

Abstract
Background
Under-five mortality in Tanzania remains a persistent issue, significantly affecting both the health and economic sectors. Despite various interventions, the under-five mortality rate (U5MR) remains high, impeding progress toward global health targets. This study investigates the factors influencing under-five mortality in Tanzania, focusing on the gross domestic product (GDP), malaria incidence, access to water, and access to sanitation.
Methods
The study employed data sets for Tanzania U5MR, GDP, access to water and sanitation, and malaria incidences from the World Bank for the years 1960–2020. Missing values are generated through the linear trend at point method. To analyses the data, correlation analysis and Bayesian linear regression are employed.
Results
The analysis reveals significant relationships between the gross domestic product (GDP), malaria incidence, access to water, access to sanitation and under-five mortality. Furthermore, an increase in malaria incidences increase under-five mortality by 0.14 (14%), while access to water and sanitation exhibit an uncertain relationship. On the other hand, results show that an increase in the GDP lowers the likelihood of U5MR.
Conclusion
These findings underscore the importance of economic development and public health interventions in reducing the child mortality rate. The study provides valuable insights for policymakers aiming to achieve Sustainable Development Goal (SDG) Target 3.2 by 2030, which aims for all countries to accomplish U5MR of 25 or less deaths per 1000 live births. By highlighting the relationships between these variables, the study contributes practical evidence to support efforts towards SDG 3.2, emphasizing the need for targeted interventions in both health and infrastructure sectors.
Keywords: Under-five, Mortality, Tanzania, GDP, Malaria, Sustainable, Development Goals
Background
Under-five mortality (U5M) is a key indicator of public health and socioeconomic well-being. Globally, millions of children under five die annually from preventable causes, such as diarrhea, pneumonia, and malaria. These deaths are often linked to socioeconomic factors, including maternal education, household wealth, and access to clean water and sanitation [1–3]. Addressing U5M is essential for achieving the Sustainable Development Goals (SDGs), particularly SDG 3.2, which targets ending preventable deaths of children under five by 2030 [4].
The under-five mortality rate (U5MR) decreased globally from 93 per 1000 live births in 1990 to 39 in 2017, but sub-Saharan Africa has the highest rate of U5MR of 76 per 1000 live births [5, 6]. About 80% of U5M commonly occur in sub-Saharan Africa, where the mortality problem of children under five is still high and unevenly distributed [4, 7, 8]. In Tanzania, despite a 54% reduction in U5MR between 1999 and 2015, child mortality remains a persistent challenge, driven by economic and healthcare inequalities [9]. U5MR has decreased as a result of macro- and microeconomic expansion, a low fertility rate, increased female education, and reinforced public health initiatives [10].
Several studies have examined the factors influencing under-five mortality both in sub-Saharan Africa and globally. A wide range of determinants have been identified, including socioeconomic, demographic, and health-related factors. Parental education, particularly maternal education, has been consistently shown to reduce child mortality by improving health practices and access to care. Some studies have emphasized the positive impact of maternal education on reducing U5M, particularly in regions with limited healthcare infrastructure [11, 12].
Additionally, maternal age, socioeconomic status, birth order, birth interval, and birth weight have also been identified as significant predictors of child mortality across different contexts [13–15]. Other studies highlight the importance of geographic and household characteristics [16–18]. The place and region of residence, gender of the child, and family structure such as the number of births in the last year and the number of children under five are associated with variations in U5M. Dejene and Girma [16] found that children living in rural areas or from larger households tend to have a higher risk of mortality due to reduced access to healthcare and economic constraints, which was also highlighted in [17, 19]. Similar regional disparities in U5M within sub-Saharan Africa are noted in [18, 20].
Furthermore, maternal and household characteristics, such as the place of delivery, previous death of siblings, marital status, and breastfeeding practices, have been identified as key predictors of child mortality. Breastfeeding significantly reduces the risk of under-five mortality (U5M) [21, 22], while marital stability also plays a crucial role in improving child survival rates [23]. Additionally, effective household management and healthy family dynamics are vital factors influencing positive child health outcomes, as highlighted in previous studies [24, 25]
Environmental factors such as access to electricity, clean water, safe sanitation, indoor air pollution and domestic factors such as household size, domestic violence have also been linked to U5M. Inadequate sanitation and air quality could increase the risk of infectious diseases, which are leading causes of child mortality in low-resource settings [11, 26, 27]. Additionally, Wang [28] and Hossain et al. [29] provide evidence that improving household amenities can mitigate these risks and significantly lower child mortality rates. The use of health and family planning services has been shown to have a significant impact on reducing child mortality [12, 25]. In fact, access to healthcare services, including family planning and maternal health services, is strongly associated with lower U5M rates, especially in sub-Saharan Africa [30, 31]. These studies underscore the need for integrated health interventions targeting both maternal and child health to effectively reduce mortality rates.
However, studies focusing specifically on Tanzania are limited, especially regarding the role of broader economic and health indicators. This gap in the literature highlights the need for a deeper understanding of the factors that influence U5M in Tanzania. This study aims to address this research gap by investigating the key factors influencing U5M in Tanzania. This study contributes to the existing literature by utilizing a Bayesian linear regression model to analyse the relationship between Gross Domestic Product (GDP), access to water and Sanitation, malaria incidences and U5M.
Methods
The data set for Tanzania U5MR, Gross Domestic Product (GDP), access to water and Sanitation and malaria incidences from World Bank for the year 1960 to 2020 was considered [32]. The study focuses on four key determinants of under-five mortality (U5M) in Tanzania: GDP, access to water, access to sanitation, and malaria incidences. The GDP represents economic health, correlating with improved healthcare and reduced child mortality. Access to water and sanitation helps prevent waterborne diseases, while malaria remains a major child health risk with high mortality and morbidity in children under five [33]. These variables were selected based on data availability and their significance in global and Tanzanian contexts. To generate missing values, a linear trend at point method was used. Though it assumes a linear pattern, which may not always hold, it was chosen for its simplicity and relevance to the study’s time-series data. This approach aligns with the expected trends in GDP, water access, sanitation, and malaria incidences.
Conceptual framework
The conceptual framework in Fig. 1 illustrates the relationships among GDP, access to water and sanitation, malaria incidence, and under-five mortality. GDP is hypothesized to influence under-five mortality positively, as higher economic growth often leads to improved healthcare access and better living conditions. Access to clean water and sanitation is expected to reduce waterborne diseases, thereby decreasing child mortality rates. Malaria incidence is directly linked to under-five mortality, with higher rates of malaria leading to increased health risks for young children.
Fig. 1.
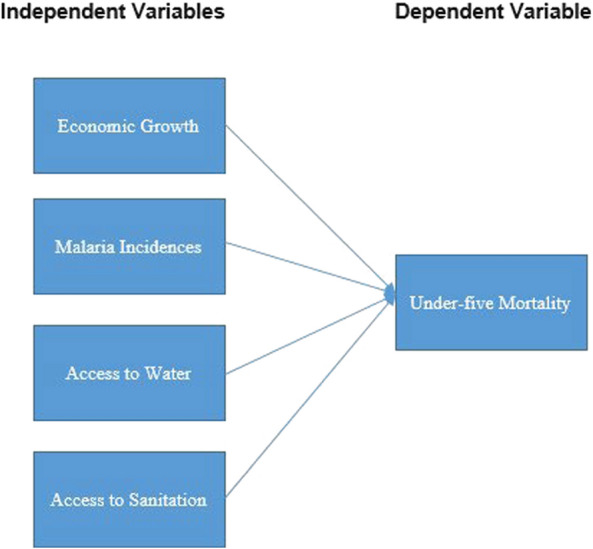
Conceptual framework
Correlation analysis
The Pearson correlation coefficient (r) which is the most common way of measuring a linear correlation was used. This calculates (quantifies the correlation between two variables) the unit to which the raw data from both variables have linear relationships. The formula is given by:
| 1 |
Bayesian linear regression
A statistical technique called regression analysis builds the estimation model by estimating the relationship between the independent variable (s) and the dependent variable [34, 35]. Bayesian linear regression is a probabilistic approach to linear regression that incorporates uncertainty into the model’s parameters and predictions [36, 37]. Bayes’ Theorem is used to update prior distributions with observed data to obtain posterior distributions for the coefficients. This Theorem expresses the posterior probability in terms of the prior probability and the conditional probability [38, 39].
Bayesian linear regression was chosen for its capacity to incorporate prior information and address uncertainty in parameter estimates. Unlike traditional regression, it generates posterior distributions, providing a better understanding of variable relationships. Bayesian linear regression model is used to show how different factors influence under-five mortality. Factors used are GDP, incidence of malaria, access to water and access to sanitation. Bayesian linear regression has the form [37]:
| 2 |
where y is the outcome variable while X is the matrix of predictor variables (features), β is a k × 1 vector of coefficients (parameters) we want to estimate, and ϵ represents the error term normally distributed that is:
| 3 |
For normally distributed errors, the likelihood function is often taken as
| 4 |
where N (µ, σ2I) is the multivariate normal distribution with mean µ and covariance matrix σ2I. The posterior distribution is denoted as
| 5 |
Results
Correlation analysis
Figure 2 illustrates the relationship between under-five mortality and GDP, malaria incidences, access to water, and access to sanitation. There is a strong positive correlation (0.985) between the incidence of malaria incidence and U5MR. Due to the serious health effects of malaria on young children, this result suggests that populations with higher rates of malaria case incidence also tend to have higher mortality rate among those under five, which agrees with WHO estimate that tropical and sub-tropical regions where malaria is endemic carry a disproportionately high share of the global malaria burden: 95% of malaria cases, 96% of malaria deaths of which about 76% are children less than 5 years of age with [40].
Fig. 2.

Correlation analysis
Access to water and under-five mortality have a very strong negative relationship, as indicated by the negative correlation coefficient of − 0.985. In this instance, it implies that the mortality rate for children under five drops dramatically with increased access to clean water. This suggests that communities with greater access to sources of clean water typically have lower rates of mortality among children under five, which makes sense given the importance of clean water for sanitation and child health. Access to sanitation and U5M have a very strong negative correlation, as indicated by the correlation coefficient of − 0.985. It indicates that the under-five mortality rate dramatically declines with improved access to sanitation facilities. Thus, lower rates of under-five mortality are typically found in areas with better sanitation facilities, which makes sense given that good sanitation can lower the risk of infections and diseases spread by water such as cholera (Fig. 2).
Furthermore, a strong negative correlation between a nation’s GDP and under five mortality is indicated by the negative correlation coefficient of − 0.839. That is, a nation’s under-five mortality rate tends to decline as its GDP rises. As a result of improved living conditions, healthcare, and nutrition, it appears that countries with higher economic wealth tend to have lower rates of under-five mortality. Although access to water and sanitation show strong negative correlations with U5M, the Bayesian regression analysis reveals wide confidence intervals for these variables, indicating significant uncertainty in their actual effect on child mortality.
Bayesian regression analysis
Analysis of trace plots for Bayesian linear regression model
Figure 3 depicts the trace plots for the Bayesian linear regression model, which assesses the convergence and mixing of the Markov Chain Monte Carlo (MCMC) samples. The trace plots show that the MCMC chains have reached a stationary state, indicating that the model has sufficiently explored the entire posterior distribution. Good mixing is observed, as the parameter values move freely without getting stuck in any specific region, suggesting that the model has converged to a reliable estimate of the posterior distribution. This convergence confirms the robustness of the results, as the posterior distributions are stable and represent the true underlying relationships between the variables.
Fig. 3.

Trace plots for Bayesian linear regression model
Model coefficients estimates
Table 1 presents the results of the Bayesian regression analysis using a Gaussian family distribution to examine the factors influencing mortality among children under five. With a wide uncertainty range shown by the 95% confidence interval (− 2163.87,1392.93), the intercept (constant variable), which represents the estimated baseline under-five mortality when all predictor variables are zero, was found to be − 380.03. The positive estimate for malaria incidences (0.14), which is reflected in a narrow confidence interval, indicates that an increase in malaria incidence is linked to a corresponding rise in mortality among children under five. Though the large confidence interval indicates significant uncertainty in the relationship, improved access to water (Estimate: 23.00) demonstrated a positive association with under-five mortality.
Table 1.
Bayesian linear regression
| Draws: 4 chains, each with iter = 15000; warmup = 500; thin = 1 | |||||
|---|---|---|---|---|---|
| Total post-warmup draws = 58000 | |||||
| Estimate | Est. Error | l-95% CI | u-95% CI | Rhat | |
| Intercept | −380.03 | 900.5 | −2163.8 | 1392.93 | 1 |
| Malaria incidence | 0.14 | 0.07 | 0 | 0.28 | 1 |
| Access to water | 23 | 43.99 | −63.6 | 110.13 | 1 |
| Access to sanitation | −29.76 | 54.62 | −137.97 | 77.72 | 1 |
| GDP | −1.9 | 1.08 | −4 | 0.25 | 1 |
On the other hand, there was a negative correlation between under-five mortality and improved access to sanitation (estimate: − 29.76). The relationship is uncertain, as indicated by the wide confidence interval. Despite access to water and sanitation showing strong correlations in the earlier analysis, the Bayesian regression reveals that the true effects of these variables may vary widely, likely due to other complex interacting factors or the nature of the data. This uncertainty suggests that while water and sanitation are crucial for child health, their impact on mortality may not be as straightforward or consistent across different contexts. With a relatively narrow confidence interval, the negative GDP estimate (− 1.90) indicates that there is a positive correlation between GDP growth and lower under-five mortality. Effective sample sizes and Rhat values near 1.00 support the overall convergence to a stable solution of the model, ensuring the reliability and accuracy of the results. Based on the results, only malaria incidences and GDP were found to have effects on under-five mortality due to the narrow confidence interval, which indicates a significant relationship. Access to water and to sanitation show a relationship with under-five mortality during correlation analysis but show an uncertainty relationship in Bayesian linear regression due to the wide confidence interval.
Discussion
Mortality of children under the age of five from preventable causes is a major challenge worldwide. Addressing critical causes of U5M is an essential component for achieving the SDGs. Key factors influencing under-five mortality (U5M) in Tanzania and their correlations are highlighted herein, providing insights that can inform targeted policy interventions. A major finding is the negative relationship between GDP and U5M, underscoring the role of economic development in improving child health. As the economy grows, it enables better healthcare infrastructure, improved living conditions, and greater access to essential services, all of which contribute to reducing child mortality. This aligns with prior research, such as Rahman et al. [41], which similarly found that higher GDP leads to better health outcomes by increasing resources allocated to healthcare. These results support the need for sustained economic policies aimed at equitable growth and poverty reduction, especially in regions with high child mortality rates.
The study also highlights a strong positive association between malaria incidence and U5M, pointing to the urgent need for robust malaria control measures. Malaria remains a major health risk for children in Tanzania, and the study’s results reinforce the importance of expanding malaria prevention strategies such as insecticide-treated bed nets, indoor residual spraying, and timely treatment of infections. This echoes Van Malderen et al. [2], who also identified malaria as a significant contributor to child mortality. The study suggests that reducing malaria infection rate could substantially improve child survival and general public health in Tanzania.
The impact of access to water and sanitation on U5M is more uncertain in this study, despite strong correlation, but an uncertainty relationship in Bayesian linear regression due to the wide confidence interval. While access to clean water and sanitation is widely regarded as critical for preventing waterborne diseases, the regression results suggest that their effects on child mortality might be influenced by other intervening variables or socio-economic factors. This contrasts with studies like those by Dendup et al. [1] and Sharow et al. [4], which emphasized sanitation as a key determinant of child survival. The results imply that improving water and sanitation alone may not suffice in reducing U5M without addressing broader health and socio-economic challenges, such as poverty, education, and access to healthcare.
Policy implication
The study highlights key policy implications for reducing under-five mortality (U5M) in Tanzania, with a focus on economic development, malaria control, and improvements in water and sanitation infrastructure. Promoting inclusive economic growth is essential, as higher GDP correlates with lower U5M, while scaling up malaria prevention programs is crucial due to the significant link between malaria incidence and child mortality. Despite uncertainty in the relationship between water, sanitation, and U5M, improving access to these services remains important for public health and aligns with SDG 6 (Clean Water and Sanitation). Strengthening healthcare infrastructure, enhancing data collection, and fostering cross-sectoral collaboration are also vital for achieving SDG Target 3.2 and reducing preventable child deaths.
Strength and limitation of the study
The study’s strengths lie in its extensive 60-year dataset and the use of rigorous analytical methods, offering valuable insights into the relationship between under-five mortality (U5M) and key factors like GDP, malaria incidence, and access to water and sanitation. These could potentially provide actionable, context-specific policy recommendations for Tanzania. However, limitations include potential biases from missing data, particularly for water and sanitation access, and the uncertain nature of these variables’ effects on U5M, warranting further investigation. While the Tanzania-specific focus might limit generalizability, it enhances the study’s relevance for localized policymaking, with potential for comparative studies across similar regions especially developing countries. Bayesian linear regression model provides a probabilistic framework that incorporates prior knowledge and is more resilient to outliers, making it particularly effective for analysing incomplete or uncertain data.
Conclusion
Malaria incidence and GDP are the primary predictors of under-five mortality in Tanzania, with a positive correlation between malaria cases and child mortality, and a negative correlation between GDP and child deaths. While access to water and sanitation showed uncertainty in the Bayesian regression, this should not diminish the importance of improving these services for broader public health. To reduce under-five mortality, future policies should focus on scaling up malaria prevention efforts, such as the distribution of insecticide-treated nets and access to anti-malarial treatments, as well as promoting economic growth through investments in healthcare, education, and infrastructure. For future research, deeper investigation into specific interventions for water and sanitation and the inclusion of other socioeconomic factors could provide additional insights. A comprehensive approach combining health, economic, and infrastructure policies is key to achieving reductions in child mortality and meeting the Sustainable Development Goals (SDGs).
Abbreviations
- GDP
Gross domestic product
- MCMC
Markov Chain Monte Carlo
- SDG
Sustainable development goal
- U5M
Under five mortality
- U5MR
Under five mortality rate
- UN
United Nations
- WHO
World Health Organization
Author contributions
M.K.M, S.S.M, J.M.T and I.S.M participated in conceptualization, wrote the main manuscript text, data analysis S.S.M. J.M.T and I.S.M participated in Supervision.
Funding
Not applicable.
Availability of data and materials
No datasets were generated or analysed during the current study.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Dendup T, Zhao Y, Dema D. Factors associated with under-five mortality in Bhutan: an analysis of the Bhutan national health survey 2012. BMC Public Health. 2018;18:1375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Van Malderen C, Amouzou A, Barros AJ, Masquelier B, Van Oyen H, Speybroeck N. Socioeconomic factors contributing to under-five mortality in sub-Saharan Africa: a decomposition analysis. BMC Public Health. 2019;19:760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.WHO. Global health observatory. Geneva: World Health Organization; 2013. [Google Scholar]
- 4.Sharrow D, Hug L, You D, Alkema L, Black R, Cousens S, et al. Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the un inter-agency group for child mortality estimation. Lancet Glob Health. 2022;10:e195–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.UN Inter-agency Group for Child Mortality Estimation. Levels & trends in child mortality report. Technical Report, 2018. https://www.unicef.org/reports/levels-and-trendschild-mortality-report-2018. Accessed 8 July 2024.
- 6.Wang H, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, et al. Global, regional, and national under-5 mortality, adult mortality, age-specific mortality, and life expectancy, 1970–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390:1084–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gebremichael SG, Fenta SM. Under-five mortality and associated risk factors in rural settings of Ethiopia: evidences from 2016 Ethiopian demographic and health survey. Adv Public Health. 2020;2020:8430246. [Google Scholar]
- 8.Memiah P, Bond T, Opanga Y, Kingori C, Cook C, Mwangi M, et al. Neonatal, infant, and child mortality among women exposed to intimate partner violence in East Africa: a multi-country analysis. BMC Women’s Health. 2020;20:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ogbo FA, Ekundayo O, Awosemo AO. Determinants of trends in neonatal, postneonatal, infant, child, and under-five mortalities in Tanzania from 2004 to 2016. BMC Public Health. 2019;19:1243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dieleman J, Murray C, Case M. Financing global health 2016: development assistance, public and private health spending for the pursuit of universal health coverage. Seattle: Institute for Health Metrics and Evaluation, University of Washington; 2017. [Google Scholar]
- 11.Akinyemi JO, Bamgboye EA, Ayeni O. New trends in under-five mortality determinants and their effects on child survival in Nigeria: a review of childhood mortality data from 1990–2008. Afr Popul Studies. 2013;27:25–42. [Google Scholar]
- 12.Chowdhury AH. Determinants of under-five mortality in Bangladesh. Open J Stat. 2013;3:213–9. [Google Scholar]
- 13.Dadi AF. A systematic review and meta-analysis of the effect of short birth interval on infant mortality in Ethiopia. PLoS ONE. 2015;10:e0126759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ezeh AK, Agho KE, Dibley MJ, Hall JJ, Page AN. Risk factors for postneonatal, infant, child, and under-5 mortality in Nigeria: a pooled cross-sectional analysis. BMJ Open. 2015;5:e006779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kanmiki EW, Bawah AA, Agorinya I, Achana FS, Awoonor-Williams JK, Oduro AR, et al. Socio-economic and demographic determinants of under-five mortality in rural northern Ghana. BMC Int Health Human Rights. 2014;14:24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dejene T, Girma E. Social determinants of under-five mortality in Ethiopia: event history analysis using evidence from Ethiopian demographic and health survey (EDHS). Health. 2013;5:879–84. [Google Scholar]
- 17.Adhikari R, Podhisita C. Household headship and child death: evidence from Nepal. BMC Int Health Hum Rights. 2010;10:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lee H-Y, Van Do D, Choi S, Trinh O, To K. Trends and determinants of infant and under-five childhood mortality in Vietnam, 1986–2011. Glob Health Action. 2016;9:29312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kitole FA, Shukla S. Cloud horizons: strengthening rural healthcare through telemedicine’s digital canopy. Health Serv Insights. 2024;17:11786329241284400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nasejje J, Mwambi H, Achia T. Understanding the determinants of under-five child mortality in Uganda including the estimation of unobserved household and community effects using both frequentist and Bayesian survival analysis approaches. BMC Public Health. 2015;15:1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Singh R, Tripathi V. Maternal factors contributing to under-five mortality at birth order 1 to 5 in India: a comprehensive multivariate study. Springerplus. 2013;2:284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Worku Z. Factors that affect under-five mortality among South African children: analysis of the South African demographic and health survey data set. Presented at: World Congress on Engineering and Computer Science; October 20–22, 2009; San Francisco, USA.
- 23.Mani K, Dwivedi SN, Pandey RM. Determinants of under-five mortality in rural empowered action group states in India: an application of Cox frailty model. Int J Matern Child Health AIDS. 2012;1:60–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Abir T, Agho KE, Page AN, Milton AH, Dibley MJ. Risk factors for under-5 mortality: evidence from Bangladesh Demographic and Health Survey, 2004–2011. BMJ Open. 2015;5:e006722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Singh R, Tripathi V. Under-five mortality among mothers employed in agriculture: findings from a nationally representative sample. PeerJ. 2015;3:e710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kayode GA, Adekanmbi VT, Uthman OA. Risk factors and a predictive model for under-five mortality in Nigeria: evidence from Nigeria Demographic and Health Survey. BMC Pregnancy Childbirth. 2012;12:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Charmarbagwala R, Ranger M, Waddington H, White H. The determinants of child health and nutrition: a meta-analysis. Washington, DC: World Bank; 2004. [Google Scholar]
- 28.Wang L. Determinants of child mortality in LDCS: empirical findings from demographic and health surveys. Health Policy. 2003;65:277–99. [DOI] [PubMed] [Google Scholar]
- 29.Hossain MA, Sumi NS, Haque ME, Bari W. Consequences of intimate partner violence against women on under-five child mortality in Bangladesh. J Interpers Violence. 2013;29:1402–17. [DOI] [PubMed] [Google Scholar]
- 30.Chola L, McGee S, Tugendhaft A, Buchmann E, Hofman K. Scaling up family planning to reduce maternal and child mortality: the potential costs and benefits of modern contraceptive use in South Africa. PLoS ONE. 2015;10:e0130077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Askew I, Raney L, Kerrigan M, Sridhar A. Family planning saves maternal and newborn lives: why universal access to contraception must be prioritized in national maternal and newborn health policies, financing, and programs. Int J Gynaecol Obstet. 2024;164:536–40. [DOI] [PubMed] [Google Scholar]
- 32.World Bank. World development indicators. Washington, DC: World Bank Group; 2021. [Google Scholar]
- 33.Tchoumi S, Chukwu C, Diagne M, Rwezaura H, Juga M, Tchuenche J. Optimal control of a two-group malaria transmission model with vaccination. Netw Model Anal Health Inform Bioinform. 2023;12:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kurt R, Karayilmazlar S, Cabuk Y. Important non-wood forest products in Turkey: an econometric analysis. Eng Technol Appl Sci Res. 2016;6:1245–8. [Google Scholar]
- 35.Jackman S. Bayesian analysis for the social sciences. Hoboken: John Wiley & Sons; 2009. [Google Scholar]
- 36.Zeileis A, Kleiber C, Jackman S. Regression models for count data in R. J Stat Softw. 2008;27:1–25. [Google Scholar]
- 37.Permai SD, Tanty H. Linear regression model using Bayesian approach for energy performance of residential building. Procedia Comput Sci. 2018;135:671–7. [Google Scholar]
- 38.Theofilatos K, Likothanassis S, Karathanasopoulos A. Modeling and trading the EUR/USD exchange rate using machine learning techniques. Eng Technol Appl Sci Res. 2012;2:269–72. [Google Scholar]
- 39.Fahmi FH, Al-Zaidee S. Strength and deflection reliability estimation of girder steel portal frames using the Bayesian updating method. Eng Technol Appl Sci Res. 2022;12:9584–9. [Google Scholar]
- 40.WHO. World malaria report 2023. Geneva: World Health Organization; 2023. [Google Scholar]
- 41.Rahman MA, Alam K, Khanam R. Socio-economic factors affecting high infant and child mortality rates in selected African countries: does globalization play any role? Glob Health. 2022;18:69. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
No datasets were generated or analysed during the current study.