

Abstract
Several studies reported the roles of short-term exposure to fine particulate matter (PM2.5) on violent behaviors; however, existing findings had a limitation in assessing the population-representative association between violence and PM2.5 due to the limited data availability: most studies have been based on homicides in monitored urban areas. This study collected violence data from the National Hospital Discharge In-depth Injury Survey in South Korea (2015–2019), based on population-representative samples. To cover unmonitored areas, we used the daily modeled PM2.5, the predicted result driven by a machine-learning ensemble model covering all inland districts in South Korea (R2>0.94). We evaluated the national association between short-term exposure to PM2.5 and violence cases with a time-stratified case-crossover design. A total of 2,867 violence cases were included. We found an approximately linear association between short-term exposure to PM2.5 (lag 0–2 days) and an increased risk of violence, with an estimated odd ratio (OR) per 10 μg/m3 of PM2.5 of 1.07 with 95% CI: 1.02–1.12. This relationship was more prominent in males and individuals aged 64 years or less than in females and individuals aged 65 years or older for the most part. The estimated excess fraction of violence cases attributable to PM2.5 was 14.53% (95% CI: 4.54%–22.92%), and 6.42% (95% CI: 1.97%–10.26%) of the excess violence was attributable to non-compliance with the WHO guidelines (daily PM2.5 > 15 μg/m3). Our findings might be evidence of the need to establish elaborate action plans and stricter air quality guidelines to reduce the hazardous impacts of PM2.5 on violence in South Korea.
Introduction
Mental disorders have long been recognized as one of the major social and public health problems, especially related to the COVID-19 pandemic [1]. In particular, among mental disorders, violence–which is one of the major intentional injuries–is a crucial public health concern. According to the WHO fact sheet regarding injuries and violence (as of 19 June 2024) [2], injuries and violence are responsible for an estimated 10% of all years of lives with disabilities, and violence-related injuries kill 1.25 million people every year in 2019 with 6.2 deaths per 100,000 persons died due to homicide globally. In South Korea, the homicide-related mortality rate was 0.8 per 100,000 in 2019 [3], and it was higher than in neighboring East Asian countries (0.2 and 0.3 per 100,000 in Japan and Singapore) [3]. Moreover, severe violence cases have been seriously and widely addressed in mass and social media because it is a critical risk factor that destroys human well-being and quality of life [4]. Therefore studies on violence are timely and important.
Numerous studies have examined the risk factors for violence including socioeconomic and individual factors, and even genetics [5, 6]. Concurrently, rich studies have consistently reported that particulate matter (PM) is one of the important environmental risk factors for unintentional injuries including violence [7]. Historically, the hypothesis that exposure to PM might increase neurological disorders associated with cognitive responses, impulsiveness, and depression has been addressed in epidemiological studies [8, 9] as well as in laboratory studies [10, 11].
Nonetheless, previous studies on PM and violence have several limitations. First, most of the previous studies investigating this topic used homicide data [12, 13], thus there could be knowledge gaps regarding the impacts of PM on mild or moderate violence cases. Second, due to the limited exposure or violence data, many studies have included selected areas with air pollution monitoring stations with a sufficient sample size for statistical analyses [13, 14]–mostly metropolitan or urban areas could satisfy these conditions–therefore, there could be selection biases regarding the limited areas, especially if the nationwide association should be assessed for the population-representative public health policy. Lastly, most studies on air pollution and violence or crime have been conducted in the United States [9, 15], and studies in Asian regions with different lifestyles, diets, genes, social disparities, and demographic characteristics are scarce. Especially, South Korea is one of the notable countries related to mental health, because they showed a suicide rate of 24.1 per 100,000 people in 2020, which is the highest rate in the OECD countries [16]. Thus, studies on air pollution and violence in South Korea could benefit their populations and other Asian countries with similar environments, cultures, and public health issues.
Therefore, to address these gaps in knowledge, this study aims to assess the nationwide risks of fine particulate matter (PM2.5) on all types of violence cases, which allows us to provide wider information on violence than that from the homicide data that could only cover severe cases. This study used the national population-representative survey data covering all districts in South Korea, provided by the Korea Disease Control and Prevention Agency (2015–2019). Further, we used a nationwide machine learning-based ensemble prediction model for daily PM2.5 with excellent spatial resolution (1 km2) and accuracy (R2>0.94) to evaluate the less-biased association between short-term exposure to particulate matter and violence.
Materials and methods
Ethical approval
Not requested. This study used secondary and publicly available data. This data did not include any information related to the personal identification.
Data on violence
We obtained national data on hospital visits due to violence from 2015 to 2019 across 247 districts in Korea. Specifically, we collected the Korea National Hospital Discharge In-depth Injury Survey, officially operated annually and provided by the Korea Disease Control and Prevention Agency to investigate the national status regarding all types of violence and generate relevant statistics.
This survey annually sampled 150,000 to 300,000 (it has increased over the years) people discharged from the general hospital, and the target population is all people discharged from the general hospital residing in South Korea from 2005. Also, to get population representativeness, the survey adopted the two-stage stratified-cluster systematic sampling method, based on regions, age-sex structures, and the number of hospital beds in the selected hospitals. Theoretically, the entire general hospital should be a target for the survey; however, due to practical reasons, the survey targeted general hospitals with 100 beds or more. Among the general hospitals with 100 beds or more, the survey sampled a total of 250 hospitals using the Neyman allocation method [17] based on the number of hospital beds in each hospital.
This survey investigated all types of injuries (both intentional and unintentional) using the related electronic medical records from the selected hospitals. The injury was defined as S00-T98 code (certain other consequences by injury, addiction, and externalities) in main diagnosis or sub-diagnosis by KCD-8th and ICD-9-CM Vol.Ⅲ. Each recorded case also includes information on the patient’s sex, age, residential address (district; “si/gun/gu” in Korean), date of hospitalization, mechanism, etc. From this nationwide survey, this study collected violent cases based on medical information on the intentionality of the injury (intentional/unintentional) and types of intentional injuries (violence/suicide/poisoning, etc.) which included KCD-8th X85-Y09 code patients. This survey clarifies violence as violence between people, such as being punched by a person, beaten with a blunt instrument, or raped, except for violence under legal adjustment.
Modeled PM2.5 and environmental data
To cover unmonitored districts, a nationwide daily modeled PM2.5 (the predicted value using a machine-learning ensemble prediction model with a 1 km2 spatial resolution) was used as an exposure for all districts. The modeled PM2.5 (24-hour average) was provided by the AiMS-CREATE team, and their prediction models were used in previous studies [18, 19]. The ensemble model incorporates three machine-learning algorithms (random forest, extreme gradient boosting, and deep neural network). Detailed information on the model is reported in the Supplementary Materials: “1. Air pollution prediction models” and S1 Table in S1 File. The prediction models for PM2.5 showed excellent performances: across districts, a cross-validated R2 of 0.944. Daily concentration predictions at 1 km2 were aggregated to each district by averaging the predictions at grid cells with centroid points inside the boundary of each district. S1-S3 Tables in S1 File displays the prediction performance of the PM2.5 ensemble prediction model used in this study.
We collected meteorological variables as time-varying confounders from the ERA-5 Land global reanalysis dataset [20], and these variables include 24-hour average 2-m air temperature (K), relative humidity (%), and precipitation (m). This ERA-5 dataset has a horizontal resolution of 0.1° x 0.1°, with a native spatial resolution of 9–11 km, and we aggregated it to district unit (“Si/Gun/Gu”) by averaging the values at grid cells with centroid points inside the boundary of that district.
Study design
This study adopted a time-stratified case-crossover design to estimate the association between short-term PM2.5 (lag 0–2) and violence. We defined a case day as the date of each outcome and matched control days as days with the day of the week within the same month in the same year. This time-stratified self-matching controlled for confounding variables that do not change substantially in a month, such as age, sex, weight, diet, and other individual-level time invariant health behavior characteristics, and also district-level regional variables like population density, gross regional domestic product, and other socio-environmental factors including park and medical accessibilities, population composition, and access to grocery shops [21]. Furthermore, the time-stratified matching controlled potential confounding that varies across weekdays and weekends, with bidirectional control day selection that can remove biases from seasonality and long-term trends of PM2.5 and outcomes [22]. Therefore, the time-stratified case-crossover design has been widely used in studies evaluating the risk of short-term environmental exposure on acute health outcomes [21, 23–26].
Statistical analysis
We estimated the risk of violence associated with short-term exposure to PM2.5 using a conditional logistic regression model. For the main model, we selected a mean value of lag 0 to lag 2 PM2.5 exposure to address the average health risks associated with the same and the previous days’ exposures based on existing relevant studies [21, 27, 28]. We adjusted indicator variables of holiday and daily temperatures. To control potentially nonlinear confounding, temperatures were controlled using a cross-basis function with a natural cubic spline with four degrees of freedom for an exposure-response relationship, and a natural cubic spline with intercepts and one internal knot (at lag 1) for a lag-response relationship over the lag of two days. The relationship between relatively short-term temperature (one or two lag days) and violence, suicide, or other acute mental disorders has been identified in many related epidemiological studies [13, 29]. We calculated the odds ratio (OR) for a 10 μg/m3 increase in PM2.5.
Subgroup analysis
Subgroup analyses (sex, age groups, Urban/Rural, GRDP (Gross Regional Domestic Product) High/Low, and seasons) were also conducted to identify the high-risk populations. Sex groups were divided into two categories: Male and Female. Age groups were also distinguished into two categories: people aged 65 years or older and those aged less than 64 years. The region was evaluated in largely two parts: 1) urban and rural and 2) high and low areas based on GRDP (Gross Regional Domestic Product) per 100,000 persons. First, we classified all study districts (si/gun/gu) into urban (si and gu) and rural (gun) districts, based on the Local Autonomy Act of Korea, which has been used in previous studies [30, 31]. We collected annual district-level GRDP per 100,000 people from 2015 to 2019 from Statistics Korea. Then, we calculated the district-specific average GRDP per 100,000 people during the study period. We divided study districts into two categories (high/low) based on the median value of average GRDP per 100,000 persons. Two seasons were also considered: the warm season (April–September) and the cold season (October–March). To evaluate the different associations between PM2.5 and violence for each subgroup, we additionally created a case-crossover dataset for each sex, age group, urban/rural, GRDP high/low group, and season and repeated the main analysis. Further, we conducted the Wald test based on the independent assumption to check whether OR estimates between subgroups are statistically different (H0: there is no difference).
Excess violence burden attributable to PM2.5
Odd ratio estimates for short-term exposure to PM2.5 were translated into excess violence cases attributable to PM2.5, to demonstrate the excess burden attributable to PM2.5 exposures during the study period. The estimates of the excess burden (either as an attributable burden or relative excess measures of outcomes) are widely used to assess the actual and quantitative public health impacts of extreme exposures (e.g., heatwaves or high-level air pollution).
To calculate it, we created district-specific time-series datasets including daily mean PM2.5 and daily counts of violence. For each time-series data, we calculated the daily excess violence cases attributable to PM2.5 using the corresponding estimated ORs for the PM2.5 concentrations of each day (daily excess violence cases attributable to daily PM2.5: ; where t indicates the day, and ORt presents the daily OR for the PM2.5 concentrations of day t). Here in, the OR estimates were used as the approximated values of relative risk (RR) that were originally used to calculate the attributable risk estimates. When the proportion of the outcome onset is substantially small (in general, 20% or less), the OR estimates can be regarded as an approximated estimate of the RR estimates [32]. In this study, the total number of outcomes (violence cases) was 2,867 cases during the find years (2015 to 2019), and when the total number of investigation cases of the Korea National Hospital Discharge In-depth Injury Survey (sampled 150,000 to 300,000 per year). Therefore, the probability of our outcome was substantially small. Thus, we used OR estimates as the approximated values of RR estimates in this study.
The sum of daily excess violence cases indicates the total excess violence cases attributable to PM2.5 during the study period, and its ratio with the total number of violence provides the total excess fraction (%) of violence cases attributable to short-term PM2.5 exposures. Since a lot of previous studies reported that the air pollution impacts on health persist at low levels [28], we set a minimum PM2.5 concentration during the study period as the reference to calculate excess violence cases attributable to PM2.5 (i.e., the whole range of PM2.5), although we recognize that this includes natural background concentrations.
Further, we assessed the excess violence burden attributable to non-compliance with the current guidelines regarding PM2.5: the WHO guideline, the National Ambient Air Quality Standards (NAAQS) in the United States, and the Korean Air Quality Standards (KAS) in South Korea. These guidelines have been established to provide quantitative recommendations for air quality management, and exceeding these levels is associated with important risks to public health. Therefore, we calculated excess violence cases only for the subset of days with PM2.5 levels above (i.e. non-compliance) the WHO air quality guidelines (daily average PM2.5 ≤ 15 μg/m3), and the NAAQS and KAS (daily average PM2.5 ≤ 35 μg/m3), respectively, to illustrate the burden that could be prevented or reduced through compliance with the guidelines. The Monte Carlo simulations were used to compute the confidence intervals of each estimate, with 1,000 replicates [26, 33].
Sensitivity analysis
We performed a series of sensitivity analyses to examine whether our results were consistent with additional different modeling specifications in the total population. Sensitivity analyses were carried out about two aspects. First, we tried to show the robustness of PM2.5’s lag period. Single lag from 0 to 3 was executed and the moving average from lag 0–1 to 0–3 was tested. Second, for daily temperature, which was used as a covariate, we applied 3 and 7 days of lag period, and 3 and 5 degrees of freedom for an exposure-response relationship.
Results
Table 1 presents the descriptive statistics on violence outcomes during the study period (2015–2019). Total counts of violence were 2,867, of which 67.6% were males and 92.8% occurred in individuals aged less than 65 years. Annually, approximately 544 to 612 cases of violence were reported in South Korea (S4 Table in S1 File). Collisions accounted for the highest % of injury mechanisms at 88.7% (S5 Table in S1 File). Complete and partial recovery was the most common treatment outcome in 96.16% of cases (S6 Table in S1 File). Fig 1 shows geographical distributions of average PM2.5 during the study period. The national annual average concentration of PM2.5 was 23.71 μg/m3, with the lowest level recorded in 2018 at 21.71 μg/m3 and the highest in 2015 at 25.74 μg/m3 (S1 Table in S1 File).
Table 1. Descriptive information on violence cases among Korea National Hospital Discharge In-depth Injury Survey data during the study period (2015–2019) in South Korea.
Holidays include Official public holidays in Korea. We classified the study districts (si/gun/gu) into urban (si and gu) and rural (gun) districts. GRDP High and Low areas are separated by a median value.
| N | % | ||
|---|---|---|---|
| Total | 2867 | 100 | |
| Sex | Males | 1937 | 67.6 |
| Females | 930 | 32.4 | |
| Age | 0–64 years | 2660 | 92.8 |
| 0–19 years | 442 | 15.4 | |
| 20–39 years | 1023 | 35.7 | |
| 40–64 years | 1195 | 41.7 | |
| 65+ years | 207 | 7.2 | |
| 65–79 years | 174 | 6.1 | |
| 80+ years | 33 | 1.2 | |
| Holiday | Yes | 106 | 3.7 |
| No | 2761 | 96.3 | |
| Urban/Rural | Urban | 2568 | 89.6 |
| Rural | 299 | 10.4 | |
| GRDP per person | High | 1311 | 45.7 |
| Low | 1556 | 54.3 |
Fig 1. Geographical distributions of the annual averages of daily average PM2.5 (fine particulate matter; μg/m3) in South Korea from 2015 through 2019 using a machine-learning ensemble prediction model with a 1 km2 spatial resolution.
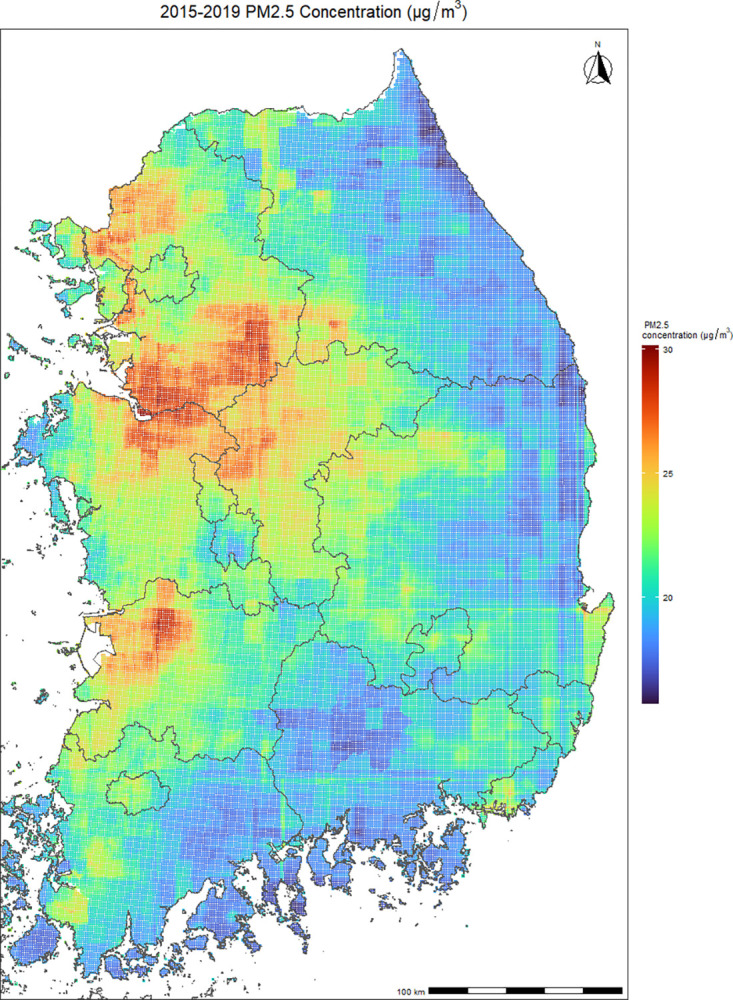
The prediction models got a 0.944 R2 score across districts. Daily concentration predictions at 1 km2 were aggregated in each district.
Fig 2 presents the nonlinear exposure-response curve between PM2.5 and violence. We found the association between PM2.5 and violence cases was approximately linearly positive; thus, we presented risk estimates based on a linear association after Fig 2.
Fig 2. Flexible association between short-term exposure to PM2.5 and violence cases.

Each Blue and Green dashed lines indicate WHO: World Health Organization air quality guidelines (daily average PM2.5: 15 μg/m3), NAAQS: National Ambient Air Quality Standards (daily average PM2.5: 35 μg/m3) in the United States, and KAS: Korean Air Quality Standards (daily average PM2.5: 35 μg/m3), respectively. A conditional logistic regression model, adjusted for holiday and daily mean temperatures, within a time-stratified case-crossover design, was used to estimate odds ratios and 95% confidence intervals.
Fig 3 shows the association between PM2.5 and violence in the total population and by sub-group. In the total population, the association between PM2.5 and violence was evident with an OR of 1.07 with 95% CI: 1.02–1.12. The association was weakly higher in rural areas (OR: 1.23, 95% CI: 1.02–1.48) than in urban areas (OR: 1.06, 95% CI: 1.01–1.12) (Wald test p-value: 0.096). Further, the association between PM2.5 and violence was statistically pronounced in cold seasons (OR: 1.08, 95% CI: 1.02–1.14) compared to warm seasons (1.05, 0.96–1.15), and the association was more pronounced in people aged 65 or older (OR: 1.33, 95% CI: 1.04–1.71) than those aged 64 or less (OR: 1.07, 95% CI: 1.00–1.13) in cold seasons (Wald test p-value: 0.042). This pattern remained consistent even when age groups were further subdivided (S7 Table in S1 File).
Fig 3. Associations between short-term exposure to PM2.5 (lag 0–2) and violence cases by season and subgroup.

OR: Odds ratio per 10 μg/m3 of PM2.5. A conditional logistic regression model, adjusted for holiday and daily mean temperatures, within a time-stratified case-crossover design, was used to estimate odds ratios and 95% confidence intervals. Wald type test was used to test the effect modification. We classified the study districts (si/gun/gu) into urban (si and gu) and rural (gun) districts. GRDP High and Low areas are separated by a median value.
Table 2 reports the excess fractions of violence attributable to PM2.5. For the total population, about 14.53% (4.54–22.92) of violence cases could be attributable to PM2.5 exposures. Approximately 6.42% (1.97–10.26) and 1.11% (0.34–1.77) of excess violence cases were attributable to non-compliance with the WHO air quality guidelines (15 μg/m3) and NAAQS and KAS (35 μg/m3), respectively. The excess burden was also higher in males and individuals aged 64 years or less than in females and those aged 65 years or older. The burden of violence related to PM2.5 was more pronounced during the cold season compared to the warm season in the total population and all subgroups.
Table 2. Excess numbers and fractions of violence cases attributable to PM2.5 and non-compliance with the current WHO air quality guidelines, NAAQS in the United States, and KAS in South Korea.
WHO: World Health Organization, NAAQS: National Ambient Air Quality Standards. KAS: Korean Air Quality Standards. We classified the study districts (si/gun/gu) into urban (si and gu) and rural (gun) districts. GRDP High and Low areas are separated by a median value.
| Excess numbers (%) | Excess fractions (%) | |||||
|---|---|---|---|---|---|---|
| Total season | Total population | Whole PM 2.5 | 416.58 | (130.21, 657.14) | 14.53 | (4.54, 22.92) |
| WHO guidelines (>15 μg/m 3 ) | 184.08 | (56.38, 294.19) | 6.42 | (1.97, 10.26) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 31.77 | (9.79, 50.62) | 1.11 | (0.34, 1.77) | ||
| Males | Whole PM 2.5 | 299.36 | (47.45, 508.15) | 15.45 | (2.45, 26.23) | |
| WHO guidelines (>15 μg/m 3 ) | 133.77 | (20.66, 230.69) | 6.91 | (1.07, 11.91) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 24.78 | (3.86, 42.61) | 1.28 | (0.2, 2.2) | ||
| Females | Whole PM 2.5 | 109.89 | (-73.94, 263.35) | 11.82 | (-7.95, 28.32) | |
| WHO guidelines (>15 μg/m 3 ) | 48.00 | (-30.78, 117.54) | 5.16 | (-3.31, 12.64) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 6.95 | (-4.54, 16.94) | 0.75 | (-0.49, 1.82) | ||
| 0–64 years | Whole PM 2.5 | 372.77 | (96.33, 601.02) | 14.01 | (3.62, 22.59) | |
| WHO guidelines (>15 μg/m 3 ) | 164.74 | (41.68, 269.15) | 6.19 | (1.57, 10.12) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 28.39 | (7.23, 46.24) | 1.07 | (0.27, 1.74) | ||
| 65 years or older | Whole PM 2.5 | 47.34 | (-49.18, 101.25) | 22.87 | (-23.76, 48.91) | |
| WHO guidelines (>15 μg/m 3 ) | 21.53 | (-20.27, 47.8) | 10.4 | (-9.79, 23.09) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 3.79 | (-3.75, 8.5) | 1.83 | (-1.81, 4.1) | ||
| Urban | Whole PM 2.5 | 320.17 | (62.91, 581.01) | 12.47 | (2.45, 22.63) | |
| WHO guidelines (>15 μg/m 3 ) | 142.23 | (27.37, 261.99) | 5.54 | (1.07, 10.2) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 25.26 | (4.9, 46.33) | 0.98 | (0.19, 1.8) | ||
| Rural | Whole PM 2.5 | 103.97 | (10.83, 166.89) | 34.77 | (3.62, 55.82) | |
| WHO guidelines (>15 μg/m 3 ) | 45.48 | (4.35, 76.58) | 15.21 | (1.45, 25.61) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 5.89 | (0.55, 10.04) | 1.97 | (0.18, 3.36) | ||
| GRDP High | Whole PM 2.5 | 173.77 | (-13.89, 337.93) | 13.25 | (-2.37, 25.78) | |
| WHO guidelines (>15 μg/m 3 ) | 80.07 | (-13.89, 158.09) | 6.11 | (-1.06, 12.06) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 15.91 | (-2.79, 31.3) | 1.21 | (-0.21, 2.39) | ||
| GRDP Low | Whole PM 2.5 | 237.09 | (19.08, 419.70) | 15.24 | (1.23, 26.97) | |
| WHO guidelines (>15 μg/m 3 ) | 101.05 | (7.86, 182.56) | 6.49 | (0.51, 11.73) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 14.67 | (1.15, 26.44) | 0.94 | (0.07, 1.70) | ||
| Warm seasons | Total population | Whole PM 2.5 | 139.75 | (-147.1, 368.71) | 9.02 | (-9.50, 23.8) |
| WHO guidelines (>15 μg/m 3 ) | 51.49 | (-50.94, 138.47) | 3.32 | (-3.29, 8.94) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 3.63 | (-3.48, 9.84) | 0.23 | (-0.22, 0.64) | ||
| Males | Whole PM 2.5 | 123.20 | (-92.84, 297.97) | 11.73 | (-8.84, 28.38) | |
| WHO guidelines (>15 μg/m 3 ) | 45.12 | (-31.82, 111.92) | 4.3 | (-3.03, 10.66) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 3.32 | (-2.29, 8.32) | 0.32 | (-0.22, 0.79) | ||
| Females | Whole PM 2.5 | 25.46 | (-146.19, 160.04) | 5.10 | (-29.3, 32.07) | |
| WHO guidelines (>15 μg/m 3 ) | 10.55 | (-49.79, 63.25) | 2.11 | (-9.98, 12.67) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 0.72 | (-2.99, 4.22) | 0.14 | (-0.6, 0.85) | ||
| 0–64 years | Whole PM 2.5 | 176.21 | (-72.62, 398.96) | 12.28 | (-5.06, 27.8) | |
| WHO guidelines (>15 μg/m 3 ) | 64.94 | (-25.31, 151.04) | 4.53 | (-1.76, 10.53) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 4.60 | (-1.75, 10.82) | 0.32 | (-0.12, 0.75) | ||
| 65 years or older | Whole PM 2.5 | -57.79 | (-249.01, 35.07) | -50.7 | (-218.43, 30.76) | |
| WHO guidelines (>15 μg/m 3 ) | -17.19 | (-67.45, 14.07) | -15.08 | (-59.16, 12.35) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | -0.95 | (-3.47, 0.99) | -0.84 | (-3.04, 0.87) | ||
| Urban | Whole PM 2.5 | 86.13 | (-186.27, 305.19) | 6.22 | (-13.45, 22.04) | |
| WHO guidelines (>15 μg/m 3 ) | 32.21 | (-64.47, 114.98) | 2.33 | (-4.65, 8.3) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 2.26 | (-4.34, 8.09) | 0.16 | (-0.31, 0.58) | ||
| Rural | Whole PM 2.5 | 51.30 | (-28.18, 103.46) | 31.28 | (-17.18, 63.08) | |
| WHO guidelines (>15 μg/m 3 ) | 19.27 | (-9.00, 41.67) | 11.75 | (-5.49, 25.41) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 1.47 | (-0.68, 3.19) | 0.89 | (-0.42, 1.95) | ||
| GRDP High | Whole PM 2.5 | 68.28 | (-114.45, 212.04) | 9.84 | (-16.49, 30.55) | |
| WHO guidelines (>15 μg/m 3 ) | 26.34 | (-40.42, 83.08) | 3.79 | (-5.82, 11.97) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 2.34 | (-3.46, 7.42) | 0.34 | (-0.50, 1.07) | ||
| GRDP Low | Whole PM 2.5 | 75.04 | (-128.23, 241.67) | 8.78 | (-15.00, 28.27) | |
| WHO guidelines (>15 μg/m 3 ) | 27.50 | (-43.54, 90.04) | 3.22 | (-4.98, 10.53) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 1.49 | (-2.16, 4.94) | 0.17 | (-0.25, 0.58) | ||
| Cold seasons | Total population | Whole PM 2.5 | 233.62 | (60.63, 380.68) | 17.73 | (4.6, 28.88) |
| WHO guidelines (>15 μg/m 3 ) | 119.33 | (30.22, 197.62) | 9.05 | (2.29, 14.99) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 28.41 | (7.2, 47.07) | 2.16 | (0.55, 3.57) | ||
| Males | Whole PM 2.5 | 164.11 | (19.9, 292.52) | 18.50 | (2.24, 32.98) | |
| WHO guidelines (>15 μg/m 3 ) | 85.55 | (10.06, 155.59) | 9.64 | (1.13, 17.54) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 21.66 | (2.54, 39.5) | 2.44 | (0.29, 4.45) | ||
| Females | Whole PM 2.5 | 62.69 | (-46.26, 146.17) | 14.55 | (-10.73, 33.91) | |
| WHO guidelines (>15 μg/m 3 ) | 31.05 | (-21.69, 73.97) | 7.2 | (-5.03, 17.16) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 6.30 | (-4.47, 14.96) | 1.46 | (-1.04, 3.47) | ||
| 0–64 years | Whole PM 2.5 | 186.68 | (2.61, 342.28) | 15.24 | (0.21, 27.94) | |
| WHO guidelines (>15 μg/m 3 ) | 95.4 | (1.3, 177.88) | 7.79 | (0.11, 14.52) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 22.57 | (0.31, 42.09) | 1.84 | (0.03, 3.44) | ||
| 65 years or older | Whole PM 2.5 | 41.16 | (5.73, 60.99) | 44.25 | (6.16, 65.58) | |
| WHO guidelines (>15 μg/m 3 ) | 21.41 | (2.76, 33.2) | 23.03 | (2.96, 35.70) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 5.72 | (0.72, 9.13) | 6.15 | (0.77, 9.81) | ||
| Urban | Whole PM 2.5 | 187.08 | (27.78, 331.17) | 15.81 | (2.35, 27.99) | |
| WHO guidelines (>15 μg/m 3 ) | 96.05 | (13.91, 172.8) | 8.12 | (1.18, 14.61) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 23.63 | (3.43, 42.52) | 2.00 | (0.29, 3.59) | ||
| Rural | Whole PM 2.5 | 56.31 | (-1.59, 92.44) | 41.71 | (-1.18, 68.47) | |
| WHO guidelines (>15 μg/m 3 ) | 29.11 | (-0.73, 51.03) | 21.56 | (-0.54, 37.8) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 4.89 | (-0.12, 8.84) | 3.62 | (-0.09, 6.55) | ||
| GRDP High | Whole PM 2.5 | 96.11 | (-36.64, 204.64) | 15.58 | (-6.26, 33.17) | |
| WHO guidelines (>15 μg/m 3 ) | 51.23 | (-19.81, 111.20) | 8.30 | (-3.21, 18.02) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 13.54 | (-5.25, 29.41) | 2.19 | (-0.85, 4.77) | ||
| GRDP Low | Whole PM 2.5 | 137.2 | (13.83, 237.86) | 19.57 | (1.97, 33.93) | |
| WHO guidelines (>15 μg/m 3 ) | 67.64 | (6.56, 120.01) | 9.65 | (0.94, 17.12) | ||
| NAAQS & KAS (> 35 μg/m 3 ) | 14.15 | (1.37, 25.17) | 2.02 | (0.20, 3.59) | ||
Lastly, the results of sensitivity analyses showed that our main results were consistent with different modeling selections (S8 Table in S1 File).
Discussion
To our knowledge, this is the first and largest epidemiological study investigating the national association between short-term PM2.5 exposure and violence with a population-representative survey dataset in South Korea. The association between short-term PM2.5 and violence was statistically evident in the total population, and the association was more pronounced in males and individuals aged 64 years or less, compared to females and individuals aged 65 years or older. We also found that the excess fractions of violence attributable to non-compliance with WHO guidelines and NAAQS and KAS were 6.42% and 1.11%, respectively.
It is not long since violence was addressed from a public health perspective [34]. Throughout the 1970s and 1980s, the risk of suicide and homicide steadily increased in vulnerable populations, and this trend prompted responses from governments. In particular, intentional injuries such as violence are viewed as preventable [35], highlighting the importance of identifying modifiable risk factors. These include demographic factors (i.e., age, sex, and ethnicity), socioeconomic factors (i.e., education and employment status), and environmental factors (i.e., neighborhood safety and exposure to pollution). Furthermore, recent studies have reported consistent evidence that environmental factors might be associated with violence. Previous studies suggested that sudden weather changes (rising temperature, rain, an increase in humidity) can increase violent crimes, such as homicides, assaults, and sex offenses [36], and some theories (thermal or climatic discomfort can increase impulsivity and aggression, and changes in routine activities due to changing weather, such as outdoor events and social engagements) supports these results on weather and violence [36, 37]. In this context, the findings of this study are also anticipated to contribute valuable evidence for developing environmental epidemiological strategies aimed at violence prevention.
There has been a growing literature that has examined the association between air pollution and assault or homicides [9, 13, 38]. One study in the US found that each 10 μg/m3 change in daily PM2.5 was associated with a 1.17% increase in violent crime rates, with a particularly strong association observed in assault [9]. Similarly, a study in Seoul, South Korea, found that exposure to air pollutants is related to a risk of injuries, with a 1.08% increase in assault injuries for each interquartile range increase of PM2.5 [38]. On the other hand, one study in California, US, on suicides and homicides found a significant association with ambient temperatures, but not with air pollutants [13]. Likewise, there have been no consistent findings on the association between air pollution and violence, and considering that most of the previous studies have been conducted in specific cities or regions, this nationwide study is expected to contribute to the limited literature.
Some plausible hypotheses have been suggested to explain the link between increased PM2.5 and the risk of violence. Repeated exposure to PM2.5 can cause immune dysregulation and trigger inflammatory processes, increasing the possibility of negative responses to various stressors [39]. The entry of PM2.5 into the brain can diminish cognitive resources needed to guide choices and behaviors, potentially leading to cognitive decline [40]. These damages to the neurologic system have been shown to affect judgment and emotional processing, which can cause mental disorders such as depression and aggressive behavior [8, 41]. Although we could not clearly distinguish between victims or perpetrators of violence due to data limitations, it can be inferred that exposure to PM2.5 may affect violence and related mental health problems, increasing the risk of being involved in violent incidents.
We found a greater association between short-term increases in PM2.5 and violence in males than in females. Globally, males are overwhelmingly more likely to be involved in violent crimes, both as perpetrators and victims [42], as shown in the dataset of this study. Some researchers have hypothesized that masculine norms, which emphasize that men should be strong and willing to take risks, are strongly linked to interpersonal violence [43], and that gender can shape individuals’ activity patterns, such as labor proclivities, which may affect the magnitude of exposure to air pollution [44]. We also found a more evident association between PM2.5 and violence among individuals aged 64 years or less, which is inconsistent with previous findings that air pollution has a greater impact on mortality and morbidity in the elderly [45]. However, this inconsistency may be due to different lifestyles and behaviors. In the case of air pollution and violence, younger people, who tend to be more socially active and spend more time outdoors, may be more likely to be affected by PM2.5 and involved in violent situations. More research is needed to understand these possible sex and age differences in the effects of air pollution on violence.
Our finding of stronger effects of PM2.5 in the cold season is consistent with several previous studies [14, 45]. One study in Shanghai, China, found that the impacts of air pollutants on mortality from all causes and cardiorespiratory diseases were more evident in the cold season than in warm seasons [45]. Another study in California, US, also found a stronger association between PM2.5 and homicide during cold seasons [14]. In this study, cold seasons have been found to have higher concentrations of PM2.5 compared to warm seasons in South Korea, but more research is needed to understand the seasonal variations in the chemical composition and toxicity of PM2.5. Additionally, it is worth noting that in this study only those aged 65 years or older had a significantly higher risk during the cold season compared to all seasons, while the risk estimates for those aged 64 years or less did not change by season. Older adults, who may experience weakened immune systems, worsening of underlying conditions, and decline in physical function during the cold season, can be more vulnerable to exposure to air pollution and risk of injury during this season. Further, alcohol consumption, which is closely linked to violent behavior [46], tends to increase during the cold months; cold weather and reduced sunlight, as well as holidays such as New Year’s and Christmas, are associated with higher alcohol intake [47–49]. This is especially concerning for older adults (65+ years), as increased alcohol consumption can worsen pre-existing vulnerabilities to physical and mental health problems [50]. Moreover, in South Korea, rural areas generally have a higher drinking rate with higher average ages [51], thus the alcohol consumption hypothesis could be associated with a higher association between PM2.5 and violence in rural areas than in urban areas. However, further studies are required to examine the hypotheses.
This study has several strengths. First, we focused on understudied health outcomes: injuries from violence, which also include nonfatal cases that have been less examined in comparison to homicide. In addition, we used a nationwide dataset of daily modeled PM2.5 concentrations and injuries from violence in South Korea to gain a more comprehensive understanding of the associations between PM2.5 and violence across the country. The nationwide study could improve the generalizability and robustness of risk estimates compared to previous studies.
Nevertheless, this study has some limitations. First, this study used district-level residential addresses to assign exposures to air pollution, which may lead to measurement errors in exposure. However, these errors are likely to be random and the estimates of the effect can go towards the null [52]. Second, there could be some unmeasured time-varying confounders (i.e., high-risk drinking and daily mood) that might affect our estimates. Third, due to the limited data availability, we were unable to explore the associations between PM2.5 and violence by individual socioeconomic factors, such as occupation or income levels, although these socioeconomic factors could be substantially associated with violence. Fourth, because our dataset only covered patients who were diagnosed admitted to, and discharged from the hospital, there was a limitation in capturing information on patients who were not admitted or who died before reaching the hospital. Also, the outcome definition relies on diagnosis codes, which may lead to an underestimation of the actual cases of violence. In addition, although we reported the descriptive statistics on subtypes of violence based on diagnostic code, we could not present the stratified association between PM2.5 and violence by subtype because of the insufficient sample size of each subtype: the majority of violence cases were due to collisions (around 90%). It would be helpful to improve the understanding of the underlying mechanisms between air pollution and violence if future studies could examine the types of violence with larger prospective cohort data. Fifth, although the survey dataset aimed to get population representativeness through specific sampling methods, we acknowledge that there may still be potential bias, and caution is needed when interpreting the findings. Sixth, we could not perform two-pollutant models because of the data limitation regarding different modeled pollutants (e.g., ozone and nitrogen dioxide). Lastly, our findings need to be further validated not only in South Korea but also in other regions and countries, especially those with different climate zones.
Conclusions
Our study evaluated that short-term PM2.5 exposures are associated with violence incidence in South Korea and found that the association was more prominent in males and younger populations than in females and older populations. Our study provides evidence for establishing more targeted action plans against PM2.5 and violence at the national scale. In addition, our estimated excess violence burden attributable to non-compliance with WHO air quality guidelines and the NAAQS and KAS suggests the potential benefits of more stringent air quality standards aligned with global-standard air quality guidelines or standards.
Supporting information
(DOCX)
Data Availability
All files related to the Korea National Hospital Discharge In-depth Injury Survey are publicly available from the Korea National Hospital Discharge In-depth Injury Survey database (https://www.kdca.go.kr/injury/biz/injury/recsroom/rawDta/rawDtaDwldMain.do#) for research purpose. People who want to download this data should submit the application form with their research objects and receive approval from the Korea Disease Control and Prevention Agency to use it.
Funding Statement
WL was supported by the National Institute of Environmental Research (NIER) funded by the Ministry of Environment (MOE) of the Republic of Korea (NIER-2021-03-03-007). JP was supported by Institute of Information & communications Technology Planning & Evaluation (IITP) under the Artificial Intelligence Convergence Innovation Human Resources Development (IITP-2024-RS-2023-00254177) grant funded by the Korea government (MSIT). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Min J, Oh J, Kim SI, Kang C, Ha E, Kim H, et al. Excess suicide attributable to the COVID-19 pandemic and social disparities in South Korea. Scientific Reports. 2022;12(1):18390. doi: 10.1038/s41598-022-22751-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.World Health Organization. Injuries and violence 2024 [19 June 2024]. Available from: https://www.who.int/news-room/fact-sheets/detail/injuries-and-violence. [Google Scholar]
- 3.World Health Organization. World Health Organization 2024 data, Mortality rate due to homicide (per 100 000 population) 2024. [13 June 2024]. Available from: https://data.who.int/indicators/i/60A0E76/361734E [Google Scholar]
- 4.Moore MH. Public Health and Criminal Justice Approaches to Prevention. Crime and Justice. 1995;19:237–62. doi: 10.1086/449232 [DOI] [Google Scholar]
- 5.Tiihonen J, Rautiainen MR, Ollila HM, Repo-Tiihonen E, Virkkunen M, Palotie A, et al. Genetic background of extreme violent behavior. Molecular Psychiatry. 2015;20(6):786–92. doi: 10.1038/mp.2014.130 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dabaghi N, Amini-Rarani M, Nosratabadi M. Investigating the relationship between socioeconomic status and domestic violence against women in Isfahan, Iran in 2021: A cross-sectional study. Health Science Reports. 2023;6(5):e1277. doi: 10.1002/hsr2.1277 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Plante C, Allen JJ, Anderson CA. Effects of Rapid Climate Change on Violence and Conflict. Oxford University Press; 2017. [Google Scholar]
- 8.Chen J-C, Schwartz J. Neurobehavioral effects of ambient air pollution on cognitive performance in US adults. NeuroToxicology. 2009;30(2):231–9. doi: 10.1016/j.neuro.2008.12.011 [DOI] [PubMed] [Google Scholar]
- 9.Berman JD, Burkhardt J, Bayham J, Carter E, Wilson A. Acute Air Pollution Exposure and the Risk of Violent Behavior in the United States. Epidemiology. 2019;30(6):799–806. doi: 10.1097/EDE.0000000000001085 00001648-201911000-00004. [DOI] [PubMed] [Google Scholar]
- 10.Yokota S, Moriya N, Iwata M, Umezawa M, Oshio S, Takeda K. Exposure to diesel exhaust during fetal period affects behavior and neurotransmitters in male offspring mice. The Journal of Toxicological Sciences. 2013;38(1):13–23. doi: 10.2131/jts.38.13 [DOI] [PubMed] [Google Scholar]
- 11.Allen JL, Liu X, Weston D, Prince L, Oberdörster G, Finkelstein JN, et al. Developmental Exposure to Concentrated Ambient Ultrafine Particulate Matter Air Pollution in Mice Results in Persistent and Sex-Dependent Behavioral Neurotoxicity and Glial Activation. Toxicological Sciences. 2014;140(1):160–78. doi: 10.1093/toxsci/kfu059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Xu R, Xiong X, Abramson MJ, Li S, Guo Y. Ambient temperature and intentional homicide: A multi-city case-crossover study in the US. Environment International. 2020;143:105992. doi: 10.1016/j.envint.2020.105992 [DOI] [PubMed] [Google Scholar]
- 13.Rahman MM, Lorenzo M, Ban-Weiss G, Hasan Z, Azzouz M, Eckel SP, et al. Ambient temperature and air pollution associations with suicide and homicide mortality in California: A statewide case-crossover study. Science of The Total Environment. 2023;874:162462. doi: 10.1016/j.scitotenv.2023.162462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nguyen A-M, Malig BJ, Basu R. The association between ozone and fine particles and mental health-related emergency department visits in California, 2005–2013. PloS one. 2021;16(4):e0249675. doi: 10.1371/journal.pone.0249675 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Younan D, Tuvblad C, Franklin M, Lurmann F, Li L, Wu J, et al. Longitudinal Analysis of Particulate Air Pollutants and Adolescent Delinquent Behavior in Southern California. Journal of Abnormal Child Psychology. 2018;46(6):1283–93. doi: 10.1007/s10802-017-0367-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.OECD. Health at a Glance 20232023. [Google Scholar]
- 17.Cai Y, Rafi A. On the performance of the Neyman Allocation with small pilots. Journal of Econometrics. 2024;242(1):105793. 10.1016/j.jeconom.2024.105793. [DOI] [Google Scholar]
- 18.Kim Y, Oh J, Kim S, Kim A, Park J, Ahn S, et al. Relationship between short-term ozone exposure, cause-specific mortality, and high-risk populations: a nationwide, time-stratified, case-crossover study. Environmental Research. 2024:119712. doi: 10.1016/j.envres.2024.119712 [DOI] [PubMed] [Google Scholar]
- 19.Min J, Lee W, Kang D-H, Ahn S, Kim A, Kang C, et al. Air pollution and acute kidney injury with comorbid disease: A nationwide case-crossover study in South Korea. Environmental Research. 2024;260:119608. doi: 10.1016/j.envres.2024.119608 [DOI] [PubMed] [Google Scholar]
- 20.Buontempo C, Burgess SN, Dee D, Pinty B, Thépaut J-N, Rixen M, et al. The Copernicus climate change service: climate science in action. 2022;103(12):E2669–E87. [Google Scholar]
- 21.Wei Y, Wang Y, Di Q, Choirat C, Wang Y, Koutrakis P, et al. Short term exposure to fine particulate matter and hospital admission risks and costs in the Medicare population: time stratified, case crossover study. BMJ. 2019;367:l6258. doi: 10.1136/bmj.l6258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Levy D, Lumley T, Sheppard L, Kaufman J, Checkoway H. Referent Selection in Case-Crossover Analyses of Acute Health Effects of Air Pollution. Epidemiology. 2001;12(2):186–92. doi: 10.1097/00001648-200103000-00010 -200103000-00010. [DOI] [PubMed] [Google Scholar]
- 23.Wellenius GA, Burger MR, Coull BA, Schwartz J, Suh HH, Koutrakis P, et al. Ambient Air Pollution and the Risk of Acute Ischemic Stroke. Archives of Internal Medicine. 2012;172(3):229–34. doi: 10.1001/archinternmed.2011.732 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zanobetti A, Dominici F, Wang Y, Schwartz JD. A national case-crossover analysis of the short-term effect of PM2.5 on hospitalizations and mortality in subjects with diabetes and neurological disorders. Environmental Health. 2014;13(1):38. doi: 10.1186/1476-069X-13-38 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sun S, Weinberger KR, Nori-Sarma A, Spangler KR, Sun Y, Dominici F, et al. Ambient heat and risks of emergency department visits among adults in the United States: time stratified case crossover study. BMJ. 2021;375:e065653. doi: 10.1136/bmj-2021-065653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Park J, Kim A, Kim Y, Choi M, Yoon TH, Kang C, et al. Association between heat and hospital admissions in people with disabilities in South Korea: a nationwide, case-crossover study. The Lancet Planetary Health. 2024;8(4):e217–e24. doi: 10.1016/S2542-5196(24)00027-5 [DOI] [PubMed] [Google Scholar]
- 27.Lee W, Wu X, Heo S, Kim Joyce M, Fong Kelvin C, Son J-Y, et al. Air Pollution and Acute Kidney Injury in the U.S. Medicare Population: A Longitudinal Cohort Study. Environmental Health Perspectives. 2023;131(4):047008. doi: 10.1289/EHP10729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sun Y, Milando CW, Spangler KR, Wei Y, Schwartz J, Dominici F, et al. Short term exposure to low level ambient fine particulate matter and natural cause, cardiovascular, and respiratory morbidity among US adults with health insurance: case time series study. BMJ. 2024;384:e076322. doi: 10.1136/bmj-2023-076322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kim Y, Ng CFS, Chung Y, Kim H, Honda Y, Guo YL, et al. Air Pollution and Suicide in 10 Cities in Northeast Asia: A Time-Stratified Case-Crossover Analysis. Environmental Health Perspectives. 2018;126(3):037002. doi: 10.1289/EHP2223 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Park J, Kim A, Bell ML, Kim H, Lee W. Heat and hospital admission via the emergency department for people with intellectual disability, autism, and mental disorders in South Korea: a nationwide, time-stratified, case-crossover study. The Lancet Psychiatry. 2024;11(5):359–67. doi: 10.1016/S2215-0366(24)00067-1 [DOI] [PubMed] [Google Scholar]
- 31.Kang C, Park C, Lee W, Pehlivan N, Choi M, Jang J, et al. Heatwave-Related Mortality Risk and the Risk-Based Definition of Heat Wave in South Korea: A Nationwide Time-Series Study for 2011–2017. International Journal of Environmental Research and Public Health. 2020;17(16):5720. doi: 10.3390/ijerph17165720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cook A, Sheikh A. Descriptive statistics (Part 2): Interpreting study results. Primary Care Respiratory Journal. 2000;8(1):16–7. doi: 10.1038/pcrj.2000.6 [DOI] [Google Scholar]
- 33.Lee W, Prifti K, Kim H, Kim E, Yang J, Min J, et al. Short-term Exposure to Air Pollution and Attributable Risk of Kidney Diseases: A Nationwide Time-series Study. Epidemiology. 2022;33(1). [DOI] [PubMed] [Google Scholar]
- 34.Dahlberg LL, Mercy JA. The history of violence as a public health issue. 2009. [DOI] [PubMed] [Google Scholar]
- 35.OECD/Eurostat. Avoidable mortality: OECD/Eurostat lists of preventable and treatable causes of death (November 2019 version). 2019. [Google Scholar]
- 36.Mahendran R, Xu R, Li S, Guo Y. Interpersonal violence associated with hot weather. The Lancet Planetary Health. 2021;5(9):e571–e2. doi: 10.1016/S2542-5196(21)00210-2 [DOI] [PubMed] [Google Scholar]
- 37.Heo S, Choi HM, Lee J-T, Bell ML. A nationwide time-series analysis for short-term effects of ambient temperature on violent crime in South Korea. Scientific Reports. 2024;14(1):3210. doi: 10.1038/s41598-024-53547-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Jung J, Kim G, Kang S-W, Jeong S, Kang Y, Lee J-Y, et al. Short-term exposure to ambient air pollution and injuries due to external causes according to intentions and mechanisms. Science of the total environment. 2024;912:169202. doi: 10.1016/j.scitotenv.2023.169202 [DOI] [PubMed] [Google Scholar]
- 39.Calderón-Garcidueñas L, Kulesza RJ, Doty RL, D’Angiulli A, Torres-Jardón R. Megacities air pollution problems: Mexico City Metropolitan Area critical issues on the central nervous system pediatric impact. Environmental research. 2015;137:157–69. doi: 10.1016/j.envres.2014.12.012 [DOI] [PubMed] [Google Scholar]
- 40.Kristiansson M, Sörman K, Tekwe C, Calderón-Garcidueñas L. Urban air pollution, poverty, violence and health–Neurological and immunological aspects as mediating factors. Environmental research. 2015;140:511–3. doi: 10.1016/j.envres.2015.05.013 [DOI] [PubMed] [Google Scholar]
- 41.Gładka A, Rymaszewska J, Zatoński T. Impact of air pollution on depression and suicide. International journal of occupational medicine and environmental health. 2018;31(6):711–21. doi: 10.13075/ijomeh.1896.01277 [DOI] [PubMed] [Google Scholar]
- 42.Fleming PJ, Gruskin S, Rojo F, Dworkin SL. Men’s violence against women and men are inter-related: Recommendations for simultaneous intervention. Social science & medicine. 2015;146:249–56. doi: 10.1016/j.socscimed.2015.10.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Pleck JH. The gender role strain paradigm: An update. 1995. [Google Scholar]
- 44.Clougherty JE. A growing role for gender analysis in air pollution epidemiology. Environmental health perspectives. 2010;118(2):167–76. doi: 10.1289/ehp.0900994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kan H, London SJ, Chen G, Zhang Y, Song G, Zhao N, et al. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environmental health perspectives. 2008;116(9):1183–8. doi: 10.1289/ehp.10851 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Parker RN, Auerhahn K. Alcohol, drugs, and violence. Annual review of sociology. 1998;24(1):291–311. [Google Scholar]
- 47.Ventura‐Cots M, Watts AE, Cruz‐Lemini M, Shah ND, Ndugga N, McCann P, et al. Colder weather and fewer sunlight hours increase alcohol consumption and alcoholic cirrhosis worldwide. Hepatology. 2019;69(5):1916–30. doi: 10.1002/hep.30315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Lloyd B, Matthews S, Livingston M, Jayasekara H, Smith K. Alcohol intoxication in the context of major public holidays, sporting and social events: a time–series analysis in M elbourne, A ustralia, 2000–2009. Addiction. 2013;108(4):701–9. doi: 10.1111/add.12041 [DOI] [PubMed] [Google Scholar]
- 49.Lee W, Kang C, Park C, Bell ML, Armstrong B, Roye D, et al. Association of holidays and the day of the week with suicide risk: multicountry, two stage, time series study. BMJ. 2024;387:e077262. doi: 10.1136/bmj-2024-077262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Sacco P, Bucholz KK, Spitznagel EL. Alcohol use among older adults in the National Epidemiologic Survey on Alcohol and Related Conditions: A latent class analysis. Journal of studies on alcohol and drugs. 2009;70(6):829–38. doi: 10.15288/jsad.2009.70.829 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kim D, Jeong J, Ko Y, Kwon Y, Kim YT. The construction of database of community health outcomes and health determinants in the Republic of Korea. Public Health Wkly Rep KCDC. 2018;(11):979–83. [Google Scholar]
- 52.Guo Y, Gasparrini A, Armstrong B, Li S, Tawatsupa B, Tobias A, et al. Global variation in the effects of ambient temperature on mortality: a systematic evaluation. Epidemiology. 2014;25(6):781–9. doi: 10.1097/EDE.0000000000000165 [DOI] [PMC free article] [PubMed] [Google Scholar]