparities to oil and gas exposure (Gonzalez, Francis, et al., 2022). Our approach to the hypothesized relationship between our measured covariates is further described in our Directed Acyclic Graph (Figure S2 in Supporting Information S1).
2.5. Statistical Models
To account for multiple observations per census block group and for spatial clustering of census block groups within census tracts, we employed three‐level hierarchical Poisson models for our two outcomes of interest, diagnosed COVID‐19 cases and COVID‐19 deaths (Paciorek, 2010). Specifically, we used random intercept models with clustering of block groups within tracts. We examined both crude and adjusted models with covariates. To allow for improved model fit, we also tested negative binomial and zero‐inflated Poisson models using Akaike Information Criteria (AIC) (Lee et al., 2006). All analyses were conducted using R Statistical Software using the “lme4” and “glmmTMB” packages (v4.2.1; RStudio Team, 2020).
We additionally conducted a series of interaction analyses to further investigate the potential relationship between production and COVID‐19 outcomes within subgroups. Specifically, we assessed statistical interaction and report stratified estimates for age group and Area Deprivation Index, categorizing the latter into three groups (levels 1–4, 5–7, and 8–10). We did not include racial demographics due to missingness in the case data, as we did not believe area‐level measures would be sufficient to assess interaction.
2.6. Sensitivity Analyses
As a sensitivity analysis, we also estimated quartiles and quantiles of block‐group level oil and gas production in addition to tertiles. We also tested the addition of area‐level health outcomes as covariates in our models. Specifically, we obtained the age‐adjusted rates of emergency department (ED) visits in block groups from 2017 to 2019 for asthma, diabetes, obesity, pulmonary hypertension, and heart failure. Studies have linked each of these outcomes to our air pollution and production measures, but they may also occur more frequently in areas where oil and gas wells are located due to other environmental hazards or spatially distributed health disparities (Brakefield et al., 2022; Fairburn et al., 2019; Gonzalez, Nardone, et al., 2022). Mediation analysis was outside the scope of this sensitivity analysis as these health outcomes could act both as potential confounders (preceding the exposure) or potential mediators (consequences of the exposure) (Brakefield et al., 2022; Frank & Wali, 2021). Finally, although the focus of this study is the total effect of residence near oil and gas production, we also assessed average annual estimated NO2 and PM2.5 concentrations within our study blocks from 2018 to 2020 using block group‐level concentration estimates developed by the Center for Air, Climate and Energy Solutions using v1 empirical models as described by Kim et al. (2020).
3. Results
There were 3,221,507 confirmed cases of COVID‐19 and 43,036 linked deaths identified by CDPH during the study period and successfully geocoded. Of these, 1,358,106 (42.2%) cases and 24,006 (55.8%) deaths occurred in the 8,560 census block groups included in the final sample of exposed and unexposed block groups within 10 km of at least one active‐producing oil and gas well. Across our study sample, case and mortality rates of COVID‐19 increased over the course of the study period, with the highest case rates among people aged 20–44 and the highest mortality rates among persons over 65 (Figure S1 in Supporting Information S1).
Block groups with active oil and gas wells were more likely to be rural, have less estimated area deprivation (lower ADI), a higher proportion of non‐Hispanic Black residents and a lower proportion of non‐Hispanic Asian residents (Table 1). Block groups with higher COVID‐19 case rates were less likely to be rural, more likely to have a higher proportion of Hispanic/Latino residents and non‐Hispanic Black residents, and to have higher levels of deprivation. We observed similar patterns for block groups with higher mortality rates (Table S1 in Supporting Information S1).
Table 1.
Characteristics of Census Block Groups (BGs) Within 10 km of an Active Oil and Gas Well, California, 1 February 2020–31 January 2021 (n = 8,560)
| Distance from an active well | 3–10 km | 1–3 km | 0–1 km | – | ||
| Production tertile (0–1 km only) | ||||||
| Exposure classification (n) | Unexposed (5,028 BGs) | Intermediate (2,339 BGs) | Lowest (399 BGs) | Middle (398 BGs) | Highest (396 BGs) | All (n = 8,560) |
| Average annual barrel of oil equivalent (BOE), (range (average)) | 0.5–3,104 (1,271) | 3,123–27,936 (12,741) | 27,936–3,068,014 (154,785) | 0–3,068,014 (56,168) | ||
| Age group proportion (mean) | ||||||
| 20–44 years | 35.1 | 36.9 | 34.9 | 36.8 | 35.6 | 35.7 |
| 45–64 years | 25.7 | 25.1 | 25.7 | 25.4 | 26.8 | 25.6 |
| >65 years | 14.1 | 14.0 | 14.7 | 14.3 | 15.9 | 14.1 |
| Percent female (mean) | 50.0 | 50.0 | 50.0 | 50.0 | 50.0 | 50.0 |
| Area rurality* (mean) | 5.0 | 3.8 | 16.5 | 16.1 | 15.4 | 6.2 |
| Race/Ethnicity of BG (mean) | ||||||
| Hispanic/Latino | 46.2 | 45.7 | 45.5 | 39.5 | 33.5 | 45.2 |
| Non‐Hispanic Asian | 14.5 | 11.7 | 10.8 | 10.7 | 11.3 | 13.3 |
| Non‐Hispanic Black | 5.0 | 8.0 | 6.1 | 8.1 | 10.5 | 6.5 |
| Non‐Hispanic White | 31.2 | 30.3 | 33.9 | 38.3 | 41.0 | 31.8 |
| ADI** State Rank (CA) (%) | ||||||
| 1–2 | 13.4 | 20.2 | 21.1 | 20.9 | 29.0 | 16.7 |
| 3–4 | 24.7 | 20.6 | 19.3 | 20.4 | 26.0 | 23.2 |
| 5–6 | 26.8 | 24.6 | 19.8 | 22.6 | 16.2 | 25.2 |
| 7–8 | 11.3 | 22.1 | 20.1 | 17.8 | 16.4 | 22.1 |
| 9–10 | 11.3 | 11.3 | 18.8 | 16.3 | 10.1 | 11.8 |
| Unavailable | 0.8 | 1.2 | 1.0 | 2.0 | 2.3 | 1.0 |
| Median age‐adjusted ED visit rate (per 10,000 residents) | ||||||
| Asthma | 179 | 179 | 179 | 180 | 190 | 179 |
| Diabetes | 466 | 455 | 474 | 462 | 430 | 460 |
| Heart failure | 153 | 150 | 141 | 150 | 150 | 150 |
| Obesity | 158 | 144 | 138 | 150 | 145 | 149 |
| Pulmonary hypertension | 23 | 22 | 20 | 23 | 28 | 23 |
Note. *Area rurality is defined as the proportion of the block group total area overlapping with census urban area polygons. **ADI, area deprivation index; higher ADI values indicate higher degree of deprivation.
COVID‐19 cases: Across the entire study period we did not observe an association between oil and gas production and COVID‐19 cases (Table 2). In interaction models, we did observe statistically significant interaction by period, and in our time‐stratified models, we found that after accounting for potential confounders, all levels of production volume were positively associated with COVID‐19 case rates in the first 4 months (February–May 2020). Specifically, we observed 34% higher rates of reported disease (IRR: 1.34, 95% CI (1.20, 1.49)) in block groups with the highest production volume compared to unexposed block groups (Table 2). Across the lower two production tertiles, the relationship persisted in the second period, with a slight reduction in the relative rate; across all three tertiles, the relationship attenuated to the null in the third and final period. Across all models, we observed high variance between block groups, although the between‐tract variance was reduced with the inclusion of our specified covariates.
Table 2.
Incidence Rate Ratios (IRR 95% CI) and Mortality Rate Ratios (MRR 95% ICI) of Confirmed COVID‐19 Cases in CA Block Groups (BGs), February 2020–January 2021 (n = 8,560 BGs)
| Incidence Rate Ratios (February 2020–January 2021) | |||||||
|---|---|---|---|---|---|---|---|
| Reference: no estimated production (n = 5,028) | Stratified by time period | ||||||
| BOE (range) | Crude | Adjusted a | +Comorbidities a , b | February–May 2020 a | June–September 2020 a | October–January 2021 a | |
| Exposure to oil and gas production (BOE) | |||||||
| Lowest tertile (n = 399) | 0,4–3,104 | 0.98, (0.92,1.04) | 1.00, (0.96,1.05) | 1.00, (0.96,1.04) | 1.12, (1.01,1.24) | 1.05, (1.00,1.12) | 0.98, (0.93,1.02) |
| Middle tertile (n = 398) | 3,123–27,936 | 0.91, (0.86,0.97) | 0.97, (0.93,1.02) | 0.97, (0.93,1.01) | 1.10, (0.99,1.22) | 1.03, (0.97,1.09) | 0.95, (0.91,1.00) |
| Highest tertile (n = 396) | 28,050–3,068,014 | 0.86, (0.81,0.92) | 0.98, (0.94,1.03) | 0.96, (0.92,1.01) | 1.34, (1.20,1.49) | 1.00, (0.94,1.06) | 0.95, (0.90,0.99) |
| Intermediate (n = 2,339) | – | 0.99, (0.96,1.03) | 0.99, (0.97,1.01) | 1.00, (0.97,1.02) | 1.16, (1.10,1.22) | 1.01, (0.98,1.04) | 0.97, (0.95,1.00) |
| Tract:BG variance | 0.33 | 0.35 | 0.33 | 0.69 | 0.46 | 0.37 | |
| Tract variance | 0.53 | 0.18 | 0.16 | 0.70 | 0.34 | 0.25 | |
| Mortality Rate Ratios (February 2020–December 2020) | |||||||
|---|---|---|---|---|---|---|---|
| Reference: no estimated production (n = 5,028) | Stratified by time period | ||||||
| BOE (range) | Crude | Adjusted a | +Comorbidities a , b | February–May 2020 a | June–September 2020 a | October–December 2020 a | |
| Exposure to oil and gas production (BOE) | |||||||
| Lowest tertile (n = 399) | 0,4–3,104 | 0.95, (0.82,1.09) | 1.01, (0.88,1.15) | 0.99, (0.87,1.13) | 1.23, (0.92,1.65) | 0.99, (0.81,1.21) | 0.96, (0.83,1.11) |
| Middle tertile (n = 398) | 3,123–27,936 | 0.80, (0.69,0.93) | 0.94, (0.82,1.09) | 0.94, (0.82,1.08) | 0.81, (0.58,1.15) | 1.02, (0.83,1.26) | 0.96, (0.83,1.12) |
| Highest tertile (n = 396) | 28,050–3,068,014 | 1.00, (0.86,1.16) | 1.16, (1.01,1.33) | 1.13, (0.99,1.30) | 1.52, (1.14,2.03) | 0.95, (0.76,1.19) | 1.07, (0.92,1.24) |
| Intermediate (n = 2,339) | – | 1.03, (0.95,1.10) | 1.03, (0.97,1.10) | 1.04, (0.97,1.11) | 1.25, (1.08,1.44) | 0.99, (0.90,1.10) | 0.98, (0.91,1.05) |
| Tract:BG variance | 0.79 | 0.79 | 0.79 | 1.44 | 1.01 | 0.77 | |
| Tract variance | 0.57 | 0.33 | 0.31 | 0.67 | 0.40 | 0.45 | |
Note. We used 3‐level random intercept Poisson models to assess the relationship between area‐level exposure to oil and gas production (BOE) and reported COVID‐19 incidence. Crude and Adjusted models cover the entire study period.
Adjusted for individual age category and sex, block group level census proportions of non‐Hispanic Black, non‐Hispanic White, non‐Hispanic Asian, and Hispanic identified population, rurality, and time period.
Adjusted additionally for census tract‐level rates of ED visits for asthma, COPD, heart failure, pulmonary hypertension, diabetes, and obesity in a subset of blocks group where data were available (n = 8,559 block groups).
COVID‐19 deaths: Across the entire study period, we observed a higher mortality rate in block groups in the highest estimated production tertile (MRR: 1.16, 95% CI: 1.01, 1.33). In our time‐stratified models, we observed the strongest association between the highest production block groups and COVID‐19 mortality (MRR: 1.52, 95% CI: 1.14, 2.03) in the first 4 months (February–May 2020); there was also an association in the first production tertile, though it was not statistically significant (MRR: 1.23, 95% CI: 0.92, 1.65). Conversely, we observed a negative association for the middle tertile (MRR: 0.81, 95% CI: 0.58, 1.15), although all exposed block groups trended toward the null in the final 5 months of the study. As with cases, we observed significant between‐block group variance across our estimates and particularly high variance in the time‐stratified models.
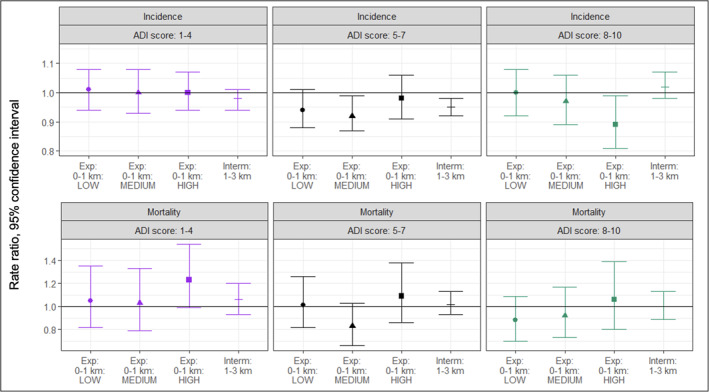
Stratified analysis: We did not observe statistical interaction across most categories of Area Deprivation Index or age. In our stratified results, we observed an association between the highest level of production and case rates in the over 65 population and with mortality rates in the over 45 population (Figure 2). Across Area Deprivation Index categories, the association varied more substantially from the main result for both cases and deaths (Figure 3). In addition to looking across the entire study, we conducted ADI and age group interaction tests and stratified results for the first 4‐month time period (Figure S5 in Supporting Information S1).
Figure 2.
Incidence Rate Ratios (IRR 95% CI) and Mortality Rate Ratios (MRR 95% ICI) of confirmed COVID‐19 Cases in CA Block Groups (BGs) stratified by Area Deprivation Index score, February 2020–January 2021 (n = 8,472 BGs). *88 block groups were not assigned an ADI score (assigned a different value related to low or congregate populations), and were excluded from the stratified analysis. The rate ratios described follow the methods in Table 2, and specifically the “adjusted” models. “Exp” refers to “exposed” block groups; “Interm” refers to “intermediately exposed” block groups.
Figure 3.
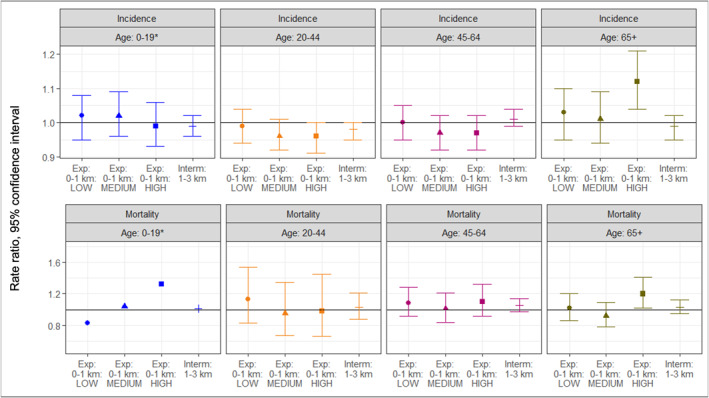
Incidence Rate Ratios (IRR 95% CI) and Mortality Rate Ratios (MRR 95% ICI) of confirmed COVID‐19 Cases in CA Block Groups (BGs) stratified by area‐level age groups, February 2020–January 2021 (n = 8,560 BGs). *95% confidence interval estimates that exceeded 0.5 and 1.5 were excluded from the graphic to allow comparability across results. The rate ratios described follow the methods in Table 2, and specifically the “adjusted” models. “Exp” referes to “exposed” block gropus; “Interm” refers to intermediately exposed block groups.
Sensitivity analyses: The results of our sensitivity analyses did not change our overall conclusions; as seen in Table 2, adjustment for specified comorbidities did not substantially change our estimates. Similarly, assessing exposure in quartiles and quintiles, rather than tertiles, did not substantially change our conclusions (Figure S2 in Supporting Information S1) and reflected similar variability to tertiles.
4. Discussion
We examined the relationship between residential proximity to oil and gas production and reported COVID‐19 case and mortality rates. In the early months of the COVID‐19 pandemic, we found higher rates of both disease and mortality in block groups near active production, and the strongest association among groups at the highest estimated level of production. Across the entire study period, we observed an association between production and mortality for block groups only at the highest level of exposure, but did not observe an association between estimated block‐group level production and COVID‐19 case rates. To our knowledge, this is the first study to investigate the relationship between exposure to oil and gas development and COVID‐19. Under the assumption that production volume correlates with air pollution, the mix of null and positive findings is consistent with studies of people exposed to ambient air pollutants such as PM2.5, PM10, NO2, and ozone (Carballo et al., 2022; English et al., 2022), particularly with longer‐term exposure, and to respiratory illness related to drilling (Dahlgren et al., 2007; Johnston et al., 2021). Overall, our results support further research into both the environmental drivers of COVID‐19 spread, and further consideration of the potential impacts of oil and gas production on population health.
Across the entire study period, we generally observed null or inconsistent associations between our exposure and outcome; however, in the earliest time period of the pandemic, we observed higher COVID‐19 case and mortality rates among communities with presumed exposure to oil and gas production, particularly at the highest levels of production. Although we did not have time‐varying data on testing or response measures at the block group level, at the beginning of the pandemic, testing resources were limited and sometimes included restricted access, resulting in significant under detection of cases. For example, in July 2020, California state officials adopted new testing guidance with 4 tiers of prioritization related to symptom presentation, disease severity, contact tracing, employment and other factors (Luna, 2020). If residents with more severe or symptomatic disease were more likely to be detected in the first period, this may suggest that exposed residents living near oil and gas wells were more likely to progress to symptomatic or severe disease, resulting in higher case rates. This hypothesis is supported by concurrently higher mortality rates and across the entire study period, as they represent both further disease progression and are less likely to be under detected (Park et al., 2021). Mechanisms and pathways by which drilling‐related activities may have enhanced vulnerability to COVID‐19 infection or increased mortality risk include decreased immune response, higher susceptibility and severity through the impacts of air pollution or other associated stressors on chronic disease incidence, or the effects of air pollution on the persistence of viral particles in the air, facilitating viral penetration and infection (Bourdrel et al., 2021). Prior studies have found drilling and operating oil and gas wells results in higher concentrations of PM2.5, ozone, volatile organic compounds, and other ambient air pollutants (Garcia‐Gonzales, Shamasunder, & Jerrett, 2019; Garcia‐Gonzales, Shonkoff, et al., 2019; Gonzalez, Francis, et al., 2022); although we did not have information on other sources of air pollution for this study, we observed variable rates of NO2 and PM2.5 across our included block groups (Supporting Information S1). It is also possible that communities with historical exposure to oil and gas production may have been at increased susceptibility to infection at a time when prevention and treatment knowledge was limited, resulting in higher transmission and mortality. While our study may be underpowered to examine the association between production and COVID‐19 in subgroups, we did observe some variability by age and area‐level socioeconomic measures; this was true both of the entire study period, and in a focused review of the February–May period (Supporting Information S1).
Within the incidence rate ratios from February to May 2020, both the lower and middle tertiles of the exposed group and the intermediately exposed group had higher rates of confirmed COVID‐19 cases when compared to the unexposed group, but lower rates than the most highly exposed group. This may represent a dose‐response relationship and a potential threshold but may also represent residual spatial confounding. For deaths, the positive associations were not monotonic, and across all our estimates, we observed high variance estimates for our random effects. This is likely the result of true variability between block groups and may come from unknown and unmeasured factors (e.g., testing availability, public behavior, treatment knowledge and availability, shifts in public health policy), that are likely to have affected SARS‐CoV‐2 spread, severity and reporting and detection rates.
For both cases and deaths, the mix of positive and null findings is consistent with results from a 2022 systematic review of air pollution and COVID‐19, which reported that around half of studies, most of which were also ecological, found a positive relationship between air pollution and infection or mortality (Carballo et al., 2022). However, it is worth noting that in our analysis, the positive associations between oil and gas production and rates of COVID‐19 mortality persist even when controlling for age, sex, SES characteristics, and comorbidities, and with methods to account for spatial clustering. As our analysis was conducted before highly effective COVID‐19 vaccines became widely available, with only 1.8% of people in California having completed a primary vaccine series by 1st February 2021, we do not expect differential vaccination rates would have significantly impacted the association results (California, 2023); similarly, we do not expect a large proportion of cases to be reinfections as our analysis was limited to the first year. Finally, in our sensitivity analysis of quantiles and quintiles (Figure S3 in Supporting Information S1), although we did observe some differences in our estimates using a different exposure quantile, particularly for deaths, they did not shift our conclusions.
4.1. Limitations
Given constraints in the health data set, we were only able to assess exposure to active‐producing oil and gas wells based on proximity to the block group of residence. This method may result in misclassification of exposures at locations other than the residence or for individuals who changed residences during the study period and does not provide information on duration or intensity of individualized exposure. Pollutant emissions from oil and gas wells may have fluctuated and people may have moved over the course of the study period, leading to potential exposure misclassification. Additionally, our exposure measurement precludes identification of specific pathways through which exposures to active‐producing wells may affect COVID‐19 outcomes, which could include stressors associated with air and water pollution, noise, and excessive light. The cumulative exposure–response curve of all of the potential hazards and health outcomes may differ than that for each individual pathway (Morello‐Frosch et al., 2011). Nevertheless, surrogate measures of population exposures to active oil and gas production, including proximity to wells and production volume, are useful aggregate measures of the potential cumulative chemical, physical, and social stressors and exposure pathways associated with oil and gas development (Johnston et al., 2019). Numerous prior epidemiological studies have assessed exposure to oil and gas development using residential proximity, and this approach has the advantage of capturing the complex the mixture of plausible etiologic agents associated with this exposure (Deziel, Clark, et al., 2022).
It was not feasible to conduct an individual‐level study in this analysis due the lack of a control population and data quality concerns; as a population‐level study, we cannot directly approximate individual risk of COVID‐19 and related mortality given exposure to well production. Case data reported to CDPH are unlikely to be completely accurate due to limited testing access in the first several months of the pandemic, and access to testing and reporting of these results likely varied both between and within block groups and over time. In employing random effects, we looked to quantify residual variance related to the exposure; we also note that hierarchical models require correct specification of the latent variable, an assumption which is not testable (Austin, 2017). Furthermore, there was no feasible way to identify false positives among the cases. Case data was also missing information on treatment and symptoms, precluding our ability to investigate disease severity. Although we did investigate the timing, we were not able to control for all ways in which time trends may have influenced our effect estimates. Additionally, geocoded confirmed case data was only available until 31 January 2021, limiting our assessment to a time before testing was more broadly available. Finally, the lack of individual data on race, ethnicity, and underlying health precluded us from further investigating the additional ways in which these factors may affect the exposure‐outcome relationship.
As researchers appropriately identify the limitations of the many recent studies of COVID‐19 and air pollution (Conte et al., 2024), we believe that our methods, our identification of specific wells and production estimates, and our efforts to examine the relationship in the context of overlapping social and environmental risk factors helped us to limit residual confounding and may be built upon in future research. Finally, given the demographic and geographic diversity within California, our findings may be generalizable to other regions with oil and gas development near residential areas.
4.2. Conclusion
In this study, we assessed whether residential proximity to oil and gas production was associated with higher rates of reported COVID‐19 cases and related deaths. While we observed a mix of positive and null findings across the study period, elevated case and mortality rates in the first 4 months of the pandemic suggest that communities near to oil and gas production may have been disproportionately affected by severe disease at a time when testing and treatment options were more limited. Additional research in this area, particularly at the individual level, may help further characterize the observed variability and to elucidate the biological mechanisms through which exposure to environmental pollutants may affect risk for COVID‐19 and related diseases. Furthermore, it may help to identify potential health impacts of oil and gas production and to identify community‐level risk factors that are associated with severe respiratory disease outcomes, particularly given higher rates of production in communities with a higher proportion of Black residents. Overall, this study contributes to the evidence on adverse health effects related to oil and gas production and supports policy guidance around the mitigation of hazards associated with new and active wells (Deziel, McKenzie, et al., 2022) and equitable pandemic preparedness.
Conflict of Interest
The authors declare no conflicts of interest relevant to this study.
Supporting information
Supporting Information S1
Acknowledgments
The authors thank Julie von Behren and Gina Solomon for their additional support of this project. The California Department of Public Health (CDPH) provided the data on SARS‐CoV‐2 infections and COVID‐19 deaths. Data on oil and gas well production was provided by the California Air Resources Board contract 19RD029. Support for this research was provided by core center Grant P30‐ES030284 from the National Institute of Environmental Health Sciences, National Institutes of Health, and the Center on Race, Poverty & the Environment. The statements and conclusions in this manuscript are those of the authors and do not necessarily represent those of the CDPH.
Archer, H. , González, D. J. X. , Walsh, J. , English, P. , Reynolds, P. , Boscardin, W. J. , et al. (2024). Upstream oil and gas production and community COVID‐19 case and mortality rates in California, USA. GeoHealth, 8, e2024GH001070. 10.1029/2024GH001070
All authors have contributed to and reviewed the manuscript as aligned with CRediT taxonomy.
Contributor Information
Helena Archer, Email: hiarcher@berkeley.edu.
Rachel Morello‐Frosch, Email: rmf@berkeley.edu.
Data Availability Statement
Data from the US Census, the American Community Survey, and the University of Wisconsin are publicly available and accessible through their respective websites (American Community Survey, 2019; University of Wisconsin, 2020; U.S. Census Bureau, 2021). Gridded population sociodemographic estimates from California from Depsky et al. (2022), may be accessed through Github as described in their published article (https://pubmed.ncbi.nlm.nih.gov/35834564/). Oil and gas data are available from CalGEM through the WellSTAR portal (CalGEM, 2024). Data supporting this research on health outcomes are available from the California Department of Public Health and are not accessible to the public or research community due to restrictions around human subjects approval (IRB) and data use agreements. Researchers may gain access by reaching out to the department directly to propose research topic and negotiate data use agreements. Software used in this study includes R Studio (RStudio Team, 2020) and QGIS (QGIS.org, 2024) for data management and data visualizations.
References
- Abedi, V. , Olulana, O. , Avula, V. , Chaudhary, D. , Khan, A. , Shahjouei, S. , et al. (2020). Racial, economic, and health inequality and COVID‐19 infection in the United States. Journal of Racial and Ethnic Health Disparities, 8(3), 1–11. 10.1007/s40615-020-00833-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Community Survey . (2019). 2019: ACS 5‐year estimate detailed tables [Table B01001] [Dataset]. US Census Bureaus. Retrieved from https://data.census.gov/table/ACSDT5Y2019.B01001?g=0400000US06$150000&y=2019&d=ACS%205‐Year%20Estimates%20Detailed%20Tables
- Austin, P. C. (2017). A tutorial on multilevel survival analysis: Methods, models and applications. International Statistical Review, 85(2), 185–203. 10.1111/insr.12214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birkholzer, J. T. , Camarillo, M. K. , Foxall, W. , Houseworth, J. , Jin, L. , Lindsey, N. J. , et al. (2015). An independent scientific assessment of well stimulation in California volume II: Potential environmental impacts of hydraulic fracturing and acid stimulations (LBNL‐189356). California Council on Science and Technology. 10.2172/1236176 [DOI] [Google Scholar]
- Bourdrel, T. , Annesi‐Maesano, I. , Alahmad, B. , Maesano, C. N. , & Bind, M.‐A. (2021). The impact of outdoor air pollution on COVID‐19: A review of evidence from in vitro, animal, and human studies. European Respiratory Review, 30(159), 200242. 10.1183/16000617.0242-2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brakefield, W. S. , Olusanya, O. A. , White, B. , & Shaban‐Nejad, A. (2022). Social determinants and indicators of COVID‐19 among marginalized communities: A scientific review and call to action for pandemic response and recovery. Disaster Medicine and Public Health Preparedness, 17, 1–28. 10.1017/dmp.2022.104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler, D. C. , Petterson, S. , Phillips, R. L. , & Bazemore, A. W. (2013). Measures of social deprivation that predict health care access and need within a rational area of primary care service delivery. Health Services Research, 48(2 Pt 1), 539–559. 10.1111/j.1475-6773.2012.01449.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- CalGEM . (2024). California geologic energy management division (CalGEM) [Dataset]. WellSTAR. Retrieved from https://wellstar‐public.conservation.ca.gov/General/Home/PublicLanding
- California, S. of . (2023). Vaccination data. https://covid19.ca.gov/vaccination‐progress‐data/
- Carballo, I. H. , Bakola, M. , & Stuckler, D. (2022). The impact of air pollution on COVID‐19 incidence, severity, and mortality: A systematic review of studies in Europe and North America. Environmental Research, 215, 114155. 10.1016/j.envres.2022.114155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Casey, J. A. , Cushing, L. , Depsky, N. , & Morello‐Frosch, R. (2021). Climate justice and California’s methane superemitters: Environmental equity assessment of community proximity and exposure intensity. Environmental Science & Technology, 55(21), 14746–14757. 10.1021/acs.est.1c04328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- CDC . (2020). Cases, data, and surveillance. Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/coronavirus/2019‐ncov/covid‐data/investigations‐discovery/hospitalization‐death‐by‐age.html [Google Scholar]
- CDC . (2022). Risk for COVID‐19 infection, hospitalization, and death by age group [Data and Surveillance]. Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/coronavirus/2019‐ncov/covid‐data/investigations‐discovery/hospitalization‐death‐by‐age.html#print [Google Scholar]
- Clough, E. , & Bell, D. (2016). Just fracking: A distributive environmental justice analysis of unconventional gas development in Pennsylvania, USA. Environmental Research Letters, 11(2), 025001. 10.1088/1748-9326/11/2/025001 [DOI] [Google Scholar]
- Conte, M. N. , Gordon, M. , Swartwood, N. A. , Wilwerding, R. , & Yu, C. A. (2024). Observational studies generate misleading results about the health effects of air pollution: Evidence from chronic air pollution and COVID‐19 outcomes. PLoS One, 19(1), e0296154. 10.1371/journal.pone.0296154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtis, L. (2021). PM2.5, NO2, wildfires, and other environmental exposures are linked to higher COVID 19 incidence, severity, and death rates. Environmental Science and Pollution Research International, 28(39), 54429–54447. 10.1007/s11356-021-15556-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Czolowski, E. D. , Santoro, R. L. , Srebotnjak, T. , & Shonkoff, S. B. C. (2017). Toward consistent methodology to quantify populations in proximity to oil and gas development: A national spatial analysis and review. Environmental Health Perspectives, 125(8), 086004. 10.1289/EHP1535 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dahlgren, J. , Takhar, H. , Anderson‐Mahoney, P. , Kotlerman, J. , Tarr, J. , & Warshaw, R. (2007). Cluster of systemic lupus erythematosus (SLE) associated with an oil field waste site: A cross sectional study. Environmental Health, 6(1), 8. 10.1186/1476-069X-6-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Denham, A. , Willis, M. D. , Croft, D. P. , Liu, L. , & Hill, E. L. (2021). Acute myocardial infarction associated with unconventional natural gas development: A natural experiment. Environmental Research, 195, 110872. 10.1016/j.envres.2021.110872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Depsky, N. J. , Cushing, L. , & Morello‐Frosch, R. (2022). High‐resolution gridded estimates of population sociodemographics from the 2020 census in California. PLoS One, 17(7), e0270746. 10.1371/journal.pone.0270746 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deziel, N. C. , Clark, C. J. , Casey, J. A. , Bell, M. L. , Plata, D. L. , & Saiers, J. E. (2022). Assessing exposure to unconventional oil and gas development: Strengths, challenges, and implications for epidemiologic research. Current Environmental Health Reports, 9(3), 436–450. 10.1007/s40572-022-00358-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deziel, N. C. , McKenzie, L. M. , Casey, J. A. , McKone, T. E. , Johnston, J. E. , Gonzalez, D. J. X. , et al. (2022). Applying the hierarchy of controls to oil and gas development. Environmental Research Letters, 17(7), 071003. 10.1088/1748-9326/ac7967 [DOI] [PMC free article] [PubMed] [Google Scholar]
- English, P. B. , Von Behren, J. , Balmes, J. R. , Boscardin, J. , Carpenter, C. , Goldberg, D. E. , et al. (2022). Association between long‐term exposure to particulate air pollution with SARS‐CoV‐2 infections and COVID‐19 deaths in California, U.S.A. Environmental Advances, 9, 100270. 10.1016/j.envadv.2022.100270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairburn, J. , Schüle, S. A. , Dreger, S. , Karla Hilz, L. , & Bolte, G. (2019). Social Inequalities in exposure to ambient air pollution: A systematic review in the WHO European region. International Journal of Environmental Research and Public Health, 16(17), 3127. 10.3390/ijerph16173127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frank, L. D. , & Wali, B. (2021). Treating two pandemics for the price of one: Chronic and infectious disease impacts of the built and natural environment. Sustainable Cities and Society, 73, 103089. 10.1016/j.scs.2021.103089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frumkin, H. (2021). COVID‐19, the built environment, and health. Environmental Health Perspectives, 129(7), 75001. 10.1289/EHP8888 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garcia‐Gonzales, D. A. , Shamasunder, B. , & Jerrett, M. (2019). Distance decay gradients in hazardous air pollution concentrations around oil and natural gas facilities in the city of Los Angeles: A pilot study. Environmental Research, 173, 232–236. 10.1016/j.envres.2019.03.027 [DOI] [PubMed] [Google Scholar]
- Garcia‐Gonzales, D. A. , Shonkoff, S. B. C. , Hays, J. , & Jerrett, M. (2019). Hazardous air pollutants associated with upstream oil and natural gas development: A critical synthesis of current peer‐reviewed literature. Annual Review of Public Health, 40(1), 283–304. 10.1146/annurev-publhealth-040218-043715 [DOI] [PubMed] [Google Scholar]
- Glance, L. G. , Thirukumaran, C. P. , & Dick, A. W. (2021). The unequal burden of COVID‐19 deaths in counties with high proportions of black and Hispanic residents. Medical Care, 59(6), 470–476. 10.1097/MLR.0000000000001522 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzalez, D. J. X. , Francis, C. K. , Shaw, G. M. , Cullen, M. R. , Baiocchi, M. , & Burke, M. (2022). Upstream oil and gas production and ambient air pollution in California. The Science of the Total Environment, 806(Pt 1), 150298. 10.1016/j.scitotenv.2021.150298 [DOI] [PubMed] [Google Scholar]
- González, D. J. X. , Morton, C. M. , Hill, L. A. L. , Michanowicz, D. R. , Rossi, R. J. , Shonkoff, S. B. C. , et al. (2023). Temporal trends of racial and socioeconomic disparities in population exposures to upstream oil and gas development in California. GeoHealth, 7(3), e2022GH000690. 10.1029/2022GH000690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzalez, D. J. X. , Nardone, A. , Nguyen, A. V. , Morello‐Frosch, R. , & Casey, J. A. (2022). Historic redlining and the siting of oil and gas wells in the United States. Journal of Exposure Science and Environmental Epidemiology, 33(1), 76–83. 10.1038/s41370-022-00434-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzalez, D. J. X. , Sherris, A. R. , Yang, W. , Stevenson, D. K. , Padula, A. M. , Baiocchi, M. , et al. (2020). Oil and gas production and spontaneous preterm birth in the San Joaquin Valley, CA: A case‐control study. Environmental Epidemiology, 4(4), e099. 10.1097/EE9.0000000000000099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston, J. E. , Enebish, T. , Eckel, S. P. , Navarro, S. , & Shamasunder, B. (2021). Respiratory health, pulmonary function and local engagement in urban communities near oil development. Environmental Research, 197, 111088. 10.1016/j.envres.2021.111088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston, J. E. , Lim, E. , & Roh, H. (2019). Impact of upstream oil extraction and environmental public health: A review of the evidence. The Science of the Total Environment, 657, 187–199. 10.1016/j.scitotenv.2018.11.483 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, S.‐Y. , Bechle, M. , Hankey, S. , Sheppard, L. , Szpiro, A. A. , & Marshall, J. D. (2020). Concentrations of criteria pollutants in the contiguous U.S., 1979–2015: Role of prediction model parsimony in integrated empirical geographic regression. PLoS One, 15(2), e0228535. 10.1371/journal.pone.0228535 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kind, A. J. H. , & Buckingham, W. R. (2018). Making neighborhood‐disadvantage metrics accessible—The neighborhood Atlas. New England Journal of Medicine, 378(26), 2456–2458. 10.1056/NEJMp1802313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kroepsch, A. C. , Maniloff, P. T. , Adgate, J. L. , McKenzie, L. M. , & Dickinson, K. L. (2019). Environmental justice in unconventional oil and natural gas drilling and production: A critical review and research agenda. Environmental Science & Technology, 53(12), 6601–6615. 10.1021/acs.est.9b00209 [DOI] [PubMed] [Google Scholar]
- Lee, A. H. , Wang, K. , Scott, J. A. , Yau, K. K. W. , & McLachlan, G. J. (2006). Multi‐level zero‐inflated Poisson regression modelling of correlated count data with excess zeros. Statistical Methods in Medical Research, 15(1), 47–61. 10.1191/0962280206sm429oa [DOI] [PubMed] [Google Scholar]
- Lipsitt, J. , Chan‐Golston, A. M. , Liu, J. , Su, J. , Zhu, Y. , & Jerrett, M. (2021). Spatial analysis of COVID‐19 and traffic‐related air pollution in Los Angeles. Environment International, 153, 106531. 10.1016/j.envint.2021.106531 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luna, T. (2020). California sets new priorities for who is tested for coronavirus as demand surges. Los Angeles Times. Retrieved from https://www.latimes.com/california/story/2020‐07‐14/california‐testing‐priorities‐covid‐19 [Google Scholar]
- Meo, S. A. , Abukhalaf, A. A. , Alomar, A. A. , Alessa, O. M. , Sami, W. , & Klonoff, D. C. (2021). Effect of environmental pollutants PM‐2.5, carbon monoxide, and ozone on the incidence and mortality of SARS‐COV‐2 infection in ten wildfire affected counties in California. The Science of the Total Environment, 757, 143948. 10.1016/j.scitotenv.2020.143948 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morello‐Frosch, R. , Zuk, M. , Jerrett, M. , Shamasunder, B. , & Kyle, A. D. (2011). Understanding the cumulative impacts of inequalities in environmental health: Implications for policy. Health Affairs, 30(5), 879–887. 10.1377/hlthaff.2011.0153 [DOI] [PubMed] [Google Scholar]
- Nationwide Parcel Data & Property Level Geocodes|SmartParcels . (2018). [Computer software]. DMP LightBox. Retrieved from https://www.digmap.com/platform/smartparcels/
- Paciorek, C. J. (2010). The importance of scale for spatial‐confounding bias and precision of spatial regression estimators. Statistical Science: A Review Journal of the Institute of Mathematical Statistics, 25(1), 107–125. 10.1214/10-STS326 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park, Y. M. , Kearney, G. D. , Wall, B. , Jones, K. , Howard, R. J. , & Hylock, R. H. (2021). COVID‐19 Deaths in the United States: Shifts in hot spots over the three phases of the pandemic and the spatiotemporally varying impact of pandemic vulnerability. International Journal of Environmental Research and Public Health, 18(17), 8987. 10.3390/ijerph18178987 [DOI] [PMC free article] [PubMed] [Google Scholar]
- QGIS.org . (2024). QGIS geographic information system [Computer software]. Open Source Geospatial Foundation Project. Retrieved from http://qgis.org [Google Scholar]
- RStudio Team . (2020). RStudio: Integrated development for R (version 1.1.463) [R; R]. RStudio, PBC. Retrieved from http://www.rstudio.com/ [Google Scholar]
- Tanne, J. H. (2022). COVID‐19: US passes one million deaths as mask mandates return. BMJ, 377, o1147. 10.1136/bmj.o1147 [DOI] [PubMed] [Google Scholar]
- Tran, K. V. , Casey, J. A. , Cushing, L. J. , & Morello‐Frosch, R. (2020). Residential proximity to oil and gas development and birth outcomes in California: A retrospective cohort study of 2006–2015 births. Environmental Health Perspectives, 128(6), 067001. 10.1289/EHP5842 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tran, K. V. , Casey, J. A. , Cushing, L. J. , & Morello‐Frosch, R. (2021). Residential proximity to hydraulically fractured oil and gas wells and adverse birth outcomes in urban and rural communities in California (2006‐2015). Environmental Epidemiology, 5(6), e172. 10.1097/EE9.0000000000000172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- University of Wisconsin, C. for H. D. R . (2020). Neghborhood Atlas (Area Deprivation index) (version 2020) [Dataset]. Retrieved from https://www.neighborhoodatlas.medicine.wisc.edu/
- US Building Footprints . (2019). US Building Footprints [Computer software]. Microsoft. Retrieved from https://planetarycomputer.microsoft.com/dataset/ms‐buildings
- U.S. Census Bureau . (2021). Geographic unit (GU) block maps [Dataset]. U.S. Census Bureau. Retrieved from https://data.census.gov/
- U.S. Energy Information Administration . (2022). The distribution of U.S. oil and natural gas wells by production rate. U.S. Energy Information Administration. Retrieved from https://www.eia.gov/petroleum/wells/pdf/full_report.pdf [Google Scholar]
- Weaver, A. K. , Head, J. R. , Gould, C. F. , Carlton, E. J. , & Remais, J. V. (2022). Environmental factors Influencing COVID‐19 incidence and severity. Annual Review of Public Health, 43(1), 271–291. 10.1146/annurev-publhealth-052120-101420 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, J. , Dong, X. , Liu, G. , & Gao, Y. (2023). Risk and protective factors for COVID‐19 morbidity, severity, and mortality. Clinical Reviews in Allergy and Immunology, 64(1), 90–107. 10.1007/s12016-022-08921-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Citations
- American Community Survey . (2019). 2019: ACS 5‐year estimate detailed tables [Table B01001] [Dataset]. US Census Bureaus. Retrieved from https://data.census.gov/table/ACSDT5Y2019.B01001?g=0400000US06$150000&y=2019&d=ACS%205‐Year%20Estimates%20Detailed%20Tables
- CalGEM . (2024). California geologic energy management division (CalGEM) [Dataset]. WellSTAR. Retrieved from https://wellstar‐public.conservation.ca.gov/General/Home/PublicLanding
- Nationwide Parcel Data & Property Level Geocodes|SmartParcels . (2018). [Computer software]. DMP LightBox. Retrieved from https://www.digmap.com/platform/smartparcels/
- University of Wisconsin, C. for H. D. R . (2020). Neghborhood Atlas (Area Deprivation index) (version 2020) [Dataset]. Retrieved from https://www.neighborhoodatlas.medicine.wisc.edu/
- US Building Footprints . (2019). US Building Footprints [Computer software]. Microsoft. Retrieved from https://planetarycomputer.microsoft.com/dataset/ms‐buildings
- U.S. Census Bureau . (2021). Geographic unit (GU) block maps [Dataset]. U.S. Census Bureau. Retrieved from https://data.census.gov/
Supplementary Materials
Supporting Information S1
Data Availability Statement
Data from the US Census, the American Community Survey, and the University of Wisconsin are publicly available and accessible through their respective websites (American Community Survey, 2019; University of Wisconsin, 2020; U.S. Census Bureau, 2021). Gridded population sociodemographic estimates from California from Depsky et al. (2022), may be accessed through Github as described in their published article (https://pubmed.ncbi.nlm.nih.gov/35834564/). Oil and gas data are available from CalGEM through the WellSTAR portal (CalGEM, 2024). Data supporting this research on health outcomes are available from the California Department of Public Health and are not accessible to the public or research community due to restrictions around human subjects approval (IRB) and data use agreements. Researchers may gain access by reaching out to the department directly to propose research topic and negotiate data use agreements. Software used in this study includes R Studio (RStudio Team, 2020) and QGIS (QGIS.org, 2024) for data management and data visualizations.